Back to Journals » International Journal of Nanomedicine » Volume 20
Inhalable Exosomes in Respiratory Therapies with the Transformative Potential
Authors Gou J, Zhang L ![]() , Wang G, Li Z, Yin Q, Pan Y
, Wang G, Li Z, Yin Q, Pan Y ![]()
Received 11 June 2025
Accepted for publication 8 September 2025
Published 28 November 2025 Volume 2025:20 Pages 14219—14252
DOI https://doi.org/10.2147/IJN.S545306
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yan Shen
Jinming Gou,1,* Lina Zhang,2,* Guowei Wang,3 Zhiqi Li,2 Qimin Yin,4 Yuanming Pan2
1Department of General Practice, Troops of the People’s Liberation Army, Urumqi, Xinjiang, 830009, People’s Republic of China; 2Cancer Research Center, Beijing Chest Hospital, Capital Medical University, Beijing Tuberculosis & Thoracic Tumor Research Institute, Beijing, 101149, People’s Republic of China; 3Department of Geriatric Medicine, General Hospital of Xinjiang Military Command, Urumqi, Xinjiang, 830000, People’s Republic of China; 4Department of Respiratory and Critical Care Medicine, Beijing Chest Hospital, Capital Medical University, Beijing Tuberculosis & Thoracic Tumor Research Institute, Beijing, 101149, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yuanming Pan, Cancer Research Center, Beijing Chest Hospital, Capital Medical University, Beijing Tuberculosis & Thoracic Tumor Research Institute, No. 9 Beiguan Street, Tongzhou District, Beijing, 101149, People’s Republic of China, Tel/Fax +86 10 89509372, Email [email protected] Qimin Yin, Department of Respiratory and Critical Care Medicine, Beijing Chest Hospital, Capital Medical University, Beijing Tuberculosis & Thoracic Tumor Research Institute, No. 9 Beiguan Street, Tongzhou District, Beijing, 101149, People’s Republic of China, Tel/Fax +86 10 89509000, Email [email protected]
Abstract: Exosomes are nanoscale extracellular vesicles secreted by various cell types and have become key mediators of intercellular communication, immune regulation, and tissue regeneration. With advancements in inhalable or nebulized formulations, their potential as therapeutic agents has been significantly enhanced, allowing for targeted delivery to the respiratory system while minimizing systemic side effects. This review provides a comprehensive overview of the fundamental biology, biogenesis, and cargo composition of exosomes, emphasizing their role in intercellular signaling and low immunogenicity. The rationale for local pulmonary delivery is discussed, highlighting advantages such as enhanced bioavailability, reduced systemic exposure, and improved patient compliance. Current preclinical and clinical studies demonstrate the efficacy of inhaled exosomes in treating acute lung injury (ALI), acute respiratory distress syndrome (ARDS), chronic obstructive pulmonary disease (COPD), pulmonary fibrosis and lung cancer. Additionally, exosomes exhibit promising immunomodulatory and anti-aging properties, including macrophage polarization, alleviation of cytokine storms, and mitochondrial restoration. Challenges surrounding large-scale production, standardization, and regulatory approval are addressed, while the prospects for engineering exosomes with enhanced payloads and specificity are envisioned. The combination of nanotechnology and biomimetic systems, along with personalized medicine approaches, underscores the transformative potential of inhaled exosomes in respiratory and systemic therapies.
Keywords: exosomes, inhalation therapy, respiratory diseases, immune regulation, anti-aging
Introduction
The exploration of extracellular vesicles, particularly exosomes, has redefined our understanding of cell communication and opened new avenues for therapeutic intervention. Exosomes are nanoscale vesicles secreted by nearly all cell types and have become important participants in intercellular signaling, immune regulation, and tissue regeneration, even serving as carriers for targeted drug delivery. In recent years, increasing attention has focused on the development of inhalable or nebulized exosome formulations for the treatment of respiratory diseases, immune disorders, and even age-related diseases. This review provides a comprehensive overview of the basic biology of exosomes, explains the rationale for their targeted delivery to the lungs, outlines the current state of preclinical and clinical research, and discusses the prospects for utilizing inhalable exosomes as a novel therapeutic approach.
Basic Concept and Biological Characteristics of Exosomes
Exosomes are defined as membrane-bound extracellular vesicles ranging in diameter from 30 to 150 nanometers. They are secreted via endogenous pathways, originating from inward budding of the plasma membrane, forming early endosomes, and subsequently maturing into multivesicular bodies (MVBs). During this maturation process, intraluminal vesicles are formed within the multivesicular bodies and are ultimately released into the extracellular environment when the multivesicular bodies fuse with the plasma membrane (Figure 1A). This biogenesis pathway involves both the endosomal sorting complexes required for transport (ESCRT)-dependent and ESCRT-independent mechanisms, allowing a number of bioactive molecules to be selectively incorporated into exosomes, making them ideal messengers for intercellular communication1 (Figure 1B).
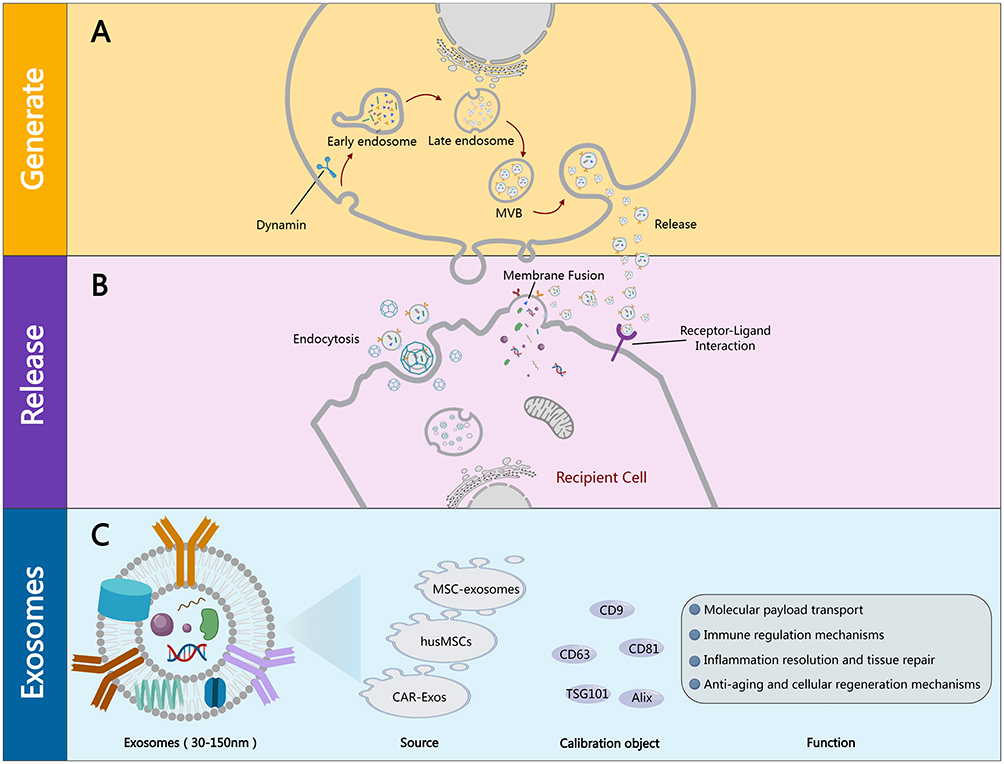 |
Figure 1 The generation, release, and related characteristics and functions of exosomes. (A) Generation: Early endosomes within the cell gradually mature into late endosomes; late endosomes further form multivesicular bodies, which fuse with the cell membrane to release various substances contained within into the extracellular space. (B) Release: Exosomes can interact with target cells in various ways. First, through membrane fusion; second, through endocytosis; third, through receptor-ligand interactions. (C) Exosome characteristics and functions: ① They have a lipid bilayer membrane structure and contain nucleic acids, proteins, etc.; ② Sources include mesenchymal stem cells, human umbilical cord mesenchymal stem cells, and antigen receptor-modified exosomes; ③ Markers: Including CD9, CD63, CD81, TSG101, Alix, etc.; ④ Functions: Involving transport, immune regulation, inflammation suppression, tissue repair and regeneration, and anti-aging, etc. |
Definition, Biosynthesis, and Composition
At its core, exosomes are small extracellular vesicles encased in a lipid bilayer that reflect the characteristics of the parent cell. The process is initiated when part of the plasma membrane invaginates to form early endosomes. As the endosomes mature, a complex sorting mechanism-typically mediated by ESCRT-selects specific proteins, RNA, and lipids to be incorporated into the lumen of the vesicle (Figure 1A).
The generated exosomes are composed of a lipid bilayer rich in cholesterol, ceramide, and sphingomyelin, which imparts stability and protects the internal cargo. In this closed environment, exosomes contain complex molecular cargoes, including messenger RNA (mRNA), microRNA (miRNA), proteins (such as the four transmembrane proteins CD9, CD63, and CD81, as well as heat shock proteins), and various bioactive lipids (Figure 1C). Their molecular composition reflects the cell of origin, making exosomes powerful tools for the discovery of diagnostic biomarkers and for therapeutic delivery. For example, changes in the exosomal miRNA profile have been used as indicators for early lung cancer diagnosis, highlighting the intrinsic connection between exosomal components and the pathophysiological state of the donor cells.1,2
In addition, the biogenesis of exosomes is not merely a matter of cellular waste disposal, but rather a highly regulated dynamic process that actively influences the microenvironment. The formation of MVBs involves the coordination of multiple intracellular sorting mechanisms that determine which bioactive molecules are tagged for secretion. This selective loading is crucial as it defines the functional specificity of exosomes, enabling them to modulate the behavior of recipient cells by transferring complete mRNA, proteins, and signaling lipids capable of altering gene expression and cellular processes in target cells. In summary, the diversity of mechanisms underlying exosome biogenesis and the resulting variations in cargo composition underscore the adaptability of exosomes as natural carriers of cellular information.
The Role in Cell-Cell Communication and Low Immunogenicity
Exosomes have rapidly become key mediators of intercellular communication due to their ability to transfer complex bioactive molecules between cells. Once released into the extracellular space, exosomes can travel to local or distant sites, where recipient cells absorb them through mechanisms such as clathrin-mediated endocytosis, phagocytosis, macropinocytosis, or direct membrane fusion. Once internalized, the delivered cargo can regulate gene expression, influence cellular metabolism, and even reprogram cell behavior in ways that are critical to tissue homeostasis and repair (Figure 1B).
One of the most significant characteristics of exosomes is their inherently low immunogenicity. Due to the similarity of their membrane components to those of normal host cells, exosomes typically achieve good tolerance when administered. This low immunogenic feature makes them attractive candidates for repeated dosing regimens, which is particularly beneficial in chronic diseases that require ongoing treatment. In a therapeutic context, exosomes can deliver drugs or genetic material without triggering the strong immune responses often associated with synthetic nanocarriers or viral vectors. However, it is important to note that under certain conditions-such as when derived from stressed or transformed cells-the surface markers of exosomes may change, potentially eliciting an immune response. Nevertheless, existing evidence suggests that exosomes largely evade immune detection, supporting their safe use as therapeutic carriers. In addition to their role in the transport of molecular cargo, exosomes also actively participate in the modulation of immune responses. By carrying immune regulatory molecules, exosomes can prompt macrophages to transition to an anti-inflammatory phenotype or promote T cell polarization, which is crucial for suppressing excessive inflammatory responses. This dual capability of facilitating communication and immune modulation positions exosomes at the forefront of novel acellular therapeutic interventions, particularly in the fields of regenerative medicine and inflammatory disease management.3–5
Reasons for Inhaling/Aerosolizing Exosomes
Conventional drug delivery routes-especially systemic injection-often face significant limitations, including rapid clearance by the reticuloendothelial system, nonspecific distribution, and the potential for adverse systemic effects. In the context of respiratory diseases, inhalation provides a unique and highly advantageous alternative. By delivering exosomes directly to the lungs through inhalation or nebulization, local treatment can be achieved, enhancing bioavailability at the target site while significantly reducing systemic exposure. From the perspective of regenerative medicine, stem cell-derived exosomes can effectively transport therapeutic substances, thereby stimulating cell proliferation and differentiation, regulating immune responses, alleviating inflammation, promoting angiogenesis, and enhancing tissue repair potential.6–8
Given the rapid progress and multidimensional potential of inhalable/nebulized exosome therapy, this review aims to provide a comprehensive and integrative perspective on this emerging field. The main objective is to examine the preparation, mechanisms of action, applications, and the prospects of inhalable exosomes in various therapeutic areas, including lung injury, respiratory diseases, immune regulation, and anti-aging therapies.
Advantages of Local Delivery in the Respiratory System
Inhalation as a therapeutic approach has several key advantages, especially for pulmonary diseases. The respiratory system, due to its extensive surface area and highly vascularized structure, serves as an ideal site for the localized delivery of therapeutic drugs. Engineered aerosolized exosomes are designed to possess an optimal particle size distribution, facilitating their deposition deep within the lungs. Particles within the optimal range (typically 1–5 μm) can reach the alveolar regions where gas exchange occurs, ensuring that therapeutic exosomes are accurately delivered to the sites of injury or disease.
Directly administering exosomes to the respiratory tract can bypass many obstacles associated with systemic delivery. This local deposition maximizes the concentration of the therapeutic agents at the site of disease while minimizing exposure to non-target tissues, thereby reducing the likelihood of off-target effects. Furthermore, due to the unique anatomical structure of the respiratory system, inhalation therapies can avoid first-pass metabolism in the liver, which typically reduces the efficacy of systemically administered drugs.
Recent advancements in aerosol delivery technology have enhanced the potential of this method. For example, vibrating mesh nebulizers and dry powder inhalers have been optimized to produce aerosols with a uniform particle size distribution, thereby maintaining the structural integrity and biological activity of exosomes. Research using these advanced nebulization technologies has demonstrated their high efficiency in delivering exosomes to lung parenchyma, as evidenced in in vivo tracing and biodistribution analyses. The convenience of inhalation therapy further improves patient compliance, particularly among patients with chronic respiratory diseases who require repeated dosing.
This precise targeting not only enhances the therapeutic index but also provides a means for therapeutic intervention in cases where systemic administration is contraindicated or less effective. By leveraging the advantages of local administration, inhaled exosomes represent a paradigm shift in the treatment of diseases characterized by acute and chronic respiratory diseases, as well as local inflammation and cancer.
Preparation of Inhaled/Atomized Exosomes
Source Selection and Cell Culture Conditions
Comparison of Cell Types (Eg, MSC, Lung Epithelial Cells, Immune Cells)
Mesenchymal stem cells (MSCs), lung epithelial cells, and immune cells are the main cell types used for exosome production, each having unique advantages and disadvantages in terms of exosome yield, carriers, and therapeutic potential.9–12 MSCs are easily isolated from adipose tissue, possess a high differentiation capacity, strong paracrine functions, and immunoregulatory abilities compared to exosomes from other sources.13 MSC-derived exosomes (MSC-Exos) have shown critical roles in cell protection and ischemic injury repair through angiogenesis, immunoregulation, and other therapeutic effects.10 Studies indicate that the therapeutic effects of MSCs in various experimental paradigms can be entirely attributed to their exosomes.14 In contrast, the advantage of lung epithelial cells lies in their ability to produce exosomes with native lung microenvironment carriers, which may enhance targeted delivery and efficacy against pulmonary diseases.5 Immune cells, such as T cells, can be engineered to express chimeric antigen receptors (CAR) and produce CAR-Exos to target specific cancer cells.15
The specific study compared the performance of these cell types in generating inhalable/ nebulized exosomes. For example, exosomes derived from three-dimensional cultured human umbilical cord mesenchymal stem cells (hucMSCs) show promise in improving pulmonary fibrosis in a mouse silicosis model.16 In applications that prefer certain cell types based on the disease context, exosomes derived from MSCs are often preferred for systemic inflammation due to their immunomodulatory properties, while exosomes from pulmonary epithelial cells might be more suitable for lung-specific conditions.10,14
The Impact of Cultural Conditions and External Stimuli on the Yield and Activity of Exosomes
Cultivation conditions significantly affect the yield and quality of exosomes.7 The composition of the culture medium, oxygen partial pressure, and pH are key factors.7 For example, a three-dimensional (3D) dynamic system can be used to culture hucMSC spheroids in microcarrier suspension to produce exosomes in serum-free culture medium.7 External stimuli, such as hypoxia, mechanical stress, or exposure to cytokines, can enhance exosome secretion and alter their molecular cargo.16
Preclinical studies indicate that these factors influence downstream therapeutic effects through inhalation.17 For example, engineered exosomes treated with lipopolysaccharide (LPS) activated macrophages exhibit anti-inflammatory effects, as confirmed by cytokine detection.17 Additionally, hypoxic preconditioning of MSCs can enhance the yield of exosomes with augmented angiogenic and anti-inflammatory properties.10,13
Isolation and Extraction Techniques
Ultracentrifugation, Chemical Precipitation, and Size Exclusion Chromatography
Ultracentrifugation, chemical precipitation (eg, using polyethylene glycol), and size exclusion chromatography (SEC) are conventional separation methods with varying efficiencies, implementation difficulties, cost impacts, and limitations in clinical application scalability.10,14,18 Ultracentrifugation involves multiple high-speed centrifugation steps to precipitate exosomes, but this can be time-consuming and may damage the exosome structure.18 Chemical precipitation is a simpler method but may lead to lower purity and potential contamination from the precipitant. SEC separates exosomes based on size, providing higher purity but potentially lower yields compared to ultracentrifugation.18
The relevant literature compares the recovery rate, purity, and functional activity of exosomes isolated by these techniques. SEC typically offers higher purity than ultracentrifugation and chemical precipitation, but it may have lower recovery rates. The choice of method depends on the ideal balance between purity, yield, and scalability in a specific application.18
Emerging Technologies (Eg, Microfluidic-Based Technologies)
Emerging technologies such as microfluidic-based platforms have improved the separation speed and throughput of exosomes while maintaining high purity.18 These systems utilize principles such as inertial focusing, membrane filtration, or immunoaffinity capture. Microfluidic devices offer several advantages, including reduced processing time, lower sample volume requirements, and improved control over separation parameters.18
To prepare inhalable exosomes, microfluidic technology has advantages due to its ability to maintain the integrity and functionality of exosomes.18 When widely adopting these technologies, current challenges include the need for specialized equipment and expertise, as well as the limited availability of validated protocols for large-scale production.18
Purification and Quality Control
Physical Characterization Methods
Physical characterization methods are crucial for ensuring the quality of the prepared exosomes. Dynamic light scattering (DLS), transmission electron microscopy (TEM), and nanoparticle tracking analysis (NTA) are commonly used methods. DLS measures the size distribution of exosomes, TEM visualizes their morphology, and NTA determines their concentration.
These parameters are crucial for optimizing inhalation delivery.7 For example, particle size is essential for determining lung deposition patterns, with smaller exosomes often able to reach deeper into the lungs.16 Recent advances have combined multiple techniques to obtain comprehensive data. For instance, combining DLS and NTA can provide more accurate measurements of size and concentration, while TEM can confirm the presence of exosomes and assess their structural integrity.16
Biochemical Identification of Specific Markers (Eg, CD9, CD63, CD81)
Biochemical assays are used to confirm the identity of exosomes, with a focus on common surface markers (CD9, CD63, CD81) and intracellular proteins (eg, TSG101, Alix).16 Verifying marker expression ensures purity and functionality.16 Western blotting, flow cytometry, and ELISA are key tools in this process, along with emerging label-free methods.16
These markers are transmembrane proteins rich on the exosomal membrane, used to confirm the presence and purity of exosomes.16 Western blotting is used to detect the presence of these markers, flow cytometry quantifies the percentage of exosomes expressing these markers, and enzyme-linked immunosorbent assay (ELISA) measures the concentration of these markers in exosomal preparations.16 Emerging label-free methods, such as surface plasmon resonance (SPR), offer rapid and non-destructive analysis of exosomal markers.16
Formulation Strategies for Inhalation Administration
Atomization Technology and Aerosol Properties
Preparing exosomes in an aerosol form requires attention to the optimal particle size (< 5 μm) to achieve deep lung deposition.16 Various nebulizer designs (jet, ultrasonic, vibrating mesh) differ in their suitability for delivering fragile exosomes without compromising their structural integrity.16 Jet nebulizers use compressed gas to aerosolize liquids, ultrasonic nebulizers use high-frequency vibrations, and vibrating mesh nebulizers use a vibrating mesh to generate mist.16
The research findings on particle size optimization, stability under aerosolization, and regional pulmonary deposition patterns are crucial.16 Smaller particle sizes typically lead to greater deposition in the lower respiratory tract, while larger particles tend to deposit in the upper respiratory tract. Stability under aerosolization is essential for maintaining the integrity of exosomes during the nebulization process.16
Advanced Formulation Methods
Innovative formulation strategies enhance stability, bioavailability, and patient compliance.19 Dry Powder Inhaler (DPI) technology can overcome issues associated with liquid formulations.20 DPI delivers exosomes in dry powder form, eliminating the need for liquid carriers and improving stability.19 The mixing system combines liposomes with exosomes to improve loading capacity and targeting efficiency.19
Lipidosome-exosome hybrid biomimetic vesicles show great promise in enhancing the treatment of pulmonary fibrosis.19 Successful case studies and experimental models have validated the feasibility of these methods.21,22 For example, inhaled CAR-T cell-derived exosomes loaded with paclitaxel can reduce tumor size and prolong survival in an in situ lung cancer mouse model, with reduced toxicity.21
Scalability and Standardization Challenges
Expanding exosome production for clinical translation faces challenges. There are bottlenecks in both upstream and downstream processes (cell culture amplification and separation, purification). Large-scale production of exosomes with consistent quality remains a significant obstacle.23,24
Standardized protocols need to be established between the laboratory and manufacturers to ensure repeatability and consistency.23,24 Regulatory requirements must be met during the large-scale production process.23,24 Areas for achieving scalable and cost-effective solutions include developing efficient cell culture methods, optimizing separation and purification techniques, and establishing robust quality control testing.23,24
Key Result Indicators (Pulmonary Function, Inflammation Index, Histopathology)
In the preclinical animal models evaluating inhalable exosomes, key outcome indicators include lung function, inflammation index, and histopathology.
Lung function is usually assessed by measuring parameters such as tidal volume (TV), peak inspiratory flow (PIF), peak expiratory flow (PEF), expiratory flow at 50% forced vital capacity (EF50), respiratory index (RI), and end-expiratory pause (EEP).25 Improvement in these parameters indicates that exosomes are effectively restoring or maintaining respiratory mechanics.
The inflammation index involves quantitative analysis of pro-inflammatory and anti-inflammatory mediators in bronchoalveolar lavage fluid (BALF) and plasma. Commonly measured cytokines include tumor necrosis factor alpha (TNF-α), interleukin-1 beta (IL-1β), and interleukin-6 (IL-6) to assess the degree of inflammation, while interleukin-10 (IL-10) is typically evaluated as an indicator of immune regulation. Additionally, levels of matrix metalloproteinase-9 (MMP-9) and surfactant protein-C (SP-C) can be assessed to evaluate tissue remodeling and alveolar function, respectively.
Histopathology provides a detailed examination of lung tissue structure and injury. Histological analysis can reveal the extent of alveolar damage, inflammatory cell infiltration, and fibrosis.20,26 Staining techniques, such as hematoxylin-eosin (H&E), are used to visualize general tissue morphology, while Masson’s trichrome staining can highlight collagen deposition in fibrotic areas.15,20
The data supporting these outcome indicators is crucial for validating the therapeutic effects of inhalable exosomes. For example, a study using HSF1-EVs in a mouse model of HS-induced lung injury showed a significant reduction in the wet-to-dry weight ratio and total protein concentration in BALF, indicating reduced pulmonary edema and vascular leakage.26 Histopathological examination revealed that HSF1-EVs alleviated alveolar damage and neutrophil infiltration in lung tissue.26
Mechanisms of Action of Exosomes
Molecular Load Transport
Exosomes, as carriers for transporting various bioactive molecules, referred to as “molecular cargo,” transfer these to recipient cells, thereby mediating intercellular communication and exerting therapeutic effects.2,27 These cargos include nucleic acids (mRNA, miRNA), proteins, lipids, and even mitochondrial components.2,28 The therapeutic potential of exosomes depends on their ability to deliver these functional biomolecules to target cells, thus influencing the behavior of these cells and regulating disease processes.27
Packaging molecular cargo into exosomes is a highly regulated process that occurs during exosome biogenesis. In this process, specific proteins, mRNA, and miRNA are selectively sorted into the forming exosomes.1,2 The composition of exosomal cargo is not static; it varies depending on cell type, its physiological state, and external stimuli.1,13 For example, cells under stress may package specific stress-related molecules into exosomes to signal other cells to initiate protective mechanisms.13 This dynamic composition highlights the versatility of exosomes as therapeutic agents (Figure 2).
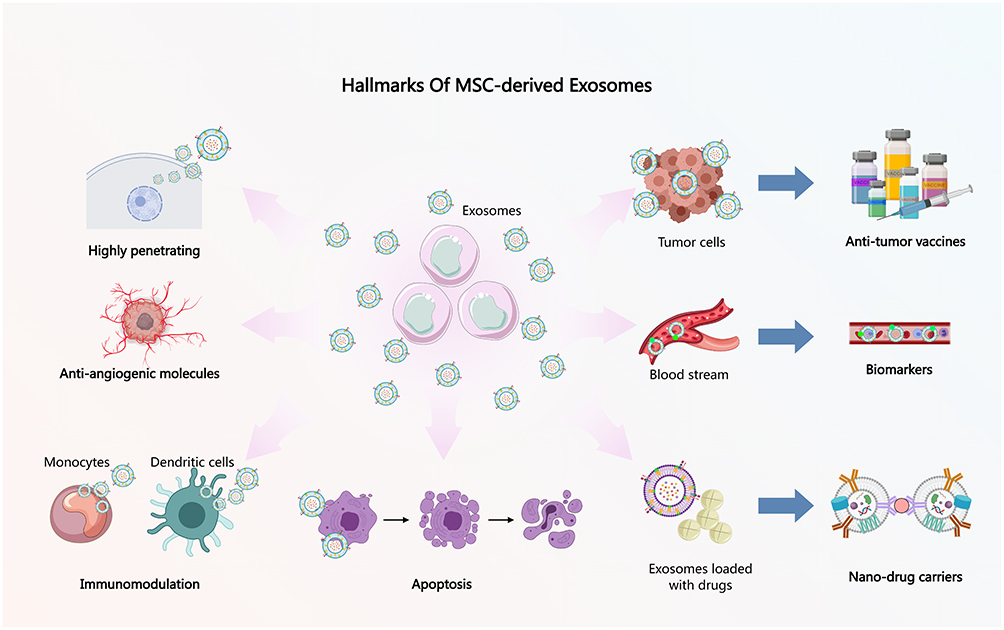 |
Figure 2 The application potential and diverse functions of stem cell-derived exosomes in biomedicine. (1) High permeability: Exosomes can effectively enter cells. (2) Anti-angiogenic molecules: Exosomes inhibit the formation of new blood vessels. (3) Immune modulation: Exosomes Influence monocytes and dendritic cells via regulating immune responses. (4) Apoptosis: Exosomes are Involved in the process of cell apoptosis. (5) Tumor cells: Exosomes interact with tumor cells. (6) Anti-tumor vaccines: Exosomes are used for vaccine development. (7) In vitro testing: Circulates in the blood as biomarkers. (8) Drug-loaded exosomes: Exosomes serve as effective nanoscale carriers for drugs. |
Mechanisms of Target Cell Uptake (Endocytosis, Membrane Fusion)
Exosomes interact with target cells and enter them through various mechanisms, primarily endocytosis and membrane fusion. The efficiency of these uptake mechanisms is influenced by factors such as surface ligands, the size of exosomes, and their charge.9
Endocytosis
This is a primary mechanism involving the internalization of exosomes by target cells. It involves several endocytic pathways, including:
Receptor-Mediated Endocytosis
Exosomes bind to specific receptors on the surface of target cells, triggering internalization. Integrins and heparan sulfate proteoglycans are examples of receptors that facilitate the interaction between exosomes and cells.9
Phagocytosis: Immune cells, such as macrophages, can engulf exosomes through phagocytosis, removing them from the extracellular space or utilizing their contents.13
Macrophagic Engulfment
This involves the non-selective absorption of extracellular fluid and its contents, including exosomes, into large vesicles known as macropinosomes.13
Membrane Fusion
Under specific conditions, exosomes may directly fuse with the cell membrane of target cells, releasing their contents into the cytoplasm.9 The compatibility of the lipid bilayer and pH-dependent fusion events are factors that influence this process.9
The Functional Roles of Transferred mRNA, miRNA, and Proteins
The therapeutic effects of exosomes are largely attributed to the functional roles of transferred mRNA, miRNA, and proteins.
mRNA
The mRNA transported by exosomes can be translated into functional proteins in recipient cells, resulting in regenerative or immune regulatory effects.2,3 For example, mRNA encoding growth factors can stimulate tissue repair2,3 (Figure 3A).
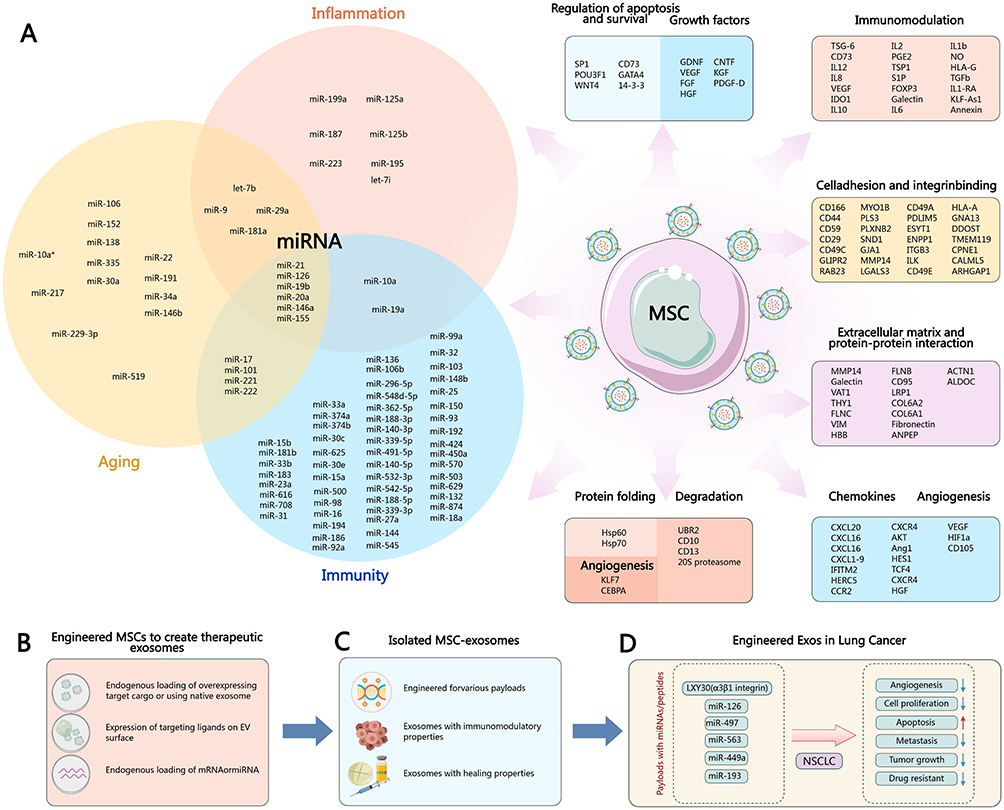 |
Figure 3 The role and mechanisms of stem cell exosomes in biological processes such as inflammation, aging, and immunity. Specific content includes: (A) The intersection of miRNAs and inflammation: Lists miRNAs associated with inflammation. Immunity: Displays miRNAs related to immune responses. Aging: Contains miRNAs associated with the aging process. These miRNAs have intersections in different biological processes, indicating their important role in regulating these pathways.3 (B) Engineered stem cells create therapeutic exosomes through engineered MSCs. Endogenous loading: Can overexpress target molecules or utilize natural exosomes. Expression of targeting ligands: Displaying targeting ligands on the surface of exosomes. Endogenous loading of mRNA: Such as miRNA. (C) The isolation of exosomes mentions various characteristics of isolating MSC exosomes. Immune regulatory characteristics. Promote healing characteristics. (D) Therapeutic applications illustrate the potential of engineered exosomes in therapy by combining different miRNAs or peptides with therapeutic drugs.29–35 Overall, the illustration emphasizes the profound impact of stem cell exosomes in various biological processes and their potential applications in clinical therapy. |
miRNA
These small non-coding RNAs regulate gene expression post-transcriptionally. Exosomal miRNAs can inhibit the expression of target genes in recipient cells, reducing inflammation or promoting tissue repair2,3,7 (Figure 3A).
Proteins
Exosomes carry various bioactive proteins, including enzymes, cytokines, growth factors, and transcriptional regulators. These proteins can regulate signaling pathways, enhance enzyme activity, and provide structural support in recipient cells2,3 (Figure 3A).
The synergistic effect of mRNA, miRNA, and proteins enhances the therapeutic efficacy of exosomes in various disease contexts2,3 (Figure 3A).
Immune Regulation Mechanism
Exosomes play a central role in regulating innate and adaptive immune responses.4,11 They can exert pro-inflammatory and anti-inflammatory effects depending on their cellular origin, cargo, and targeted immune cells.4,13
Regulation of Cytokine Secretion and Immune Cell Polarization
Exosomes influence the cytokine network and polarize immune cells toward specific phenotypes.4
Cytokine Secretion
Exosomes can stimulate or inhibit the production of cytokines by immune cells such as macrophages, dendritic cells, and T cells.13 For example, MSC-Exos can induce the secretion of IL-10, thereby inhibiting inflammation.10,11 Pulmonary epithelial cell-derived extracellular vesicles activate macrophage-mediated inflammatory responses and increase the secretion of pro-inflammatory cytokines.13
Immune Cell Polarization
Exosomes can induce polarization of macrophages (M1 and M2) and changes in T cell subpopulations (Th1/Th2 balance).4 Preclinical data have demonstrated these effects in acute lung injury or chronic inflammation models.4,13
Weakening of Hyperinflammatory Response
Exosomes alleviate excessive inflammatory responses, such as the cytokine storm in ARDS.12,36 Inhalation delivery of exosomes with high expression of CD24 (EXO-CD24) reduced the secretion of cytokines and chemokines and lung damage in ARDS.37
Mechanism
Exosomes can block overactive inflammatory signal pathways, such as JAK-STAT or NF-κB activation.37 CD24 inhibits the NF-kB pathway and the production of cytokines/chemokines.37
Clinical Relevance
Studies indicate that in animal models of sepsis or acute respiratory distress syndrome receiving exosome therapy, mortality rates decrease or conditions improve12 (Table 1).
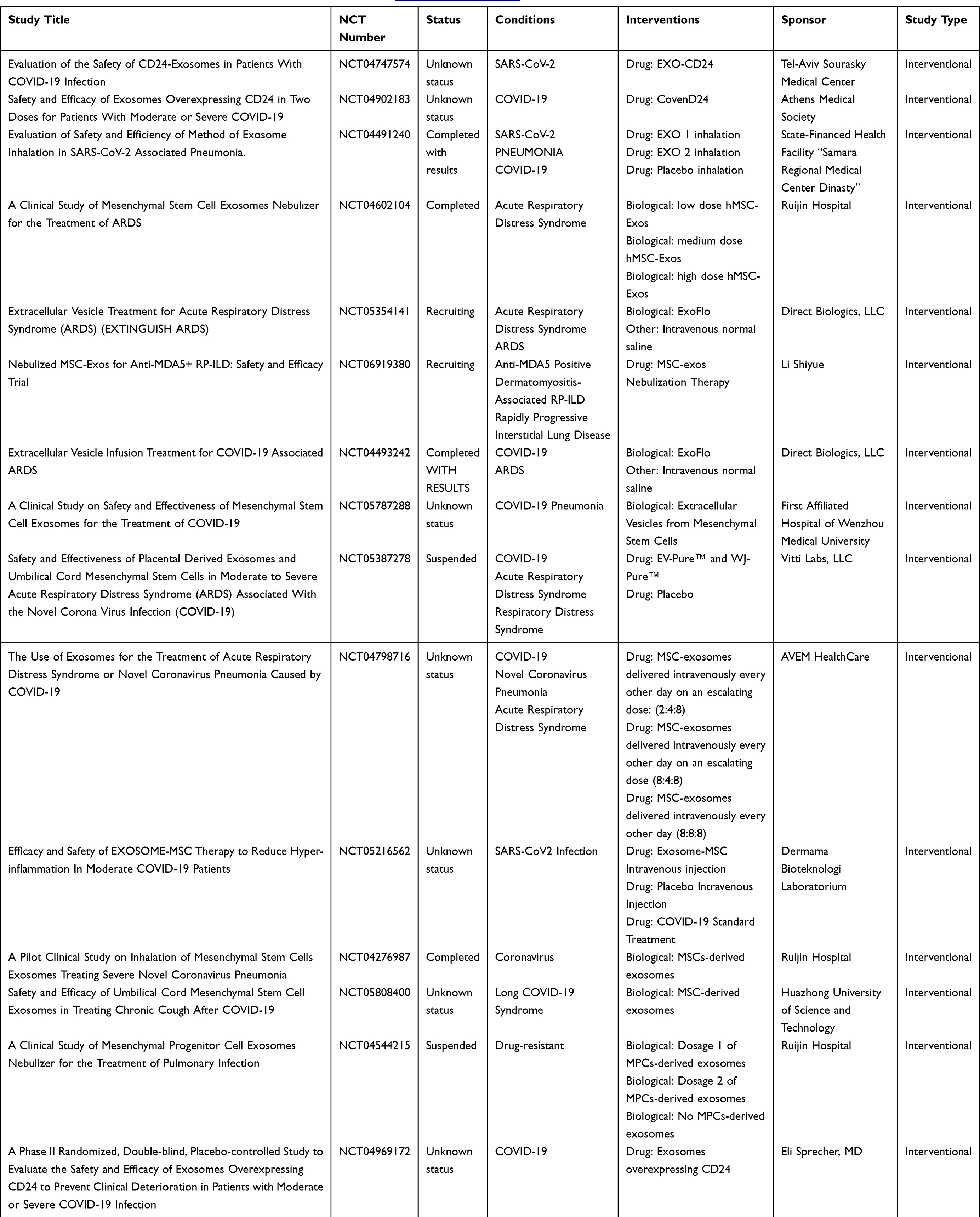 |
Table 1 Clinical Trials of Exosomes in the Treatment of Lung Diseases (https://clinicaltrials.gov/) |
Inflammation Resolution and Tissue Repair
Exosomes play a dual role in terminating inflammation and repairing damaged tissues.28
Inhibition of Pro-Inflammatory Signaling Pathways (Eg, NF-κB, HMGB1)
Exosomes interfere with key mediators of chronic inflammation.11
NF-κB Pathway
Exosomes prevent the nuclear translocation of NF-κB subunits, inhibiting their driving role in persistent inflammation.11
Neutralization of HMGB1
Exosomes clear extracellular HMGB1, preventing late-stage inflammatory response.11
Promote Angiogenesis and Regeneration
Exosomes stimulate vascular and parenchymal regeneration.19
Angiogenesis
Exosomes promote new blood vessel formation through VEGF, HIF-1α, and other pro-angiogenic factors.19
Regeneration
Exosomes enhance epithelial barrier integrity and stimulate progenitor cell proliferation/differentiation in damaged tissues.19 Adipose-derived mesenchymal stem cells exosomes (AdMSC-Exos) can effectively donate mitochondrial components, improving the mitochondrial integrity and oxidative phosphorylation levels of macrophages, thereby restoring the metabolic and immune homeostasis of airway macrophages and alleviating pulmonary inflammatory pathology.28
Anti-Aging and Cell Regeneration Mechanisms
Extracellular vesicles combat aging-related degeneration.18
Regulation of Cellular Senescence and Mitochondrial Function
Exosomes combat aging markers and restore mitochondrial health.18
Aging Markers
Exosomes reduce p16INK4a and p21WAF1 levels, while increasing SIRT1 activity.18
Mitochondrial Restoration
Mitochondrial transfer is a mechanism for rescuing energy-deficient cells.28 AdMSC-Exos can transfer stem cell-derived mitochondrial components into alveolar macrophages in a dose-dependent manner. By supplementing the damaged mitochondria, AdMSC-Exos demonstrate the ability to enhance mtDNA levels, mitochondrial membrane potential (MMP), oxidative phosphorylation (OXPHOS) activity, and ATP production, while alleviating mROS stress in macrophages under LPS challenge.28
Stimulation of Stemness and Tissue Regeneration
Exosomes remodel somatic cells and enhance tissue regeneration.17
Stemness Induction
Exosomal induction of pluripotency markers, such as OCT4, SOX2, and NANOG.17
Organ Regeneration
Exosomes combat age-related degeneration of the skin, lungs, and other organs.17,38
Preclinical and Clinical Studies of Inhalable Exosomes
Inhaled exosomes have demonstrated their potential as therapeutic agents through an increasing number of preclinical studies and early-stage clinical trials. The key mechanism of human MSC-Exos in regulating injury repair lies in their rich miRNA content, which can target and regulate fibrosis-related genes; They significantly alleviate inflammation, clear collagen deposition, and repair alveolar structure in mouse models. In recent years, clinical explorations of stem cell exosome therapy for pulmonary fibrosis have shown a diversification trend, with nebulized inhalation gradually becoming the mainstream mode of administration. Studies have found that nebulized inhalation allows for non-invasive targeted delivery, with drug concentrations in the lungs increasing 10–20 times compared to intravenous injection, while also reducing systemic side effects. At the same time, nebulized inhaled exosomes can be combined with drugs to further enhance efficacy.39
Importantly, the multifunctionality of exosomal cargo provides a unique platform for future therapeutic combinations. By engineering exosomes to carry additional therapeutic agents-such as siRNA, microRNA, or even small molecule drugs-it may be possible to customize their content to target specific pathological processes. This capability paves the way for personalized medical approaches, where exosomes not only serve as natural mediators of intercellular signaling but also as customizable, targeted drug delivery vehicles, with potential applications in oncology, autoimmune diseases, and age-related degeneration.
Research covering various lung injury models, including acute lung injury (ALI), acute respiratory distress syndrome (ARDS), chronic obstructive pulmonary disease (COPD), pulmonary fibrosis (PF) and lung cancer, provides compelling evidence for the efficacy of exosome therapy delivered via inhalation.
Evidences of ALI/ARDS, COPD and PF
Preclinical studies in animal models have shown that exosomes can have profound therapeutic effects in models of lung injury. Based on years of preclinical research exploring MSCs and their Exos in refractory lung diseases, new directions have emerged in terms of drug delivery routes for clinical translational applications, providing strong evidence for advancing the clinical translation of nebulized MSC-Exos in refractory lung diseases. In the phosgene-induced acute lung injury experimental model, the administration of exosomes derived from MSCs significantly improved respiratory parameters, such as increased tidal volume, improved peak inspiratory flow, and reduced pulmonary edema by inhibiting the pyroptosis of alveolar macrophages and reducing inflammation response. Histopathological assessments indicated that the reduction of inflammatory infiltrates and the preservation of alveolar structure jointly facilitated the recovery of lung function25,40,41 (Figure 4A).
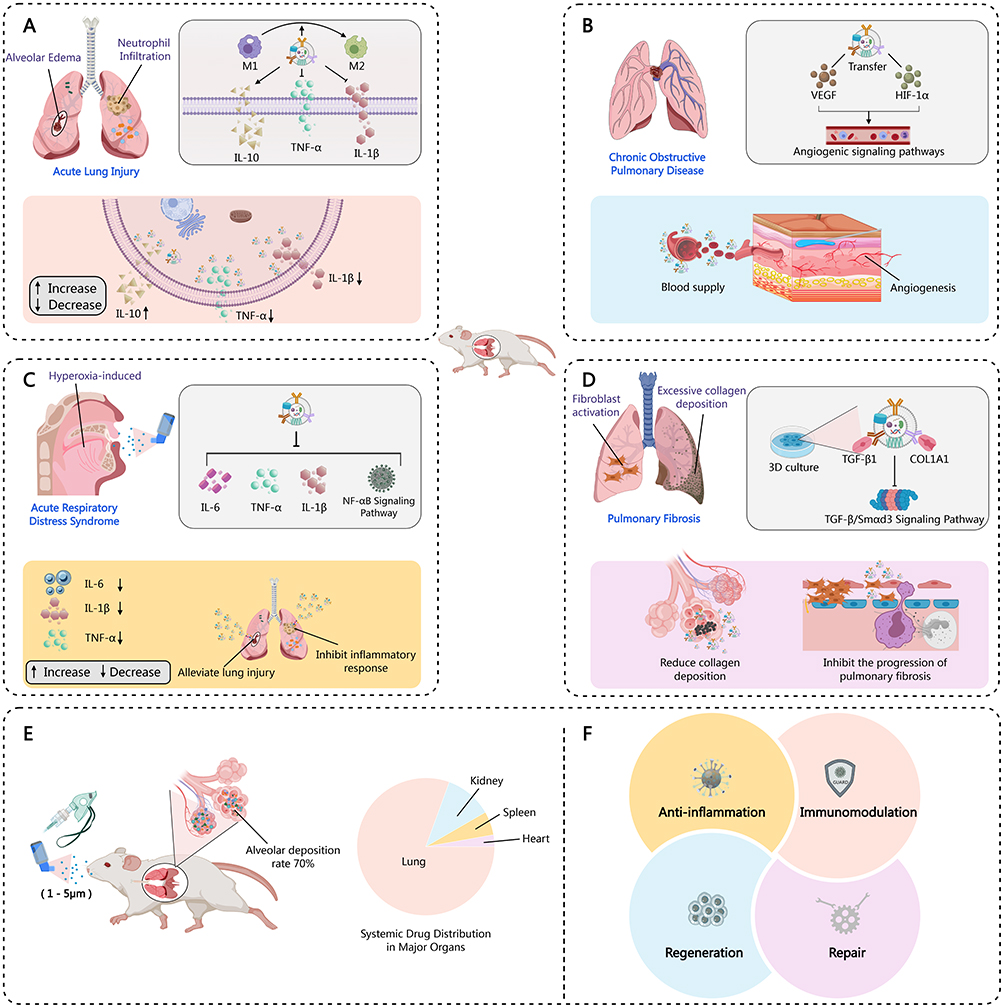 |
Figure 4 The mechanism of action and functional characteristics of exosomes in lung-related diseases. Diseases and Mechanisms of Action: (A) Acute lung injury: Phosgene-induced acute lung injury, exosomes promote the transformation of macrophages from M1 to M2 type, exerting immune regulatory effects; (B) Chronic obstructive pulmonary disease: Exosomes exert tissue regeneration by transferring vascular endothelial growth factor and hypoxia-inducible factor - 1α; (C) Acute respiratory distress syndrome: Hyperoxia-induced ARDS, exosomes can inhibit the NF-κB signaling pathway, alleviating lung inflammation; (D) Pulmonary fibrosis: Exosomes target TGF-β1 and COL1A1, blocking the progression of pulmonary fibrosis. Characteristics of exosomes: (E) Pulmonary deposition rate: Exosomes have a deposition rate of 70% in the lungs, with very little distribution in organs such as the lungs, heart, and spleen; (F) Functional characteristics: Exosomes possess immune regulation, inflammation suppression, and tissue repair and regeneration. |
In lung injury models, exosomes derived MSCs have shown great promise in improving damage. For example, MSC-Exos alleviate phosgene-induced ALI by reversing changes in respiratory function, improving pathological changes, and reducing the wet-to-dry weight ratio and total protein content in BALF.10 These exosomes also lower the levels of pro-inflammatory cytokines such as TNF-α, IL-1β, and IL-6, while increasing the levels of the anti-inflammatory cytokine IL-10 in both BALF and plasma.10 Similarly, exosomes from AdMSC-Exos have been shown to alleviate acute lung injury by transferring mitochondrial components to alveolar macrophages, improving their homeostasis.28 This mitochondrial donation enhances mtDNA levels, mitochondrial membrane potential, OXPHOS activity, and ATP production, while reducing mitochondrial ROS stress in LPS-challenged macrophages, transforming them into an anti-inflammatory phenotype.28 In a mouse model of lung injury induced by hemorrhagic shock (HS), inhalation of exosomes from HSF1-overexpressing MSCs (HSF1-Exos) showed better protective effects than exosomes from control MSCs, reducing neutrophil infiltration, oxidative stress, and lung cell apoptosis while upregulating key proteins of the lung epithelial barrier.26
Prof.Qu Jieming et al42 verified the feasibility and safety of clinical application of nebulized inhaled MSC extracellular vesicles for the first time. Nebulized MSC-Exos can exert therapeutic effects in a mouse lung injury model by reducing the level of lung inflammation and alleviating the degree of lung tissue pathological damage, significantly improving the 96-hour survival rate. A dose-response effect of aerosol inhalation of MSC-Exos was also observed in the mouse lung injury model: within the treatment dose range of 2×10^5 to 2×10^6 particles, a higher dose resulted in better therapeutic effects, but in the high-dose group exceeding 2×10^6 particles, the dose was negatively correlated with efficacy, indicating that an appropriate dose is a prerequisite for the therapeutic effect of MSC-Exos. Importantly, the aerosolized MSC-Exos also have good tolerance in clinical applications among healthy volunteers.
ARDS is a common clinical problem with a significant morbidity and mortality, and no effective pharmacotherapy exists. Biotherapeutic products containing MSC secretome provide a novel therapeutic paradigm for the healthcare due to their immunomodulating and regenerative abilities. The content and regenerative capacity of the secretome depends on cell origin and type of cultivation (2D or 3D). They investigated the effects of these freeze-dried secretome from 2D- and 3D-cultured placental MSC and lung fibroblasts (LFBs) on survival, lung tissue regeneration, lung inflammation, fibrin deposition in a lethal ARDS model using the inhaled medications. Three inhaled administrations of freeze-dried secretome from 2D- and 3D-cultured placental MMSC and LFB protected mice from death, repaired the histological structure of damaged lungs and reduced fibrin deposition. Moreover, 3D MSC secretome exhibited a more pronounced trend in lung recovery than 2D MSC and LFB-derived secretome.43 In the ARDS model, EXO-CD24 showed promise in reducing cytokine and chemokine secretion and pulmonary injury in mice.44 ARDS remains a significant global health issue with unmet needs. A study assessed EXO-CD24, an inhaled immune modulation treatment, for its potential in providing humane care for ARDS caused by infection in critically ill intubated patients. Eleven critically ill patients diagnosed with post-infectious ARDS (ten with COVID-19 and one with adenovirus-associated infection) received EXO-CD24 treatment at four medical centers in Israel. These patients had multiple comorbidities and met the Berlin classification criteria for severe ARDS. EXO-CD24 was administered via inhalation, with adverse medical events carefully monitored. The administration of EXO-CD24 did not result in any recorded adverse events. The median hospital stay was 11.5 days, and the overall mortality rate was 36%. Patients treated at the Tel Aviv Sourasky Medical Center (TASMC) exhibited a 12.5% lower mortality rate. Compared to baseline levels upon admission, WBC and CRP levels decreased, with rapid responses occurring even in kidney transplant patients who were extubated within days and subsequently discharged shortly after. All patients demonstrated significant suppression of cytokine and chemokine production, including those who had deceased. Among the patients at TASMC, four who had kidney transplants and were on immunosuppressive medications all fully recovered and were discharged. The study concluded that EXO-CD24 shows promise as a therapeutic agent at all stages of ARDS, demonstrating good safety without apparent side effects.44
These findings suggest that exosomes may have potential therapeutic effects in responding to the high inflammatory state characteristic of ARDS. More data indicated that inhalation of MSC-exosomes can be considered as a promising strategy in ARDS patients by reducing the secretion of pro-inflammatory cytokines such as IL-1β, TNF-α, and macrophage inflammatory protein-2 (MIP-2)45–47 (Figure 4C).
In animal models of COPD, local administration of exosomes was associated with effective values, enhanced angiogenesis, and significant tissue regeneration. The ability of exosomes to directly deliver growth factors and regulatory microRNAs to lung parenchyma may contribute to the reversal of pathological remodeling and maintain the integrity of lung tissue over a longer period. Overall, these preclinical findings provide a solid foundation for the clinical translation of inhaled exosome therapies for various pulmonary diseases48,49 (Figure 4B and Table 1).
Vladislav Volarevic et al14 designed MSC-derived product “Exosome-derived Multiple Allogeneic Protein Paracrine Signaling (Exo-d-MAPPS)” to apply in the chronic airway inflammation using a COPD mice model (chronic exposure to cigarette smoke, CS) and clinical data obtained from Exo-d-MAPPS-treated COPD patients. Exo-d-MAPPS apparently attenuated chronic airway inflammation in COPD mice, improved the respiratory function, as well as the downregulation of serum inflammatory cytokines (IL-1β, IL-12, IFN-γ and TNF-α), and upregulation of immunosuppressive IL-10 expression, accompanied with the reduced lung-infiltrated macrophages, neutrophils, and the expansion IL-10-producing alternatively activated macrophages, regulatory DCs, and CD4+FoxP3+T regulatory cells in inflamed lungs, resulting in the attenuation of chronic airway inflammation. Importantly, Exo-d-MAPPS was well tolerated in the 30 COPD patients, without any adverse effects after administration, which can improve the pulmonary status and quality of life of these patients.
More evidence exhibited that MSC-Exosomes reduced rat fibroblast proliferation and inhibited the expression of fibrosis genes: collagen III (COL III) and α-smooth muscle actin (α-SMA) in vitro.50–52 Exosomes derived from 3D cultured hucMSCs have been shown to improve this condition in a mouse silicosis model. Treatment with hucMSC-Exos reduced the gene expressions of collagen I A1 (COL1A1) and fibronectin (FN), inhibited silica-induced pulmonary fibrosis, and modulated pulmonary function. In vitro experiments confirmed that hucMSC-Exos reduced collagen deposition in silica-exposed NIH-3T3 cells. Additionally, inhalable liposomes or liposome-exosome hybrid biomimetic vesicles have been developed to enhance selectivity, targeting efficiency, and sustained release capabilities for the treatment of pulmonary fibrosis (Figure 4D). In the rat tendon adhesion model, topical application of MSC-Exos contributed to relief of tendon adhesion. Specifically, the fibrosis and inflammation-related genes were simultaneously inhibited by MSC-Exos. Further, miRNA sequencing of MSCs and MSC-Exos showed that miR-21a-3p was expressed at low abundance in MSC-Exos. The antagonist targeting miR-21a-3p was recruited for treatment of MSCs, and harvested MSC-Exos, which expressed low levels of miR-21a-3p, and expanded the inhibition of tendon adhesion in subsequent in vitro experiments. MSC-Exos may manipulate p65 activity by delivering low-abundance miR-21a-3p, ultimately inhibiting tendon adhesion.51
Interestingly, a secretome derived from lung stem cells (LSC) in a bleomycin-induced mouse model of pulmonary fibrosis, which reduced lung fibrosis by 50%, achieving complete remission.17,43 Furthermore, they reveals that LSC-Sec and LSC-Exo treatments could reduce and resolve bleomycin- and silica-induced fibrosis by reestablishing normal alveolar structure and decreasing both collagen accumulation and myofibroblast proliferation. These materials exhibit more therapeutic benefits than their counterparts derived from traditional MSC-exosomes. These results showed that an inhalation treatment of LSC-Sec and LSC-Exo exhibited therapeutic potential for lung regeneration in rodent models of pulmonary fibrosis.17
Zhang WY et al18 targetedly delivered anti-fibrotic small molecules, such as miRNA-486-5p, through exosomes to enhance their efficacy in regulating lung tissue inflammation and treating pulmonary fibrosis. In this work, the researchers developed engineered MSC exosomes (miR-486-RBD-MSC-Exo) modified with SARS-CoV-2-S-RBD and miR-486-5p, and observed that miR-486-RBD-MSC-Exo achieved long-term retention in lung tissue after intravenous administration. MiR-486-RBD-MSC-Exo significantly inhibited ferroptosis and fibrosis in lung epithelial cells in vitro, alleviating radiation-induced lung injury and long-term pulmonary fibrosis in ACE2 humanized mice. Furthermore, miR-486-MSC-Exo exerted anti-fibrotic effects by targeting the inhibition of SMAD2 and activating Akt phosphorylation. This study provides a potential therapeutic approach for intervening in pulmonary fibrosis.
In clinical trials, the 2025 study included 24 patients suffered pulmonary fibrosis who were randomly assigned to receive 7 days of MSC-Exos/placebo nebulization treatment. Follow-up assessments were conducted, and the results were encouraging: Excellent safety: All patients tolerated the treatment well, with no severe adverse events reported; Improvement in lung function: Forced vital capacity (FVC) and maximum voluntary ventilation (MVV) significantly increased; Enhanced quality of life: St. George’s Respiratory Questionnaire (SGRQ) scores decreased significantly; · Reversal of pulmonary fibrosis lesions: Thin-layer CT scans of two patients showed significant regression of fibrotic lesions. Notably, the study found that patients with post-inflammatory pulmonary fibrosis (such as post-COVID syndrome) may represent a target population for this therapy.20
Furthermore, in the single case, a patient was a 55-year-old woman with a 10 years history of severe systemic sclerosis (SSc) complicated by severe interstitial lung disease (ILD). Her lung disease progressed to interstitial fibrosis despite being treated with mycophenolate mofetil and monthly pulses of cyclophosphamide. Thus, she was treated with eight doses of placenta MSC-Exos. Four weeks after the third dose (Day 31 after the first dose), she reported marked improvement in her clinical symptoms, such as dyspnea and cough. Also, chest computed tomography (CT) scans demonstrated a significant reduction in ground glass consolidations and fibrotic changes. The patient was subsequently followed for twelve months, with findings showing significant improvement in exercise tolerance and reduced supplemental oxygen need. Collectively, MSC-Exos provide a promising efficient treatment for ILD; and further experimental investigation and clinical trials should be necessary.53
Research has found that MSC-Exos synergistically reverse the fibrosis process through multiple mechanisms28,54–73 (Figure 5A):
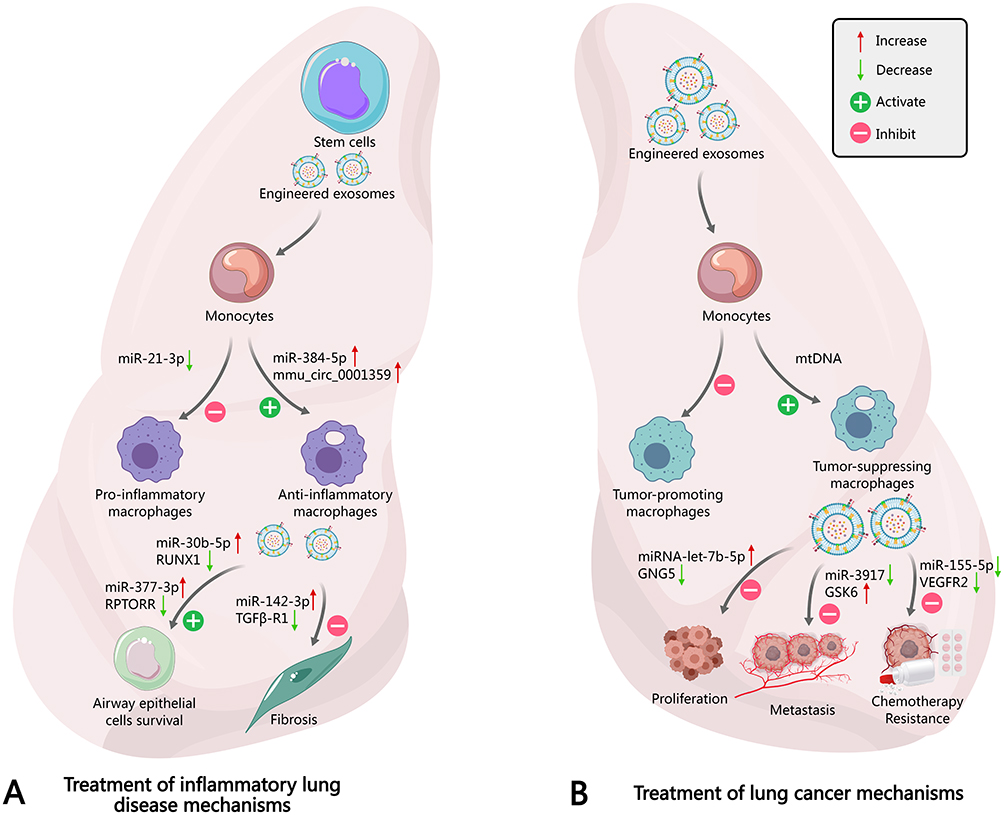 |
Figure 5 The engineered stem cell-derived exosomes mediate the immune regulatory effects of monocytes on pulmonary inflammation and tumor-related diseases. (A) Stem cell-derived exosomes can regulate miRNA to protect alveolar epithelial cells and inhibit the proliferation of cells related to inflammation and pulmonary fibrosis: MiR-21-3p: inhibits the formation of pro-inflammatory macrophages;55 MiR-384-5p and mmu_circ_0001359: promote the formation of anti-inflammatory macrophages.56,57 MiR-30b-5p (by regulating the RUNX1 target gene) and miR-377-3p (by regulating the RPTOR1 target gene): respectively activate and inhibit cell survival and fibrosis-related mechanisms.58,59 MiR-142-3p (by regulating the TGFβ-R1 target gene): inhibits pulmonary fibrosis.56 Exosomal modification participates in the overall regulatory mechanism to suppress inflammation and fibrosis processes, thereby playing a role in the treatment of inflammatory lung diseases.60 Engineered exosomal modifications improve tumor-associated macrophages, inhibit inflammatory macrophages, and influence tumor malignancy through mtDNA and miRNAs.61 (B) The impact of stem cell-engineered exosomes in lung cancer treatment specifically includes: 1. Monocytes: Exosomes affect the functions of monocytes, thereby influencing the tumor microenvironment.62 2. Tumor-promoting macrophages: Exosomes can activate mtDNA, promoting the formation of tumor-associated macrophages.28,63 3. Tumor-suppressive macrophages: Certain components of exosomes promote the generation of tumor-suppressive macrophages.64 4. miRNA regulation: miRNA-let-7b-5p: inhibits the proliferation and metastasis of cancer cells.65 miR-3917: inhibits tumor development by targeting GSK6.66 miR-155-5p: associated with VEGFR2, may affect angiogenesis.67 Chemotherapy resistance: Exosomes may participate in tumor cell resistance to chemotherapy drugs by influencing the expression of related miRNAs. Overall, the figure demonstrates the complex roles of exosomes in regulating macrophages and miRNA networks in the progression and treatment of lung cancer. |
- Immune regulation: Stem cell exosomes promote the polarization of alveolar macrophages to the anti-inflammatory M2 type, upregulating anti-fibrotic factors while downregulating pro-fibrotic factors.56,68,69
- Anti-fibrosis and epithelial repair: Exosomes carried by stem cells, containing miR-29b and the miR-200 family, can effectively inhibit the TGF-β/Smad3 and Wnt/β-catenin pathways, blocking fibroblast activation and collagen deposition. At the same time, the secretion of growth factors activates repair signals, promoting alveolar epithelial regeneration. Current research indicates that MSC-Exos can reduce lung cell death, inhibit TGF-β and Smad signaling pathways, reverse pulmonary fibrosis, and increase the number of alveolar macrophages and monocytes.70
- Multi-omics synergy: Exosomes are loaded with a mini “toolbox” of molecules. Proteomics: Various proteins participate in tissue reconstruction, including various collagens and cytoskeletal components; miRNA profile: 58.69% are miRNAs, with miR-486-5p being the most abundant; Metabolomics: Various metabolites are involved in glutamine metabolism and other repair pathways.59,71,72
Beyond the boundaries of classic lung diseases, inhaled exosomes have also been studied in lung injuries related to COVID-19 (Table 1). According to the fifth edition of the COVID-19 diagnosis and treatment guidelines from the National Health Commission, the severity requirement for COVID-19 patients to be tested is severe or critical. Seven eligible patients were assigned to receive daily doses of haMSCs-Exos (2.0×10^8 particles) for five consecutive days. The study demonstrated that inhalation of clinical-grade haMSC-Exos at doses up to 2.0×10^9 for five consecutive days is feasible and well-tolerated in seven COVID-19 patients, with no evidence of predefined adverse events, immediate clinical instability, or dose-related toxicity at any tested doses. Even in severe COVID-19 patients, there were no reported designated adverse events with the use of exosome nebulization therapy. This indicates that exosome nebulization therapy offers greater safety and effectiveness compared to traditional pneumonia treatment protocols. In terms of safety, all 7 COVID-19 patients had good tolerance to MSC-Exos nebulization, with no evidence of any pre-specified adverse events or clinical instability, nor exacerbation of existing symptoms occurring during or immediately after nebulization. The vital signs (body temperature, heart rate, respiratory rate, and oxygen saturation) of the seven patients remained stable during the five-day aerosol inhalation period.73
In terms of efficacy, varying degrees of lung lesions regression were observed in all patients after aerosol inhalation of MSC-Exos. The experiment showed that inhaling clinical-grade MSC-Exos at a continuous dose of up to 2.0×10^9 over 5 days is feasible and well tolerated among seven COVID-19 patients, with no evidence of any pre-specified adverse events, immediate clinical instability, or dose-related toxicity at any tested dose. Even in critically ill COVID patients, the use of exosome nebulization therapy did not result in any specified adverse events. This indicates that exosome nebulization therapy is safer and more effective compared to traditional pneumonia treatment plans.
Insights from Emerging Immunomodulation and Anti-Aging Applications
Aging is a complex process involving cellular senescence, mitochondrial dysfunction, and impaired regenerative capacity.18 Exosomes combat these effects by delivering rejuvenation signals to target cells.18
Although the initial focus of inhalable exosome research mainly concentrated on acute and chronic lung injury, an increasing body of evidence suggests that these nanovesicles have broader therapeutic applications in immune regulation and anti-aging therapies. Exosomes themselves possess the ability to modulate immune responses through the cargo they carry, which includes immunoregulatory proteins and specific microRNAs that affect the behavior of immune cells. For example, exosomal therapy has been shown to induce the polarization of macrophages from a pro-inflammatory (M1) to an anti-inflammatory (M2) phenotype, thereby reducing the production of local inflammatory mediators and promoting tissue repair36,37 (Figure 5A).
In addition to their immune regulatory capabilities, the potential of exosomes in cell rejuvenation and anti-aging is increasingly recognized. Aging is often accompanied by increased oxidative stress, mitochondrial dysfunction, and chronic low-grade inflammation, all of which leads to tissue degeneration. Preliminary studies indicate that exosomes can transfer functional mitochondrial components and regulatory RNA, helping to restore mitochondrial integrity, enhance oxidative phosphorylation, and reduce the accumulation of reactive oxygen species. These effects may delay cellular aging and promote regenerative processes in aging tissues, including the lungs. These findings suggest that the therapeutic scope of inhaled exosomes may extend far beyond the treatment of acute inflammatory conditions, providing a multifaceted approach that encompasses tissue regeneration and anti-aging interventions.
Exosomes derived from human embryonic stem cells (hESC-Exos) reversed cellular aging in vitro by restoring the proliferation capacity of senescent cell lines (SnCs). In aging mice, hESC-Exos treatment remodeled the proliferative state of SnCs, demonstrating significant anti-aging effects such as prolonged lifespan, improved physical performance, and reduced aging markers. Through Ago2 Clip-seq analysis, miR-302b is enriched in hESC-Exos, specifically targets the cell cycle inhibitory factors Cdkn1a and Ccng2. Furthermore, miR-302b treatment reversed the proliferation arrest of SnCs in vivo, and no safety concerns were observed during a 24-month follow-up, achieving an anti-aging effect. These findings indicate that exosomal miR-302b has the potential to reverse cellular aging, providing a promising strategy for alleviating aging-related pathologies and slowing down the aging process.74
Exosome Carriers in Lung Cancer
In terms of targeting, exosomes have unique advantages compared to other types of carriers due to the presence of specific proteins (such as CD47) on their surface, such as a long circulation half-life after intravenous injection. More interestingly, exosomes are influenced by “organ-specific distribution,” which is determined by the unique integrin expression characteristics on the surface of exosomes. Recent studies have shown that these organ-specific exosomes preferentially fuse with the main cell types in the target organs rather than with other cell types. However, in past research on exosome drug delivery, researchers often underestimated the impact of this organ-targeting nature of exosomes (Figure 5B).28,61–67
Designing next-generation exosome nanocarriers for cancer therapy based on the organ-targeting characteristics of exosomes. To validate this hypothesis, researchers studied breast cancer, which often presents with pulmonary metastasis in advanced patients.29–31 Jia L et al31 established an interesting biological scenario to verify the lung homing effect of exosomes secreted by breast cancer. Exosomes derived from breast cancer cells MDA-MB-231 (231-Exo) preferentially localize in the lungs. This unique lung distribution of exosomes is mediated by a high binding affinity between SPC protein-positive epithelial cells in the lung and integrin beta 4 (ITGβ4) overexpressed on the surface of breast cancer exosomes. Similar enrichment effects were observed in epithelial lung cancer such as A549 cells. Furthermore, researchers tested the performance of 231-Exo as a microRNA delivery vector for lung cancer. MicroRNA-126 was selected due to its significant inhibitory effect on A549 cells. Mechanistic studies indicated that the upregulation of miRNA-126 led to an increase in PTEN levels, accompanied by downregulation of PI3K and phosphorylated AKT, ultimately inhibiting proliferation, migration, and invasion abilities. Therefore, the proposed research model suggests that the organ-targeting characteristics of 231-Exo can be used to effectively target and inhibit A549 lung cancer, mediated by the high affinity between exosomal ITGβ4 and epithelial cell SPC.
They revealed the crucial role of ITGβ4 and SPC interactions in lung targeting and prepared and fully characterized lung-targeted exosomes, which were further used for miRNA-126 encapsulation. The results showed that 231-Exo could recognize A549 cells in the blood and effectively escape immune surveillance in vitro. The miRNA-126 loaded in the exosome carrier (miRNA-231-Exo) significantly inhibited the proliferation and migration of A549 lung cancer cells by disrupting the PTEN/PI3K/AKT signaling pathway. In the lung metastatic model of nude mice, systemic administration of miRNA-126-loaded exosomes achieved effective anti-cancer effects. Overall, the study demonstrated the feasibility of utilizing the organ-targeting capabilities of exosomes in designing exosome carriers, resulting in effective anti-tumor metastasis effects in mouse models.31
Applications in Immune Modulation and Inflammation Relief
Regulation of Innate and Adaptive Immune Responses
The Impact on Macrophage Polarization and T Cell Balance
Inhalable or nebulized exosomes have been shown to have the ability to modulate macrophage polarization, particularly affecting the transition from the pro-inflammatory M1 phenotype to the anti-inflammatory M2 phenotype.28 This regulation is crucial for maintaining the immune homeostasis of the respiratory system. Targeted interactions with alveolar macrophages can be achieved through the inhalation delivery of exosomes, with alveolar macrophages playing a key role in the initiation and resolution of lung inflammation. AdMSC-Exos can improve the homeostasis of alveolar macrophages. Preclinical studies highlighted the ability of AdMSC-Exos to promote the transition to the M2 phenotype, characterized by the production of anti-inflammatory cytokines such as IL-10 and Arg-1, while downregulating the secretion of pro-inflammatory cytokines such as IL-1β, TNF-α, and iNOS. This phenotypic transition is crucial for resolving inflammation and promoting tissue repair in the context of lung injury.28
Rebalancing immunity and alleviating the inflammation storm, the key molecule carried by MSC-Exos, such as miR-1470, can effectively promote the proliferation of regulatory T cells (Tregs) with strong immunosuppressive capabilities.75 Tregs act as the “peacemakers” of the immune system, significantly inhibiting the release of pro-inflammatory factors IL-4, IL-5, and IL-13.76,77 Meanwhile, miR-146a-5p in the exosomes can precisely target and downregulate the activity of innate lymphoid cells type 2 (ILC2s).78,79
Transforming macrophages from destruction to repair, MSC-Exos inhibit the key adaptor protein TRAF1, which blocks the NF-κB signaling pathway while activating the protective PI3K/AKT pathway. This significantly reduces tissue damage and promotes inflammation resolution.80 Targeting the core issue, studies have shown that miR-188 in MSC-Exos effectively blocks the key signaling axis JARID2/Wnt/β-catenin that drives goblet cell proliferation.81 Meanwhile, miR-301a-3p can inhibit the activation of signal transducer and activator of transcription 3 (STAT3), which is a key driver of smooth muscle cell proliferation.82
Precise targeting and long-lasting retention. The tiny aerosol particles formed by atomization can directly reach the bronchi and alveoli. Research shows that exosomes can be efficiently enriched in the lungs after inhalation and remain for more than 7 days, providing a time guarantee for sustained effect.83
Exosomes also play a regulatory role in T cell subpopulations, affecting the balance between Th1, Th2, Th17, and Treg cells.84 This balance is crucial for determining the outcome of pulmonary immune responses, and its disruption often leads to chronic respiratory diseases. Exosomes can transport specific cargo, such as miRNAs and proteins, directly affecting T cell differentiation and function. By regulating the expression of key transcription factors and signaling molecules, exosomes can promote the expansion of Treg cells, which is vital for maintaining immune tolerance and suppressing excessive inflammation.36
In preclinical models of respiratory diseases such as asthma, COPD, and ARDS, exosome-induced immunomodulation shows promising prospects (Figure 4F). For example, in asthma models, exosomes have been found to inhibit Th2-mediated allergic inflammation by promoting the development of regulatory T cells (Tregs) and reducing the production of Th2 cytokines such as IL-4 and IL-5.85,86 Similarly, in COPD models, exosomes have demonstrated the ability to reduce neutrophilic inflammation and promote tissue repair by modulating macrophage polarization and T cell responses.87 In ARDS models, inhaled exosomes have been shown to alleviate excessive inflammatory responses and improve lung function by restoring the balance between pro-inflammatory and anti-inflammatory immune cells.
Regulation of Cytokine/Chemokine Networks
Exosomal cargo, including miRNAs and proteins, plays an important role in regulating the secretion of cytokines and chemokines, which are key mediators of the immune response in the respiratory system. Exosomes can modulate the production of critical cytokines such as IL-10, TGF-β, TNF-α, and IL-6, thereby affecting the overall inflammatory environment in the lungs.
Research shows that exosomes can inhibit the secretion of pro-inflammatory cytokines in a state of hyperinflammation. For example, exosomes derived from MSCs have been shown to reduce the production of TNF-α and IL-6, which are major drivers of cytokine storms in severe respiratory illnesses such as acute respiratory distress syndrome and COVID-19. This inhibition is often mediated by miRNA that target the mRNA transcripts of these cytokines, leading to their degradation or translational repression.
In contrast, exosomes can also promote the secretion of anti-inflammatory cytokines such as IL-10 and TGF-β, which are crucial for anti-inflammation and promoting tissue repair. In particular, IL-10 is a potent immunosuppressive cytokine that can inhibit the activation of immune cells and suppress the production of pro-inflammatory mediators.28 On the other hand, TGF-β promotes tissue remodeling and fibrosis, which may be beneficial in the later stages of lung injury repair (Figure 4D).
The immune regulatory role of exosomes may vary depending on their cellular origin. For example, exosomes derived from MSCs are generally considered to have anti-inflammatory and immunoregulatory effects, while exosomes from activated immune cells may have pro-inflammatory effects. In addition, exosomes derived from lung epithelial cells can also modulate immune responses, both by activating macrophages and promoting inflammation, and by transmitting signals that promote tissue repair and regeneration. The specific cargo and surface molecules present on exosomes determine their immunoregulatory properties and their ability to interact with target cells.
Treatment Methods for Hyperinflammatory State
Handling Cytokine Storms in Severe Respiratory Diseases
Exosome therapy has become a promising approach to alleviating cytokine storms, which are hallmarks of severe respiratory diseases such as COVID-19, ARDS, and ALI. Cytokine storms are characterized by the excessive production of pro-inflammatory cytokines, leading to uncontrolled inflammation and tissue damage in the lungs. Exosomes can help mitigate this hyperinflammatory response by delivering anti-inflammatory cargo and modulating the activity of immune cells (Figure 4F).
Clinical trials, such as the EXO-CD24 study, evaluated the efficacy of inhaled exosomes in suppressing cytokine storms in patients with severe COVID-19-induced acute respiratory distress syndrome.44 EXO-CD24 consists of genetically engineered exosomes that overexpress the CD24 protein, which is an immune checkpoint molecule that inhibits the NF-κB pathway and reduces the production of cytokines and chemokines.37 The results of these trials indicate that EXO-CD24 is safe and well-tolerated, and it may reduce inflammatory markers and improve clinical outcomes in patients with severe acute respiratory distress syndrome.37,44
The mechanism by which exosomes mitigate cytokine storms involves several key pathways. An important mechanism is the inhibition of the NF-κB signaling pathway, which is a central regulator of inflammation. By delivering cargo that inhibits NF-κB activation, exosomes can reduce the production of pro-inflammatory cytokines such as TNF-α, IL-1β, and IL-6.37 Another mechanism is the neutralization of HMGB1, a pro-inflammatory mediator released from damaged cells that promotes the exacerbation of inflammation. Exosomes can bind to HMGB1, preventing its activation of immune cells.37
In addition, exosomes can regulate inflammasomes, which are multiprotein complexes that activate caspase-1, leading to the maturation and release of interleukin-1β and interleukin-18, both of which are potent pro-inflammatory cytokines. By inhibiting the assembly or activation of inflammasomes, exosomes can reduce the production of these cytokines and alleviate the inflammatory response (Figure 4F). The ability of exosomes to modulate these diverse pathways makes them a versatile therapeutic tool for addressing cytokine storms in severe respiratory diseases.
Synergistic Effects with Other Anti-Inflammatory Drugs
Exosomes can be used in combination with other anti-inflammatory drugs, such as corticosteroids, biologics, or small molecule drugs, to achieve a synergistic therapeutic effect when treating excessive inflammatory conditions. Using exosomes alongside these medications can enhance efficacy and reduce drug resistance, thereby improving clinical outcomes.
In preclinical models, exosomes have been shown to enhance the anti-inflammatory effects of corticosteroids. For example, exosomes can enhance the ability of dexamethasone to suppress pro-inflammatory cytokine production and reduce lung inflammation in animal models of ARDS. This synergistic effect may be due to the ability of exosomes to deliver corticosteroids directly to target cells, increasing their intracellular concentration and enhancing their therapeutic efficacy.
Exosomes can also combine with biological agents, such as TNF-α inhibitors or IL-6 receptor antagonists, to achieve synergistic anti-inflammatory effects. TNF-α inhibitors, such as etanercept and infliximab, block the activity of TNF-α, which is a major inflammatory driver in many autoimmune and inflammatory diseases. Similarly, IL-6 receptor antagonists, such as tocilizumab, block the activity of IL-6, which is another important pro-inflammatory cytokine. Administering exosomes in conjunction with these biological agents can enhance their ability to suppress inflammation and improve clinical outcomes.36
In addition, exosomes can bind to low molecular weight drugs that target specific signaling pathways involved in inflammation. For example, exosomes can associate with NF-κB inhibitors or MAPK inhibitors to enhance their ability to suppress inflammation and promote tissue repair. This combinatorial approach is particularly useful in cases where resistance has already emerged, as exosomes can help overcome resistance mechanisms and restore drug sensitivity.
Exosome Engineering for Enhanced Immune Regulation
Optimization of Targeted Genetic and Surface Modification
Engineering exosomes through genetic and surface modifications provides a good strategy to optimize their targeting ability and enhance immune regulatory functions. Genetic modifications can involve the overexpression of immune regulatory miRNAs or proteins within the exosomes, while surface modifications can involve the binding of targeting ligands to improve lung-specific delivery.
One strategy for engineering exosomes is to overexpress immunoregulatory miRNAs, such as miR-146a or miR-10a, which have been shown to inhibit inflammation by targeting key signaling molecules in the NF-κB and MAPK pathways. Delivering these miRNAs via exosomes can achieve a more robust and sustained anti-inflammatory effect. Furthermore, exosomes can be engineered to express surface ligands, such as CD47, which is a “don’t eat me” signal that can inhibit macrophage phagocytosis, enhance immune evasion, and prolong circulation time.37
Surface modification plays a crucial role in enhancing the targeting and delivery of exosomes to specific cells or tissues. One common modification is polyethylene glycolylation (PEG), which involves attaching polyethylene glycol (PEG) molecules to the surface of exosomes. PEGylation can increase the stability of exosomes in circulation, reduce their immunogenicity, and extend their half-life.19 Another strategy is to conjugate antibodies or targeting peptides to the surface of exosomes, enabling them to selectively bind to specific cell types in the lungs, such as epithelial cells or immune cells. For example, the CREKA peptide specifically binds to fibronectin (FN).19
In exosome engineering, maintaining the stability and bioactivity of exosomes after modification is a significant challenge. Modifications can sometimes alter the structure or function of exosomes, reducing their therapeutic efficacy. Therefore, it is crucial to carefully optimize the modification process to minimize any adverse effects on the stability and bioactivity of exosomes. Techniques such as cryopreservation and freeze-drying can be used to maintain the integrity of modified exosomes during storage and transportation.19
Combination of Delivery Systems for siRNA, miRNA, or Small Molecule Drugs
Hybrid exosome systems, such as exosome-liposome mixtures and exosome-loaded nanoparticles, represent a novel approach for co-delivering therapeutic nucleic acids or drugs to target cells in the lungs. These systems combine the advantages of exosomes with those of other drug delivery carriers, such as liposomes and nanoparticles, to achieve enhanced therapeutic efficacy19 (Figure 3B and C).
Exosome-liposome mixtures can be created by fusing exosomes with liposomes, forming vesicles that combine the targeting properties of exosomes with the drug loading capacity of liposomes. These mixtures can load siRNA, miRNA, or small molecule drugs for delivery to target cells in the lungs through inhalation. The exosomal components in the mixture ensure that the therapeutic payload is specifically delivered to target cells, while the liposomal components provide a protective environment for the payload and enhance its cellular uptake ability19 (Figure 3D).
Nanoparticles loaded with exosomes can be created by encapsulating the nanoparticles within the exosomes, producing vesicles that combine the targeting characteristics of exosomes and the controlled release properties of nanoparticles. These systems can be used to deliver various therapeutics to target cells in the lungs, including chemotherapy drugs, anti-inflammatory drugs, and gene therapy vectors. The exosomal components of the system ensure that the nanoparticles are specifically delivered to the required cells, while the nanoparticle components provide the functionality of sustained release of therapeutics, thereby extending their therapeutic effects.19
Engineered exosomes enhance the delivery of siRNA/miRNA to immune cells (such as macrophages and dendritic cells). siRNA and miRNA can be used to silence specific genes associated with inflammation or immune activation, thereby regulating the immune response in the lungs. Using exosomes as delivery vehicles for these nucleic acids can enhance their cellular uptake and reduce degradation, leading to more robust and lasting therapeutic effects.8
Scalability and regulatory considerations pose significant challenges to the clinical translation of engineered exosomes. Large-scale production of exosomes requires efficient and reproducible manufacturing processes, along with stringent quality control measures to ensure the safety and efficacy of the final product. Regulatory agencies like the FDA demand extensive preclinical and clinical data to demonstrate the safety and efficacy of exosome-based therapies before approval for clinical use. Addressing these challenges is crucial for realizing the full potential of engineered exosomes as a treatment modality for respiratory diseases.
In a rat model of ALI induced by phosphates, exosomes derived from MSCs reversed the changes in respiratory function, showing increased levels of TV, PIF, PEF, and EF50, along with decreased levels of RI and end-expiratory carbon dioxide partial pressure (EEP). Furthermore, MSC-derived exosomes improved pathological changes, reduced the wet-to-dry ratio and total protein content in BALF. They also decreased levels of TNF-α, IL-1β, and IL-6, while increasing levels of IL-10 in BALF and plasma. MSC-derived exosomes suppressed the levels of MMP-9 and increased the levels of SP-C. The study concluded that MSC-derived exosomes have beneficial effects on phosphate-induced ALI by modulating inflammation, inhibiting MMP-9 synthesis, and increasing SP-C levels.25
A study indicates that small extracellular vesicles (sEVs) can be delivered to the lungs of mice via a vibrating mesh nebulizer (VMN). In vivo sEV tracking demonstrated that the inhaled sEVs are localized solely in the lungs, primarily accumulating in pulmonary macrophages and airway epithelial cells. Furthermore, sEVs loaded with small RNAs were successfully delivered to the lungs. Inhalation of siMyd88-loaded sEVs reduced LPS-induced lung injury in mice. This research proposed a new method for delivering sEV-mediated small RNAs into mouse lungs through nebulization and suggested a potential sEV-based therapeutic strategy for human lung diseases.8
Inhaled polyether ether ketone (PTX) encapsulated in CAR-exosomes accumulated in the tumor region, reducing tumor size and prolonging survival in an ectopic lung cancer mouse model, with minimal toxicity. Furthermore, PTX@CAR-exosomes reprogrammed the tumor microenvironment, reversing immunosuppression, which was attributed to the infiltration of CD8+ T cells and the increased levels of IFN-γ and TNF-α. This study provides a nanovesicle-based delivery platform to enhance the efficacy of chemotherapy drugs in lung cancer treatment while reducing side effects.21
Exosomes released by AdMSC-Exos can transfer stem cell-derived mitochondrial components to alveolar macrophages in a dose-dependent manner. By supplementing damaged mitochondria, AdMSC-Exos enhance mitochondrial DNA (mtDNA), mitochondrial membrane potential (MMP), OXPHOS activity, and ATP production levels, while alleviating the mROS stress observed in macrophages challenged with LPS. Restoration of mitochondrial integrity through AdMSC-Exos treatment leads to a shift of macrophages towards an anti-inflammatory phenotype, accompanied by a downregulation of IL-1β, TNF-α, and iNOS secretion, as well as an increase in the production of the anti-inflammatory cytokine IL-10 and Arg-1. The depletion of alveolar macrophages largely eliminates the protective effect of AdMSC-Exos. AdMSC-Exos can effectively donate mitochondrial components, improve the mitochondrial integrity and oxidative phosphorylation levels of macrophages, restore the metabolic and immune homeostasis of airway macrophages, and reduce pulmonary inflammation pathology.28
In the pig model, both aerosolized and intravenously administered platelet-derived exosome products (PEP) resulted in global uptake of exosomes in lung parenchyma, with the highest degree of uptake observed for aerosolized exosomes. The administration method guided by a pulmonary artery balloon catheter enabled targeted delivery to the lungs. No off-target absorption was observed in the heart, spleen, or kidneys. However, significant uptake was primarily seen in the liver of animals treated with aerosolization (Figure 4E). Aerosolization also led to uptake in the trachea, while no significant absorption was noted in the esophagus. This study demonstrated the feasibility of pulmonary delivery of exosomes using aerosolization or intravenous infusion, or localized delivery guided by a pulmonary artery balloon catheter.9
In a study on PF, inhalable FN-binding liposomes or liposome-exosome hybrid biomimetic vesicles were developed to enhance PF treatment. Modified liposome-chitosan (CS) microspheres SM (CT-lipo) loaded with cryptotanshinone (CTS) and liposome-exosome hybrid biomimetic vesicles-CS microsphere SM (LE) were evaluated. SM (CT-lipo) and SM (LE) achieved specific targeting of lung myofibroblasts through the homing effect of CREKA peptide specifically binding to FN and exosomes, thereby facilitating the efficient delivery of anti-fibrotic drugs to the lung lesions. The efficacy obtained by inhaling SM (CT-lipo) and SM (LE) every two days was similar to that of daily use of conventional microsphere SM (NC) and pirfenidone (PFD), demonstrating excellent sustained release capability. The results indicate that the developed SM (CT-lipo) and SM (LE) delivery strategies can achieve more precise, efficient, and safe treatment for chronic PF.19
In a pilot study involving patients with severe COVID-19, nebulized exosomes derived from allogenic adipose tissue mesenchymal stem cells (haMSC-Exos) were well-tolerated, with no pre-defined adverse events or clinical instability observed during or immediately after nebulization. There was a slight increase in serum lymphocyte counts among all patients. Improvement in pulmonary lesions of varying degrees was observed in all patients following inhalation of haMSC-Exos, with more significant improvements noted in 4 out of 7 patients. The study indicated that the cumulative dose of clinically graded haMSC-Exos inhaled for 5 consecutive days, reaching 2.0 × 10^9 nanovesicles, is feasible and well-tolerated, with no adverse events, immediate clinical instability, or dose-related toxicity found at any tested dosage. This safety profile was corroborated by improvements seen through CT imaging within 7 days.14
Meng Li., et al20 performed a phase l clinical trial in 24 patients with pulmonary fibrosis using additional nebulized hucMSC-Exos or routine treatment. Patients used additional nebulized hucMSC-Exos gained significant benefits compared with those accepted only routine treatment. Interestingly, two patients with advanced post-inflammatory pulmonary fibrosis exhibited clinically significant regression on serial CT scans after hucMSC-Exos therapy. These results imply that nebulized hucMSC-Exos could be used as a promising therapeutic strategy for treating pulmonary fibrosis diseases.
Future Perspectives and Challenges
The field of inhalable/aerosolized exosomes holds great promise for the treatment of various respiratory and systemic diseases, but its path to clinical translation is fraught with challenges. Overcoming technical barriers, establishing robust manufacturing processes, and addressing the regulatory landscape are crucial to realizing the full therapeutic potential of this innovative approach.
Technical Challenges and Standardization
The widespread application of inhalable exosome therapy is currently limited by several technical barriers. There is a significant gap between the requirements of laboratory-scale research and industrial-scale production, which necessitates the development of efficient and scalable manufacturing processes.
Optimization of Large-Scale Production and Separation Methods
Current methods of exosome production typically suffer from low yields and batch-to-batch variability, hindering their widespread application.88 Traditional methods such as ultracentrifugation are widely used but are time-consuming, may damage exosomes, and are difficult to scale up.2,23,27 Emerging production platforms, such as bioreactors and three-dimensional culture systems, offer potential solutions for improving exosome yield and maintaining consistent quality.88 These advanced culture systems can simulate the in vivo microenvironment, promoting cell growth and exosome secretion. However, challenges remain in optimizing these systems for specific cell types and the desired exosome characteristics.89
Maintaining the integrity of exosomes during large-scale separation is another key challenge. Exosomes are fragile vesicles that can be easily damaged by harsh physical or chemical treatments. Automation and process optimization strategies are needed during separation and purification to minimize exosome damage. Methods based on microfluidic technology offer a promising alternative to traditional methods, allowing for gentle and efficient exosome separation with minimal sample handling.
Establish Unified Quality Control and Regulatory Standards
The lack of standardized characterization protocols poses significant challenges to the development and commercialization of inhalable exosome therapies.18,24 Defining critical quality attributes (CQA) is essential to ensure the safety and efficacy of these products. CQA includes physical parameters such as particle size distribution and concentration, biochemical markers such as surface proteins and cargo components, and functional assays to assess bioactivity and purity.18,24
Physical characterization methods, such as DLS, TEM, and NTA, are used to determine the size, morphology, and concentration of exosomes. Biochemical identification of specific markers, such as CD9, CD63, and CD81, confirms the presence of exosomes and assesses their purity. Functional assays are essential for evaluating the bioactivity of exosomes, including their ability to modulate immune responses, promote tissue repair, or deliver therapeutic payloads.
The existing regulatory frameworks, such as those provided by the FDA and EMA, lack specific guidelines for exosome therapies. A roadmap for the development of industry-wide standards is needed to fill this gap and ensure the quality, safety, and efficacy of these products. This roadmap should include the establishment of standardized characterization protocols, the definition of CQAs, and the development of appropriate functional assays.
Engineering Progress and Targeted Delivery
Technological innovation is crucial for overcoming current limitations and enhancing the therapeutic potential of inhalable exosomes. An interdisciplinary approach combining bioengineering and nanotechnology offers exciting opportunities for improving exosome efficacy, specificity, and delivery.
Strategies for Enhancing Loading and Specificity
Several engineering approaches can be used to enhance the loading and specificity of exosomes. By genetically modifying the parent cells, the expression of therapeutic proteins or RNAs within the exosomes can be increased. After separation, binding to ligands or antibodies on the surface can target exosomes to specific types of cells or tissues. Mixed systems, such as exosome-liposome complexes, can combine the advantages of exosomes and liposomes to enhance the loading and delivery efficiency of drugs (Figure 3B and C).
Engineered exosomes show potential in respiratory targeting. For example, modified exosomes with lung-homing peptides demonstrated improved delivery to the lungs in preclinical studies. However, there is a trade-off between natural and engineered exosomes. Natural exosomes may have superior biocompatibility and immunocompatibility, while engineered exosomes may offer enhanced loading and specificity.
Integration with Nanotechnology and Biomimetic Systems
Cooperative technologies, such as smart nanoparticles for co-delivery and biomimetic coatings for immune evasion, can further enhance the therapeutic potential of inhalable exosomes. Smart nanoparticles can carry drugs or other therapeutic agents and be co-delivered with exosomes to target cells. Biomimetic coatings can be used to disguise exosomes, reducing their immunogenicity and extending their circulation time. Stimulus-responsive release systems can be utilized to trigger the release of therapeutic cargo from exosomes at the target site.
The challenges of complexity and scalability remain a significant barrier to these advanced technologies. However, the future integration with AI-driven design platforms may accelerate the development and optimization of engineering exosomes.
Regulatory, Ethical, and Translational Considerations
The clinical translation of inhalable exosome therapy requires careful consideration of regulatory, ethical, and translational issues. A solution-oriented approach is needed to address existing barriers and promote the development of safe and effective therapies.
Clinical Approval and Long-Term Safety Challenges
The inhalation route of administration presents unique regulatory challenges. Due to factors such as particle size, deposition efficiency, and lung clearance mechanisms, dose determination can be quite complex. Careful evaluation of biodistribution and clearance issues is required to ensure that exosomes are delivered to the target tissue without accumulating in other organs. The immunogenicity risk of repeated administration needs to be assessed to minimize the potential for adverse immune reactions.
The current clinical trial designs may be insufficient to address these challenges. A safety monitoring framework is needed for long-term use to detect and manage potential adverse reactions.
Future Directions of Personalization and Combination Therapy
Emerging paradigms, such as exosome therapy for specific patients and the rational combination with small molecules/biologics, provide promising avenues for improving the efficacy and safety of inhaled exosome therapy. Exosome therapy for specific patients, using autologous or allogeneic exosomes, can be customized according to the needs of each patient. Rational combinations with small molecules or biologics can enhance the therapeutic effects of exosomes and address multiple disease pathways. Therapeutic diagnostic applications, which combine diagnosis with treatment, can be tailored based on individual patient responses, allowing for personalized treatment strategies.
The ethical issues in personalized exosome medicine need to be approached with caution. The clinical development path for combination products needs to be clearly defined.
In summary, realizing the full potential of inhalable exosome therapy requires collaborative efforts from academia, industry, and regulatory agencies. Addressing technical challenges, establishing robust manufacturing processes, and navigating the regulatory environment are crucial for translating these promising therapies into clinical practice. Focusing on advanced engineering strategies, targeted delivery systems, and personalized medicine approaches will accelerate the development of safe and effective inhalable exosome therapies to address a wide range of diseases. Although the timeline for clinical implementation may vary, the potential impact of these therapies on immune regulation, inflammatory repair, and anti-aging treatments is significant.
Conclusions and Prospects
Summary of Key Discoveries and Therapeutic Advantages of Inhaled Exosomes
This review comprehensively examines the latest developments of inhaled or nebulized exosomes as an acellular therapeutic modality, outlining the progress in preparation, characterization, mechanisms of action, and clinical applications. A core finding is that exosomes are nanoscale vesicles naturally secreted by various cells (including mesenchymal stem cells, lung epithelial cells, immune cells, and even gene-modified variants) that can be specifically engineered and formulated for pulmonary delivery. The inhalation route not only allows for the direct deposition of drugs in the respiratory system but also minimizes the risk of systemic side effects. This significant advantage ensures high local drug concentration at the lesion site while reducing non-target toxicity.
A key aspect of inhalable exosome therapy is maintaining the natural biological cargo within these vesicles, including mRNA, microRNA, proteins, and lipids. These cargos are responsible for mediating therapeutic effects ranging from anti-inflammatory and immune modulation to tissue regeneration and cell repair. Preparation methods, such as ultracentrifugation, size exclusion chromatography, and emerging microfluidic-based techniques, have been optimized to preserve vesicle integrity during the aerosolization process. Additionally, advanced formulation strategies-including the use of vibrating mesh nebulizers and innovative dry powder inhaler systems-have been shown to allow exosomes to retain their bioactivity post-nebulization, ensuring effective lung deposition and improved clinical outcomes.
Preclinical data provide strong support for the therapeutic effects of inhaled exosomes. For example, in animal model studies of lung injury-from phosgene-induced acute lung injury to silica-induced pulmonary fibrosis-it was shown that exosomes derived from mesenchymal stem cells can significantly alleviate inflammatory responses and improve pulmonary function parameters. In specific models, such as phosgene-induced rat injury, administration of mesenchymal stem cell-derived exosomes restored respiratory parameters to normal and reduced pro-inflammatory cytokine levels, indicating significant restoration of alveolar structure and function. Similar protective effects have also been observed in hemorrhagic shock models, where exosomes from mesenchymal stem cells overexpressing HSF1 reduced pulmonary edema, inhibited inflammatory cytokines, and preserved epithelial barrier integrity.
Moreover, the immunoregulatory potential of inhalable exosomes stands out as a unique therapeutic advantage. Their ability to regulate cytokine secretion, promote macrophage polarization toward an anti-inflammatory phenotype, and inhibit key pro-inflammatory signaling pathways (such as NF-κB and HMGB1) has been consistently validated across different experimental environments. These characteristics are particularly important in clinical scenarios characterized by cytokine storms, such as severe ARDS, where timely suppression of excessive inflammation may be crucial for saving lives. For example, preliminary clinical studies using inhaled EXO-CD24-a genetically modified exosome preparation designed to overexpress the CD24 immune checkpoint protein-have demonstrated good safety profiles and significant inhibition of inflammatory markers in patients with severe ARDS associated with COVID-19.44 These findings emphasize that inhalable exosomes not only serve as carriers of bioactive mediators but also actively regulate host immune responses, thus enhancing tissue repair and regeneration capabilities.
Another important finding emphasized in this review is the scalability and biodistribution characteristics of inhalable exosomes. Studies utilizing advanced imaging and biodistribution techniques have confirmed that nebulized exosomes exhibit preferential accumulation in lung parenchyma, with minimal off-target distribution. For instance, in pig models, inhalation resulted in widespread but controlled uptake of exosomes in lung tissue, ensuring therapeutic agents were precisely concentrated at the desired site without causing excessive systemic exposure. This selective deposition is further supported by the nanoscale size of exosomes, allowing them to traverse complex alveolar structures and deposit in distal airway and alveolar regions.
Beyond pulmonary applications, this review emphasizes the potential of inhaled exosomes’ biological cargo in the broader applications of immune modulation in systemic inflammatory diseases, anti-aging interventions, and even regeneration therapies in non-pulmonary tissues. Given that exosomes can carry various molecular information reflecting their source cells, they possess an inherent ability to reprogram recipient cells by transferring functional mRNA and microRNA. In models where exosomes have been shown to promote stem cell and tissue renewal, their inhalable delivery may offer an innovative approach to address age-related decline and chronic inflammatory conditions. Therefore, inhaled exosomes serve as a multifunctional therapeutic platform that not only acts locally in the respiratory system but also has the potential to regulate systemic biological processes triggered by their complex molecular cargo.
In summary, the main findings of the review indicate that inhaled or aerosolized exosomes offer several unique therapeutic advantages:
They can be delivered directly to the respiratory system, thus concentrating their therapeutic effects at the site of disease while reducing systemic toxicity.
They preserve a rich and diverse biological payload, including nucleic acids and proteins that are crucial for regulating inflammatory responses and promoting tissue regeneration.
They exhibited good biodistribution and deposition characteristics in preclinical models, ensuring optimal binding with lung tissue.
They have shown good results in both preclinical studies and early clinical trials, especially with significant efficacy observed in diseases like ARDS, pulmonary fibrosis, and severe COVID-19-related lung injury (Table 1).
These multi-layered pieces of evidence collectively emphasize the potential of inhalable exosomes as a safe, effective, and innovative strategy for treating respiratory diseases and other illnesses.
Clinical Significance and Future Research Roadmap
Promising preclinical and early clinical results have paved the way for the translation of inhalable exosome therapy into broader clinical practice. The clinical significance of inhalable exosomes is varied, from the treatment of acute and chronic respiratory diseases, such as ARDS, pulmonary fibrosis, and COPD, to potential adjunctive therapies for lung cancer and infectious diseases (Figure 4).
In the current clinical environment, one of the most compelling applications is in the management of severe lung injury, which has been confirmed in studies using EXO-CD24 to treat refractory ARDS patients (Table 1). The favorable safety and reduction of inflammation markers observed in these preliminary studies suggest that inhaled exosome therapy may soon become a key tool in intensive care, especially for conditions associated with cytokine storms or uncontrolled inflammatory responses. In addition to ARDS, experimental models of pulmonary fibrosis, including the silica lung model, indicate that exosomes from human umbilical cord mesenchymal stem cells significantly reduced collagen deposition and improved lung function, suggesting that inhaled exosomes may serve as an effective therapeutic option for interstitial lung diseases that have been difficult to manage so far.
Despite these encouraging results, several obstacles still need to be overcome before inhalable exosome therapy can achieve widespread clinical application. One major challenge is scaling up the production of clinical-grade exosomes while ensuring strict standardization between batches. Currently, methods such as ultracentrifugation, size exclusion chromatography, and novel microfluidic technologies are used for exosome isolation. However, a significant barrier is the lack of universally accepted protocols for exosome purification and quality control. It is crucial to develop robust, high-throughput manufacturing processes that maintain the integrity and bioactivity of exosomes. In this context, interdisciplinary collaboration involving cell biologists, bioengineers, and pharmaceutical scientists is essential for optimizing culture conditions, isolation protocols, and subsequent aerosol delivery formulations.
Another clinical obstacle is related to the optimization of delivery devices and formulation strategies. The effectiveness of aerosolized exosome therapy largely depends on maintaining the integrity of the vesicles during aerosolization. Vibrating mesh nebulizers have shown promise in this regard; however, further improvements are needed to enhance particle size distribution and deposition efficiency. Future research should focus on combining advanced nebulization technologies with novel formulation methods such as dry powder inhalers and liposome-exosome hybrid systems. These innovations can not only protect the exosome load during delivery but also promote targeted deposition in specific lung regions, thereby improving therapeutic efficacy and reducing dosing frequency.
Long-term safety is another key research priority. Although preliminary clinical studies have shown good safety and few adverse events, comprehensive long-term studies are needed to fully assess the immunogenicity and toxicity of inhaled exosomes. Given that exosomes are naturally secreted by cells, they are typically considered to have low immunogenicity. However, engineering processes and repeated inhalation may provoke unexpected immune responses. Preclinical studies with longer follow-up periods, as well as multicenter clinical trials, are necessary to monitor any delayed or cumulative side effects and ensure that these therapies meet the highest safety standards.
In addition to optimizing delivery and safety parameters, future research must also address the delivery and pharmacokinetic characteristics of inhaled exosome therapies. The unique biodistribution characteristics observed in preclinical models-where inhaled exosomes are primarily concentrated in the lung parenchyma-provide significant advantages over systemic administration. However, determining the optimal particle size, dosage, and treatment frequency requires systematic investigation. Further research should incorporate advanced imaging techniques, biomarker analysis, and computational modeling to refine the delivery strategies, maximize therapeutic effectiveness, and minimize potential toxicity.
The future research roadmap should also explore the potential of combination therapies utilizing the multifaceted properties of exosomes. Inhalable exosomes can be designed to carry additional therapeutic agents-such as siRNA, microRNA, or traditional chemotherapy drugs-thus providing an integrated approach to managing complex disease states. For example, exosomes designed to enhance drug loading have been used in preclinical models of lung cancer, facilitating the targeted delivery of paclitaxel while reducing systemic toxicity.19 Similar strategies could be applied to the synergistic combination in ARDS, where anti-inflammatory drugs or regenerative factors are co-delivered with natural exosome carriers, potentially improving therapeutic efficacy.
Collaboration among academia, clinical researchers, and regulatory agencies is crucial for advancing this field. The clinical translation of inhaled exosome therapies requires not only comprehensive scientific validation but also the development of a standardized regulatory framework that can accommodate the unique aspects of acellular biologics. Regulatory agencies need to establish guidelines for the production, characterization, and clinical evaluation of exosome therapeutic drugs, similar to the standards already in place for traditional drug formulations. In addition, economic considerations and cost-benefit analysis should be integrated into future research. Despite the promising prospects of exosome therapy, the costs of large-scale production and the complexities of quality control may pose challenges for widespread clinical implementation. Addressing these issues will involve assessing the entire supply chain-from cell culture and vesicle isolation to formulation and distribution-to ensure that these therapies are not only effective but also accessible to patients in need.
Collectively, the clinical significance of inhaled exosome technology is immense, with the potential to fundamentally change the treatment paradigm of various respiratory diseases and inflammatory conditions. The roadmap for future research is clear: standardization and scaling of production processes, optimization of delivery devices and formulations, comprehensive long-term safety and dosage studies, exploration of combination therapies, and establishing a robust regulatory framework. Achieving these goals will require coordinated multidisciplinary efforts to bridge basic research with clinical practice, ultimately translating promising laboratory discoveries into commercially viable and widely accessible treatment options.
Final Review on the Potential Effects of Immune Regulation, Inflammation Repair, and Anti-aging and Cancer Therapy
Reviewing the collective insights from this evaluation, it is evident that inhalable exosome therapy represents a transformative leap in modern medicine. Their unique ability to directly deliver bioactive payloads to the site of injury-especially within the complex structures of the lungs-positions these nanoscale vesicles at the forefront of immune modulation, inflammatory repair, and innovative strategies for potential anti-aging interventions.
One of the most striking aspects of inhalable exosomes is their dual ability to regulate the immune system while promoting tissue regeneration. By transferring functional nucleic acids and proteins, inhalable exosomes can reprogram recipient cells, shifting the balance from destructive inflammatory responses to protective and reparative processes. This is particularly evident when exosomes have been shown to reduce levels of pro-inflammatory mediators such as TNF-α, IL-1β, and IL-6, while increasing anti-inflammatory cytokines like IL-10. This immunomodulatory effect is especially crucial for diseases characterized by a hyper-inflammatory state, including severe ARDS and cytokine storms associated with COVID-19, as confirmed by clinical humanitarian research. The ability to rapidly suppress the inflammatory cascade while activating repair pathways underscores the potential for fundamental changes in treatment outcomes in acute respiratory distress and other diseases through foundational exosome therapies.10,11
Moreover, the effects of inhalable exosomes extend to the fields of tissue repair and regeneration. In preclinical models of lung injury, these vesicles not only alleviate damage but also stimulate recovery mechanisms such as angiogenesis, epithelial barrier repair, and stem cell activation. By promoting the expression of regenerative markers and regulating apoptotic pathways, inhalable exosomes can facilitate the recovery of lung structure and function even in cases of severe tissue damage. In this process, they offer a promising alternative to traditional therapies, which often focus solely on symptom management rather than true tissue regeneration. This dual action-reducing inflammation while actively promoting repair-could revolutionize the management of acute and chronic pulmonary diseases and other degenerative diseases where inflammation and cellular aging play a key role.
The potential applications of inhalable exosome therapy are not limited to the lung field. The fundamental characteristics of exosomes that can modulate immune responses and stimulate tissue repair may also be utilized in anti-aging therapies. Aging is intrinsically linked to chronic low-grade inflammation, often referred to as “inflammaging,” as well as the gradual decline in tissue regeneration capacity. Inhalable exosomes, with their ability to deliver rejuvenating biomolecules, may help restore mitochondrial function, reduce cellular aging, and promote the maintenance of youthful cell phenotypes. Early experimental evidence suggests that exosomes can regulate cellular pathways associated with aging and decline, thus opening new avenues for interventions aimed at delaying or even reversing certain aspects of the aging process. Although further research is needed to fully elucidate these mechanisms and translate them into clinical therapies, the prospects are undoubtedly exciting.
Importantly, the acellular properties of exosome-based therapies have significant advantages over traditional cell therapies. The use of whole cells in regenerative medicine is limited by issues such as immune rejection, poor cell implantation, and the risk of tumorigenesis. In contrast, exosomes, as naturally occurring vesicles, possess low immunogenicity and are less likely to provoke adverse immune reactions. This inherent safety, combined with their ease of storage and transport, makes them particularly attractive for clinical applications. Furthermore, their engineering capabilities-whether through overexpressing specific proteins like CD24 or loading therapeutic RNA molecules-broaden the range of potential interventions and enable the development of personalized medicine approaches tailored to individual patient needs.
From a societal perspective, the adoption of inhaled exosome therapy has far-reaching ethical and economic implications. As global healthcare systems grapple with challenges related to chronic inflammatory diseases, acute respiratory failure, and age-related decline, the introduction of such innovative therapies could significantly enhance patients’ quality of life and reduce long-term healthcare costs by lowering the incidence of complications and hospital readmissions. However, these benefits come with responsibilities that must be addressed through careful regulation, transparent clinical trials, and equitable access to advanced treatments. Establishing comprehensive ethical guidelines and regulatory frameworks will be crucial to ensure that the development and implementation of these new therapies are both safe and reasonable within the broader context of public health.
Looking to the future, the success of inhaled exosome therapy will rely on ongoing interdisciplinary collaboration. The combination of innovations in nanotechnology, bioengineering, and molecular biology with clinical research and regulatory science is crucial to overcoming the current limitations related to scalability, delivery optimization, and long-term safety. As research efforts expand, it is essential for both academic institutions and industry stakeholders to invest in large-scale randomized controlled trials to validate the efficacy and safety across different patient populations. Moreover, the development of standardized protocols for the isolation, characterization, and storage of exosomes will be fundamental to ensuring the reproducibility and quality of different therapeutic products.
The potential impact of inhaled exosome therapy on immune modulation, inflammatory repair, and anti-aging treatment is extensive and multifaceted. By harnessing the natural repair and regulatory capabilities of exosomes, these therapies offer a paradigm shift from traditional pharmaceutical approaches to more holistic, targeted, and personalized treatment strategies. Although challenges remain in areas such as large-scale production, delivery device optimization, and regulatory standardization, positive preclinical results and encouraging early clinical data provide a solid foundation for future advancements. With ongoing research efforts, strategic interdisciplinary collaboration, and rigorous regulatory oversight, inhaled exosomes are expected to become a cornerstone of next-generation therapeutic interventions, addressing unmet medical needs in respiratory diseases while also offering transformative potential for managing systemic inflammation, promoting tissue regeneration, and alleviating the effects of aging.
Exosome characteristics are biocompatible, prefer tumor recruitment, have tunable targeting efficiency, and are stable, making them outstanding and eye-catching medication delivery systems for cancer and other disorders. Exosomes, which are cell-derived nanovesicles, have a lot of potential for application in cancer immunotherapy due to their immunogenicity and molecular transfer function. More significantly, exosomes can transfer their cargo to specified cells and so affect the phenotypic and immune-regulation capabilities of those cells. The use of exosomes as drug-delivery systems for small compounds, macromolecules, and nucleotides has recently advanced.54
Especially, the Nucleic acids therapeutics represent a highly promising treatment approach in modern medicine. However, their therapeutics face numerous challenges in clinical practical applications, particularly regarding their stability, effectiveness, cellular uptake efficiency, and limitations in delivering them specifically to target lung tissues. To overcome these obstacles, researchers have developed various innovative delivery systems, including exosomes, lipid nanoparticles, inorganic nanoparticles, viral vectors, polymer nanoparticles, protein carriers, antibody oligonucleotide conjugates, and DNA nanostructure-based delivery systems.90,91
Our review provides a comprehensive overview of MSC-exosomes delivery systems by integrating the latest advancements in biomaterials science, nanotechnology, and gene editing technologies, emphasizing their transformative potential in precision medicine.
The journey ahead is both challenging and exciting, and we hope that the insights provided by this summary can inspire further innovation and clinical exploration. Inhalable exosome therapy embodies the fusion of cutting-edge science and patient-centered care, promising a future where precise, effective, and minimally invasive treatments become the new standard in medical practice. As we stand on the brink of this exciting transformation, the ongoing progress in this field has significant potential to enhance global healthcare outcomes, improve the lives of countless individuals, and reshape our understanding of regenerative medicine and immunotherapy.
Abbreviations
AdMSC-Exos, Adipose-derived mesenchymal stem cells; α-SMA, α-smooth muscle actin; ALI, Lung injury; ARDS, Acute respiratory distress syndrome; BALF, Bronchoalveolar lavage fluid; CAR, Chimeric antigen receptors; CCNE1, Cyclin E1; COL III, Collagen III; COL1A1, collagen I A1; COPD, Chronic obstructive pulmonary disease; CQA, Critical quality attributes; CS, Cigarette smoke; CT, Computed tomography; DLS, Dynamic light scattering; DPI, Dry Powder Inhaler; EEP, End-expiratory pause; EF50, Expiratory flow at 50% forced vital capacity; ELISA, Enzyme-linked immunosorbent assay; ESCRT, The endosomal sorting complexes required for transport; EXO-CD24, Exosomes with high expression of CD24; Exo-d-MAPPS, Exosome-derived Multiple Allogeneic Protein Paracrine Signaling; FN, Fibronectin; FVC, Forced vital capacity; H&E, Hematoxylin-eosin; HDGF, hepatoma-derived growth factor; hESC-Exos, human embryonic stem cells; HS, Hemorrhagic shock; HSF1-Exos, Exosomes from HSF1-overexpressing MSCs; hucMSCs, human umbilical cord mesenchymal stem cells; ILC2s, Innate lymphoid cells type 2; ILD, Interstitial lung disease; IL-1β, Interleukin-1 beta; IL-6, Interleukin-6; IL-10, Interleukin-10; ITGβ4, Integrin beta 4; LFBs, Lung fibroblasts; LPS, Lipopolysaccharide; LSC, Lung stem cells; MIP-2, Macrophage inflammatory protein-2; miRNA, microRNA; MMP-9, Metalloproteinase-9; MMP, Mitochondrial membrane potential; mRNA, messenger RNA; MSCs, Mesenchymal stem cells; MSC-Exos, MSC-derived exosomes; mtDNA, Mitochondrial DNA; MVBs, Subsequently maturing into multivesicular bodies; MVV, Maximum voluntary ventilation; NTA, Nanoparticle tracking analysis; OXPHOS, Oxidative phosphorylation; PEP, Platelet-derived exosome products; PEF, Peak expiratory flow; PF, Pulmonary fibrosis; PIF, Peak inspiratory flow; PTX, Polyether ether ketone; RI, Respiratory index; SEC, Size exclusion chromatography; SP-C, Surfactant protein-C; sEVs, small extracellular vesicles; SGRQ, St. George’s Respiratory Questionnaire; SnCs, Senescent cell lines; SPR, Surface plasmon resonance; SSc, Severe systemic sclerosis; STAT3, Signal transducer and activator of transcription 3; TASMC, Tel Aviv Sourasky Medical Center; TEM, Transmission electron microscopy; TNF-α, Tumor necrosis factor alpha; Tregs, Regulatory T cells; TV, Tidal volume; VEGF-A, Vascular endothelial growth factor-A; YAP1, Yes-associated protein 1; VMN, Vibrating mesh nebulizer.
Data Sharing Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Acknowledgments
We would like to thank our colleagues and advisors for their valuable feedback and support during the preparation of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; We have agreed on the journal to which the article has been submitted and agreed to be accountable for all aspects of the work. Jinming Gou and Lina Zhang share the first authorship.
Funding
Beijing Municipal Administration of Hospital Incubating Program (PX2023059); The Capability Program of Beijing Tuberculosis & Thoracic Tumor Research Institute (NLTS2024-16); The National Natural Science Foundation of China (82260846); Beijing Municipal Public Welfare Development and Reform Pilot Project for Medical Research Institutes (JYY2023-14) and the Research Project of Inner Mongolia Medical University Affiliated Hospital (2023NYFYLHZD007) to YM P. The National Natural Science Foundation of China (62171441) to LN Z.
Disclosure
The authors have no competing interests to declare that are relevant to the content of this article.
References
1. Dan L, Chunlei L, Lun W, et al. Advances of exosomes extraction and its mechanism in early diagnosis of lung cancer. Chin J Lung Cancer. 2020;23(11):999–1006. doi:10.3779/j.issn.1009-3419.2020.101.24
2. Ali H, Heshu R, Alexander M, et al. Mesenchymal stem/stromal cell-derived exosomes in regenerative medicine and cancer; overview of development, challenges, and opportunities. Stem Cell Res Ther. 2021;12(1):297. doi:10.1186/s13287-021-02378-7
3. Prattichizzo F, Micolucci L, Cricca M, et al. Exosome-based immunomodulation during aging: a nano-perspective on inflamm-aging. Mech Ageing Dev. 2017;168:44–53. doi:10.1016/j.mad.2017.02.008
4. Gao Y, Liu MF, Li Y, et al. Mesenchymal stem cells-extracellular vesicles alleviate pulmonary fibrosis by regulating immunomodulators. World J Stem Cells. 2024;16(6):670–689. doi:10.4252/wjsc.v16.i6.670
5. Li S, Zhang J, Feng G, et al. The emerging role of extracellular vesicles from mesenchymal stem cells and macrophages in pulmonary fibrosis: insights into miRNA delivery. Pharmaceuticals. 2022;15(10):1276. doi:10.3390/ph15101276
6. Keshtkar S, Azarpira N, Ghahremani MH. Mesenchymal stem cell-derived extracellular vesicles: novel frontiers in regenerative medicine. Stem Cell Res Ther. 2018;9(1):63. doi:10.1186/s13287-018-0791-7
7. Masterson H, McCarthy D, O’Toole D, et al. The role of cells and their products in respiratory drug delivery: the past, present, and future. Expert Opin Drug Delivery. 2020;17(12):1689–1702. doi:10.1080/17425247.2020.1814732
8. Han Y, Zhu Y, Youngblood HA, et al. Nebulization of extracellular vesicles: a promising small RNA delivery approach for lung diseases. J Control Release. 2022;352:556–569. doi:10.1016/j.jconrel.2022.10.052
9. Kaspi H, Semo J, Abramov N, et al. MSC-NTF (NurOwn®) exosomes: a novel therapeutic modality in the mouse LPS-induced ARDS model. Stem Cell Res Ther. 2021;12(1):72. doi:10.1186/s13287-021-02143-w
10. Dos Santos CC, Lopes-Pacheco M, English K, et al. The MSC-EV-microRNAome: a perspective on therapeutic mechanisms of action in sepsis and ARDS. Cells. 2024;13(2):122. doi:10.3390/cells13020122
11. Hu Z, Zhu L, Zhu Y, Xu Y. Mesenchymal stem extracellular vesicles in various respiratory diseases: a new opportunity. J Inflamm Res. 2024;9041–9058. doi:10.2147/JIR.S480345
12. Abbaszadeh H, Ghorbani F, Abbaspour-Aghdam S, et al. Chronic obstructive pulmonary disease and asthma: mesenchymal stem cells and their extracellular vesicles as potential therapeutic tools. Stem Cell Res Ther. 2022;13(1):262. doi:10.1186/s13287-022-02938-5
13. Maremanda KP, Sundar IK, Rahman I. Protective role of mesenchymal stem cells and mesenchymal stem cell-derived exosomes in cigarette smoke-induced mitochondrial dysfunction in mice. Toxicol Appl Pharmacol. 2019;385:114788. doi:10.1016/j.taap.2019.114788
14. Harrell CR, Miloradovic D, Sadikot R, et al. Molecular and cellular mechanisms responsible for beneficial effects of mesenchymal stem cell-derived product “Exo-d-MAPPS” in attenuation of chronic airway inflammation. Anal Cell Pathol. 2020;2020:3153891. doi:10.1155/2020/3153891
15. Yao Z, Li J, Wang X, et al. MicroRNA-21-3p engineered umbilical cord stem cell-derived exosomes inhibit tendon adhesion. J Inflamm Res. 2020:303–316. doi:10.2147/JIR.S254879
16. Rizzo A, Bagwell S, Schiebel P, et al. Pulmonary biodistribution of platelet-derived regenerative exosomes in a porcine model. Int J Mol Sci. 2024;25(5):710–723. doi:10.3390/ijms25052642
17. Dinh PC, Paudel D, Brochu H, et al. Inhalation of lung spheroid cell secretome and exosomes promotes lung repair in pulmonary fibrosis. Nat Commun. 2020;11(1):1064. doi:10.1038/s41467-020-14344-7
18. Zhang WY, Wen L, Du L, et al. S-RBD-modified and miR-486-5p-engineered exosomes derived from mesenchymal stem cells suppress ferroptosis and alleviate radiation-induced lung injury and long-term pulmonary fibrosis. J Nanobiotechnol. 2024;22(1):662. doi:10.1186/s12951-024-02830-9
19. Wang X, Wan W, Jing L, et al. Inhalable FN-binding liposomes or liposome-exosome hybrid bionic vesicles encapsulated microparticles for enhanced pulmonary fibrosis therapy. Int J Pharm. 2024;656:124096. doi:10.1016/j.ijpharm.2024.124096
20. Li M, Huang H, Wei X, et al. Clinical investigation on nebulized human umbilical cord MSC-derived extracellular vesicles for pulmonary fibrosis treatment. Signal Transduct Target Ther. 2025;10(1):179. doi:10.1038/s41392-025-02262-3
21. Zheng W, Zhu T, Tang L, et al. Inhalable CAR-T cell-derived exosomes as paclitaxel carriers for treating lung cancer. J Transl Med. 2023;21(1):383. doi:10.1186/s12967-023-04206-3
22. Kim G, Lee Y, Junkyu H, et al. Engineering exosomes for pulmonary delivery of peptides and drugs to inflammatory lung cells by inhalation. J Control Release. 2021;330:684–695. doi:10.1016/j.jconrel.2020.12.053
23. Nazmul S, Iffath M, Maryam A, et al. Exosomes in osteoarthritis: a review on their isolation techniques and therapeutic potential. Indian J Orthop. 2024;58(7):866–875. doi:10.1007/s43465-024-01175-7
24. Jiaqi T, Zhengpu H, Dandan S, et al. Engineered exosome for drug delivery: recent development and clinical applications. Int J Nanomed. 2023;18:7923–7940. doi:10.2147/IJN.S444582
25. Ning X, Shao Y, Kaili Y, et al. Mesenchymal stem cell-derived exosomes attenuate phosgene-induced acute lung injury in rats. Inhalation Toxicol. 2019;31(2):52–60. doi:10.1080/08958378.2019.1597220
26. Jia D, Huan Z, Han J, et al. HSF1 enhances the attenuation of exosomes from mesenchymal stem cells to hemorrhagic shock induced lung injury by altering the protein profile of exosomes. Int Immunopharmacol. 2023;123:110693. doi:10.1016/j.intimp.2023.110693
27. Nahla H, Hanaa M. Exosomal therapy is a luxury area for regenerative medicine. Tissue Cell. 2024;91:102570. doi:10.1016/j.tice.2024.102570
28. Xia L, Zhang C, Nianyin L, et al. AdMSC-derived exosomes alleviate acute lung injury via transferring mitochondrial component to improve homeostasis of alveolar macrophages. Theranostics. 2022;12(6):2928–2947. doi:10.7150/thno.69533
29. Qian L, Chen P, Zhang S, et al. The uptake of extracellular vesicles: research progress in cancer drug resistance and beyond. Drug Resist Updates. 2025:101209. doi:10.1016/j.drup.2025.101209
30. Orooji N, Fadaee M, Kazemi T, et al. Exosome therapeutics for non-small cell lung cancer tumorigenesis. Cancer Cell Int. 2024;24(1):360. doi:10.1186/s12935-024-03544-6
31. Nie H, Xie X, Zhang D, et al. Use of lung-specific exosomes for miRNA-126 delivery in non-small cell lung cancer. Nanoscale. 2020;12(2):877–887. doi:10.1039/c9nr09011h
32. Yang M, Zhou W, Han X, et al. Modified bone marrow mesenchymal stem cells derived exosomes loaded with MiRNA ameliorates non-small cell lung cancer. J Cell Mol Med. 2024;28(18):e70115. doi:10.1111/jcmm.70115
33. Jeong K, Yu YJ, You JY, et al. Exosome-mediated microRNA-497 delivery for anti-cancer therapy in a microfluidic 3D lung cancer model. Lab Chip. 2020;20(3):548–557. doi:10.1039/c9lc00958b
34. Gao W, Yang N, Yin C, et al. Engineered exosomes loaded with miR-563 inhibit lung cancer growth. J Oncol. 2022;2022:6141857. doi:10.1155/2022/6141857
35. Zhou W, Xu M, Wang Z, et al. Engineered exosomes loaded with miR-449a selectively inhibit the growth of homologous non-small cell lung cancer. Cancer Cell Int. 2021;21(1):485. doi:10.1186/s12935-021-02157-7
36. Chrzanowski W, Kim Y, McClements L. Can stem cells beat COVID-19: advancing stem cells and extracellular vesicles toward mainstream medicine for lung injuries associated with SARS-CoV-2 infections. Front Bioeng Biotechnol. 2020;554. doi:10.3389/fbioe.2020.00554
37. Shapira S, Ben M, Hay-Levi M, et al. A novel platform for attenuating immune hyperactivity using EXO-CD24 in COVID-19 and beyond. EMBO Mol Med. 2022;14(9):e15997. doi:10.15252/emmm.202215997
38. Masoud K-N, Hesam H, Ali M, et al. Application of stem cell-derived exosomes in anterior segment eye diseases: a comprehensive update review. The Ocular Surface. 2025;36:209–219. doi:10.1016/j.jtos.2025.01.012
39. Murgia N, Akgun M, Blanc PD, et al. Issue 3-The occupational burden of respiratory diseases, an update. Pulmonology. 2025;31(1):2416808. doi:10.1016/j.pulmoe.2024.03.004
40. Liu P, Yang S, Shao X, et al. Mesenchymal stem cells-derived exosomes alleviate acute lung injury by inhibiting alveolar macrophage pyroptosis. Stem Cells Transl Med. 2024;13(4):371–386. doi:10.1093/stcltm/szad094
41. Chen F, Chen Z, Wu HT, et al. Mesenchymal stem cell-derived exosomes attenuate murine cytomegalovirus-infected pneumonia via NF-κB/NLRP3 signaling pathway. Viruses. 2024;16(4):619. doi:10.3390/v16040619
42. Shi MM, Yang QY, Monsel A, et al. Preclinical efficacy and clinical safety of clinical-grade nebulized allogenic adipose mesenchymal stromal cells-derived extracellular vesicles. J Extracell Vesicles. 2021;10(10):e12134. doi:10.1002/jev2.12134
43. Kudinov VA, Artyushev RI, Zurina IM, et al. Inhaled placental mesenchymal stromal cell secretome from two- and three-dimensional cell cultures promotes survival and regeneration in acute lung injury model in mice. Int J Mol Sci. 2022;23(7):3417. doi:10.3390/ijms23073417
44. Green O, Shenberg G, Baruch R, et al. Inhaled exosomes genetically manipulated to overexpress CD24 (EXO-CD24) as a compassionate use in severe ARDS patients. Biomedicines. 2023;11(9):2523. doi:10.3390/biomedicines11092523
45. Zubair M, Abouelnazar FA, Iqbal MA, et al. Mesenchymal stem cell-derived exosomes as a plausible immunomodulatory therapeutic tool for inflammatory diseases. Front Cell Dev Biol. 2025:1563427. doi:10.3389/fcell.2025.1563427
46. Liang D, Liu C, Yang M. Mesenchymal stem cells and their derived exosomes for ALI/ARDS: a promising therapy. Heliyon. 2023;9(10):e20387. doi:10.1016/j.heliyon.2023.e20387
47. Guo H, Su Y, Deng F. Effects of mesenchymal stromal cell-derived extracellular vesicles in lung diseases: current status and future perspectives. Stem Cell Rev Rep. 2021;17(2):440–458. doi:10.1007/s12015-020-10085-8
48. Liu C, Lu J, Yuan T, et al. EPC-exosomal miR-26a-5p improves airway remodeling in COPD by inhibiting ferroptosis of bronchial epithelial cells via PTGS2/PGE2 signaling pathway. Sci Rep. 2023;13(1):6126. doi:10.1038/s41598-023-33151-w
49. Ouyang C, Wang W, Wu D, et al. Analysis of serum exosome microRNAs in the rat model of chronic obstructive pulmonary disease. Am J Transl Res. 2023;15(1):138–150.
50. Qin L, Liu N, Bao CL, et al. Mesenchymal stem cells in fibrotic diseases-the two sides of the same coin. Acta Pharmacol Sin. 2023;44(2):268–287. doi:10.1038/s41401-022-00952-0
51. Chen W, Peng J, Tang X, et al. MSC-derived exosome ameliorates pulmonary fibrosis by modulating NOD 1/NLRP3-mediated epithelial-mesenchymal transition and inflammation. Heliyon. 2024;11(2):e41436. doi:10.1016/j.heliyon.2024.e41436
52. Liang J, Zhao J, Yang L, et al. MSC-exosomes pretreated by Danshensu extracts pretreating to target the hsa-miR-27a-5p and STAT3-SHANK2 to enhanced antifibrotic therapy. Stem Cell Res Ther. 2025;16(1):40. doi:10.1186/s13287-025-04181-0
53. Assar S, Mohammadzadeh D, Norooznezhad AH, et al. Improvement in the clinical manifestations of interstitial lung disease following treatment with placental mesenchymal stromal cell extracellular vesicles in a patient with systemic sclerosis: a case report. Respir Med Case Rep. 2023:101923. doi:10.1016/j.rmcr.2023.101923
54. Agarwal P, Anees A, Harsiddharay RK, et al. A comprehensive review on exosome: recent progress and outlook. Pharm Nanotechnol. 2023. doi:10.2174/2211738511666230523114311
55. Madhyastha R, Madhyastha H, Nurrahmah QI, et al. MicroRNA 21 elicits a pro-inflammatory response in macrophages, with exosomes functioning as delivery vehicles. Inflammation. 2021;44:1274–1287. doi:10.1007/s10753-021-01415-0
56. Liu X, Gao C, Wang Y, et al. BMSC-derived exosomes ameliorate LPS-induced acute lung injury by miR-384-5p-controlled alveolar macrophage autophagy. Oxid Med Cell Longev. 2021;2021:9973457. doi:10.1155/2021/9973457
57. Shang Y, Sun Y, Xu J, et al. Exosomes from mmu_circ_0001359-modified ADSCs attenuate airway remodeling by enhancing FoxO1 signaling-mediated M2-like macrophage activation. Mol Ther Nucleic Acids. 2020:951–960. doi:10.1016/j.omtn.2019.10.049
58. Wei X, Yi X, Lv H, et al. MicroRNA-377-3p released by mesenchymal stem cell exosomes ameliorates lipopolysaccharide-induced acute lung injury by targeting RPTOR to induce autophagy. Cell Death Dis. 2020;11:657. doi:10.1038/s41419-020-02857-4
59. Zhu L, Xu Y, Wang J, et al. Mesenchymal stem cells-derived exosomes carrying microRNA-30b confer protection against pulmonary fibrosis by downregulating Runx1 via Spred2. Mol Genet Genomics. 2024;299(1):33. doi:10.1007/s00438-024-02116-7
60. Guiot J, Cambier M, Boeckx A, et al. Macrophage-derived exosomes attenuate fibrosis in airway epithelial cells through delivery of antifibrotic miR-142-3p. Thorax. 2020;75(10):870–881. doi:10.1136/thoraxjnl-2019-214077
61. Weng Z, Zhang B, Wu C, et al. Therapeutic roles of mesenchymal stem cell-derived extracellular vesicles in cancer. J Hematol Oncol. 2021;14(1):136. doi:10.1186/s13045-021-01141-y
62. Khan FH, Reza MJ, Shao YF, et al. Role of exosomes in lung cancer: a comprehensive insight from immunomodulation to theragnostic applications. Biochim Biophys Acta Rev Cancer. 2022;1877(5):188776. doi:10.1016/j.bbcan.2022.188776
63. Zhao M, Liu S, Wang C, et al. Mesenchymal stem cell-derived extracellular vesicles attenuate mitochondrial damage and inflammation by stabilizing mitochondrial DNA. ACS Nano. 2021;15(1):1519–1538. doi:10.1021/acsnano.0c08947
64. Chen Y, Du Z, Jiang W, et al. Engineered IFNγ-loaded exosomes reprogram macrophage polarization and suppress tumor cell proliferation in vitro. Int Immunopharmacol. 2025;162:115170. doi:10.1016/j.intimp.2025.115170
65. Peng J, Li S, Li B, et al. Exosomes derived from M1 macrophages inhibit the proliferation of the A549 and H1299 lung cancer cell lines via the miRNA-let-7b-5p-GNG5 axis. PeerJ. 2023;11:e14608. doi:10.7717/peerj.14608
66. Song S, Zhao Y, Wang X, et al. M2 macrophages-derived exosomal miR-3917 promotes the progression of lung cancer via targeting GRK6. Biol Chem. 2022;404(1):41–57. doi:10.1515/hsz-2022-0162
67. Fang H, Chi X, Wang M, et al. M2 macrophage-derived exosomes promote cell proliferation, migration and EMT of non-small cell lung cancer by secreting miR-155-5p. Mol Cell Biochem. 2025;480(5):3019–3032. doi:10.1007/s11010-024-05161-3
68. Mansouri N, Willis GR, Fernandez-Gonzalez A, et al. Mesenchymal stromal cell exosomes prevent and revert experimental pulmonary fibrosis through modulation of monocyte phenotypes. JCI Insight. 2019;4(21):e128060. doi:10.1172/jci.insight.128060
69. Kang J, Hua P, Wu X, et al. Exosomes: efficient macrophage-related immunomodulators in chronic lung diseases. Front Cell Dev Biol. 2024:1271684. doi:10.3389/fcell.2024.1271684
70. Long Y, Yang B, Lei Q, et al. Targeting senescent alveolar epithelial cells using engineered mesenchymal stem cell-derived extracellular vesicles to treat pulmonary fibrosis. ACS Nano. 2024;18(9):7046–7063. doi:10.1021/acsnano.3c10547
71. Kletukhina S, Mutallapova G, Titova A, Gomzikova M. Role of mesenchymal stem cells and extracellular vesicles in idiopathic pulmonary fibrosis. Int J Mol Sci. 2022;23(19):11212. doi:10.3390/ijms231911212
72. Azhdari MH, Goodarzi N, Doroudian M, et al. Molecular insight into the therapeutic effects of stem cell-derived exosomes in respiratory diseases and the potential for pulmonary delivery. Int J Mol Sci. 2022;23(11):6273. doi:10.3390/ijms23116273
73. Zhu YG, Shi M, Monsel A, et al. Nebulized exosomes derived from allogenic adipose tissue mesenchymal stromal cells in patients with severe COVID-19: a pilot study. Stem Cell Res Ther. 2022;13(1):220. doi:10.1186/s13287-022-02900-5
74. Bi Y, Qiao X, Cai Z, et al. Exosomal miR-302b rejuvenates aging mice by reversing the proliferative arrest of senescent cells. Cell Metab. 2025;37(2):527–541.e6. doi:10.1016/j.cmet.2024.11.013
75. Zhuansun Y, Du Y, Huang F, et al. MSCs exosomal miR-1470 promotes the differentiation of CD4+CD25+FOXP3+ Tregs in asthmatic patients by inducing the expression of P27KIP1. Int Immunopharmacol. 2019:105981. doi:10.1016/j.intimp.2019.105981
76. Cui J, Xu H, Yu J, et al. IL-4 inhibits regulatory T cells differentiation by HDAC9-mediated epigenetic regulation. Cell Death Dis. 2021;12(6):501. doi:10.1038/s41419-021-03769-7
77. Mao YM, Zhao CN, Leng J, et al. Interleukin-13: a promising therapeutic target for autoimmune disease. Cytokine Growth Factor Rev. 2019:9–23. doi:10.1016/j.cytogfr.2018.12.001
78. Huang H, Zhu J, Gu L, et al. TLR7 mediates acute respiratory distress syndrome in sepsis by sensing extracellular miR-146a. Am J Respir Cell Mol Biol. 2022;67(3):375–388. doi:10.1165/rcmb.2021-0551OC
79. Wang S, Yang Y, Suen A, et al. Role of extracellular microRNA-146a-5p in host innate immunity and bacterial sepsis. Iscience. 2021;24(12):103441. doi:10.1016/j.isci.2021.103441
80. Dong B, Wang C, Zhang J, et al. Exosomes from human umbilical cord mesenchymal stem cells attenuate the inflammation of severe steroid-resistant asthma by reshaping macrophage polarization. Stem Cell Res Ther. 2021;12(1):204. doi:10.1186/s13287-021-02244-6
81. Shan L, Liu S, Zhang Q, et al. Human bone marrow-mesenchymal stem cell-derived exosomal microRNA-188 reduces bronchial smooth muscle cell proliferation in asthma through suppressing the JARID2/Wnt/β-catenin axis. Cell Cycle. 2022;21(4):352–367. doi:10.1080/15384101.2021.2020432
82. Feng CY, Bai SY, Li ML, et al. Adipose-derived mesenchymal stem cell-derived exosomal miR-301a-3p regulates airway smooth muscle cells during asthma by targeting STAT3. J Asthma Allergy. 2022:99–110. doi:10.2147/JAA.S335680
83. Chen S, Gao J, Zhang T. From mesenchymal stem cells to their extracellular vesicles: progress and prospects for asthma therapy. Asian J Pharm Sci. 2024;19(4):100942. doi:10.1016/j.ajps.2024.100942
84. Chen W, Huang Y, Han J, et al. Immunomodulatory effects of mesenchymal stromal cells-derived exosome. Immunol Res. 2016;64(4):831–840. doi:10.1007/s12026-016-8798-6
85. Mortaz E, Alipoor SD, Varahram M, et al. Exosomes in severe asthma: update in their roles and potential in therapy. Biomed Res Int. 2018;2018:2862187. doi:10.1155/2018/2862187
86. Cheema NA, Castagna A, Ambrosani F, et al. Extracellular vesicles in asthma: intercellular cross-talk in TH2 inflammation. Cells. 2025;14(7):542. doi:10.3390/cells14070542
87. Finicelli M, Digilio FA, Galderisi U, et al. The emerging role of macrophages in chronic obstructive pulmonary disease: the potential impact of oxidative stress and extracellular vesicle on macrophage polarization and function. Antioxidants. 2022;11(3):464. doi:10.3390/antiox11030464
88. Jin C, Yixin S, Yong M, et al. Engineering of MSC-derived exosomes: a promising cell-free therapy for osteoarthritis. Membranes. 2022;12(8). doi:10.3390/membranes12080739
89. Jianghong H, Jianyi X, Lei Y, et al. Cell-free exosome-laden scaffolds for tissue repair. Nanoscale. 2021;13(19):8740–8750. doi:10.1039/d1nr01314a
90. Ullah A, Khan M, Zhang Y, et al. Advancing therapeutic strategies with polymeric drug conjugates for nucleic acid delivery and treatment. Int J Nanomed. 2025;20:25–52. doi:10.2147/IJN.S429279
91. Bian X, Zhou L, Luo Z, et al. Emerging delivery systems for enabling precision nucleic acid therapeutics. ACS Nano. 2025;19(4):4039–4083. doi:10.1021/acsnano.4c11858
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.