Back to Journals » Psychology Research and Behavior Management » Volume 19
Integrating Existential Perspectives into Schema Therapy: A Conceptual Framework with Clinical Illustrations
Authors Prasko J ![]() , Gecaite-Stonciene J, Abeltina M, Ociskova M
, Gecaite-Stonciene J, Abeltina M, Ociskova M ![]() , Vanek J
, Vanek J ![]() , Krone I
, Krone I ![]() , Bite I, Slepecky M, Juskiene A
, Bite I, Slepecky M, Juskiene A
Received 11 January 2026
Accepted for publication 14 April 2026
Published 27 May 2026 Volume 2026:19 595379
DOI https://doi.org/10.2147/PRBM.S595379
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Jan Prasko,1– 4 Julija Gecaite-Stonciene,5 Marija Abeltina,6 Marie Ociskova,1,2 Jakub Vanek,1 Ilona Krone,7 Ieva Bite,6 Milos Slepecky,3 Alicja Juskiene5,8
1Department of Psychiatry, Faculty of Medicine and Dentistry, Palacky University Olomouc, University Hospital, Olomouc, The Czech Republic; 2Centre for Mental Rehabilitation, Jessenia Inc. - Rehabilitation Hospital Beroun, Akeso Holding, Czech Republic; 3Department of Psychology Sciences, Faculty of Social Science and Health Care, Constantine the Philosopher University in Nitra, Nitra, Slovak Republic; 4Department of Psychotherapy, Institute for Postgraduate Training in Health Care, Prague, Czech Republic; 5Laboratory of Behavioral Medicine, Neuroscience Institute, Lithuanian University of Health Sciences, Palanga, Lithuania; 6Department of Health Psychology and Pedagogy, University of Latvia, Riga, Latvia; 7Department of Psychology, Riga’s Stradins University, Riga, Latvia; 8Department of Health Psychology, Faculty of Public Health, Lithuanian University of Health Sciences, Kaunas, Lithuania
Correspondence: Jan Prasko, Department of Psychiatry, Faculty of Medicine and Dentistry, Palacky University Olomouc, University Hospital, I. P. Pavlova 6, Olomouc, 77520, The Czech Republic, Tel +420 603 414 930, Email [email protected]
Background: Existential concerns such as meaninglessness, isolation, freedom, responsibility, and death anxiety represent core dimensions of human suffering and may underlie chronic psychological distress, particularly in patients with personality pathology. Although schema therapy implicitly addresses such themes, their systematic integration has remained conceptually underdeveloped.
Methods: This paper presents a narrative review and theoretical synthesis of schema therapy and existential psychotherapy, including existential analysis and logotherapy. Relevant literature was identified through searches of PubMed, PsycINFO, Web of Science, and Google Scholar. Theoretical integration was complemented by de-identified composite clinical vignettes derived from accumulated clinical experience.
Results: The paper introduces an existentially informed schema therapy framework in which existential concerns are conceptualized as interacting with early maladaptive schemas and schema modes, while the clinical illustrations demonstrate how existential reflection may be incorporated into standard schema therapy interventions.
Conclusion: Schema therapy with an existential dimension offers a coherent conceptual framework and a clinically promising direction for addressing existential suffering in patients with complex psychological disorders. Integrating existential perspectives may deepen meaning-making, strengthen the Healthy Adult mode, and support identity integration and more authentic engagement with life. Future empirical research is needed to evaluate its clinical effectiveness and mechanisms of change.
Keywords: schema therapy, existential psychotherapy, schema modes, meaning in life, personality disorders
Introduction
Existential concerns such as meaninglessness, isolation, freedom, responsibility, and awareness of mortality constitute fundamental dimensions of human existence and represent a significant source of psychological suffering across diagnostic categories.1–3 These concerns often become particularly salient in individuals with chronic emotional distress, personality pathology, and identity instability, where symptoms persist despite standard psychotherapeutic interventions.4,5 Existential psychotherapy conceptualizes psychological suffering as rooted in “problems of living” rather than discrete symptoms, emphasizing meaning-making, authenticity, and responsibility as core therapeutic aims.6–8 Despite shared phenomenological and humanistic assumptions, existential concerns have not yet been systematically integrated into schema therapy’s conceptual model, often remaining implicit or deferred to later therapy phases.4,5
Schema therapy represents a theoretically rich and clinically structured integrative psychotherapy originally developed to address early maladaptive schemas and unmet emotional needs in patients with personality disorders.9,10 As a result, existential suffering is often addressed implicitly or without a clearly articulated conceptual framework linking existential themes to schemas and modes.9,11 This conceptual gap may limit the capacity of schema therapy to fully address patients who report chronic emptiness, loss of meaning, fear of freedom, or existential anxiety despite measurable progress in symptom reduction.
The present article aims to address this gap by proposing a coherent integration of existential psychotherapy into schema therapy. We introduce an existentially informed schema therapy framework that conceptualizes existential concerns as dynamically interacting with early maladaptive schemas, coping styles, and schema modes across developmental stages. Rather than viewing existential themes as an optional or terminal phase of therapy, we argue that existential needs—such as meaning, authenticity, responsibility, and transcendence—can be systematically integrated into schema conceptualization, experiential work, and behavioral change.12,13 This perspective extends recent theoretical developments in schema therapy that emphasize self-coherence, fairness, and the experience of a meaningful world as core psychological needs.10
In addition to outlining theoretical convergences between schema therapy, existential psychotherapy, existential analysis, and logotherapy, this article provides practically applicable clinical guidance for therapists. Using de-identified composite clinical vignettes, we illustrate how existential questions, experiential techniques, and value-oriented behavioral experiments can be incorporated into different phases of schema therapy. In doing so, schema therapy with an existential dimension extends the therapeutic focus from alleviating distress toward supporting patients in living more authentic, meaningful, and self-directed lives.6,12,14,15
Although schema therapy and existential psychotherapy share important phenomenological and relational foundations, existential concerns have not yet been systematically integrated into schema therapy’s conceptual model. The present article addresses this gap by proposing a coherent framework in which existential concerns dynamically interact with early maladaptive schemas, coping styles, and schema modes across development and clinical practice.
Methods
Design
This paper is a narrative review with a practice-oriented theoretical synthesis aimed at mapping conceptual overlaps between schema therapy and existential psychotherapy and translating these overlaps into clinical procedures.
Search Strategy
We searched PubMed, PsycINFO, Web of Science, and Google Scholar for English-language sources using combinations of the terms “schema therapy”, “early maladaptive schemas”, “schema modes”, “existential psychotherapy”, “existential analysis”, “logotherapy”, “meaning in life”, “death anxiety”, “existential isolation”, “freedom”, and “responsibility”. Reference lists of key articles and book chapters were hand-searched to identify additional relevant sources.
Eligibility and Selection
We included (a) foundational texts in schema therapy and existential psychotherapy, (b) theoretical papers discussing integration of existential themes into CBT/schema therapy, and (c) empirical and clinical papers relevant to meaning-making, existential anxiety, and personality pathology. We prioritized peer-reviewed literature and widely cited scholarly books. Sources were screened for relevance by the senior authors and synthesized into thematic domains corresponding to the existential “givens” and schema therapy constructs (needs, schemas, modes, coping).
Synthesis Approach
Findings were synthesized narratively into (1) theoretical convergences and (2) practical application steps, with clinical techniques illustrated through de-identified composite vignettes.
Given the conceptual nature of this paper, the aim was not to test efficacy but to develop a theoretically coherent and clinically grounded framework that can serve as a basis for future empirical investigation.
All clinical material is presented in the form of de-identified composite vignettes based on multiple clinical experiences; no identifiable patient information is included, and the manuscript does not report original clinical data requiring institutional ethical approval.
The composite clinical vignettes presented in this paper primarily reflect patients with moderate to relatively high levels of functioning, who were able to engage in reflective dialogue and experiential techniques. This may have facilitated the integration of existential themes into schema therapy. The applicability of this approach to patients with lower levels of functioning, severe instability, or limited reflective capacity may require adaptation, including a stronger emphasis on stabilization, pacing, and supportive interventions.
Theoretical Framework
Schema therapy is an integrative psychotherapeutic approach that conceptualizes psychological disorders as the outcome of chronically unmet emotional needs, early maladaptive schemas (EMS), and dysfunctional schema modes that develop in adverse relational contexts and persist across the lifespan.9,10 Within this framework, psychopathology is understood not as a collection of isolated symptoms but as a coherent pattern of cognition, emotion, and behavior shaped by early interpersonal experiences and maintained through maladaptive coping strategies.
In Young et al’s original formulation, core emotional needs include: (1) secure attachments to others (safety, stability, nurturance, and acceptance), (2) autonomy, competence, and a sense of identity, (3) freedom to express valid needs and emotions, (4) spontaneity and play, and (5) realistic limits and self-control.9 Young’s model articulated these needs primarily at a conceptual level, as part of the developmental explanation of early maladaptive schemas, rather than as an empirically formalized structure. More recent work has begun to refine and empirically examine the organization of core emotional needs. For example, Louis et al16 identified four higher-order domains—Connection and Acceptance, Healthy Autonomy and Performance, Reasonable Limits and Healthy Standards, and Reciprocity—thereby extending the empirical basis of schema therapy’s needs model. In this context, meaning is not presented here as part of Young’s original list, but rather as an existential dimension that may enrich and extend schema therapy’s conceptualization of human needs.
More recent developments in schema theory have emphasized additional needs related to fairness and self-cohesiveness, reflecting increasing attention to identity integration and the subjective experience of a coherent and meaningful self.10 When these needs remain unmet, early maladaptive schemas emerge as enduring belief structures about the self, others, and the world, accompanied by intense affective responses and rigid behavioral patterns.9,10,13
Schemas are activated by situational triggers reminiscent of early adverse experiences and give rise to characteristic coping responses—schema surrender, avoidance, or overcompensation—that aim to reduce emotional distress while paradoxically reinforcing the schema over time.9 In contrast, healthy coping involves the capacity to recognize schema activation, regulate emotional responses, and respond flexibly in ways that support need fulfillment and adaptive functioning.13
To capture the moment-to-moment dynamics of schema activation, schema therapy employs the concept of schema modes, defined as transient emotional–cognitive–behavioral states reflecting the interaction of schemas and coping styles.9,10 Dysfunctional modes include, among others, the Vulnerable or Abandoned Child, the Punitive or Demanding Parent, the Impulsive or Angry Child, and various Overcompensator modes such as the Self-Aggrandizer. Functional modes, by contrast, include the Happy Child and the Healthy Adult, often encompassing qualities of a Kind or Nurturing Parent.9,17 Therapeutic change is conceptualized as the gradual weakening of dysfunctional modes and the strengthening of the Healthy Adult, understood as a reflective, self-regulating mode capable of meeting emotional needs in adaptive ways.13
Schema therapy integrates cognitive, experiential, behavioral, and relational interventions to facilitate change at multiple levels. These include psychoeducation, cognitive restructuring, imagery rescripting, chairwork, historical role-play, behavioral experiments, homework assignments, and guided discovery.9,18 A defining feature of schema therapy is limited reparenting, through which the therapist seeks, within appropriate professional boundaries, to meet core emotional needs that were insufficiently met during childhood and thereby provide a corrective relational experience, while maintaining appropriate professional boundaries.9,18–20
Traditionally, existential concerns were not an explicit focus of cognitive-behavioral therapy, and future orientation was often confined to relapse prevention or goal setting in later treatment phases.11 However, developments within the so-called “third wave” of CBT have increasingly emphasized experiential processes, authenticity, values, self-determination, and the therapist’s presence as an engaged person rather than a technical expert.9,20,21 These shifts have created conceptual space for integrating perspectives historically associated with humanistic and existential psychology.
Existential psychotherapy encompasses a diverse group of approaches grounded in existential philosophy and phenomenology, including existential analysis, existential-humanistic therapy, and existential-integrative therapy.4–6 Despite their diversity, these approaches converge in their focus on fundamental “givens” of human existence—such as freedom, responsibility, isolation, mortality, and meaninglessness—that cannot be eliminated but must be confronted and integrated into one’s life.6,7 From this perspective, psychological suffering is understood less as a disease entity and more as an expression of difficulties in living, reflecting attempts to manage existential anxiety and uncertainty.4,8
Within this broad tradition, Viktor Frankl’s logotherapy occupies a prominent position by explicitly conceptualizing the will to meaning as a primary motivational force in human life.1 Logotherapy emphasizes the individual’s capacity to choose an attitude toward life circumstances, even in the face of suffering, and employs meaning-oriented interventions such as Socratic dialogue, dereflection, and paradoxical intention to support value-based engagement with life.1
Taken together, schema therapy and existential psychotherapy show important areas of compatibility, particularly regarding subjective experience, therapeutic relationship, agency, and the search for coherence in lived experience.
This convergence suggests that existential concerns can be meaningfully integrated into schema therapy, particularly in patients whose difficulties are characterized by chronic emptiness, identity disturbance, or struggles with meaning.
Similarities of Schema Therapy and Existential Psychotherapy
Rather than representing distinct or competing paradigms, schema therapy and existential psychotherapy show clinically important areas of compatibility, especially in their attention to lived experience, agency, therapeutic presence, and the meaning attributed to internal and interpersonal events. Both approaches adopt a phenomenological stance, prioritizing the individual’s lived experience and the meaning attributed to internal and interpersonal events over purely symptom-focused explanations.5,6,9 This shared orientation positions therapeutic work firmly in the here-and-now, where past relational patterns are actively re-enacted and transformed within the therapeutic relationship.
This convergence further suggests a shared emphasis on emotional experience and reflective awareness. While acknowledging unconscious processes, both approaches primarily focus on conscious and semi-conscious experiential processing, fostering the individual’s capacity to recognize, understand, and transform emotional responses.4,9 In this sense, schema therapy’s work with schemas and modes parallels existential psychotherapy’s focus on lived experience, emotional resonance, and personal meaning.
A particularly important point of convergence concerns agency, choice, and responsibility. Schema therapy conceptualizes psychological health as the capacity to activate a Healthy Adult mode capable of reflective decision-making and adaptive self-regulation.9,17 Existential psychotherapy similarly views human beings as fundamentally responsible for shaping their lives through choices, even within the constraints imposed by biological, social, and historical conditions.2,6 This shared emphasis challenges deterministic models of psychopathology and highlights the individual’s potential for growth and self-authorship.
The therapeutic relationship represents another core area of overlap. In schema therapy, limited reparenting provides a secure relational context for emotional exploration and corrective experiences.9 Existential psychotherapy likewise emphasizes the therapist’s authenticity, presence, and willingness to engage with existential concerns as essential therapeutic factors.6,7 In both approaches, the therapist functions not as a neutral technician but as an engaged participant in a meaningful interpersonal encounter.
Several existential psychotherapy strategies appear particularly compatible with schema therapy and may enhance its effectiveness, especially in patients with pronounced existential distress. These include the explicit confrontation of existential themes, such as meaning, freedom, responsibility, and mortality, which can illuminate how early maladaptive schemas constrain life choices and reinforce avoidance of authenticity.22 In addition, existential perspectives on anxiety as an inevitable aspect of human existence align closely with schema therapy’s emphasis on emotional tolerance, mode awareness, and Healthy Adult functioning, offering a structured way to acknowledge and integrate existential anxiety without resorting to avoidance or overcompensation.4,5
This convergence suggests that existential concerns are not external to schema therapy but are deeply intertwined with schema formation, maintenance, and transformation. This insight provides the theoretical rationale for the structured integration outlined below.
Integration of Schema Therapy and an Existential Perspective
Schema therapy with an existential dimension is grounded in the assumption that psychological suffering arises not only from unmet emotional needs in early attachment relationships, but also from unmet existential needs that persist across the lifespan. While classical schema therapy emphasizes the developmental origins of early maladaptive schemas in childhood experiences with caregivers, an existentially informed perspective extends this model by recognizing that individuals continuously face existential challenges related to meaning, freedom, responsibility, authenticity, and transcendence throughout adulthood.13,23 When these existential needs remain unmet or are persistently avoided, they may interact with early maladaptive schemas and schema modes, contributing to chronic experiences of emptiness, existential anxiety, resignation, or nihilism.
From this perspective, dysfunctional schemas and schema modes can be conceptualized as maladaptive yet understandable responses to existential dilemmas, initially serving a protective function against overwhelming anxiety, loss, or disconnection, but later constraining personal growth and meaningful engagement with life. Schema therapy with an existential dimension therefore aims not only to modify dysfunctional schemas and coping styles, but also to facilitate active engagement with existential questions that shape identity, values, and life direction. Although constructs such as responsibility, authenticity, and life engagement are not unique to existential psychotherapy, existential traditions place particular emphasis on meaning, finitude, mortality, and the human confrontation with ultimate concerns; for some patients, spiritual or religious frameworks may also shape how these concerns are experienced and resolved. This integration deepens schema therapy’s existing developmental and needs-based focus by adding more explicit attention to meaning, responsibility, authenticity, and life direction, thereby supporting the development of a coherent, meaningful, and self-directed life narrative.
Acceptance represents a central point of convergence between existential psychotherapy and schema therapy’s principle of limited reparenting. Existential approaches emphasize an accepting and respectful stance toward the individual’s lived experience, viewing the client’s perspective as a meaningful expression of their way of being in the world rather than as irrational or deficient.6,13 Similarly, schema therapy prioritizes empathic attunement, emotional validation, and corrective relational experiences within a therapeutic relationship characterized by authenticity, warmth, and appropriate limits.9,23 In both approaches, understanding the client’s subjective reality precedes attempts at change, fostering psychological safety and openness to exploration.24–26
Clinically, schema therapy with an existential dimension employs standard schema therapy techniques while placing greater emphasis on existential themes and meaning-oriented interventions. A core component involves the systematic use of existentially focused questions addressing values, responsibility, choice, authenticity, and life priorities. Embedded within a schema formulation, such questions help patients recognize how dysfunctional schemas and modes restrict meaningful life choices and reinforce avoidance of responsibility or authenticity.1,22
Existentially informed experiential techniques further deepen this process. Existential imagery builds on established imagery rescripting methods by incorporating future-oriented reflection on life choices, missed opportunities, and alternative paths, allowing patients to emotionally process the consequences of different value-based decisions. In this way, experiential work links emotional processing with purpose and meaning, rather than focusing primarily on past trauma, adverse childhood experiences, and the deprivation of core emotional needs.1,13
Behavioral change is supported through existential experiments that parallel schema therapy’s behavioral interventions while explicitly targeting existential needs. Within the therapeutic relationship, here-and-now experiments explore responsibility, authenticity, and interpersonal engagement, using techniques such as limit-setting and empathic confrontation to address modes associated with avoidance or inauthentic self-presentation.9,17 In there-and-then contexts, patients are encouraged to engage in concrete, value-consistent actions, such as relational risk-taking, creative expression, or engagement with spiritual, cultural, or community-based sources of transcendence, thereby translating existential insight into lived experience and strengthening the Healthy Adult mode as an agent of choice and responsibility.14
Taken together, this integration constitutes a conceptual contribution to schema therapy by systematically linking existential needs with schemas, schema modes, and therapeutic processes. The following section translates this conceptual model into a structured and clinically applicable framework for psychotherapy practice.
Practical Application
Schema therapy with an existential dimension operationalizes the proposed conceptual integration by systematically embedding existential reflection into standard schema therapy processes across the course of treatment. Rather than introducing new techniques, this model specifies how and when existential themes, such as meaning, responsibility, authenticity, and life direction, are addressed within established schema therapy phases. The phased structure outlined below translates the conceptual framework into a clinically applicable treatment trajectory. The phase numbering (1–20) reflects a structured, though flexible, progression commonly used in schema therapy to organize treatment across assessment, experiential work, cognitive integration, and behavioral change, rather than rigid or strictly sequential stages.
Phases 1–3: Evaluation and Case Conceptualization
The initial phase involves a comprehensive assessment that integrates standard schema therapy procedures with an explicit focus on existential needs. In addition to clinical interviews and validated questionnaires, case conceptualization links the patient’s life narrative, early maladaptive schemas, and dominant schema modes with existential themes such as meaning, values, responsibility, authenticity, and transcendence. The therapeutic alliance is established through empathic attunement and limited reparenting, while the rationale and goals of existentially informed schema therapy are collaboratively formulated. This phase provides a coherent framework that connects developmental origins of schemas with current existential concerns and future-oriented life goals.
Phases 4–9: Emotional Processing and Experiential Work
During the emotional processing phase, experiential techniques central to schema therapy; such as imagery rescripting, chairwork, and here-and-now experiments, are used to access and transform emotionally charged schema modes.9,13,14 Within an existentially informed framework, these interventions explicitly address experiences related to existential anxiety, loss of meaning, restricted life choices, and avoidance of responsibility.12,27 Limited reparenting within the therapist’s Healthy Adult (including Kind Parent) mode provides emotional containment and validation, enabling patients to tolerate intense affect while exploring alternative, more authentic ways of relating to themselves, others, and their life circumstances.23
Phases 10–15: Cognitive Integration and Meaning-Oriented Reflection
In this phase, cognitive and reflective interventions consolidate changes achieved through experiential work. Psychoeducation about schemas, schema modes, and emotional needs is complemented by structured mode dialogues and cognitive restructuring of schema-driven beliefs. Existential questions are systematically incorporated to address patients’ perspectives on the future, responsibility for choices, personal values, and life direction. Therapeutic work focuses on strengthening the Healthy Adult and Happy Child modes, facilitating a shift from schema-driven survival strategies toward reflective, value-consistent decision-making and an increasingly coherent sense of identity.
Phases 16–20: Behavioral Change and Value-Based Action
The final phase emphasizes translating emotional and cognitive change into everyday life. Behavioral experiments, homework assignments, communication training, and “there-and-then” existential experiments support patients in acting in accordance with their personal values and chosen life goals.9,19 Behavioral change is framed not merely as symptom reduction, but as the enactment of a consciously chosen way of living. This phase supports responsibility-taking, tolerance of uncertainty, and engagement in meaningful activities and relationships, thereby consolidating the Healthy Adult mode as an agent of choice, responsibility, and meaning-making (Figure 1).
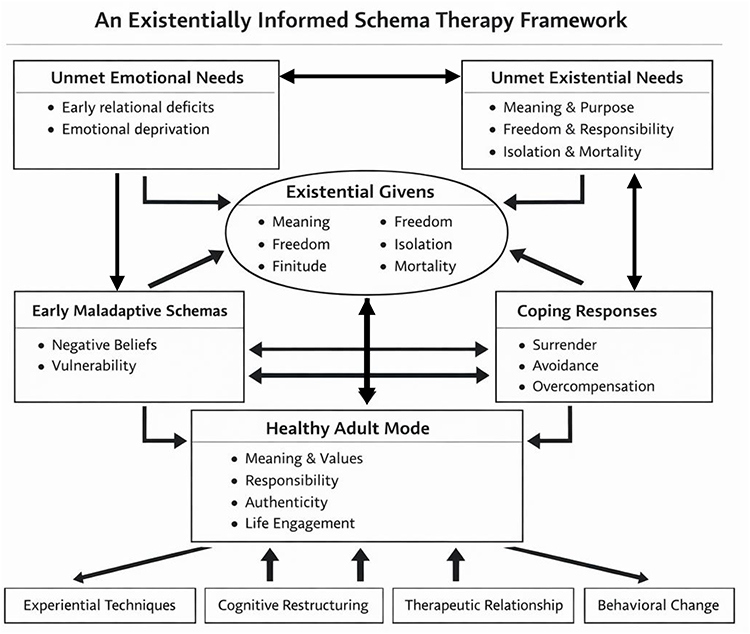 |
Figure 1 An existentially informed schema therapy framework. This figure illustrates the proposed conceptual integration of schema therapy and existential psychotherapy. The model depicts how unmet emotional needs and existential concerns interact across the lifespan, contributing to the development and maintenance of early maladaptive schemas and schema modes. The model preserves the central schema therapy assumption that early maladaptive schemas primarily arise from unmet emotional needs, while additionally illustrating how existential concerns dynamically interact with schema activation, coping styles, and mode functioning. Bidirectional arrows indicate reciprocal influences between existential concerns, schema modes, and coping processes, reflecting their dynamic interaction across the lifespan. Therapeutic change is conceptualized as the strengthening of the Healthy Adult mode as a multidimensional integrative agent mediating between emotional needs and existential concerns through experiential, cognitive, relational, and value-based interventions. |
Case Reports
This section illustrates the clinical applicability of the proposed conceptual contribution through selected case reports. All cases are presented as de-identified composite clinical vignettes derived from accumulated clinical experience and do not refer to identifiable individual patients. The cases demonstrate how schema therapy enriched by an existential perspective can address not only early maladaptive schemas and schema modes, but also existential themes such as meaning, responsibility, freedom, and fear of abandonment. Each case exemplifies how experiential, relational, and value-oriented interventions support the strengthening of the Healthy Adult mode and facilitate meaningful life engagement.
Case 1: Anna
Anna is a 35-year-old woman diagnosed with dependent personality disorder. She is married and has two school-aged children. Anna presents with chronic low self-esteem, a pronounced need for approval, and a pervasive fear of abandonment. Her interpersonal functioning is characterized by submissiveness, difficulties expressing needs and boundaries, oscillations between compliance and resentment, and recurrent doubts regarding the meaning and direction of her life.
From a schema therapy perspective, Anna exhibited prominent early maladaptive schemas including Abandonment, Dependence/Incompetence, Subjugation, Defectiveness/Shame, Failure, and Mistrust/Abuse. These schemas were predominantly activated within the Vulnerable/Abandoned Child, Compliant Surrenderer, Punitive Critic, and Angry/Impulsive Child modes.
Therapeutic work focused on stabilizing the therapeutic alliance through limited reparenting, enhancing emotional safety, and gradually fostering Anna’s Healthy Adult and Kind Parent modes. Experiential techniques, particularly imagery rescripting and chairwork, were employed to process early relational trauma, challenge the internalized Punitive Critic, and support emotional differentiation from maladaptive coping modes.
In parallel, existential interventions were integrated to explicitly address themes of choice, responsibility, autonomy, and meaning. Rather than offering directive advice, the therapist consistently emphasized Anna’s existential freedom and responsibility for her life decisions, thereby counteracting her habitual dependency patterns.
Therapist:Hello, Anna. Thank you for coming. How are you feeling today?
Anna:Hello. I feel tired and sad. I do not feel like doing anything.
Therapist:I am sorry to hear that. What happened?
Anna:Paul told me again that I am stupid and worthless and that no one else would want me, and I should be grateful that he is with me. I do not know if I should stay with him or divorce him. It cannot go on like this; he’s bothering me. Could you help me? Should I stay with him or divorce him? What is best for me?
Therapist:I cannot advise you on that. Everyone makes such an important choice for themselves. However, I can help you understand how different needs affect this decision. I can also accompany you in finding what is important to you, which needs and values enter your choice.
Anna:But he really hurts me. And I cannot decide for myself.
Therapist:That sounds very painful… What do you experience when you are with your husband?
Anna:I feel inner pain and hopelessness. Then I get mad at him.
Therapist:It is understandable. How did you react to that?
Anna:I just kept silent and nodded my head. I do not know what to say. I am afraid that if I contradict him, he might leave me, and it will be even worse. But other times, I blame him for leaving a coffee mug in the living room. Then we fight, and I get scared that he will leave me. Other times, on the other hand, I think about divorcing him. That’s how it changes in me. I am confused about it. I do not know what I want. In the end, I am afraid that I will be alone.
Therapist:I understand it’s still hard for you to imagine being alone. Are you scared? But do you know that what he is telling you is not true? When we worked with the Defectiveness schema, you started recognizing that you are a valuable and loving woman…
Anna:At that moment, I felt good for one day. But now I do not think so. I have never felt like this. From childhood, my parents told me that I was bad and incapable. That I do not deserve love or respect!
Therapist:That must have been very difficult for you. And how do you feel now?
Anna:When I think about it, I feel helpless and hopeless. I feel like a little abandoned child.
Therapist:I want to help you feel better. To find your strength and freedom, it is important to change your negative self-attitudes and schema modes that trouble and limit you.
Anna:That does not look very easy. And can it be changed?
Therapist:We will look for alternative ways of perceiving and reacting to situations. We will strengthen your Healthy adult who can face problems and find solutions.
Anna:And how do we do it?
Therapist:We will use different methods of schema therapy and existential therapy. For example, we will rescript upsetting things from the past in imagery and change the story for a better outcome. We will do experiments with behaviour in and outside of the session. I always explain it to you before we do anything. You then choose whether we try it or not.
Anna:But this often causes a problem for me. I usually cannot decide on important things. I need to talk to someone.
Therapist:That’s normal. Choice brings responsibility. When we have the impression that we cannot rely on ourselves, it is difficult for us to choose. However, deciding for yourself is very important. It allows us to fulfil our needs and do what gives us meaning. We can shape our lives according to our values and chosen goals. I suggest that we do a chair experiment together on this topic. What do you think about it?
Anna:Okey. I do not know what it is, but I will see.
Therapist:Good. Here, we have two chairs facing each other. On one, you will sit as little abandoned Anna who feels fear and helplessness in her relationship with her partner. And on the other hand, you’ll be sitting in the other chair as the Healthy Adult Anna - feeling free, self-assured and strong. We will try to make it so that you can talk to yourself from the perspective of the Abandoned Child and the Healthy Adult. We start with you sitting in the first chair as the Abandoned Child.
Anna (sits on the first chair)Good.
Therapist:Now tell me, as the abandoned Anna - how do you feel about your relationship with your partner? What do you need? What do you want?
Anna (as the Abused Child mode):I feel terrible about my relationship with him. I feel like his slave or toy. He does not give me love or respect or support or anything good. He hurts me with words and actions. I need love, care and help from him, others, and myself. I want to be happy and satisfied in my life. I will never get his love and support. He will never change. He is mean and selfish. He’s just using me and manipulating me.
Therapist:This is a painful realization. I feel with you. You would like your husband to show you love and care, but he does not. I have a question for you. It may be even more important than what your spouse is doing. What do you do for yourself? How do you take care of yourself?
Anna (as the Abused Child mode):I cannot care for myself. I do not know how to do it. I am clueless. I am dependent on him. I am afraid of being alone and abandoned.
Therapist:I understand. I feel for you, Anna. It’s uncomfortable to feel this dependent. Now, let us try to find out if there is something in which you are not clueless and helpless. Try to find something where you make decisions on your own without your husband.
Anna (as the Abused Child mode):I do not know about anything like that.
Therapist:I believe that together, we will find it. Now I’d like you to sit in the other chair as a Healthy Adult and tell me what she sees when she watches Abused Child.
Anna (sitting in the other chair like a Healthy Adult):Okay.
Therapist:Now tell me like a Healthy Adult looking at the facts. What do you think of Anna? There is something she is good at or has done quite well in the past. Try to think of what she did or is doing independently without consulting. It can be at home, at work, or in your free time. Maybe we can start with your work…
Anna (sitting in the other chair like the Healthy Adult mode):When I think broadly about it, I realize I make my own decisions at work. I make decisions independently because the company’s management is far away, and I am expected to make decisions. I do not have any problems there. It’s true; I am independent at work, and others depend on my choices, so I am also responsible.
Therapist:I see that you make decisions completely independently at work. You are responsible because other people depend on you. How satisfied are they with your decision-making?
Anna:People praise me. Management appreciates me for being independent and responsible.
Therapist:They appreciate your independence and responsibility. It makes me happy. And what about those other areas - in the family and in free time?
Anna:I also make decisions at home, for example, about shopping, about children’s free time activities, and also about where we will go on vacation or for the weekend. I also chose the furniture for the apartment. My husband leaves that to me.
Therapist:You seem to make important decisions at home. Are there also things your husband consults you about?
Anna:Yes, he consults me on some matters. For example, when we were buying land for a house or when we were choosing the design of the house, I had the decisive word. He also advises me when purchasing a new car. At the same time, it’s typically a man’s thing, but he always wanted to discuss it with me.
Therapist:Your husband seems to rely a lot on you.
Anna:I did not even realize it.
Therapist:Now tell me like a Healthy Adult. How do you feel about your relationship with your husband? What do you need, and what do you want?
Anna (in the Healthy Adult mode):When I look at my Abused Child, I realize I feel frustrated and angry in the relationship. I feel trapped. I would need him to show me love, respect, and support. It hurts me not to feel that from him. I want to be happy and satisfied in life. But I cannot get it from him. When I look at it from the point of view of a Healthy Adult, I realize that my husband relies on me for things and talks to me about important things. From this point of view, I can see that he respects my decision. From this point of view, I can see that they respect my decision. Maybe it would be nice to ask him if he likes me and if he could support me more.
Therapist:I like that you see the situation more comprehensively from the perspective of a Healthy Adult. You talk about needing expressions of love and appreciation from your husband. You also talked about asking him for them. That seems to be very free-thinking. In what way would you tell him if you freely choose to do so?
Anna:I guess I could tell him I need him because he is important. It is very important that he let me know that I am also important to him or that he likes me. I would also need him to appreciate me some time.
Therapist:That’s much courage to ask for fulfilling your needs. I must appreciate it because most people do not dare to do it. They passively wait for the other to do it and get angry when the other does not.
Anna:I did not do it either, but I will be braver and freer if possible. However, I do not know if I will have the courage to do it.
Therapist:We are going to put your husband in that chair here. You can imagine him sitting there if you want. It’s better for you if that chair is empty or if we put some symbol there, like a plush toy you can choose (open a box with different stuffed toys).
Anna:This dog with a scarf and glasses could be my husband. He’s also a bit of a gentleman, wears glasses, and cares about elegance.
Therapist:Absolutely. You chose a cute stuffed animal. What would you like to say to him? He symbolizes your husband…
Anna:Paul, I would like to talk to you. I want to tell you that you are important to me. And not only because we have two children together, but because I still love you. Sometimes, I get mad at you and argue, but I still love you. I need to know from you that I am important to you, too. That you also appreciate what I do for you and the children. It would help me if you could understand me some time. I did not appreciate you and took everything you did for the family for granted. But now I want to tell you that I like how you treat children. I am grateful to you for caring for the house and the car, and I appreciate how you manage our money. And you still impress me as a man.
Therapist:That sounds very good. I think there’s a chance your husband will hear it.
Anna:I never said anything like that to him. I want to try it.
Therapist:Now, you have decided to be bold about meeting your own needs, but you have also, as I perceived it, taken care of your husband’s needs. I did not ask you to do that, but you freely decided. I liked it. Now, I want to ask if you could think about how you can willingly fulfil your needs so that it is not dependent on others. What can you decide about how to take care of your needs? What can you do for yourself? How can you take care of yourself?
Anna (in the Healthy Adult mode):I try to care for myself. For example, I take care of my nails. I also eat healthily. I am learning how to communicate better with you. I try to realize and express my needs, feelings and opinions to my husband. I also try to say no and set boundaries for my husband, children and management. I also try to find what has value and meaning in life.
Therapist:That sounds very good. Please explain to me how you do it.
Anna (as the Healthy Adult mode):I am doing it with your help. Because you supported me, I started exercising, listening to music, and eating healthy.
Therapist:I am glad about that. But are you taking care of yourself or me? Did you do it for yourself or me?
Anna (as the Healthy Adult mode):You are right, for my own sake. But with your support.
Therapist:I will happily support you in any independent decision you make. Now, I would like to return to the situation with Paul, who told you that you are stupid and worthless and that no one else would want you, and you should be grateful that he is with you. When you look at it from your Healthy Adult perspective, what do you say?
Anna: (speaking to the chair where the stuffed animal representing the husband is sitting):It hurts when you say this to me. It hurts me. I understand that you are angry with me for not agreeing with you. Still, please treat me with respect. I am mad at you right now, so I want to take a break. But I will happily return to it when we both calm down.
Therapist:And what does the husband say about that? Sit in his chair.
Anna (sitting in her husband’s chair and speaking for him):You annoy me too. You keep blaming me for something, and you are dissatisfied with everything.
Therapist:Try to return to your chair and answer.
Anna (in her role):You are right. I often complain and am dissatisfied. And then I wrong you. But in reality, I respect you and think a lot about how you take care of the house, the car and how you take care of the children. I love you. I feel like you do not love me anymore.
Therapist:What about the husband?
Anna (as husband):But I like you too. You bully me a lot, and I must also appreciate it sometimes.
Anna (as herself):You are right. I rarely tell you how important you are to me. But you are important to me. I still love you.
Therapist:Let us try to get out of role-playing. How are you feeling now, Anna?
Anna:It’s nice, and I am a little moved. If only it were true.
Therapist:You are right that it can happen in different ways. You would like to try and talk to your husband. It’s your choice.
Anna:I will try. I hesitated about whether to be with him for a long time and could not decide what was better for me. Now, I decided to give it a chance and try it. Because truth be told, I still love him.
Therapist:I am very glad you decide for yourself what you want. Now, it seems that there is a balance of reason and emotion in your decision. What do you think about it yourself?
Anna:I think there’s more emotion because I still love him. But there is already much sense. It helped me a lot when we talked about what decisions I make at home, at work and in my free time, and I realized that I make decisions in many things and I am not as dependent on my husband as I thought. I also realized after a long time that I still love him. And that’s important to me.
Therapist:May I ask you something more difficult? What would it mean for you to exist without him—not only practically, but as a person?
Anna:It feels frightening. As if I would lose not only him, but also the picture of who I am. As if I would disappear.
Therapist:So, the fear is not only of separation, but of losing your own existence as someone who matters?”
Anna:Yes… exactly. As if I had no value by myself.
Therapist:Then perhaps the question is not only whether to stay or leave, but what kind of life would be worth living for you—even if it includes loneliness, uncertainty, or pain.
Anna:I have never thought about it that way. I think I would want a life in which I can respect myself, where I am not only waiting to be chosen.
Schema–Existential Clinical Analysis
This case exemplifies how dependent personality pathology can be conceptualized not only as a manifestation of unmet emotional needs, but also as a disruption of core existential needs, particularly freedom, agency, and authentic self-authorship.
Anna’s dependence on her partner functioned as an existential avoidance strategy, protecting her from the anxiety associated with autonomy, responsibility, and potential loneliness. The therapist’s refusal to make decisions on Anna’s behalf was a deliberate existential intervention, reinforcing her capacity for choice while tolerating uncertainty and emotional discomfort.
Chairwork dialogues between the Abandoned Child and Healthy Adult modes served a dual function:
- schema-level restructuring of maladaptive beliefs about incompetence and worthlessness, and
- existential integration of responsibility, enabling Anna to experience herself as an active agent rather than a passive recipient of external validation.
The use of here-and-now experiments in relational communication facilitated a transition from schema-driven submission toward value-consistent behavior. Importantly, therapeutic change was not framed as eliminating relational anxiety, but as learning to act meaningfully despite it.
Overall, this case illustrates how an existentially informed schema therapy approach can transform dependency-driven suffering into a process of authentic decision-making, reinforcing the Healthy Adult mode as a locus of meaning, responsibility, and relational engagement.
Case 2: Peter
Peter is a 40-year-old man diagnosed with narcissistic personality disorder. He presents as confident, ambitious, and achievement-oriented, occupying a managerial position associated with high responsibility and social status. Interpersonally, Peter demonstrates pronounced sensitivity to criticism, a tendency toward devaluation of others, and difficulties forming stable and emotionally intimate relationships. Despite external success, he reports chronic feelings of emptiness, dissatisfaction, and a lack of meaning in life.
Schema assessment revealed prominent early maladaptive schemas including Approval-Seeking, Failure, Mistrust/Abuse, Unrelenting Standards, Entitlement/Grandiosity, Insufficient Self-Control, and Abandonment/Instability. Dominant schema modes included the Self-Aggrandizer, Punitive Critic, Angry/Impulsive Child, and Abandoned/Vulnerable Child.
Therapeutic work initially focused on establishing a stable therapeutic alliance, which required careful balancing of empathy and limit-setting due to Peter’s oscillation between devaluation and idealization. Experiential techniques, particularly imagery rescripting and chairwork, were used to process traumatic childhood experiences involving physical abuse and emotional abandonment by his father and inconsistent caregiving by his mother. These interventions facilitated access to the Vulnerable Child mode, which had been chronically avoided through narcissistic overcompensation.
The therapist systematically worked to weaken the Punitive Critic mode while strengthening the Healthy Adult and Kind Parent modes. As existential themes emerged—particularly emptiness, fear of loneliness, and lack of meaning—the therapist integrated existential reflection focused on values, freedom, responsibility, and meaningful engagement with life.
Therapist:Hello, Peter. Today, I would like to work with you on the mode of the Critic who constantly accuses and puts you down. Can you tell me what this mode tells you about you and your life?
Peter:My Critic repeatedly tells me I am incompetent, worthless, weak, and embarrassing. Also, I will never be different; no one likes me that. I am a poor, selfish liar who deserves punishment and abandonment.
Therapist:And how do you feel when this mode tells you this?
Peter:I feel terrible. I feel downtrodden, sad and lonely. I feel like a weak little child who is helpless and defenseless.
Therapist:I see. It must be hard. Do not know where this mod came from? Who has told or indicated this to you in the past?
Peter:Well, it was mainly Dad. Dad was a tyrannical alcoholic. He often beat me, knocked me down, and tormented me. He showed no love or appreciation. He told me I was useless and that I had failed him.
Therapist:It was not easy. And how did you react to his behaviour?
Peter:I was trying to please him. I tried to be good, obedient and study well. But it was never enough. He always found something to blame me for or beat me up for.
Therapist:So, you have learned that you must be perfect and better than others to deserve acceptance?
Peter:Yes, exactly.
Therapist:And how did it help and hurt you during your life?
Peter:It probably helped me a lot to be successful at work and in society. But it hurt me a lot in relationships. I could not trust others or show them who I was. I was afraid of their criticism and rejection. So, I either controlled people or ignored them.
Therapist:And how do you feel now?
Peter:Now I feel empty and unsatisfied. I see no meaning in life. I do not have any real friends or a partner. I am dating a woman who uses me but does not love me. I do not love her either; I just cannot be alone. I would feel like a total loser, so I maintain that relationship-non-relationship. We do not even sleep together anymore; she does not want to. She criticizes me for not doing more for her. At the same time, I feed and dress her. She does not have to work. She is doing well.
Therapist:That’s hard. You cannot give her up so you will not be alone, but you do not love her, and she does not love you. You said that she abuses you. And what would you like to change? What would you like instead?
Peter:I do not know, but I want to be happy and satisfied. I would like to have people who like me the way I am. I would also like to say that some things have meaning for me.
Therapist:When you speak about emptiness, I wonder what it tells you about how you have been living.
Peter:Maybe that I built everything around performance, but not around what is truly alive for me.
Therapist:And if success, admiration, and proving yourself were taken away, who would you be?
Peter:That is exactly what scares me. I am not sure I know.
Therapist:Then perhaps one of the central questions is not only how to silence the Critic, but what kind of life you are willing to take responsibility for—even if it is uncertain and does not guarantee admiration.
Peter:I think I would want a life that feels real, not only impressive.
Therapist:Those are legitimate wishes. And do you think it is possible to fulfil them?
Peter:I do not know. I think it is not easy.
Therapist:Why do you think that?
Peter:Because that Punitive Critic mode keeps telling me I cannot do it. That I do not deserve it.
Therapist:And what if we tried to oppose this mode? Prove him wrong? And tell him what we thought of him?
Peter:I do not know if it will work. How could we do this?
Therapist:We can use chairwork. A Punitive Critic will be sitting in that chair across from you. And you sit in this chair like a Healthy Adult. Your Healthy Adult is the part of you that recognizes you are valuable, lovable, and capable. This is the part of you that intelligently supports and protects you.
Peter:And what should I do?
Therapist:You can talk to the Punitive Critic. Tell him how you feel about him. Be it anger, pity, or helplessness before him. You can also tell him you no longer want to obey or submit to him. You can also tell him your wishes and needs.
Peter:And what will he answer me?
Therapist:You move to the other chair he is sitting on and answer as he does. And then you go back to your chair as a Healthy Adult.
Peter:That sounds weird.
Therapist:You are right. It is like a theatre. But dividing your experiences into Critic and Healthy Adult allows you to become aware of how you are hurting yourself and how to protect yourself.
Peter:Okay then. We can try it.
Therapist:Now you are sitting in this chair as a Healthy Adult, and across from you is your Punitive Critic. Look at him and tell him whatever you want.
Peter (in the Healthy Adult mode):Listen! I have had enough of your reproaches, lies and insults! You have nothing to do here! I will not let you ruin my life anymore!
(Peter moves to the other chair as the Punitive Critic).
Peter (in the Punitive Critic mode):What are you doing? Who do you think you are? You are just pathetic trash! You are incompetent! You are selfish and a liar! Nobody loves or wants you!
(Peter returns to his chair in the Healthy Adult mode).
Peter (in the Healthy Adult mode):That’s not true! You are pathetic trash! You are unable to encourage and care for me. I do not want you. Go away. You are an incompetent and evil parent! You are selfish and a liar! It bothers me that you did not give me love or appreciation! You were cruel and dropped me! Now, pull away!
(Peter moves to the other chair in the Punitive Critic mode).
Peter (in the Punitive Critic mode):That’s a lie! I gave you everything you needed! I gave you discipline and motivation! I wanted to help you be strong and successful!
(Peter returns to his chair in the Healthy Adult mode).
Peter (as the Healthy Adult mode):What you are giving me is no help! It’s abuse! You hurt me and abused me! You took away my happiness and the meaning of life!
(Peter moves to the other chair in the Punitive Critic mode).
Peter (in the Punitive Critic mode):That’s nonsense! You deserved it! You were bad and disobedient! You let me down and betrayed me!
(Peter returns to his chair in the Healthy Adult mode).
Peter (in the Healthy Adult mode):That’s a lie! I was neither bad nor naughty! I was a good and loving child! I did not let you down or betray you! You did not see or hear me!
(Peter moves to the other chair in the Punitive Critic mode).
Peter (in the Punitive Critic mode):That’s a lie! I saw and heard you! I knew you better than anyone! I loved you more than anyone!
(Peter returns to his chair in the Healthy Adult mode).
Peter (in the Healthy Adult mode):That was not love! That was manipulation and control! You did not want to see or hear me as I was! You tried to change me in your image!
(Peter moves to the other chair in the Punitive Critic mode).
Peter (in the Punitive Critic mode):That’s a lie! I wanted to protect and teach you to live in this harsh world! I tried to save you from pain and suffering!
(Peter returns to his chair in the Healthy Adult mode).
Peter (as the Healthy Adult mode):That’s not protection or learning! This is oppression and restriction! You caused me pain and suffering! You took away my freedom and identity! You listen! I never want to hear or see you again! I do not take you seriously or believe your words! I do not need you. I do not want you in my life! I already rejected you and threw you out of my head and heart!
Therapist:How is Peter now?
Peter:I am better, but I feel some sadness inside me. And empty, too. When I banish Critic mode, it’s like nothing happened.
Therapist:It’s as if another mode has been heard.
Peter:Yes, I feel abandoned. It will be the Abandoned Child. Without criticism, I feel alone and abandoned.
Therapist:Your Abandoned/Vulnerable Child will sit in this chair, and I am here for you as your therapist. What do you want to tell me?
Peter(in the Vulnerable child mode): I feel alone and abandoned. I do not know what to do. I need someone to guide me.
Therapist:Here on this chair sits the Kind Parent, and on this sits the Healthy Adult. Try switching to Kind Parent and answering the Vulnerable Child. Yes, it’s hard.
Peter (in the Kind Parent mode):I know you are feeling alone, and it’s not easy. But I will always be with you. Other people are with you, too. You know about them. They like you.
Therapist:Please tell him specifically who it is.
Peter:You have a good friend, Honza, who likes you very much. Your sister likes you very much too. You can call them anytime. And you can also be alone and not be bored. You enjoy working with wood, and you are good at it. And at work, you work for others. They like you. Maybe a little solitude would not hurt you.
Therapist:Try speaking directly as a Kind Parent to the Vulnerable Child sitting in your original chair.
Peter:Hello, little Peter. I am your Loving parent. I love you so much. I know you are smart. I am still with you, and I will always help you. You are never alone because I am always with you.
Therapist:Sit in little Peter’s chair and answer him.
Peter (in the Vulnerable child’s chair):That’s very nice to hear. I feel better.
Therapist:Try to put Peter in the Healthy adult chair and make a reasonable plan for the future. What would you like to do in the future so that it gives you meaning and joy?
Peter (in the Healthy adult chair):Well, I do not know…
Therapist:Well, how about starting with something simple and pleasant? Something that will entertain and relax you?
Peter (as a Healthy adult):Like what? Like listening to music, I like? Or read a book that interests me?
Therapist:That looks good. Choose something you want to do now.
Peter (as a Healthy adult):Okay. I choose to… listen to music.
Therapist:Good choice. And what kind of music do you want to listen to?
Peter (as a Healthy adult):I want to listen to… rock music.
Therapist:Rock music? It is interesting. And why rock music?
Peter:Because it gives me energy and courage. It makes me feel strong and free.
Therapist:That’s great. And what kind of rock music do you like? Do you have a favourite band or song?
Peter:Well, I like… AC/DC. And my favourite song is… Highway to Hell.
Therapist:AC/DC and Highway to Hell? That’s a classic. And what do you like about that song?
Peter:I like… the beat, the melody, the lyrics, the vocals.
Therapist:And what do the lyrics of that song tell you?
Peter:It tells me that life is an adventure and that I should enjoy it according to my rules. I should not let anything and no one spoil my joy, and I should follow my dreams and desires.
Therapist:That’s an interesting message. And do you feel that way when you listen to this song?
Peter:Yes, I feel that way. I feel good. I feel happy and satisfied.
Therapist:That’s perfect. I am glad you are feeling well. And what would you like to do now?
Peter:I do not know. Do you have any idea?
Therapist:Choose something you want to do now.
Peter:Okay. I choose to… dance.
Therapist:Good choice. And how do you want to dance? What style or movement?
Peter:Rock’n’roll.
Therapist:Rock’n’roll? That’s great. And can you dance rock’n’roll?
Peter:Not much. But I want to learn it.
Therapist:That’s perfect. Dance is about learning and trying, joy and relaxation.
Peter:Okay. So, I will do it.
Therapist:So now stand up and start dancing to the music. And I will give you tips and encourage you. Now you are on your feet and start dancing to the music. And I am here for you as your therapist. What do you want to tell me?
Peter:That’s fun. I feel good. I feel free and alive.
Therapist:That’s great. I am glad you are having fun. And see how well you are doing. How well do you move and keep the rhythm?
Peter:Yes, I see. Thank you.
Therapist:You are welcome. And what would you like to do now? What would you like to try?
Peter:Well, how about trying some steps or figures? Or imagine dancing with someone I like? Or invent style or choreography?
Therapist:That sounds good. Will you go for it?
Peter:I could. I choose... to imagine myself dancing with someone I like.
Therapist:Good choice. And who is that someone you like?
Peter:She’s... my friend Lenka.
Therapist:Lenka? That’s a nice name. And what is Lenka like?
Peter:Lenka is... very kind and nice. She is my friend from work. We have a lot in common.
Therapist:That’s nice. And what do you have in common?
Peter:Well, we like the same music, movies, books. And also similar humour and opinions, similar goals and dreams.
Therapist:That’s great. And what are your goals and dreams?
Peter:We want to be happy and satisfied, have good relationships with people, and do something meaningful and useful.
Therapist:Those are nice goals and dreams. And how do you manage to fulfil them?
Peter:Well, we try to be good people. To be kind, honest, considerate and noble. Helping others and protecting nature.
Therapist:That’s amazing. And how do you feel when you do it?
Peter:I feel good. I feel proud and satisfied.
Therapist:That’s great. And what would you like to do now? What would you like to try?
Peter:Well, how about imagining some nice experience with Lenka? Something we have experienced together or would like to experience?
Therapist:So, try it. Choose something you want to visualize now.
Peter:I imagine… that we are on vacation together. That we are on the beach by the sea. The weather is beautiful and sunny. We swim, sunbathe, and play with sand.
Therapist:That’s very nice. And how do you feel when you imagine that?
Peter:I feel very good, relaxed and joyful.
Therapist:That’s great. And what are you doing with Lenka? How does she react?
Peter:We laugh together, we talk, we hug each other. We are kissing.
Therapist:And how do you feel when you do that?
Peter:I feel good. Loved and happy.
Therapist:That’s great. And what would you like to do now? What would you like to try?
Peter:I do not know. Do you have any idea?
Therapist:Well, how about imagining you are together in the future? That you are together long and happily?
Peter:I could.
Therapist:So, try it. Choose something you want to present now.
Peter:I imagine... we are married. We have a nice house and garden. We also have two children and a dog. We are satisfied and happy.
Therapist:That’s very nice. And how do you feel when you imagine that?
Peter:I feel good. I feel fulfilled and grateful. I imagine… that we are older and wiser together. We experienced many beautiful and difficult moments together but are still in love and happy.
Therapist:And where is your Punitive Critic?
Peter:I forgot about that. It’s gone, completely replaced by a Kind parent, Healthy adult, and Happy child. I am glad I found it.
Therapist:Me too. And I congratulate you for making it so that you have freed yourself from the Punitive Critic and built a Happy child with the support of a Healthy adult and Kind parent.
Schema–Existential Clinical Analysis
From a schema therapy perspective, Peter’s narcissistic functioning can be understood as a dominant overcompensatory strategy aimed at managing deep-seated schemas of defectiveness, abandonment, and emotional deprivation. The Self-Aggrandizer mode served as a protective structure shielding the Vulnerable Child from experiences of shame, dependency, and emotional pain, while the Punitive Critic perpetuated internalized abuse and conditional self-worth.
From an existential perspective, Peter’s presenting complaint of emptiness reflects an existential vacuum characterized by disconnection from meaning, authentic relationships, and value-based living.12 His compulsive pursuit of success and admiration functioned as a substitute for meaning, temporarily alleviating existential anxiety while reinforcing emotional isolation.
The chairwork confrontation with the Punitive Critic illustrates a crucial point of integration between schema therapy and existential psychotherapy. Schema-therapeutically, this intervention externalized and weakened a maladaptive introject; existentially, it represented a reclaiming of freedom and agency, enabling Peter to reject an internal authority that denied his right to exist unconditionally. The emergence of sadness and emptiness following the Critic’s deactivation highlights a central existential phenomenon: the loss of defensive structure exposes the individual to previously avoided existential loneliness.
Subsequent activation of the Kind Parent and Healthy Adult modes provided not only emotional containment but also a foundation for existential reorientation. Experiential engagement with music, movement, imagination, and relational imagery supported Peter’s reconnection with vitality, pleasure, and value-based aspirations. These interventions facilitated a shift from narcissistic self-enhancement toward authentic engagement with life, characterized by creativity, relational openness, and responsibility for one’s choices.
Overall, this case demonstrates how an existentially informed schema therapy approach can transform narcissistic defenses from rigid self-protective structures into opportunities for meaning-making and identity integration, supporting a transition from externally validated worth toward internally grounded purpose and connection.
Case 3 Eugen
Eugen is a 42-year-old successful businessman who has achieved considerable financial and professional success but reports persistent feelings of emptiness and lack of fulfilment. Despite his external achievements, he has no close interpersonal relationships and spends most of his time working or engaging in superficial romantic encounters. Eugen frequently questions the meaning of his life and expresses doubts about whether he will ever experience genuine happiness, intimacy, or love.
Eugen sought psychotherapy following a panic attack that occurred during an important business meeting. He was referred to a therapist experienced in working with patients struggling with existential anxiety, loneliness, and meaninglessness. During the initial assessment, Eugen described a childhood marked by an abusive father and an emotionally neglectful mother. In response to these early experiences, he developed a strong orientation toward self-reliance, independence, and achievement, using success as a primary means of emotional regulation and self-validation. However, this coping style was accompanied by chronic fears of abandonment, mistrust of others, and oscillations between feelings of defectiveness and entitlement.
Eugen reported that he had been married previously but divorced eight years earlier. He has a 12-year-old daughter who lives with her mother, with whom he has limited contact. Although Eugen expressed guilt and sadness regarding his emotional distance from his daughter, he felt uncertain about how to re-establish a meaningful relationship and feared rejection or further failure.
Schema assessment revealed elevated scores on schemas related to Abandonment, Mistrust/Abuse, Defectiveness/Shame, Entitlement, and Emotional Deprivation. Clinically, Eugen also struggled with balancing his desire for freedom and autonomy against the inherent limitations of human existence, including dependency, emotional vulnerability, and finitude.
Together, Eugen and the therapist established a therapeutic alliance grounded in empathy, curiosity, and authenticity. Therapy focused on integrating schema-focused cognitive-behavioral techniques with existential exploration. Cognitive restructuring and experiential methods, including imagery rescripting and chairwork, were used to address maladaptive beliefs and unresolved emotional experiences from childhood. In parallel, existential dialogue explored values, life priorities, responsibility, authenticity, and transcendence. Through this work, Eugen gradually recognized that interpersonal connection and emotional engagement—rather than material success—constituted central sources of meaning for him.
Therapist:You have achieved much of what many people strive for. Yet when you speak about your life, the word that returns is emptiness. What do you think that emptiness is asking from you?
Eugen:Probably that I should stop running. I filled my life with work and achievement, but I avoided people who could really matter.
Therapist:And when you think of your daughter, what does that tell you about the kind of life you want to live?
Eugen:That I want more than success. I want to be someone who is present. Someone who does not arrive too late.
Therapist:So, the question becomes not only how to reduce anxiety, but what responsibility you want to take for the life that is still possible.
Eugen:Yes. I cannot change the years behind me, but I do not want to hide from the years ahead”.
As therapy progressed, Eugen began to translate insight into action. A particularly significant area of change involved his relationship with his daughter. By taking responsibility for past avoidance and initiating contact, Eugen experienced a growing sense of connection, fulfilment, and purpose, which contrasted markedly with the emotional emptiness associated with his earlier achievement-focused lifestyle.
Schema–Existential Clinical Analysis
From a schema therapy perspective, Eugen’s psychological difficulties can be conceptualized as the interaction of abandonment, emotional deprivation, and defectiveness schemas, managed predominantly through avoidance and overcompensation via achievement and emotional distancing. His professional success functioned as a compensatory strategy that protected him from vulnerability and relational disappointment while simultaneously reinforcing emotional isolation.
From an existential standpoint, Eugen’s presentation reflects a classic existential vacuum, characterized by a loss of meaning, superficial engagement with life, and disconnection from authentic values.12 His panic attack can be understood as a moment in which existential anxiety broke through long-standing defensive structures, confronting him with the limits of control, performance, and self-sufficiency.
The integration of schema-focused interventions with existential exploration was central to therapeutic change. Schema work enabled Eugen to recognize how early relational trauma shaped his avoidance of intimacy and mistrust of others. Existential dialogue complemented this process by addressing the broader life implications of these patterns, particularly the tension between freedom and responsibility. Rather than framing change solely as symptom reduction, therapy emphasized value-based choice and responsibility for relational engagement.
Reconnecting with his daughter represented a critical existential shift from self-protective autonomy toward meaningful commitment. This behavioral change symbolized the strengthening of the Healthy Adult mode, capable of tolerating emotional risk, accepting imperfection, and engaging in relationships aligned with personal values. Overall, this case illustrates how schema therapy enriched by an existential perspective can facilitate movement from achievement-driven self-definition toward a more authentic, relationally grounded, and meaningful way of living.
Case 4: Gin
Gin is a highly intellectual woman who has been preoccupied with profound existential questions and has been engaged in psychotherapy to explore issues of meaning, freedom, and responsibility. She reports persistent anxiety related to mortality, time limitation, and the perceived burden of choice. In therapy, Gin seeks clarity regarding how to live authentically while facing uncertainty and the inevitability of death.
In the following session, Gin openly discusses her fear of death and the overwhelming sense of responsibility associated with freedom of choice. The therapist supports her in exploring these concerns while linking existential themes to underlying schemas and coping strategies.
Therapist:Good afternoon, Gin. It’s nice to see you again. How have you been since our last session?
Gin:Hi, yeah, I have been okay, I guess. But I have been thinking a lot lately about some deeper stuff, you know? Like, what’s the purpose of everything? Why are we here? Why am I all alone? It’s been really bothering me.
Therapist:It’s natural to have those kinds of questions. Within your therapy, we also explore these existential concerns. What specifically has been bothering you about the purpose of life?
Gin:Well, I have been grappling with this fear of death. It’s like this constant presence in the back of my mind, reminding me that everything I do is temporary. It’s like I am stuck between wanting to live fully and fearing that it will all end anyway and I will die alone.
Therapist:Understandably, you are struggling with these thoughts. Many people have similar fears about death and feeling alone. It can be tough to balance our desire for the freedom of living fully with the reality of our limitations that out life will end. What do you think about that? Is there anything specific that’s been on your mind?
Gin:Yeah, that makes sense. I have been reading some existential philosophy lately, and they are talking about the same things. I have come across this idea of freedom of choice, but it’s overwhelming, too. With so many choices, how do I know I am making the right ones? The really perfect one?
Therapist:Having the freedom to choose can be exciting and overwhelming. It’s normal to feel the weight of responsibility when making decisions. In our therapy sessions, we can explore how your past experiences might influence how you approach making choices. Sometimes, our fears about making the wrong decision come from past experiences where our options were not validated or respected. For example, if you grew up with high expectations placed on you, it might be harder for you to feel confident in your decisions. For example, your schema of unrelenting standards might play an important role when searching for the right answer. Or suppose you have experienced abandonment or social isolation in the past and developed the abandonment and social isolation schema. In that case, it might make you more hesitant to make choices that could lead to being alone, especially at your death. What do you think about that? Does any of this resonate with you?
Gin:Yeah, I can see that. I have always been worried about disappointing others and afraid to be left alone, so I end up overthinking everything, always looking for a way to control and find the right answers. But what if I make the wrong choice? What if I look back and regret how I have lived my life?
Therapist:Those are valid concerns. The existential perspective encourages us to confront the reality of uncertainty and the inevitability of facing regret, as we all are fallible and make mistakes. It’s about acknowledging that regret and disappointment are part of the human experience. That we all humans are in these struggles together. We can work together to help you develop a sense of authenticity in your choices so that whatever path you take aligns with your core values and aspirations. Following your values and what is true for you is much more important than just finding the objective right answers, which no one probably knows.
Gin:I get that, but it’s still hard to shake off the fear of death. I am worried about leaving things unfinished and not having enough time for everything I want to do.
Therapist:On the one hand, it is stressful, and I can see how difficult it is for you to experience this anxiety. However, we can also look at this as an opportunity. The fear of death often drives us to reflect on what truly matters. What if we could explore the underlying schemas that might amplify this fear? By identifying and challenging those negative patterns of thinking, we can work towards finding more balance in how we perceive time and its limitations and how you can use it most meaningfully.
Gin:I appreciate that perspective. It’s just a lot to think about, you know?
Therapist:Yes, and perhaps part of the difficulty is that no perfect answer exists. What do you think it means to be a human being who must choose without certainty?
Gin:Maybe that we are always incomplete. That we act without guarantees.
Therapist:And if that is true, then perhaps making mistakes is not proof of failure, but part of being human.
Gin:I can understand that logically. Emotionally, it is harder.
Therapist:Of course. And perhaps this is also where questions of death and meaning meet: if life is finite and imperfect, what becomes important enough to live for anyway?
Gin:Relationships, probably. Being real with people. Not only thinking about life, but actually living it.
Therapist:Absolutely. These are deep and complex topics; taking your time processing them is okay. In the schema therapy process, we can continue exploring these existential questions, your fears, and your aspirations in a way that helps you build a more resilient and authentic understanding of yourself. I am grateful that you are open today to share about them.
Gin:Thank you for understanding and guiding me through this. It’s giving me a lot to reflect on.
Therapist:You are welcome. Remember, this is a journey, and I am here to support you every step of the way. Let us continue to delve into these thoughts and feelings in our upcoming sessions.
Schema–Existential Clinical Analysis
From a schema therapy perspective, Gin’s existential distress is closely linked to schemas of Unrelenting Standards, Abandonment, and Social Isolation, which manifest cognitively as perfectionistic decision-making and emotionally as chronic fear of regret and loneliness. Her tendency to intellectualize existential questions functions as a coping strategy that provides temporary control over anxiety while simultaneously preventing emotional integration and value-based action.
From an existential perspective, Gin’s fear of death and preoccupation with making the “right” choices reflect a heightened sensitivity to existential freedom and finitude. Rather than avoiding responsibility, Gin experiences freedom as overwhelming, accompanied by anticipatory guilt and fear of future regret. This pattern illustrates how existential anxiety may be amplified by schema-driven beliefs about conditional acceptance and the necessity of perfection.
Therapeutic dialogue in this case integrates schema-focused exploration with existential normalization of uncertainty and fallibility. By linking existential fears to underlying schemas, the therapist helps Gin recognize that her anxiety is not evidence of failure, but a human response intensified by maladaptive internal standards. The therapeutic task thus shifts from eliminating anxiety to fostering authentic choice-making, grounded in personal values rather than fear-driven perfectionism.
This case demonstrates how schema therapy with an existential dimension can support patients in tolerating uncertainty, relinquishing the demand for perfect decisions, and engaging more fully with life despite the awareness of mortality. Strengthening the Healthy Adult mode in this context involves cultivating acceptance of limits, responsibility for values-based choices, and compassion toward one’s own human vulnerability.
Cross-Case Synthesis
Across the four presented case reports, a consistent clinical pattern emerges: existential distress does not appear as a separate therapeutic domain but is deeply intertwined with early maladaptive schemas, schema modes, and coping strategies. Although the patients differed in diagnosis, personality organization, and symptom presentation, existential themes, such as fear of abandonment, meaninglessness, responsibility, freedom, and mortality, were recurrent and clinically salient across all cases.
From a schema-therapeutic perspective, existential suffering was consistently mediated by maladaptive schemas rooted in early relational experiences. From an existential perspective, these schemas functioned as strategies to manage core human givens, including uncertainty, loneliness, finitude, and responsibility. Therapeutic change occurred when experiential schema work was combined with explicit existential reflection, allowing patients to move from schema-driven avoidance or overcompensation toward value-based, responsible engagement with life.
Importantly, across cases, symptom reduction alone did not constitute the primary marker of progress. Instead, therapeutic effects were reflected in increased authenticity, relational engagement, tolerance of uncertainty, and the capacity to make meaningful choices—core indicators of a strengthened Healthy Adult mode within an existentially informed framework. These cross-case observations support the proposed conceptual contribution of schema therapy with an existential dimension as a clinically coherent and transdiagnostically applicable model (Table 1).
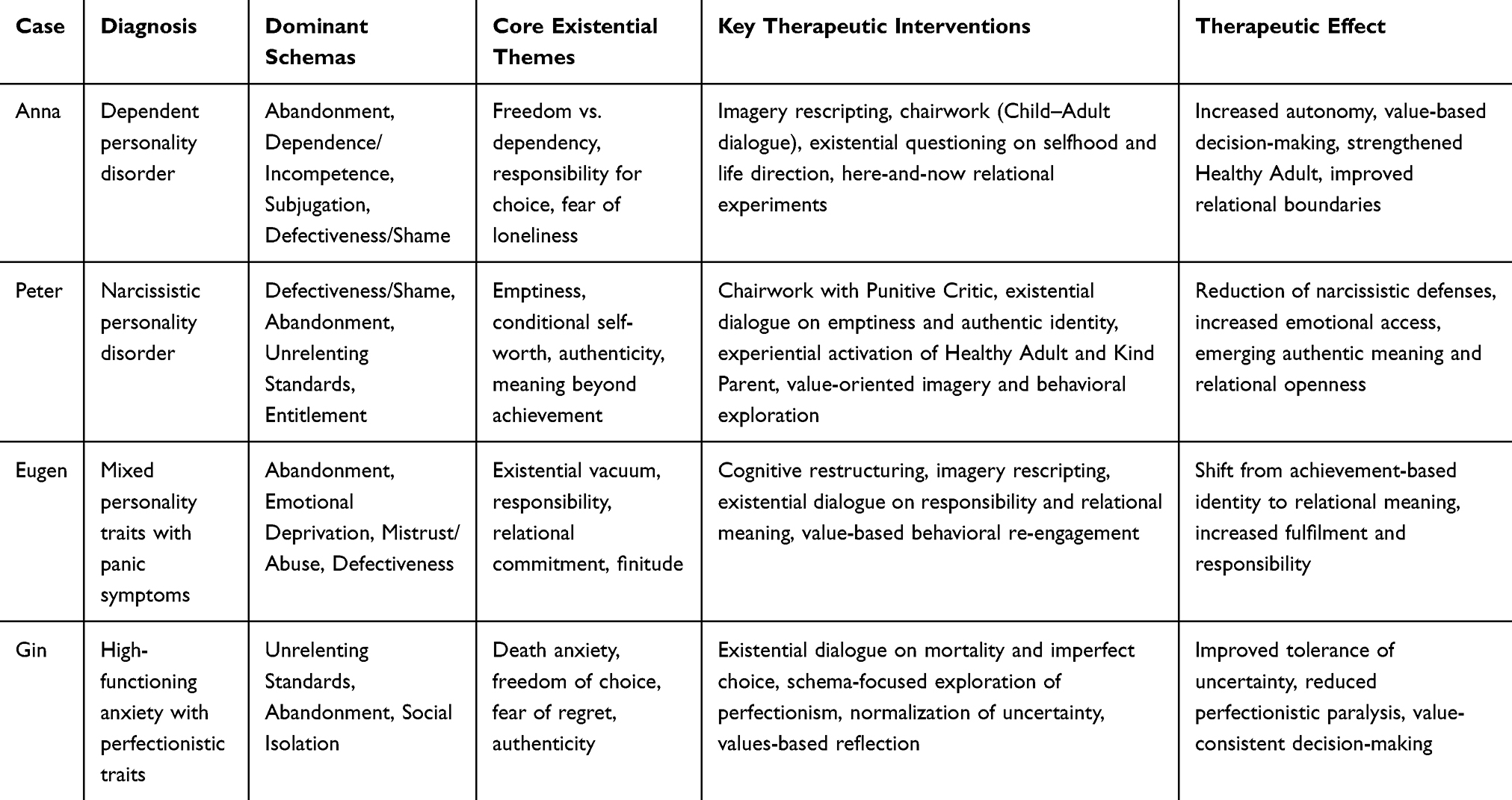 |
Table 1 Cross-Case Summary of Schema-Existential Integration |
Together, these cases demonstrate that integrating existential themes into schema therapy enhances both conceptual depth and clinical effectiveness, particularly in patients whose suffering extends beyond symptomatology to questions of identity, meaning, and existence.
Discussion
The present paper aimed to address a conceptual gap in schema therapy by systematically integrating existential psychotherapy perspectives into its theoretical and clinical framework. Drawing on a narrative synthesis of the literature and illustrative case reports, we proposed an existentially informed schema therapy model that conceptualizes existential concerns as dynamically interacting with early maladaptive schemas, schema modes, and coping strategies across the lifespan.
Importantly, across cases, therapeutic progress was not best understood solely in terms of symptom change, but also in terms of need fulfilment, identity coherence, authenticity, relational engagement, and the capacity to make meaningful choices. Across all four cases, existential distress emerged not as a separate or secondary phenomenon, but as a central organizing dimension of patients’ suffering. Themes such as meaninglessness, fear of abandonment, responsibility for choice, freedom, and mortality were consistently intertwined with schema-driven patterns of avoidance, surrender, or overcompensation. These findings support the view that existential concerns can be meaningfully conceptualized within schema therapy as expressions of unmet existential needs that amplify and maintain maladaptive schemas and dysfunctional modes, rather than as issues to be addressed only after symptomatic improvement.
An important contribution of the proposed model lies in reconceptualizing schemas and schema modes as existential coping structures. From this perspective, maladaptive schemas do not merely reflect distorted beliefs rooted in early experiences, but also represent attempts to manage fundamental existential givens such as uncertainty, isolation, and finitude. For example, dependency and abandonment schemas functioned as defences against existential loneliness and responsibility (Case 1), narcissistic overcompensation protected against existential emptiness and shame (Case 2), achievement-oriented avoidance served to bypass vulnerability and relational loss (Case 3), and unrelenting standards mitigated anxiety related to freedom and mortality (Case 4). This reframing extends existing schema theory by embedding developmental psychopathology within a broader existential context.
Clinically, the integration of existential perspectives did not require the introduction of fundamentally new techniques, but rather a shift in therapeutic focus and timing. Standard schema therapy interventions, such as imagery rescripting, chairwork, limited reparenting, and behavioral experiments, were augmented by explicit existential reflection on values, responsibility, authenticity, and life direction. Importantly, therapists refrained from providing solutions to existential dilemmas, instead emphasizing patients’ freedom to choose and their responsibility for shaping meaningful lives. This stance appeared particularly important in strengthening the Healthy Adult mode as an agent of value-based decision-making rather than merely an internal regulator of affect and behavior.
The cross-case synthesis suggests that existential concerns systematically interact with early maladaptive schemas and schema modes across diagnostic categories, highlighting the need for future empirical studies examining whether explicitly integrating existential interventions into schema therapy enhances long-term outcomes, identity coherence, and meaning-making beyond symptom reduction.
The cross-case synthesis further suggests that therapeutic change was reflected in patients’ increased tolerance of uncertainty, willingness to engage in relationships despite vulnerability, capacity to make autonomous choices, and emerging sense of meaning and coherence. These outcomes are consistent with both schema therapy’s emphasis on Healthy Adult functioning and existential psychotherapy’s emphasis on authenticity, responsibility, and engagement with life.28–31 Schema therapy with an existential dimension may therefore be particularly suited for patients who report persistent emptiness, identity diffusion, or existential anxiety despite measurable improvement on symptom-based outcomes. In line with recent efforts to emphasize positive constructs within schema therapy, the Healthy Adult may be understood not only as a regulatory mode, but also as a multidimensional adaptive structure capable of meaning-making, responsibility-taking, authenticity, and life engagement.32,33
An important factor influencing the applicability of existentially informed schema therapy is the therapist’s capacity to engage authentically with existential themes. Existential dialogue requires tolerance of uncertainty, emotional presence, and the ability to work without prematurely structuring or resolving the patient’s experience. In the presented cases, interventions were delivered by experienced clinicians trained in both schema therapy and existential approaches, which may have contributed to the effectiveness of the integration. Future studies should examine the extent to which therapist experience, personal stance, and training moderate treatment outcomes, as well as how this approach can be adapted for therapists with varying levels of expertise. Additionally, the cases may reflect a socio-cultural context in which patients have sufficient psychological and social resources to engage in value-based reflection, which may influence generalizability to more disadvantaged populations.
Several limitations should be acknowledged. First, the clinical material is based on de-identified composite case reports derived from clinical experience rather than systematically collected empirical data. While this approach is appropriate for theory development and illustration, it limits generalizability. Second, the integration model has not yet been empirically tested against standard schema therapy, and its incremental effectiveness remains an open question. Third, existential themes may vary in salience across cultural contexts, diagnostic groups, and stages of therapy, requiring further conceptual refinement and empirical investigation.
These convergent case patterns indicate that existentially informed schema therapy constitutes a testable clinical model, warranting future controlled studies to examine its mechanisms of change, differential indications, and additive effects over standard schema therapy.
Future research should examine whether existentially informed schema interventions enhance long-term identity integration and meaning in life beyond symptomatic improvement, and whether these effects are mediated by changes in Healthy Adult functioning. Future research should therefore focus on empirically evaluating existentially informed schema therapy using mixed-methods designs. Randomized controlled trials could examine whether explicit integration of existential interventions enhances long-term outcomes, particularly regarding meaning in life, identity coherence, and relapse prevention. Process research may help clarify mechanisms of change, such as whether strengthening the Healthy Adult mode mediates improvements in existential functioning. Additionally, qualitative studies could explore patients´ lived experiences of integrating existential reflection into schema-focused work.
In conclusion, schema therapy with an existential dimension represents a coherent and clinically applicable conceptual contribution that extends schema therapy beyond symptom-focused change toward facilitating authentic, meaningful, and responsible engagement with life. By systematically linking existential needs with schemas, schema modes, and therapeutic processes, this model offers a theoretically grounded framework for addressing forms of suffering that lie at the intersection of psychopathology and the human condition.
A potential criticism of the proposed model is that existential concerns may be considered overly abstract or culturally dependent. However, the present framework does not introduce existential themes as philosophical abstractions, but operationalizes them through schema modes, experiential techniques, and behavioral choices, thereby anchoring existential reflection in observable clinical processes. Future research should focus on operationalizing this framework into structured treatment protocols and evaluating its efficacy across different patient populations, including those with varying levels of functioning and clinical severity.
Conclusion
This article demonstrates that schema therapy can be meaningfully enriched by an explicit existential dimension without compromising its theoretical coherence or clinical structure. Schema therapy and existential psychotherapy share several foundational principles, including a phenomenological orientation, a strong emphasis on the therapeutic relationship, attention to subjective meaning, and a focus on personal growth and self-realization.9,28–31, By integrating existential perspectives, schema therapy may more comprehensively address forms of suffering that extend beyond symptomatology to questions of meaning, identity, responsibility, and authenticity.19,24
Existentially informed interventions—such as confronting existential themes, fostering authenticity, and working with existential anxiety, appear particularly relevant for patients whose early maladaptive schemas are intertwined with chronic emptiness, identity diffusion, or persistent dissatisfaction despite standard cognitive-behavioral interventions.24 From this perspective, existential integration supports not only schema change but also the strengthening of the Healthy Adult mode as an agent capable of reflective choice, responsibility, and value-based living.14,15
The proposed model has several implications for both theory and clinical practice. Conceptually, it extends schema theory by situating early maladaptive schemas and schema modes within a broader existential framework, viewing them as adaptive attempts to manage fundamental human givens such as uncertainty, isolation, and finitude. Clinically, it offers a structured yet flexible approach for addressing existential concerns within an established therapeutic model, potentially increasing relevance and depth for patients who struggle with meaning-related distress.
Several limitations must be acknowledged. First, the present contribution is primarily conceptual and illustrative, supported by clinical case material rather than systematic empirical evaluation. Second, the integration presented here focuses on selected existential strategies most compatible with schema therapy, and other existential approaches may offer additional insights. Consequently, further theoretical refinement and empirical research are warranted.
Future studies should examine the effectiveness and mechanisms of existentially informed schema therapy, particularly regarding long-term outcomes, identity coherence, and meaning in life. As emerging schemas, such as unfairness, lack of self-cohesiveness, or perceptions of an incomprehensible world, gain prominence within contemporary schema theory, their conceptual alignment with existential needs such as authenticity and coherence deserves systematic investigation.10
In conclusion, schema therapy with an existential dimension represents a promising and clinically meaningful extension of schema therapy. By integrating developmental, experiential, and existential perspectives, this approach offers a pathway for addressing not only how patients suffer, but also how they may consciously and responsibly shape meaningful lives.
Disclosure
The authors declare that they have no conflicts of interest related to this work. Artificial intelligence tools were used solely to support language editing and clarity; all theoretical concepts, clinical interpretations, and conclusions are the original work of the authors.
References
1. Frankl VE. Man’s Search for Meaning: An Introduction to Logotherapy (Lasch I,). Beacon Press books. Boston, (Original work published 1946); 1962.
2. May R. Psychology and the Human Dilemma. Princeton, NJ: Van Nostrand; 1967.
3. Binswanger L. Grundformen und Erkenntnis menschlichen Daseins. Niehans; 1942.
4. Cooper M. Existential Therapies. Sage; 2003.
5. Spinelli E. Practicing Existential Therapy: The Relational World.
6. Yalom ID. Existential Psychotherapy. New York: Basic Books; 1980.
7. Van Deurzen E. Everyday Mysteries. A Handbook of Existential Psychotherapy.
8. Stein DJ. Problems of Living: Perspectives From Philosophy, Psychiatry, and Cognitive-Affective Science. Academic Press; 2021.
9. Young JE, Klosko JS, Weishaar ME. Schema Therapy: A Practitioner’s Guide. New York: Guilford Press; 2003.
10. Arntz A, Rijkeboer M, Chan E, et al. Towards a reformulated theory underlying schema therapy: position paper of an international workgroup. Cogn Ther Res. 2021; 1–24. doi:10.1007/s10608-021-10209-5.
11. Fava GA, Rafanelli C, Grandi S, Conti S, Belluardo P. Prevention of recurrent depression with cognitive behavioral therapy: preliminary findings. Arch Gen Psych. 1998;55(9):816–820. doi:10.1001/archpsyc.55.9.816
12. Frankl VE. From Death-Camp to Existentialism: A Man’s Search for Meaning. Beacon Press; 1961.
13. Van Genderen H, Jacob G, Seebauer L. Breaking Negative Thinking Patterns: A Schema Therapy Self-Help and Support Book. Hoboken: John Wiley & Sons; 2019.
14. Farrell JM, Reiss N, Shaw IA. The Schema Therapy Clinician’s Guide: A Complete Resource for Building and Delivering Individual, Group and Integrated Schema Mode Treatment Programs. Wiley Blackwell; 2014.
15. Roediger E, Zarbock G. Schematherapie bei Persönlichkeitsstörungen. Eine Standortbestimmung [Schema therapy for personality disorders. A critical review]. Nervenarzt. 2015;86(1):60–71. [PMID: 24676551]. doi:10.1007/s00115-014-4008-8
16. Louis J, Lockwood G, Louis K. A model of core emotional needs and toxic experiences: their links with schema domains, well-being, and ill-being. Behav Sci. 2024;14(6):443. doi:10.3390/bs14060443
17. Edwards DJA. Using schema modes for case conceptualization in schema therapy: an applied clinical approach. Front Psychol. 2022;12:763670. PMID: 35126233; PMCID: PMC8813040. doi:10.3389/fpsyg.2021.763670
18. Prasko J, Dicevicius D, Ociskova M, et al. Imagery in cognitive behavioral supervision. Neuro Endocrinol Lett. 2020;41(1):33–45. PMID: 32338851.
19. Roediger E, Stevens BA, Brockman R. Contextual Schema Therapy: An Integrative Approach to Personality Disorders, Emotional Dysregulation, and Interpersonal Functioning. Oakland: New Harbinger Publications; 2016.
20. Brockman RN, Simpson S, Hayes C, van der Wijngaart R, Smout M. Cambridge Guide to Schema Therapy. Cambridge University Press; 2023.
21. Beck AT. The past and future of cognitive therapy. J Psychother Pract Res. 1997;6(4):276–284. PMID: 9292441 PMCID: PMC3330473.
22. Längle A. Personale Existenzanalyse. In: Längle A, editor. Wertbegegnung. Phänomene und methodische Zugänge. Wien: GLE-Verlag; 1989:133–159.
23. Young J. Cognitive Therapy for Personality Disorders: A Schema-Focused Approach. Sarasota FL: Professional Resource Exchange; 1994.
24. Worrell M. CBT and Existential Psychology: Philosophy, Psychology and Therapy. John Wiley & Sons; 2022.
25. Bygstad-Landro M, Giske T. Risking existence: the experience and handling of depression. J Clin Nurs. 2018;27(3–4):e514–e522. doi:10.1111/jocn.14056
26. Frankl VE. Suffering from the Meaninglessness of Life [Utrpení z nesmyslnosti života. In: Czech. Praha: Portál; 2016.
27. Hayes SC, Feldman G. Clarifying the construct of mindfulness in the context of emotion regulation and the process of change in therapy. Clin Psychol Sci Pract. 2004;11(3):255–262. doi:10.1093/clipsy.bph080
28. Bakewell S. At the Existentialist Café. Freedom, Being and Apricot Cocktails. Chatto & Windus; 2016.
29. Leahy RL. A model of emotional schemas. Cogn Behav Pract. 2002;9(3):177–190. doi:10.1016/S1077-7229(02)80048-7
30. Hayes SC. Acceptance and commitment therapy, relational frame theory, and the third wave of behavioral and cognitive therapies. Behav Ther. 2004;35(4):639–665. doi:10.1016/j.beth.2016.11.006
31. Yalom ID, Josselson R. Existential psychotherapy. In: Wedding D, Corsini RJ, editors. Current Psychotherap.
32. Louis JP. Clinical psychology: Development of measures for schema therapy. [doctoral dissertation]. University of Stirling; 2018. Available from: http://hdl.handle.net/1893/27350.
33. van Donzel L, Claassen AM, Ouwens MA, et al. Positive constructs in schema therapy: a scoping review. J Clin Psychol. 2026. PMID: 41734134. doi:10.1002/jclp.70111.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.