Back to Journals » International Journal of Women's Health » Volume 17
Integrating Chinese Herbal Medicine in IVF: A Protocol for Randomized Controlled Trial of Gushen Antai Pill
Authors Xu Y, Hu X, Ai KL, Sun ZG ![]() , Song JY
, Song JY ![]()
Received 19 July 2025
Accepted for publication 19 November 2025
Published 25 November 2025 Volume 2025:17 Pages 4855—4866
DOI https://doi.org/10.2147/IJWH.S554939
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Matteo Frigerio
Ying Xu,1,2 Xin Hu,1 Kai-Liang Ai,1 Zhen-Gao Sun,2 Jing-Yan Song1
1The First Clinical College, Shandong University of Traditional Chinese Medicine, Jinan, People’s Republic of China; 2Reproductive Center of Integrated Medicine, The Affiliated Hospital of Shandong University of Traditional Chinese Medicine, Jinan, People’s Republic of China
Correspondence: Jing-Yan Song; The First Clinical College, Shandong University of Traditional Chinese Medicine, No. 42, Wen Hua Xi Road, Lixia District, Jinan, 250011, People’s Republic of China, Tel +86-0531-68901236, Email [email protected] Zhen-Gao Sun, Reproductive Center of Integrated Medicine, The Affiliated Hospital of Shandong University of Traditional Chinese Medicine, No. 42, Wen Hua Xi Road, Lixia District, Jinan, 250011, People’s Republic of China, Tel +86-0531-68901236, Email [email protected]
Introduction: Effective ovarian stimulation and luteal phase support (LPS) are key factors for the success of in vitro fertilization and embryo transfer (IVF-ET) The present multicenter randomized trial evaluates whether adding Gushen Antai Pill (GSATP) to standard LPS improves the ongoing pregnancy rate (OPR) in women with normal ovarian reserve (NOR) undergoing fresh embryo transfer.
Methods: This study is a multicenter, randomized, double-blind, placebo-controlled trial, taking place at 20 reproductive centers within public tertiary hospitals. We plan to enroll around 800 women who are expected to have a NOR. Participants are randomized 1:1 using a stratified block randomization method with block sizes of 4 and 6, stratified by age (< 35 vs ≥ 35 years). The primary endpoint is the OPR, with comprehensive safety evaluations also being performed. Data analysis will adhere to both intention-to-treat (ITT) and per-protocol (PP) principles to ensure robust statistical validity.
Discussion: This randomized controlled trial (RCT) aims to evaluate the effectiveness and safety of combining LPS with GSATP to improve pregnancy outcomes in women with NOR who are undergoing fresh embryo transfer. By rigorously evaluating endpoints such as OPR and early pregnancy complications, this study seeks to establish evidence for GSATP as a potential adjuvant therapy in IVF-ET protocols. The findings may offer innovative therapeutic perspectives for integrating traditional Chinese medicine (TCM) into contemporary assisted reproductive technology, particularly in enhancing implantation conditions and reducing miscarriage risks during fresh cycles.
Trial Registration: ClinicalTrials.gov, ID: NCT04872660, 05/04/2021.
Keywords: Traditional Chinese Medicine, Gushen Antai Pill, threatened miscarriage, IVF-ET, ongoing pregnancy rate
Introduction
Infertility is an increasingly common reproductive health problem, affecting approximately 15% of couples in reproductive age.1 As reproductive medicine continues to advance, more and more individuals struggling with infertility are turning to Assisted Reproductive Technology (ART) to achieve a successful live birth. In China, the infertility rate among couples of childbearing age trying to conceive is notably high, reaching 25%.2 Although IVF-ET have successfully overcome issues with sperm-egg interaction and fertilization, challenges with implantation conditions and endometrial receptivity continue to limit pregnancy success, highlighting the need for further improvements. Central to successful IVF-ET is the careful optimization of ovarian stimulation protocols and LPS. Existing evidence indicates that nearly all patients undergoing controlled ovarian stimulation experience luteal insufficiency,3–5 highlighting the critical need for effective LPS strategies. In IVF-ET cycles, natural progesterone is commonly chosen for LPS. However, there is still ongoing debate about the best way to administer progesterone, including the route, dosage, and duration, as well as whether additional medications are needed. There is currently no consensus on corpus luteal support programs in clinical practice, and different corpus luteal support programs may cause different pregnancy outcomes. Recent clinical studies have shown that combining progesterone-based LPS with estrogen or human chorionic gonadotropin (hCG) does not significantly improve live birth rates or the OPR.6 In contrast, using hCG together with LPS has been linked to a higher risk of ovarian hyperstimulation syndrome (OHSS).6 In our previous RCT, we found that adding GSATP to artificial cycle endometrial preparation in the FET cycle significantly improved the ongoing pregnancy rate (56.62% vs. 44.44%, p=0.045) and reduced the risk of threatened miscarriage in early pregnancy (10% vs 23.08%, p=0.032), especially in patients aged 35 or younger.7 A prospective study by Lu Yue et al showed that the OPR with LPS combined with GSATP was significantly higher compared to conventional LPS alone (63.83% vs. 42.86%, p=0.039).8
Chinese women with threatened miscarriage (TM) are widely treated with GSATP as an adjunctive therapy, and the results are still satisfactory.9 Wei et al observed 87 patients with recurrent miscarriage with kidney deficiency and liver depression type corpus luteal insufficiency and found that the use of progesterone capsules combined with GSATPs can improve pregnancy rate and reduce miscarriage rate.10 After genetic analysis of the abortion tissues of 13 of the abortion patients, it was found that the combination of medication can also reduce the abnormal rate of embryonic chromosomes.10 In TCM, the kidney is widely recognized as the foundation of the innate body, playing a pivotal role in growth, development, and the storage of essence (“Jing”). It is believed to promote the maturation of reproductive organs, maintain reproductive functions, and is intricately linked to male sperm production and female ovulation. Regarding TM, TCM theory emphasizes its close association with the liver, kidney, and spleen. The primary pathological mechanisms are attributed to kidney deficiency, spleen qi deficiency, and liver qi stagnation, which disturb the balance of qi and blood and ultimately affect reproductive health.11,12 For decades, GSATP has been used clinically to treat TM, based on the principles of tonifying the kidneys, stimulating the spleen, and regulating the liver.13 GSATP comprises ten different types of Chinese herbal medicine (Uncaria, Herba Taxilli, Cistanche Deserticola, Polygonum Multiflori, Rehmannia Glutinosa, Cuscutae Semen, Atractylodes, Scutellariae, Paeoniae, and Dipsaci), each of which has its own therapeutic properties.13 Dipsaci, Cuscutae Semen, and Herba Taxilli are considered the monarch drugs, as they contain ingredients that help tonify the kidney, replenish essence, nourish blood, and consolidate Chong vessels.12 Accordingly, Rehmannia Glutinosa, Cistanche Deserticola, and Polygonum Multiflori were included to strengthen the effects of kidney support, liver and spleen invigoration, and blood nourishment.13,14 Furthermore, Atractylodes, Uncaria, and Scutellariae help to invigorate Qi, clear heat, regulate Qi, calm the liver, and detoxify the body.15,16 Briefly, all the herbal ingredients work together to create a balanced, calming effect on the fetus, helping to prevent miscarriage.
Based on existing statistical data, the clinical pregnancy rate for fresh embryo transfer cycles in women with normal ovarian reserve is approximately 40% to 60%17,18, the OPR is about 30% to 50%,19 and the live birth rate is usually 30% to 38%.18,20 Pregnancy outcomes vary significantly due to factors such as age. In fresh IVF cycles, a prior study suggested that combining LPS with GSATP might enhance embryo implantation, clinical pregnancy, and OPR while reducing early miscarriage risks.8 However, the research’s methodological limitations hindered definitive conclusions about GSATP’s efficacy. Critical shortcomings included an unclear randomization process, lack of allocation concealment and blinding, absence of a placebo control group, and ambiguous inclusion/exclusion criteria. These flaws underscore the need for a rigorously designed randomized controlled trial (RCT) to systematically evaluate GSATP’s safety and efficacy in optimizing reproductive outcomes for women with NOR undergoing fresh IVF cycles. In summary, whether GSATP can improve pregnancy outcomes during fresh IVF cycles remains unclear. Because luteal physiology and endocrine dynamics differ between frozen-thawed and fresh embryo transfer cycles, existing evidence cannot be directly extrapolated. Therefore, this study aims to determine whether GSATP can improve the ongoing pregnancy rate in fresh IVF cycles through the implementation of standardized protocols and robust statistical methods. An interim analysis planned in the protocol has already been performed and its results were published separately (Xu et al, Contraception and Reproductive Medicine).21 This manuscript describes the trial protocol and prespecified methods. Results from the interim analysis are cited for context only and are not repeated here.
Methods and Analysis
This protocol was developed in accordance with the SPIRIT 2013 guidance for clinical trial protocols. A completed SPIRIT checklist is provided as Supplementary File S1 This RCT has been registered in the clinical trials database of the National Institutes of Health (NIH). Consequently, the study methodology described below will draw partially from the website (https://clinicaltrials.gov/study/NCT04872660).22
Study Design
The study is a prospective, multicenter, randomized, double-blind, placebo-controlled trial carried out at 20 reproductive centers in public tertiary hospitals. The 20 centers include: Shandong University of Traditional Chinese Medicine Affiliated Hospital; The First Affiliated Hospital of Wenzhou Medical University; Shanxi Provincial Children’s Hospital (Shanxi Maternal and Child Health Hospital); Zaozhuang Maternal and Child Health Hospital; Dezhou Hospital of Qilu Hospital of Shandong University; Liaocheng People’s Hospital; Weifang People’s Hospital; The Affiliated Reproductive Hospital of Shandong University; The 960th Hospital of the Joint Logistics Support Force of the Chinese People’s Liberation Army; Zibo Maternal and Child Health Hospital; Affiliated Hospital of Weifang Medical University; Yantai Yantaishan Hospital; Tai’an Central Hospital; Shandong Maternal and Child Health Hospital; The Second Affiliated Hospital of Shandong University of Traditional Chinese Medicine; Linyi People’s Hospital; Jinan Maternal and Child Health Hospital; Heze Hospital of Traditional Chinese Medicine; Yantai Yuhuangding Hospital and Qingdao Women and Children’s Hospital. A total of 800 eligible participants will be recruited. In June 15 2021, the clinical study began and is expected to end on 30 2026. The study flowchart is presented in Figure 1, while the study timeline is detailed in Table 1.
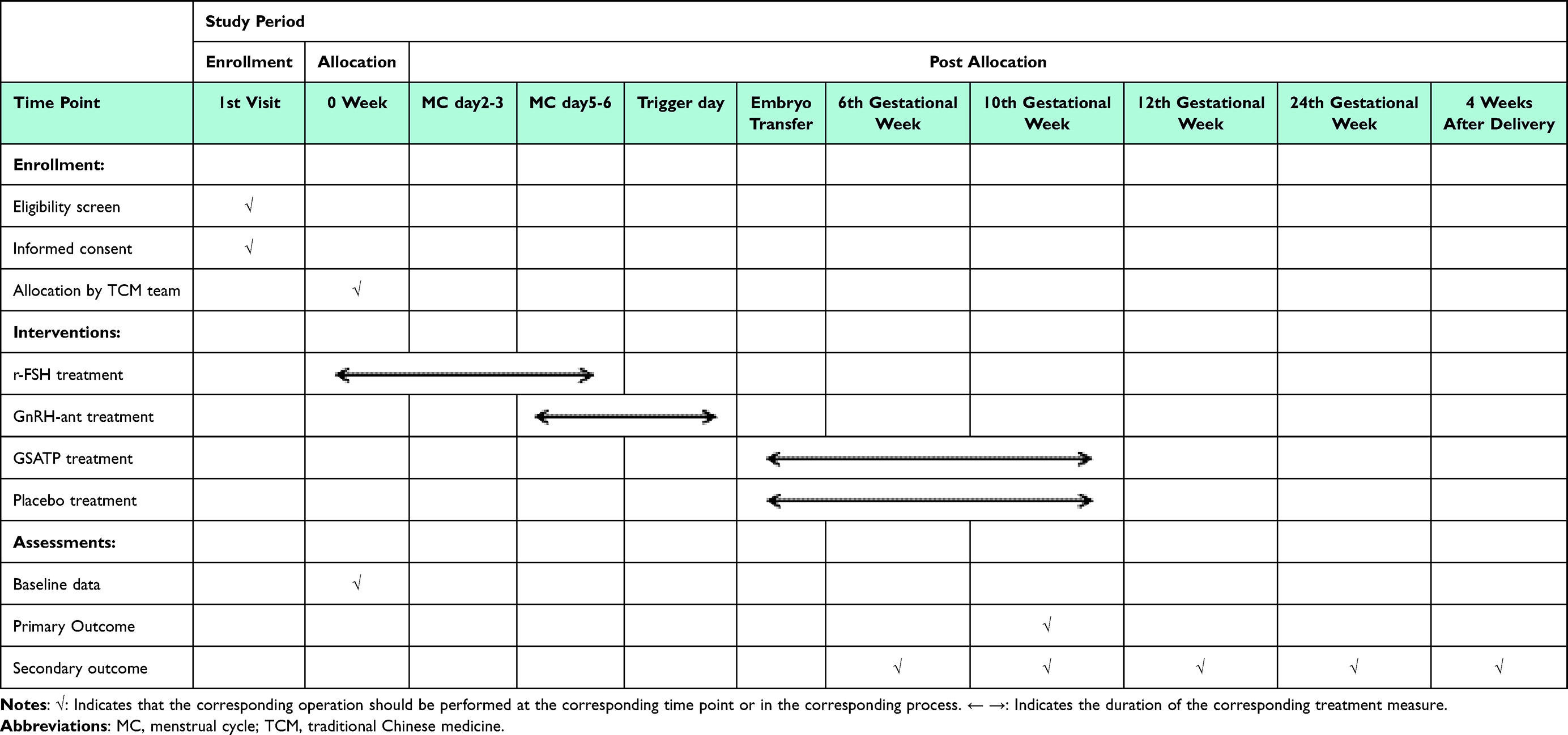 |
Table 1 Schedule of the Study Process (SPIRIT Figure) |
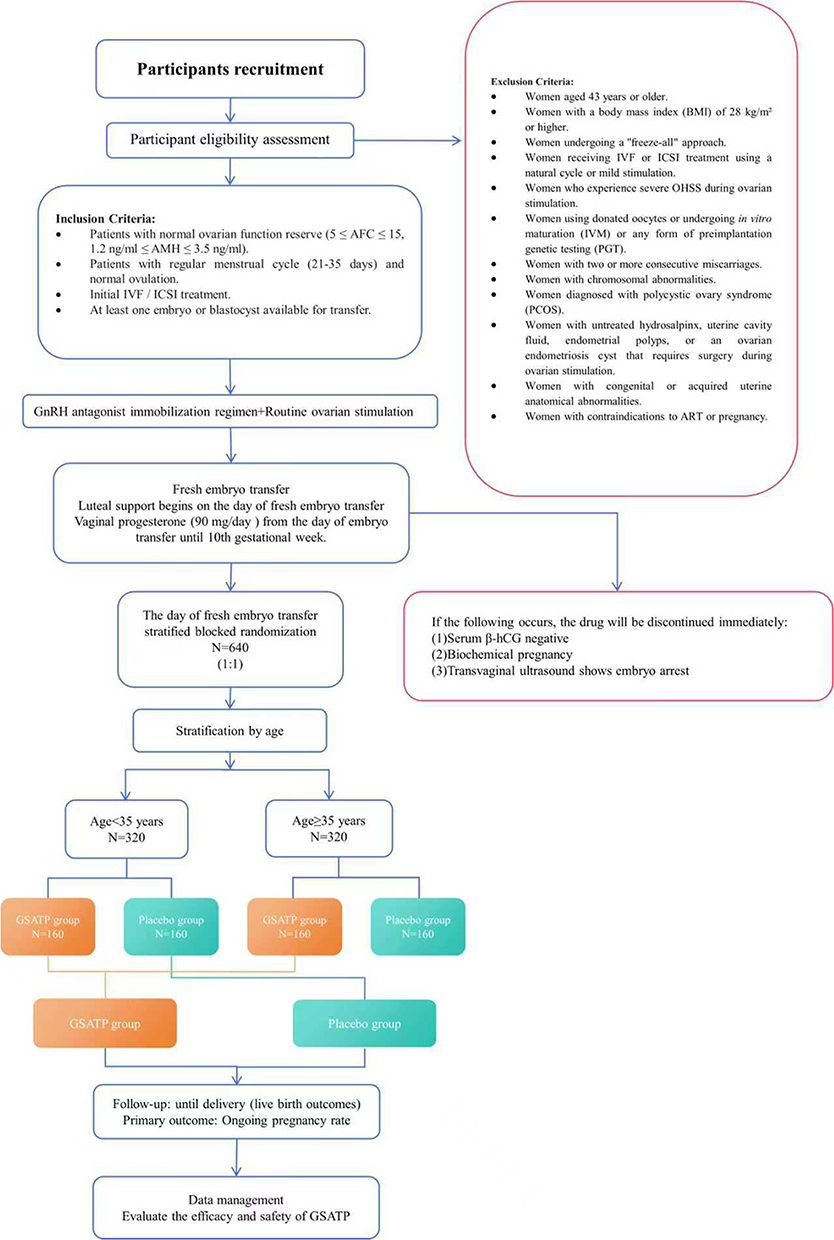 |
Figure 1 Flow diagram of participant recruitment. |
Recruitment and Consent
The enrollment process starts with ovarian stimulation and continues through to the day of embryo transfer (ET). During this period, each patient’s medical history will undergo thorough review, complemented by transvaginal ultrasound assessments and biochemical analyses to evaluate eligibility. Once potential participants meet the predefined inclusion and exclusion criteria, our research team will proactively contact them to explain the study objectives and extend an invitation to participate. Recruitment will adhere strictly to the established criteria to ensure a homogeneous study population. Eligible participants will be guided to complete a detailed case report form (CRF), documenting comprehensive baseline characteristics, including demographic data, medical history, and reproductive parameters. Prior to formal enrollment, a physician from the Reproductive Center will provide a detailed explanation of the study protocol, addressing any questions or concerns to ensure full comprehension. Each participant will provide written informed consent, confirming their voluntary involvement and understanding of the potential risks and benefits of the study. This structured approach aims to maintain scientific rigor while prioritizing participant autonomy and safety throughout the recruitment phase.
Eligibility Criteria
Inclusion Criteria
- Women with NOR defined by an AFC between 5 and 15 and AMH levels between 1.2 ng/mL and 3.5 ng/mL.23,24
- Women with a regular menstrual cycle (21–35 days) and normal ovulation. Regular menstrual cycle is defined as cycle length 21–35 days, which aligns with commonly used clinical definitions in reproductive medicine and reflects ovulatory cycles in reproductive-age women. Normal ovulation is documented by at least one of the following within the preceding 6 months: (1) mid-luteal serum progesterone ≥ 3 ng/mL in a spontaneous cycle, (2) biphasic basal body temperature chart consistent with ovulation, or (3) ultrasound evidence of ovulation (dominant follicle rupture). At screening, clinicians will document the patient’s menstrual history and available ovulation data; if ovulatory status is uncertain, a single mid-luteal progesterone measurement will be obtained.
- Women undergoing their first IVF or ICSI treatment.
- Women with at least one viable day-3 embryo or blastocyst for transfer.
- This study did not include participants based on traditional Chinese medicine syndrome differentiation. GSATP, although historically used for the kidney-deficiency (kidney Yin deficiency) type of threatened miscarriage, was evaluated here as an adjuvant therapy within a modern biomedical framework for women with normal ovarian reserve undergoing IVF.
Exclusion Criteria
- Women aged 43 years or older.
- Women with a body mass index (BMI) of 28 kg/m² or higher.
- Women undergoing a “freeze-all” approach.
- Women receiving IVF or ICSI treatment using a natural cycle or mild stimulation.
- Women who experience severe OHSS during ovarian stimulation.
- Women using donated oocytes or undergoing in vitro maturation (IVM) or any form of preimplantation genetic testing (PGT), including but not limited to PGT for aneuploidy (PGT-A), monogenic disorders (PGT-M), or structural rearrangements (PGT-SR), as well as preimplantation genetic diagnosis (PGD) or screening (PGS).
- Women with two or more consecutive miscarriages.
- Women with chromosomal abnormalities.
- Women diagnosed with polycystic ovary syndrome (PCOS).
- Women with untreated hydrosalpinx, uterine cavity fluid, endometrial polyps, or an ovarian endometriosis cyst that requires surgery during ovarian stimulation.
- Women with congenital or acquired uterine anatomical abnormalities.
- Women with contraindications to ART or pregnancy.
Dropout and Discontinuation Criteria
- Women who do not follow the prescribed medication schedule or dosage, or who stop taking the medication without consultation.
- Women taking other medications that may interfere with study outcomes during the treatment.
- Women who experience adverse drug reactions that prevent them from continuing the treatment, including clinically significant reactions related to GSATP or progesterone products used concurrently.
- Women with insufficient follicle growth, premature ovulation (defined as ovulation occurring earlier than expected based on the individual’s follicular development and hormone monitoring, rather than menstrual cycle length), failure to retrieve a follicle, or cycle cancellation for individual reasons.
Randomization, Allocation, and Blinding
Previous studies showed that the OPR was significantly higher in the GSATP group for women under 35, while vaginal bleeding rates were notably lower in women 35 and older compared to the placebo group. Given the limitations of post-hoc analysis, we will use Stratified Block Randomization, grouping participants by age (< 35 years vs ≥ 35 years), after voluntary enrollment in the study. For each age group, 400 participants will be enrolled, with 200 in the GSATP and 200 in the placebo group. Randomization is performed using R software (version 3.5.1) with stratified block randomization, applying randomly varying block sizes of 4 and 6 and a 1:1 allocation ratio between the two groups. The allocation sequence is held by a designated nurse not involved in outcome assessment. On the day of embryo transfer, the nurse opens the corresponding sequentially numbered opaque envelope and dispenses the assigned study medication to the patient. Participants themselves do not handle the randomization envelopes, ensuring full allocation concealment and blinding.
GSATP and placebo tablets will be individually coded to ensure a strict one-to-one correspondence with each patient’s unique identifier, with all grouping details securely managed by the dedicated drug management center. Both interventions are meticulously formulated to be indistinguishable in appearance, taste, and packaging, minimizing any potential bias from sensory cues. A comprehensive blinding protocol will be implemented, ensuring that clinicians, outcome evaluators, statisticians, and participants remain unaware of the treatment assignments throughout the trial. This strict blinding mechanism extends to all stages of care, including medication administration and data collection. Upon completion of the clinical trial, the final unblinding process will be conducted by authorized researchers in a controlled manner, ensuring the integrity of the study’s statistical analysis and interpretation.
Interventions
Drug Preparation and Administration
The herbal formula GSATP (Z20030144) consists of ten botanical components, including Polygonum multiflorum root, prepared Rehmannia glutinosa root, Cistanche deserticola, Dipsacus asperoides root, Uncaria rhynchophylla, Cuscuta chinensis seed, Atractylodes macrocephala rhizome, Scutellaria baicalensis root, and Paeonia lactiflora root. GSATP is used to treat early threatened miscarriage, associated with kidney yin deficiency syndrome in TCM. This product is manufactured in full compliance with Good Manufacturing Practice (GMP) standards. It is formulated as water-based honey pills, with each sachet containing 6 grams.
Placebo Preparation and Administration
The placebo is identical in appearance and taste to GSATP. Manufactured by Beijing Boran Pharmaceutical Inc., it is made from soybean powder, starch, carbon melanin, and refined honey. While it mimics the color, smell, and texture of GSATP, it contains no active ingredients and thus has no clinical effect. The placebo is packaged in the same manner as GSATP to prevent participants from identifying their group assignment, which could influence compliance, and to avoid the potential confounding effect of using vitamins as a placebo.
COS and Oocytes Retrieval
Ovarian stimulation starts on day 2 or 3 of the menstrual cycle, with all patients receiving recombinant follicle-stimulating hormone (r-FSH, Gonal-F, Merck Serono, Switzerland). The initial dose of r-FSH will be decided by the doctor, based on factors such as the patient’s age, AFC, basal FSH, estradiol (E2) levels, and BMI, typically ranging from 150 to 225 IU/day. The FSH dose will be adjusted every 2–3 days based on ovarian response, estradiol levels, and follicle development monitored via transvaginal ultrasound. From day 5 or 6 of ovarian stimulation until the trigger day, all patients will receive gonadotropin-releasing hormone antagonist (GnRH-ant, cetrorelix acetate, Cetrotide; Merck Serono, Germany). When more than two follicles reach a size of at least 18mm, a 250 μg dose of recombinant human chorionic gonadotropin (r-hCG, Ovidrel, Merck Serono, Italy) will be given to trigger final follicular maturation. Oocyte retrieval will be performed 35–37 hours later under transvaginal ultrasound guidance, followed by standard IVF/ICSI procedures as previously described.10 To minimize inter-center variability, all participating sites followed a unified ovarian stimulation protocol and trigger criteria developed by the coordinating center. Each center’s investigators and embryologists underwent standardized training before patient recruitment, ensuring consistent implementation of clinical and laboratory procedures.
Embryo Transfer and Luteal Phase Support
In all cases, embryos at the cleavage stage were transferred on day 3 after oocyte retrieval, or blastocysts on day 5, unless any of the following conditions applied: serum E2 > 5000 pg/mL on trigger day; ≥ 15 oocytes retrieved; ovarian hyperstimulation syndrome; uterine or endometrial conditions such as endometriosis, fibroids, polyps, or intrauterine adhesions; serum progesterone > 1.5 ng/mL before trigger day; or patient refusal of fresh embryo transfer. No more than two embryos will be transferred in a single cycle. The number of embryos transferred in each cycle (1 or 2) will be recorded in the CRF.
LPS starts from embryo transfer and continues until the 10th week of pregnancy. All participants will take 90 mg of Progesterone Vaginal Sustained-Release Gel (Selenone® 8%, Merck Serono, Germany) daily. Participants will be randomly assigned to one of two groups: one group will receive 6g of GSATP (Beijing Boran Pharmaceutical Inc., China) three times daily, while the other will receive a placebo. Treatment will be stopped immediately if serum β-hCG is negative, if a biochemical pregnancy loss occurs, or if transvaginal ultrasound shows embryo arrest. Strategies to improve adherence to the intervention or control protocol included standardized training, clear instructions, and regular monitoring of compliance throughout the study.
Outcomes
Efficacy Outcomes
The primary outcome is OPR at 10 weeks after the day of embryo transfer.
Secondary outcomes include:
(1) Positive pregnancy: A serum β-hCG level ≥ 10 mIU/mL, measured 14 days after embryo transfer.
(2) Embryo implantation rate: The percentage of transferred embryos that result in a visible gestational sac.
(3) Clinical pregnancy: Detection of an intrauterine gestational sac with a fetal heartbeat via transvaginal ultrasound at 4 weeks post-embryo transfer.
(4) Ectopic pregnancy: A pregnancy where implantation occurs outside the uterus, confirmed 4 weeks after embryo transfer.
(5) Pregnancy loss: Spontaneous loss of pregnancy recognized clinically before 12 weeks of gestation.
(6) Multiple pregnancy: Presence of two or more fetuses within the uterus.
(7) The prevalence of pregnancy constipation: The percentage of participants experiencing constipation during pregnancy, defined by at least two of the following symptoms: straining, hard stools, incomplete evacuation, anorectal obstruction/blockage, manual intervention for defecation, and fewer than three bowel movements per week. Symptoms must occur in at least 25% of defecations and last for at least one month.
(8) Threatened miscarriage: Abdominal pain and vaginal bleeding during the first trimester, with survival of the intrauterine fetus at 10 weeks after embryo transfer.
(9) Live birth: Birth of at least one child with breath and heartbeat, surviving beyond 24 weeks of gestation.
Safety Outcomes
Preclinical studies have identified potential adverse effects of GSATP, including gastrointestinal discomfort, diarrhea, allergic reactions, and skin rashes. In addition, given that mild gastrointestinal discomfort was more frequently observed in the GSATP group during our previous FET trial, particular attention will be paid to gastrointestinal symptoms throughout the study period. Routine laboratory tests, including liver and renal function (ALT, AST, ALP, total bilirubin, serum creatinine, and urea nitrogen), will be performed at baseline and during follow-up visits to monitor drug safety. Any clinically significant laboratory abnormalities will be recorded as adverse events and assessed for causal relationship with the study medication. Throughout the trial, all adverse events (AEs) experienced by participants will be systematically recorded and assessed by trained researchers to monitor safety profiles. Mild to moderate AEs will be managed according to established protocols, with close clinical follow-up. In the event of serious adverse events (SAEs), defined as those causing severe harm, hospitalization, or threatening life, researchers will immediately terminate the participant’s study treatment, provide appropriate medical intervention, and report the incident to the institutional review board (IRB) and trial monitoring committee (TMC) in accordance with Good Clinical Practice (GCP) guidelines.
Statistical Analysis
Sample Size Calculation
Historical records from our center show that the OPR for women with normal ovarian reserve undergoing IVF-ET with a single fresh embryo transfer is roughly 40%. Building on our prior research,7 we hypothesized that an absolute 12% difference in OPR between groups would represent a clinically meaningful effect. This study aims to detect a 12% OPR difference (52% vs 40%) between the GSATP and placebo groups at a 0.05 significance level with 90% statistical power. To ensure a minimum of 358 participants per group, a sample size of 800 was determined, accounting for a 10% dropout rate. Using PASS 2021 (developed by NCSS, LLC, Kaysville, Utah) for the calculation, 400 participants were allocated to each group.
Planned Data Analysis
The data from all participants will be analyzed using intention-to-treat (ITT) principles, with a per-protocol analysis conducted after excluding cases lost to follow-up. The initial analysis of differences in OPR between the two groups will be based on ITT. Missing data will be handled using multiple imputations. Continuous variables will be compared using the t-test, while categorical variables will be assessed with the chi-square test. Additionally, subgroup analysis will be carried out based on the pre-established age categories. If the randomization does not achieve equilibrium comparability between the two groups, we will use multivariate logistic regression analysis to assess potential confounding factors, such as, BMI (≤30kg/m2 vs >30kg/m2), the number of embryo transfers (1 vs 2), “cleavage vs blastocyst transfer” and dominant embryo transfer (Yes vs No), etc. In cases where the results from the ITT and per-protocol analyses differ, we will prioritize the findings from the initial ITT analysis when interpreting the study outcomes. All statistical analyses will be conducted using SPSS version 26.0 and R 3.5.1, with a significance level set at P < 0.05.
To further minimize potential confounding factors that may influence implantation and pregnancy outcomes, several IVF-related variables will be systematically recorded and adjusted for in the analysis. These include:
(1) Endometrial thickness (EMT) measured by transvaginal ultrasound on the trigger day and the day before embryo transfer; EMT will be treated as a continuous variable and categorized as <7 mm, 7–8.9 mm, or ≥9 mm for subgroup analyses.
(2) Use of nutritional supplements, such as folic acid, vitamin D3, coenzyme Q10, omega-3, or iron, recorded at baseline (within 3 months before stimulation) and during the IVF cycle, including dose and duration. Routine folic acid supplementation (0.4–0.8 mg/day) is permitted.
(3) Preimplantation genetic testing (PGT): patients undergoing embryo biopsy for PGT/PGS/PGT-A are excluded per the exclusion criteria, and any unexpected PGT procedures will be recorded and handled in sensitivity analyses.
(4) Post-conception adjuvant therapies, including low-dose aspirin, corticosteroids, or low-molecular-weight heparin, are allowed according to each center’s standard practice but must be fully documented (agent, dosage, timing, and duration). These therapies will be incorporated as covariates in multivariable models and evaluated in pre-planned sensitivity analyses excluding exposed cases.
Multivariable logistic regression will be performed to adjust for these potential confounders (age, BMI, embryo stage, number of embryos transferred, EMT, supplement use, and post-conception adjuvant therapies) to ensure robustness of the findings.
Data Collection and Management
This study used a structured electronic case report form (eCRF) to collect data on demographics, medical history, reproductive parameters, treatment details, clinical and lab results, pregnancy outcomes, and adverse events. Baseline data were collected at screening. During treatment, ovarian response, embryo number, and quality were recorded. Outcome data were collected at set time points with serum β-hCG, ultrasound, and pregnancy follow-up. Safety data, including adverse events and liver/kidney tests, were recorded in real time. Staff received standardized training, and the coordinating center provided uniform manuals and assessment standards. Study nurses completed eCRF entry and cross-checked with source records within 24 hours. Quarterly audits checked data completeness and compliance. Data were double-entered by independent operators, verified for consistency, and cleaned using logic checks. Missing data were handled with multiple imputation. Electronic data were stored on an encrypted server with role-based access, and paper records were scanned and stored separately. Personal identifiers were replaced with unique study IDs. Daily database backups were kept offsite to ensure security and traceability.
Trial Monitoring
This clinical study started in June 2021 and is scheduled to end in December 2026. So far, we have obtained ethical approval from the Ethics Committee of Reproductive Medicine at the affiliated hospital of Shandong University of TCM (SDUTCM-RME2021-0211) and registered the trial in the NIH clinical trials database (ID: NCT04872660, 05/04/2021).
Discussion
The debate over whether fresh embryo transfer or FET is superior has long been a focal point in ART.25 Fresh embryo transfer carries the risk of OHSS, particularly in patients with high ovarian response to stimulation protocols. While whole embryo freezing can mitigate OHSS incidence, this strategy prolongs the timeline from ART initiation to live birth, as patients must undergo additional cycles for embryo thawing and transfer. Moreover, the cumulative costs of embryo freezing, storage, and resuscitation impose significant economic burdens on patients, adding a layer of complexity to treatment decisions. Fresh embryo transfer remains a commonly used clinical strategy in many IVF programs and differs from frozen-thawed transfer in corpus luteum physiology and immediate endocrine milieu. Prior evidence derived from FET cycles cannot be directly generalized to fresh cycles because luteal hormone dynamics and the presence of corpus luteum differ substantially. Since GSATP is hypothesized to interact with luteal-endometrial function, evaluating its effect specifically in fresh cycles addresses a clinically relevant and mechanistically distinct question. We acknowledge that elective freeze-all strategies are increasingly used and may show differing pregnancy outcomes; this limits generalizability and will be discussed as a study limitation Furthermore, a recent meta-analysis of 11 well-conducted RCTs suggested that the freeze-all strategy is not suitable for women with normal ovarian reserve, as it was linked to a higher risk of preeclampsia compared with fresh embryo transfer.11 This study primarily targets women with normal ovarian reserve, but its findings could have wider relevance for a broader population. The motivation behind this clinical trial stems from the observation that conventional luteal phase support supplemented with medications like estrogen or hCG has failed to demonstrate tangible benefits for pregnancy outcomes in fresh embryo transfer cycles. In our prior research,7 it was discovered that when LPS was used in conjunction with GSATP during FET, it could notably boost the OPR and lower the incidence of TM. However, previous evidence from FET cycles cannot be directly generalized to fresh cycles, as there are significant differences in the dynamic changes of luteal hormones and the presence of the corpus luteum. We acknowledge that the application of the selective full embryo cryopreservation strategy is becoming increasingly widespread and may show different pregnancy outcomes, which limits the generalizability of the study and is one of the limitations of our research. Against this backdrop, this randomized controlled trial seeks to explore a novel approach: evaluating whether the addition of GSATP to standard LPS can optimize the OPR for women undergoing fresh embryo transfer. It should be emphasized that pregnancy outcomes are influenced by multiple factors and cannot be attributed to a single intervention. In our study, potential confounders such as male factor infertility, underlying causes of infertility, thyroid function abnormalities, and thrombotic tendencies were carefully screened and controlled to minimize their impact on early pregnancy outcomes. Recurrent pregnancy loss (defined here as two or more consecutive clinical miscarriages) is excluded because recurrent loss represents a distinct clinical entity with specific etiologies (eg, parental chromosomal rearrangements, acquired thrombophilia, uterine anomalies) and management strategies that could confound the evaluation of GSATP as luteal support in routine IVF cycles. Excluding women with recurrent loss improves cohort homogeneity and reduces potential bias. Any subject who is found after enrollment to meet criteria for recurrent pregnancy loss will be documented and handled in predefined sensitivity analyses.
Moreover, modern pharmacological research has identified key active compounds in GSATP, including baicalein, flavanone, norwogonin, rhynchophylline, polysaccharides, methoxyflavone, acacetin, anthraquinone glycosides, and triterpenoid saponins. These compounds contribute to improving blood circulation, enhancing placental blood flow, regulating immune responses (both cellular and humoral), and addressing endocrine dysfunction. Among these, baicalein and norwogonin are particularly recognized for their role in supporting uterine health.7,26 Among these, baicalein and norwogonin are recognized for enhancing uterine blood flow, nourishing the embryo, strengthening immune modulation, and reducing allergic reactions, all of which help provide protection for the fetus.27,28 Further, Flavanone, methoxyflavone, and acacetin can inhibit TNF-α production via the MAPK signaling pathways, offering anti-inflammatory and antimicrobial effects. These actions help stabilize the intrauterine environment and lower the risk of miscarriage.29–31
This randomized, double-blind, placebo-controlled multicenter trial aims to provide high-quality evidence to demonstrate that GSATP, as an adjunct to standard LPS, may help maintain the stability of early pregnancy, thereby indirectly improving the ongoing pregnancy rate and live birth rate in women with NOR who undergo fresh embryo transfer. Strengths include multicenter design, centralized randomization with age stratification, blinded placebo control, and prespecified sensitivity analyses for key confounders. Limitations include restriction to fresh transfer cycles (which may limit generalizability to elective freeze-all populations), exclusion of distinct clinical subgroups such as PCOS and recurrent pregnancy loss, and potential variability in center practices despite standardized protocols.
Abbreviations
IVF-ET, in vitro fertilization and embryo transfer; ICSI, intracytoplasmic sperm injection; AMH, anti-Mullerian hormone; AFC, antral follicle count; RCT, randomized controlled trial; NOR, normal ovarian reserve; FET, frozen-thawed embryo transfer; TM, threatened miscarriage; GSATP, Gushen Antai Pill; OPR, ongoing pregnancy rate; CRF, case report form; ITT, intention-to-treat; LPS, luteal phase support; hCG, human chorionic gonadotropin; OHSS, ovarian hyperstimulation syndrome; TCM, Traditional Chinese Medicine; TMC, trial monitoring committee.
Data Sharing Statement
The authors will provide the raw data for this article, and it will not be retained inappropriately.
Ethics Approval and Consent to Participate
We confirm that this trial will adhere to the principles outlined in the Declaration of Helsinki. The study has been approved by the Ethics Committee of Reproductive Medicine at the affiliated hospital of Shandong University of Traditional Chinese Medicine (SDUTCM-RME2021-0211). Written informed consent will be obtained from all eligible participants prior to their involvement in the study.
Acknowledgment
The authors wish to thank all the participants and researchers for their valuable contributions to this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was sponsored by the Natural Science Foundation of Shandong Province (ZR2023LZY021).
Disclosure
The authors declare no conflicts of interest related to this manuscript.
References
1. Gurunath S, Pandian Z, Anderson RA, et al. Defining infertility—a systematic review of prevalence studies. Hum Reprod Update. 2011;17(5):575–588. doi:10.1093/humupd/dmr015
2. Zhou Z, Zheng D, Wu H, et al. Epidemiology of infertility in China: a population-based study. BJOG. 2018;125(4):432–441. doi:10.1111/1471-0528.14966
3. Ubaldi F, Bourgain C, Tournaye H, et al. Endometrial evaluation by aspiration biopsy on the day of oocyte retrieval in the embryo transfer cycles in patients with serum progesterone rise during the follicular phase. Fertil Sterility. 1997;67(3):521–526. doi:10.1016/S0015-0282(97)80080-5
4. Tavaniotou A, Devroey P. Luteal hormonal profile of oocyte donors stimulated with a GnRH antagonist compared with natural cycles. Reprod Biomed Online. 2006;13(3):326–330. doi:10.1016/S1472-6483(10)61435-6
5. Kolibianakis EM, Bourgain C, Platteau P, Albano C, Van Steirteghem AC, Devroey P. Abnormal endometrial development occurs during the luteal phase of nonsupplemented donor cycles treated with recombinant follicle-stimulating hormone and gonadotropin-releasing hormone antagonists. Fertil Sterility. 2003;80(2):464–466. doi:10.1016/S0015-0282(03)00663-0
6. Van Der Linden M, Buckingham K, Farquhar C, et al. Luteal phase support for assisted reproduction cycles. Cochrane Database Syst Rev. 2015;2016(10).
7. Cao X-L, Song J-Y, Zhang -X-X. Effects of a Chinese patent medicine Gushen’antai Pills on ongoing pregnancy rate of hormone therapy FET cycles: a multi-center, randomized, double-blind, placebo-controlled clinical trial. Front Endocrinol. 2020;11:581719. doi:10.3389/fendo.2020.581719
8. Lu Y, Long X. Clinical efficacy of Gushen Antai Pill combined with progesterone after in vitro fertilization-embryo transfer. Maternal Child Health Care China. 2017;32(9):1980–1982.
9. Chen K, Liu X, Meng X, et al. Efficacy and safety of Gushen Antai Pills combined with dydrogesterone in the treatment of threatened miscarriage: a systematic review and meta-analysis. Front Pharmacol. 2023;14:1138968. doi:10.3389/fphar.2023.1138968
10. Wei Q, Yang X. Efficacy of Gushen Antai Pill in the treatment of early recurrent abortion with kidney deficiency and liver depression syndrome. Maternal Child Health Care China. 2018;33(23):5528–5530.
11. Zeng P, Zhou H, Guo P, et al. Efficacy and safety of traditional Chinese herbal medicine in the treatment of threatened abortion: a protocol for systematic review and meta-analysis. Medicine. 2021;100(5):e23288. doi:10.1097/MD.0000000000023288
12. Zhang L, Dong B, Yuan X. Clinical observation of Gushen Antai Pill combined with dalteparin sodium in the treatment of recurrent abortion with positive anticardiolipin antibody (ACA). China Pharm. 2023;34(7):863–867.
13. Ma Y-J, Cao X-L, Ma T. Study protocol: a multi-center, double-blind, randomized, 6-month, placebo-controlled trial to investigate the effect of supplementing hormone therapy FET cycles with Gushen’antai pills on the outcomes of in vitro fertilization. Trials. 2021;22(1):657. doi:10.1186/s13063-021-05614-w
14. Ding J, Tan X, Song K, et al. Bushen huoxue recipe alleviates implantation loss in mice by enhancing estrogen-progesterone signals and promoting decidual angiogenesis through FGF2 during early pregnancy. Front Pharmacol. 2018;9:437. doi:10.3389/fphar.2018.00437
15. Yang M, Luo J, Yang Q, et al. Research on the medication rules of Chinese herbal formulas on treatment of threatened abortion. Complement Ther Clin Pract. 2021;43:101371. doi:10.1016/j.ctcp.2021.101371
16. Wei D. Clinical effect of Gushen Antai Pill combined with dydrogesterone in the treatment of recurrent spontaneous abortion. Clin Res Pra. 2019;4(2):139–140,158.
17. Feng L, Fan R, Jiang A, et al. The effect of flexible low-dose GnRH antagonist on pregnancy outcome in the fresh embryo transfer cycle of IVF-ET: a randomized controlled trial. Reprod Biol Endocrinol. 2022;20(1):55. doi:10.1186/s12958-022-00927-0
18. Chinese society of reproductive medicine. Assisted reproductive technology data report, 2017–2021. Beijing: Chinese Society of Reproductive Medicine; 2025.
19. Ye H, Shi L, Quan X, et al. Cumulative live birth rate of in vitro fertilization cycle via progestin-primed ovarian stimulation versus gonadotropin-releasing hormone antagonist protocol in infertile women with normal ovarian reserve: an open-label, randomized controlled trial. Human Fertil. 2024;27(1):2316005. doi:10.1080/14647273.2024.2316005
20. Liu X, Wen W, Wang T, et al. Increased versus standard gonadotrophin dosing in predicted poor responders of IVF: an open-label randomized controlled trial. Hum Reprod. 2022;37(8):1806–1815. doi:10.1093/humrep/deac113
21. Xu Y, Hu X, Ai KL, et al. Gushen Antai Pill for expected normal ovarian responders undergoing IVF-ET (GSATP-FreET): interim analysis of a randomized controlled trial. Contracep Reprod Med. 2025;10(1):19. doi:10.1186/s40834-025-00352-9
22. Song JY. Efficacy and safety of Gushen Antai Pill on ongoing pregnancy rate in women with normal ovarian reserve undergoing in vitro fertilization embryo transfer: a prospective, multicentre, randomised, double-blind, placebo-controlled trial: NCT04872660[R]. clinicaltrials.gov. 2024.
23. Deadmond A, Koch CA, Parry JP. Ovarian reserve testing[M]//Endotext [internet]. MDText.com, Inc. 2022.
24. Yeung T, Chai J, Li R, et al. A double-blind randomised controlled trial on the effect of dehydroepiandrosterone on ovarian reserve markers, ovarian response and number of oocytes in anticipated normal ovarian responders. BJOG. 2016;123(7):1097–1105. doi:10.1111/1471-0528.13808
25. Roque M, Haahr T, Geber S, et al. Fresh versus elective frozen embryo transfer in IVF/ICSI cycles: a systematic review and meta-analysis of reproductive outcomes. Hum Reprod Update. 2019;25(1):2–14. doi:10.1093/humupd/dmy033
26. Dang C-X, Wang D, Liu P-F, Liu J-X, Yu X. Network pharmacological analysis and molecular docking of Huangqin-Baizhu herb pair in the treatment of threatened abortion. Medicine. 2022;101(36):e30417. doi:10.1097/MD.0000000000030417
27. Wu L, Yang FR, Xing ML, et al. Multi-material basis and multi-mechanisms of the Dahuang Zhechong pill for regulating Treg/Th1 balance in hepatocellular carcinoma. Phytomedicine. 2022;100:154055. doi:10.1016/j.phymed.2022.154055
28. Liao H, Ye J, Gao L, et al. The main bioactive compounds of Scutellaria baicalensis Georgi. for alleviation of inflammatory cytokines: a comprehensive review. Biomed Pharmacother. 2021;133:110917.
29. Chang W, Wu QQ, Xiao Y, et al. Acacetin protects against cardiac remodeling after myocardial infarction by mediating MAPK and PI3K/Akt signal pathway. J Pharmacol Sci. 2017;135(4):156–163. doi:10.1016/j.jphs.2017.11.009
30. Singh S, Meena A, Luqman S, et al. Acacetin and pinostrobin as a promising inhibitor of cancer-associated protein kinases. Food Chem Toxicol. 2021;151:112091. doi:10.1016/j.fct.2021.112091
31. Dang C-X, Wang D, Liu P-F, Liu J-X, Yu X. Network pharmacological analysis and molecular docking of Huangqin-Baizhu herb pair in the treatment of threatened abortion. Medicine. 2022;101(36):e30417.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.