Back to Journals » International Journal of Women's Health » Volume 17
Integrated HPV Testing, TCT, and Colposcopic VIA/VILI Improves Detection Rate for HSIL and Cervical Cancer: A Retrospective Cohort in China
Authors Xie H, Huang J, Ye M, Xu J, Zou R, Zhang Z, Luo J, Wang S, Liu G, Wang G, Geng J, Huang W ![]()
Received 3 July 2025
Accepted for publication 5 November 2025
Published 19 November 2025 Volume 2025:17 Pages 4649—4660
DOI https://doi.org/10.2147/IJWH.S551316
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Hong Xie,1,2,* Jian Huang,2,3,* Mei Ye,4 Jie Xu,3 Rong Zou,3 Zhaoqi Zhang,5 Jun Luo,2,6 Shanyun Wang,7 Guohong Liu,3 Gang Wang,3 Jianxiang Geng,2,8 Wanqiu Huang3
1Department of Gynecology, Shenzhen People’s Hospital (The First Affiliated Hospital, Southern University of Science and Technology; The Second Clinical Medical College, Jinan University), Shenzhen, 518020, People’s Republic of China; 2The Cross-Strait Precision Medicine Association-HPV Infection Disease Professional Committee, Nanjing, People’s Republic of China; 3Key Laboratory of Systems Biomedicine (Ministry of Education), Shanghai Centre for Systems Biomedicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 4Nanjing Jiangning District Maternal and Child Health and Family Planning Service Center, Nanjing, People’s Republic of China; 5Department of General Surgery, Shanghai General Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 6Reproductive Testing Quality Control Department of Central Laboratory, Jiangsu Health Vocational College, Nanjing, People’s Republic of China; 7Zhongshan Hospital of Traditional Chinese Medicine, the Second Clinical School of Guangzhou University of Chinese Medicine, Zhongshan, People’s Republic of China; 8Department of Pathology, Nanjing Hospital of Traditional Chinese Medicine, Nanjing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wanqiu Huang, Key Laboratory of Systems Biomedicine (Ministry of Education), Shanghai Centre for Systems Biomedicine, Shanghai Jiao Tong University, Shanghai, 200240, People’s Republic of China, Email [email protected]
Purpose: To evaluate the diagnostic performance of the current three-step cervical cancer screening strategy in Chinese women and explore the optimized value of integrating human papillomavirus (HPV) testing, ThinPrep cytology test (TCT), and colposcopic visual inspection with acetic acid/Lugol’s iodine (VIA/VILI) for improving cervical disease detection.
Patients and Methods: A retrospective study was conducted on 11,405 outpatients of Shenzhen People’s Hospital (2018– 2023). Inclusion criteria were a history of sexual activity plus at least one of the following: high-risk HPV (HR-HPV) positivity, abnormal TCT results, or highly suspicious symptoms. Exclusions included prior hysterectomy, cervical cancer (CC) treatment history, pregnancy, or incomplete medical records. The diagnostic performance of HR-HPV testing, TCT, and colposcopic VIA/VILI results was evaluated using pathologically confirmed high-grade squamous intraepithelial lesion (HSIL) and CC as the reference standard. The calculated metrics comprised sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and area under the curve (AUC).
Results: Among the cohort, the positive rates were 71.56% for HR-HPV, 32.57% for abnormal cytology, and 9.34% for colposcopic VIA/VILI. For detecting HSIL/CC, the NPVs of HPV testing, TCT, and colposcopic VIA/VILI were 0.976, 0.955, and 0.965, respectively. Combined use of the three modalities achieved an NPV of 0.999 for HSIL/CC. Integrating colposcopic VIA/VILI into primary screening also reduced both false-positive and false-negative results compared with single-modality strategies.
Conclusion: In this large real-world retrospective cohort, combining HPV testing, TCT, and colposcopic VIA/VILI improves the diagnostic accuracy of high-grade cervical disease (HSIL and CC), with practical feasibility for clinical application. However, this integrated approach needs prospective multi-center validation before widespread promotion in cervical cancer screening among community populations.
Keywords: uterine cervical neoplasms, human papillomavirus, cytology, colposcopy, mass screening, China
Introduction
Cervical cancer (CC) is the second most prevalent malignancy in the female reproductive system, following breast cancer. According to the GLOBOCAN 2022 report, an estimated 661,000 new cases and 349,000 deaths occurred globally, ranking eighth in overall cancer incidence and fourth among women.1 In China, approximately 150,700 new cases and 55,700 deaths were reported in 2022.2 In China, incidence has increased and mortality has risen in specific regions or age groups, particularly in rural populations, despite overall fluctuations in the national age-standardized mortality rate.3,4 These figures highlight an urgent need to strengthen early detection and prevention strategies.
CC is among the most preventable and treatable malignancies when detected in its early stages.5 Early identification of precancerous lesions combined with timely intervention can prevent the progression to invasive CC.5 In 2020, the World Health Organization (WHO) launched the Global Strategy to Accelerate the Elimination of Cervical Cancer, setting ambitious 2030 targets to achieve 70% screening coverage among women using a high-performance test.6,7 The widely adopted WHO-recommended three-step screening strategy—comprising primary screening with human papillomavirus (HPV) testing or cytology (TCT), colposcopic examination for screen-positive cases, and histopathological confirmation—was designed to improve diagnostic accuracy and ensure accessibility, particularly in resource-limited settings.7–9 However, in clinical practice, the implementation of this strategy faces several challenges, especially in China.10,11 First, the high prevalence of HPV infection in the Chinese population often results in a large number of HPV-positive but histologically negative cases, leading to unnecessary colposcopy referrals and increased healthcare burden.12 Second, the sensitivity of TCT for detecting high-grade lesions varies widely across regions, depending on the quality of sample collection and the availability of experienced cytopathologists.13,14 Third, cytology-based screening is constrained in primary and resource-limited settings by the shortage of trained cytologists/pathologists and dedicated laboratories, which has driven programs to adopt HPV-based primary screening.15 Additionally, a proportion of cervical cancers are HPV-negative which may lead to delayed diagnosis if colposcopy is performed only in HPV- or TCT- positive women.16,17
Given these challenges, there is a need to evaluate the diagnostic performance of existing screening modalities and to explore more practical approaches that balance accuracy, efficiency, and feasibility in the Chinese healthcare context.18 Electronic colposcopy combined with visual Inspection with Acetic Acid (VIA) and Lugol’s Iodine (VILI) has recently gained attention as a moderately priced, real-time visual diagnostic tool that can complement laboratory-based screening.19–21
Therefore, we conducted a large-scale retrospective analysis of 11,405 Chinese women to compare the diagnostic performance of HPV testing, TCT, and colposcopic VIA/VILI, using histopathological diagnosis as the gold standard. Our primary objective was to quantify the diagnostic yield of each approach for detecting high-grade squamous intraepithelial lesions (HSIL) and cervical cancer in an outpatient population, which is consistent with screening research and guideline frameworks, accuracy was benchmarked against cervical intraepithelial neoplasia II + (CIN II+) histology, operationalized clinically as HSIL or invasive CC.6,22–24 A secondary objective was to outline a pragmatic screening pathway that aligns with national program goals while accommodating local service capacity. Ultimately, we sought to provide evidence to optimize cervical cancer screening by improving diagnostic accuracy, reducing unnecessary procedures, and using healthcare resources more efficiently.
Materials and Methods
Study Design and Population
We conducted a retrospective study using the gynecological outpatient electronic medical record database of Shenzhen People’s Hospital (Grade IIIA tertiary hospital, Guangdong Province, China) for the period 2018–2023. After applying the predefined inclusion and exclusion criteria and confirming data completeness with histopathological results, 11,405 records were included in the final analysis (Table S1).
Inclusion criteria included: ①history of sexual activity; ②autonomous symptoms like abnormal vaginal discharge or postcoital bleeding; ③abnormal TCT results or HR-HPV positivity; ④cervical abnormal findings on routine gynecologic examination (Table S1). Exclusion criteria included: ①cervical cancer patients who had prior surgery, radiotherapy, or chemotherapy; ②patients with a total hysterectomy; ③patients in special physiological periods, such as pregnancy (Figure S1).
Statistical Analysis
SPSS 22.0 (IBM Corp., Armonk, NY, USA) was used for statistical analysis. Categorical variables were expressed as frequencies and percentages. The comparisons between groups were performed using the Pearson chi-square test or Fisher’s exact test when any expected cell count was <5. The diagnostic performance of HPV testing, TCT, and colposcopic VIA/VILI for detecting HSIL/CC was evaluated by calculating sensitivity, specificity, PPV, and NPV based on histopathological results as the reference standard. Sensitivity, specificity, PPV, and NPV were calculated using the following formulas: Specificity = TN / (TN + FP), PPV = TP / (TP + FP), NPV = TN / (TN + FN), where TP, TN, FP, and FN represent true positive, true negative, false positive, and false negative cases, respectively. Receiver operating characteristic (ROC) curves were constructed, and the area under the curve (AUC) was used to assess overall diagnostic accuracy. A two-sided P value <0.05 was considered statistically significant.
Patient and Public Involvement
Our study was conducted by analyzing anonymized data from clinical database. As such, patients were not involved in the design, conduct, reporting, or dissemination plans of this research.
Additional methodological details are described in Supplementary Materials and Methods.
Results
Histopathological Outcomes in Women Referred for Colposcopy-Directed Biopsy
A total of 11,405 outpatients with biopsy based on predefined clinical indications, including HR-HPV positivity, abnormal TCT results, or highly suspicious signs (eg, postcoital bleeding or visible suspicious lesions) (Figure S1). Colposcopy-directed biopsies yielded 189 CCs (1.66%) and 919 HSILs (8.06%) (Figure 1A and Table 1). The remaining 90.28% (10,297/11,405) were diagnosed with other cervical pathologies (eg, low-grade squamous intraepithelial lesion (LSIL), chronic inflammation (CI)) (Figure 1A and Table 1).
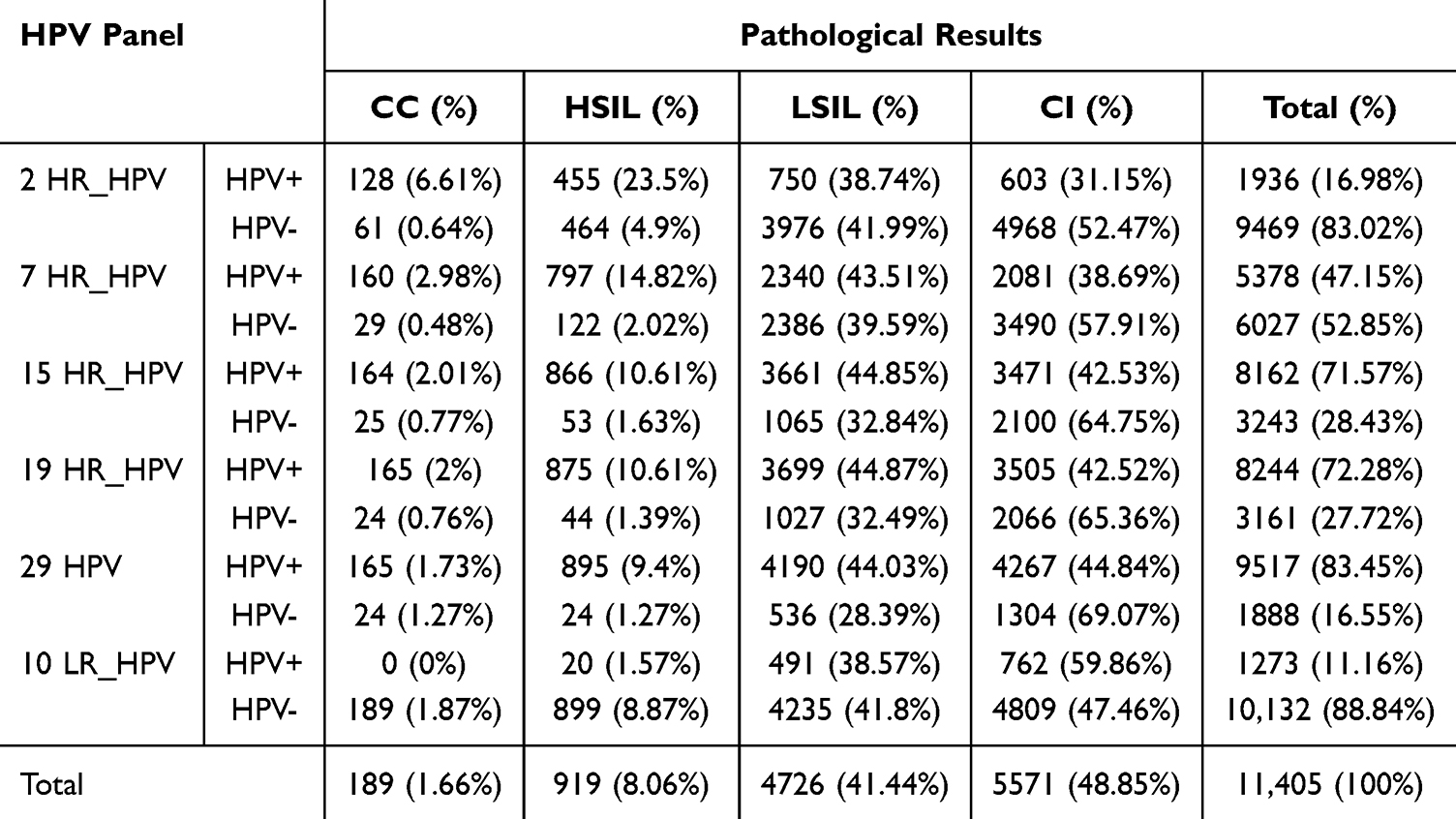 |
Table 1 Distribution of Infection Rate of Different HPV Genotypes in 11,405 Women Compared to the Results by Gold Standard |
 |
Figure 1 Pathological diagnosis and HPV infection characteristics among 11,405 outpatient women. (A) Bar chart showing the distribution of different pathological diagnoses. (B) Histogram illustrating the age distribution of 11,405 women. (C) Age-specific distribution of HSIL and CC cases. Triple peaks are observed in the age groups 31–35 (10.11%), 56–60 (14.10%), and 71–75 (38.00%). (D) Comparative distribution of LSIL and CI across different age groups. (E) Pie chart indicating the proportion of HPV-positive and HPV-negative women among the study population. (F) HPV infection rates across different pathological categories. Abbreviations: SCC, squamous cell carcinoma; ACC, adenocarcinoma; CC, cervical cancer; HSIL, high-grade squamous intraepithelial lesion; LSIL, low-grade squamous intraepithelial lesion; CI, chronic inflammation. |
Participants were aged 15 to 80, with an average age of 39.83 ± 11.04 years. They mainly aged between 26 and 50, accounting for 73.90% (8,431/11,405), with the peak value occurring between 31 and 40 years old (Figure 1B and Table S2). This indicates that middle-aged and young women are the primary population affected by female lower reproductive tract diseases. Consistent with screening research and guideline frameworks, accuracy was benchmarked against CIN II+ histology, operationalized clinically as HSIL or invasive CC.6,7,22–26 Therefore, we separately calculated the age-specific distribution of CC+HSIL and LSIL+CI (Figure 1C and D). The age-specific distribution of CC+HSIL exhibited a trimodal pattern, with three distinct incidence peaks are observed at 31–35, 56–60, and 71–75 years (Figure 1C and Table S2). Despite the relatively low outpatient attendance among women over the age of 66, the proportion of CC+HSIL diagnoses increased with advancing age, indicating the need to include older women in the management of cervical cancer screening.27 In contrast, LSIL and CI demonstrated different age-associated patterns, suggesting no significant age predisposition (Figure 1D and Table S2).
The Diagnostic Value of HPV in Identifying CC and HSIL
We calculated the positive rates for five different panels of HPV genotypes (2, 7, 15, 19, and 29 HPV genotypes). The results showed HPV positivity varies materially with the size of the genotype panel (Table 1). Hence, statistical work related to HPV positive rates must clearly identify the number of HPV genotypes. In epidemiological and clinical genotyping studies, the 14 or 15 HR-HPV genotypes are commonly used as an “extended HR-HPV panel”.25,28–32 In this study, we specifically focused on evaluating the diagnostic performance of the 15-type HPV panel for detecting CC and HSIL, as it offers a comprehensive assessment of HR-HPV types relevant to high-grade cervical disease. As expected, positivity and sensitivity increase with larger panels, whereas specificity decreases due to broader inclusion of high-risk types (Table 1). Notably, the overall HR-HPV positivity was 71.57% (8,162/11,405) with the 15-type panel (Figure 1E and F). It is broadly consistent with the HR-HPV rates reported in colposcopy-referred populations (approximately 57.8% to 66.8%).33–35
In this study, the detection results of different HR-HPV panel were compared with the pathological diagnosis results of CC and HSIL (Table 2). Using HPV16/18 only, the sensitivity for identifying CC and HSIL in 11,405 outpatients was 0.526, with a higher specificity of 0.869. In contrast, the 15-type HR-HPV panel yielded a sensitivity of 0.930 with a specificity of 0.307; while the 19-type HR-HPV panel showed a very similar sensitivity of 0.936 but further reductions in specificity of 0.3 (Table 2). These findings confirm the trade-off between sensitivity and specificity as the panel expands. However, among all 15 HR-HPV-positive cases, only 12.62% (1,030/8,162) were true positives, including 164 cases of CC and 866 cases of HSIL (Table 2). The PPV of 15-type panel was only 0.126 for CC and HSIL (Table 2). In our high-prevalence setting, HR-HPV testing identifies many infections that are histologically negative for HSIL/CC at the index visit, resulting in low PPV and substantial colposcopy referrals, thereby increasing healthcare burden.
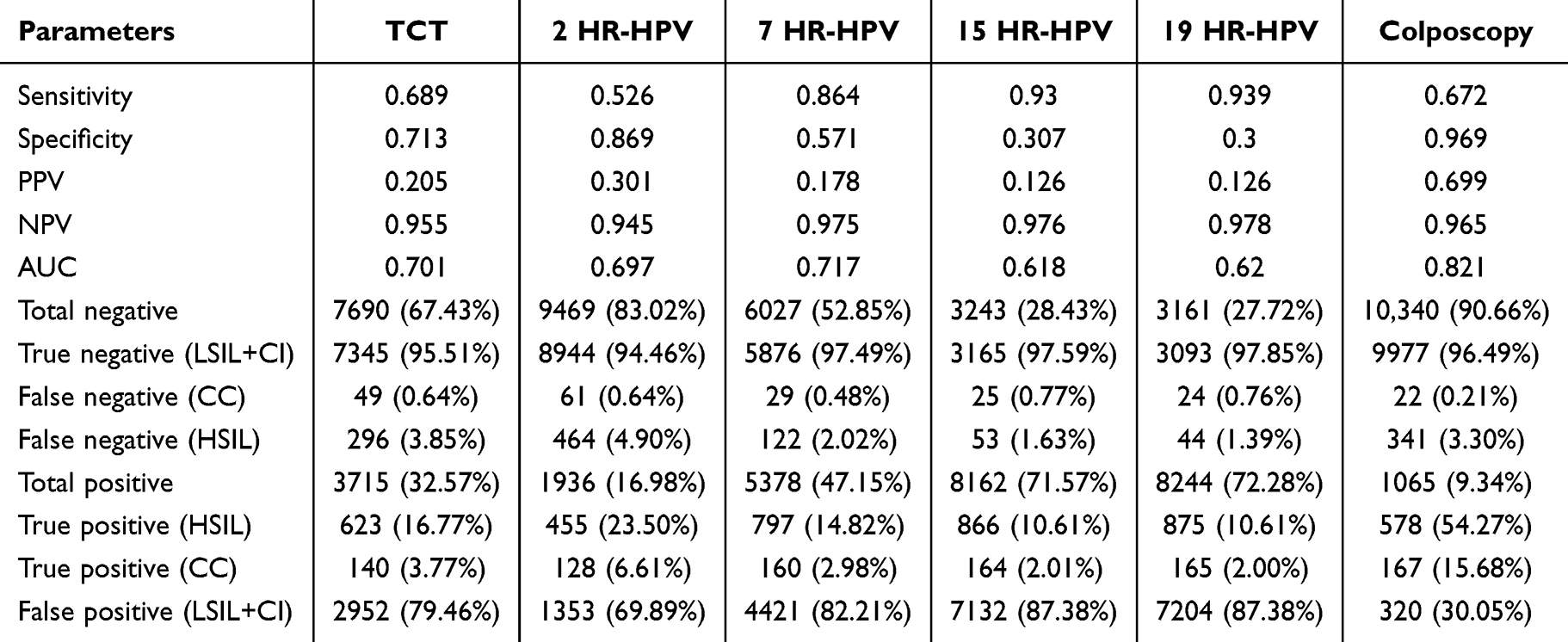 |
Table 2 The Parameters from Three Methods Compared to the Results by Gold Standard |
The Diagnostic Value of TCT in Identifying CC and HSIL
In this study, 32.57% (3,715/11,405) “ASC-US and above” results were defined as TCT-positive cases. Among TCT-positive cases, 20.54% (763/3,715) were histologically confirmed as HSIL/CC, comprising 140 cervical cancers and 623 HSIL (Table S3), yielding a PPV of 0.205 (Table 2). When benchmarked against histopathologic HSIL/CC, the sensitivity and specificity of TCT were 0.689 and 0.713, respectively, with an AUC value of 0.701 (Table 2).
Then, among 79.46% (2,952/3,715) TCT-positive cases with histological LSIL/CI, cytology predominantly reflected low-grade abnormalities: ASC-US accounted for 1,990/2,952 (67.41%) and LSIL for 789/2,952 (26.73%) (Table S3). And the less frequent categories comprised 173 in 2,952 cases (5.86%), including AGC (n=25), ASC-H (n=102), and HSIL (n=46) (Table S3). These results underscored the limited positive predictive value of TCT for clinically actional HSIL/CC detection and highlight the importance of rigorous cytopathology quality assurance and appropriately designed triage to minimize unnecessary downstream procedures.
The Value of Colposcopic VIA/VILI in Diagnosing CC and HSIL
In this study, aberrant results on VIA/VILI tests under colposcopy indicating “suspicious CC or HSIL” were defined as “colposcopic positive” results. When compared with the histopathological diagnosis of CC and HSIL, colposcopic positivity demonstrated a sensitivity of 0.672 and specificity of 0.969, with an AUC of 0.821, suggesting strong diagnostic performance for CC or HSIL (Table 2). In the 1,065 cases with positive colposcopic impressions, histology confirmed HSIL/CC in 745 cases (69.65%), including 167 CCs and 578 HSILs (Table S4). The corresponding PPV was 0.699, which was significantly higher than that of HPV testing or TCT (p<0.05) (Table 2).
Among the 90.66% (10,340/11,405) of colposcopically negative cases (VIA/VILI impression of LSIL or CI), only 3.51% (363/10,340) were false negatives, including 0.21% (22/10,340) CCs and 3.29% (341/10,340) HSILs (Table S4), resulting in a very high NPV of 0.965 (Table 2). These findings indicate that that colposcopic VIA/VILI alone is highly effective for ruling out disease.
To assess the diagnostic reliability of colposcopic VIA/VILI, two experienced senior gynecologists re-evaluated the original colposcopy images of all 361 false-negative cases. 8/22 misclassified CC cases were reclassified as HSIL according colposcopy features (Figures S2–S4). While 47/341 misclassified HSIL cases were reclassified as HSIL (Tables S1–S4). These findings confirm that colposcopic VIA/VILI, when performed with high-resolution imaging and experienced interpretation, exhibits excellent specificity and favorable diagnostic accuracy in primary cervical cancer screening.
The Diagnose Value of Colposcopic VIA/VILI in HPV-Negative Cases
Among the 3,243 (28.43% of 11,405) HR-HPV (15-type panel) negative cases (Table S5), 2.41% (78/3,243) had positive colposcopic VIA/VILI findings, comprising 16 CCs and 62 HSILs (Table S5). Of these 78 cases, 57.69% (45/78) were confirmed as true positives and 42.31% (33/78) were false positives by histopathology HSIL/CC (Table S6). Negative colposcopic VIA/VILI results accounted for 97.59% (3,165/3,243), including 72.25% LSILs and 25.35% CIs (Table S5). False negative cases (histopathology HSIL/CC) accounted for only 1.04% (33/3,165), comprising four CCs and 29 HSILs (Table S7). Notably, although all four cervical cancer cases were negative on both HR-HPV testing and colposcopic VIA/VILI, they presented with postcoital bleeding. In accordance with colposcopy guidelines,36 these clinically suspicious cases were referred for colposcopy-directed biopsy, and histopathology confirmed cervical cancer (two adenocarcinomas, one clear cell carcinoma, and one squamous cell carcinoma), thereby preventing missed diagnoses (Table S1).
In the 29 cases of HSIL missed by colposcopic VIA/VILI, five cases could be classified as HSIL after re-examination the colposcopy images by experienced gynecologists (Table S1). This result suggested that accurate colposcopic identification of high-grade lesions (CIN II+) remain particularly challenging due to their non-specific or inconspicuous visual characteristics. Future research should explore the integration of molecular biomarkers such as DNA methylation profiling, or gene mutation analysis, which may provide additional diagnostic value beyond visual inspection.37,38
Diagnostic Value of the Combined HPV, TCT, and Colposcopy in Detecting CC and HSIL
Our results showed that the NPVs for identifying CC and HSIL using HPV testing, TCT, or colposcopic VIA/VILI were 0.976, 0.955, and 0.965, respectively (Table 2), with no significant differences among the three approaches (p>0.05). However, when all these techniques were applied in combination, the NPV for detecting CC reached 0.999 (Table 3). Only three cases of CC were missed (Table 4 and Figure 2). Upon re-evaluation of the original colposcopic images for these three cases, two could be reclassified as HSIL, while the remaining case demonstrated typical features of a Type 3 transformation zone (Table S1 and Figure 2). Therefore, high-quality colposcopic evaluation using VIA/VILI reduces the rate of missed cervical cancer cases where both HPV testing and TCT yield negative results. Our findings suggest that the combination of all three methods into routine screening protocols may significantly enhance detection rates and reduce missed diagnoses of HSILs and CCs.
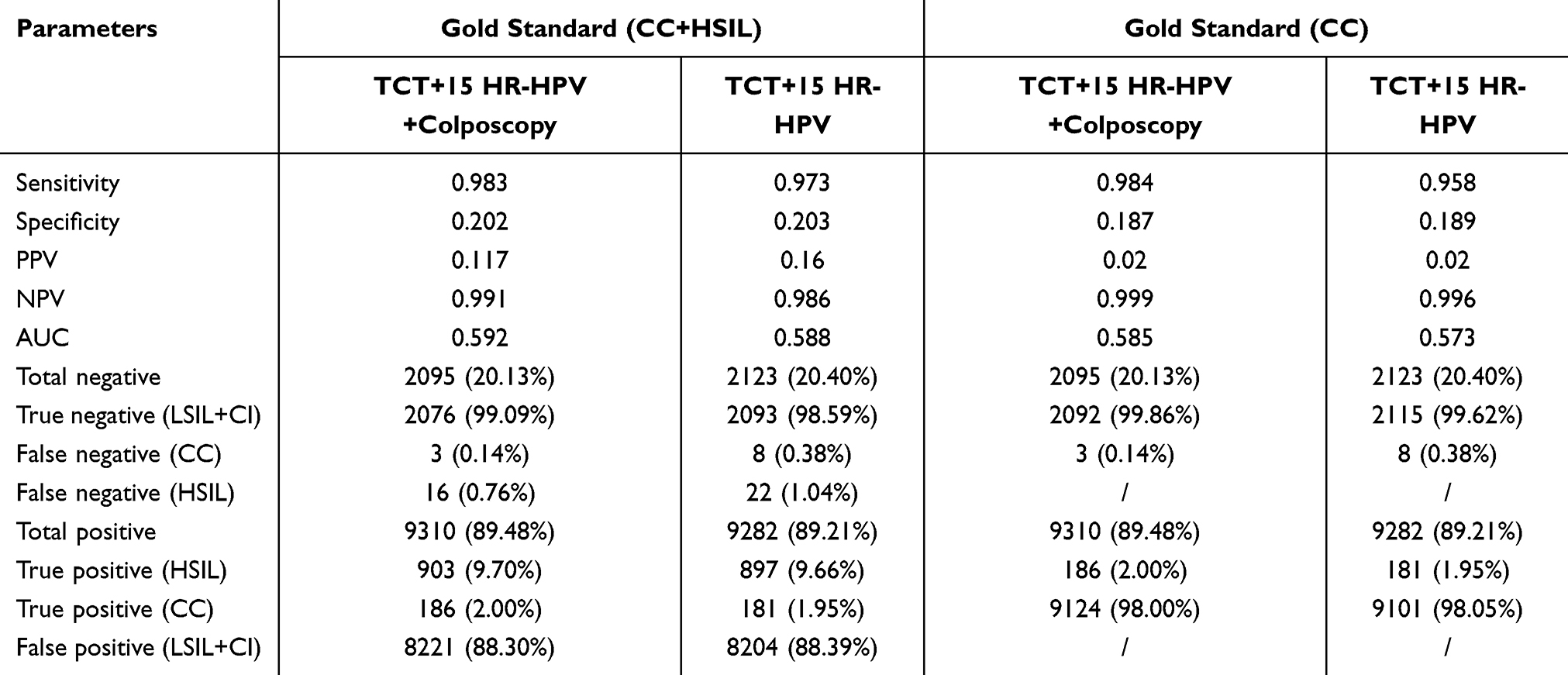 |
Table 3 The Parameters from Different Methods Compared to the Results by Gold Standard |
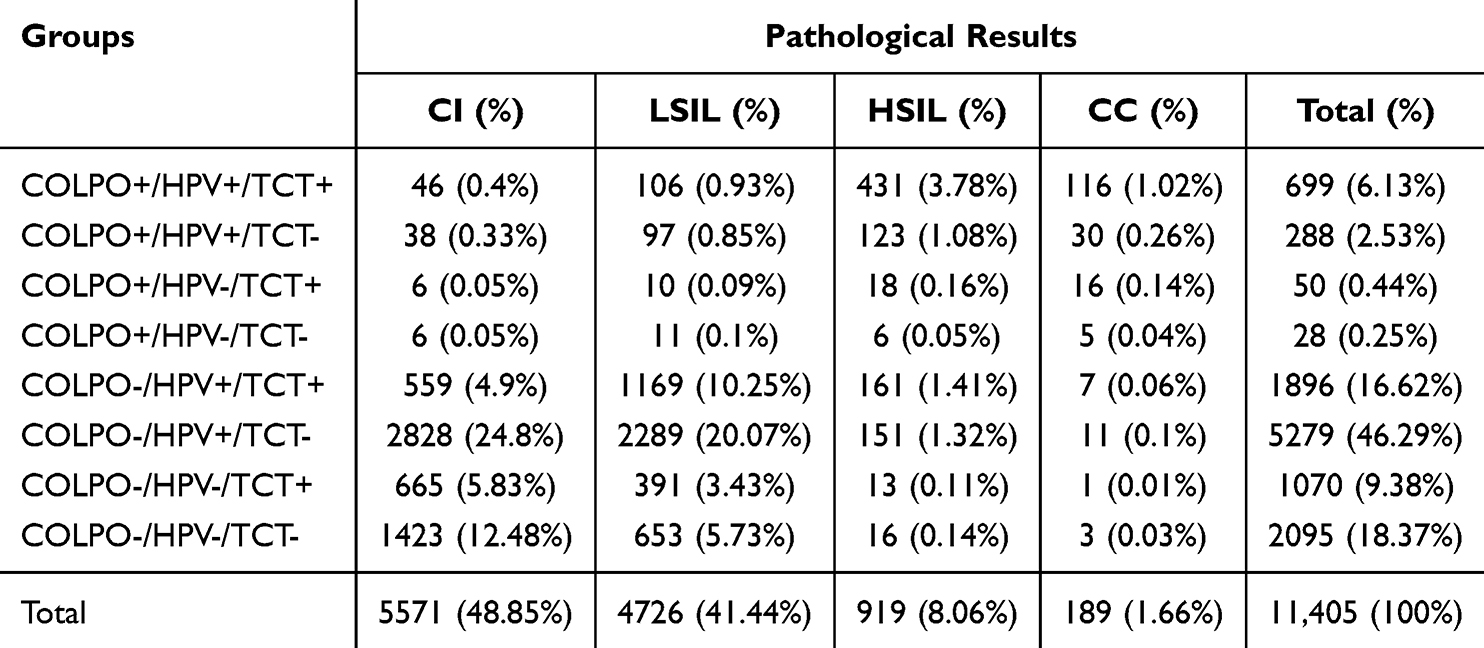 |
Table 4 The Combined Results of HPV/TCT/COLPO Methods Compared to the Results by Gold Standard |
 |
Figure 2 Representative colposcopic images from three cervical cancer cases initially missed by the combined screening strategy (HR-HPV, TCT, and VIA/VILI). (A) Squamous cell carcinoma (SCC; case END_09341). (B) Adenocarcinoma (ADC; case END_03321). (C) Adenocarcinoma (ADC; case END_09159). Abbreviations: SCC, squamous cell carcinoma; ADC, adenocarcinoma. |
Discussion
In 2020, the WHO launched the Global Strategy to Accelerate the Elimination of Cervical Cancer, targeting an incidence below 4 cases per 100,000 women by 2030.6,7 China has actively implemented relevant policies. However, it still requires a better balance among cost, efficiency, and diagnostic accuracy, and the development of screening paradigms that are operationally feasible in Chinese healthcare settings while reducing both false positives and false negatives.10,39
Challenges of the WHO-Recommended Three-Step Strategy in Real-World Practice
The WHO-recommended “three-step strategy” (primary HPV or cytology, colposcopy for positives, histopathology for abnormalities) has enabled scale-up of screening worldwide.8,9,23,40 Nonetheless, under China’s uneven distribution of medical resources, our data indicate room for improvement with respect to downstream resource utilization, missed diagnoses, and programmatic feasibility.
First, “false-positive” screen results remain a predominant driver of downstream overuse. Using histopathology-confirmed HSIL and CC as the positive reference (clinically actionable disease), the 15-type HR-HPV assay achieved high sensitivity (0.930) but low specificity (0.307) for HSIL/CC, translating into predominance of low-grade histology results (87.38% LSIL/CI in 8,162 HR-HPV-positive cases) (Table 2). Although TCT improved specificity (0.713), 79.46% of TCT-positive biopsies were still LSIL/CI (Table 2). Even combined HR-HPV and TCT testing provided strong rule-out performance (NPV for HSIL/CC 0.987) (Table 3), but the majority of HPV/TCT-positive biopsies were LSIL/CI (88.38%) (Table S7), indicating that over-biopsy remains insufficiently mitigated. Under current algorithms, these patients typically undergo colposcopy and even biopsy, increasing anxiety and costs and straining limited colposcopy capacity.39,41,42
Second, single-modality screening risks clinically meaningful misses. Among HR-HPV-negative cases (3,243/11,405), histology revealed 2.39% missed HSIL/CC (Tables 2 and S5). While in TCT-negative cases (7,690/11,405), the missed HSIL/CC fraction was 4.49% (Tables 2 and S3). Importantly, 5/8 CCs (HPV- and TCT-negative) were detected because of abnormal VIA/VILI impression and immediate biopsy (Tables S1–S5). For non-16/18 HR-HPV-positive but TCT-negative women, annual surveillance is commonly recommended. However, 2.86% (124/4,337) had HSIL/CC, and 33.87% (42/124) were identified at the initial visit by VIA/VILI (Tables S8 and S9). These observations suggest that in populations or regions with suboptimal adherence, the current pathway risks missed or delayed diagnosis among HPV/TCT-negative patients.17,38
Third, resource constraints impede implementation. At the primary-care level, limited HPV testing capacity and shortages of cytology experts hinder universal HPV testing or TCT as the first-triage implementation. Colposcopy is generally positioned downstream as triage, rather than as a same-visit assessment, concentrating demand at tertiary hospitals, lengthening referral chains, and reducing adherence.19,43 Prior reports likewise indicate that 28.9% of screen-positive (either ASC-US+ or HR-HPV positive), women do not complete colposcopy, increasing the risk of disease progression.44
Value of Combining HPV, TCT, and Colposcopic VIA/VILI
To address these problems, we evaluated a coordinated strategy of HR-HPV + TCT + colposcopic VIA/VILI. Importantly, this approach does not replace the WHO-endorsed HPV-first entry. It constitutes a resource-stratified, stepwise combined triage pathway (an exploratory optimization concept) within the WHO framework, leveraging complementary modalities to enhance accuracy and resource efficiency.
Addressing insufficient specificity to avoid overtreatment. In our cohort, colposcopic VIA/VILI achieved specificity 0.969, substantially higher than HR-HPV (0.307) and TCT (0.713) (Table 2). Its PPV was 0.699, indicating that nearly 70% of VIA/VILI-positive cases were HSIL/CC on histopathology, compared with PPVs of 0.126 (HR-HPV) and 0.205 (TCT) (Table 2). When VIA/VILI was front-loaded as triage, limiting biopsy to VIA/VILI-abnormal cases among HR-HPV-positive women reduced the biopsy rate from 87.38% to 30.05% (Table S4). VIA performed by trained providers maintained high sensitivity for cervical precancer detection among HPV-positive women, achieving a marked decrease in referral rates and improving overall screening efficiency.20 These findings align with the multicenter ESTAMPA study, in which VIA among HR-HPV-positive women achieved 85.9% sensitivity for CIN3+ with 58.6% specificity.20 Additional studies on smartphone-enabled VIA/VILI and AI-assisted interpretation reported comparable diagnostic performance.45,46
Capturing HPV-negative disease to reduce missed cases. Among HPV-negative women, 2.41% (78/3,243) were VIA/VILI-positive, 57.69% (45/78) of whom were true HSIL/CC (Table S6). Even in HPV- and TCT-negative individuals, VIA/VILI can reveal suspicious lesions in symptomatic patients (eg, post-coital bleeding), preventing misses. With the three-modality combination, NPV for CC improved from 0.976 (HR-HPV alone) to 0.999, and NPV for HSIL/CC improved from 0.976 to 0.991 (Tables 2 and 3), substantially lowering the risk of missed actionable disease. For non-16/18 HR-HPV-positive, TCT-negative women, VIA/VILI functioned as an “immediate triage tool” identifying 33.87% of HSIL/CC at the initial visit (Tables S8 and S9) and mitigating progression due to surveillance delays.
Adapting to heterogeneous resource settings. In resource-limited primary care, VIA/VILI can serve as an independent initial screen, offering rapid assessment with simple workflows and minimal consumables while also detecting other lower-genital-tract pathology.21,47 In our cohort, VIA/VILI achieved an NPV of 0.965, consistent with a prospective study reporting NPV 0.933.43 Performance data from Switzerland further support its utility, with naked-eye VIA sensitivity 80.8% and digital VIA sensitivity 92.0%.48 When colposcopic VIA/VILI-positive women are subsequently referred for HPV/TCT confirmation, referral pressure for biopsy can be attenuated while preserving safety.20 In resource-rich settings, the three modalities together support precise evaluation of “HPV-positive/TCT-negative” and “HPV-negative but symptomatic” subgroups, enhancing both efficiency and safety.
Digital infrastructure further enables scale: electronic colposcopes are widely available in Chinese county hospitals, tele-review by experienced specialists can offset variability in operator expertise, and integrated screening-to-follow-up information systems reduce manual burden and improve adherence.19,49 Meta-analytic evidence reporting VIA/VILI sensitivity and specificity for CIN2+ consistent with our performance underscores its utility in resource-constrained environments.45,46
Limitations and Future Directions
This single-center, retrospective cohort has limitations. Participants were drawn from outpatient clinics rather than community screening, introducing potential selection bias that warrants validation in population-based cohorts. Formal cost-effectiveness analyses were not performed, and the long-term economic value of the combined pathway requires prospective evaluation. VIA/VILI performance is operator-dependent, and inter-center variability may affect reproducibility.19 While the use of HSIL/CC as the reference-positive endpoint enhances the clinical relevance of the screening, it may also reduce specificity, particularly when there is a high prevalence of LSIL or other benign abnormalities. This trade-off is inherent in prioritizing the detection of clinically actionable disease, which may result in increased sensitivity at the cost of specificity.
Our future work will focus on: multicenter prospective studies across eastern, central, and western China to test feasibility and cost-effectiveness in community settings, with particular attention to primary-care implementation; the development of standardized operating and interpretation criteria (eg, VIA/VILI acetowhitening extent, morphological features; thresholds for HPV/TCT confirmation) to reduce variability; and AI-assisted colposcopic image analysis to automate detection of suspicious lesions, lessen reliance on operator experience, and support scalable deployment.
Conclusions
Drawing on data from 11,405 Chinese women, we propose a resource-stratified, stepwise combined triage pathway (an exploratory optimization concept). Within the WHO-recommended framework, coordinated use of HR-HPV testing, TCT, and colposcopic VIA/VILI (front-loaded usage) preserves the high sensitivity of HPV screening while leveraging VIA/VILI’s high specificity to optimize triage. The strategy increases detection of HSIL/CC and reduces both overtreatment and missed diagnoses, and can be flexibly deployed according to local resources. Prospective, multicenter studies are now needed to confirm generalizability and long-term value and to inform evidence-based optimization of China’s cervical cancer screening policy.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article and the supplementary information files.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Review Committee for Human-related Scientific Research at Shanghai Jiao Tong University (Approval Number: B20240650I). The research was conducted in accordance with the Declaration of Helsinki and adhered to relevant national and international ethical guidelines for research involving human participants.
Informed Consent Statement
Informed consent was obtained from all individuals who provided clinical information, and their privacy and personal information were rigorously protected in line with ethical guidelines.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by grants from the Fundamental Research Funds for the Central Universities (grant number: KLSB2024KF-06 (ZQZ and JH), and KLSB2022QN-01 (WQH)), the Project of Maternal and Child Health in Jiangsu Province (grant numbers: F202222 (MY)), Initiation program for new teachers of Shanghai Jiao Tong University (grant number: 23X010502168 (WQH)), Medical-Industrial Crossover Research Fund of Shanghai Jiao Tong University (grant numbers: YG2022QN070 (ZQZ and JH)), Science and Technology Innovation Action Plan Startup Project (Sail Special) of Science and Technology Commission of Shanghai (grant number: 22YF1420500 (WQH)).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H. et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Han B, Zheng R, Zeng H, et al. Cancer incidence and mortality in China, 2022. J Natl Cancer Cent. 2024;4(1):47–53. doi:10.1016/j.jncc.2024.01.006
3. Wu S, Jiao J, Yue X, Wang Y. Cervical cancer incidence, mortality, and burden in China: a time-trend analysis and comparison with England and India based on the global burden of disease study 2019. Front Public Health. 2024;12:1358433. doi:10.3389/fpubh.2024.1358433
4. Li ML, Qi JL, Ma YQ, et al. National age-specific mortality trends for cervical and breast cancers in urban-rural areas of China from 2009 to 2021: a population-based analysis. Mil Med Res. 2024;11(1):55. doi:10.1186/s40779-024-00561-4
5. Sundstrom K, Elfstrom KM. Advances in cervical cancer prevention: efficacy, effectiveness, elimination? PLoS Med. 2020;17(1):e1003035. doi:10.1371/journal.pmed.1003035
6. WHO. Global strategy to accelerate the elimination of cervical cancer as a public health problem. 2020. Available from: https://www.who.int/publications/i/item/9789240014107.
7. Das M. WHO launches strategy to accelerate elimination of cervical cancer. Lancet Oncol. 2021;22(1):20–21. doi:10.1016/S1470-2045(20)30729-4
8. Li M, Wei L, Sui L, et al. Guidelines for cervical cancer screening in China. Gynecol Obstet Clin Med. 2023;3(4):189–194. doi:10.1016/j.gocm.2023.10.005
9. Li M, Li J, Li X, et al. Guidelines for cervical cancer screening in China II. Gynecol Obstet Clin Med. 2025;5(2):e000205. doi:10.1136/gocm-2025-000205
10. Yan H, Wang Q, Qiao Y. Cervical cancer prevention in China: where are we now, and what’s next? Cancer Biol Med. 2024;21(3):213–217. doi:10.20892/j.issn.2095-3941.2023.0432
11. Wu Y, Luo J, Ye D, Gao S. Benefits and challenges of cervical cancer screening since the implementation of the ‘two cancer’ screening programme in China: findings from Shangyu, Zhejiang in 2019-23. J Glob Health. 2025;15:04064. doi:10.7189/jogh.15.04064
12. Xue H, Gao H, Zheng J, et al. Use of extended HR-HPV genotyping in improving the triage strategy of 2019 ASCCP recommendations in women with positive HR-HPV diagnosis and simultaneous LSIL cytology results. J Cancer. 2021;12(14):4332–4340. doi:10.7150/jca.55826
13. Li T, Lai Y, Yuan J. The diagnostic accuracy of TCT + HPV-DNA for cervical cancer: systematic review and meta-analysis. Ann Transl Med. 2022;10(14):761. doi:10.21037/atm-22-1732
14. Ma DY, Dong Y, Feng H, Wang TT, Zhao J. Analysis of factors influencing the false-negative diagnosis of cervical/vaginal liquid based cytology. Zhonghua Bing Li Xue Za Zhi. 2020;49(8):806–811. doi:10.3760/cma.j.cn112151-20200106-00013
15. Zhu J, Ge Z, Xia J, et al. Status quo and problem analysis of cervical cancer screening program in China: based on RE-AIM framework. Front Public Health. 2022;10:987787. doi:10.3389/fpubh.2022.987787
16. Xing B, Guo J, Sheng Y, Wu G, Zhao Y. Human papillomavirus-negative cervical cancer: a comprehensive review. Front Oncol. 2020;10:606335. doi:10.3389/fonc.2020.606335
17. Macios A, Nowakowski A, Dommerich S. False negative results in cervical cancer screening-risks, reasons and implications for clinical practice and public health. Diagnostics. 2022;13(1):12. doi:10.3390/diagnostics13010012
18. Rezhake R, Abuduxikuer G, Abudurexiti G, et al. Evaluation of the multiple HPV-based “screen and triage” algorithms in real-world settings of rural China. Cancer Biol Med. 2025;22:1053–1067. doi:10.20892/j.issn.2095-3941.2025.0384
19. Zeufack SCM, Omoto J, Owaya A, et al. Feasibility of incorporating the pocket colposcope into nurse-led cervical cancer screening programs in Western Kenya. Ecancermedicalscience. 2025;19:1925. doi:10.3332/ecancer.2025.1925
20. Baena A, Mesher D, Salgado Y, et al. Performance of visual inspection of the cervix with acetic acid (VIA) for triage of HPV screen-positive women: results from the ESTAMPA study. Int J Cancer. 2023;152(8):1581–1592. doi:10.1002/ijc.34384
21. Egede J, Ajah L, Ibekwe P, et al. Comparison of the accuracy of papanicolaou test cytology, visual inspection with acetic acid, and visual inspection with lugol iodine in screening for cervical neoplasia in Southeast Nigeria. J Glob Oncol. 2018;4:1–9. doi:10.1200/JGO.17.00127
22. IAfRo C. Cervical Cancer Screening. IARC Handbooks of Cancer Prevention. 18. Lyon (FR): IARC; 2022.
23. WHO. WHO Guideline for Screening and Treatment of Cervical Pre-Cancer Lesions for Cervical Cancer Prevention.
24. Perkins RB, Guido RS, Castle PE, et al. ASCCP risk-based management consensus guidelines for abnormal cervical cancer screening tests and cancer precursors. J Low Genit Tract Dis. 2020;24:32.
25. Suba EJ, Ortega RE, Mutch DG. The IARC perspective on cervical cancer screening. N Engl J Med. 2022;386:607.
26. WHO. WHO Guideline for Screening and Treatment of Cervical Pre-Cancer Lesions for Cervical Cancer Prevention. WHO Guidelines Approved by the Guidelines Review Committee.
27. Wu Y, Wang J, et al. Chinese Geriatrics Society. Chinese expert consensus on screening and abnormal management of cervical lesions in elderly women (2023 edition). Chin J Appl Gynecol Obstet. 2023;39:531–536.
28. Tang X, Zhang H, Wang T, et al. Single and multiple high-risk human papillomavirus infections in histopathologically confirmed cervical squamous lesions: incidences, distribution, and associated detection rates for precancerous and cancerous lesions. Lab Invest. 2023;103(11):100234. doi:10.1016/j.labinv.2023.100234
29. Yang X, Qi S, Dai L, Ye Q, Li X. Trends in HPV-positive cervical cancer prevalence: a retrospective study from 2013 to 2020. Virol J. 2025;22(1):199. doi:10.1186/s12985-025-02830-7
30. Liu S, Mei B, Ouyang Y, Li C. Prevalence and genotype distribution of human papillomavirus infection among women in Jingzhou, China: a population-based study of 51,720 women. Virol J. 2023;20(1):297. doi:10.1186/s12985-023-02262-1
31. Mo B, Ye Y, Yu M, et al. Prevalence and genotype distribution of HPV combined with cervical pathological results in women from Sichuan, China: a cross-sectional study based on post-vaccination period 2019 to 2023. Cancer Med. 2024;13(16):e70148. doi:10.1002/cam4.70148
32. Dun C, Yuan M, Zhao X, et al. Clinical evaluation of primary human papillomavirus (HPV) testing with extended HPV genotyping triage for cervical cancer screening: a pooled analysis of individual patient data from nine population-based cervical cancer screening studies from China. Cancer Med. 2024;13(11):e7316. doi:10.1002/cam4.7316
33. Li Y, Wu X. Evaluating HPV E6/E7 mRNA expression and genotype prevalence in cervical cytology and biopsy samples from Yunnan Province, China. Ecancermedicalscience. 2025;19:1893. doi:10.3332/ecancer.2025.1893
34. Berza N, Zodzika J, Kivite-Urtane A, et al. Understanding the high-risk human papillomavirus prevalence and associated factors in the European country with a high incidence of cervical cancer. Eur J Public Health. 2024;34(4):826–832. doi:10.1093/eurpub/ckae075
35. Young AP, Olorunfemi M, Morrison L, et al. Cervical cancer screening: impact of collection technique on human papillomavirus detection and genotyping. Preventive Medicine Reports. 2025;50:102971. doi:10.1016/j.pmedr.2025.102971
36. Fei C, Zhixue Y, Long S, et al. Chinese Expert consensus on colposcopy application. Chin J Obstet Gynecol. 2020;55:443–449.
37. Burdier FR, Waheed DE, Nedjai B, et al. DNA methylation as a triage tool for cervical cancer screening - A meeting report. Prev Med Rep. 2024;41:102678. doi:10.1016/j.pmedr.2024.102678
38. Schreiberhuber L, Barrett JE, Wang J, et al. Cervical cancer screening using DNA methylation triage in a real-world population. Nat Med. 2024;30(8):2251–2257. doi:10.1038/s41591-024-03014-6
39. Xia C, Qiao Y, Zhang Y, Zhao F. WHO global strategy for the elimination of cervical cancer and the challenges and countermeasures faced by China. Chin J Med. 2020;100:3484–3488.
40. Qiu L, Chen F, Weidong Z, et al. White paper on screening and early accurate diagnosis of cervical cancer in 2024. Chin J Pracl Gynecol Obstet. 2024;40:85–95.
41. Aker SS, Agar E, Tinelli A, Hatirnaz S, Ortac F. The impact of HPV diagnosis and abnormal cervical cytology results on sexual dysfunction and anxiety. Int J Environ Res Public Health. 2023;20(4):3630. doi:10.3390/ijerph20043630
42. Marlow LAV, McBride E, Ridout D, et al. Patterns of anxiety and distress over 12 months following participation in HPV primary screening. Sex Transm Infect. 2022;98(4):255–261. doi:10.1136/sextrans-2020-054780
43. Petignat P, Kenfack B, Wisniak A, et al. ABCD criteria to improve visual inspection with acetic acid (VIA) triage in HPV-positive women: a prospective study of diagnostic accuracy. BMJ Open. 2022;12(4):e052504. doi:10.1136/bmjopen-2021-052504
44. Liang LA, Zeissig SR, Schauberger G, et al. Colposcopy non-attendance following an abnormal cervical cancer screening result: a prospective population-based cohort study. BMC Womens Health. 2022;22(1):285. doi:10.1186/s12905-022-01851-6
45. Allanson ER, Phoolcharoen N, Salcedo MP, Fellman B, Schmeler KM. Accuracy of smartphone images of the cervix after acetic acid application for diagnosing cervical intraepithelial neoplasia grade 2 or greater in women with positive cervical screening: a systematic review and meta-analysis. JCO Glob Oncol. 2021;7(7):1711–1721. doi:10.1200/GO.21.00168
46. Poli UR, Gudlavalleti AG, Bharadwaj YJ, et al. Development and clinical validation of visual inspection with acetic acid application-artificial intelligence tool using cervical images in screen-and-treat visual screening for cervical cancer in south India: a pilot study. JCO Glob Oncol. 2024;10(10):e2400146. doi:10.1200/GO.24.00146
47. Asgary R, Beideck E, Naderi R. Comparative assessment of test characteristics of cervical cancer screening methods for implementation in low-resource settings. Prev Med. 2022;154:106883. doi:10.1016/j.ypmed.2021.106883
48. Dufeil E, Kenfack B, Tincho E, et al. Addition of digital VIA/VILI to conventional naked-eye examination for triage of HPV-positive women: a study conducted in a low-resource setting. PLoS One. 2022;17(5):e0268015. doi:10.1371/journal.pone.0268015
49. Huang J, Geng J. Expert consensus on integration program for cervical cancer screening and management measures for abnormal population. J Med Postgra. 2020;33:230–233.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.