Back to Journals » Journal of Asthma and Allergy » Volume 18
Inhalant-Specific IgE Profiles to Guide the Clinical Management and Prevention of Children with Respiratory Allergies in Fuzhou: A Cross-Sectional Cohort Study Based on ImmunoCAP
Authors Li Y, Lin C, Wang Q, Zhang L, Zhu Z, Cheng F, Wang B
Received 23 July 2025
Accepted for publication 12 December 2025
Published 21 December 2025 Volume 2025:18 Pages 1847—1856
DOI https://doi.org/10.2147/JAA.S549970
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Yadong Li,1,* Chenye Lin,2,* Qianyun Wang,3,* Li Zhang,4 Zhirong Zhu,5 Feng Cheng,1 Bin Wang1
1Department of Clinical Laboratory, Fujian Children’s Hospital (Fujian Branch of Shanghai Children’s Medical Center), College of Clinical Medicine for Obstetrics and Gynecology and Pediatrics, Fujian Medical University, Fuzhou, Fujian, People’s Republic of China; 2Department of Respiratory, Fujian Children’s Hospital (Fujian Branch of Shanghai Children’s Medical Center), College of Clinical Medicine for Obstetrics and Gynecology and Pediatrics, Fujian Medical University, Fuzhou, Fujian, People’s Republic of China; 3Department of Clinical Laboratory, Wu Mengchao Memorial Hospital of Fujian Medical University, Fuzhou, Fujian, People’s Republic of China; 4Department of Laboratory Medicine, the School of Medical Technology and Engineering, Fujian Medical University, Fuzhou, Fujian, People’s Republic of China; 5Information Center, Fujian Children’s Hospital (Fujian Branch of Shanghai Children’s Medical Center), College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, Fuzhou, Fujian, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Feng Cheng, Department of Clinical laboratory, Fujian Children’s Hospital (Fujian Branch of Shanghai Children’s Medical Center), College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, Fuzhou, 350000, People’s Republic of China, Email [email protected] Bin Wang, Department of Clinical laboratory, Fujian Children’s Hospital (Fujian Branch of Shanghai Children’s Medical Center), College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, Fuzhou, 350000, People’s Republic of China, Email [email protected]
Rational: The incidence of pediatric respiratory allergic diseases is rising annually. However, no study has systematically investigated the spectrum of inhalant allergens in children from Fuzhou, China, using ImmunoCAP assay technology and cohort analysis. This study aimed to characterize the distribution of allergen-specific IgE (sIgE) in children aged 0– 14 years with respiratory allergies in Fuzhou, providing theoretical support for etiological diagnosis, treatment, and prevention.
Methods: A total of 196 children underwent allergen screening: 116 diagnosed with allergic rhinitis (AR) and 80 with asthma (AS). Serum sIgE antibodies against inhalant allergens were detected using the ImmunoCAP system.
Results: In the AR group, Dermatophagoides pteronyssinus (d1) showed the highest sensitization rate (112/116), followed by Dermatophagoides farinae (d2) (110/116). In the AS group, d1 and d2 had equally high positivity rates (both 78/80), while Blattella germanica (i6) sensitization was significantly higher in AS than in AR. Sensitization to the animal epithelium panel (ex1) differed significantly between diseases in the 4-6-year age group. Correlation analysis revealed a strong positive correlation between tree pollen mix (tx5) and weed pollen mix (wx5) in both groups, and a significant correlation between d2 and d1.
Conclusion: Dermatophagoides pteronyssinus (d1) and D. farinae (d2) are the predominant allergens in pediatric respiratory allergies in Fuzhou. This study offers valuable insights for preventing and treating these conditions.
Keywords: respiratory allergic diseases, children, specific IgE, Immuno-CAP system
Introduction
The global incidence of allergic diseases has shown a consistent upward trend over the past few decades, with asthma (AS), allergic rhinitis (AR), and atopic dermatitis (AD) demonstrating particularly marked increases in prevalence.1 Pediatric populations exhibit disproportionate vulnerability, where severe manifestations potentially progress to fatal outcomes while imposing substantial psychological distress and socioeconomic burdens on affected families.2 These disorders essentially reflect maladaptive immune responses to exogenous proteins, mediated via complex multifactorial regulatory mechanisms. Allergenicity is determined not solely by protein molecular characteristics, but also by the synergistic interactions among exposure parameters (dose and duration), environmental cofactors, and Th2- polarizing immunomodulatory components within allergens.3
As the core effector molecule in allergic reactions, the identification of allergen- specific IgE (sIgE) established the theoretical basis for Th2- type immune responses that contribute to disease progression.4 sIgE levels demonstrate dose- dependent correlations with disease susceptibility, where polysensitization confers exponentially increased risk.5 Substantial evidence supports the pivotal role of sIgE- mediated sensitization to aeroallergens (such as dust mites, pollens, fungal spores) in the development of respiratory allergies, particularly AS and AR.6 Upon inhalation, aeroallergen- sIgE complexes bind high-affinity FcεRI receptors on mast cells, triggering degranulation and histamine- mediated immediate hypersensitivity reactions that manifest as acute bronchospasm or rhinorrhea. Chronic exposure perpetuates Th2- polarized inflammation via sustained IgE- FcεRI signaling, thereby exacerbating airway hyperresponsiveness and correlating directly with clinical severity.4 This mechanistic cascade positions sIgE as both a core biomarker and a therapeutic target in the management of allergic airway disease.
Allergen distribution patterns demonstrate spatiotemporal variability influenced by climatic conditions, geographic features, and anthropogenic factors, with significant interindividual response variations across age groups and genders.3 Wang B et al have demonstrated that allergic diseases typically manifest early in life and may decline progressively with age. Furthermore, during childhood, the incidence of allergic diseases is generally higher in boys than in girls.7,8 Systematic investigation of allergic pathogenesis requires a comprehensive analysis of allergen generation mechanisms, spatial dispersion dynamics, and physicochemical characteristics. Developing region- specific allergen distribution profiles emerge as an essential prerequisite for the implementation of precision allergy prevention strategies.
Clinically, allergen diagnostics predominantly rely on skin prick testing and serum sIgE quantification. In comparison to in vivo methods, sIgE immunoassays provide several distinct advantages: component- resolved diagnostics that address the limitations of extract- based approaches, improved safety especially for pediatric applications, and consistent technical reproducibility independent of cutaneous reactivity or operator- dependent techniques.9 The ImmunoCAP system is recognized as the global gold standard for sIgE detection, providing standardized quantitative analysis with exceptional reproducibility. In addition to diagnosing sensitization to inhalant or food allergens, the ImmunoCAP system’s quantification of sIgE levels facilitates risk stratification for symptom progression and aids in the selection of candidates for immunotherapy.10
This epidemiological study systematically investigated the patterns of allergic rhinitis (AR) and asthma (AS) in children from Fuzhou, Fujian Province, China. The study quantified sIgE levels for seven inhalant allergens using the ImmunoCAP system. Statistical analyses comparing sensitization rates and profiles across age and sex subgroups offer evidence- based insights to guide precision prevention strategies and personalized management approaches for pediatric respiratory allergies.
Materials and Methods
Study Population
This retrospective cohort study assessed clinically confirmed AR and AS cases that were managed via outpatient or inpatient care at Fujian Provincial Children’s Hospital between January 2023 and August 2024. Children aged 0–14 years with at least one positive inhalant allergen were included in the study. Demographic characteristics, including age and gender, as well as sIgE profiles for common inhalant allergens, were systematically collected. Diagnostic confirmation was based on the guidelines from ARIA (Allergic Rhinitis and its Impact on Asthma) and GINA (Global Initiative for Asthma consensus guidelines).11 All children who visited our hospital and met the above inclusion criteria in our manuscript were continuously recruited as potential research subjects. This retrospective study received ethics approval with a waiver of informed consent (Approval No.: 2025ETKLRK04002). The requirement for consent was waived by the ethics committee because the research involved only the analysis of pre-existing, anonymized patient records, posing minimal risk to participants. No patient intervention or identifiable information was used. The researchers verify that all studies were conducted in compliance with the applicable guidelines and regulations for research involving human participants, including the the Declaration of Helsinki or equivalent standards.
sIgE Analysis
Following blood collection, 3 mL of venous blood was obtained from each participant. The samples were allowed to clot at room temperature for 1 hour and then centrifuged at 4,000 rpm for 10 minutes to separate the serum. The resulting serum aliquots were stored at 4°C and analyzed for sIgE and tIgE levels either on the same day or within two days. Quantitative measurement of sIgE reactivity to inhalant allergens was conducted using the Phadia 1000 automated fluorescence enzyme immunoassay system (Phadia AB, Uppsala, Sweden) with manufacturer-calibrated reagents. The allergen panel consisted of the following components: an animal epithelium panel (ex1) including cat, dog, cattle, and horse dander; a fungal mix (mx2) comprising Penicillium chrysogenum, Cladosporium herbarum, Aspergillus fumigatus, Candida albicans, and Alternaria alternata; a weed pollen mix (wx5) consisting of ragweed, mugwort, daisy, dandelion, and goldenrod; a tree pollen mix (tx5) encompassing grey alder, hazel, elm, willow, and poplar; Blattella germanica (i6); Dermatophagoides pteronyssinus (d1); and Dermatophagoides farinae (d2). Strict adherence to the manufacturer’s protocols ensured consistent quality control and standardized sample processing. sIgE quantification was performed according to the World Allergy Organization (WAO) diagnostic thresholds, with sensitization positivity defined as ≥ 0.35 IU/mL.11 Semiquantitative grading was applied as follows: Class 0 (<0.35 IU/mL, subthreshold), Class 1 (0.35–0.7 IU/mL, low), Class 2 (0.7–3.5 IU/mL, moderate), Class 3 (3.5–17.5 IU/mL, high), Class 4 (17.5–50 IU/mL, very high), Class 5 (50–100 IU/mL, extremely high), and Class 6 (≥100 IU/mL, ultra- high). This classification ensures a granular stratification of allergic sensitization intensity.
Statistical Analysis
Analytical procedures were performed using SPSS 29.0. Categorical variables were presented as frequencies or percentages, and between-group comparisons of sensitization rates were assessed using χ2-tests. Continuous variables that were not normally distributed were analyzed with the Mann–Whitney U-test, a robust non-parametric alternative. Two-tailed hypothesis testing was applied throughout the analysis. Fisher’s exact test was used instead of χ2 analysis when expected cell frequencies did not meet the threshold requirements. A significance level of P < 0.05 was predefined for all inferential statistics. Data visualization was conducted using R’s ggplot2 package to generate correlation heatmaps and stratified bar plots, supplemented by radar charts created with the ggradar package after data preprocessing using dplyr.
Results
General Characteristics of the Study Cohort
The analysis encompassed 196 participants, consisting of 116 AR cases and 80 AS cases. Demographic evaluation indicated a male predominance in both disease groups. Sensitization profiling revealed prevalent polysensitization patterns, where most cases showed concurrent reactivity to two or three dominant allergens. Detailed demographic distributions and allergen co-occurrence matrices are summarized in Table 1.
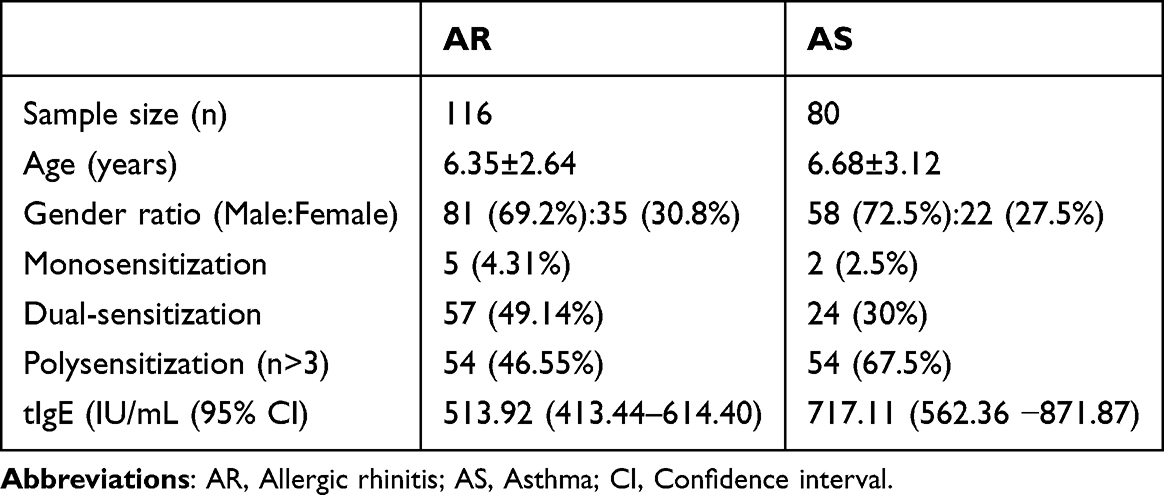 |
Table 1 Clinical Characteristics and Total IgE Levels in 196 Pediatric Cases |
sIgE Seroprevalence Across Disease Cohorts
A comparative analysis of the sensitization profiles between AR and AS cohorts revealed nearly identical immunodominance hierarchies among the seven inhalant allergens (Table 2). In the AR group, the highest sensitization rates were observed for d1 (96.5%, 112/116), followed by d2 (94.8%, 110/116). By contrast, AS patients exhibited comparable peak sensitization frequencies for both d1 and d2 (98.5%, 78/80 each). Statistical analysis indicated that the positive rate of i6 was significantly higher in AS than in AR (p = 0.029). No statistically significant differences were detected in the positive rates of the remaining six allergens between the two disease groups (p > 0.05).
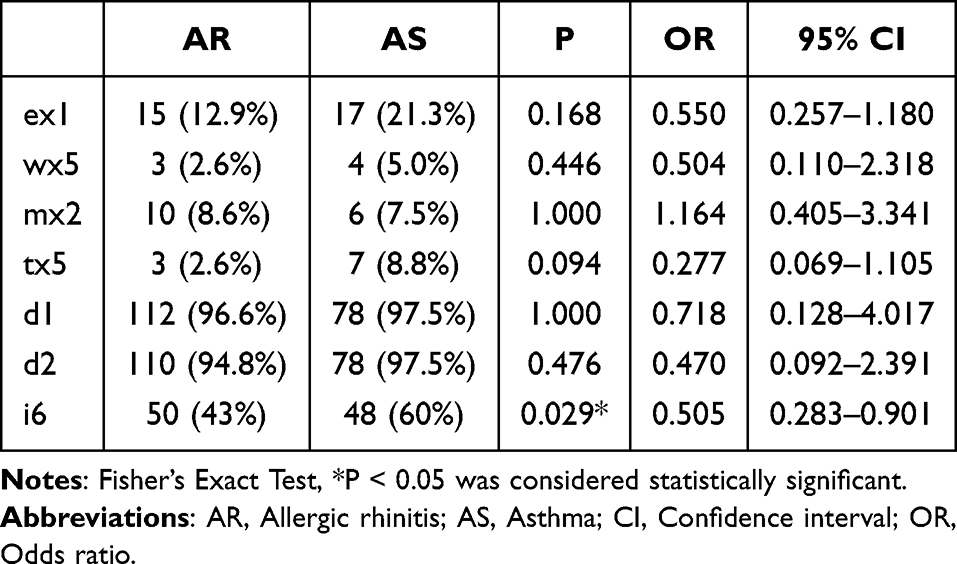 |
Table 2 Allergen Sensitization Profiles in AR and AS Cohorts |
Age-Stratified Sensitization Patterns and Gender-Specific Sensitization Profiles
Age-stratified analysis (0–3 years, 4–6 years, 7–14 years cohorts; Table 3) demonstrated a consistent increase in the prevalence of sensitization to all seven allergens with advancing age. The positivity rate of ex1 was significantly higher in AS than in AR (p < 0.05) among the 4-6-year cohorts, while the remaining six allergens showed no statistically significant differences (p > 0.05) at various ages across both disease groups. Sex-stratified analysis revealed consistent immunodominance hierarchies across both AR and AS cohorts, with d1, d2, and i6 showing the highest sensitization prevalence in both males and females. No statistically significant gender-specific differences in seropositivity rates were observed for any of the seven allergens within disease subgroups (p > 0.05), as detailed in Tables 4 and 5.
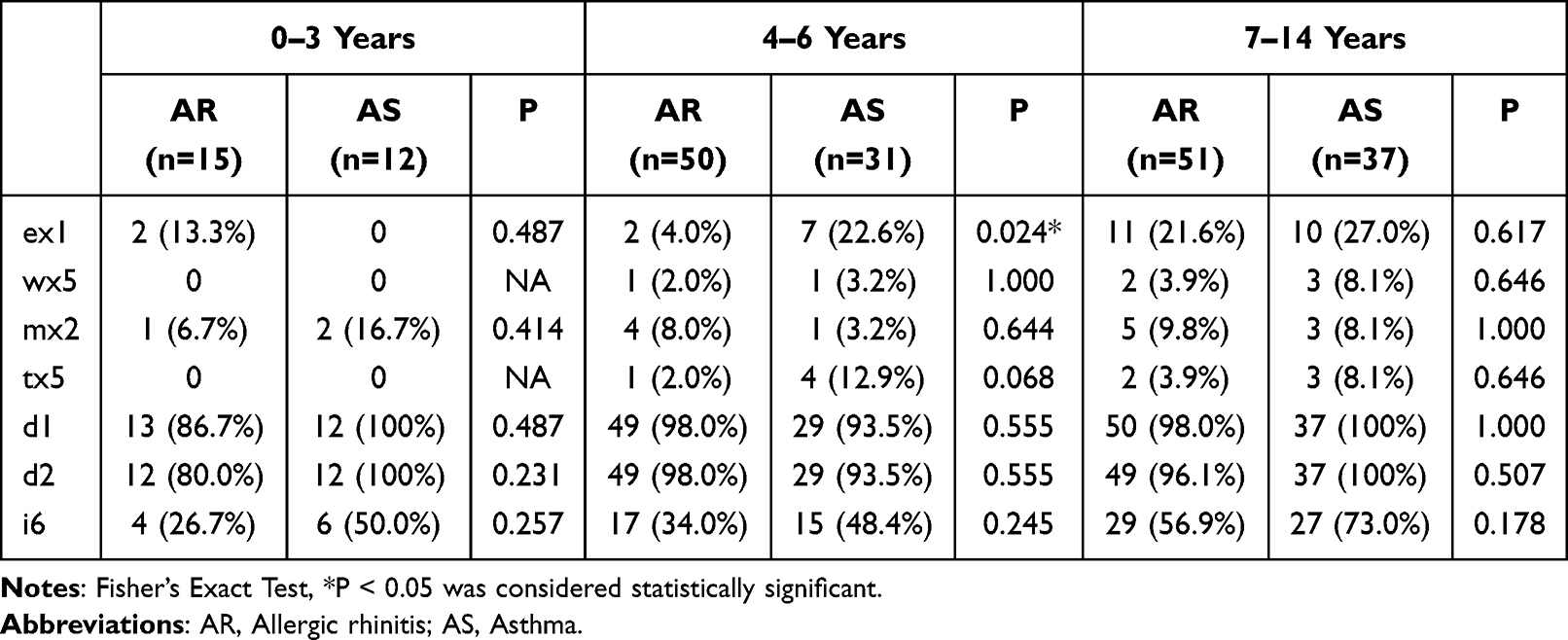 |
Table 3 Age-Stratified Allergen Sensitization Profiles in AR and AS Cohorts |
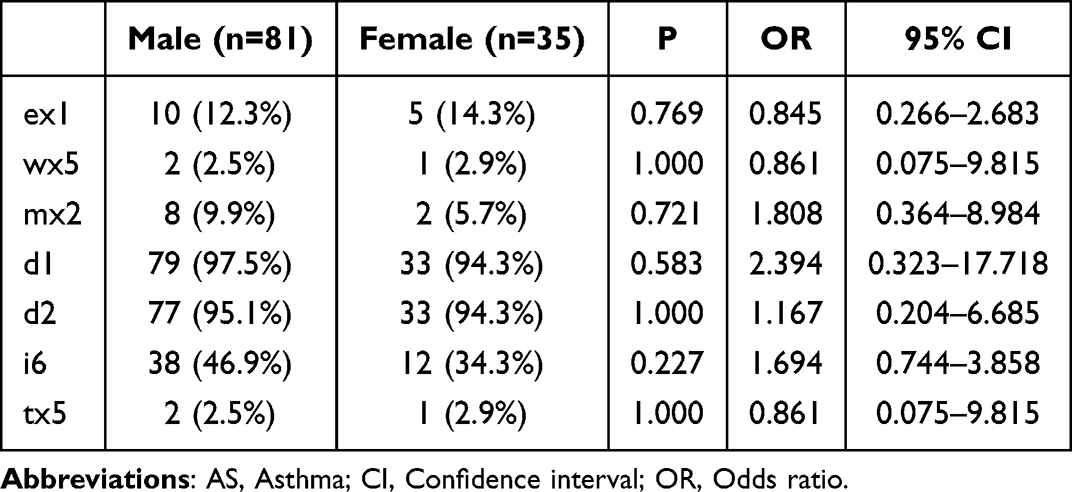 |
Table 4 Gender-Specific Allergen Sensitization Profiles in the AS Cohort |
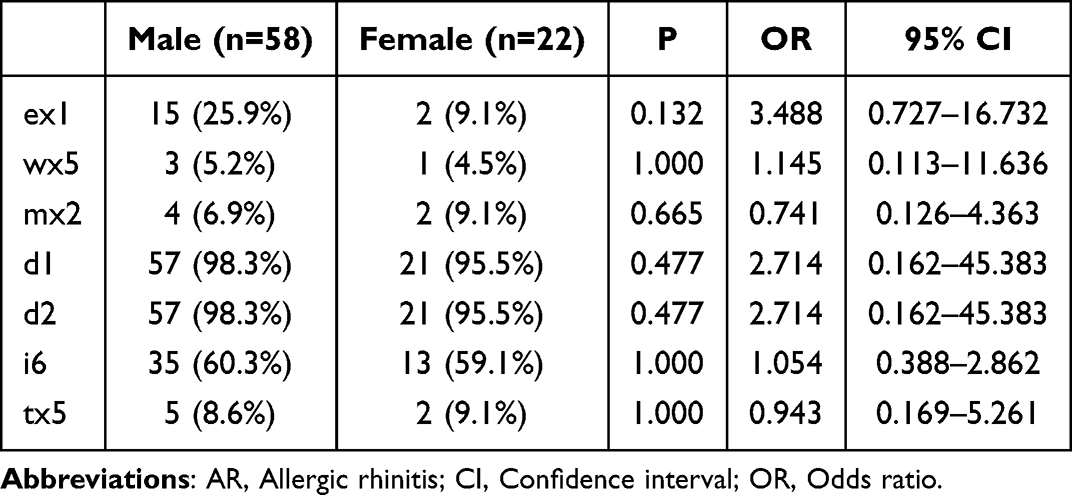 |
Table 5 Gender-Specific Allergen Sensitization Profiles in the AR Cohort |
Allergen Correlation Patterns Across Disease Cohorts
Spearman analysis uncovered distinct inter-allergen covariation profiles between the AR and AS groups. In the AR group, tx5 showed near-perfect concordance with wx5 (ρ= 0.95, p < 0.01), paralleled by robust cross-reactivity of Dermatophagoides spp. allergens (d1-d2: ρ= 0.84, p < 0.001), whereas other allergen pairs exhibited negligible associations (ρ< 0.5). In contrast, AS patients demonstrated even stronger codominance between tx5 and wx5 (ρ= 0.99, p < 0.001) and greater synchrony among mite allergens (d1-d2: ρ= 0.86, p < 0.001), with non-significant correlations observed for all other antigen pairs (ρ< 0.5) (Figure 1A and B).
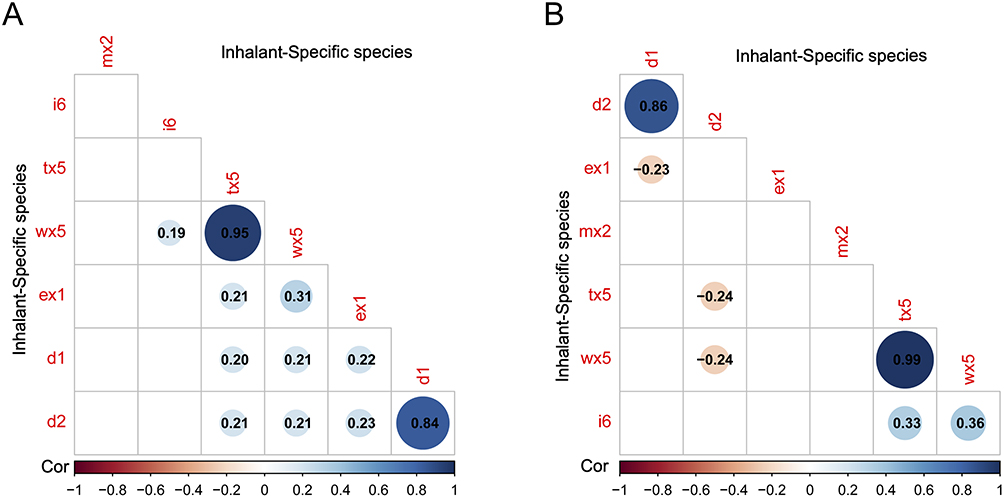 |
Figure 1 (A) Spearman correlation analysis of seven allergen sIgE in AR. (B) Spearman correlation analysis of seven allergen sIgE in AS. |
Distribution of d1-sIgE and d2-sIgE Levels at Different Disease Groups
In the AR group, the levels of d1-and d2-sIgE were predominantly at levels 4 and 5, respectively, whereas the remaining allergens were mostly at level 0 (Figure 2A). In the AS group, the levels of d1-and d2-sIgE were primarily distributed across levels 4, 5, and 6, while the other allergens were largely at level 0 (Figure 2B).The radar chart depicting the allergen level distribution for d1, d2, and i6 reveals that in the AR group, the highest positive rate of ex1 occurred when d1 was at level 2 (Figure 3A); the highest positive rate of d1 across all levels from 1 to 6 was observed when d2 was at level 6 (Figure 3B); the highest positive rate of ex1 was noted when i6 was at level 1, while the highest positive rates of d1 and d2 were observed at levels 2 and 3 of i6 (Figure 3C). In the AS group, the highest positive rate of ex1 occurred when d1 was at level 0, and the highest positive rate of i6 was observed when d1 was at level 1 (Figure 3D); the highest positive rate of d1 across all levels from 1 to 6 was seen when d2 was at level 6 (Figure 3E); the highest positive rates of d1 and d2 were observed when d2 was at levels 1 to 3 (Figure 3F).
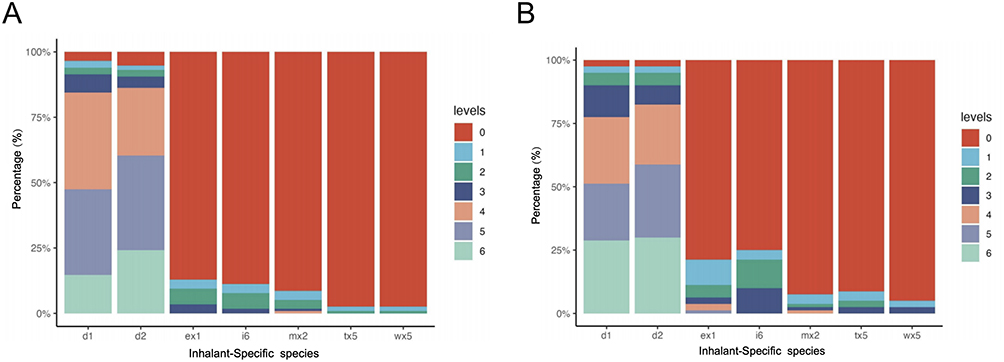 |
Figure 2 (A) Distribution of sIgE levels for seven allergens in AR. (B) Distribution of sIgE levels for seven allergens in AS. |
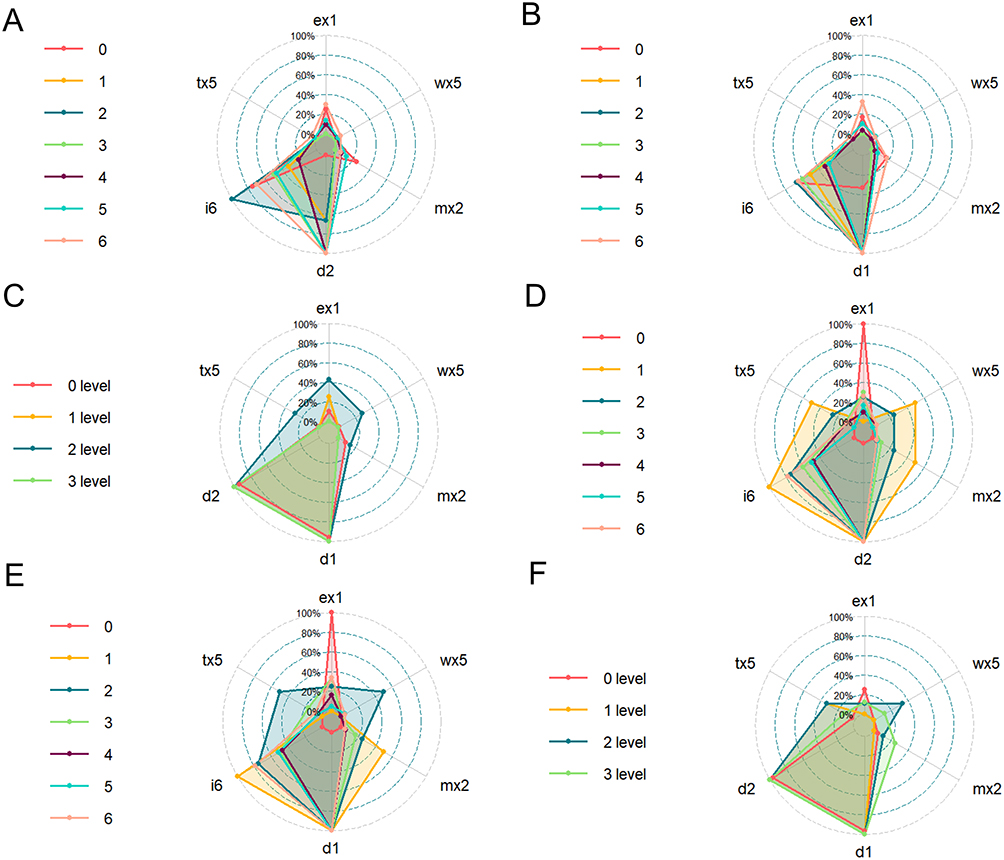 |
Figure 3 (A) Radar chart analysis of the influence of d1 sensitization level on the positive rates of other allergens in AR. (B) Radar chart analysis of the influence of d2 sensitization level on the positive rates of other allergens in AR. (C) Radar chart analysis of the influence of i6 sensitization level on the positive rates of other allergens in AR. (D) Radar chart analysis of the influence of d1 sensitization level on the positive rates of other allergens in AS. (E) Radar chart analysis of the influence of d2 sensitization level on the positive rates of other allergens in AR. (F) Radar chart analysis of the influence of i6 sensitization level on the positive rates of other allergens in AS. |
Discussion
The escalating global burden of allergic diseases has catalyzed an epidemiological transition, underscoring the imperative of allergy management as a critical public health priority. Epicutaneous sensitization, facilitated by impaired cutaneous barrier function, triggers a cascade of immunological responses, promoting localized type 2 inflammation and systemic immune dysregulation, which in turn predisposes individuals to the development of atopic march disorders, such as AD, AR, and AS.12 Geospatial heterogeneity analyses reveal distinct region- specific sensitization profiles influenced by synergistic environmental- climatic factors and anthropogenic modifications,11 underscoring the necessity for localized allergen surveillance systems. Emerging molecular allergology approaches reveal that longitudinal monitoring of personalized sensitization signatures, especially the precise identification of evolving allergen cluster dynamics and IgE epitope spreading patterns, facilitates predictive stratification of high-risk cohorts. Emerging molecular allergology approaches, which enable the monitoring of personalized sensitization signatures and allergen cluster dynamics, hold potential to inform future prevention strategies. These may include school-based interventions or targeted environmental controls, aimed at microbiome modulation and allergen avoidance prior to irreversible Th2 immune polarization.13 However, validation of these approaches necessitates well-designed longitudinal and interventional studies.
Located on the southeast coast of China, between longitudes 118°08’ - 120°31’ E and latitudes 25°15’ - 26°39’ N, Fuzhou exhibits a typical subtropical maritime monsoon climate. The city is continuously influenced by oceanic monsoons throughout the year, creating ideal biotopes for the perennial proliferation of Dermatophagoides spp. and Aerophilic fungi. Despite this environment that predisposes individuals to allergies, there remains a significant lack of data concerning pediatric sIgE sensitization profiles in populations with AR and AS.
This investigation encompassed 116 pediatric AR cases and 80 pediatric AS cases, revealing that more than 50% of children in both disease groups exhibited significantly positive serum sIgE levels to at least one antigen within the tested allergen profiles. A population-based study conducted by Huang Z et al14 investigated sensitization profiles among 1,722 children aged 0–14 years in Sichuan Province and revealed that a substantial proportion of participants exhibited polysensitization (concurrent specific immune reactivity to ≥2 allergens). This finding highlights the potential mechanistic role of cross- sensitization or co- sensitization between distinct allergenic sources in the development of pediatric allergic disorders within this geographic cohort. A cross-sectional study conducted at a pediatric clinic in New York demonstrated that 63.6% of children exhibited consistent evidence of heightened allergic sensitization to at least one aeroallergen, as corroborated by both questionnaire self-reports and serum sIgE seropositivity.15 This result aligns with existing epidemiological data, providing further support for the convergent validity and reinforcing the methodological rigor and reproducibility of the dataset used in this study.
This study reveals that the high sensitization rates of d1, d2, and i6 are ranked among the top three in both AR and AS cohorts. This phenomenon may be attributed to the humid and hot climate in Fuzhou, which promotes the growth and reproduction of dust mite populations, as well as the widespread exposure to cockroaches in urban living environments. Scholars such as Wang et al conducted multicenter research in four cities in southern China and found that the sIgE positivity rate for the mixture of cockroach and mite allergens was highest in Liuzhou City, Guangxi Province. This may be attributed to the region’s humid and hot climate, as subtropical and tropical areas typically exhibit higher humidity and temperature levels, which are conducive to the growth and reproduction of dust mites. As a coastal city in southern China, Shenzhen has a relatively dry climate throughout the year, particularly in summer when temperatures remain around 22.4 °C, making it less favorable for mite proliferation.3 In Shanghai (an coastal city in eastern China), house dust mites are among the most common inhaled allergens associated with respiratory diseases in children.11 Researchers have also confirmed that house dust mites are the predominant allergen in Chinese patients with asthma and/or rhinitis.16
In this study, the positive rate of sIgE in ex1 ranked fourth among the seven allergens, likely attributed to children’s frequent interaction with pets and their close contact. Consistent with these findings, Sun’s research also demonstrated a significant 16% increase in the positive rate of sIgE for cat and dog hair among young individuals.17 In addition, our study suggested that the positive rate of Blattella germanica allergen exposure (i6) was significantly higher in patients with AS than in those with AR (Table 2). Consistent with our findings, Rocchi S et al reported that in pediatric populations, Blattella germanica allergens were associated with a higher incidence of asthma compared to other common allergens, such as dust mites, cats, and dogs.18 The aforementioned finding provides further compelling evidence to support the prevention and treatment strategies for childhood asthma (AS). In the future, focusing on the eastern and southeastern coastal regions of China, the comprehensive control of Blattella germanica and the modification of their habitats and breeding environments may significantly contribute to asthma prevention efforts.
Comparative age- stratified analysis revealed significant immunological divergence in sensitization profiles, with ex1 showing a higher seroprevalence in the AS cohort compared to the AR cohort, indicative of preferential upper respiratory tract tropism for fur- derived allergens. Although wx5, mx2, tx5, and i6 allergens exhibited no significant inter- group variation, their sensitization gradients demonstrated a progressive age-dependent increase (Table 3). The age-related rise in sensitization is driven by two immunological mechanisms: the maturation of the thymic T-cell repertoire, which enhances effector responses, and the prolonged duration of exposure to environmental allergens.19 Notably, d1 and d2 demonstrated non- linear sensitization trajectories across age quartiles, which may reflect either statistical power limitations in this single- center cross-sectional cohort or ceiling effects associated with perennial mite allergen sensitization. These patterns are consistent with Wang et al3‘s pediatric surveillance data, which reveal an annual increase in aeroallergen sIgE seroconversion rates, presumably driven by gene- environment interactions that exacerbate age-related immune dysregulation.
Emerging evidence suggests that genetic polymorphisms and early-life endocrine exposures play critical roles in gender-dimorphic allergic sensitization. Specifically, prenatal androgen exposure and postnatal estrogen-progesterone dynamics may predispose males to increased IgE-mediated reactivity during prepubescent stages.20,21 This also indicates that the incidence of allergic diseases is higher in males than in females, which aligns with our findings (Table 1). On the contrary, a growing body of evidence suggests that women experience a higher incidence of allergic diseases compared to men. Firstly, sex hormones such as estrogen can increase susceptibility to allergies by modulating Th2- type immune responses. Secondly, the functional characteristics of the female skin barrier may facilitate allergen penetration. Additionally, differences in environmental exposure patterns within the female population further contribute to an elevated risk of developing allergies.7 Our null findings regarding gender-based sensitization disparities in AR and AS cohorts may be attributed to three non-exclusive factors: first, the limited statistical power inherent in subgroup analyses; second, geoclimatic factors that exert homogenizing effects on sensitization patterns across genders; third, the allergen spectrum failing to encompass allergens known for gender-specific differences. Future investigations integrating longitudinal cohort studies with epitope-resolved IgE profiling are essential to unravel these complex gene-environment-hormone interactions in allergic progression.
This study analyzed the sIgE detection data of AR and AS and found a significant correlation pattern between their allergen sensitization characteristics, specifically manifested as a high correlation between d2 and d1. This finding is consistent with trends reported in previous studies.9,22 There is a significant correlation between wx5 and tx5, a finding that has been rarely documented in both domestic and international literature. This correlation may stem from their biological similarities and analogous protein structures. Additionally, the overlap of pollen seasons among certain trees and herbaceous plants could contribute to cross-reactivity. Unlike previous studies, our findings revealed that the levels of d1-sIgE and d2-sIgE in the two diseases were predominantly distributed across grades 4, 5, and 6 (Figure 2). This indicates that clinical practitioners can more precisely develop personalized management strategies and identify optimal targets for desensitization therapy. Additionally, the study demonstrated that as the levels of d1-sIgE and d2-sIgE progressively increased, sensitization to other allergens also rose. This suggests that single-target desensitization therapy may not be the most effective approach in clinical practice.
While this investigation has generated clinically relevant findings, several methodological limitations necessitate careful consideration. First, the single-center design with geographically constrained sampling may compromise generalizability due to potential confounding by region-specific climatic factors and population genetic stratification. Second, the cross-sectional approach, although effective in characterizing concurrent sensitization patterns, does not permit temporal inference regarding causal pathways in allergic progression. Third, the limited sample size led to underpowered subgroup analyses, which may have masked clinically meaningful effect sizes. Fourth, the allergen panel’s exclusive focus on inhalant antigens excluded the assessment of potentially relevant food allergens. Therefore, in future research, we propose combining multi-center cohort validation with expanded longitudinal studies to enhance the level of evidence.
Conclusions
This study reveals a dynamic interplay between gender, age, and allergen sensitivity, offering a new theoretical foundation for allergy research. By synthesizing existing evidence, it enhances the understanding of molecular characteristics of allergens and their regional variations, while informing more effective clinical diagnosis and treatment strategies. We propose multidimensional interventions: controlling house dust mites in domestic environments through measures such as using anti-mite bedding and maintaining indoor humidity below 50%, mitigating cockroach allergens in urban public spaces, and advancing personalized immunotherapy via molecular diagnostics. Future research should incorporate multi-center studies and longitudinal validation to enhance the generalizability of the findings.
Data Sharing Statement
Due to the respect to and the protection of patient privacy, the data generated and/or analyzed in this study are not publicly available. However, the data generated and analyzed during this study are available upon reasonable request from the corresponding author, Dr. Bin Wang (email: [email protected]).
Ethics Approval
This study was approved by the Medical Ethics Committee of Fujian Children’s Hospital (2025ETKLRK04002).
Funding
This work was supported by the Natural Science Foundation of Fujian Province, China (2022J01438).
Disclosure
Yadong Li, Chenye Lin, and Qianyun contributed equally to this work and shared first authorship. The authors declare no conflicts of interest.
References
1. Yang C, Zeng Q, Lu G, Li H, Liu W. A retrospective comparison of aeroallergen sensitization among different allergic diseases in Guangzhou, China. Mediators Inflamm. 2024;2024:8896646. doi:10.1155/mi/8896646
2. Yang L, Gao K, Gong W, et al. Sources of allergens detected through allergen-specific serum ige antibody test in children with suspected allergic diseases in central China. J Asthma Allergy. 2024;17:769–781. doi:10.2147/jaa.S469503
3. Wang X, Zhou L, Wei G, Zhang H, Yang B. Prevalence of allergen-specific IgE in southern China: a multicenter research. Aging. 2021;13(14):18894–18911. doi:10.18632/aging.203341
4. Irahara M, Yamamoto-Hanada K, Saito-Abe M, et al. Fluctuations of aeroallergen-specific immunoglobulins and children’s allergic profiles: Japan environment & children’s study of a pilot cohort. Allergol Inter. 2022;71(3):335–344. doi:10.1016/j.alit.2022.01.002
5. Zhang W, Xie B, Liu M, Wang Y. Associations between sensitisation to allergens and allergic diseases: a hospital-based case-control study in China. BMJ Open. 2022;12(2):e050047. doi:10.1136/bmjopen-2021-050047
6. Tanaka J, Fukutomi Y, Shiraishi Y, et al. Prevalence of inhaled allergen-specific IgE antibody positivity in the healthy Japanese population. Allergol Inter. 2022;71(1):117–124. doi:10.1016/j.alit.2021.08.009
7. Wang B, Zhang D, Jiang Z, et al. Analysis of allergen positivity rates in relation to gender, age, and cross-reactivity patterns. Scientific Reports. 2024;14(1):27840. doi:10.1038/s41598-024-78909-y
8. Gutiérrez-Brito JA, Lomelí-Nieto JA, Muñoz-Valle JF, et al. Sex hormones and allergies: exploring the gender differences in immune responses. Frontiers in Allergy. 2024;7(5):1483919. doi:10.3389/falgy.2024.1483919
9. Liao CX, Huang DM, Hu HS, et al. Analysis of serum allergen-specific IgE in children with respiratory allergic disease in Guangdong. Zhonghua yu fang yi xue za zhi. 2021;55(5):613–619. doi:10.3760/cma.j.cn112150-20201217-01467
10. Takahagi S, Moriwaki M, Ishii K, Asakura N, Hide M. Detection of anti-MGL_1304 IgE using the ImmunoCAP system for diagnosis of type I allergy to sweat. Allergol Inter. 2025;74(2):316–324. doi:10.1016/j.alit.2024.11.004
11. Ying X, Qi X, Yin Y, et al. Allergens sensitization among children with allergic diseases in Shanghai, China: age and sex difference. Resp Res. 2022;23(1):95. doi:10.1186/s12931-022-02008-7
12. Engebretsen KA, Thyssen JP. Skin barrier function and allergens. Curr Probl Dermatol. 2016;49:90–102. doi:10.1159/000441548
13. Shaker M. New insights into the allergic march. Curr Opinion Pediatrics. 2014;26(4):516–520. doi:10.1097/mop.0000000000000120
14. Huang Z, Feng W, Wei W, Yang B, Wang L. Prevalence of food-allergen and aeroallergen sensitization among people in Sichuan, Western China: an 8-year observational study. J Clin Laboratory Analysis. 2019;33(3):e22723. doi:10.1002/jcla.22723
15. Pham MN, Andrade J, Mishoe M, Chun Y, Bunyavanich S. Perceived versus actual aeroallergen sensitization in urban children. J Allergy Clin Immunol Prac. 2019;7(5):1591–1598.e4. doi:10.1016/j.jaip.2018.12.026
16. Wang W, Wang J, Song G, et al. Environmental and sensitization variations among asthma and/or rhinitis patients between 2008 and 2018 in China. Clin Transl Allergy. 2022;12(2):e12116. doi:10.1002/clt2.12116
17. Sun X, Zhao J, Wang Q, Shi G, Yang J, Ming L. Prevalence of allergen sensitization among 15,534 patients with suspected allergic diseases in Henan Province, China. Asian Pacific J Allergy Immunol. 2019;37(2):57–64. doi:10.12932/ap-160817-0137
18. Rocchi S, Valot B, Laboissière A, et al. Development of a cockroach (Blattella germanica) qPCR for the objective measurement of exposure at home. Sci Total Environ. 2023;864:160965. doi:10.1016/j.scitotenv.2022.160965
19. Liu T, Lai SY, Li WS, Jiang YM. Prevalence of food allergen and aeroallergen sensitization among children in Sichuan province. Medicine. 2020;99(27):e21055. doi:10.1097/md.0000000000021055
20. Uekert SJ, Akan G, Evans MD, et al. Sex-related differences in immune development and the expression of atopy in early childhood. J Allergy Clin Immunol. 2006;118(6):1375–1381. doi:10.1016/j.jaci.2006.09.008
21. Leffler J, Stumbles PA, Strickland DH. Immunological processes driving ige sensitisation and disease development in males and females. Inter J Molecular Sci. 2018;19(6):1554. doi:10.3390/ijms19061554
22. Liu X, Zheng P, SG Z, et al. Co-sensitization and cross-reactivity of Blomia tropicalis with two Dermatophagoides species in Guangzhou, China. J Clin Laboratory Analysis. 2019;33(9):e22981. doi:10.1002/jcla.22981
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.