Back to Journals » Therapeutics and Clinical Risk Management » Volume 16
Inter-Gender Pelvic Shape Variations as a Cause of DDH Overdiagnosis
Authors Abdalla KM ![]() , Abdelrahman MA
, Abdelrahman MA ![]() , Aleshawi AJ, Al Taweel AS
, Aleshawi AJ, Al Taweel AS ![]() , Bani-Ata M, Obeidat K
, Bani-Ata M, Obeidat K ![]()
Received 8 June 2020
Accepted for publication 10 October 2020
Published 10 November 2020 Volume 2020:16 Pages 1075—1080
DOI https://doi.org/10.2147/TCRM.S265038
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Khalid M Abdalla,1 Mostafa A Abdelrahman,2 Abdelwahab J Aleshawi,3 Alaha S Al Taweel,1 Majid Bani-Ata,4 Khaled Obeidat5
1Department of Diagnostic Radiology and Nuclear Medicine, Faculty of Medicine, Jordan University of Science and Technology, Irbid 22110, Jordan; 2Department of Allied Medical Sciences, Faculty of Applied Medical Sciences, Jordan University of Science and Technology, Irbid 22110, Jordan; 3Department of Special Surgery, Ophthalmology Division, Jordan University of Science and Technology, Irbid 22110, Jordan; 4Department of Special Surgery, Otolaryngology Division, Faculty of Medicine, Jordan University of Science and Technology, Irbid 22110, Jordan; 5Department of General Surgery, Faculty of Medicine, Jordan University of Science and Technology, Irbid 22110, Jordan
Correspondence: Khalid M Abdalla
Department of Diagnostic Radiology and Nuclear Medicine, Faculty of Medicine, Jordan University of Science and Technology, P. O. Box: 3030, Irbid 22110, Jordan
Tel +962 799273019
Fax +962 2 7201064
Email [email protected]
Objective: Developmental dysplasia of the hip (DDH) is an abnormal relationship between the acetabulum and the head of the femur. Plain x-ray of both hips at the age of 3 months is still in use in some countries. On plain films, classic lines and angles are evaluated to meet current guidelines for positive DDH. Among these is the acetabular angle (AA), which most did not exceed 30° in normal pelvis regardless of gender. A flat promontory gives the impression of a high AA angle, whereas a sharp promontory gives the impression of a low AA angle.
Materials and Methods: All anteroposterior (AP) pelvic digital x-ray studies performed to rule out DDH were collected from the PACS systems. A novel angle was measured between a line parallel to the lateral aspect of the region of the inferior iliac spines and a line that extends along the acetabular roof to quantify the roundness of the iliac promontory. We called the former line the Miral line and the formed angle the iliac promontory angle.
Results: We show that the promontory shape is significantly different between genders, and therefore it is mistaken to generalize an upper AA limit for males and females. In addition, we show that the current guideline of the upper limit of AA did not predict the incidence of DDH.
Conclusion: We suggest that the current practice is introducing a high rate of false positive, especially among females, and the current guidelines on AA should be reviewed and assigned separately for males and females. This is more important for countries that did not utilize the ultrasonographic assessment for DDH.
Keywords: acetabular angle, DDH, plain x-ray, head of the femur
Introduction
Developmental hip dysplasia (DDH) describes a wide spectrum of abnormal relationships between the socket of the acetabulum and the ball of the head of the femur, which eventually result in hip dislocation, subluxation, or instability.1,2 Its incident rate is approximately 1.3–20 in 1000 and it is 4 times more prevalent in females than males.1,3,4 It has congenital as well as environmental components.
DDH should be detected and prevented/treated early to avoid dire outcomes including duck-like gait, chronic pain, loss of agility, osteoarthritis, and avascular necrosis. In addition, early treatment may only cost 10 JOD for an DDH apparatus, whereas late diagnosis could require a number of surgeries, each costing around 27,000 JOD.
The current practice for screening for DDH is through physical examination and radiologic studies. Physical examination generally has poor sensitivity and specificity, especially when it is conducted by poorly trained physicians.2,5–7
The diagnosis of early DDH using plain films taken at the age of 5 months is done by inspecting classic lines and angles that are helpful in evaluating the immature hip. Among these landmarks, an angle formed between a horizontal line that connects both triradiate cartilages (Hilgenreiner’s line) and a second line parallel to the acetabular roof is measured. This angle is called the acetabular angle (index) (AA), and, according to the current standards, should be less than 28 degrees at birth, 23.5 degrees at 6 months, and 20 degrees at 2 years.2 Thirty degrees is considered the upper limit of normal.2
The line parallel to the acetabular roof connects the acetabular superolateral ridge (iliac promontory) with the acetabular inferomedial ridge. Our hypothesis is that as a result of the natural difference between the male (android) and female (gynaecoid) hips, the iliac promontory in the female pelvis is more rounded (flat) in oppose to the more acute (sharp) iliac promontory in the male population. This is resulting in an overestimation of the AA on x-rays, hence, higher rate of false-positive incidents among females.
It is important to highlight also that many developing countries did not utilize the ultrasonographic assessment for the DDH. In addition, the ultrasound is an operator-dependent method. Accordingly, the aim of this study is to investigate the difference in iliac promontory shape between male and female infants, and to reevaluate the current practice in the light of this difference.
Materials and Methods
Data Collection
The Institutional Review Board was obtained from Jordan University of Science and Technology (Project ID: 20190423). This was a retrospective study conducted in a single center in Amman. All anteroposterior (AP) pelvic digital x-ray studies performed to rule out DDH in the period from July 2014 to July 2019 were collected from the PACS systems. Information about gender and age was also collected. Cases without follow-up of at least 6 months, treated at the time of follow-up, poorly positioned as identified by one of the authors (KA), or with radiographically apparent ossification center of the head of femur were excluded from the final analysis. A total of 998 cases were collected, of which 587 were excluded, leaving 411 cases (822 hip joints) for the final analysis. Approximately 55% (n = 546) of the cases had no follow up studies, 2% (n = 15) had been treated, 5% (n = 50) were labeled as incorrectly positioned, and 20% (n = 197) had visible ossification center. There was an overlap between more than one exclusion criterion in some cases. The criteria for correctly positioned radiographs included no rotation in pelvis as evident by symmetrical alae of ilium and obturator foramina, and correct internal rotation of both legs as demonstrated by both greater trochanters being visible in profile with the lesser trochanter being invisible.
Measured Parameters
The included radiographs were simultaneously reviewed by two radiologists to measure AA bilaterally; one with experience of 15 years and the other with 5 years. AA1 refers to AA at the time of first visit, while AA2 to AA at the time of follow up. Cases who developed DDH at the time of follow-up were identified by inspecting classic lines and angles including Shenton lines, femur lateralization, and AA2. Also, the shape of the iliac promontory was identified; it was subjectively described as either flat if it looked more rounded, or sharp if it looked more acute. A novel angle was measured between a line parallel to the lateral aspect of the region of the inferior iliac spines and a line that extends along the acetabular roof to quantify the roundness of the iliac promontory (Figure 1). We called the former line the Miral line, and the formed angle the iliac promontory angle (IPA). The images were reviewed on Totoku Medical Monitors (JVC, CA, USA), 3 Megapixel, and size 21 inches workstation.
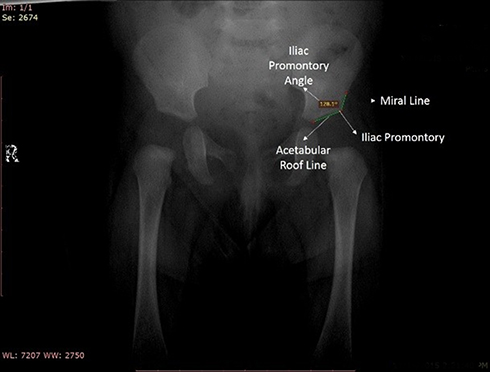 |
Figure 1 Illustration to the components that form the Iliac Promontory Angle. |
Data Analysis
Descriptive analysis was performed for gender, age, AA readings at the time of first visit (AA1) per hip, subjective description of the shape of the iliac promontory (sharp vs flat) per hip, IPA at the time of first visit bilaterally, and DDH status per hip at follow up. The shape of the iliac promontory and IPA were further described in terms of gender. Whereas AA1 was further described in terms of gender, iliac promontory shape, and DDH status at the time of follow up.
Chi-square (χ2) was used to test the association between gender and the shape of the iliac promontory. The independent-sample t-test was used to compare the difference in AA1 and IPA between genders, iliac promontory shapes, and DDH statuses. P-values of less than 0.05 were considered significant. Data were analyzed using IBM SPSS (IBM Corp., v.21.0.Armonk, NY, U.S.).
Results
A total of 998 cases were collected, of which 587 were excluded, leaving 411 cases (822 hip joints) for the final analysis. Most infants were females (92.0%). The mean (SD, range) age at the first visit was 3 months (1 week, 10–14 weeks), and at the follow up was 9.5 months (2 weeks, 35–42 weeks). The median age for both males and females in the study is similar. The median values are provided in Table 1. None of the cases had DDH at the time of follow up.
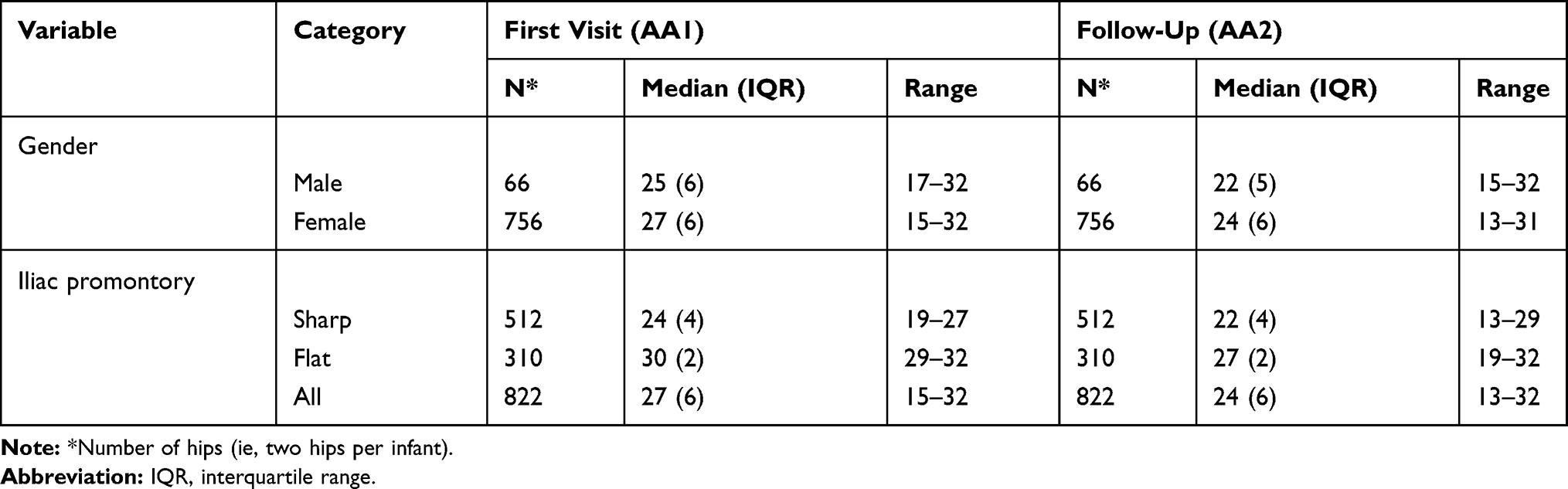 |
Table 1 Summary of Acetabular Angle (AA) Measurements in Degrees |
Measurements of the AA are summarized in Table 1. AA1 was significantly larger in females compared to males (mean difference = 1.6°, P<0.01) and in flat iliac promontory compared to sharp (mean difference = 6.2°, P<0.001). At the time of follow-up, AA significantly decreased from 26.2° (3.9°) to 23.6° (3.7°) (P<0.001). This was true for both males (mean difference = 2.1°, P<0.001) and females (mean difference = 2.6°, P<0.001), and for both sharp (mean difference = 2.4°, P<0.001) and flat iliac promontory (mean difference = 3.3°, P<0.001). It was noticed that the reduction in AA at follow up was more significant in flat promontory than sharp (P<0.001) and did not differ within gender (P = 0.131).
The population of the study did not include AA1 larger than 32° because all hips with larger angles were treated at the time of follow up. This caused the distribution of AA1 in the study sample to skew to the left (Figure 1). Surprisingly, despite that 48.4% of hips with flat iliac promontory (N = 150) had AA1 that exceeded the upper limit for positive DDH (ie, ≥30°), none had DDH at the time of follow-up.
The shape of the iliac promontory had a strong association with gender (χ2:17.7, P< 0.001), where 39.8% of female infants had flat iliac promontory at the time of the first visit, compared to 13.6% of males.
Measurements of the IPA are summarized in Table 2. IPA ranged from 115.0°-150.1° with a binomial distribution (Figure 2). It was significantly larger in flat iliac promontory compared to sharp (mean difference = 19.2°, P< 0.001) as subjectively described by the image readers. IPA also was larger in females compared to males (mean difference = 5.1°, P<0.001).
 |
Table 2 Summary of Iliac Promontory Angle (IPA) Measurements in Degrees |
 |
Figure 2 Examples of subjectively described flat and sharp hips. We named the line parallel with the lateral aspect of the region of the inferior iliac spines the Miral line. Iliac Promontory Angle (IPA) is an angle between the Miral Line and a line parallel to the acetabular roof (Acetabular Roof Line). (A) IPA for the both hips in a female infant aged 3 months. This hip was described as sharp by both radiologists. (B) IPA for the both hips in a male infant aged 3 months. This hip was described as flat by both radiologists. |
A strong positive correlation was found between AA1 and IPA (R2 = 0.93, P< 0.001), as was geometrically expected. It was evident that the transition between the visual description of the iliac promontory as sharp or flat hovered around the 135°IPA, which coincides with the 28° AA (Figure 3). Therefore, based on Figures 2 and 3, we suggest 135° as a quantitative cutoff angle to the visual perception of flat and sharp iliac promontory. The abrupt shallowing in the IPA distribution over AA1 around the 28°AA1 in Figure 2 may be caused by the absence of AA1 larger than 32° in the population of this study as demonstrated in Figure 1.
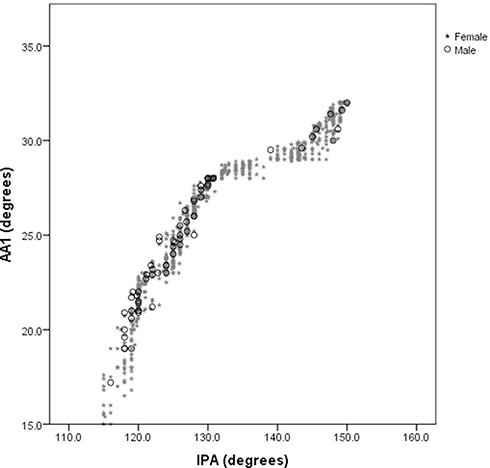 |
Figure 3 Histogram showing the distribution of acetabular angle measurements taken at the first visit (AA1). The histogram is skewed to the left as a result of absence of AA1 larger than 32° in the population of this study. |
Discussion
The management of DDH poses financial, psychological, and cultural stress to the families of the affected children. Therefore, it is important to eliminate the false positives. Although ultrasound performed at the age of 6 weeks is the examination of choice for the identification of DDH, plain pelvic x-ray is still commonly performed at the age of 3 months to rule out DDH in Jordan.8
In the population of this study, the range of AA at the ages of around 3 months and 9.5 months were 15°-32° and 13°-32°, with mean values of 26.2° and 23.6°, respectively. It will be misleading to compare these numbers with other reports because of the variability in the upper limit of included AA measurement, which will reflect on the mean value. In our clinic, we noticed that the pelvis in female infants as demonstrated in plain films at the age of 3 months had more rounded iliac promontory more frequently than in males. We thought that this could be a normal anatomical difference between genders, and it might be contributing to the currently considered abnormal AA, and the higher rate of DDH incidence in females, which, based on the results of this study, we believe it is rather a higher rate of false positives. Therefore, a novel angel was suggested to quantify the level of roundness in iliac promontory and named the Iliac Promontory Angle (IPA).
In the middle of a busy practice, it is commonplace among radiologists in Jordan to report DDH in plain films if they find the iliac promontory flat, even if all other classic lines and angles are normal. This is usually justified by unformed sufficient cupping of the acetabulum, which eventually may fail to encapsulate the head of the femur. In this study, radiologists were asked to describe the iliac promontory as flat or sharp, and an IPA of 135° was found to be the transitional angle between what is subjectively perceived as flat or sharp iliac promontory (Figures 4 and 5). IPA of 135° was also found to coincide with AA of 28°.
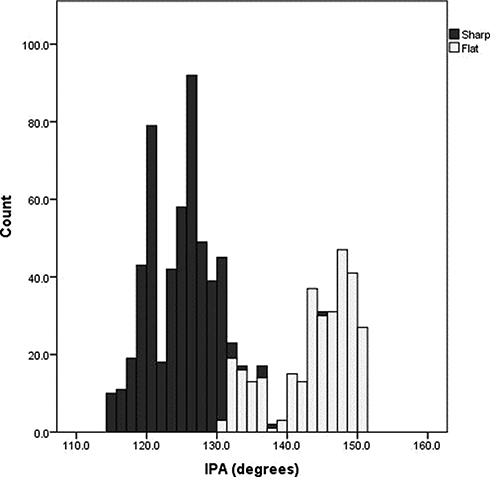 |
Figure 4 Histogram showing the distribution of iliac promontory angle (IPA) taken at the first visit. The binomial distribution segregates the hips that were subjectively described as sharp or flat by the radiologists. |
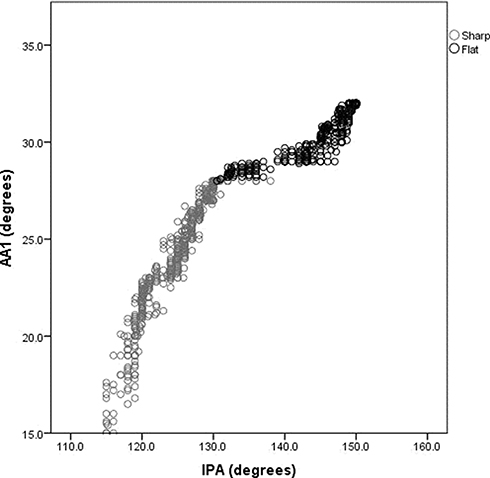 |
Figure 5 Correlation between acetabular angle (AA1) and iliac promontory angle (IPA) measurements taken at the first visit (R2 = 0.93, P < 0.001). It could be withdrawn from the figure that IPA of 130° is the cutoff angle between sharp and flat hips, which corresponds to AA1 of 28°. |
This study demonstrated that flat iliac promontory with IPA ≥ 135° was 3.7 times more prevalent in females than males. It was interesting to find that none of the infants with flat iliac promontory had DDH at follow up, despite the fact that approximately half of them had AA exceeding 30°, which is believed to be the upper limit of normal.2 This led us to believe that the flat iliac promontory is a normal anatomical variation that occurs more frequently in the female population, and it is contributing to a mistakenly believed higher incidence of DDH among female infants.
Also, it was noticed in this study that approximately 18% of the hips had AA> 30° as measured on plain films at the first visit. However, none developed to DDH at the time of follow up. The upper limit of 30o of the AA was first proposed by Laurenson RD in 1959, and since then the number has not been reviewed and has become the standard practice until today.9 In addition, there is wide inter- (±3.0°) and intra-observer (±3.6°) variability in AA measurement as was reported by Spatz et al (1997).10 Also, current guidelines on the AA upper limit do not differentiate between genders. Therefore, we suggest reviewing the criteria of AA in the diagnosis of DDH and investigating the differences between males and females. Good and early diagnosis and treatment may prevent late and very serious problems such as high hip luxation, which may lead to a very difficult operation.11
Similar to other works, this study has limitations. First, it was not possible to suggest a new AA upper limit for flat hips because AA did not exceed 32° in this study. Second, no reproducibility test was performed for the new IPA, which could be the aim of future work. Third, the female population was substantially larger than the male, which is due to the higher prevalence of flat promontory in females. Also, it might be a reflection of the current biased concern of Jordanian parents, or recommendations from their pediatricians. Finally, no clinical information was provided regarding the family history of DDH, breach or clinical examination, Ortolani or other tests.
Conclusion
Our study shows that there are anatomical differences between the male and female pelvis as it appears on pelvic x-rays at the age of 3 months old. It was noticed that flat iliac promontory was 3 times more prevalent in females than males, which might have been contributing to the higher prevalence of DDH in the female population. Also, it was found that the current upper limit of normal AA angle (ie, 30°) did not predict the incidence of DDH in this study. In fact, AA of up to 32° did not develop into DDH. Therefore, we recommend reviewing the current AA guidelines, especially in terms of the upper limit of normal, and in relation to gender.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author.
Ethical Statement
The Institutional Review Board was obtained from Jordan University of Science and Technology (Project ID: 20190423). The study was conducted in accordance with the Declaration of Helsinki. The consent was waived due to the retrospective nature of the study. We confirm that the privacy of the participants was saved, and the data were anonymized and maintained with confidentiality.
Funding
This work was supported by the Deanship of Research at Jordan University of Science and Technology (grant 20190481).
Disclosure
The authors declare no competing interests.
References
1. Shipman SA, Helfand M, Moyer VA, et al. Screening for developmental dysplasia of the hip: a systematic literature review for the US preventive services task force. Pediatrics. 2006;117:e557–576. doi:10.1542/peds.2005-1597
2. Noordin S, Umer M, Hafeez K, et al. Developmental dysplasia of the hip. Orthop Rev (Pavia). 2010;2:e19. doi:10.4081/or.2010.e19
3. Kotlarsky P, Haber R, Bialik V, et al. Developmental dysplasia of the hip: what has changed in the last 20 years? World J Orthop. 2015;6:886–901. doi:10.5312/wjo.v6.i11.886
4. Yang S, Zusman N, Lieberman E, et al. Developmental dysplasia of the hip. Pediatrics. 2019;143:
5. Souza BGSE, de Melo TE, Resende TM, et al. Developmental dysplasia of the hip: do the responsible for screening know what to do? Acta Ortop Bras. 2016;24:312–317. doi:10.1590/1413-785220162406165319
6. Williams N. Improving early detection of developmental dysplasia of the hip through general practitioner assessment and surveillance. Aust J Gen Pract. 2018;47:619–623. doi:10.31128/AJGP-03-18-4524
7. Dogruel H, Atalar H, Yavuz OY, et al. Clinical examination versus ultrasonography in detecting developmental dysplasia of the hip. Int Orthop. 2008;32:415–419. doi:10.1007/s00264-007-0333-x
8. Omeroğlu H. Use of ultrasonography in developmental dysplasia of the hip. J Child Orthop. 2014;8:105–113. doi:10.1007/s11832-014-0561-8
9. Laurenson RD. The acetabular index: a critical review. J Bone Joint Surg. 1959;41–B:702–710. doi:10.1302/0301-620X.41B4.702
10. Spatz DK, Reiger M, Klaumann M, et al. Measurement of acetabular index intraobserver and interobserver variation. J Pediatr Orthop. 1997;17:174–175. doi:10.1097/01241398-199703000-00007
11. Necas L, Hrubina M, Melisik M, et al. Cementless hip arthroplasty and transverse shortening femoral osteotomy with the S-ROM stem for Crowe type IV developmental dysplasia. Eur J Orthop Surg Traumatol. 2019;29:1025–1033. doi:10.1007/s00590-019-02400-y
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.