Back to Journals » International Journal of Women's Health » Volume 18
Integrating Mind Mapping with Virtual Simulation: A Cognitive Scaffolding for Clinical Reasoning in Residency
Received 8 April 2026
Accepted for publication 23 May 2026
Published 4 June 2026 Volume 2026:18 615354
DOI https://doi.org/10.2147/IJWH.S615354
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marta Barba
Qinqing Chen, Fangfang Xi, Min Lv
Department of Obstetrics, Women’s Hospital School of Medicine Zhejiang University, Hangzhou, People’s Republic of China
Correspondence: Min Lv, Department of Obstetrics, Women’s Hospital School of Medicine Zhejiang University, Hangzhou, People’s Republic of China, Email [email protected]
Objective: To investigate the efficacy of Mind Mapping–Virtual Simulation (MM-VSP) in enhancing clinical reasoning and procedural application competencies among residents.
Methods: A retrospective study was conducted with second-year residents (n=80) during their obstetrics and gynecology (OB/GYN) rotations (January 2023 - December 2024). Participants were categorized to either the study group (n=40, receiving MM-VSP training) or the control group (n=40, receiving VSP training), all trained by a unified faculty team using identical clinical cases. Primary outcomes—theoretical knowledge, clinical competency, and learner satisfaction—were extracted from anonymized annual competency assessments.
Results: Baseline characteristics were balanced between groups (all p > 0.05). No group difference was found in theoretical knowledge (p = 0.76). The study group demonstrated higher scores in History Taking (p < 0.01, Cohen’s d = 0.92), Clinical Reasoning (p < 0.01, r = 0.47), and OB/GYN Specialty Skills (p < 0.01, Cohen’s d = 0.88). Most subdomains of clinical reasoning favoured the study group (p < 0.01, r = 0.41– 0.53). Additionally, the study group reported higher instructional satisfaction (p < 0.01, r = 0.36) and higher perceived learning outcomes (p < 0.01, r = 0.68).
Conclusion: In this retrospective study, MM-VSP was associated with better complex reasoning and procedural skills in OB/GYN residents, without additional cognitive load.
Keywords: obstetrics and gynecology, residents, mind mapping, virtual simulation, clinical reasoning
Introduction
Standardized residency training bridges the gap between theoretical knowledge and independent clinical practice1–3 by cultivating robust clinical reasoning.4,5 This need is particularly acute in Obstetrics and Gynecology (OB/GYN), a specialty characterized by high-acuity conditions, sensitive patient interactions, and inherent limitations in hands-on trainee exposure, often constraining traditional apprenticeship models.6–10
In response, simulation-based education has become indispensable. Virtual Simulation Platforms (VSPs) provide immersive, risk-free clinical environments for practicing patient management.11–15 However, conventional VSP use tends to emphasize procedural adherence to pre-set pathways. This format may improve operational familiarity but can inadvertently promote a “gaming” mentality, where learners focus on navigating the interface rather than engaging in the deep, active cognitive work of differential diagnosis and decision-tree construction. Consequently, VSPs alone may not sufficiently scaffold the active knowledge construction essential for clinical reasoning development.16
Addressing this gap requires a pedagogical strategy grounded in constructivist learning theory, which holds that knowledge is actively constructed by integrating new experiences with existing cognitive frameworks within authentic contexts.17 Central tenets include: (1) learning as an active process of meaning-making; (2) the necessity of prior knowledge activation; (3) the critical role of authentic, situated experiences; and (4) reflection and social negotiation as catalysts for cognitive restructuring. Mind Mapping (MM) operationalizes this principle as a dynamic cognitive scaffold: its radiant, hierarchical structure compels learners to actively organize fragmented knowledge, establish logical connections, and externalize evolving mental models.18 This process directly embodies constructivist “active construction,” transforming learning from passive reception into deliberate knowledge integration, thereby strengthening memory networks and stimulating critical thinking.19,20
Integrating MM with VSP creates a theoretically coherent, constructivist-aligned cycle of construction, context, and reflection. First, MM activates prior knowledge and scaffolds an individualized diagnostic framework. The VSP then provides an authentic, immersive context in which this constructed mental model is dynamically tested—fulfilling the constructivist emphasis on situated learning. Crucially, discrepancies between the initial mind map and simulated patient trajectories become focal points for guided reflection during structured debriefing. Through instructor-facilitated dialogue and peer discussion (social negotiation), learners critically evaluate, revise, and consolidate their clinical reasoning structures. Thus, MM-VSP systematically embeds active knowledge building, contextual application, and reflective iteration, transcending the limitations of either tool alone.
Our faculty team had previously implemented the MM-VSP integrated model on a small scale, but systematic data on its effectiveness were lacking. Therefore, we conducted this retrospective study aiming to comparatively evaluate the educational outcomes and implementation characteristics of the MM-VSP instructional model versus conventional VSP training. We purposefully selected second-year residents as the study population, as this stage represents a critical transition where foundational knowledge must be restructured into integrated clinical reasoning, while learners remain particularly susceptible to surface-level, interface-focused learning without adequate cognitive scaffolding. The primary focus was on fostering core clinical competencies, while simultaneously assessing implementation feasibility and learner acceptance.
Methods
Participants and Study Design
This retrospective study was conducted within the standardized residency training program at the Women’s Hospital School of Medicine Zhejiang University, spanning from January 2023 to December 2024. The participants were strictly limited to second-year residents rotating through obstetrics and gynecology under the guidance of a single core teaching team, comprising five senior attending physicians or higher with unified teaching certification. Both groups underwent training during the same study period, with identical rotation duration, clinical cases, and assessment instruments.
During the study period (January 2023 to December 2024), the training that each resident received was determined by their rotation schedule rather than by prospective random assignment. The study group was retrospectively defined as all second-year residents who underwent MM-VSP training under the core teaching team and met the inclusion criteria (n = 40). From the pool of second-year residents who received conventional VSP training under the same teaching team during the identical period, 40 individuals were randomly selected using a random number table to serve as the control group. This random sampling aimed to obtain a comparable comparison group and mitigate selection bias. No formal a priori sample size or power calculation was performed, as the sample size was determined by the available complete datasets from the two training modalities. Given the relatively small sample of 40 residents per group, findings should be interpreted with appropriate caution.
Inclusion criteria: (1) Second-year residents in the Obstetrics and Gynecology program at Women’s Hospital, School of Medicine, Zhejiang University; (2) Attendance rate of ≥ 90% during the rotation; (3) Availability of complete assessment data and satisfaction surveys. Exclusion criteria: (1) Prior systematic training in mind mapping methods; (2) Previous involvement or familiarity with the development/testing of the virtual simulation cases used in this study; (3) Missing critical evaluation data.
All data were sourced and analyzed after anonymization. The study was approved by the Ethics Committee of Women’s Hospital, School of Medicine, Zhejiang University (IRB-20250434-R), with a waiver of informed consent, adhering to the principles outlined in the Declaration of Helsinki.
Training Method
The training protocols for both groups were implemented over the standardized obstetrics and gynecology rotation period, utilizing identical clinical cases and assessment instruments. The core divergence lay in the cognitive scaffolding strategy prior to simulation engagement.
Study Group (MM-VSP)
- Structured Mind Mapping: For a given chief complaint, residents were first required to individually create a detailed mind map. This map was to comprehensively cover differential diagnoses, necessary history questions, pertinent physical examinations, and potential investigative and therapeutic interventions.
- Immersive Virtual Simulation: Residents then logged into the hospital’s virtual simulation platform to manage the same clinical case. The platform presented a series of coherent and independent simulated scenarios—including outpatient consultation, physical examination, ancillary testing, diagnostic analysis, and basic procedural skills—that evolved dynamically with the patient’s condition, thereby enhancing the authenticity and completeness of the clinical narrative. Within this virtual environment, residents applied the structure of their mind maps to conduct consultations, order tests, establish diagnoses, and initiate treatment.
- Guided Debriefing and Evaluation: A debriefing session was conducted upon completion of the simulation. During this session, the resident’s pre-constructed mind map was systematically compared with their actual decisions and actions taken in the virtual platform. The discussion focused on analyzing discrepancies, reinforcing sound clinical reasoning, and solidifying logical patient management pathways.
Control Group (VSP-Only)
Residents engaged directly with the identical VSP cases without pre-simulation cognitive preparation. Post-simulation, instructors conducted a summary session reviewing case objectives, evidence-based guidelines, and common pitfall. All procedural modules and system assessments remained consistent with the study group.
Data Collection
Data for this study were retrospectively extracted from anonymized records of the standardized second-year annual competency assessment administered to obstetrics and gynecology residents at our institution—an accredited national training base for standardized residency programs. Three core domains were systematically extracted and analyzed:
Theoretical Knowledge Assessment
The theoretical knowledge assessment comprised a 100-point examination entirely composed of multiple-choice questions, meticulously designed in alignment with National Standardized Residency Training requirements to evaluate core obstetric and gynecologic principles and applied clinical reasoning scenarios. All examinations were objectively scored by the institutional assessment committee using a pre-validated answer key, ensuring scoring consistency and minimizing evaluator bias.
Clinical Competency Evaluation
A multi-station Objective Structured Clinical Examination (OSCE), implemented with identical procedures and scoring criteria to the graduation assessment protocol of our institutional residency training base, evaluated core clinical competencies:
Station 1: Patient Interview and Physical Examination with Standardized Patient (SP) – History taking (scored 0–100) and physical examination (scored 0–100).
Station 2: Initial Progress Note Documentation (Structured Clinical Note Writing; Scored 0–100).
Station 3: Clinical Reasoning and Decision-Making (total score: 0–100 points) – Assessed using a validated rubric with seven predefined subdomains: summary of history features (15 points), diagnosis and supporting evidence (15 points), key points of differential diagnosis (15 points), treatment principles and measures (15 points), professional knowledge application (15 points), ethics/humanities/professional integrity (15 points), and synthesis/communication/expression (10 points).
Station 4: Fundamental Procedural Skills (randomly allocated by the examination management system: cardiopulmonary resuscitation or endotracheal intubation; scored 0–100).
Station 5: OB/GYN Specialty Procedural Skills (Scored 0–100).
In Station 1, history taking and physical examination were scored independently as distinct competency metrics. All stations adhered to the institutional graduation assessment protocol in procedures and scoring criteria. Evaluations were performed by 2 trained assessors blinded to group allocation.
Instructional Satisfaction Survey
Two previously validated questionnaires were employed to assess the learners’ educational experience. The first 5-item instructional satisfaction21 questionnaire assessed perceptions across course content, resources, classroom interaction, teaching methods, and learning burden. The second 7-item perceived learning outcomes questionnaire22 evaluated self-reported impacts on core competencies: stimulate learning interest, improve thinking and problem solving skills, cultivate clinical thinking, enhance communication skills, enhance clinical learning confidence, improve practical operation ability and suitable for standardized training. Both instruments utilized a 5-point Likert scale (satisfaction: 1 = very dissatisfied to 5 = very satisfied; learning outcomes: 1 = strongly disagree to 5 = strongly agree), yielding total score ranges of 5–25 and 7–35, respectively. Consistent with methodological best practices for cross-contextual instrument application, internal consistency was recalculated within the current cohort for both scales (satisfaction scale: Cronbach’s α of 0.85; teaching mode scale: Cronbach’s α of 0.82), confirming reliability consistent with original validation studies.
Data Analysis
All statistical analyses were performed using Python 3.9 (pandas, NumPy, SciPy, statsmodels). Continuous variables were assessed for normality using the Shapiro–Wilk test (α= 0.05). For normally distributed data with equal variances (Levene’s test), group comparisons were performed using the independent samples t-test; otherwise, Welch’s t-test was applied. Results are reported as mean ± SD, mean difference with 95% confidence interval (CI), and Cohen’s d (pooled standard deviation). For variables violating normality, the Mann–Whitney U-test with continuity correction was used. Results are presented as median (IQR), Hodges-Lehmann estimate of median difference with 95% CI (Bauer, 1972), and effect size r = |Z| / √(n1 + n2). Categorical variables were compared using the chi-square test and reported as frequencies (percentages). A two-sided P value < 0.05 was considered statistically significant for all comparisons. Effect sizes were interpreted according to conventional thresholds: for Cohen’s d, values of 0.2, 0.5, and 0.8 were considered small, medium, and large, respectively; for r, values of 0.1, 0.3, and 0.5 were considered small, medium, and large, respectively (Cohen, 1988).
Results
Baseline Characteristics
A total of 80 second-year obstetrics and gynecology residents were retrospective included in this analysis (Study group: n = 40; Control group: n = 40). All participants in both groups completed the full set of required virtual simulation cases, ensuring exposure to the core clinical scenarios. There were no statistical differences between the two groups in age, sex, or academic background (all p > 0.05; Table 1).
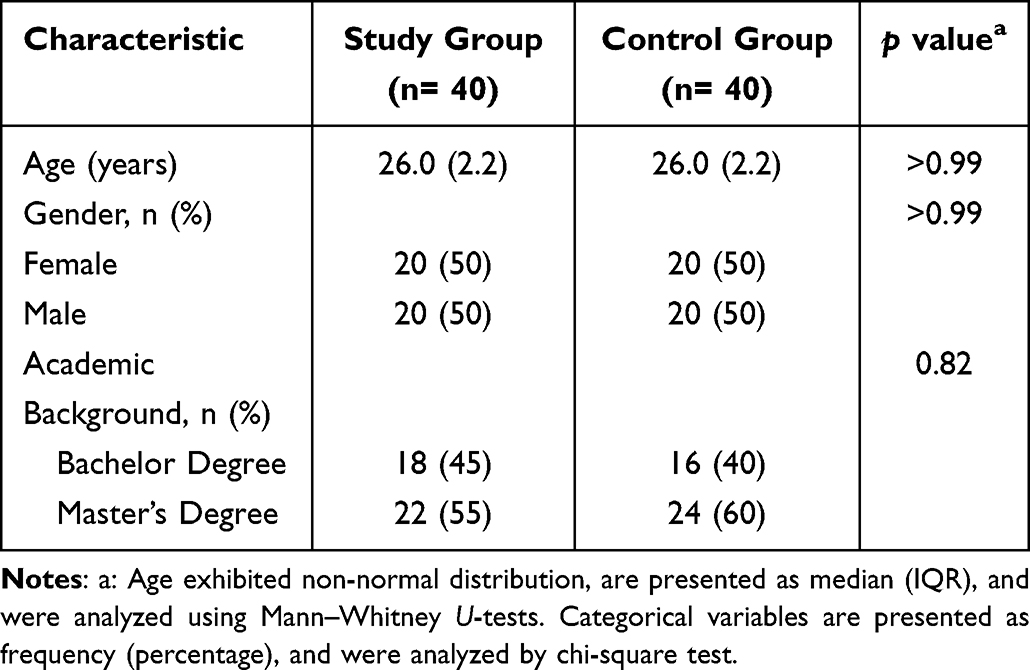 |
Table 1 Baseline Characteristics of Study Participants |
Comparison of Theoretical Knowledge and OSCE Performance
No statistically significant difference was observed in the theoretical knowledge scores between the study group (mean = 75.00, SD = 8.51) and the control group (mean = 74.45, SD = 7.79; mean difference = 0.55, 95% CI: −3.08 to 4.18, p = 0.76). For the OSCE stations, there were no statistically significant differences between the two groups in Physical Examination (p = 0.98) or Initial Progress Note (p = 0.76). However, the study group showed higher scores than the control group in History Taking (mean = 81.90, SD = 5.85 vs. 76.83, SD = 5.20; mean difference = 5.08, 95% CI: 2.61 to 7.54, p < 0.01), Clinical Reasoning and Decision‑Making (median = 76.50, IQR = 5.00 vs. 71.00, IQR = 6.00; median difference = 5.00, 95% CI: 3.00 to 7.00, p < 0.01), and OB/GYN Specialty Skills (mean = 83.20, SD = 6.31 vs. 77.83, SD = 5.91; mean difference = 5.38, 95% CI: 2.65 to 8.10, p < 0.01) (Table 2).
 |
Table 2 Comparison of Theoretical Knowledge and OSCE Station Scores |
Among the seven subdomains, the study group showed higher scores than the control group in four areas: diagnosis and supporting evidence (median difference = 1.00, 95% CI: 1.00 to 2.00, p < 0.01, r = 0.50), key points of differential diagnosis (median difference = 1.00, 95% CI: 1.00 to 2.00, p < 0.01, r = 0.50), professional knowledge application (median difference = 2.00, 95% CI: 1.00 to 2.00, p < 0.01, r = 0.53), and synthesis/communication/expression (median difference = 1.00, 95% CI: 0.00 to 1.00, p < 0.01, r = 0.41). No statistically significant differences were observed in the remaining three subdomains: summary of history features (mean difference = −0.12, 95% CI: −1.09 to 0.84, p = 0.80; Cohen’ s d= −0.06), treatment principles and measures (median difference = 0.00, 95% CI: 0.00 to 1.00, p = 0.45; r = 0.08), and ethics/humanities/professional integrity (median difference = 0.00, 95% CI: −1.00 to 0.00, p = 0.75; r = 0.03) (Table 3).
 |
Table 3 Comparison of Clinical Reasoning and Decision-Making (Station 3) |
Instructional Satisfaction and Perceived Learning Outcomes
The study group reported higher overall instructional satisfaction scores than the control group (median = 23.00, IQR = 2.00 vs. 21.50, IQR = 2.00; median difference = 1.00, 95% CI: 1.00 to 2.00, p < 0.01, r = 0.36). For the domain-specific items, the study group showed higher scores in classroom interaction (median = 5.00, IQR = 0.00 vs. 4.00, IQR = 2.00; median difference = 1.00, 95% CI: 0.00 to 1.00, p < 0.01, r = 0.40) and teaching methods (median = 5.00, IQR = 0.25 vs. 4.00, IQR = 2.00; median difference = 0.00, 95% CI: 0.00 to 1.00, p < 0.01, r = 0.31). No statistically significant differences were observed between the two groups for course content (p = 0.43), course resources (p = 0.85), or learning burden (p = 0.94) (Table 4).
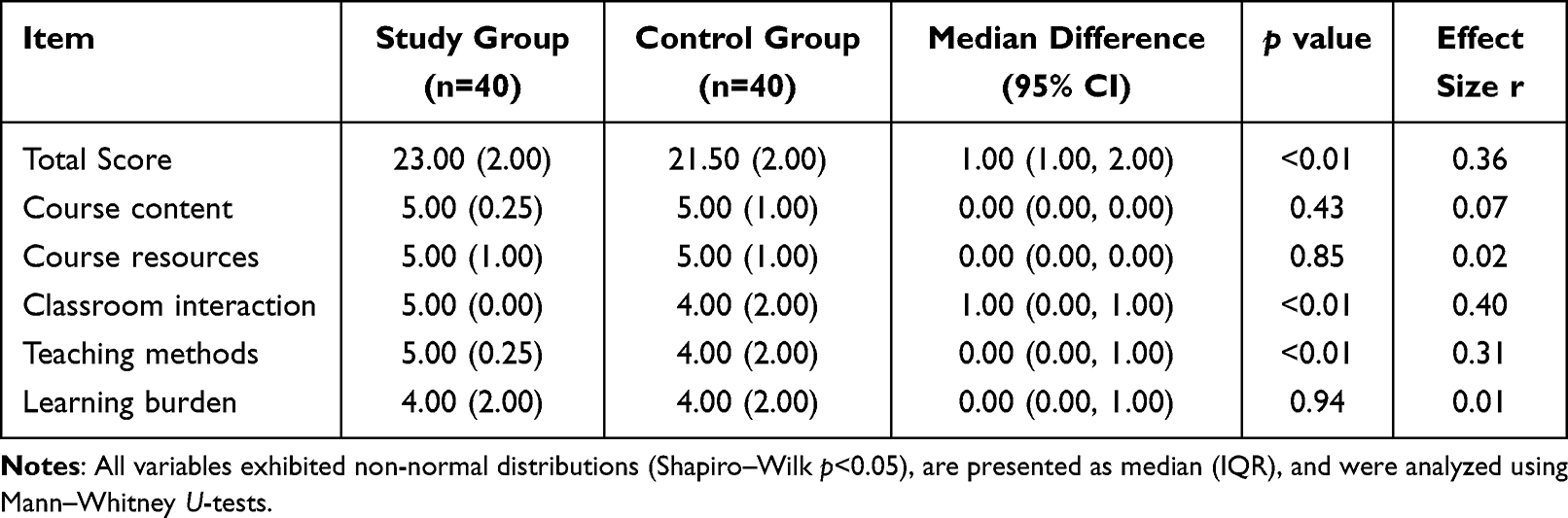 |
Table 4 Comparison of Instructional Satisfaction Scores |
The study group also had higher total scores on the perceived learning outcomes questionnaire compared with the control group (median = 32.00, IQR = 1.50 vs. 28.00, IQR = 2.25; median difference = 4.00, 95% CI: 3.00 to 5.00, p < 0.01, r = 0.68). Statistically significant differences in favour of the study group were observed for six of the eight competency domains (all p < 0.05), including stimulate learning interest (p = 0.02, r = 0.24), improve thinking and problem‑solving skills (p < 0.01, r = 0.31), cultivate clinical thinking (p = 0.02, r = 0.25), enhance communication skills (p < 0.01, r = 0.35), enhance clinical learning confidence (p < 0.01, r = 0.43), and improve practical operation ability (p < 0.01, r = 0.33). No significant difference was found for suitable for standardised training (p = 0.22, r = 0.11) (Table 5).
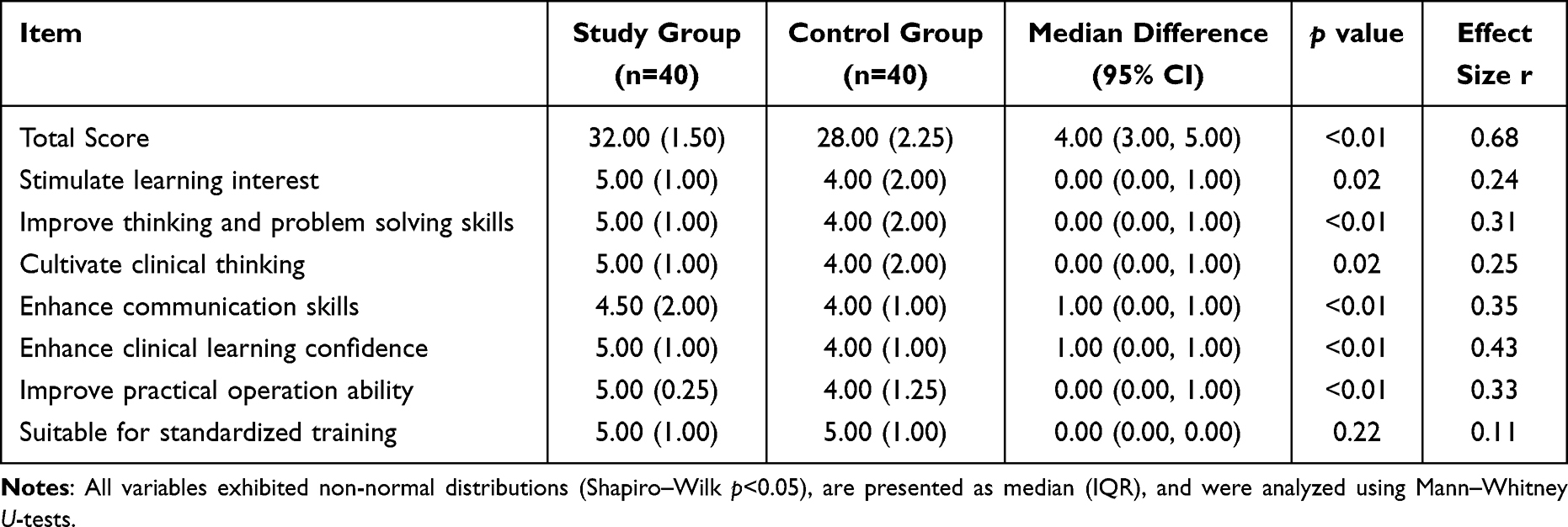 |
Table 5 Comparison of Perceived Learning Outcomes |
Discussion
This study provides initial evidence that integrating mind mapping (MM) with virtual simulation (VSP) is associated with enhanced targeted educational outcomes in residency training. The key finding—that the significant improvement in clinical thinking and procedural skills without a corresponding increase in theoretical knowledge scores—may suggest that the MM-VSP model is related to changes in how knowledge is organized and applied, rather than how much is acquired. This pattern aligns with the model’s design intention: to shift learning from passive reception to active construction and application, though the retrospective design limits causal inference.
The comparable theoretical scores between groups help establish baseline equivalence and lend support to the possibility that the observed differences in higher-order skills are indeed related to the intervention. However, residual confounding cannot be excluded due to the non-randomized design. This selective enhancement aligns with prior research. For instance, studies have shown that mind mapping alone can improve critical thinking and knowledge integration by externalizing cognitive structure.19,23,24 This is supported by findings in nursing and respiratory therapy education, where mind mapping significantly improved students’ analytical abilities and diagnostic reasoning.18,19,23,24 Similarly, simulation is established as a method for practicing skills in a safe environment.14,15 Our findings extend this literature by suggesting that sequencing these tools—using MM before VSP—may create a synergistic, cognition-driven learning cycle. This sequencing appears to address a known limitation of standalone simulation, where learners may focus on procedural steps without deeply engaging the underlying clinical reasoning.16 Prior evaluations of virtual platforms have noted that without structured cognitive tasks, simulation can degenerate into a passive, “button-clicking” exercise, limiting its impact on clinical judgment.25 The mind mapping task necessitates active diagnostic reasoning upfront, thereby potentially making the subsequent simulation a test of a pre-formed mental model rather than a series of prompted actions.
The synergy can be understood through a constructivist lens.17,26–28 The MM phase may act as a cognitive organizer, helping residents structure diagnostic hypotheses and management plans explicitly. This process of externalizing and organizing knowledge resonates with the concept of “cognitive offloading” shown to improve complex decision-making in other clinical learning contexts.17,26 The VSP phase then serves as an authentic but safe environment to apply and refine this mental model. Discrepancies between the planned approach (mind map) and the simulated patient’s course can generate cognitive conflict, which is resolved during the structured debriefing. This iterative cycle of “cognitive preparation → applied practice → guided reflection” may help bridge declarative knowledge (“knowing that”) and procedural competence (“knowing how”), which is a core objective of clinical training. Similar iterative, reflective cycles have been identified as key components of effective mastery learning in surgical skills training.27,28
The significantly higher instructional satisfaction scores reported by the MM-VSP group, further supports the model’s implementation feasibility. This is consistent with the findings of previous studies on simulation-based teaching, where learners reported increased confidence and satisfaction.29,30 Such congruence between subjective experience and objective measures reinforces the model’s relevance and acceptability, a factor critical for successful implementation of educational innovations.31 This positive reception is consistent with reports from other blended learning interventions, where active, participant-centered designs consistently yield higher learner motivation and perceived value compared to traditional, passive formats.31
Our study has several important limitations that warrant careful consideration. First, the retrospective, non-randomized design, although control selection was randomized from available cohorts, may still introduce selection bias and unmeasured confounding, thereby limiting our ability to establish causation. Second, the relatively small sample size (40 per group), derived from a single academic center, reduces the statistical power to detect smaller effects and restricts generalizability beyond this specific institutional context. Third, the lack of long-term follow-up means that the durability of the observed gains in clinical reasoning and their translation into real-world clinical performance remain unknown. Fourth, the intervention was exclusively implemented among second-year obstetrics and gynecology residents, restricting generalizability to other training levels. This limitation is particularly significant because clinical reasoning develops progressively across residency years—first-year residents may lack foundational knowledge to effectively engage with mind mapping, while third-year residents may have already developed fixed cognitive patterns that could interact differently with the MM-VSP model. Future research must expand to multi-year, multi-center cohorts to evaluate developmental appropriateness and external validity. Fifth, the study did not account for individual differences in baseline cognitive abilities, prior simulation experience, or learning styles, which could substantially moderate the intervention’s impact. While our assessment tools captured cognitive and procedural outcomes, they did not incorporate direct measures of real-world clinical decision quality or patient outcomes, and the absence of long-term follow-up further limits our ability to fully contextualize the educational impact within the clinical ecosystem.
Conclusions
In conclusion, the MM-VSP model offers a potential pathway for enhancing clinical reasoning and procedural competence in OB/GYN residency training. By embedding constructivist principles—active knowledge construction, contextual application, and reflective iteration—into simulation, the approach appears to support the translation of knowledge into clinical practice. These associations were evidenced by higher scores in complex reasoning domains and procedural skills without increased learning burden, alongside higher learner satisfaction. As medical education evolves toward more cognitive-focused training, models like MM-VSP that prioritize structured knowledge application over procedural repetition may provide valuable support for preparing residents to manage complex clinical scenarios in high-acuity specialties. Larger, prospective, multi-center studies with long-term follow-up are needed to confirm these results and evaluate the durability of the observed educational benefits.
Abbreviations
OB/GYN, Obstetrics and Gynecology; MM, Mind Mapping; VSP, Virtual Simulation Platform; MM-VSP, Mind Mapping–Virtual Simulation Platform; IRB, Institutional Review Board;
OSCE, Objective Structured Clinical Examination; SP, Standardized Patient; SD, Standard Deviation; IQR, Interquartile Range.
Data Sharing Statement
The data supporting the findings of this study are available upon request from the corresponding author. Requests to access the datasets should be directed to [email protected].
Ethics Approval and Consent to Participate
The study was approved by the Ethics Committee of Women’s Hospital, School of Medicine, Zhejiang University (IRB-20250434-R), with a waiver of informed consent.
Acknowledgments
The authors sincerely thank the dedicated clinical teaching faculty of the Obstetrics and Gynecology Residency Training Base at Women’s Hospital, School of Medicine, Zhejiang University. We are deeply grateful for their expert mentorship, thoughtful guidance during simulation sessions. Their passion for medical education profoundly shaped this work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Zhejiang University School of Medicine Obstetrics and Gynecology Institute Educational Reform Project (Grant No. ZDFY202504) and Scientific Research Fund of Zhejiang Provincial Education Department (Grant No.Y202352853).
Disclosure
The authors declare no competing interests in this work.
References
1. Wang C, Qi X, Chen X, Yu Q, Xing L. The establishment of China standardized residency training system. Zhonghua Yi Xue Za Zhi. 2015;95(14):1041–10.
2. Cui Y, Wang T. From the residency training in the united states to see the challenges and directions of china residency standardized training. Zhongguo Fei Ai Za Zhi. 2016;19(6):321–327. doi:10.3779/j.issn.1009-3419.2016.06.03
3. Monestime GM, Baird I, Rebarber A, Shirazian T. ACGME Milestones in global health: need for standardized assessment of global health training in obstetrics/gynecology residency. Int J Gynaecol Obstet. 2022;157(3):522–526. doi:10.1002/ijgo.13914
4. Wang L, Zhao Y, Wang P, Qian A, Hong H, Xu S. Application of clinical thinking training system based on entrustable professional activities in emergency teaching. BMC Med Educ. 2024;24(1):1294. doi:10.1186/s12909-024-06302-4
5. Alston MJ, Autry AM, Wagner SA, et al. Attitudes of trainees in obstetrics and gynecology regarding the structure of residency training. Obstet Gynecol. 2019;134(1):22s–8s. doi:10.1097/AOG.0000000000003430
6. Hirai CM, Chern IY, Kumura NDS, Hiraoka M. Perceptions regarding pediatric and adolescent gynecology training among obstetrics and gynecology residents in Hawai. Hawaii J Health Soc Welf. 2021;80(8):179–183. doi:10.1016/j.jpag.2013.06.017
7. Zhang W, Hao Y, Zhang T, et al. Standardized training assessment of residents in obstetrics and gynecology on entrustable professional activities. BMC Med Educ. 2025;25(1):789. doi:10.1186/s12909-025-06973-7
8. Topcu EG, Kapustin R, Ami O, Ramirez A, Gabor P, Ubom AE. Assessment of obstetrics and gynecology training during residency: a global perspective. Int J Gynaecol Obstet. 2025;170(3):1380–1394. doi:10.1002/ijgo.70420
9. Kang HY, Kim HR. Impact of blended learning on learning outcomes in the public healthcare education course: a review of flipped classroom with team-based learning. BMC Med Educ. 2021;21(1):78. doi:10.1186/s12909-021-02508-y
10. Dayan R, Quach TTT, With S, Ubhi J, Ezzat H, Chen LYC. Classroom-based learning in an academic obstetrics and gynecology residency training program. J Med Educ Curric Dev. 2023;10:23821205231208790. doi:10.1177/23821205231208790
11. Zhu H, Zhang C, Li N, et al. Satisfaction survey on graduates of standardised training for resident doctors in Guizhou Province, China. BMJ Open. 2024;14(10):e085789. doi:10.1136/bmjopen-2024-085789
12. Neveu ML, Kikuchi JY, Ledebur LR, Long JB, Qiao E, Chen CCG. Virtual education in urogynecology: enhancing understanding and management of pelvic fistulas. MedEdPORTAL. 2024;20:11407. doi:10.15766/mep_2374-8265.11407
13. Asfaw ZK, Todd R, Abasi U, et al. Use of virtual platform for delivery of simulation-based laparoscopic training curriculum in LMICs. Surg Endosc. 2023;37(2):1528–1536. doi:10.1007/s00464-022-09438-w
14. Sadeghi AH, Peek JJ, Max SA, et al. Virtual reality simulation training for cardiopulmonary resuscitation after cardiac surgery: face and content validity study. JMIR Serious Games. 2022;10(1):e30456. doi:10.2196/30456
15. Liu K, Yang K, Pu D, Han Y, Zhou Z, Hu J. Construction and exploration of simulative virtual curriculum of laparoscopy for standardized surgical residency training. Sichuan Da Xue Xue Bao Yi Xue Ban. 2023;54(6):1133–1138. doi:10.12182/20231160302
16. Locke R, Mason A, Coles C, Lusznat RM, Masding MG. The development of clinical thinking in trainee physicians: the educator perspective. BMC Med Educ. 2020;20(1):226. doi:10.1186/s12909-020-02138-w
17. Xie Z, Ren L, Zhan Q, Liu Y. A constructivist ontology relation learning method. IEEE Trans Cybern. 2022;52(7):6434–6441. doi:10.1109/TCYB.2021.3138452
18. Wu HZ, Wu QT. Impact of mind mapping on the critical thinking ability of clinical nursing students and teaching application. J Int Med Res. 2020;48(3):300060519893225. doi:10.1177/0300060519893225
19. Sajadi AS, Babajani A, Maroufi SS, Sarraf N. Using the mind map method in medical education, its advantages and challenges: a systematic review. J Educ Health Promot. 2024;13:483. doi:10.4103/jehp.jehp_1323_23
20. Aljamal H, Alawneh R, Derbas A, et al. Efficacy of mind maps and concept maps in enhancing academic performance among undergraduate medical students in the preclinical stage: a systematic review. Adv Health Sci Educ Theory Pract. 2025;31:705–725. doi:10.1007/s10459-025-10437-4
21. Yueyang C, Li W, Haiyan C. The value of One-Minute Preceptor combined with Flipped Classroom teaching model in clinical teaching of general practice. BMC Med Educ. 2025;25(1):1196. doi:10.1186/s12909-025-07787-3
22. Liu R, Li L, Zhou Y, Xiong L. The application of CBL and mind mapping combined with Mini-CEX teaching mode in the cultivation of clinical competence of ultrasound residents. PLoS One. 2025;20(7):e0327739. doi:10.1371/journal.pone.0327739
23. Turkestani FA, Zipp GP, Nufaiei ZA, et al. Mind mapping to enhance critical thinking skills in respiratory therapy education. J Educ Health Promot. 2024;13:198. doi:10.4103/jehp.jehp_1816_23
24. Wang L, Wang Y, Wang X, Xue C. Effects of mind mapping based on standardized patient program in patient education among postgraduate nursing students in clinical setting. BMC Med Educ. 2023;23(1):982. doi:10.1186/s12909-023-04944-4
25. Hamilton A. Artificial Intelligence and Healthcare Simulation: the Shifting Landscape of Medical Education. Cureus. 2024;16(5):e59747. doi:10.7759/cureus.59747
26. Lockey A, Conaghan P, Bland A, Astin F. Educational theory and its application to advanced life support courses: a narrative review. Resusc Plus. 2021;5:100053. doi:10.1016/j.resplu.2020.100053
27. Ross S, Pirraglia C, Aquilina AM, Zulla R. Effective competency-based medical education requires learning environments that promote a mastery goal orientation: a narrative review. Med Teach. 2022;44(5):527–534. doi:10.1080/0142159X.2021.2004307
28. Richardson D, Kinnear B, Hauer KE, et al. Growth mindset in competency-based medical education. Med Teach. 2021;43(7):751–757. doi:10.1080/0142159X.2021.1928036
29. Al Yazeedi B, Al Azri Z, Prabhakaran H, et al. Efficacy of high fidelity pediatric simulation on nursing students’ self-awareness and empathy in a Middle Eastern County. Heliyon. 2025;11(4):e42524. doi:10.1016/j.heliyon.2025.e42524
30. Altinbas BC, Çalık KY, Erdöl EK, et al. The effect of simulation-based laboratory training on undergraduate nursing students’ clinical skill, satisfaction, and self-confidence. BMC Nurs. 2025;24(1):1322. doi:10.1186/s12912-025-04004-w
31. Ricotta DN, Richards JB, Atkins KM, et al. Self-directed learning in medical education: training for a lifetime of discovery. Teach Learn Med. 2022;34(5):530–540. doi:10.1080/10401334.2021.1938074
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.