Back to Journals » Clinical Ophthalmology » Volume 20
Influence of Refractive Error, Age, and Ophthalmic Anatomical Characteristics on Refractive Surgery Choices
Authors Wörtz G ![]() , Wiley WF, Donaldson KE
, Wiley WF, Donaldson KE
Received 23 October 2025
Accepted for publication 15 January 2026
Published 22 January 2026 Volume 2026:20 576219
DOI https://doi.org/10.2147/OPTH.S576219
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Gary Wörtz,1 William F Wiley,2 Kendall E Donaldson3
1Commonwealth Eye Surgery, Lexington, KY, USA; 2Cleveland Eye Clinic, Brecksville, OH, USA; 3Bascom Palmer Eye Institute, Plantation, FL, USA
Correspondence: Gary Wörtz, Commonwealth Eye Surgery, 2353 Alexandria Drive, #260, Lexington, KY, 40504, USA, Tel +1(859)224-2655, Email [email protected]
Purpose: To assess the characteristics of patients presenting to American-European Congress of Ophthalmic Surgery (AECOS) member practices for vision correction procedures and determine how age, refractive error, and ophthalmic anatomical characteristics determine the choice of refractive procedure.
Patients and Methods: This retrospective multicenter cohort study included data of myopic patients who underwent bilateral refractive surgery in 2023 at 18 refractive surgery practices. Study parameters included the procedure performed, surgical location, manifest refraction (MRSE), Pentacam D value, anterior chamber depth, and central pachymetry.
Results: Overall, 1,866 eyes of 933 patients were included. LASIK was the most common refractive surgery procedure (65.5%), followed by ICL (13.3%), PRK (12.1%), and KLEx (8.6%). Of all the procedures, 59.4% were performed in a laser suite, 26.3% in an in-office operating room (OR), 13.8% in an ambulatory surgery center (ASC), and 0.5% in a hospital OR. The mean MRSE was − 4.36 D. Among laser vision correction procedures (LASIK, PRK, and KLEx), 43.6% had low myopia (MRSE range: − 0.25 to − 3.00 D), 43.1% had moderate (− 3.01 to − 6.00 D), and 13.3% had high myopia (> 6.00 D). Among all ICL cases, 3.6%, 21.0%, and 75.4% were performed in low, moderate, and high myopes, respectively. Among eyes that underwent LASIK or KLEx, 2.8% had thinner corneas (central pachymetry < 500 μm), which was significantly lower than 12.4% of eyes undergoing PRK (p< 0.001) and 11.7% of those undergoing ICL surgery (p< 0.001).
Conclusion: The study’s findings help to understand and better define the refractive surgery choices made by patients and surgeons. LASIK contributed to almost two-thirds of the refractive surgery procedures.
Keywords: refractive surgery trends, phakic IOL, laser vision correction, implantable collamer lens, office-based surgery
Introduction
Refractive surgery has been performed in the US for more than 25 years. The contemporary refractive surgery practice offers patients the opportunity for spectacle independence with both corneal and lens-based technologies. Corneal refractive surgery procedures include laser in situ keratomileusis (LASIK), photorefractive keratectomy (PRK), and femtosecond laser keratorefractive lenticule extraction (KLEx) procedures, such as small-incision lenticular extraction (SMILE). Excimer lasers in the US are approved to treat up to 12.00 D of myopia and 6.00 D of astigmatism. The VisuMax femtosecond laser (Carl Zeiss Meditec AG, Jena, Germany) used in most KLEx procedures in the US is approved to treat up to 10.00 D of myopia and up to 3.00 D of astigmatism. Corneal laser refractive surgery may not be appropriate for patients with thin or compromised corneas, very high myopia, or a projected high rate of tissue removal from the laser treatment.1–4
Lens-based refractive surgery options include implantation of a phakic intraocular lens or removal of the crystalline lens and replacement with an intraocular lens (IOL) in a refractive lens exchange (RLE). The STAAR EVO Implantable Collamer Lens (ICL) implanted in phakic IOL surgeries is approved for between 3.00 and 20.00 D of myopia and up to 4.00 D of astigmatism.5 RLE can be performed with any commercially-available IOL but is typically delayed until patients have lost significant accommodative capabilities with their natural lens. Lens-based surgery is more invasive than corneal laser refractive surgery; however, it may provide more spectacle freedom for presbyopic patients and those who have even the early stages of dysfunctional lens syndrome.
Extensive market information is available on the total number of procedures performed in the US, based on laser cards and lenses sold. In the early years of refractive surgery, Leaming and Duffey published annual surveys that addressed surgeons’ refractive choices and thresholds for various refractive procedures.6–10 Since then, despite technology advancements, there have been almost no published studies focusing on the patient characteristics that determine which refractive procedure is selected for treatment. Additionally, there is little information about the influence of type and degree of refractive error or other patient characteristics that determine the procedures that are offered by surgeons and ultimately selected by patients in the contemporary refractive surgery practice.
The purpose of this study was to enhance the understanding of the characteristics of patients presenting to AECOS member practices for vision correction procedures and to analyze how age, refractive error, and ophthalmic anatomical characteristics determine the choice of refractive procedure. Additionally, this study was designed to gather insights regarding the procedure site of service.
Materials and Methods
This retrospective chart review was conducted in accordance with the tenets of the Declaration of Helsinki and was approved by the Salus Independent Review Board with a waiver of informed consent, as data were collected as a part of routine clinical practice. No protected health information was collected, and anonymized data was used for analysis.
The authors conducted this retrospective study on behalf of the AECOS Refractive Interest Group. Nineteen participating refractive surgeons at 18 private practices were asked to collect retrospective data on myopic patients who underwent refractive surgery in 2023. Cases were recorded beginning 12/31/2023 and working backwards until 100 eyes of 50 patients had been recorded by each practice. This provided data from a sample of 1,866 eyes from AECOS participating sites across the US.
All of the participating sites included in the study had access to the lens-based vision correction options (phakic IOL/RLE) and one or more of the laser vision correction technologies (LASIK/PRK/KLEx) from various manufacturers. Patients aged 18 to 45 years with healthy eyes undergoing bilateral refractive surgery were included in the analysis. This age range was chosen to encompass patients who would generally have been eligible to undergo either lens-based or cornea-based vision correction procedures and who had not yet developed cataracts or significant presbyopia. Refractive surgery is considered to be elective surgery; as such, insurance coverage or authorization was generally not relevant to determining procedure choice in the evaluated cases. Eyes that were undergoing treatment for hyperopia, re-treatment, treatment post-keratoplasty, phototherapeutic keratectomy (PTK), relaxing incisions only, or any refractive surgery performed in conjunction with cataract surgery, intracorneal ring segments, or corneal collagen cross-linking were excluded. Also, patients requiring more than one refractive treatment (bioptics or enhancement procedures) were excluded.
Data collected included patient demographic information, laterality, date of surgery, procedure performed, surgical location, and pre-operative manifest refraction. In addition, ACD (anterior chamber depth - distance from the epithelium to the anterior surface of the lens (anterior capsule), or AQD (aqueous depth - distance from the endothelium to the anterior capsule of the lens), as routinely used by the site depending upon the measurement device available, central pachymetry, and Pentacam “Final D” value (if a site used the Pentacam device for screening) were also collected. The final “D” value from the Pentacam’s Belin/Ambrósio Enhanced Ectasia Display (BAD) is a diagnostic score used to assess the risk of corneal ectasia following surgery.11,12 A final D value of less than 1.6 is considered normal; between 1.6 and 2.6 suggests a suspicion of ectasia; and a value greater than 2.6 indicates a high risk of developing ectasia.11,12
Statistical Analysis
No a priori hypothesis testing was performed in the present study; therefore, no a priori sample size calculations were performed. A sample of 100 from each participating surgeon was planned to yield a fairly large sample of ~1900 eyes across the participating clinical sites. Data analysis was performed using SPSS software version 27 for Windows (IBM SPSS Statistics 27, IBM Inc., Armonk, NY). Descriptive statistics on continuous variables included mean and standard deviation, where appropriate. For categorical/ordinal data, the descriptive values included frequencies or percentages. Normality of the scale data was checked using the Kolmogorov–Smirnov test. Analyses were planned post hoc to identify statistically significant trends and associations/correlations, where applicable. Analyses stratifying results by the availability of KLEx technology and volume of ICL surgery per center were also conducted.
For the comparison of the scale data between two subgroups (where applicable), an independent t-test was used if data were normally distributed, or the non-parametric counterpart, the Mann–Whitney test was used for non-normally distributed data. To compare proportions, the Chi-square test was used. All analyses were exploratory, and they were run on the observed data (no imputations were performed) and not adjusted for multiplicity. P values of <0.05 were considered statistically significant.
Logistic regression was used to evaluate the association of demographic (patient age and gender) and baseline parameters, such as sphere, cylinder, MRSE, Pentacam D value, ACD, AQD, and pachymetry, on the choice of refractive procedure. Variables showing p <0.05 in the binary logistic regression were again assessed in multiple logistic regression to identify the association of these parameters with the procedure choice.
Results
In all, 1,866 eyes of 933 patients were included in the analysis. Table 1 shows the demographic and refractive characteristics of patients across all the refractive procedures analyzed. The mean age of patients was 31.7. LASIK was the most commonly performed refractive surgery procedure overall (65.5%), followed by ICL (13.3%), PRK (12.1%), and KLEx (8.6%) (Figure 1A). Among the 18 practices reporting data, LASIK ranged from 5.9% to 100% of each practice’s total refractive procedures during the study period; PRK from 0% to 66.7%; ICL from 0% to 34.7%; KLEx from 0% to 65%; and RLE from 0% to 6.1%. In a subgroup analysis of patients with myopia >3.0 D, the percentage of patients receiving ICL was 20% (241/1,197).
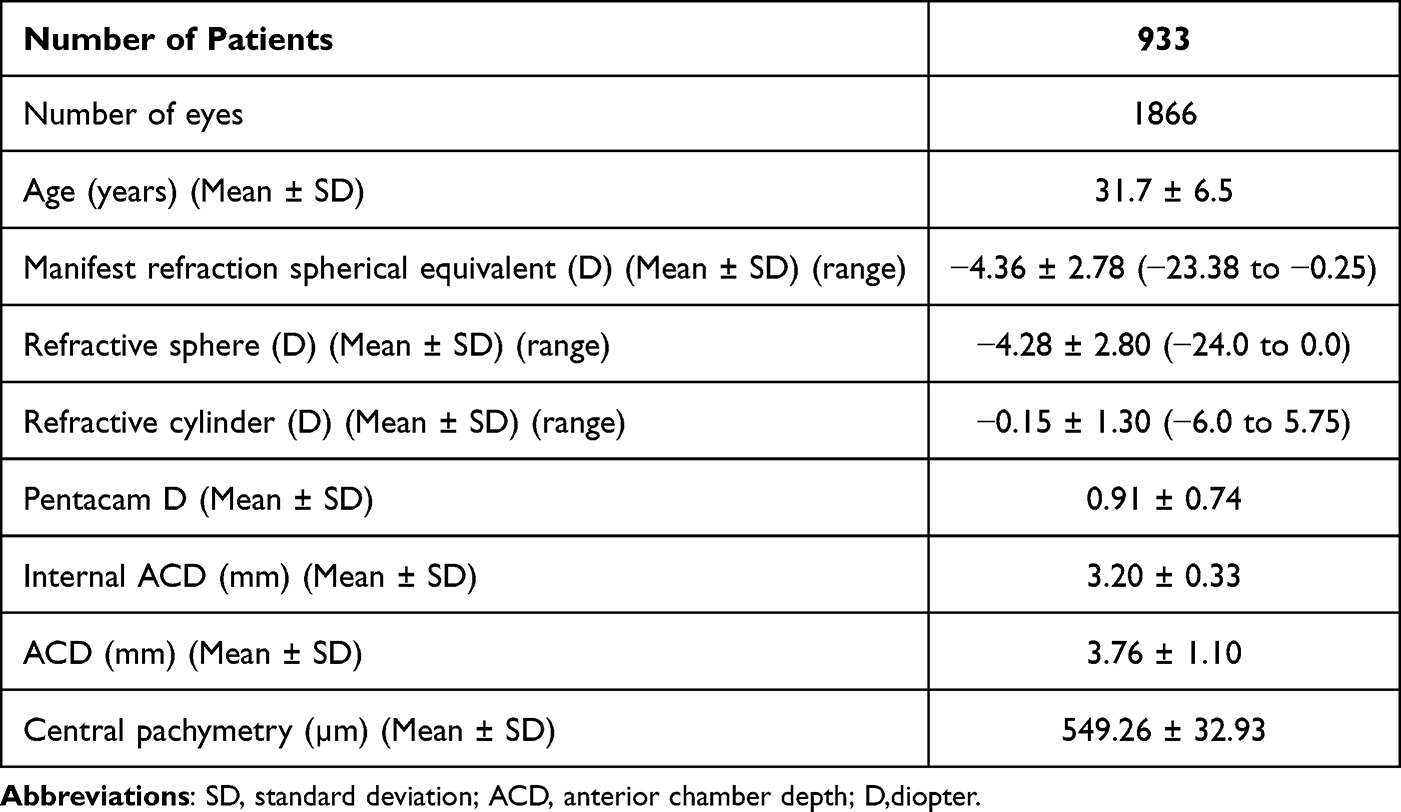 |
Table 1 Demographics and Baseline Characteristics |
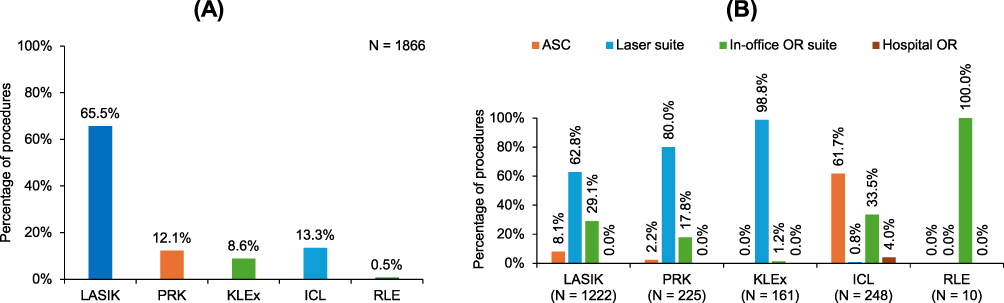 |
Figure 1 (A) Proportion of each type of refractive surgery procedure, (B) site of service for laser vision correction and lens-based refractive surgery procedures. Abbreviations: LASIK, Laser-Assisted in Situ Keratomileusis; PRK, Photorefractive Keratectomy; ICL, Implantable Collamer Lens; RLE, Refractive Lens Exchange; KLEx- femtosecond laser, keratorefractive lenticule extraction procedures. |
The mean age of patients undergoing LASIK was 31.3 years compared to 30.3 for PRK, 31.7 for KLEx, 32.0 for ICL, and 39.6 for RLE. All procedures were performed across the full age range of patients evaluated in the study (age 18–45) except for RLE, which was not performed in any patient younger than 33 years of age.
Overall, 59.4% of all the procedures were performed in a laser suite, 26.3% in an in-office operating room (OR), 13.8% in an ambulatory surgery center (ASC), and 0.5% in a hospital OR. Laser procedures were primarily performed in a laser suite or in-office OR, while lens-based procedures were primarily performed in an ASC or in-office OR suite (Figure 1B).
The mean manifest refractive spherical equivalent (MRSE), spherical error, and astigmatism by procedure are shown in Figure 2. The distribution of the cylinder is shown in Figure 3. Overall, 29.7% of eyes had refractive cylinder ≤0.25 D, 38.6% had cylinder between 0.26 D and 1.00 D, 21.5% of eyes had refractive cylinder between 1.01 and 2.00 D, and 10.2% of eyes showed refractive cylinder >2.00 D. Among all laser vision correction (LVC, combination of LASIK, PRK, and KLEx) procedures, 43.6% were in low myopes (MRSE of −0.25 to −3.00 D), 43.1% were in moderate myopes (−3.01 to −6.00 D) and 13.3% were performed in high myopes (>6.00 D). Among all ICL procedures, 3.6%, 21.0%, and 75.4% were performed in low, moderate, and high myopes, respectively (Figure 4). The average degree of myopia treated was −8.72 D in ICL patients compared to −3.63 D in LVC patients.
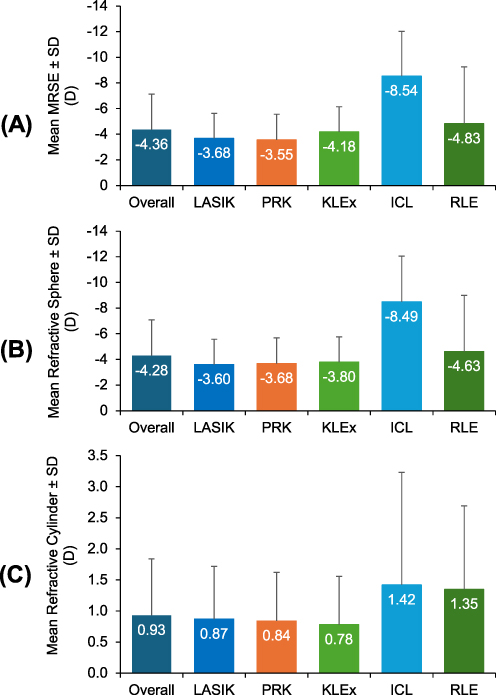 |
Figure 2 Mean (A) manifest refractive spherical equivalent, (B) refractive sphere, and (C) refractive cylinder by procedure. Abbreviations: LASIK, Laser-Assisted in Situ Keratomileusis; PRK, Photorefractive Keratectomy; ICL, Implantable Collamer Lens; RLE, Refractive Lens Exchange; KLEx- femtosecond laser, keratorefractive lenticule extraction procedures. |
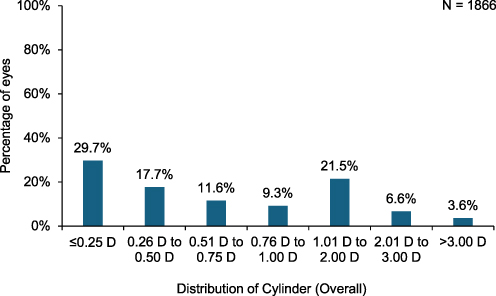 |
Figure 3 Distribution of refractive cylinder. |
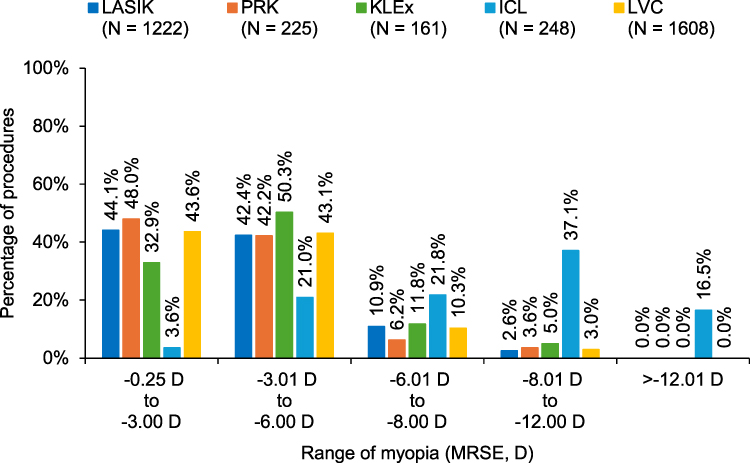 |
Figure 4 Distribution of procedure type by degree of myopia. Abbreviations: LASIK, Laser-Assisted in Situ Keratomileusis; PRK, Photorefractive Keratectomy; ICL, Implantable Collamer Lens; RLE, Refractive Lens Exchange; KLEx- femtosecond laser, keratorefractive lenticule extraction procedures. |
There was a statistically significant but very weak correlation between sphere and cylinder (R = 0.13, p <0.001). The odds of performing ICL over LVC were analyzed in the right and left eyes separately using multiple logistic regression. Sphere and cylinder were found to be independently contributing to the odds of undergoing ICL vs LVC. As the magnitude of the myopic sphere or cylinder increased, the odds of undergoing ICL increased significantly (p <0.001). ICL patients had an average of 1.42 D of refractive cylinder, while the LVC patients had an average of 0.86 D. Additionally, 50.8% of patients receiving an ICL had >1.00 D of astigmatism, more than for any other procedure and nearly double the percentage of LVC patients (28.7%) with >1.00 D of astigmatism.
Of the 1,866 eyes included in the study, Pentacam D values were available for 1,351 eyes, and analyses were performed on the observed data (n=1351). Mean Pentacam D in eyes treated with LASIK or KLEx was 0.86, compared to 1.06 in PRK eyes (p <0.001) and 1.01 in ICL eyes (p = 0.253). Mean ACD was 3.76 ± 1.10 mm and mean AQD was 3.20 ± 0.33 mm across all procedures, with minimal variation by procedure choice. Mean central pachymetry was 549.26 ± 32.93 µm across all procedures; the distribution of central pachymetry is shown in Figure 5. Overall, 5.6% of eyes had central pachymetry ≤500 µm, and 94.4% of eyes had a central pachymetry >500 µm. Mean central pachymetry in eyes treated with LASIK or KLEx was 551.5 ± 31.2 µm, compared to 540.7 ± 36.5 µm in PRK eyes (p <0.001) and 544.9 ±37.3 µm in ICL eyes (p = 0.056). Among eyes that underwent LASIK or KLEx, 2.8% had thinner corneas (central pachymetry <500 µm). This was significantly lower than the 12.4% of eyes undergoing PRK (p <0.001) that had thinner corneas and 11.7% of those undergoing ICL surgery (p <0.001).
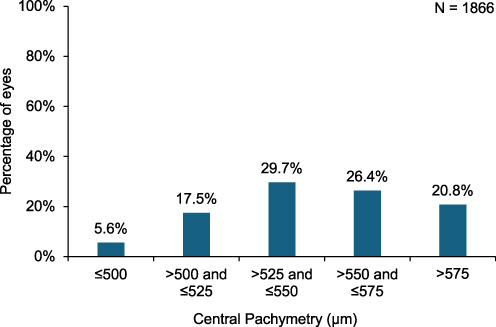 |
Figure 5 Distribution of central pachymetry. |
The overall proportion of procedures performed was stratified by ICL usage: higher (>20% of all procedures during the study period were ICL) and lower (≤20% of all procedures were ICL). Among higher ICL usage sites, laser-based procedures accounted for 70.9% of the procedures, whereas for lower ICL usage sites, 91.7% were laser-based procedures (Table 2). Higher ICL usage sites performed 29.4% of ICL procedures on patients with low to moderate myopia (≤6.00 D), compared with 18.7% by lower ICL usage sites (Figure 6). For sites performing KLEx procedures, excimer laser-based procedures such as LASIK and PRK accounted for 46.1% of procedures. For sites not performing KLEx procedures, 88.5% of all procedures were excimer laser-based procedures (Figure 7).
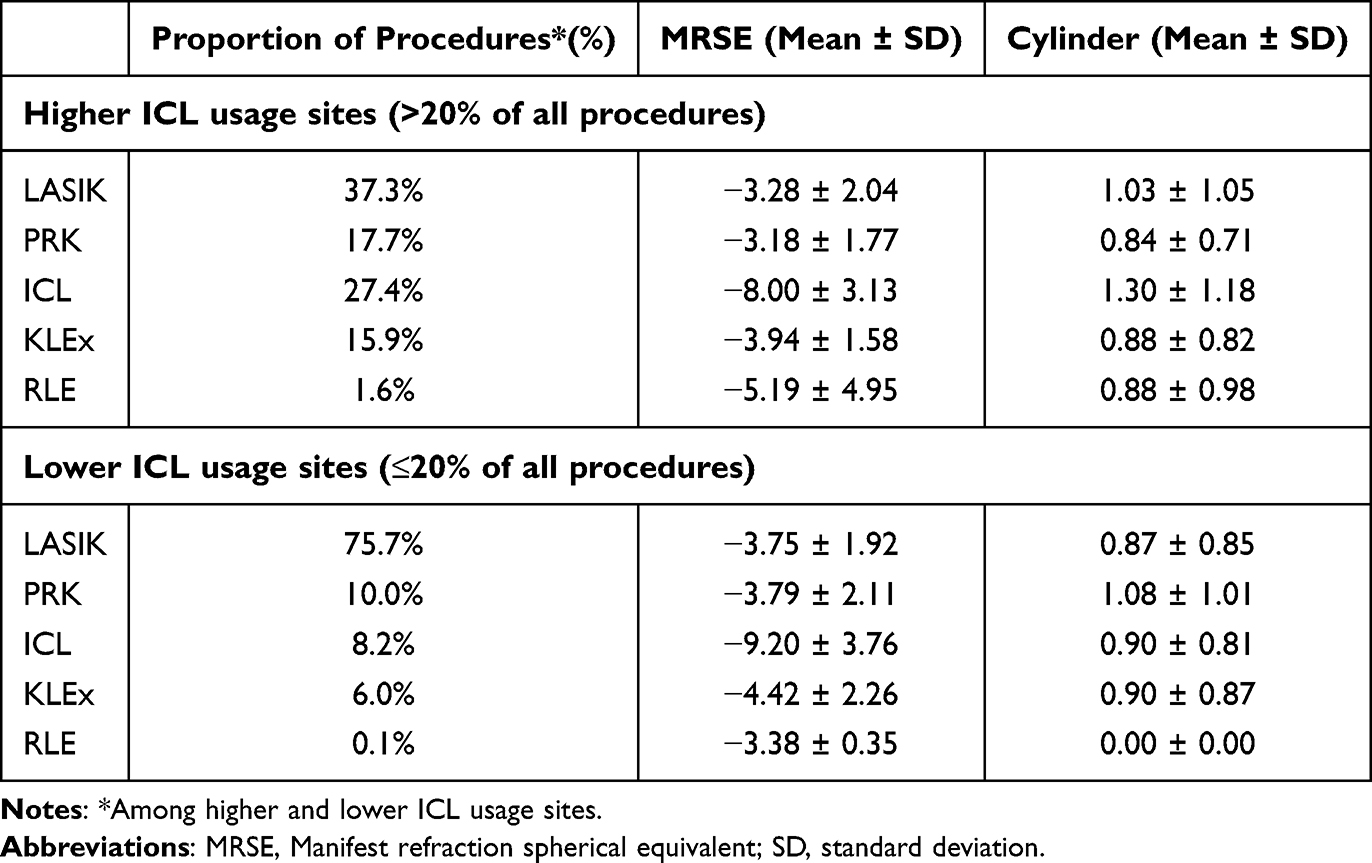 |
Table 2 The Overall Proportion of Procedures, Mean MRSE, and Cylinder for Each Procedure, Stratified by ICL Volume During the Study Period |
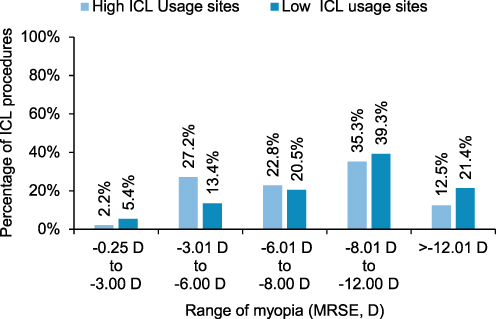 |
Figure 6 Proportion of ICL procedures for different ranges of myopia stratified by the sites having higher or lower ICL volume during the study period. |
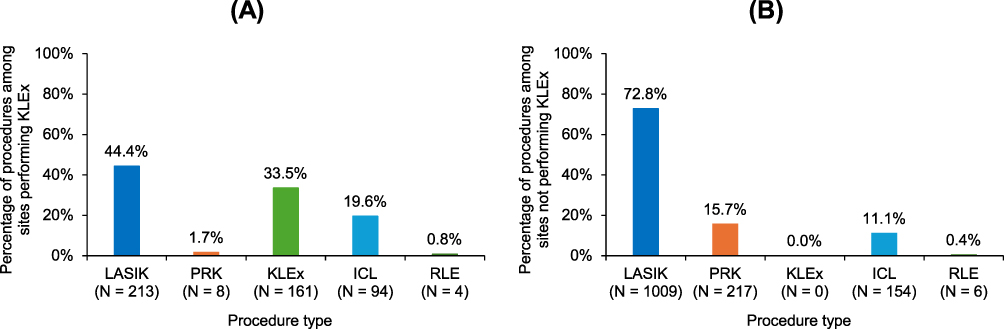 |
Figure 7 Proportion of refractive procedures stratified by the (A) practices reporting KLEx procedures and (B) practices reporting no KLEx procedures during the study period. Abbreviations: LASIK, Laser-Assisted in Situ Keratomileusis; PRK, Photorefractive Keratectomy; ICL, Implantable Collamer Lens; RLE, Refractive Lens Exchange; KLEx- femtosecond laser, keratorefractive lenticule extraction procedures. |
The 5 surgeons who performed KLEx procedures in the study performed fewer LASIK/PRK procedures (46.0% vs 88.5%, p <0.001) and more ICL procedures (19.6% vs 11.1%, p <0.001) than surgeons at the other 14 centers. One site had access to a KLEx laser but did not perform any KLEx procedures.
Discussion
LASIK has been the dominant refractive surgery procedure in the US since 1999.13 Among this sample of US refractive surgeons who are members of AECOS, LASIK was found to still be the most commonly selected procedure, accounting for 65.5% of all procedures performed. The widespread popularity of LASIK stems from its consistent delivery of excellent outcomes, with minimal postoperative pain and inflammation, and rapid visual rehabilitation.14–16 However, not all patients are good candidates for LASIK. As refractive technology has evolved, many refractive surgeons perform multiple types of laser- and lens-based surgery, with the goal of finding the best-fit procedure for each patient. Centers that performed any KLEx procedures during the present study performed fewer PRK and LASIK procedures and more ICL procedures than centers that did not perform any KLEx. Access to specific laser technologies may affect procedure choice.
Lens-based procedures are increasingly important, with the present study finding that almost 14% of procedures performed were ICL or RLE. This mirrors trends in Europe. According to the 2023 European Society of Cataract and Refractive Surgery (ESCRS) Clinical Trends Survey,17 the majority of European refractive surgeons (66%) foresee their usage of phakic IOLs increasing in the coming years due to the perceived advantages of corneal tissue preservation and reversibility. However, cost and lack of access remain barriers, according to respondents to that survey.
The present study shows that 59.4% of all refractive procedures are performed in a laser suite, compared to 26.3% in an in-office OR suite, 13.8% in an ASC, and 0.5% in a hospital OR. All KLEx procedures (100%) and almost all PRK procedures (97.8%) were performed in the office, in either a laser or an OR suite. Compared to the other two forms of laser refractive surgery, LASIK is slightly more likely to be performed in an ASC, although most LASIK procedures (91.9%) were still performed in the office.
ICL procedures were more likely to be performed in an in-office OR suite (33.5%) or in an ASC (61.7%). Having access to an ASC or in-office OR suite may be an important factor when surgeons are considering offering ICL, as these settings may be more conducive to the bilateral, same-day surgery typically favored for ICL surgery. Conversely, it may be a barrier to adoption for those who do not have access. Additionally, the approved treatment range for the various refractive technologies may also affect procedure choice.
In this sample of procedures performed in 2023, nearly 22% of the eyes treated were highly myopic (>6.00 D of myopia), which is significantly higher than the approximately 4% incidence of high myopia among US adults,18 supporting the long-held belief that high myopes are more likely to seek out refractive surgery.
While some of these highly myopic eyes may have fallen within the approved indications for LASIK or PRK, the literature suggests that clinicians often have a lower threshold for the range at which they are comfortable performing LVC.19
In a recent meta-analysis, Fu et al reported that higher myopes (≥6.00 D of myopia) treated with KLEx or femtosecond LASIK had similarly safe and efficacious outcomes, although there appeared to be come advantages for KLEx in terms of aberrations and corrected distance acuity.20 Multiple authors have suggested that it is reasonable to choose phakic IOL surgery for patients with ≥6.00 D of myopia.21,22 In the present study, the distribution of procedure type by MRSE shows that ICL has a much higher mean degree of myopia than other procedures. In all, 75.4% of ICL procedures were performed in high myopes. However, 13.5%, 9.8%, and 16.8% of LASIK, PRK, and KLEx procedures were performed in high myopes.
Patients with either high sphere or high cylinder were more likely to undergo ICL implantation than any LVC procedure. However, it is also notable that 24.6% of ICL cases were in eyes with ≤6.00 D of myopia, and 8.4% of ICL cases were in eyes with ≤4.00 D of myopia, suggesting that surgeons’ comfort with phakic IOL surgery in mild to moderate myopia may be increasing.23 Good efficacy in such populations has been reported.23 Centers with higher ICL usage performed more of their ICL procedures on patients with low to moderate (≤6.00 D of myopia) (29.4%) compared to those with lower levels of ICL utilization (18.7%).
More than 70% of the patients who underwent refractive surgery in this large retrospective study conducted in practices across the US had significant astigmatism (>0.25 D) (Figure 6). This should counter the persistent myth that patients with astigmatism cannot have LVC.
RLE was rarely performed in this study population of patients aged 45 years or younger. With only 10 of 1,866 eyes receiving RLE, the number of cases of RLE in the age group studied was too low to make valid comparisons to other groups. Although presbyopic add power and lens status were not evaluated in the study, one can presume that RLE is more commonly performed in patients with older age and more advanced presbyopia. In addition, the risk of retinal detachment after lens removal, while still low, is higher in young myopic patients who have not yet developed a posterior vitreous detachment (PVD). Thus, clear lens extraction is not as likely to be recommended in young patients until a PVD has developed, thus decreasing the patient’s risk profile.
Final D is a measure of ectasia risk automatically calculated by the Pentacam device’s BAD. Patients with higher D values are at higher risk of ectasia when undergoing LASIK and KLEx,11,24 while this is less of a concern when undergoing PRK or ICL. However, only the PRK cohort in the present study had a D value that was significantly higher than the D value of the LASIK and KLEx cohorts. The average D value in the ICL group fell between the PRK and LASIK/KLEx groups, but the differences were not statistically significant.
Patients undergoing PRK tended to have thinner corneas, on average, than patients undergoing LASIK or KLEx. Patients with very thin corneas (with central corneal pachymetry <500 µm) were significantly more likely to undergo tissue-sparing PRK or ICL procedures, rather than LASIK or KLEx.
Implantation of an ICL requires a “true” ACD (measured from the corneal endothelium to the anterior crystalline lens capsule) of ≥3.00 mm.23 Although most subjects in the present study (76.9%) had an ACD that would not have disqualified them from ICL surgery, an ACD shallower than 3.0 mm, disqualifying the patient from receiving an ICL, may have been a factor in procedure choice for some patients.
Practices that performed KLEx during the study period performed almost no PRK and performed fewer LASIK procedures than practices that did not report any KLEx procedures. Most of the practices that did not perform any KLEx procedures did not have the laser technology needed for this procedure.
Results were stratified by the volume of ICL implantation per practice. Practices were divided into two groups: the “top quartile”, which included 5 surgeons whose ICL procedures made up 20% or more of their total refractive surgeries, and the “bottom three quartiles”, which included the remaining 14 surgeons for whom ICLs constituted less than 20% of their refractive procedures. This stratification allowed for comparison of refractive trends between high-ICL volume practices and those with lower ICL usage. Mean MRSE for ICL procedures was −8.00 ± 3.13 D (N = 136) in the higher ICL usage group, compared to a mean MRSE of −9.20 ±3.76 D (N = 112) in the lower ICL usage group, suggesting that surgeons who are more comfortable performing ICL offer it to a wider range of patients.
This is a real-world retrospective study to determine the overall trends in refractive surgery choices across the 18 participating US sites and, therefore, had some limitations. While the participating sites had access to lens-based vision correction options (phakic IOL/RLE) and to one or more laser vision correction technologies (LASIK/PRK/KLEx), not all practices had access to all the different procedures available in the US market. Differences in surgeon practice models, where the availability of refractive procedures and measurement devices across sites is likely to vary, may introduce selection bias and influence the findings observed in this study. Analyses were planned post hoc to identify statistically significant trends and associations/correlations. Since a priori sample size calculations were not warranted in this trend analysis, all analyses were exploratory and were not adjusted for multiplicity; statistical inferences should be interpreted cautiously. Since bioptics/enhancement procedures were excluded, the study reflects trends observed in primary cases. While the present study was designed to identify current trends in refractive procedure choice across AECOS member sites, future studies across a wider range of sites and geographical locations may provide more generalizable insights. Future studies may incorporate participating surgeons’ procedure selection criteria, outcomes, and patient-reported outcomes to provide more comprehensive insights.
To the best of our knowledge, the present study is the first of its kind in many years to evaluate trends in refractive surgery across multiple US refractive practices. We found wide variation in procedure choice by practice, irrespective of patient characteristics. Even among this relatively high volume, experienced sample of refractive practices, surgeon experience, practice orientation, and technology access can produce quite different profiles of procedure choice and surgery site.
As participating practices were all in the US, the distribution of refractive procedures, demographics, and procedure site preferences may differ in other countries. A limitation of the study is that only 6 of 19 participating surgeons had access to the laser used to perform KLEx procedures, which may have skewed their choices. Additionally, practices were asked to report their last 100 eyes treated in 2023. It is possible that if a longer period (more eyes) had been assessed, or data had been gathered in 2024, the trends might be slightly different.
Conclusion
This retrospective evaluation of age, gender, refractive error, and ophthalmic anatomical features of a large cohort of treated patients can help better understand and define the refractive surgery patient and the refractive surgery choices of patients and surgeons at participating AECOS member practices in the US. More than 85% of the procedures were performed in a laser suite or an in-office OR suite. LASIK procedures made up almost two-thirds of the refractive surgery procedures. Patients with high sphere or cylinder were more likely to undergo ICL implantation than LVC procedure; however, a quarter of ICL cases were in eyes with myopia of ≤6.00 D, suggesting that surgeons are becoming comfortable with performing phakic IOL surgery in eyes with mild to moderate myopia. In addition, patients are being educated to consider a variety of laser options and intraocular lens based alternatives to traditional laser vision correction, when appropriate. Overall, refractive trends are evolving as surgeons have more options to customize a patient’s treatment according to age and degree of myopia and astigmatism.
Abbreviations
AECOS, American European Congress of Ophthalmic Surgery; ESCRS, European Society of Cataract and Refractive Surgery; MRSE, Manifest refraction spherical equivalent; LASIK, laser in situ keratomileusis; PRK, photorefractive keratectomy; KLEx, femtosecond laser keratorefractive lenticule extraction; WMILE, small-incision lenticular extraction; ICL, Implantable Collamer Lens; IOL, intraocular lens; RLE, refractive lens exchange; PTD, phototherapeutic keratectomy; ACD, anterior chamber depth; OR, operating room; ASC, ambulatory surgery center; LVC, laser vision correction; PVD, posterior vitreous detachment; BAD, Belin-Ambrosio Display.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author (GW), upon reasonable request.
Acknowledgments
Raman Bedi, MD (IrisARC - Analytics, Research & Consulting, Chandigarh, India) and Jan Beiting (Wordsmith Consulting, Cary, North Carolina) provided statistical analysis and editorial assistance for this manuscript.
Funding
This study was funded by the American-European Congress of Ophthalmic Surgeons (AECOS), which received an independent research grant from STAAR Surgical, Monvrovia, CA, USA.
Disclosure
GW is a consultant for Alcon, Bausch + Lomb, BVI, Carl Zeiss Meditec, Dompé, Johnson & Johnson Vision, Lensar, Ocular Science, Tarsus, RxSight, Science Based Health, and Rayner and received research support from Staar via an unrestricted education grant through AECOS to fund this study. WFW is a consultant for Staar, Zeiss, Alcon, Bausch and Lomb, RxSight, and Johnson & Johnson Vision, and has received research support from Staar via a grant to AECOS to help fund this study. He reports no other financial interests related to the subject of this article. KED serves as a consultant for Alcon, Johnson & Johnson Vision, Bausch + Lomb, BVI, Carl Zeiss Meditec, Lensar, and Rayner and received research support from Staar via an unrestricted educational grant through AECOS to fund this study. The authors report no other conflicts of interest related to the subject of this article.
References
1. Hwang HS. Visual outcomes after three different surgical procedures for correction of refractive error in patients with thin corneas. Int J Ophthalmol. 2020;13(6):970–11. doi:10.18240/ijo.2020.06.18
2. Moshirfar M, Somani SN, Patel BC. Small incision lenticule extraction. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025.
3. Bamashmus MA, Saleh MF, Awadalla MA. Reasons for not performing keratorefractive surgery in patients seeking refractive surgery in a hospital-based cohort in “Yemen”. Middle East Afr J Ophthalmol. 2010;17(4):349–353. doi:10.4103/0974-9233.71605
4. Farooqui JH, Acharya M, Kekan M. Current trends in surgical management of myopia. Community Eye Health. 2019;32(105):S5–S6.
5. Packer M. Evaluation of the EVO/EVO+ sphere and toric Visian ICL: six month results from the United States food and drug administration clinical trial. Clin Ophthalmol. 2022;16:1541–1553. doi:10.2147/OPTH.S369467
6. Duffey RJ, Leaming D. U.S. trends in refractive surgery: 2001 international society of refractive surgery survey. J Refract Surg. 2002;18(2):185–188. doi:10.3928/1081-597X-20020301-14
7. Duffey RJ, Leaming D. US trends in refractive surgery: 2002 ISRS survey. J Refract Surg. 2003;19(3):357–363. doi:10.3928/1081-597X-20030501-14
8. Duffey RJ, Leaming D. US trends in refractive surgery: 2003 ISRS/AAO survey. J Refract Surg. 2005;21(1):87–91. doi:10.3928/1081-597X-20050101-16
9. Duffey RJ, Leaming D. US trends in refractive surgery: 2004 ISRS/AAO survey. J Refract Surg. 2005;21(6):742–748. doi:10.3928/1081-597X-20051101-14
10. Duffey RJ, Leaming D. Trends in refractive surgery in the United States. J Cataract Refract Surg. 2004;30(8):1781–1785. doi:10.1016/j.jcrs.2004.05.038
11. Toprak İ, Martin Ç, Gunes CE, Alio J. Revisiting Pentacam parameters in the diagnosis of subclinical and mild keratoconus based on different grading system definitions. Turk J Ophthalmol. 2023;53(6):324–335. doi:10.4274/tjo.galenos.2023.68188
12. Yakar K, Alacamli G, Ozgur G. Early posterior corneal changes and Belin/Ambrósio scores following photorefractive keratectomy: a pentacam study. OphthalmolTherapy. 2025;14(9):2141–2154. doi:10.1007/s40123-025-01199-8
13. Maller BS. Market trends in refractive surgery. Int Ophthalmol Clin. 2000;40(3):11–19. doi:10.1097/00004397-200007000-00004
14. Moshirfar M, Bennett P, Ronquillo Y. Laser in situ keratomileusis (LASIK). In: StatPearls [Internet]. StatPearls Publishing; 2023.
15. Wilkinson JM, Cozine EW, Kahn AR. Refractive eye surgery: helping patients make informed decisions about LASIK. Am Fam Physician. 2017;95(10):637–644.
16. Alio JL, Ortiz D, Muftuoglu O, Garcia MJ. Ten years after photorefractive keratectomy (PRK) and laser in situ keratomileusis (LASIK) for moderate to high myopia (control-matched study). Br J Ophthalmol. 2009;93(10):1313–1318. doi:10.1136/bjo.2007.131748
17. ESCRS Clinical Trends Survey 2023 Results. EuroTimes supplement. 2024. Available at: https://www.escrs.org/media/jg0hzpys/escrs_clinicaltrendssurvey2023_sept24.pdf.
18. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–1042. doi:10.1016/j.ophtha.2016.01.006
19. Alsulami R, Alzahrani S, AlQahtani B, Khayyat H, Alghamdi S. Reasons for not performing surface ablation refractive surgery in Saudi population. Saudi J Ophthalmol. 2020;34(1):35–39. doi:10.4103/1319-4534.301294
20. Fu Y, Yin Y, Wu X, et al. Clinical outcomes after small-incision lenticule extraction versus femtosecond laser-assisted LASIK for high myopia: a meta-analysis. PLoS One. 2021;16(2):e0242059. doi:10.1371/journal.pone.0242059
21. Albarrán-Diego C, Muñoz G, Ferrer-Blasco T, García-Lázaro S, Belda-Salmerón L. Foldable iris-fixated phakic intraocular lens vs femtosecond laser–assisted LASIK for myopia between −6.00 and −9.00 diopters. J Refract Surg. 2012;28(6):380–387. doi:10.3928/1081597X-20120508-01
22. Joosse MV, Snoek C, van Minderhout HM. Comparison of wavefront-guided photorefractive keratectomy and foldable iris-fixated phakic intraocular lens implantation for low to moderate myopia. J Cataract Refract Surg. 2011;37(2):370–377. doi:10.1016/j.jcrs.2010.08.051
23. Packer M. The EVO ICL for moderate myopia: results from the US FDA clinical trial. Clin Ophthalmol. 2022;16:3981–3991. doi:10.2147/OPTH.S393422
24. Bamdad S, Sedaghat MR, Yasemi M, Vahedi A, Dobrowolski D. Sensitivity and specificity of belin ambrosio enhanced ectasia display in early diagnosis of keratoconus. J Ophthalmol. 2020;2020:7625659. doi:10.1155/2020/7625659
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.