Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 10
Insulin glargine 300 U/mL for basal insulin therapy in type 1 and type 2 diabetes mellitus
Authors Lau IT ![]() , Lee KF, So WY, Tan K, Yeung VTF
, Lee KF, So WY, Tan K, Yeung VTF
Received 30 December 2016
Accepted for publication 20 April 2017
Published 30 June 2017 Volume 2017:10 Pages 273—284
DOI https://doi.org/10.2147/DMSO.S131358
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ming-Hui Zou
Ip Tim Lau,1 Ka Fai Lee,2 Wing Yee So,3 Kathryn Tan,4 Vincent Tok Fai Yeung5
1Department of Medicine, Tseung Kwan O Hospital, 2Department of Medicine and Geriatrics, Kwong Wah Hospital, 3Department of Medicine and Therapeutics, Chinese University of Hong Kong, Prince of Wales Hospital, 4Department of Medicine, Queen Mary Hospital, University of Hong Kong, 5Department of Medicine and Geriatrics, Our Lady of Maryknoll Hospital, Hong Kong, China
Objective: To review published clinical studies on the efficacy and safety of new insulin glargine 300 units/mL (Gla-300), a new long-acting insulin analog, for the treatment of type 1 and type 2 diabetes mellitus (T1DM, T2DM)
Materials and methods: Data sources comprised primary research articles on Gla-300, including pharmacodynamic, pharmacokinetic, and clinical studies.
Results: In pharmacodynamic and pharmacokinetic studies, Gla-300 showed a flatter time–action profile and longer duration of action than Gla-100. Noninferiority of Gla-300 versus Gla-100 for lowering of glycated hemoglobin was demonstrated in Phase III clinical studies covering a range of T1DM and T2DM patient populations. Over 6–12 months of follow-up, Gla-300 consistently showed comparable glycemic efficacy with less hypoglycemia vs Gla-100, even during the first 8 weeks of treatment. Although titrated insulin doses were 11%–17% higher with Gla-300 vs Gla-100, changes in body weight were similar or favored Gla-300.
Conclusion: Clinical studies provide evidence that the pharmacodynamic and pharmacokinetic properties of Gla-300 may translate into clinical benefits in both T1DM and T2DM. Gla-300 may provide a new option for people initiating basal insulin, those requiring higher basal insulin doses, those with T1DM, and those who may be at increased risk for hypoglycemia, such as people with chronic kidney disease, the elderly, and those with cardiovascular comorbidities.
Keywords: diabetes mellitus, long-acting insulin, insulin glargine
Introduction
Persistent uncontrolled hyperglycemia is associated with a host of long-term complications, such as cardiovascular (CV) or cerebrovascular disease, nerve damage, renal failure, or vision loss.1–4 Insulin is considered the most effective glucose-lowering therapy available, and is required by people with type 1 diabetes mellitus (T1DM) to control their blood glucose (BG) levels. Many people with T2DM will also eventually require insulin therapy, due to the progressive nature of the disease. Recognizing this, international diabetes-management guidelines recommend that insulin therapy be initiated in people with T2DM uncontrolled on oral antidiabetics (OADs).5,6 However, patients’ and physicians’ concerns about hypoglycemia, pain associated with needles and injections, weight gain, lifestyle impact, and financial cost to patients all contribute to delays in initiating and titrating insulin, or to discontinuation of treatment.7–9
In people with T2DM uncontrolled on OADs, insulin therapy may be initiated with basal insulins.5,6 Used alone, in combination with OADs, or as a component of basal–bolus insulin regimens, basal insulins are designed to provide a steady supply of insulin to meet the body’s baseline (nonmeal) insulin needs throughout the day and night. Delivery is in the form of once- or twice-daily injections at the same time each day. A variety of intermediate- and long-acting insulins are currently used for basal insulin therapy; their characteristics are summarized in Table 1. To mimic normal physiological patterns of basal insulin secretion, the “ideal” basal insulin would have a long duration of action,10 providing adequate control of fasting BG with a single injection per day. Importantly, it would carry a low risk of hypoglycemia, with a peakless or “flat” time–action profile and minimal day-to-day variability.10 Although more costly, long-acting analogs, such as insulin glargine and insulin detemir (Table 1), are preferred to the intermediate-acting neutral protamine Hagedorn (NPH) insulin, as they exhibit lower variability in absorption. Clinically, this translates into more predictable glucose-lowering activity and less nocturnal hypoglycemia than with NPH.11–14
 | Table 1 Characteristics of basal insulins Notes: aVaries depending on dose; b100 U/mL and 200 U/mL formulations of insulin degludec were demonstrated to be bioequivalent in terms of peak serum concentration achieved and area under the curve for blood concentration versus time.62 |
Insulin glargine 100 U/mL (Gla-100; Lantus®; Sanofi-Aventis US, LLC, Bridgewater, NJ, USA) has a well-understood mode of action, and its efficacy and safety profile are well established.15,16 Gla is created by substituting glycine for asparagine 21 in the A chain and adding two arginines to the C terminus of the B chain. The resulting protein, 21A-Gly31B-Arg32B-Arg-insulin, is stable and soluble in acid solution, but forms microprecipitates at physiological pH (7.4). Gla forms a subcutaneous depot at the injection site, from which it is slowly released. This gradual release results in an extended duration of action, with a less pronounced activity peak than older intermediate-acting insulins, such as NPH.17 While Gla-100 and other long-acting analogs represent an improvement over NPH in terms of hypoglycemia, a proportion of people treated with long-acting insulins still experience hypoglycemic episodes.18,19
As the most common and potentially most serious adverse effect of insulin treatment, hypoglycemia remains a key unmet medical need in insulin-treated diabetes. Insulin-related hypoglycemia and insulin-use errors accounted for nearly one in ten emergency department (ED) visits for adverse drug events in the US over a 5-year period.20 Certain groups of people with diabetes, notably the elderly20–22 and those with renal impairment,22–24 are at increased risk of hypoglycemia and require careful management on basal insulin therapy.
The new Gla-300 formulation (Toujeo®; Sanofi-Aventis US) was developed to have a flatter and more extended time–action profile than Gla-100. These characteristics may translate into more stable and sustained glycemic control over a 24-hour dosing interval. As of early 2016, Gla-300 has been approved for treatment of T1DM and T2DM in adults within Europe, the US, and major regions, including Japan and Australia. Gla-300 is undergoing regulatory review in a number of Asia-Pacific countries/territories. We reviewed published studies of Gla-300 to assess its potential place in diabetes therapy.
Materials and methods
Medline-indexed publications on Gla-300 were retrieved using the search terms “Gla-300”, “insulin glargine 300 units/mL”, “insulin glargine U300”, and “glargine U300”. We included English-language publications that reported primary research on Gla-300. We also identified conference presentations on Gla-300 from the 2014 and 2015 American Diabetes Association and European Association for the Study of Diabetes annual meetings. Six Phase IIIA clinical studies – four pharmacokinetic/pharmacodynamic studies, one patient-level meta-analysis, and one pilot study – were identified. Of 14 Gla-300 studies registered in the ClinicalTrials.gov database in June 2016, nine had been completed and five were ongoing or recruiting participants.
Results
Pharmacokinetics and pharmacodynamics
As the Gla molecule is the same in both formulations, Gla-300 has the same metabolism as Gla-100.25 However, the Gla-300 formulation delivers the same amount of insulin as Gla-100 in a third of the injection volume. This produces a smaller subcutaneous depot with reduced surface area, resulting in more prolonged and constant release of insulin into the bloodstream.26
Glucose-clamp studies in people with T1DM showed that a steady state is reached within 3–4 days of once-daily Gla-300 administration at clinically relevant doses.26 The half-life of Gla-300 at a steady state is approximately 19 hours.26,27 With Gla-100, steady state is reached after 2–4 days of once-daily administration, with a half-life of 12 hours.28 Under steady-state conditions, Gla-300 shows a flatter profile (Figure 1) and longer duration of action than Gla-100.26 Plasma insulin-concentration and glucose infusion-rate profiles show lower maxima and are more evenly distributed over a 24-hour interval after dosing with Gla-300 vs Gla-100.26 Tight BG control (≤105 mg/dL, 5.8 mmol/L) was maintained for approximately 5 hours longer on 0.4 U/kg/day Gla-300 (median time of 30 hours) vs 0.4 U/kg/day Gla-100.26 In participants with T1DM, Gla-300 shows within- and between-day variability in exposure at a steady state;27 the glucose-lowering effect of Gla-300 is more evenly distributed across the 24-hour dosing interval than that of Gla-100.27 Similarly, an exploratory continuous glucose-monitoring study reported lower within- and between-day variability with Gla-300 vs Gla-100, although these differences did not reach statistical significance.29
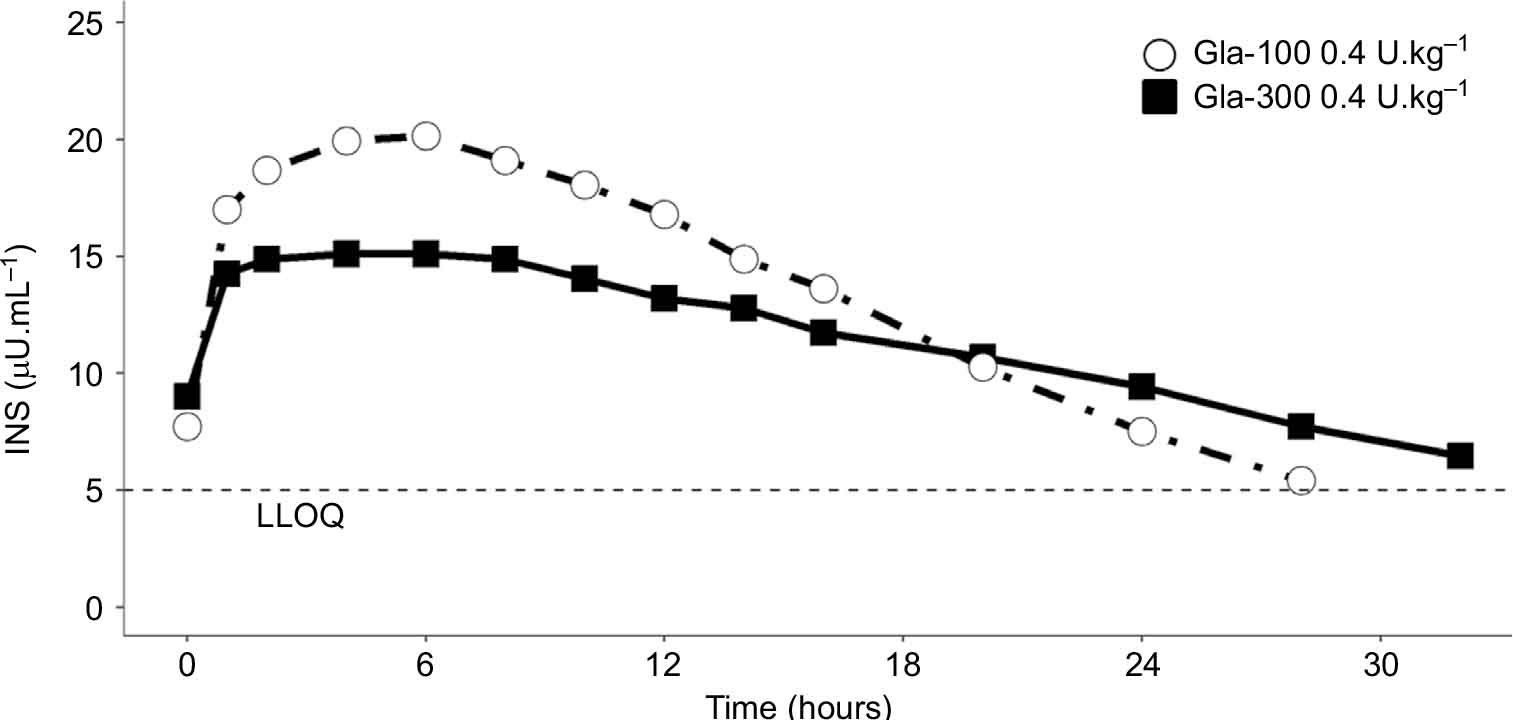 | Figure 1 Profile of mean plasma insulin (INS) in a cohort of patients with type I diabetes mellitus after multiple doses of Gla-300 or Gla-100 in steady-state. Notes: Published previously in Becker et al, Diabetes Care, American Diabetes Association, 2015. Copyright and all rights reserved. Material from this publication has been used with the permission of American Diabetes Association.26 Abbreviations: Gla-100, insulin glargine 100 U/mL; Gla-300, insulin glargine 300 U/mL; INS, insulin; LLOQ, lower limit of quantitation. |
Results from multiple-dose studies were consistent with other single-dose studies performed in people with T1DM. In Japanese and European individuals with T1DM who were given single doses of Gla-300 or Gla-100, a more constant and prolonged exposure profile was seen with Gla-300 vs Gla-100. In the Japanese cohort, glucose-lowering activity was detectable for up to 36 hours with Gla-300.30
Efficacy and safety of Gla-300 in randomized controlled studies
The efficacy and safety of once-daily Gla-300 for glycemic control was investigated in the EDITION series of multicenter randomized open-label active-control Phase IIIA studies.31–36 These included a total of 792 participants with T1DM and 2,737 participants with T2DM (Table 2). Four were global studies,31,32,34,36 with two smaller studies conducted in Japanese populations.33,35 The EDITION trials were treat-to-target studies that aimed to assess the efficacy and safety of Gla-300 vs Gla-100, and thereby address whether comparable glycemic control could be achieved with Gla-300 vs Gla-100 without increased hypoglycemia.
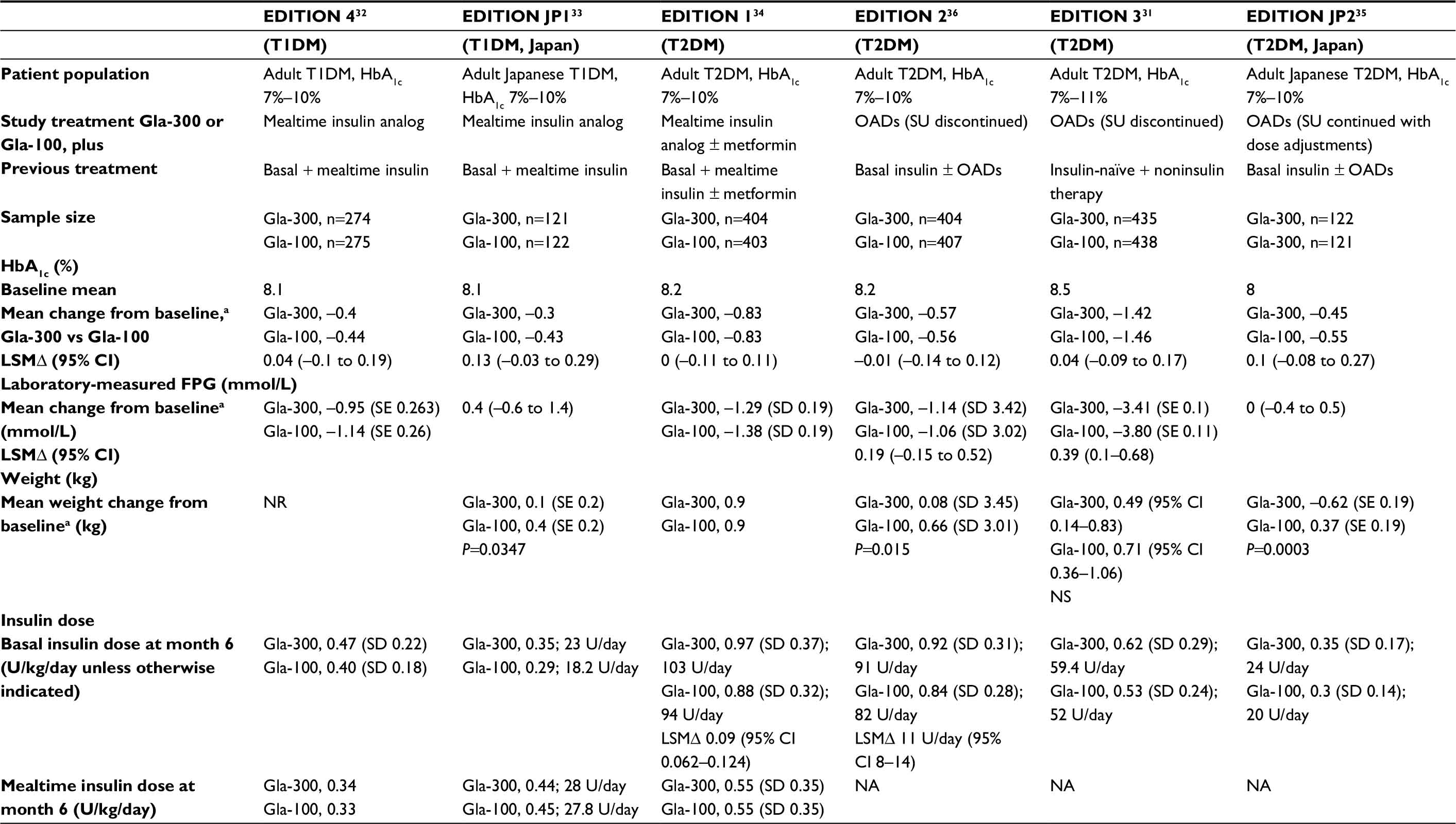 | Table 2 Efficacy of insulin glargine 300 U/mL (Gla-300) in clinical studies Notes: aLSMΔ at month 6 or last observation on treatment (last observation carried forward). Abbreviations: T1DM, type 1 diabetes mellitus; HbA1c, glycated hemoglobin; LSMΔ, least-squares mean difference; CI, confidence interval; SD, standard deviation; SE, standard error; FPG, fasting plasma glucose; OADs, oral antidiabetic drugs; NR, not reported; NA, not applicable; Gla-300, insulin glargine 300 U/mL; Gla-100, insulin glargine 100 U/mL; T2DM, type 2 diabetes mellitus; SU, sulfonylurea. |
EDITION 432 and JP133 compared once-daily Gla-300 with Gla-100 in participants with T1DM on basal plus mealtime insulin. EDITION 1, 2, and 3 and JP2 compared once-daily Gla-300 with Gla-100 in participants with T2DM with the following treatment backgrounds:
- basal plus mealtime insulin, with or without metformin (EDITION 1)34
- basal insulin plus OADs (EDITION 2)36
- insulin-naïve, uncontrolled on OAD therapies (EDITION 3)31
- basal insulin plus OADs (EDITION JP2).35
All six studies were treat-to-target noninferiority trials of 6 months’ duration (up to 26 weeks), with planned 6-month extension phases. As of June 2016, 12-month data had been published in full for two of these studies: EDITION 1 and 2.37,38
Owing to differences in the Gla-300 and Gla-100 injection devices, all were open-label studies. In EDITION 1, 2, and 3, the study drug (Gla-300 or Gla-100) was administered once daily in the evening (predinner to bedtime) at the same time of day for each patient. In EDITION 4, the study drug was administered once daily, either in the morning (prebreakfast to prelunch period) or in the evening. Starting basal insulin doses in EDITION 1 and 2 were equivalent to the participant’s previous total daily dose for those on once-daily glargine or 80% of the total daily dose of previously twice-daily NPH.
The EDITION studies all used a treat-to-target algorithm for basal insulin titration. Basal insulin dose adjustments were performed weekly in EDITION 1. In EDITION 2, 3, and 4, doses could be adjusted more frequently, but not more than every three days. Doses were adjusted to achieve fasting (prebreakfast) self-measured plasma glucose (SMPG) values in the target range of 80–100 mg/dL (4.4–5.6 mmol/L) in EDITION 1, 2, and 3 and JP2, and 80–130 mg/dL (4.4–7.2 mmol/L) for EDITION 4 and JP1, based on the median of the preceding 3 measurements. In EDITION 1, 2, and 3, basal insulin dose was increased by 3 U if SMPG readings were >5.6 and <7.8 mmol/L and by 6 U if ≥7.8 mmol/L; the dose was decreased by 3 U if SMPG readings were <4.4 mmol/L or at the investigator’s discretion. Smaller minimum-dose steps were permitted in EDITION 4, EDITION JP1, and EDITION JP2 (1.5 U for Gla-300 and 1 U for Gla-100) for the respective SMPG-target ranges.
The primary end point was change in glycated hemoglobin (HbA1c) from baseline to month 6 or to the last visit on treatment (last observation carried forward). For EDITION 1, 2, and 3, the main secondary end point was the percentage of participants with one or more confirmed nocturnal (≤3.9 mmol/L) or severe hypoglycemic events from week 9 to month 6 (defined in the “Hypoglycemia in type 1 and type 2 diabetes” section). Other parameters, such as weight change, insulin dose, and adverse events (AEs) were also assessed. The trials were designed to demonstrate noninferiority of Gla-300 vs Gla-100 for the primary end point (change in HbA1c) from baseline to month 6. Noninferiority was demonstrated if the upper bound of the two-sided 95% confidence interval (CI) of the least-squares (LS) mean difference was less than the predefined noninferiority margin (0.4% HbA1c).
Glycemic control in type 1 diabetes
The EDITION 4 trial (NCT01683266) included 549 adults with T1DM on basal insulin (≥42 units/day of NPH or Gla-100) plus mealtime insulin.32 Individuals using premixed insulins, human regular insulin as mealtime insulin, and/or any glucose-lowering drugs other than basal insulin and mealtime insulin analogs were excluded. At baseline, mean HbA1c was 8.1%, mean body mass index (BMI) was 27.6 kg/m2, and average T1DM duration was 21 years. Participants were randomized in a 1:1:1:1 ratio to Gla-300 or Gla-100, injected in the morning or evening. All groups continued their use of mealtime insulin analogs.
EDITION JP1 (NCT01689129) included 243 Japanese adults with T1DM on basal plus mealtime insulin.33 Inclusion and exclusion criteria were similar to those in the EDITION 4 study. At baseline, mean HbA1c was 8.1% and average T1DM duration 13 years. Participants were randomized to once-daily Gla-300 or Gla-100 while continuing mealtime insulin analogs.
In both EDITION 1 and EDITION JP1, mean HbA1c reductions from baseline to month 6 were similar in the Gla-300 and Gla-100 groups, with no significant between-group differences (Table 2).32,33 In EDITION 4, no effect of injection timing (morning vs evening) was seen in terms of HbA1c or fasting plasma glucose (FPG) reductions on Gla-300 vs Gla-100 treatment.32 At month 6, mean daily basal insulin dose was slightly higher with Gla-300 than with Gla-100 (0.45 U/kg/day vs 0.36 U/kg/day, respectively) in the evening injection group (Table 2).32 Overall, daily doses of mealtime insulin were similar in the two groups. At month 6, the mean daily mealtime dose was 0.34 U/kg/day in the Gla-300 group (morning injection 0.33 U/kg/day, evening injection 0.34 U/kg/day) and 0.33 U/kg/day in the Gla-100 group (morning 0.32 U/kg/day, evening 0.34 U/kg/day).32
In EDITION JP1, the mean daily basal insulin dose at month 6 was higher with Gla-300 (0.35 U/kg/day, 23 U/day) than with Gla-100 (0.29 U/kg/day, 18.2 U/day). Mealtime insulin doses were similar in the two groups at month 6 (Gla-300, 0.44 U/kg/day [23 U/day] vs Gla-100, 0.45 U/kg/day [27.8 U/day]; Table 2).33 Over 90% of participants in both groups completed the 6-month extension phase of EDITION JP1. HbA1c reductions were maintained in both groups over 12 months, with little change in basal insulin dose from months 6 to 12 (0.36 U/kg/day [24 U/day] for Gla-300, 0.28 U/kg/day [18 U/day] for Gla-100 at month 12). Daily mealtime insulin doses were comparable in the two groups at month 12.39
Glycemic control in type 2 diabetes
The EDITION 1 trial (NCT01499082) included 807 adults with T2DM on basal insulin (≥42 units/day NPH or Gla-100) plus mealtime insulin (insulin aspart, lispro or glulisine) with or without metformin for ≥1 years. Individuals using mealtime insulins, premixed insulins, or basal insulins other than NPH or Gla-100 were excluded. At baseline, the mean HbA1c was 8.2%, mean BMI 36.6 kg/m2, and average diabetes duration 16 years.
At month 6, mean reductions in HbA1c were similar in the Gla-300 (n=404) and Gla-100 (n=403) groups (0.83% in both groups; Table 2).34 Body weight was slightly increased (0.9 kg in both groups). Daily basal insulin dosage increased in both groups over 6 months of treatment (Table 2). Doses at month 6 were higher with Gla-300 than with Gla-100 (mean daily dose 0.97 U/kg/day [103 U/day] vs 0.88 U/kg/day [94 U/day]). Nearly 90% of participants in both groups completed the 6-month open-label extension phase. After 12 months of treatment, the Gla-300 group showed a slightly larger reduction in HbA1c (Gla-300 0.86% vs Gla-100 0.69%) (Table 2).37
EDITION 2 (NCT01499095) included 811 adults with T2DM on basal insulin (≥42 units/day NPH or Gla-100) plus OADs for ≥6 months. Individuals on premixed insulins or basal insulins other than NPH or Gla-100 were excluded. Over 90% of participants were on prior metformin, and <5% had used sulfonylureas. Participants discontinued sulfonylureas, but continued other OADs at prestudy doses. At baseline, the mean HbA1c was 8.24%, mean BMI 34.8 kg/m2, and average diabetes duration 13 years.
After 6 months, LS mean change in HbA1c was similar in the two groups (Gla-300 –0.57% vs Gla-100 –0.56%; Table 2).36 There were no significant between-treatment differences for either HbA1c or FPG. Body weight increased in both groups, although significantly less weight gain occurred with Gla-300 vs Gla-100 (LS mean difference 0.08 kg vs 0.66 kg, P=0.015) (Table 2). At month 6, the mean daily basal insulin dose was higher with Gla-300 than with Gla-100 (0.92 U/kg/day vs 0.84 U/kg/day, corresponding to 91 U/day vs 82 U/day). Approximately 80% of participants in both groups completed the 6-month extension phase. HbA1c reductions were maintained at 12 months without significant between-treatment differences (LS mean change at month 12, –0.55% for Gla-300, –0.5% for Gla-100).38 Mean body-weight increase at 12 months was lower with Gla-300 than with Gla-100 (0.4 kg vs 1.2 kg).38
The EDITION 3 trial (NCT01676220) included insulin-naïve adults with T2DM who had been uncontrolled on noninsulin therapies for ≥6 months. Most participants (91.3%) had previously used metformin, 58.8% had used sulfonylureas, and 21.6% had used DPP4 inhibitors. On randomization to Gla-300 or Gla-100, participants discontinued sulfonylureas and glinides, but continued other prior therapies at prestudy doses. At baseline, mean HbA1c was 8.5%, mean BMI 33 kg/m2, and average diabetes duration 9.8 years.
At month 6, both groups showed moderate reductions in HbA1c (Gla-300 1.42%, Gla-100 1.46%, Table 2).31 FPG decreased slightly more in the Gla-100 than in the Gla-300 group, while weight gain was lower with Gla-300 than with Gla-100, although the difference was not statistically significant (Table 2). In both groups, basal insulin dose increased over the 6-month treatment period, though more so in the Gla-300 group (mean dose at month 6, 0.62 vs 0.53 U/kg/day, corresponding to 59.4 U/day vs 52 U/day) (Table 2).
The three global T2DM studies (EDITION 1–3) employed similar study designs and end points, permitting a patient-level meta-analysis of 6-month data to be performed on the combined population of almost 2,500 participants. Consistent treatment effects across the studies indicated the appropriateness of a pooled analysis of all three studies. This pooled analysis confirmed the noninferiority of Gla-300 vs Gla-100 in the combined T2DM population (Gla-300, n=1,247; Gla-100, n=1,249).40 The LS mean change in HbA1c was –1.02% in both groups, with over a third of participants in both groups achieving target HbA1c (<7%) at 6 months (36.2% with Gla-300 vs 35.5% with Gla-100). Participants on Gla-300 achieved comparable glycemic control to those on Gla-100, without increased risk of hypoglycemia. In the combined population, less weight gain occurred with Gla-300 vs Gla-100 (LS mean change of 0.51 kg and 0.79 kg, respectively), and this difference was statistically significant (LS mean difference –0.28, 95% CI –0.55 to –0.01; P=0.039). At 12 months, more sustained HbA1c reduction was achieved with Gla-300 vs Gla-100, without increased risk of nocturnal or anytime hypoglycemia. LS mean change from baseline in HbA1c was –0.91% for Gla-300 and –0.8% for Gla-100, and LS mean difference between groups was –0.1 (95% CI –0.18 to –0.02) (P=0.0174) in favor of Gla-300.41
EDITION JP2 (NCT01689142) included 241 Japanese adults with T2DM on basal insulin plus OADs for ≥6 months.35 Participants were randomized to once-daily Gla-300 or Gla-100 while continuing OADs, including sulfonylureas. At baseline, mean HbA1c was 8%, mean BMI 25.3 kg/m2, and average diabetes duration 14 years. LS mean HbA1c reduction was similar in the two groups (Gla-300 0.45%, Gla-100 0.55%), without a significant between-treatment difference (Table 2).35 Mean daily basal insulin doses at month 6 were higher with Gla-300 than with Gla-100 (0.35 U/kg/day vs 0.30 U/kg/day, corresponding to 24 U/day vs 20 U/day). Most of the participants in both groups (Gla-300, 88.4%; Gla-100, 95.8%) completed the 6-month extension phase of EDITION JP2. From baseline to month 12, HbA1c reductions were comparable in the Gla-300 and Gla-100 groups (mean change in HbA1c –0.28% and –0.33%, respectively).42
Hypoglycemia in type 1 and type 2 diabetes
Another major objective of the EDITION studies was to address whether glycemic control could be achieved without increased hypoglycemia. All potential hypoglycemic events were recorded, whether or not they were confirmed by SMPG and whether symptomatic or asymptomatic. Hypoglycemia was categorized according to American Diabetes Association definitions:43
- “documented symptomatic hypoglycemia”: symptomatic events with SMPG ≤3.9 mmol/L (≤70 mg/dL)
- “severe hypoglycemia”: events that required assistance by another person to administer carbohydrate, glucagon, or other therapy.
“Confirmed (≤3.9 mmol/L) or severe hypoglycemia” included documented symptomatic or asymptomatic hypoglycemia and severe events. Hypoglycemic events were categorized by time of day [nocturnal (12–5:59 am) or any time of day (24 hours)], and by study period (baseline to week 8, week 9 to month 6, baseline to month 6).
Hypoglycemia measures included the percentage of participants with one or more events and event rates per participant-year of exposure. The main hypoglycemia measure in EDITION 1–3 was the percentage of participants with one or more confirmed (≤3.9 mmol/L) or severe nocturnal hypoglycemic events from week 9 to month 6.
EDITION 1 and 2 included participants requiring high basal insulin doses (mean dose approximately 80–100 U/day; Table 2). In both of these studies, a lower proportion of participants on Gla-300 vs Gla-100 had confirmed (≤3.9 mmol/L) or severe nocturnal hypoglycemia from week 9 to month 6, with relative risk (RR) reductions of over 20% with Gla-300 in both studies (Table 3).34,36 Risk reductions were also observed for nocturnal and anytime (24-hour) hypoglycemia from baseline to week 8 and for the overall 6-month treatment period (Table 3). In EDITION 3 (insulin-naïve participants), the percentage of participants with one or more confirmed nocturnal (≤3.9 mmol/L) or severe hypoglycemic events from week 9 to month 6 was similar in the Gla-300 and Gla-100 groups (Table 3). Over the 6-month treatment period, fewer participants on Gla-300 vs Gla-100 experienced one or more confirmed nocturnal (≤3.9 mmol/L) or severe hypoglycemic events (Table 3).
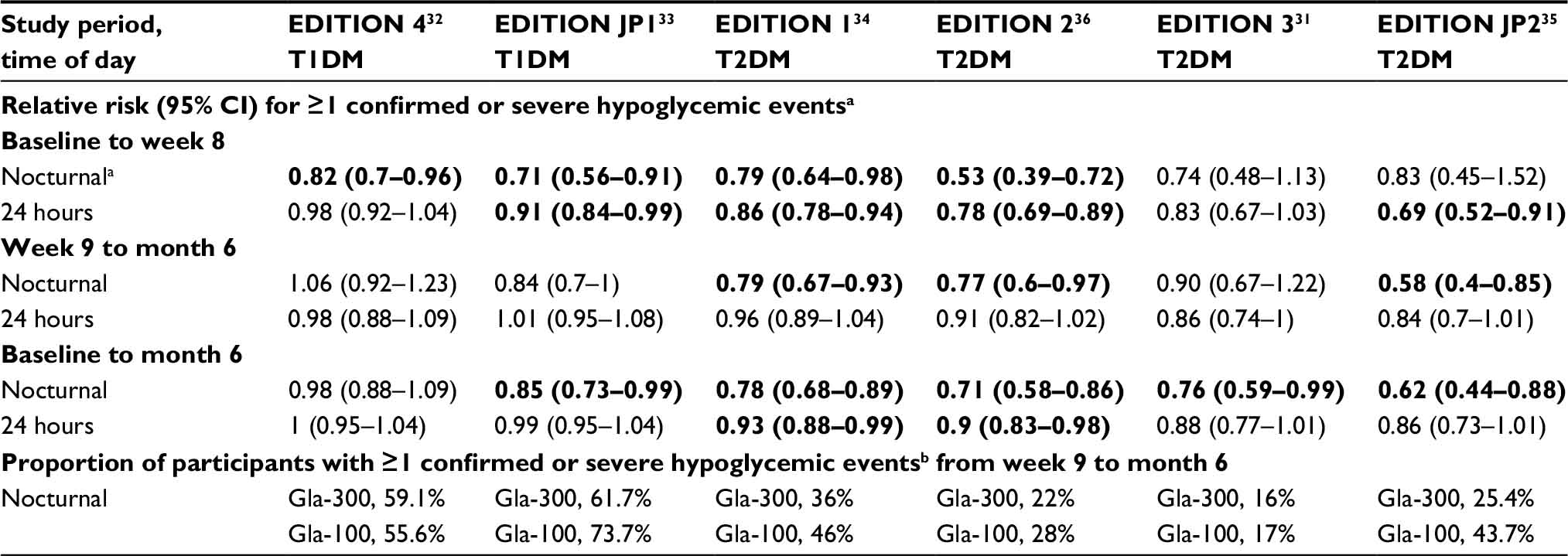 | Table 3 Confirmed (≤3.9 mmol/L, ≤70 mg/dL) or severe hypoglycemia Notes: a12–05:59 am; bconfirmed (≤3.9 mmol/L [≤70 mg/dL]) or severe hypoglycemic events. Severe hypoglycemic events were those requiring assistance by another person to administer carbohydrate, glucagon, or other therapy. Results reported are for the safety population in each trial. Numbers in bold represent statistically significant between-group differences in relative risk for the stated portion of the study period and time of day. Abbreviations: T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus; CI, confidence interval; Gla-300, insulin glargine 300 U/mL. |
Consistent with the trends seen in the individual EDITION 1–3 studies, the patient-level meta-analysis showed reductions in hypoglycemia favoring Gla-300. From baseline to month 6, a lower proportion of participants on Gla-300 vs Gla-100 had one or more confirmed (≤3.9 mmol/L) or severe hypoglycemic events at any time of day (66% vs 72%, RR 0.91, 95% CI 0.87–0.96) and at night (30% vs 40%, RR 0.75, 95% CI 0.68–0.83). Annualized rates of confirmed (≤3.9 mmol/L) or severe hypoglycemia were also lower on Gla-300 vs Gla-100. Over 6 months, this corresponded to a 31% difference in rate ratio for nocturnal hypoglycemia and a 14% difference for anytime (24-hour) hypoglycemia.40 The reduction in hypoglycemia rates was apparent even in the first 8 weeks (relative reduction of 23%), the initiation phase, when insulin doses would have increased the most. The authors noted also that Gla-300 provided control with less hypoglycemia through the morning and up to the early afternoon (2 pm), beyond the prespecified nocturnal period (12–5:59 am). They suggested that this might provide benefits in terms of reduced impact of hypoglycemia on daytime activities.
In Japanese participants with T2DM (EDITION JP2), a lower proportion of participants on Gla-300 vs Gla-100 reported confirmed (≤3.9 mmol/L) or severe hypoglycemic events at any time, even during the first 8 weeks (Table 3). From week 9 to month 6, the risk of confirmed nocturnal (≤3.9 mmol/L) or severe hypoglycemia was significantly lower on Gla-300 vs Gla-100 treatment (Table 3).35 The between-group difference in nocturnal hypoglycemia risk was maintained up to the end of the open-label extension period (RR 0.73 for Gla-300 vs Gla-100 for the whole 12-month study period).42
In the EDITION 4 study (T1DM), participants were randomized in a 1:1:1:1 ratio to Gla-300 or Gla-100, injected either in the morning or in the evening. This design allowed the feasibility of morning injections to be assessed. Overall, the confirmed (≤3.9 mmol/L) nocturnal hypoglycemia rate was lower with Gla-300 vs Gla-100 over the first 8 weeks; there was no significant between-treatment difference from week 9 to month 6 (Table 3).32 Confirmed (≤3.9 mmol/l) or severe 24-hour hypoglycemia was similar in the two groups from week 9 to month 6 and for the overall 6-month period, regardless of injection timing (Table 3).
In EDITION JP1, hypoglycemia rates from week 9 to month 6 were comparable in the Gla-300 and Gla-100 groups (Table 3). As observed in the global study (EDITION 4), risk of confirmed nocturnal (≤3.9 mmol/l) or severe hypoglycemia was significantly lower with Gla-300 vs Gla-100 during the first 8 weeks, and was similar in the two groups from week 9 to month 6 (Table 3).33 Over the full 6-month period, a significantly lower proportion of participants on Gla-300 vs Gla-100 had confirmed nocturnal (≤3.9 mmol/L) or severe hypoglycemia. Results from separate analyses applying the stricter threshold of <3 mmol/L (<54 mg/dL) were consistent with those for the 3.9 mmol/L cutoff: fewer participants experienced one or more confirmed (≤3.9 mmol/L) or severe hypoglycemic events on Gla-300 vs Gla-100 in both EDITION 4 and JP1.32,33
Other treatment-emergent adverse events
Other than hypoglycemia, the most common treatment-emergent AEs reported in the EDITION studies were infections, gastrointestinal system disorders, and musculoskeletal disorders.31–36 Across the EDITION studies, injection-site reactions were reported by ≤4% (0.7%–4%) of participants receiving Gla-300 and ≤5% (0.8%–5%) of participants receiving Gla-100.31–36 Safety profiles in the two groups were comparable, with no evidence of between-treatment differences in AEs.31–36 Gla-300 was well tolerated, with <2% of all trial participants discontinuing treatment due to treatment-emergent AEs, similar to that for the Gla-100 group.
Dosing and delivery
Gla-300 is administered using a disposable prefilled injection device, an optimized SoloStar pen calibrated to deliver Gla-300 in an appropriate volume (a third of that required for Gla-100).28,44 The pen delivers a maximum dose of 80 units per injection.
For people switching to once-daily Gla-300 from once-daily basal insulins, Gla-300 may be initiated at the same unit-for-unit dose.44 Those switching from Gla-100 to Gla-300 may subsequently require dose adjustments to achieve their glycemic targets, since the two formulations are not equivalent. In trials, titrated doses were 11%–15% higher on average with Gla-300 vs Gla-100 in participants with T2DM, and 17.5% higher in participants with T1DM. The higher doses are thought to reflect the lower bioavailability of Gla-300 resulting from increased residence time in the subcutaneous depot.34,36 For people switching to Gla-300 from twice-daily basal insulin, the recommended starting dose of Gla-300 is 80% of the previous total daily dose of basal insulin.44 Changes in basal insulin dose may be needed, along with adjustment of concomitant glucose-lowering therapy. Close monitoring of BG levels is advisable during and after changes in therapy.
Like Gla-100, Gla-300 is recommended for administration once daily at the same time each day.28,44 However, with Gla-300, the extended duration of action may allow some flexibility in dosing time. The potential for flexible vs fixed dosing was explored in two follow-on substudies of EDITION 1 and EDITION 2, each lasting 3 months.45 Participants receiving Gla-300 in EDITION 1 (n=109) and EDITION 2 (n=89) were randomized at month 6 to continue a fixed (24-hour interval) dosing regimen or switch to a flexible regimen that allowed between-injection intervals of 24±3 hours on at least 2 days a week. After 3 months, changes in HbA1c and FPG were similar in the flexible- and fixed-regimen groups, with comparable percentages experiencing hypoglycemic events at night or at any time of the day.45 These results support occasional flexibility in dosing time (up to 3 hours).
Discussion
Nature of benefit and clinical considerations
Pharmacokinetic and pharmacodynamic studies have shown that Gla-300 provides a flatter profile and more prolonged glucose-lowering activity over ≥24 hours compared with the Gla-100 formulation.26,27 Lower within-day and day-to-day glycemic variability is also observed at clinically-relevant basal insulin doses.27,29 To assess whether these properties can be translated into clinical benefit, the EDITION studies examined the efficacy and safety of Gla-300 vs Gla-100 in various T1DM and T2DM patient populations.
Noninferiority of Gla-300 vs Gla-100 for glycemic control was demonstrated across all the EDITION studies. Trends in weight change were similar in the two groups or slightly favored Gla-300. In terms of HbA1c and FPG, Gla-300 offers comparable glycemic control to Gla-100 in both T1DM and T2DM. This, coupled with the lower hypoglycemia risk (especially nocturnal hypoglycemia), represents the main clinically relevant benefit with Gla-300.
In participants with T1DM, reductions in confirmed (≤3.9 mmol/L) or severe nocturnal hypoglycemic events for Gla-300 vs Gla-100 were most evident during the first 8 weeks of treatment, when most of the uptitration of basal insulin would have occurred.32,33 Although the benefit was less clear for daytime or anytime hypoglycemia in these two studies, it should be noted that daytime hypoglycemia in T1DM is more strongly related to the use of rapidly acting or mealtime insulins than to basal insulin use.
Among participants with T2DM (both insulin-naïve individuals and those requiring high insulin doses), significantly less nocturnal hypoglycemia was observed with Gla-300 than Gla-100 over the 6-month treatment period.31,34–36 Additionally, in the trials involving T2DM participants on high-dose insulin (EDITION 1 and 2), there were significant reductions in nocturnal and anytime hypoglycemia during the first 8 weeks of treatment.34,36
One major limitation of the EDITION studies is their open-label design. The T2DM studies (EDITION 1–3) included participants with moderately high baseline HbA1c (8%–8.6%) and a range of insulin requirements. However, since people with very high HbA1c (>10% or >11%) were excluded, the efficacy and safety of Gla-300 has not been established for this group. The majority of study participants were Caucasian and about 10% Japanese, limiting the generalization of the findings to other ethnic groups. Additional experience in a broader range of non-Caucasian populations is thus desirable. No clinical studies have directly addressed Gla-300 use in pediatric patients, pregnant women, or people with renal or hepatic impairment.44
Given the associations between symptomatic hypoglycemia and increased risk of CV events and mortality,46,47 it is important to select therapies with reduced risk of hypoglycemia, especially for people with existing CV conditions.48 Because of their increased vulnerability to hypoglycemia, older people with diabetes may stand to benefit with Gla-300 or other improved long-acting insulins. In support of this, a post hoc analysis involving people aged ≥65 years (n=659) confirmed the overall EDITION T2DM cohort findings in this patient group at both 6 and 12 months.41,49 A clinical trial investigating the efficacy and safety of Gla-300 vs Gla-100 in older people with T2DM (SENIOR, NCT02320721) is expected to report in 2017.50
Support for effective dose titration and improved treatment adherence
Apart from its impact on patient safety, hypoglycemia is frequently cited as a major barrier to effective dose titration. The reduced hypoglycemia risk with Gla-300 vs Gla-100, apparent even during the first few weeks of therapy, could promote effective insulin initiation and attainment of optimal doses, which are key unmet needs in basal insulin therapy.9
The importance of effective titration, especially in T2DM, is underscored by the HbA1c target-attainment results in the EDITION trials, which implemented a closely supervised scheme for basal insulin titration.31–36 Among participants with T2DM, 25%–40% attained HbA1c <7% in 6 months, with similar target attainment in the Gla-100 and Gla-300 groups. Studies to compare different titration approaches for Gla-300 in people with T2DM (TITRATION, NCT02401243; AUTOMATIX, NCT02585674) may provide further insights on the issue.51,52
The extended duration of action of Gla-300 and reduced intra- and interday variability could also support reliable once-daily dosing for more people with diabetes. This might be particularly important for those requiring assistance with insulin administration from a caregiver or a health care professional. Finally, having a measure of dosing-time flexibility, as demonstrated in a subset of the EDITION 1 and 2 T2DM cohorts,45 may promote treatment adherence for people with irregular lifestyles, such as shift workers.
Considerations for switching to Gla-300 from other basal insulins
Due to the shorter (<24-hour) coverage of intermediate-acting insulins, such as NPH, a proportion of people on these insulins will require twice-daily injections. In EDITION 1 and 2 (T2DM), 16.9% and 19.8% of participants were receiving twice-daily basal insulin prior to randomization.53 Post hoc analysis of these subgroups showed that those switching from twice-daily basal insulin to once-daily Gla-300 achieved similar levels of glycemic control with less hypoglycemia vs those switching to Gla-100.53 These results were in line with the overall EDITION 1 and 2 results.
In the absence of head-to-head studies comparing Gla-300 with other basal insulins, Freemantle et al performed a network meta-analysis on randomized controlled studies of intermediate-acting and ultra-long-acting basal insulins, including premixed insulin, NPH, glargine (Gla-100 and Gla-300), detemir, and degludec.54 This allowed indirect estimation of the efficacy and safety of Gla-300 relative to other basal insulins. Outcome measures by network meta-analysis included changes from baseline in HbA1c (%) and body weight (kg), and rates of documented symptomatic and/or nocturnal hypoglycemic events (per patient-year). Overall, glycemic efficacy of Gla-300 was similar to other insulins, including detemir, NPH, degludec, and premixed insulin.54 Change in body weight was comparable with Gla-300 vs detemir, NPH, and degludec (small weight increases), while weight gain with Gla-300 was significantly less than with premixed insulin. Gla-300 was associated with significantly lower nocturnal hypoglycemia (≤3.9 mmol/L) rates vs NPH and premixed insulin, whereas no significant differences were noted with Gla-300 vs detemir or degludec.54 The REAL LIFE study program, a series of Phase IV trials (ACHIEVE [NCT02451137],55 REACH, and REGAIN CONTROL), will examine efficacy and health outcomes in real-world settings for people with T2DM initiating or switching to Gla-300 compared to commercially available basal insulins (Gla-100, insulin detemir, and insulin degludec).
In routine practice, factors to consider in the decision to initiate or switch to Gla-300-based regimens may include cost and such issues as changes in dose timing or learning to use a different injection device (for people switching from insulins other than Gla-100). Improvements in injection devices, such as reduced injection force and greater ease of use,56,57 may also help enhance adherence to insulin therapy.58
Conclusion
With glucose-lowering activity lasting ≥24 hours and comparable glycemic control and reduced risk of hypoglycemia, Gla-300 offers an alternative to Gla-100 for people with T1DM or T2DM. In clinical trials, the benefit in terms of reduced hypoglycemia with Gla-300 vs Gla-100 was apparent even in the first 8 weeks of treatment. People who may benefit from this new therapeutic option include insulin-naïve individuals initiating basal insulin therapy, those currently experiencing issues with their basal insulin regimens (eg, hypoglycemia or suboptimal control), and those requiring high basal insulin doses. The potential for reduced hypoglycemia risk may be important for older people,49 people with chronic kidney disease,59 and those with CV comorbidities.48 Additional data are needed to understand the benefits and risks relative to other long-acting insulin analogs, as well as treatment of people with very high HbA1c or with comorbidities. Data on glycemic control beyond 1 year, CV outcomes, and real-world experience will also be important to inform Gla-300 use in clinical practice.
Acknowledgments
The development of this manuscript was supported by Sanofi-Aventis (Hong Kong). The authors gratefully acknowledge A Cali, R Stacey, D Milo, B Leroy, T Mallet, O Loewrick, S Bajpai, W Ngai, and P Lau (Sanofi-Aventis) for critical review of the manuscript. Manuscript drafting and editorial support was provided by G Toh, Research2Trials Clinical Solutions, Singapore. This support was funded by Sanofi.
Disclosure
KT has served on advisory boards and speaker’s bureaus for Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Janssen, MSD, Pfizer, Sanofi, and Takeda. The other authors report no conflicts of interest in this work.
References
Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329(14):977–986. | ||
Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-Year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359(15):1577–1589. | ||
Nathan DM, Cleary PA, Backlund JY, et al. Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N Engl J Med. 2005;353(25):2643–2653. | ||
Stratton IM, Adler AI, Neil HA, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ. 2000;321(7258):405–412. | ||
Handelsman Y, Bloomgarden ZT, Grunberger G, et al. American Association of Clinical Endocrinologists and American College of Endocrinology: Clinical Practice Guidelines for Developing a Diabetes Mellitus Comprehensive Care Plan – 2015. Endocr Pract. 2015;21 Suppl 1:1–87. | ||
Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes, 2015 – a patient-centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2015;38(1):140–149. | ||
Peyrot M, Barnett AH, Meneghini LF, Schumm-Draeger PM. Insulin adherence behaviours and barriers in the multinational Global Attitudes of Patients and Physicians in Insulin Therapy study. Diabet Med. 2012;29(5):682–689. | ||
Peyrot M, Rubin RR, Lauritzen T, et al. Resistance to insulin therapy among patients and providers: results of the cross-national Diabetes Attitudes, Wishes, and Needs (DAWN) study. Diabetes Care. 2005;28(11):2673–2679. | ||
Edelman S, Pettus J. Challenges associated with insulin therapy in type 2 diabetes mellitus. Am J Med. 2014;127(10 Suppl):S11–S16. | ||
Pettus J, Cavaiola TC, Tamborlane WV, Edelman S. The past, present, and future of basal insulins. Diabetes Metab Res Rev. 2016;32(6):478–496. | ||
Heise T, Nosek L, Rønn BB, et al. Lower within-subject variability of insulin detemir in comparison to NPH insulin and insulin glargine in people with type 1 diabetes. Diabetes. 2004;53(6):1614–1620. | ||
Lepore M, Pampanelli S, Fanelli C, et al. Pharmacokinetics and pharmacodynamics of subcutaneous injection of long-acting human insulin analog glargine, NPH insulin, and ultralente human insulin and continuous subcutaneous infusion of insulin lispro. Diabetes. 2000;49(12):2142-2148. | ||
Evans M, Schumm-Draeger PM, Vora J, King AB. A review of modern insulin analogue pharmacokinetic and pharmacodynamic profiles in type 2 diabetes: improvements and limitations. Diabetes Obes Metab. 2011;13(8):677–684. | ||
Little S, Shaw J, Home P. Hypoglycemia rates with basal insulin analogs. Diabetes Technol Ther. 2011;13 Suppl 1:S53–S64. | ||
Barnett AH. Insulin glargine in the treatment of type 1 and type 2 diabetes. Vasc Health Risk Manag. 2006;2(1):59–67. | ||
Poon K, King AB. Glargine and detemir: safety and efficacy profiles of the long-acting basal insulin analogs. Drug Healthc Patient Saf. 2010;2:213–223. | ||
Heinemann L, Linkeschova R, Rave K, Hompesch B, Sedlak M, Heise T. Time-action profile of the long-acting insulin analog insulin glargine (HOE901) in comparison with those of NPH insulin and placebo. Diabetes Care. 2000;23(5):644–649. | ||
Riddle MC, Rosenstock J, Gerich J. The treat-to-target trial: randomized addition of glargine or human NPH insulin to oral therapy of type 2 diabetic patients. Diabetes Care. 2003;26(11):3080–3086. | ||
Rosenstock J, Dailey G, Massi-Benedetti M, Fritsche A, Lin Z, Salzman A. Reduced hypoglycemia risk with insulin glargine: a meta-analysis comparing insulin glargine with human NPH insulin in type 2 diabetes. Diabetes Care. 2005;28(4):950–955. | ||
Geller AI, Shehab N, Lovegrove MC, et al. National estimates of insulin-related hypoglycemia and errors leading to emergency department visits and hospitalizations. JAMA Intern Med. 2014;174(5):678–686. | ||
Bron M, Marynchenko M, Yang H, Yu AP, Wu EQ. Hypoglycemia, treatment discontinuation, and costs in patients with type 2 diabetes mellitus on oral antidiabetic drugs. Postgrad Med. 2012;124(1):124–132. | ||
Bruderer SG, Bodmer M, Jick SS, Bader G, Schlienger RG, Meier CR. Incidence of and risk factors for severe hypoglycaemia in treated type 2 diabetes mellitus patients in the UK: a nested case-control analysis. Diabetes Obes Metab. 2014;16(9):801–811. | ||
Moen MF, Zhan M, Hsu VD, et al. Frequency of hypoglycemia and its significance in chronic kidney disease. Clin J Am Soc Nephrol. 2009;4(6):1121–1127. | ||
Davis TM, Brown SG, Jacobs IG, Bulsara M, Bruce DG, Davis WA. Determinants of severe hypoglycemia complicating type 2 diabetes: the Fremantle diabetes study. J Clin Endocrinol Metab. 2010;95(5):2240–2247. | ||
Steinstraesser A, Schmidt R, Bergmann K, Dahmen R, Becker RH. Investigational new insulin glargine 300 U/ml has the same metabolism as insulin glargine 100 U/ml. Diabetes Obes Metab. 2014;16(9):873–876. | ||
Becker RH, Dahmen R, Bergmann K, Lehmann A, Jax T, Heise T. New insulin glargine 300 units·mL–1 provides a more even activity profile and prolonged glycemic control at steady state compared with insulin glargine 100 units·mL–1. Diabetes Care. 2015;38(4):637–643. | ||
Becker RH, Nowotny I, Teichert L, Bergmann K, Kapitza C. Low within- and between-day variability in exposure to new insulin glargine 300 U/ml. Diabetes Obes Metab. 2015;17(3):261–267. | ||
Sanofi-Aventis. Lantus [prescribing information]. 2015. Available from: http://products.sanofi.us/lantus/lantus.pdf. Accessed April 29, 2017. | ||
Bergenstal RM, Bailey TS, Rodbard D, et al. Insulin glargine 300 U/ml vs 100 U/ml: glucose profiles of morning vs evening injections in adults with type 1 diabetes mellitus measured with continuous glucose monitoring (CGM). Diabetologia. 2014;57(1 Suppl):S388–S389. | ||
Shiramoto M, Eto T, Irie S, et al. Single-dose new insulin glargine 300 U/ml provides prolonged, stable glycaemic control in Japanese and European people with type 1 diabetes. Diabetes Obes Metab. 2015;17(3):254–260. | ||
Bolli GB, Riddle MC, Bergenstal RM, et al. New insulin glargine 300 U/ml compared with glargine 100 U/ml in insulin-naive people with type 2 diabetes on oral glucose-lowering drugs: a randomized controlled trial (EDITION 3). Diabetes Obes Metab. 2015;17(4):386–394. | ||
Home PD, Bergenstal RM, Bolli GB, et al. New insulin glargine 300 units/mL versus glargine 100 units/mL in people with type 1 diabetes: a randomized, phase 3A, open-label clinical trial (EDITION 4). Diabetes Care. 2015;38(12):2217–2225. | ||
Matsuhisa M, Koyama M, Cheng X, et al. New insulin glargine 300 U/ml versus glargine 100 U/ml in Japanese adults with type 1 diabetes using basal and mealtime insulin: glucose control and hypoglycaemia in a randomized controlled trial (EDITION JP1). Diabetes Obes Metab. 2016;18(4):375–383. | ||
Riddle MC, Bolli GB, Ziemen M, et al. New insulin glargine 300 units/mL versus glargine 100 units/mL in people with type 2 diabetes using basal and mealtime insulin: glucose control and hypoglycemia in a 6-month randomized controlled trial (EDITION 1). Diabetes Care. 2014;37(10):2755–2762. | ||
Terauchi Y, Koyama M, Cheng X, et al. New insulin glargine 300 U/ml versus glargine 100 U/ml in Japanese people with type 2 diabetes using basal insulin and oral antihyperglycaemic drugs: glucose control and hypoglycaemia in a randomized controlled trial (EDITION JP 2). Diabetes Obes Metab. 2016;18(4):366–374. | ||
Yki-Jarvinen H, Bergenstal R, Ziemen M, et al. New insulin glargine 300 units/mL versus glargine 100 units/mL in people with type 2 diabetes using oral agents and basal insulin: glucose control and hypoglycemia in a 6-month randomized controlled trial (EDITION 2). Diabetes Care. 2014;37(12):3235-3243. | ||
Riddle MC, Yki-Järvinen H, Bolli GB, et al. One-year sustained glycaemic control and less hypoglycaemia with new insulin glargine 300 U/ml compared with 100 U/ml in people with type 2 diabetes using basal plus meal-time insulin: the EDITION 1 12-month randomized trial, including 6-month extension. Diabetes Obes Metab. 2015;17(9):835–842. | ||
Yki-Järvinen H, Bergenstal RM, Bolli GB, et al. Glycaemic control and hypoglycaemia with new insulin glargine 300 U/ml versus insulin glargine 100 U/ml in people with type 2 diabetes using basal insulin and oral antihyperglycaemic drugs: the EDITION 2 randomized 12-month trial including 6-month extension. Diabetes Obes Metab. 2015;17(12):1142–1149. | ||
Matsuhisa M, Koyama M, Cheng X, Shimizu S, Hirose T. Sustained glycaemic control and less nocturnal hypoglycaemia with new insulin glargine 300 U/ml versus glargine 100 U/ml over 1 year in Japanese people with type 1 diabetes mellitus (EDITION JP 1). Diabetologia. 2015;58(1 Suppl):S2–S3. | ||
Ritzel R, Roussel R, Bolli GB, et al. Patient-level meta-analysis of the EDITION 1, 2 and 3 studies: glycaemic control and hypoglycaemia with new insulin glargine 300 U/ml versus glargine 100 U/ml in people with type 2 diabetes. Diabetes Obes Metab. 2015;17(9):859–867. | ||
Ritzel R, Roussel R, Giaccari A, et al. Patient-level meta-analysis of 1y phase 3A EDITION type 2 diabetes mellitus studies: glycaemic control and hypoglycaemia with insulin glargine 300 U/ml (Gla-300) vs glargine 100 U/ml (Gla-100). Diabetologia. 2015;58(1 Suppl):S472. | ||
Terauchi Y, Koyama M, Cheng X, Sumi M, Hirose T. Sustained glycaemic control and less hypoglycaemia over 1y with new insulin glargine 300 U/ml vs glargine 100 U/ml in Japanese type 2 diabetes mellitus people on basal insulin + OAD(s) (EDITION JP 2) [abstract 959]. Diabetologia. 2015;58(1 Suppl):S463. | ||
[No authors listed]. Defining and reporting hypoglycemia in diabetes: a report from the American Diabetes Association Workgroup on Hypoglycemia. Diabetes Care. 2005;28(5):1245–1249. | ||
Sanofi-Aventis. Toujeo [prescribing information]. 2015. Available from: http://products.sanofi.us/toujeo/toujeo.pdf. Accessed April 29, 2017. | ||
Riddle MC, Bolli GB, Home PD, et al. Efficacy and safety of flexible versus fixed dosing intervals of insulin glargine 300 U/mL in People with type 2 diabetes. Diabetes Technol Ther. 2016;18(4):252–257. | ||
Goto A, Goto M, Terauchi Y, Yamaguchi N, Noda M. Association between severe hypoglycemia and cardiovascular disease risk in Japanese patients with type 2 diabetes. J Am Heart Assoc. 2016;4(3):e002875. | ||
Hsu PF, Sung SH, Cheng HM, et al. Association of clinical symptomatic hypoglycemia with cardiovascular events and total mortality in type 2 diabetes: a nationwide population-based study. Diabetes Care. 2013;36(4):894–900. | ||
Gerstein HC, Bosch J, Dagenais GR, et al. Basal insulin and cardiovascular and other outcomes in dysglycemia. N Engl J Med. 2012;367(4):319–328. | ||
Yale JF, Aroda VR, Charbonnel B, et al. Older people with type 2 diabetes: glycemic control and hypoglycemia risk with new insulin glargine 300 U/mL. Diabetes. 2015;64 Suppl 1:A261. | ||
Sanofi. Comparison of the safety and efficacy of HOE901-U300 with Lantus in older patients with type2 diabetes insufficiently controlled on their current antidiabetic medications (SENIOR). Available from: https://clinicaltrials.gov/ct2/show/NCT02320721. NLM identifier: NCT02320721. Accessed November 22, 2015. | ||
Sanofi. Study of two titration algorithms with insulin glargine 300 units/mL in type 2 diabetes mellitus patients (TITRATION). Available from: https://clinicaltrials.gov/ct2/show/NCT02401243. NLM identifier: NCT02401243. Accessed November 22, 2015. | ||
Sanofi. Comparison of MyStar DoseCoach to Routine Titration in Adult Patients With Type 2 Diabetes Mellitus Using Toujeo (AUTOMATIX). Available from: https://clinicaltrials.gov/ct2/show/NCT02585674. NLM identifier: NCT02585674. Accessed March 14, 2016. | ||
Roussel R, D’Emden MC, Fisher M, et al. Switching from twice-daily basal insulin to once-daily new insulin glargine 300 U/mL (Gla-300): an analysis in people with T2DM (EDITION 1 and 2). Diabetes. 2015;64(1 Suppl):A261. | ||
Freemantle N, Chou E, Frois C, et al. Safety and efficacy of insulin glargine 300 U/mL compared with other basal insulin therapies in patients with type 2 diabetes mellitus: a network meta-analysis. BMJ Open. 2016;6(2):e009421. | ||
Sanofi. A “real world” trial to determine efficacy and health outcomes of Toujeo (Achieve Control Real Life Study Program). Available from: https://clinicaltrials.gov/ct2/show/NCT02451137. NLM identifier: NCT02451137. Accessed November 24, 2015. | ||
Klonoff D, Nayberg I, Erbstein F, Cali A, Brulle-Wohlhueter C, Haak T. Usability of the Gla-300 injection device compared with three other commercialized disposable insulin pens: results of an interview-based survey. J Diabetes Sci Technol. 2015;9(4):936–938. | ||
Klonoff D, Nayberg I, Thonius M, et al. Accuracy and injection force of the Gla-300 injection device compared with other commercialized disposable insulin pens. J Diabetes Sci Technol. 2015;10(1):125–130. | ||
Anderson BJ, Redondo MJ. What can we learn from patient-reported outcomes of insulin pen devices? J Diabetes Sci Technol. 2011;5(6):1563–1571. | ||
Escalada J, Halimi S, Senior PA, et al. Glycemic control and hypoglycemia benefits with insulin glargine 300 U/mL (Gla-300) extend to people with type 2 diabetes (T2DM) and mild-to-moderate renal impairment. Diabetes. 2016;65(1 Suppl):A18. | ||
Fowler MJ. Diabetes treatment, part 3: insulin and incretins. Clin Diabetes. 2008;26(1):35–39. | ||
Novo Nordisk. Levemir [prescribing information]. 2015. Available from: http://www.novo-pi.com/levemir.pdf. Accessed April 29, 2017. | ||
Novo Nordisk. Tresiba [prescribing information]. 2015. Available from: http://www.novo-pi.com/tresiba.pdf. Accessed April 29, 2017. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.