Back to Journals » Drug Design, Development and Therapy » Volume 19
Infusion-Related Reactions Among Cancer Patients Receiving Immune Checkpoint Inhibitors: The ARON-MOUSEION-013 Systematic Review and Meta-Analysis
Authors Vitale E ![]() , Rizzo A, Maistrello L, Cauli O
, Rizzo A, Maistrello L, Cauli O ![]() , Brunetti O, Monteiro FSM, Soares A, Santoni M, Mollica V, Massari F
, Brunetti O, Monteiro FSM, Soares A, Santoni M, Mollica V, Massari F
Received 29 August 2025
Accepted for publication 6 December 2025
Published 13 December 2025 Volume 2025:19 Pages 11107—11118
DOI https://doi.org/10.2147/DDDT.S560518
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Elsa Vitale,1 Alessandro Rizzo,2 Lorenza Maistrello,3 Omar Cauli,4 Oronzo Brunetti,2 Fernando Sabino Marques Monteiro,5,6 Andrey Soares,5,7 Matteo Santoni,8 Veronica Mollica,9,* Francesco Massari9,10,*
1Directorate of Health Professions and Nursing, ASL, Bari, Italy; 2S.S.D. C.O.r.O. Bed Management Presa in Carico, TDM, IRCCS Istituto Tumori “Giovanni Paolo II”, Bari, 70124, Italy; 3IRCCS San Camillo Hospital, Venice, Italy; 4Universitat de València, Valencia, Spain; Frailty and Cognitive Impairment Organized Group (FROG),University of Valencia, Valencia, 46010, Spain; 5Latin American Cooperative Oncology Group - LACOG, Porto Alegre, RS, Brazil; 6Oncology and Hematology Department, Hospital Sírio-Libanês, Brasilia, DF, Brazil; 7Hospital Israelita Albert Einstein, São Paulo, SP, Brazil; 8Oncology Unit, Macerata Hospital, Macerata, Italy; 9Medical Oncology, IRCCS Azienda Ospedaliero-Universitaria Di Bologna, Bologna, Italy; 10Department of Medical and Surgical Sciences (DIMEC), University of Bologna, Bologna, Italy
*These authors contributed equally to this work
Correspondence: Alessandro Rizzo, S.S.D. C.O.r.O. Bed Management Presa in Carico, TDM, IRCCS Istituto Tumori “Giovanni Paolo II”, Viale Orazio Flacco 65, Bari, 70124, Italy, Email [email protected]
Purpose: To investigate the incidence of Infusion-Related Reactions (IRRs) among cancer patients receiving Immune Checkpoint Inhibitors (ICIs) and immune-based combinations.
Patients and Methods: The ARON-MOUSEION-013 was registered in PROSPERO (CRD420251018433). Observational, randomized and quasi-experimental studies were included in the present review, and rates in IRR among cancer adults (≥ 18 years) receiving ICIs were recorded and then analyzed.
Results: A total of 4 records were considered for analyses, with a total of 55 observations and 35 events. The overall prevalence of IRR, considering Any Grade, was 67.4% [95% CI: 3.9%; 99.1%]. Considering Grade ≥ 3, a total of 55 observations and 8 events were registered. The overall prevalence of irAEs in IRRs was 6% [95% CI: 0.2%; 74.7%].
Conclusion: Mild-to-moderate IRRs are not rare events in patients receiving ICIs. IRRs may be avoided to manage these infusions slowly; however, severe reactions require emergency handling.
Keywords: immunotherapy, infusion-related reactions, injection site reaction, neoplasms, cancer
Introduction
Unfavorable reactions to the infusion of biological or pharmacological substances are known as infusion-related reactions (IRRs), according to the National Cancer Institute (NCI).1 IRRs may occur with several parenterally delivered anticancer therapies, ranging from cytotoxic chemotherapy to immune checkpoint inhibitors (ICIs), whether administered intravenously or subcutaneously.2 IRRs occur on the day of or the day after infusion and commonly resolve 2 days after onset. The frequency of IRR varies widely,3–5 since numerous parameters impact on this, as autoimmune disorders, B cell malignancies, prophylaxis regimens with or without corticosteroids and subsequent infusions. The incidence of IRR decreases with subsequent infusions.3
These reactions are rarely severe (grade 3 or 4) and reported in 10% of patients,6,7 more present in B-cell malignancies than in autoimmune disorders.8 In a previous study collecting data from 2005 to 2015 on IRR frequency in cancer patients, the steroid administrations prevent IRR.9 In autoimmune disorders, corticosteroid use in prophylaxis was strictly associated to a decrease in IRR rate.8 In autoimmune disorders, IRRs are lower, also due to the administration of corticosteroids.10 The frequency of severe IRR is less than 5% in appropriate premedication procedure, close monitoring and urgent management whenever it is needed.11
The essential element, which is most recorded to be linked to IRR occurrence and severity, is the lymphocyte count.3 However, when assessing clinical stage, tumor burden is not linked to the occurrence of IRR,7,9 indicating that the concentration of targeted cells, rather than tumor progression, is an important element for the occurrence of IRR.12
IRR immune manifestations can theoretically develop from several processes, like: IgE mediated hypersensitivity or anaphylactic reaction, immunogenicity of ICI treatments, complement activation and cytokine-release syndrome (CRS).13 In all these cases, clinical manifestations are very similar. All these reactions can be tested by elevated serum level of tryptase.14 It was initially suggested that IRR was activated by the complement system activation which rapidly occurred after ICIs administrations, correlating cytokine secretion and the complement activation with the severity of IRR. Conversely, it was observed that higher frequency and severity of IRR reduced complement activation. Thus, complement activation may be not considered the main initiator in IRR.15
However, adverse events remained a concern requiring further investigations, since both the pathogenic process of IRR and its related mechanism remain unknown. IRR induces the secretion of cytokines, which interact with NK cells. Evidence supports that this interaction may cause the secretion of cytokines by both NK cells and B cells.16
To prevent a possible IRR, patients can receive premedication with diphenhydramine and acetaminophen. Treatment related IRR management is provided in the study protocol, and a careful evaluation has been requested to confirm or exclude other potential causes.17
Regarding cytotoxic agents, the most frequently linked to infusion responses drugs include procarbazine, bleomycin, taxanes, pegylated liposomal doxorubicin, asparaginase, and platinum salts.18 Risk factors for standard infusion reactions for cytotoxic agents include previous allergic reactions, asthma, female sex, higher drug doses, iodine and seafood allergies, preexisting cardiac or pulmonary dysfunction, previous exposure to the drug, concomitant β-adrenergic blocker therapy, and concurrent autoimmune disease.19
The symptoms related to IRRs typically present as low-grade fever, chills, headache, or nausea. High-grade reactions can include additional symptoms of tachycardia, changes in blood pressure, hypoxemia, chest pain, cough, shortness of breath, wheezing, flushing, sweating, urticaria or pruritis, angioedema, and presyncope or syncope.20
Both immune-mediated and non-immune-mediated mechanisms may be involved in the development of IRRs, which are often categorized as non-allergic reactions or immune-mediated reactions (or true allergies) to foreign proteins.21 In the case of the IRRs-induced by ICIs, it is generally assumed that less than 5% of patients receiving immunotherapy present a severe reaction to the infusion, but this prevalence depends on several factors such as the drugs and its specific immune system targets.22 Immune responses can be innate, adaptive or both.1 The innate response is the body’s first line of defense: a rapid, nonspecific response that is triggered by the chemical properties of an antigen. The innate response involves macrophages, neutrophils, natural killer cells, dendritic cells, basophils, eosinophils, antimicrobial peptides and proteins. The IRRs mediated by innate immunity are present before the exposure of the foreign substance and are generally unaffected by repeated exposure. In contrast, in IRRs mediated by adaptive immunity, each successive exposure to the drug enhances the immune system’s defensive response and increases its effects. The adaptive response involves T cells, B cells, antigen-presenting cells and antibodies.23
In ICIS, the IRRs related symptomatology might largely differ in terms of severity, also differently affecting physiological systems, and widely differing from patient to patient and between therapeutic agents.24 For example, in the case of the anti-PD-L1 antibody, like avelumab, the IRRs are predominantly grade 1–3 in severity and manifest as chills, pyrexia and flushing.25,26 Regarding the prevalence, in avelumab-induced IRRs, it has been reported to be approximately one-quarter of all patients.17 A peculiar case among ICIs is the antibody avelumab, a fully human IgG1 monoclonal antibody that targets programmed death-ligand 1 (PD-L1) and that retains an intact Fc region, resulting in the ability to induce antibody-dependent cell-mediated cytotoxicity.18 For nivolumab, a PD-1 immune checkpoint inhibitor antibody, the frequency of drug-related hypersensitivity/infusion reactions of any grade varies from 1.6%, including two grade 3 anaphylactic reactions and one grade 4 hypersensitivity, to 5.3%; for pembrolizumab (another PD-1 immune checkpoint inhibitor antibody), the frequency reported in clinical trials was 2%.27 In case of severe reaction to the antibody infusion, the drug infusion should be discontinued and appropriate medical treatment should be administered.
Consequently, IRRs can be frequent, appearing mostly at first infusion, and requiring a specific premedication consisting in antihistamine and acetaminophen prior to the first 4 infusions.28
Because of previous inconsistencies and disparities in the terminology, grading, and reporting of the occurrence of IRRs, it has been challenging to determine the incidence of IRRs, and despite the paucity of research on the topic, what is known about it indicates that the occurrence of IRRs varies depending on the cancer type, anticancer therapies, and administration of anticancer therapies.22,29
The recent years have seen the development and advent of novel combination strategies based on immunotherapy and ICI–based treatment has established itself as a mainstay in several hematological and solid tumors.30–37 While the advent of immune checkpoint inhibitors that work by blocking the PD-L1 protein such as pembrolizumab, nivolumab, atezolizumab, durvalumab, avelumab, as well as the emerging of combinations of ICIs with anticancer agents, have represented a key step forward, some challenges remain, including the onset of toxicities, commonly defined as immune-related adverse events (irAEs).38–40 Among adverse events related to ICIs, evidence regarding the onset of IRRs is sparse in this setting.40
Herein, the ARON-MOUSEION-013 systematic review and meta-analysis aimed to investigate the incidence of IRRs among cancer patients receiving ICIs and immune-based combinations.
Materials and Methods
Research Procedure
The MOUSEION-013 was registered in PROSPERO (CRD420251018433) and carried out with the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) (Figure 1).41 The PRISMA 2020 flow diagram templates are distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/
 |
Figure 1 The PRISMA flowchart for records procedure. |
MeSH terms adopted as keywords were “Immunotherapy”, “Injection Site Reaction” and “Neoplasms” and research was performed throughout Embase, PubMed, Scopus and Web of Science databases without any time limits (Supplementary File 1).
Research question was recognized using the PIO approach (Supplementary File 2).
Inclusion and Exclusion Criteria
Only records published in English language and available in their full text versions were included. Moreover, observational, randomized and quasi-experimental studies were included in the present review. Rates in IRR symptomatology among cancer adults (≥18 years) receiving immune checkpoint inhibitor treatments were recorded and then analyzed.
The Selection Process
Identified records were registered in a systematic database search and uploaded to reference management software and then duplicates were excluded. Two independent reviewers (E.V. and L.M.) assessed their titles and abstracts to further include or exclude other selected records. Only the included articles were uploaded, and their full text versions were deeply evaluated for their eligibility. Disagreements on the selection process were discussed and, if the disagreement persisted, a new combined evaluation was performed, included a third reviewer in the discussion (A.R.).
Data was collected considering author(s), year of publication, sample size, and proportion of IRRS as adverse effects among cancer patients treated with immunotherapy.
Risk of Bias (Quality) Assessment
In observational studies, the presence of Risk of Bias was investigated using the risk of bias of exposures (ROBINS-E) tool.42 The tool consisted of seven sub dimensions exploring the presence of bias in the obtained results. These sub dimensions were recognized a shown in Figure 2.
 |
Figure 2 Risk of Bias assessment (Original). |
Strategy for Data Synthesis
Studies were assessed for quality, and their related information was highlighted in a narrative approach thanks to Table 1. Statistical analysis was performed using the R environment (version 4.4.2) and the significance level of the analysis was set at P < 0.05.
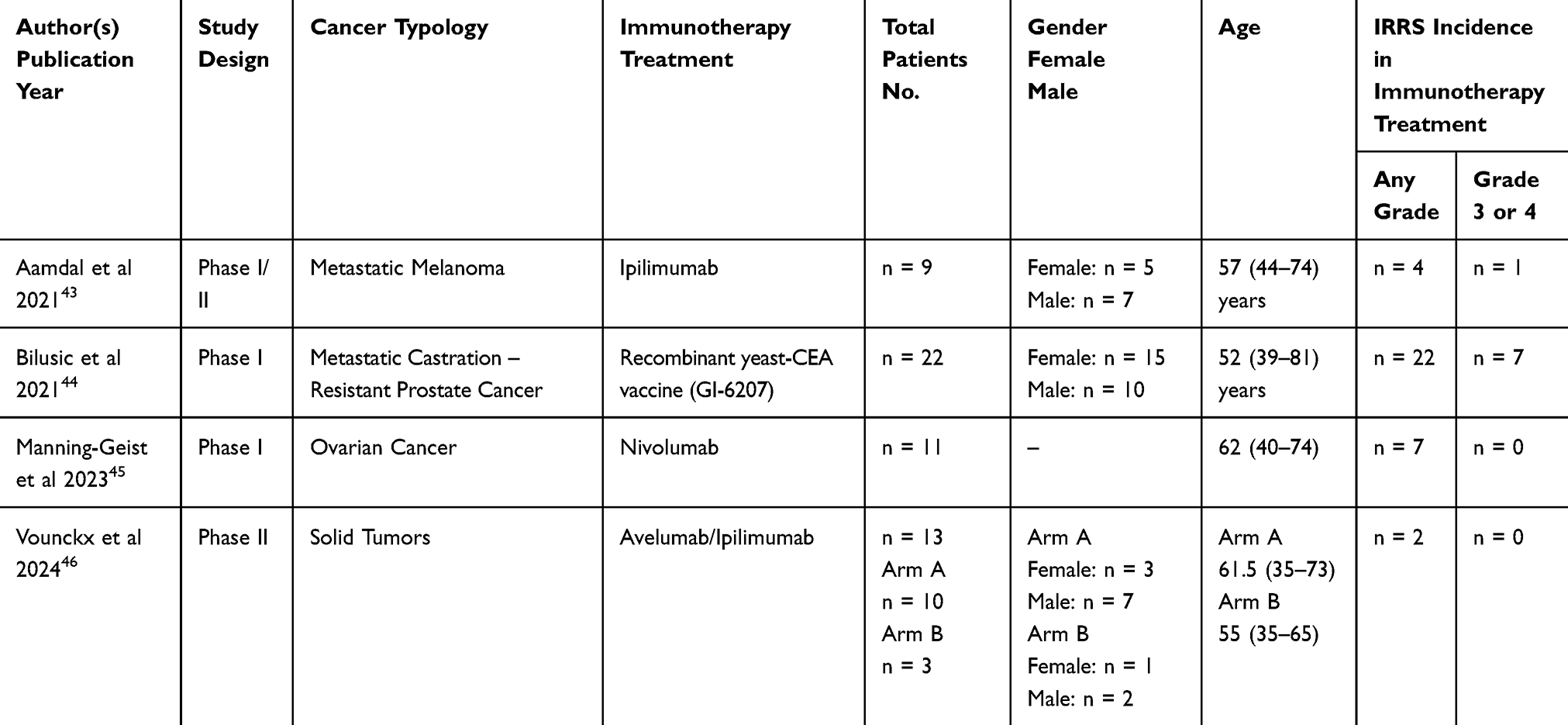 |
Table 1 Characteristics of the Selected Studies (n = 4) |
The primary outcome of this meta-analysis was the proportion of subjects for whom the adverse event occurred (defined as the number of patients with at least one infusion site reactions event (irAE) divided by the total number of patients). To this research, a meta-analysis for proportions aimed at investigating the proportion of subjects for whom infusion site reactions events occurred among patients undergoing immunotherapy.47
The effect size for each study was assessed using a logit transformation of the proportion of subjects for whom IRRs after immunotherapy infusions.48
A generalized linear mixed model (GLMM) with a logit link function was employed to estimate the pooled effect, allowing for both within-study variability and between-study heterogeneity to be explicitly modeled.49 A random-effects model was specified using the Hartung-Knapp adjustment to obtain more conservative and robust confidence intervals for the pooled estimates. Proportions were calculated for any grade of irAE and for grade ≥ 3 and two separate subgroup meta-analyses were performed, specifically one for any grade and one for grade ≥ 3, respectively.
Heterogeneity among studies was assessed using χ2-based Q test. A significant Q value (P < 0.05) suggested the presence of significant heterogeneity between included studies. Additionally, the I-squared inconsistency index (I2) was used to assess the percentage of true variability in the observed effects.50,51 I2 statistics were adopted with 25%, 50%, and 75% indicating low, moderate, and high heterogeneity degrees, respectively. Because we expected a high degree of heterogeneity among studies, a random-effects pooling models were implemented.51
Forest Plots was generated to report the results of the meta-analysis. Publication bias was not formally assessed, as the number of included studies (n = 4) was below the recommended threshold for reliable evaluation using funnel plot–based methods or Egger’s test.52
Results
Selected Studies
A total of 2786 records were identified from Embase (n = 2277), PubMed (n = 127), Scopus (n = 379) and Web of Science (n = 3) databases. Of those, 2052 records were excluded as 6 were duplicates and 2046 did not deal with IRRs or not cancer diseases. Thus, 734 were further read in their abstracts, and 727 were additionally removed since they did not focus on IRRs symptoms. Finally, 4 records were considered for analysis43–46 referring to Embase (n = 2), PubMed (n = 1) and Scopus (n = 1) databases (Figure 1). All features of the included studies were displayed in Table 1 included the main IRRs symptomatology differentiated between “any grade” and “grade 3 or 4”.
Any Grade
A total of 4 studies were included for these analyses, with a total of 55 observations and 35 events.35–38 A moderate heterogeneity was present among the studies (P < 0.001; tau2 = 5.03; I2 = 42.7% with a 95% C.I.: [0%; 80.8%]). The result of the meta-analysis shown in the Forest Plot (Figure 3) displayed the overall prevalence of adverse event infusion site reactions, considering Any Grade, was 67.4% (95% CI: [3.9%; 99.1%]). Both the symmetry of the Funnel Plot (Figure 4) and the Eggers’ test (β = 3.88; 95% CI = [−3.91; 11.67]; P = 0.432) indicate that no publication bias was present. The limited number of studies included could reduce the statistical power to identify such bias.
 |
Figure 3 Forest Plot in proportion for Any Grade. |
 |
Figure 4 Contour-enhanced Funnel Plot for Any Grade. |
Grade ≥ 3
Four studies were considered for this analysis, with a total of 55 observations and 8 events. The heterogeneity between the studies was not significant (P = 0.729; tau2 = 2.13; I2 = 0%; 95% CI: [0%; 84.7%]). The Forest Plot (Figure 5) reported the overall prevalence of irAEs in IRRs considering Grade ≥ 3 was 6.2% [95% CI: 0.2%; 74.7%]. Both the Funnel Plot (Figure 6) and the Eggers’ test (β = −2.42; 95% CI: [−2.67; −2.18; P = 0.003) indicated the presence of publication bias. Likewise, the small sample of studies may have reduced the power to detect bias.
 |
Figure 5 Forest Plot in proportion for Grade ≥ 3. |
 |
Figure 6 Contour-enhanced Funnel Plot for Grade ≥ 3. |
Discussion
The MOUSEION-013 systematic review and meta-analysis explored the rate of IRRs among cancer patients receiving ICIs and immune-based combinations.
Nowadays, combination therapy with ICIs for cancer is increasing. IRRs represent an issuefor cancer patients also implicating intensive challenges in oncology practices.53–56
Most cancer treatments, covering both cytotoxic agents and biologics, could raise risk for infusion reactions and their related symptomatology could vary from mild to moderate intensity, such as flushing to life-threatening events.57 During the infusion of ICIs, several irAEs have just been associated to different severe hypersensitivity reactions, like a complex of chills, fever, nausea, asthenia, headache, skin rash and pruritus.58–60 However, etiologies in ICIs infusion reactions continued to be ambiguous. ICIs interplayed with their molecular factors in blood and tumor cells, promoting the secretion of inflammatory cytokines, being involved in a wide range of symptoms linked with infusion reactions,61 as fever, chills, nausea, vomiting, hypotension, and dyspnea.62 Thus, we conducted a meta-analysis to systematically investigate the incidence rate of IRRs among cancer patients treated with ICIs, since we did not find any RCTs to compare the incidence in ICIs that in chemotherapy or placebo counterparts.
Our 55 observations and 35 events reported 67.4% (95% CI: [3.9%; 99.1%]) prevalence in irAEs of IRRs in Any Grade with no publication bias (Figures 3 and 4). On the other hand, considering Grade ≥ 3, the prevalence registered was 6% (95% CI: [0%; 38.7%]) with also the presence of publication bias (Figures 4 and 5). This potential bias should be interpreted with caution, as Egger’s test is known to have limited statistical power when applied to meta-analyses with a small number of studies, which is the case for this subgroup. The apparent asymmetry could also reflect true heterogeneity in study design, patient populations, or reporting standards rather than systematic bias. Nevertheless, the presence of bias cannot be excluded and underscores the need for more high-quality studies reporting severe IRRs to strengthen the robustness of future meta-analyses. Anyway, also in phases III and IV, IRRs incidence is quite low, as reported in the Supplementary File 3. However, literature explained that ICIs combinations and their related irAEs varied from cancer typologies and therapeutic protocols.63–65 Thus, some studies have begun to deeply investigate the irAEs caused by added toxicities and the clinical value associated.66,67
A recent meta-analysis focused on IRRs in patients with genitourinary tumors treated with ICIs, including 10,001 patients from 12 RCTs showed that the combination of ICIs to other therapies resulted in higher rates of grade 1–5 IRRs but not grade 3–5. In the subgroup of patients with RCC, the combination of ICI plus tyrosine kinase inhibitor (TKI) compared to sunitinib did not increase the risk of IRRs.68 The increasingly widespread use of ICIs in oncology and other medical disciplines must ensure patient safety and optimal outcomes, requiring careful monitoring at the start of infusion, rapid recognition and appropriate clinical assessment of IRRs and their severity, followed by prompt treatment. The lack of standardization in the prevention, management, and reporting of IRRs in cancer treating institutions represents not only a quality and safety gap but also a disparity in care.
Since IRRs have been reported as a frequent adverse effect in ICIs, training and communication among an expert and/or specialist and also oncology nurses should be considered as a key element to achieve a successful management of those patients69,70 to better manage them in these irAEs. Additionally, patient education seemed to be essential to also provide patient-specific educational materials to early identify signs or symptoms of an irAE.71 In this way, a prompt IRR management could avoid fatal conditions,72,73 with inevitably infusion rate reductions until interruptions according to the grade of severity.74
The ARON-MOUSEION-013 systematic review and meta-analysis had some strengths and limitations to be acknowledged. Among the strengths of the current analysis, the study included several different clinical trials by using the most updated data in terms of safety and adverse events, and belonged to the international MOUSEION projects, that has seen the publication of several papers and studies exploring irAEs in cancer patients receiving immunotherapeutic agents. However, some limitations should be underlined. First, the current meta-analysis was based on pooled data, and thus, the presence of confounding factors and single-patient variables (eg, patient age, comorbidities, concomitant medications, etc.) was not included. Second, all trials included patients treated with heterogeneous systemic treatments; all these agents present different and not superimposable efficacy and safety profiles, and thus, this element could have produced some bias affecting our results. Thus, the presence of selection bias cannot be excluded. However, the small number of available studies limited the statistical power of the meta-analysis and results in wide confidence intervals reducing the precision of the pooled estimates. Therefore, the present results should be interpreted with more caution. On the other hand, the present study represented a quantitative summary of the existing evidence and could serve as a reference point for the incidence of IRRs in cancer patients receiving immunotherapy.
Conclusions
ICIs and their related combinations have modified the scenario of cancer treatments.
Both physicians and nurses should pay attention to the safety profile to reach the optimal management of these patients with the highest clinical benefit.71 Mild-to-moderate IRRs were reported in the current literature for ICIs. Thus, IRRs may be avoided to manage these infusions slowly; however, severe reactions require emergency handling.75,76 However, future larger prospective studies will be necessary to better recognize IRRs incidence in ICIs administration, also to better organize ongoing training in this important issue including the care team to ensure that serious IRRs are avoided and promptly identified also including patient education, awareness, early detection and involvement.77
Author Contributions
Conceptualization, E.V., A.R., F.S.M.M., A.S. and V.L.; methodology, E.V. and L.M.; software, L.M.; validation, A.R. and L.M.; formal analysis, L.M.; investigation, E.V., A.R., L.M.; data curation, E.V., A.R., L.M.; writing—original draft preparation, E.V.; writing—review and editing, E.V., V.M., O.C.; visualization, O.C., E.V., A.R., F.M., M.S.; supervision, E.V., A.R., O.B., A.S., F.S.M.M. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding. The authors affiliated to the IRCCS Istituto Tumori “Giovanni Paolo II”, Bari are responsible for the views expressed in this article, which do not necessarily represent the Institute.
Disclosure
Dr Andrey Soares reports personal fees from Janssen, Pfizer, Bayer, Merck Serono, Novartis, Astra Zeneca and Adium, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Vogel WH. Infusion reactions. Clin J Oncol Nurs. 2010;14:E10–E21. doi:10.1188/10.cjon.e10-e21
2. Roselló S, Blasco I, Fabregat LG, Cervantes A, Jordan K. Management of infusion reactions to systemic anticancer therapy: ESMO clinical practice guidelines. Ann Oncol. 2017;28:iv100–iv118. doi:10.1093/annonc/mdx216
3. Topalian SL, Weiner GJ, Pardoll DM. Cancer immunotherapy comes of age. J Clin Oncol. 2011;29(36):4828–4836. doi:10.1200/JCO.2011.38.0899
4. Wahid B, Ali A, Rafique S, et al. An overview of cancer immunotherapeutic strategies. Immunotherapy. 2018;10(11):999–1010. doi:10.2217/imt-2018-0002
5. Koury J, Lucero M, Cato C, et al. Immunotherapies: exploiting the immune system for cancer treatment. J Immunol Res. 2018;2018:9585614. doi:10.1155/2018/9585614
6. Xu H, Tan P, Zheng X, et al. Immune-related adverse events following administration of anti-cytotoxic T-lymphocyte-associated protein-4 drugs: a comprehensive systematic review and meta-analysis. Drug Des Devel Ther. 2019;13:2215–2234. doi:10.2147/DDDT.S196316
7. Weber JS, Postow M, Lao CD, Schadendorf D. Management of adverse events following treatment with anti-programmed death-1 agents. oncologist. 2016;21(10):1230–1240. doi:10.1634/theoncologist.2016-0055
8. Govindan R, Szczesna A, Ahn MJ, et al. Phase III trial of ipilimumab combined with paclitaxel and carboplatin in advanced squamous non-small-cell lung cancer. J Clin Oncol. 2017;35(30):3449–3457. doi:10.1200/JCO.2016.71.7629
9. Lim YJ, Koh J, Kim K, Chie E, Kim K. Clinical Implications of cytotoxic t lymphocyte antigen-4 expression on tumor cells and tumor-infiltrating lymphocytes in extrahepatic bile duct cancer patients undergoing surgery plus adjuvant chemoradiotherapy. Targeted Oncol. 2017;12(2):211–218. doi:10.1007/s11523-016-0474-1
10. Curkovic NB, Bai K, Ye F, Johnson DB. Incidence of cutaneous immune-related adverse events and outcomes in immune checkpoint inhibitor-containing regimens: a systematic review and meta-analysis. Cancers. 2024;16(2):340. doi:10.3390/cancers16020340
11. Berman D, Parker SM, Siegel J, et al. Blockade of cytotoxic T-lymphocyte antigen-4 by ipilimumab results in dysregulation of gastrointestinal immunity in patients with advanced melanoma. Cancer Immunity. 2018;10:11.
12. Fakhrejahani F, Tomita Y, Maj-Hes A, Trepel JB, De Santis M, Apolo AB. Immunotherapies for bladder cancer: a new hope. Curr Opin Urolo. 2015;25(6):586–596. doi:10.1097/MOU.0000000000000213
13. Doessegger L, Banholzer ML. Clinical development methodology for infusion-related reactions with monoclonal antibodies. Clin. Transl. Immunol. 2015;4(7):e39. doi:10.1038/cti.2015.14
14. Sachs B, Merk HF. Akute Überempfindlichkeitsreaktionen auf monoklonale Antikörper zur zielgerichteten Therapie Acute hypersensitivity reactions associated with monoclonal antibodies for targeted therapy. Der Hautarzt; Zeitschrift fur Dermatologie, Venerologie, und verwandte Gebiete. 2018;69(4):268–277. doi:10.1007/s00105-018-4142-5
15. Satterlee AB, Yuan H, Huang L. A radio-theranostic nanoparticle with high specific drug loading for cancer therapy and imaging. J Control Release. 2015;217:170–182. doi:10.1016/j.jconrel.2015.08.048
16. Zhang B, Wu Q, Zhou YL, Guo X, Ge J, Fu J. Immune-related adverse events from combination immunotherapy in cancer patients: a comprehensive meta-analysis of randomized controlled trials. Int Immunopharmacol. 2018;63:292–298. doi:10.1016/j.intimp.2018.08.014
17. Kelly K, Infante JR, Taylor MH, et al. Safety profile of avelumab in patients with advanced solid tumors: a pooled analysis of data from the Phase 1 JAVELIN solid tumor and Phase 2 JAVELIN Merkel 200 clinical trials. Cancer. 2018;124(9):2010–2017. doi:10.1002/cncr.31293
18. Boyerinas B, Jochems C, Fantini M, et al. Antibody-dependent cellular cytotoxicity activity of a novel anti-PD-L1 antibody avelumab (MSB0010718C) on human tumor cells. Cancer Immunol Res. 2015;3(10):1148–1157. doi:10.1158/2326-6066.CIR-15-0059
19. Peterson DC. An AP perspective on infusion reactions in the era of immunotherapy. J Adv Pr Oncol. 2022;13:247–252. doi:10.6004/jadpro.2022.13.3.13
20. Schneider BJ, Naidoo J, Santomasso BD, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: ASCO guideline update. J Clin Oncol. 2021;39:4073–4126. doi:10.1200/jco.21.01440
21. Bernardez B, Franco B, Mayo N, et al. Real world of infusion related reactions in an oncology outpatient clinic. J Clin Oncol. 2018;36:e18872–e18872. doi:10.1200/jco.2018.36.15_suppl.e18872
22. Barroso A, Estevinho F, Hespanhol V, Teixeira E, Ramalho-Carvalho J, Araújo A. Management of infusion-related reactions in cancer therapy: strategies and challenges. ESMO Open. 2024;9:102922. doi:10.1016/j.esmoop.2024.102922
23. Stewart JM, Keselowsky BG. Combinatorial drug delivery approaches for immunomodulation. Adv. Drug Delivery Rev. 2017;114:161–174. doi:10.1016/j.addr.2017.05.013
24. Martins F, Sofiya L, Sykiotis GP, et al. Adverse effects of immune-checkpoint inhibitors: epidemiology, management and surveillance. Nat Rev Clin Oncol. 2019;16:563–580. doi:10.1038/s41571-019-0218-0
25. Gulley JL, Kelly K. Infusion-related reactions with administration of avelumab: mild and manageable side effects. Transl Cancer Res. 2017;6:S1296–S1298. doi:10.21037/tcr.2017.09.44
26. Vitale E, Rizzo A, Maistrello L, et al. Sex differences in adverse events among cancer patients receiving immune checkpoint inhibitors: the MOUSEION-07 systematic review and meta-analysis. Sci Rep. 2024;14(1):28309. doi:10.1038/s41598-024-71746-z
27. Eigentler TK, Hassel JC, Berking C, et al. Diagnosis, monitoring and management of immune-related adverse drug reactions of anti-PD-1 antibody therapy. Cancer Treat Rev. 2016;45:7–18. doi:10.1016/j.ctrv.2016.02.003
28. Bavencio (Avelumab) Injection. Darmstadt, Germany: Merck KGaA; 2017.
29. Rizzo A, Ricci AD, Brandi G. Trans-arterial chemoembolization plus systemic treatments for hepatocellular carcinoma: an update. J Pers Med. 2022;12:1788. doi:10.3390/jpm12111788
30. Gandhi L, Rodríguez-Abreu D, Gadgeel S, et al. Pembrolizumab plus chemotherapy in metastatic non–small-cell lung cancer. N Engl J Med. 2018;378:2078–2092. doi:10.1056/nejmoa1801005
31. Rizzo A, Cusmai A, Acquafredda S, et al. KEYNOTE-522, IMpassion031 and GeparNUEVO: changing the paradigm of neoadjuvant immune checkpoint inhibitors in early triple-negative breast cancer. Futur Oncol. 2022;18:2301–2309. doi:10.2217/fon-2021-1647
32. Rizzo A, Mollica V, Massari F. Expression of programmed cell death ligand 1 as a predictive biomarker in metastatic urothelial carcinoma patients treated with first-line immune checkpoint inhibitors versus chemotherapy: a systematic review and meta-analysis. Eur Urol Focus. 2022;8:152–159. doi:10.1016/j.euf.2021.01.003
33. Garon EB, Rizvi NA, Hui R, et al. Pembrolizumab for the treatment of non–small-cell lung cancer. N Engl J Med. 2015;372:2018–2028. doi:10.1056/nejmoa1501824
34. Schmid P, Cortes J, Pusztai L, et al. Pembrolizumab for early triple-negative breast cancer. N Engl J Med. 2020;382:810–821. doi:10.1056/nejmoa1910549
35. Janjigian YY, Kawazoe A, Bai Y, et al. Pembrolizumab in HER2-positive gastric cancer. New Engl J Med. 2024;391:1360–1362. doi:10.1056/nejmc2408121
36. Powles T, Valderrama BP, Gupta S, et al. Enfortumab vedotin and pembrolizumab in untreated advanced urothelial cancer. New Engl J Med. 2024;390:875–888. doi:10.1056/nejmoa2312117
37. Santoni M, Buti S, Myint ZW, et al. Real-world outcome of patients with advanced renal cell carcinoma and intermediate- or poor-risk international metastatic renal cell carcinoma database consortium criteria treated by immune-oncology combinations: differential effectiveness by risk group? Eur Urol Oncol. 2023;7:102–111. doi:10.1016/j.euo.2023.07.003
38. Sanchez K, Page DB, Urba W. Immunotherapy Toxicities. Surg Oncol Clin North Am. 2019;28:387–401. doi:10.1016/j.soc.2019.02.009
39. Thompson JA, Schneider BJ, Brahmer J, et al. Management of Immunotherapy-related toxicities, version 1.2022, NCCN clinical practice guidelines in oncology. J Natl Compr Cancer Netw. 2022;20:387–405. doi:10.6004/jnccn.2022.0020
40. Price M. Acute infusion-related reactions: how to recognize and intervene when these reactions occur in practice. Clin J Oncol Nurs. 2021;25:591–594. doi:10.1188/21.cjon.591-594
41. Page MJ, McKenzie JE, Bossuyt PM, et al. he PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:71. doi:10.1136/bmj.n71
42. Higgins JP, Morgan RL, Rooney AA, et al. A tool to assess risk of bias in non-randomized follow-up studies of exposure effects (ROBINS-E). Environ Int. 2024;186:108602. doi:10.1016/j.envint.2024.108602
43. Aamdal E, Inderberg EM, Ellingsen EB, et al. Combining a universal telomerase based cancer vaccine with ipilimumab in patients with metastatic melanoma - five-year follow up of a phase i/iia trial. Front Immunol. 2021;12. doi:10.3389/fimmu.2021.663865
44. Bilusic M, McMahon S, Madan A, et al. Phase I study of a multitargeted recombinant Ad5 PSA/MUC-1/brachyury-based immunotherapy vaccine in patients with metastatic castration-resistant prostate cancer (mCRPC). J Immunother Cancer. 2021;9:e002374. doi:10.1136/jitc-2021-002374
45. Manning-Geist BL, Gnjatic S, Aghajanian C, et al. Phase I Study of a Multivalent WT1 Peptide Vaccine (Galinpepimut-S) in Combination with Nivolumab in Patients with WT1-Expressing Ovarian Cancer in Second or Third Remission. Cancers. 2023;15:1458. doi:10.3390/cancers15051458
46. Vounckx M, Tijtgat J, Stevens L, et al. A randomized Phase II clinical trial of stereotactic body radiation therapy (SBRT) and systemic pembrolizumab with or without intratumoral avelumab/ipilimumab plus CD1c (BDCA-1)+/CD141 (BDCA-3)+ myeloid dendritic cells in solid tumors. Cancer Immunol Immunother. 2024;73:1–8. doi:10.1007/s00262-024-03751-0
47. Lipsey MW, Wilson DB. Practical Meta-Analysis. Sage Publications, Inc. Thousand Oaks; 2001.
48. Stijnen T, Hamza TH, Özdemir P. Random effects meta-analysis of event outcome in the framework of the generalized linear mixed model with applications in sparse data. Stat Med. 2010;29:3046–3067. doi:10.1002/sim.4040
49. Deeks JJ, Higgins JP, Altman DG. on behalf of the cochrane statistical methods group. analysing data and undertaking meta‐analyses. In: Cochrane Handbook for Systematic Reviews of Interventions. Hoboken, NJ, USA: John Wiley & Sons, Ltd.;2019:241–284. doi:10.1002/9781119536604.ch10
50. Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–560. doi:10.1136/bmj.327.7414.557
51. Knapp G, Hartung J. Improved tests for a random effects meta‐regression with a single covariate. Stat Med. 2003;22:2693–2710. doi:10.1002/sim.1482
52. Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–634. doi:10.1136/bmj.315.7109.629
53. Carneir BA, Safran H, Beck JTT, et al. Phase 1 first-in-human study of PF-07257876, a novel CD47/PD-L1 bispecific checkpoint inhibitor, in patients with PD-1/PD-L1-refractory and-naïve advanced solid tumors. J Clin Oncol. 2023;41. doi:10.1200/JCO.2023.41.16_suppl.2529
54. Matsui HM, Hazama S, Nakajima M, et al. Novel adjuvant dendritic cell therapy with transfection of heat-shock protein 70 messenger RNA for patients with hepatocellular carcinoma: a phase I/II prospective randomized controlled clinical trial. Cancer Immunol Immunother. 2020;70:945–957. doi:10.1007/s00262-020-02737-y
55. Tran B, Voskoboynik M, Bendell J, et al. A phase 1 study of the CD40 agonist MEDI5083 in combination with durvalumab in patients with advanced solid tumors. Immunotherapy. 2024;16:759–774. doi:10.1080/1750743x.2024.2359359
56. Schwartzberg LS, Stepanski EJ, Fortner BV, Houts AC. Retrospective chart review of severe infusion reactions with rituximab, cetuximab, and bevacizumab in community oncology practices: assessment of clinical consequences. Support Care Cancer. 2007;16:393–398. doi:10.1007/s00520-007-0329-5
57. Lenz H-J. Management and preparedness for infusion and hypersensitivity reactions. Oncol. 2007;12:601–609. doi:10.1634/theoncologist.12-5-601
58. Dillman RO. Infusion reactions associated with the therapeutic use of monoclonal antibodies in the treatment of malignancy. Cancer Metastasis Rev. 1999;18:465–471. doi:10.1023/a:1006341717398
59. Hara T, Suzuki R, Ohno A, et al. Safe administration of rituximab for follicular lymphoma after obinutuzumab infusion-related reaction. Int J Hematol. 2019;111:585–590. doi:10.1007/s12185-019-02793-w
60. Hiddemann W, Barbui AM, Canales MA, et al. Immunochemotherapy with obinutuzumab or rituximab for previously untreated follicular lymphoma in the GALLIUM study: influence of chemotherapy on efficacy and safety. J Clin Oncol. 2018;36:2395–2404. doi:10.1200/jco.2017.76.8960
61. Breslin S. Cytokine-release syndrome: overview and nursing implications. Clin J Oncol Nurs. 2007;11:37–41. doi:10.1188/07.cjon.s1.37-42
62. Chen X, Li P, Tian B, Kang X. Serious adverse events and coping strategies of CAR-T cells in the treatment of malignant tumors. Front Immunol. 2022;13:1079181. doi:10.3389/fimmu.2022.1079181
63. Robinson M, Geirnaert M, Anderson B, McKibbin L. Canada’s first joint oncology-allergy clinic: successful desensitization to trastuzumab following severe anaphylactic reaction in which epinephrine was inappropriately withheld. Curr Oncol. 2023;30:2862–2868. doi:10.3390/curroncol30030218
64. Shipp C, Speigl L, Janssen N, Martens A, Pawelec G. A clinical and biological perspective of human myeloid-derived suppressor cells in cancer. Cell Mol Life Sci. 2016;73:4043–4061. doi:10.1007/s00018-016-2278-y
65. Martinez SA, Segal NH, Cercek A, et al. Simplified graded infusion strategy for mitigation of oxaliplatin hypersensitivity. Clin Color Cancer. 2022;21:149–153. doi:10.1016/j.clcc.2022.01.006
66. Rafiq S, Butchar JP, Cheney C, et al. Comparative assessment of clinically utilized CD20-directed antibodies in chronic lymphocytic leukemia cells reveals divergent nk cell, monocyte, and macrophage properties. J Immunol. 2013;190:2702–2711. doi:10.4049/jimmunol.1202588
67. Sørensen N, Jensen P, Clasen‐Linde E, Larsen JM, El‐Galaly T. Fatal cardiac arrhythmia caused by tumor lysis in a patient with diffuse large B‐cell lymphoma upon start of R‐CHOP. Clin Case Rep. 2018;6:490–493. doi:10.1002/ccr3.1390
68. Montgomery RB, Lynch JA, Brown J, et al. Remote delivery of cancer genetic testing in veterans with metastatic prostate cancer: a Million Veteran Program study. J Clin Oncol. 2024;42. doi:10.1200/jco.2024.42.4_suppl.60
69. Chung C, Rome A, Desai M, Abanonu F, De la Casas C. Optimizing multidisciplinary treatment-related adverse effects detection and reduction in patients undergoing active cancer treatments in ambulatory infusion centers. JCO Oncol Pr. 2022;18:e1553–e1561. doi:10.1200/op.21.00910
70. Brockow K, Schallmayer S, Beyer K, et al. Effects of a structured educational intervention on knowledge and emergency management in patients at risk for anaphylaxis. Allergy. 2015;70:227–235. doi:10.1111/all.12548
71. Boutros C, Tarhini A, Routier E, et al. Safety profiles of anti-CTLA-4 and anti-PD-1 antibodies alone and in combination. Nat Rev Clin Oncol. 2016;13:473–486. doi:10.1038/nrclinonc.2016.58
72. Chung CH. Managing premedications and the risk for reactions to infusional monoclonal antibody therapy. Oncol. 2008;13:725–732. doi:10.1634/theoncologist.2008-0012
73. D’arena G, Simeon V, Laurenti L, et al. Adverse drug reactions after intravenous rituximab infusion are more common in hematologic malignancies than in autoimmune disorders and can be predicted by the combination of few clinical and laboratory parameters: results from a retrospective, multicenter study of 374 patients. Leuk Lymphoma. 2017;58:2633–2641. doi:10.1080/10428194.2017.1306648
74. Almuhizi F, Sanchez LDLV, Gilbert L, Copaescu AM, Isabwe GAC. Premedication protocols to prevent hypersensitivity reactions to chemotherapy: a literature review. Clin Rev Allergy Immunol. 2022;62:534–547. doi:10.1007/s12016-022-08932-2
75. Thompson LM, Eckmann K, Boster BL, et al. Incidence, risk factors, and management of infusion-related reactions in breast cancer patients receiving trastuzumab. Oncol. 2014;19:228–234. doi:10.1634/theoncologist.2013-0286
76. Cáceres MC, Guerrero-Martín J, Pérez-Civantos D, Palomo-López P, Delgado-Mingorance JI, Durán-Gómez N. The importance of early identification of infusion-related reactions to monoclonal antibodies. Ther Clin Risk Manag. 2019;15:965–977. doi:10.2147/tcrm.s204909
77. Apolo AB, Infante JR, Balmanoukian A, et al. Avelumab, an anti-programmed death-ligand 1 antibody, in patients with refractory metastatic urothelial carcinoma: results from a multicenter, phase ib study. J Clin Oncol. 2017;35(19):2117–2124. doi:10.1200/JCO.2016.71.6795
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.