Back to Journals » Medical Devices: Evidence and Research » Volume 9
Inhaled pulmonary vasodilators for persistent pulmonary hypertension of the newborn: safety issues relating to drug administration and delivery devices
Received 31 October 2015
Accepted for publication 25 January 2016
Published 12 April 2016 Volume 2016:9 Pages 45—51
DOI https://doi.org/10.2147/MDER.S99601
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Nathan Cosa,1 Edward Costa Jr2
1Department of Respiratory Care, Banner Desert Medical Center, Cardon Children's Medical Center, Mesa, AZ, 2Department of Medical Affairs, Mallinckrodt Pharmaceuticals, Hampton, NJ, USA
Abstract: Treatment for persistent pulmonary hypertension of the newborn (PPHN) aims to reduce pulmonary vascular resistance while maintaining systemic vascular resistance. Selective pulmonary vasodilation may be achieved by targeting pulmonary-specific pathways or by delivering vasodilators directly to the lungs. Abrupt withdrawal of a pulmonary vasodilator can cause rebound pulmonary hypertension. Therefore, use of consistent delivery systems that allow for careful monitoring of drug delivery is important. This manuscript reviews published studies of inhaled vasodilators used for treatment of PPHN and provides an overview of safety issues associated with drug delivery and delivery devices as they relate to the risk of rebound pulmonary hypertension. Off-label use of aerosolized prostacyclins and an aerosolized prostaglandin in neonates with PPHN has been reported; however, evidence from large randomized clinical trials is lacking. The amount of a given dose of aerosolized drug that is actually delivered to the lungs is often unknown, and the actual amount of drug deposited in the lungs can be affected by several factors, including patient size, nebulizer used, and placement of the nebulizer within the breathing circuit. Inhaled nitric oxide (iNO) is the only pulmonary vasodilator approved by the US Food and Drug Administration for the treatment of PPHN. The iNO delivery device, INOmax DSIR®, is designed to constantly monitor NO, NO2, and O2 deliveries and is equipped with audible and visual alarms to alert providers of abrupt discontinuation and incorrect drug concentration. Other safety features of this device include two independent backup delivery systems, a backup drug cylinder, a battery that provides up to 6 hours of uninterrupted medication delivery, and 27 alarms that monitor delivery, dosage, and system functions. The ability of the drug delivery device to provide safe, consistent dosing is important to consider when selecting a pulmonary vasodilator.
Keywords: nitric oxide, prostaglandin E1, prostaglandin I2, nebulizers, medical device safety, prostacyclin
Introduction
Failures in the normal postbirth transition of the pulmonary circulation can lead to a syndrome characterized by sustained elevation of pulmonary vascular resistance, right-to-left shunting, and severe hypoxemia.1,2 This syndrome, referred to as persistent pulmonary hypertension of the newborn (PPHN), occurs in approximately two of every 1,000 live births.3 The primary goal of treatment of PPHN is to reduce pulmonary vascular resistance while maintaining systemic vascular resistance; hence, the ideal therapy for PPHN is a vasodilator agent that is selective for the pulmonary circulation.1,4 Selective pulmonary vasodilation may be achieved by targeting pulmonary-specific pathways with systemically delivered drugs or by delivering vasodilators directly to the lungs. Currently, the only pulmonary vasodilator approved by the US Food and Drug Administration (FDA) for the treatment of pulmonary hypertension in neonates is inhaled nitric oxide (iNO).5 A range of other vasodilators have been used off label, including phosphodiesterase inhibitors, prostacyclin (PGI2) analogs, prostaglandin E1 (PGE1), and endothelin receptor antagonists.2
Abrupt withdrawal of pulmonary vasodilator treatment can result in the potentially dangerous complication of rebound pulmonary hypertension (RPH), which is characterized by an increase in pulmonary vascular resistance, compromised cardiac output, and/or severe hypoxemia.6,7 It is believed that RPH occurs as a consequence of downregulation of endogenous nitric oxide (NO) production and increased endothelin-1 concentrations.7,8 To avoid delivery failure and inconsistent dosing of pulmonary vasodilators, it is important to use safe and consistent delivery systems that allow for careful monitoring of drug delivery and are approved by the FDA for use in conjunction with ventilatory support. This manuscript reviews published studies of inhaled pulmonary vasodilators used in neonates with PPHN and provides an overview of drug delivery and device safety as they relate to the risk of RPH.
Inhaled aerosolized pulmonary vasodilators
Prostacyclins
PGI2 acts as a vasodilator by activating adenylate cyclase and increasing cyclic adenosine monophosphate in pulmonary arterial smooth muscle cells.2,9,10 Three different PGI2 analogs have been approved by the FDA for use in patients with pulmonary arterial hypertension (PAH; World Health Organization [WHO] Group 1), including epoprostenol (intravenous [IV] injection),11 iloprost (inhalation solution),12 and treprostinil (extended-release oral tablets,13 subcutaneous infusion,14 and inhalation solution15); none are approved for treatment of PPHN. In general, off-label use of systemic PGI2 has largely been avoided in the PPHN population because of concerns about the risk of systemic hypotension.2,16 However, inhaled aerosolized epoprostenol and iloprost have been used off label to provide selective pulmonary vasodilation in neonates with PPHN.9,16,17
Epoprostenol
Epoprostenol was the first drug approved by the FDA for the treatment of PAH18 and is approved only for IV use in the treatment of PAH (WHO Group 1) to improve exercise capacity.11 Off-label use as an inhaled aerosol in neonates with PPHN has been described in case reports16,17,19,20 and a retrospective chart review9 but has not yet been evaluated in randomized controlled trials. The reconstituted solution of epoprostenol has a pH of 10.2–10.8 and is increasingly unstable at a lower pH.11 A retrospective chart review identified 20 pediatric subjects who received aerosolized epoprostenol concomitantly with iNO and IV milrinone at a single hospital over a 2-year period.9 Most subjects (16/20) also received concomitant enteral sildenafil. The study found a significant decrease in the oxygenation index (OI) from 26.4 before treatment to 18.6 during treatment (P=0.04). The majority of subjects were neonates (13/20, 65%). In subgroup analyses by age and diagnosis, significant improvements in OI were observed only in the neonatal group and those with meconium aspiration syndrome and/or PPHN. Overall, six of the 20 subjects (five neonates) experienced at least one studied side effect during treatment with epoprostenol; the most common of these was a decrease in systolic blood pressure necessitating fluid boluses or administration of vasopressor agents. Transient difficulty with the nebulizer–ventilator interface was the most common respiratory problem requiring brief interruption of therapy, which, in some cases, caused inconsistent mean airway pressure during high-frequency oscillatory ventilation.
Epoprostenol may be aerosolized in a nebulizer connected to either the inspiratory limb of the ventilator circuit or the bilevel pulmonary arterial pressure (PAP) circuit for noninvasive ventilation at a point as close as possible to the endotracheal tube or mask. Nebulizers used in studies reported in the published literature include the Small Particle Aerosol Generator-2 (SPAG-2; ICN Pharmaceuticals, Inc., Costa Mesa, CA, USA)17,19,20 and the MiniHEART Lo-Flo nebulizer (Westmed, Inc., Tucson, AZ, USA; Table 1).9 The SPAG-2 nebulizer is rarely used in current practice and is indicated only for the administration of ribavirin.21 The use of Aeroneb® Solo Nebulizer System (Aerogen Ltd., Galway, Ireland)22 with epoprostenol has been described in other patient populations (eg, adults with acute respiratory distress syndrome),23 but not for neonates with PPHN. Because of its very short half-life (~6 minutes), epoprostenol must be administered continuously; unplanned interruptions in delivery are potentially dangerous and may lead to RPH.24 Nebulizer clogging during aerosolization of epoprostenol associated with device-related desaturation, ventricular arrhythmias, and hypotension in an adult patient has been reported to the Manufacturer and User Facility Device Experience database.25
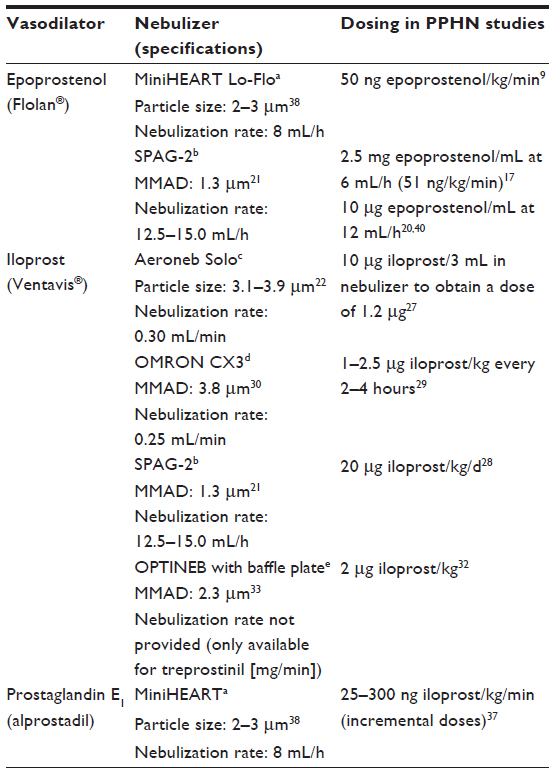 | Table 1 Aerosolized vasodilators used in PPHN: nebulizers and dosing in published studies |
Iloprost
Iloprost is a synthetic analog of PGI2 approved only for the treatment of PAH (WHO Group 1).12 It has a half-life of 20–30 minutes and is intended to be inhaled six to nine times a day using the I-neb adaptive aerosol delivery nebulizer (Philips Respironics, Respiratory Drug Delivery, Chichester, UK). The I-neb adaptive aerosol delivery is not intended for use in neonates or in a ventilator circuit.26 In published reports of aerosolized iloprost in newborns with PPHN, the drug was administered via other nebulizers, including Aeroneb® Module for SERVO-i ventilator (MAQUET Critical Care AB, Solna, Sweden),22,27 SPAG-2,21,28 CX3 (OMRON Healthcare Europe B.V., Hoofddorp, the Netherlands),29–31 and OPTINEBTM Ultrasonic Nebulizer (NEBU-TEC International, Elsenfeld, Germany32,33; Table 1). Most of these were case reports, involving a total of one to four infants.27,28,32 One retrospective review evaluated preterm infants with pulmonary hypertension who were treated with mechanical ventilation and surfactant.31 Of the 50 infants included in the study, 15 continued to have an OI >25 and pulmonary hypertension despite mechanical ventilation and surfactant treatments. This group of 15 then received inhaled iloprost with a jet nebulizer adapted to the ventilator circuit. In these patients, the mean maximum OI decreased from 38, before initiation of iloprost, to 8 at the end of iloprost treatment. The mean systolic PAP declined from 62 to 25 mmHg. The mean duration of inhaled iloprost treatment was 5 days. No clinical signs necessitating cessation of inhaled iloprost, no side effects attributable to iloprost treatment, and no nebulizer–ventilator device-related adverse events were reported. However, the authors concluded that further studies are required to evaluate the efficacy and safety of inhaled iloprost in the preterm population.31
Another retrospective study compared inhaled iloprost (n=20) with oral sildenafil (n=27) in term infants with PPHN.29 Iloprost (1–2.5 mg/kg every 2–4 hours) was administered endotracheally using the CX3 nebulizer. Subjects in the iloprost group showed significantly greater improvements versus sildenafil in time to adequate clinical response (P<0.03), duration of drug (sildenafil or iloprost) administration (P=0.03), duration of mechanical ventilation (P<0.001), use of magnesium sulfate as a second vasodilator (P=0.036), and requirement for support with extra-inotropic agents (P<0.001). While no side effects on blood pressure or homeostasis were observed in the iloprost group, the incidence of systemic hypotension was significantly higher in the sildenafil group compared to that in the iloprost group (9/27 versus 0/20; P=0.01). Four (20%) and three (11%) infants died of PPHN in the iloprost and sildenafil groups, respectively. No clinical signs requiring cessation of inhaled iloprost therapy were detected, and no side effects attributable to iloprost treatment were observed during drug administration. The authors concluded that aerosolized iloprost may provide an effective and well-tolerated treatment option for critically ill patients with PPHN in developing countries, where other treatment modalities (eg, iNO, high-frequency oscillatory ventilation, and extracorporeal membrane oxygenation) are not available.
Prostaglandin
Prostaglandin E1
PGE1 (alprostadil) injection is a vasodilator approved for palliative therapy to maintain patency of the ductus arteriosus in neonates with congenital heart defects.34 Aerosolized PGE1 has been used as a selective pulmonary vasodilator in adults with acute lung injury35 and acute respiratory distress syndrome.36 One pilot trial evaluated the use of aerosolized PGE1 in term/near-term infants with neonatal respiratory failure.37 In this study, incremental doses of inhaled PGE1 (25, 50, 150, and 300 ng/kg/min) were delivered by the MiniHEART jet nebulizer38 over a 2-hour period to 13 subjects before receiving iNO and to seven subjects who had failed to respond to previous iNO therapy; after the 2-hour administration period, study treatment was weaned over 1 hour. The mean (standard deviation) increase in partial pressure of oxygen in arterial blood (PaO2) at the end of PGE1 administration was 63 (62.3) torr in the iNO-naïve subjects (P=0.024), and 40 (62.1) torr in the iNO nonresponders (P>0.05). Eight (61.5%) iNO-naïve subjects and three (42.9%) iNO nonresponders had a full response (increase in PaO2 ≥25 torr) to PGE1. There was no evidence of RPH between doses and after cessation of inhaled PGE1, and no systemic side effects were detected. A pilot study (NCT01467076) of inhaled PGE1 in neonates with hypoxic respiratory failure and a suboptimal response to iNO was halted due to low subject enrollment.39
Delivery considerations associated with nebulizers for aerosolized vasodilators
None of the nebulization systems that have been used to aerosolize vasodilators in the PPHN literature have FDA clearance for delivery of these agents or for use in the PPHN population. When administering an inhaled vasodilator, it is important that the device used allows for consistent drug dosing to prevent potential RPH and hypoxemia. Most nebulizers, including the Aeroneb and MiniHEART, are not equipped with alarms that can alert caregivers if medication is not being delivered;22,38 the Aeroneb and MiniHEART nebulizers do not monitor medication delivery. Therefore, clinicians must visually inspect the nebulizer for aerosol output in order to ensure correct functionality. The frequency at which nebulizer output should be checked is unclear, as no guidance on this issue is provided in the user manuals. The lack of an alarm system in medical devices was identified as a major contributing factor to alarm-related events (eg, death and permanent loss of function) in a 2013 Joint Commission review of the Sentinel Event database.40 In the absence of appropriate safety features on a given delivery device, the patients themselves may become the alarm for poor drug delivery; in the case of a patient with PPHN, this can possibly manifest as signs of increased PAP, decreased cardiac output, worsening OI, and/or serious hypoxemia.29,41 Appropriate monitoring of systemic blood pressure and oxygen saturation should be kept in place to avoid rebound effects of interrupted drug delivery. It is also important to maintain availability of a backup drug delivery system when using a nebulizer. The Aeroneb and the MiniHEART Lo-Flo nebulizers do not have backup delivery modes or a backup drug supply,22,38 and setup of an additional nebulizer and/or a backup supply of prepared drug solution may require additional indirect costs and staff training.
When administering aerosolized drugs to mechanically ventilated patients, the dose of drug delivered to the lungs is often unknown.42 Aerosolized particle sizes and flow rates vary substantially between nebulizers (Table 1), and none of the nebulizers have a drug delivery monitor to determine dosing. Drug deposition in the lung is dependent on several factors, including patient size, the nebulizer used, placement of the nebulizer within the inhalation circuit, endotracheal tube size, and mechanical ventilator application (ie, high-frequency versus conventional ventilation).43,44 Guidelines are lacking on procedures for preparing these drugs for use in nebulizers; multiple individuals may be involved, including the pharmacist, the nurse, and the respiratory therapist. Also, there is currently a lack of consensus on the best placement of nebulizers within the ventilator circuit for optimal lung deposition. Overall, the fraction of the dose deposited in the alveolar space during mechanical ventilation is estimated to be <10%–20% of the administered dose,45 and the alveolar dose is even smaller in newborn infants because there is a proportionally larger dead space.17 Dose adjustments of aerosolized vasodilators can add further complexity to achieving an appropriate treatment regimen for an individual patient, as each desired drug concentration has to be mixed separately.42
Nitric oxide
NO acts as a vasodilator by binding to and activating guanylate cyclase and increasing intracellular levels of cyclic guanosine 3′,5′-monophosphate, which results in relaxation of vascular smooth muscle.5 When inhaled, NO selectively dilates the pulmonary vasculature and has minimal effect on the systemic vasculature because it is quickly inactivated by hemoglobin. iNO improves oxygenation and decreases the need for extracorporeal life support in neonates with PPHN.46–49 iNO (INOmax®; INO Therapeutics, Hampton, NJ, USA), used in conjunction with ventilator support and other appropriate agents, is indicated for the treatment of term and near-term (>34 weeks gestation) neonates with hypoxic respiratory failure associated with clinical or echocardiographic evidence of pulmonary hypertension, where it improves oxygenation and reduces the need for extracorporeal membrane oxygenation.5
Abrupt discontinuation of iNO may lead to increasing PAP and worsening oxygenation (ie, RPH) even in neonates who do not have an apparent response to iNO. One study of 97 subjects who received iNO showed that when iNO exposure was limited to 30 minutes, withdrawing iNO in neonate nonresponders did not cause increased respiratory morbidity.50 Nevertheless, weaning of iNO requires down-titration in several steps, pausing several hours at each step to monitor for hypoxemia.
When the FDA approved iNO in 1999, the risk of RPH with abrupt discontinuation of drug delivery was a major concern. In 2000, the FDA released a guidance document for the NO delivery apparatus requiring that such devices include multiple safety features, such as mechanisms to allow for constant monitoring of NO, NO2, and O2 deliveries; a backup drug delivery system; a sensor that sounds an alarm when NO concentrations are out of the specified range; and a backup power supply.51 NO delivery systems (eg, INOmax DSIR®, INOmax® DS, or INOvent®; INO Therapeutics) deliver NO in conjunction with a ventilator or breathing gas administration system after dilution with an O2/air mixture.5 The INOmax DSIR device constantly monitors NO, NO2, and O2 deliveries and has audible and visual alarms to alert providers of abrupt discontinuation of drug delivery and incorrect drug concentration. It includes two independent backup delivery systems, a backup drug cylinder, a battery that provides up to 6 hours of uninterrupted medication delivery, and 27 alarms that monitor delivery, dosage, and system functions. As such, the INOmax DSIR is the only device for administration of an inhaled pulmonary vasodilator that complies with all FDA delivery device requirements.
Summary
Although some data suggest that aerosolized PGI2 analogs may be effective pulmonary vasodilators in neonates with PPHN, these agents are not approved by the FDA in this patient population and evidence from randomized clinical trials is lacking. iNO is the only inhaled pulmonary vasodilator approved for term and near-term neonates with PPHN. Because of the risk of RPH on withdrawal, consistent dosing and avoidance of delivery failure are important considerations when selecting a pulmonary vasodilator. Also, caregivers should be trained to identify signs and symptoms of RPH, especially in the absence of device safety alarms. The use of delivery devices equipped with appropriate alarm functions and integrated backup drug delivery can help prevent disruptions in drug delivery and avoid potential device-related adverse events. When utilizing nebulizers to administer aerosolized pulmonary vasodilators, it is important that clinicians visually assess and monitor aerosol output in order to determine medication administration.
Acknowledgments
The authors thank Michael Morren, RPh, MBA, and Lela Creutz, PhD, of Peloton Advantage, LLC, Parsippany, NJ, USA, for assistance with writing and manuscript preparation, funded by Mallinckrodt Pharmaceuticals.
Disclosure
Nathan Cosa has no conflicts to disclose in this work. Edward Costa Jr is an employee of Mallinckrodt Pharmaceuticals.
References
McLaughlin VV, Archer SL, Badesch DB, et al; ACCF/AHA. ACCF/AHA 2009 expert consensus document on pulmonary hypertension: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents and the American Heart Association: developed in collaboration with the American College of Chest Physicians, American Thoracic Society, Inc., and the Pulmonary Hypertension Association. Circulation. 2009;119(16):2250–2294. | |
Nair J, Lakshminrusimha S. Update on PPHN: mechanisms and treatment. Semin Perinatol. 2014;38(2):78–91. | |
Walsh-Sukys MC, Tyson JE, Wright LL, et al. Persistent pulmonary hypertension of the newborn in the era before nitric oxide: practice variation and outcomes. Pediatrics. 2000;105(1 pt 1):14–20. | |
Steinhorn RH. Neonatal pulmonary hypertension. Pediatr Crit Care Med. 2010;11(2 suppl):S79–S84. | |
INOmax [package insert]. Hampton, NJ: INO Therapeutics; 2015. | |
Miller OI, Tang SF, Keech A, Celermajer DS. Rebound pulmonary hypertension on withdrawal from inhaled nitric oxide. Lancet. 1995;346(8966):51–52. | |
McMullan DM, Bekker JM, Johengen MJ, et al. Inhaled nitric oxide-induced rebound pulmonary hypertension: role for endothelin-1. Am J Physiol Heart Circ Physiol. 2001;280(2):H777–H785. | |
Wedgwood S, McMullan DM, Bekker JM, Fineman JR, Black SM. Role for endothelin-1-induced superoxide and peroxynitrite production in rebound pulmonary hypertension associated with inhaled nitric oxide therapy. Circ Res. 2001;89(4):357–364. | |
Brown AT, Gillespie JV, Miquel-Verges F, et al. Inhaled epoprostenol therapy for pulmonary hypertension: improves oxygenation index more consistently in neonates than in older children. Pulm Circ. 2012;2(1):61–66. | |
Vane JR, Botting RM. Pharmacodynamic profile of prostacyclin. Am J Cardiol. 1995;75(3):3A–10A. | |
Flolan [package insert]. Research Triangle Park, NC: GlaxoSmithKline; 2014. | |
Ventavis [package insert]. South San Francisco, CA: Actelion Pharmaceuticals US, Inc.; 2013. | |
Orenitram [package insert]. Research Triangle Park, NC: United Therapeutics Corporation; January 2016. | |
Remodulin [package insert]. Research Triangle Park, NC: United Therapeutics Corporation; 2014. | |
Tyvaso [package insert]. Research Triangle Park, NC: United Therapeutics Corporation; 2014. | |
Santak B, Schreiber M, Kuen P, Lang D, Radermacher P. Prostacyclin aerosol in an infant with pulmonary hypertension. Eur J Pediatr. 1995;154(3):233–235. | |
Bindl L, Fahnenstich H, Peukert U. Aerosolised prostacyclin for pulmonary hypertension in neonates. Arch Dis Child Fetal Neonatal Ed. 1994;71(3):F214–F216. | |
Waxman AB, Zamanian RT. Pulmonary arterial hypertension: new insights into the optimal role of current and emerging prostacyclin therapies. Am J Cardiol. 2013;111(5 suppl):1A–16A. | |
Kelly LK, Porta NF, Goodman DM, Carroll CL, Steinhorn RH. Inhaled prostacyclin for term infants with persistent pulmonary hypertension refractory to inhaled nitric oxide. J Pediatr. 2002;141(6):830–832. | |
Soditt V, Aring C, Groneck P. Improvement of oxygenation induced by aerosolized prostacyclin in a preterm infant with persistent pulmonary hypertension of the newborn. Intensive Care Med. 1997;23(12):1275–1278. | |
SPAG-2 User Manual. Aliso Viejo, CA: Valeant Pharmaceuticals; 2014. | |
Aeroneb® Solo System Instruction Manual. Galway: Aerogen Ltd; 2014. | |
Pacheco J, Arnold H, Skrupky L, Watts P, Micek ST, Kollef MH. Predictors of outcome in 216 subjects with ARDS treated with inhaled epoprostenol. Respir Care. 2014;59(8):1178–1185. | |
Baker CD, Abman SH, Mourani PM. Pulmonary hypertension in preterm infants with bronchopulmonary dysplasia. Pediatr Allergy Immunol Pulmonol. 2014;27(1):8–16. | |
FDA [webpage on the Internet]. MAUDE adverse event report: Aerogen LTD Aeroneb Solo, Convenience, 10/pk. U.S. Food and Drug Administration. Available from: http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfmaude/detail.cfm?mdrfoi__id=2577645. Accessed February 16, 2015. | |
I-Neb AAD System User Guide. Chichester: Philips Respironics; 2010. | |
Avila-Alvarez A, Bravo-Laguna MC, Bronte LD, Del Cerro MJ. Inhaled iloprost as a rescue therapy for transposition of the great arteries with persistent pulmonary hypertension of the newborn. Pediatr Cardiol. 2013;34(8):2027–2029. | |
Ehlen M, Wiebe B. Iloprost in persistent pulmonary hypertension of the newborn. Cardiol Young. 2003;13(4):361–363. | |
Kahveci H, Yilmaz O, Avsar UZ, et al. Oral sildenafil and inhaled iloprost in the treatment of pulmonary hypertension of the newborn. Pediatr Pulmonol. 2014;49(12):1205–1213. | |
OMRON CX3 Nebuliser Instruction Manual. Hoofddorp: OMRON Healthcare Europe; 2007. | |
Yilmaz O, Kahveci H, Zeybek C, Ciftel M, Kilic O. Inhaled iloprost in preterm infants with severe respiratory distress syndrome and pulmonary hypertension. Am J Perinatol. 2014;31(4):321–326. | |
Eifinger F, Sreeram N, Mehler K, Huenseler C, Kribs A, Roth B. Aerosolized iloprost in the treatment of pulmonary hypertension in extremely preterm infants: a pilot study. Klin Padiatr. 2008;220(2):66–69. | |
Tyvaso Inhalation System Instructions for Use. Research Triangle Park, NC: United Therapeutics Corporation; 2013. | |
Alprostadil Injection [package insert]. Irvine, CA: Teva Parenteral Medicines, Inc.; 2009. | |
Meyer J, Theilmeier G, Van Aken H, et al. Inhaled prostaglandin E1 for treatment of acute lung injury in severe multiple organ failure. Anesth Analg. 1998;86(4):753–758. | |
Putensen C, Hormann C, Kleinsasser A, Putensen-Himmer G. Cardiopulmonary effects of aerosolized prostaglandin E1 and nitric oxide inhalation in patients with acute respiratory distress syndrome. Am J Respir Crit Care Med. 1998;157(6 pt 1):1743–1747. | |
Sood BG, Delaney-Black V, Aranda JV, Shankaran S. Aerosolized PGE1: a selective pulmonary vasodilator in neonatal hypoxemic respiratory failure results of a Phase I/II open label clinical trial. Pediatr Res. 2004;56(4):579–585. | |
HEART® Nebulizers Brochure. Largo, FL: Independent Medical Associates; 2007. | |
Sood BG, Keszler M, Garg M, et al; Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Inhaled PGE1 in neonates with hypoxemic respiratory failure: two pilot feasibility randomized clinical trials. Trials. 2014;15(1):486. | |
Joint Commission. Medical device alarm safety in hospitals. Sentinal Event Alert. 2013;(50):1–3. | |
Shah PS, Ohlsson A. Sildenafil for pulmonary hypertension in neonates. Cochrane Database Syst Rev. 2011;(8):CD005494. | |
Siobal MS, Kallet RH, Pittet JF, et al. Description and evaluation of a delivery system for aerosolized prostacyclin. Respir Care. 2003;48(8):742–753. | |
Berlinski A, Willis JR. Albuterol delivery by 4 different nebulizers placed in 4 different positions in a pediatric ventilator in vitro model. Respir Care. 2013;58(7):1124–1133. | |
Gardenhire DS, Ari A, Hess D, Myers TR. A Guide to Aerosol Delivery Devices for Respiratory Therapists. 3rd ed. Irving, TX: American Association for Respiratory Care; 2013. | |
Walmrath D, Schneider T, Schermuly R, Olschewski H, Grimminger F, Seeger W. Direct comparison of inhaled nitric oxide and aerosolized prostacyclin in acute respiratory distress syndrome. Am J Respir Crit Care Med. 1996;153(3):991–996. | |
Roberts JD Jr, Fineman JR, Morin FC III, et al. Inhaled nitric oxide and persistent pulmonary hypertension of the newborn. The Inhaled Nitric Oxide Study Group. N Engl J Med. 1997;336(9):605–610. | |
Clark RH, Kueser TJ, Walker MW, et al. Low-dose nitric oxide therapy for persistent pulmonary hypertension of the newborn. Clinical Inhaled Nitric Oxide Research Group. N Engl J Med. 2000;342(7):469–474. | |
The Neonatal Inhaled Nitric Oxide Study Group. Inhaled nitric oxide in full-term and nearly full-term infants with hypoxic respiratory failure. N Engl J Med. 1997;336(9):597–604. [published correction appears in N Engl J Med. 1997;337:434]. | |
Davidson D, Barefield ES, Kattwinkel J, et al. Inhaled nitric oxide for the early treatment of persistent pulmonary hypertension of the term newborn: a randomized, double-masked, placebo-controlled, dose-response, multicenter study. The I-NO/PPHN Study Group. Pediatrics. 1998;101(3 pt 1):325–334. | |
Carriedo H, Rhine W. Withdrawal of inhaled nitric oxide from nonresponders after short exposure. J Perinatol. 2003;23(7):556–558. | |
U.S. Department of Health and Human Services; Food and Drug Administration; Center for Devices and Radiological Health [webpage on the Internet]. Guidance document for premarket notification submissions for nitric oxide delivery apparatus, nitric oxide analyzer and nitrogen dioxide analyzer. Available from: http://www.fda.gov/downloads/MedicalDevices/DeviceRegulationandGuidance/GuidanceDocuments/ucm073767.pdf. Accessed December 16, 2015. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.