Back to Journals » Clinical Ophthalmology » Volume 19
Influence of Posterior Capsulotomy Size on Visual Quality and Patient Satisfaction with Extended Depth-of-Focus IOLs
Authors Yen CY, Lin FG, Yang SS, Chang YJ, Fang IM ![]()
Received 6 September 2025
Accepted for publication 6 December 2025
Published 11 December 2025 Volume 2025:19 Pages 4573—4583
DOI https://doi.org/10.2147/OPTH.S561594
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Bharat Gurnani
Chu-Yu Yen,1 Fu-Gong Lin,2,3 Sun-Sen Yang,4 Yen-Jui Chang,5– 7 I-Mo Fang4,8– 10
1Department of Ophthalmology, Taipei City Hospital, Ren-Ai Branch, Taipei, Taiwan; 2Department of Optometry, Asia University, Taichung, Taiwan; 3School of Public Health, National Defense Medical Center, Taipei, Taiwan; 4Department of Ophthalmology, Taipei City Hospital, Zhongxiao Branch, Taipei, Taiwan; 5Department of Ophthalmology, Taipei City Hospital, Yangming Branch, Taipei, Taiwan; 6Department of Optometry, University of Kang Ning, Taipei, Taiwan; 7Department of Health and Welfare, College of City Management, University of Taipei, Taipei, Taiwan; 8Department of Ophthalmology, National Taiwan University Hospital, Taipei, Taiwan; 9Department of Special Education, University of Taipei, Taipei, Taiwan; 10Department of Optometry, Mackay Medical College, New Taipei City, Taiwan
Correspondence: I-Mo Fang, Department of Ophthalmology, Taipei City Hospital, Zhongxiao Branch, Taipei, Taiwan, Tel +886-2-27861288 Ext: 8271, Email [email protected]
Purpose: Prior studies in monofocal intraocular lenses (IOLs) suggest that larger Nd:YAG posterior capsulotomies may reduce straylight and photic phenomena, but generalizability to extended depth-of-focus (EDOF) optics is uncertain. We evaluated whether capsulotomy size affects optical quality, higher-order aberrations (HOAs), and patient-reported outcomes in eyes with EDOF IOLs.
Patients and Methods: In this prospective single-center study, 106 pseudophakic eyes with visually significant posterior capsule opacification and EDOF IOLs underwent Nd:YAG laser posterior capsulotomy. Capsulotomy size was measured at the slit lamp using a calibrated reticule in the horizontal and vertical meridians; the effective diameter was defined as the mean of these two measurements. Eyes were prospectively assigned to a small opening (S group, n=47), created to slightly exceed the IOL’s central diffractive zone (≈1.6– 1.8 mm), or a large opening (L group, n=59), extended to the margin of the outermost diffractive ring (≈4 mm). At 1-month post-treatment, visual acuity, HOAs, defocus curves, and optical quality metrics were assessed. Subjective outcomes were evaluated using the APPLES and Catquest-9SF-CN questionnaires.
Results: Both groups showed improved visual acuity, with greater corrected distance visual acuity (CDVA) gain in the L group (– 0.15 vs – 0.06 logMAR; P = 0.024). Trefoil aberration increased more in the S group than in the L group (+0.15 vs +0.02; P = 0.021), while spherical aberration decreased more in the S group than in the L group (– 0.20 vs – 0.09; P = 0.024). The APPLES questionnaire showed a greater reduction in starburst severity and frequency in the L group (Δ – 0.43 vs +0.07; P = 0.010). Multivariate analysis identified pre-treatment spherical equivalent, trefoil, mesopic pupil size, and CDVA as significant predictors of satisfaction.
Conclusion: Capsulotomy size significantly influences optical quality and patient satisfaction in eyes with EDOF IOLs. Larger openings improve CDVA and photic symptoms, while smaller ones better reduce spherical aberration but increase trefoil. Personalizing capsulotomy size may optimize outcomes.
Keywords: posterior capsule opacification, visual acuity, defocus curve, photic phenomena, trefoil aberration, patient satisfaction
Introduction
Cataract surgery with phacoemulsification and intraocular lens (IOL) implantation reliably restores vision, but posterior capsule opacification (PCO) remains the most common long-term complication, affecting 20–40% of patients.1–3 Visually significant PCO is typically treated with Nd:YAG laser capsulotomy, which rapidly improves acuity.4 Beyond visual axis clearance, growing evidence suggests that capsulotomy size may influence optical quality. Smaller capsulotomies (≤3.5 mm) are linked to better capsular stability and IOL centration, while larger openings may reduce intraocular stray light and photic disturbances such as glare and starbursts.5–7
However, these findings are based mostly on monofocal IOLs, and their relevance to extended depth-of-focus (EDOF) IOLs is uncertain. The EDOF IOL extends the range of vision by modulating spherical and chromatic aberrations, but its performance is sensitive to pupil size, centration, and higher-order aberrations (HOAs), with visual symptoms like halos and starbursts being more frequent.8–10
This study evaluates whether capsulotomy size affects optical quality, specific HOAs (spherical and trefoil), and visual symptoms in eyes with EDOF IOLs, using both objective measurements and validated patient-reported outcomes.
Materials and Methods
Study Design and Ethics
This single-center, prospective clinical study was approved by the Research Ethics Committee of Taipei City Hospital, Taiwan (TCHIRB-11103004) and adhered to the Declaration of Helsinki. Written informed consent was obtained from all participants prior to enrolment. The consent process included a face-to-face explanation of study objectives, procedures (including questionnaires), potential risks/benefits of Nd:YAG capsulotomy, data privacy/anonymisation, and the voluntary right to withdraw at any time without impact on clinical care. For participants with both eyes eligible, separate consent was obtained per eye.
Participants: Inclusion and Exclusion Criteria
We consecutively enrolled 201 pseudophakic eyes implanted with multifocal/EDOF IOLs with visually significant PCO scheduled for Nd:YAG laser posterior capsulotomy at Taipei City Hospital, Zhongxiao Branch (January 2023–December 2024) (Figure 1). To ensure optical homogeneity, the analysis was restricted a priori to a single EDOF platform (Tecnis Symfony®; Johnson & Johnson Vision, USA); consequently, 87 non-Symfony eyes were excluded before allocation/analysis. Remaining Symfony eyes were assessed against the inclusion/exclusion criteria below. PCOs were graded using retroillumination images based on Congdon’s classification, which ranges from grade 0 (no opacity or only peripheral involvement) to grade 4 (opacity that precludes fundus examination). Grades 1 to 3 indicate increasing central involvement: grade 1 is characterized by mild central changes with a clear view of the posterior pole; grade 2 slightly affects macular detail without obscuring the optic cup/disc; and grade 3 impairs cup/disc evaluation.11
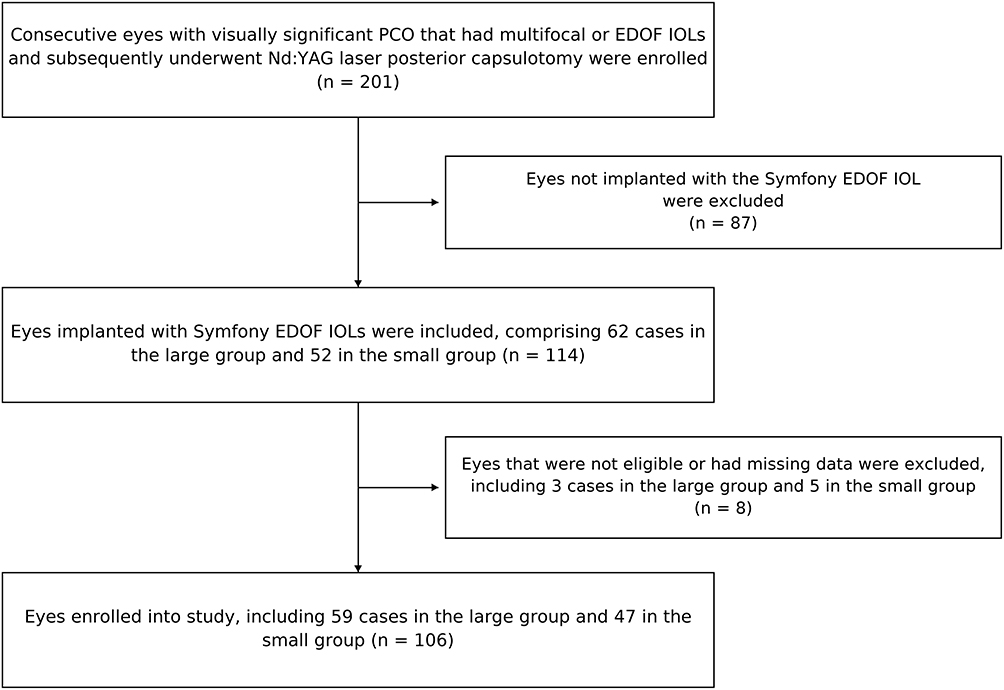 |
Figure 1 Flowchart of patient recruitment and group allocation. |
Inclusion criteria: (1) prior uneventful phacoemulsification with implantation of a Tecnis Symfony® EDOF IOL; (2) PCO graded on retroillumination images using Congdon’s classification, with grade ≥3 considered visually significant; (3) reliable fixation permitting optical quality and wavefront measurements.
Exclusion criteria: ocular comorbidities that could confound optical/visual assessments (eg, high myopia with axial length >26.0 mm, corneal opacity, clinically significant retinopathy or maculopathy, glaucoma), any ocular surgery within the prior 6 months, active ocular inflammation, or systemic disease affecting visual function.
Surgical Procedure and Allocation
All Nd:YAG capsulotomies were performed by a single surgeon (I-M.F.) under topical anaesthesia using a cruciate (cross-shaped) technique (Visulas YAG II, Zeiss, Germany) with a capsulotomy contact lens (Double Aspheric Capsulotomy Lens, Volk, USA). To implement the two target-size strategies and preserve operational feasibility, eyes were prospectively allocated according to a prespecified alternating schedule (L→S→L→S…) defined prior to study commencement to undergo either small (S) or large (L) capsulotomy:
- Small opening (S group): created to slightly exceed the IOL’s central diffractive zone (≈1.6–1.8 mm).
- Large opening (L group): extended to the margin of the outermost diffractive ring (≈4 mm).
To control size intraoperatively, the surgeon used the Symfony diffractive ring pattern as intrinsic landmarks under coaxial illumination. The cruciate cuts were enlarged by short arcuate extensions until the posterior capsule edge coincided with the intended ring boundary.
To prevent immediate postoperative IOP rise, one drop of dorzolamide–timolol was instilled pre- and post-procedure; 1% dexamethasone sodium phosphate was prescribed QID for 1 week.
Capsulotomy Size Measurement Protocol
Capsulotomy size was measured at the slit lamp using a calibrated eyepiece reticule in both horizontal and vertical meridians at 1 week and reconfirmed at 1-month post-treatment. The effective diameter was defined as the mean of the two meridional readings. Measurements were performed twice per eye by a trained examiner (I-M.F.) masked to all outcome data; if the two readings differed by >0.2 mm, a third measurement was taken and the median recorded.
Outcome Measures
Vision Assessment
At 1-month post-treatment, uncorrected distance visual acuity (UDVA) and corrected distance visual acuity (CDVA) were measured at 5 m using a Landolt-C decimal chart (converted to logMAR for analysis). Uncorrected near visual acuity (UNVA) and corrected near visual acuity (CNVA) were measured at 40 cm using a decimal near chart under standard room illumination; results were likewise converted to logMAR.
Objective Visual Quality and Wavefront Aberrations
At one-month post-treatment, wavefront and optical quality metrics were obtained with the OPD-Scan III (Nidek, Japan). This device provided quantitative data on total ocular higher-order aberrations (tHOA), internal higher-order aberrations (iHOA), as well as individual components including coma, spherical, and trefoil aberrations. Examinations were performed in a dim room after brief adaptation; participants were instructed to blink before each capture to optimize tear film. Three consecutive measurements were recorded, and the average was analyzed if device quality flags were acceptable Zernike coefficients were exported up to the 6th order; HOAs were defined as the root-mean-square (RMS) of 3rd–6th orders. Component analyses focused on spherical aberration (Z4^0) and trefoil (Z3^±3). Device-derived Strehl ratio (SR) and modulation transfer function (MTF) area were recorded. Photopic and mesopic pupil diameters were obtained from the same device output.
Defocus Curve
A defocus curve was obtained at one-month post-treatment using a comprehensive refractometer. The spherical power was adjusted incrementally from +3.0 to –4.0 diopters (D) in 0.5 D steps, and visual acuity was recorded at each level. The average visual acuity across all patients was plotted, with defocus (D) on the X-axis and visual acuity (logMAR) on the Y-axis, to evaluate postoperative visual performance across different focal ranges.
Subjective Visual Quality
To evaluate visual function-related quality of life at one-month post-treatment, the Catquest-9SF-CN and the Assessment of Photic Phenomena and Lens Effects (APPLES) questionnaires were administered. These instruments provide a multidimensional assessment of visual function that extends beyond visual acuity alone.12,13 The Catquest-9SF-CN is the validated Chinese version of the Catquest-9SF questionnaire, designed to assess patients’ self-reported visual function and satisfaction following cataract surgery and IOL implantation. It consists of nine core single-choice items, each rated on a 4- or 5-point Likert scale. The response options are coded as follows: “Very great difficulty” = 4, “Some difficulty” = 3, “A little difficulty” = 2, and “No difficulty” = 1. Responses marked as “Not applicable” are typically excluded from scoring. The total score is calculated as the sum of all applicable item scores, with lower scores indicating better perceived visual function. The Catquest-9SF-CN scores were converted to Rasch-calibrated logit scores to quantify surgical satisfaction. Logit scores before and after capsulotomy, as well as the degree of change, were analyzed between subgroups. The APPLES questionnaire assesses the presence, severity, and frequency of various photic symptoms, including glare, halos, starbursts, and others. Each symptom is rated separately for severity and frequency using a 4-point Likert scale: 1 = none, 2= mild/occasional, 3 = moderate/frequent, and 4 = severe/always. A composite score is calculated by multiplying the severity and frequency scores for each symptom. Higher scores indicate more bothersome visual disturbances. In this study, composite scores were used to compare the impact of different capsulotomy sizes on specific symptoms. Changes in scores before and after treatment were analyzed to evaluate the effectiveness of the intervention on subjective visual quality.
Statistical Analysis
Descriptive statistics were used to summarize baseline characteristics, including age, sex, and ocular laterality. Continuous variables were reported as mean ± standard deviation (SD), while categorical variables were expressed as counts and percentages. To evaluate the impact of capsulotomy size on vision-related satisfaction, pre- and post-treatment Likert scale scores (ranging from 1 to 4) from the questionnaire were converted into Rasch person measures (logits) using the rasch() function in the eRm package in R. Analytic statistics were conducted using SPSS version 23.0 (SPSS Inc., Chicago, IL). The change in satisfaction was measured by the difference in Rasch scores before and after laser treatment. Within-group comparisons of pre- and post- treatment scores were analyzed using paired t-tests. Between-group differences in score changes (L group vs S group) were evaluated using independent t-tests. To evaluate factors associated with changes in Rasch-transformed Catquest-9SF-CN scores, we used generalised estimating equations (GEE) with an exchangeable working correlation to (1) account for potential clustering of eyes within the same participant and (2) provide robust standard errors under mild misspecification—an approach recommended for ophthalmic data with possible inter-eye correlation. Models adjusted for age, sex, pupil size, spherical equivalent (SE), optical aberrations, and corrected visual acuity as covariates.
Overall, eight eyes were excluded from the analysis set due to ineligibility after screening and/or missing 1-month primary outcomes (L group = 3; S group = 5). Statistical significance was defined as a two-sided p-value of < 0.05. All tests were two-sided with α = 0.05 to balance Type I/II error risk for exploratory comparative effectiveness research. Where relevant, 95% confidence intervals and effect sizes are provided to aid clinical interpretation.
Results
Demographic and Baseline Characteristics
A total of 106 eyes were included in the analysis, with 59 in the L group and 47 in the S group. As shown in Table 1, there were no significant differences between the groups in age, gender distribution, pre- and post-treatment spherical equivalent, pupil size under photopic or mesopic conditions, distance between photopic and mesopic pupil center, axial length, or baseline PCO grade. However, both the horizontal and vertical capsulotomy diameters were significantly larger in the L group (P<0.001).
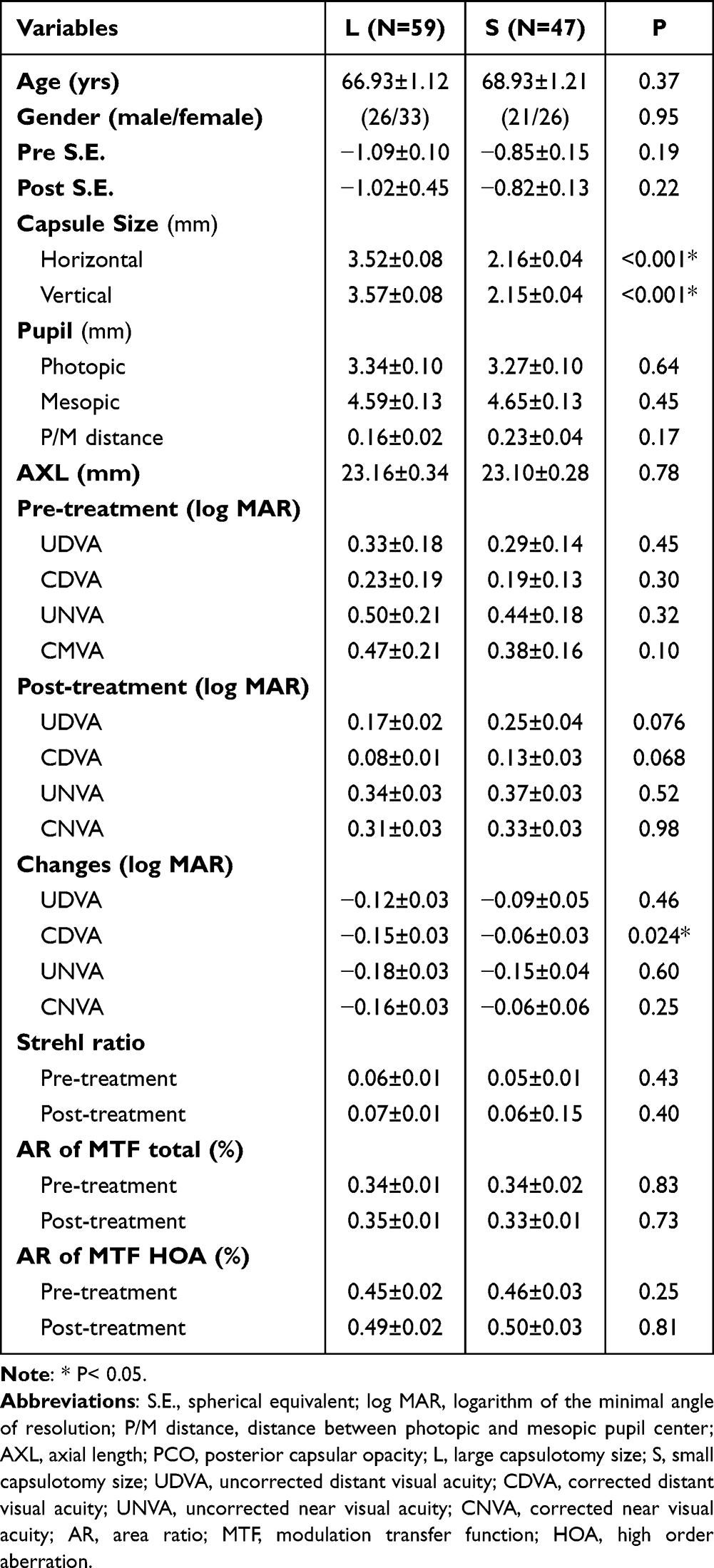 |
Table 1 Comparison of Clinical Characteristics, Pre- and Post-Treatment Visual Acuity, Visual Quality and Their Changes Between Large and Small Capsulotomy Size Groups |
Visual Acuity Outcomes
Both groups experienced improvements in all visual acuity parameters one month after Nd:YAG capsulotomy. While changes in UDVA, UNVA, and CNVA were not statistically different between groups, the improvement in CDVA was significantly greater in the L group (ΔCDVA: –0.15 ± 0.03 vs –0.06 ± 0.03; P=0.024). Although statistically significant, the between-group mean difference (~0.09 logMAR) is approximately one ETDRS line, indicating minimal clinical impact for patients. Objective indicators of optical performance were also analyzed. Both groups showed slight improvements in Strehl ratio following treatment. Regarding the MTF area ratio (total), the L group showed a mild increase, while the S group showed a slight decrease. Similarly, the MTF area ratio for HOA showed small changes. However, none of the intergroup differences in optical performance parameters reached statistical significance.
Optical Quality Analysis
Pre- and post-treatment wavefront analyses are summarized in Table 2. Total aberration decreased in both groups. Tilt aberration also decreased. HOA (RMS) values declined.
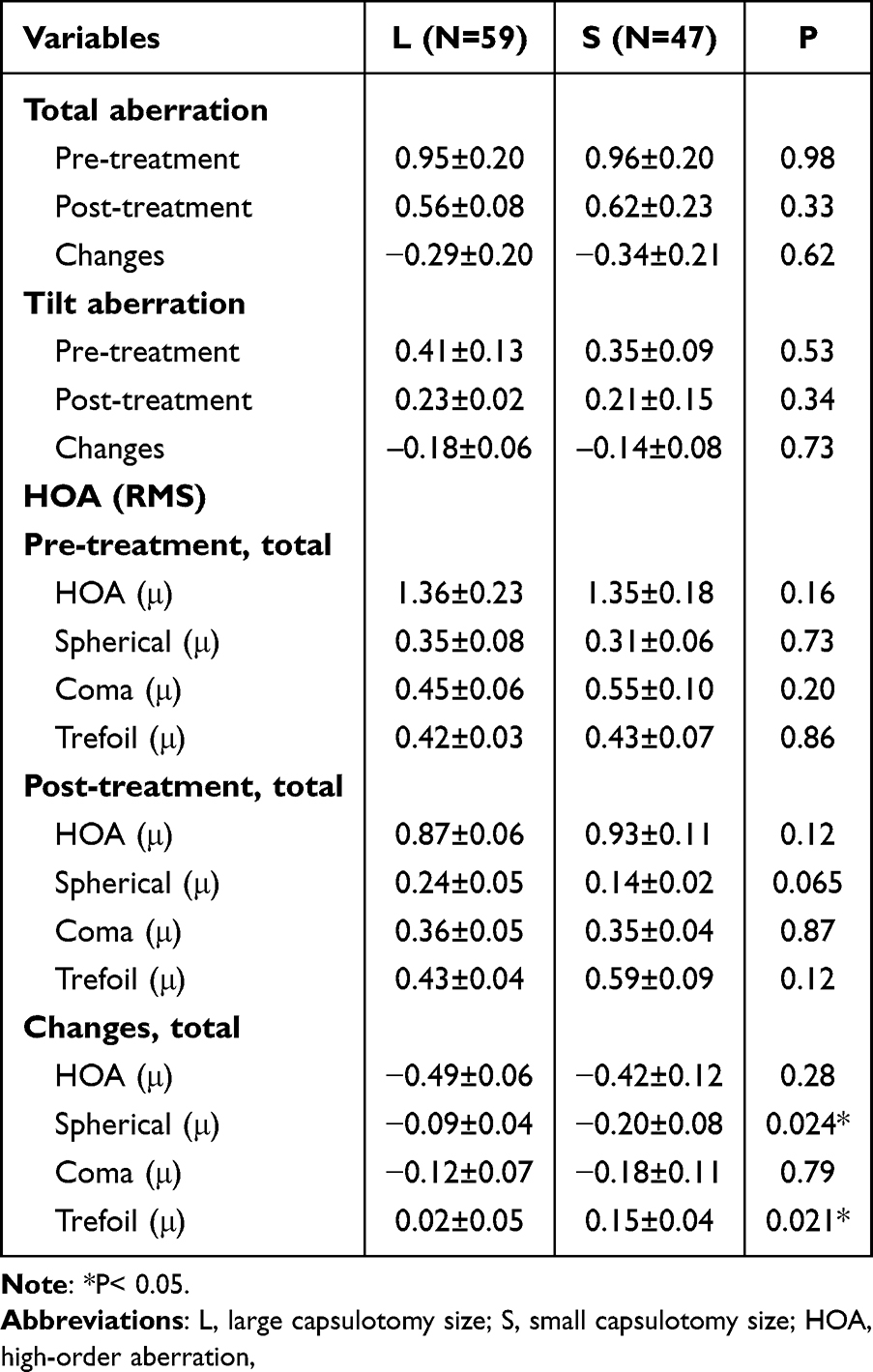 |
Table 2 Comparison of Pre- and Post-Treatment Optical Aberration and Their Changes Between Large and Small Capsulotomy Size Groups |
The HOA (RMS) values represent the root mean square of all higher-order aberration components. To further elucidate the sources of these changes, we analyzed individual HOA components—specifically spherical aberration (SA), coma aberration, and trefoil aberration—as each contributes differently to overall optical quality. SA was significantly more reduced in the S group (Δ = –0.20 ± 0.08) compared to the L group (Δ = –0.09 ± 0.04; P = 0.024). In contrast, coma aberration showed a slight decrease in both groups, with no statistically significant difference between them. Notably, trefoil aberration increased significantly in both the S group (+0.15 ± 0.04) and the L group (+0.02 ± 0.05), with the increase being significantly greater in the S group (P = 0.021).
Defocus Curve and Visual Function
Figure 2 illustrates the defocus curves for the L and S groups at one month postoperatively. Both groups exhibited a wide range of functional vision (logMAR ≤ 0.2) across the defocus range from +1.0 D to –3.0 D, which is consistent with the optical design of the EDOF IOL. After treatment, visual acuity improved in both groups across the defocus range of +3.0 D to –4.0 D. However, no statistically significant differences were observed between the L and S groups in pre-treatment, post-treatment, or the changes in logMAR visual acuity over the range of +3.0 D to –4.0 D.
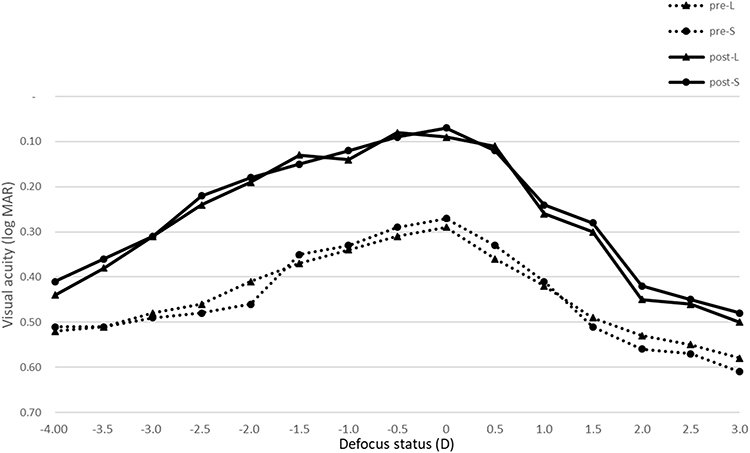 |
Figure 2 Defocus Curves One Month After Nd:YAG Capsulotomy in Eyes with Extended Depth-of-Focus Intraocular Lenses. |
APPLES Questionnaires Results
Table 3 presents APPLES scores before and after treatment. The L group demonstrated a statistically significant improvement in starburst symptoms, with scores decreasing from 1.97 ± 0.38 pre-treatment to 1.54 ± 0.30 post-treatment. In contrast, the S group showed a slight worsening of symptoms, with scores increasing from 1.72 ± 0.23 to 1.79 ± 0.41. The change in starburst scores differed significantly between groups, with the L group showing a greater reduction (Δ–0.43) compared to a slight increase in the S group (Δ+0.07; P = 0.01).
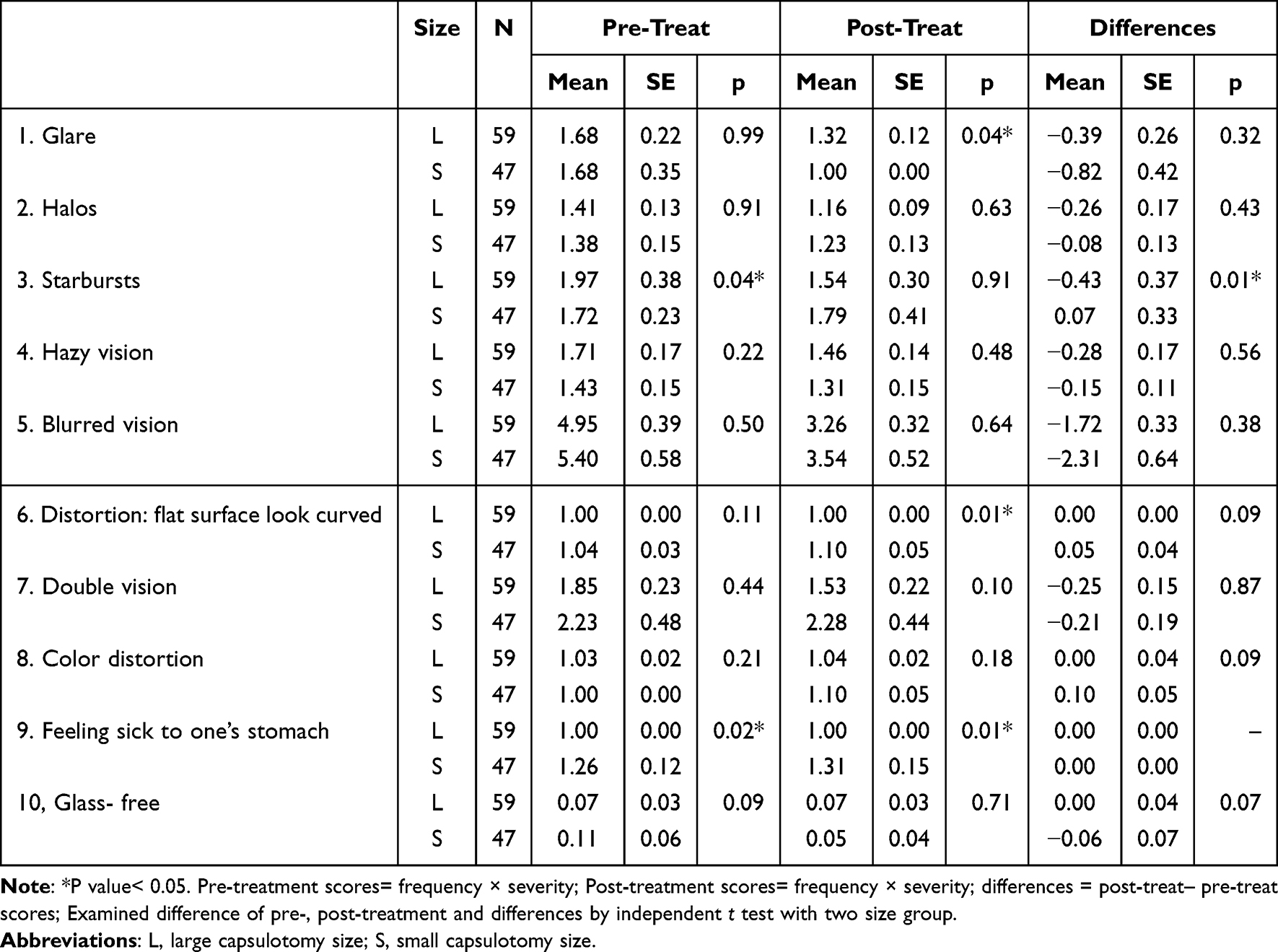 |
Table 3 Comparison of Pre- and Post-Treatment Assessment of Photic Phenomena and Lens Effects (APPLES) Questionnaire Scores and Their Differences Between Large and Small Capsulotomy Size Groups |
Catquest-9SF-CN Results and Predictive Factors
Catquest-9SF-CN logit scores showed a general improvement from baseline to one-month post-treatment. The L group had a significantly lower post-treatment logit score compared to the S group (1.06 ± 0.58 vs 1.29 ± 0.38; P = 0.02), indicating better subjective satisfaction. Although the L group showed a greater numerical improvement in logit scores from baseline (0.56 ± 0.58) compared to the S group (0.36 ± 0.60), this difference in the magnitude of improvement did not reach statistical significance (P = 0.10). The absence of a significant between-group difference in change likely reflects that Catquest-9SF-CN captures global vision-related function over common daily tasks, which may be less sensitive over a 1-month horizon to the domain-specific improvement in photic symptoms captured by APPLES.
A generalized estimating equations (GEE) multiple regression model was conducted to identify factors associated with changes in Rasch-transformed Catquest-9SF-CN scores (Table 4). The analysis revealed that greater refractive error, as measured by spherical equivalent, was significantly associated with reduced subjective visual quality (all models, P = 0.01). Increased tHOAs were also negatively correlated with Rasch scores (Model II: β = –0.15, P < 0.001; Model IV: β = –0.11, P = 0.03), particularly total trefoil aberration (Model I: β = –0.37, P < 0.01; Model III: β = –0.38, P = 0.01). In addition, larger mesopic pupil diameter (β range: –0.39 to –0.45; all P = 0.02), worse corrected distance visual acuity (CDVA: β = –1.13 and –1.25, P < 0.001), and worse corrected near visual acuity (CNVA: β = –0.71, P = 0.02; β = –0.80, P = 0.01) were significantly associated with decreased satisfaction regarding subjective visual quality.
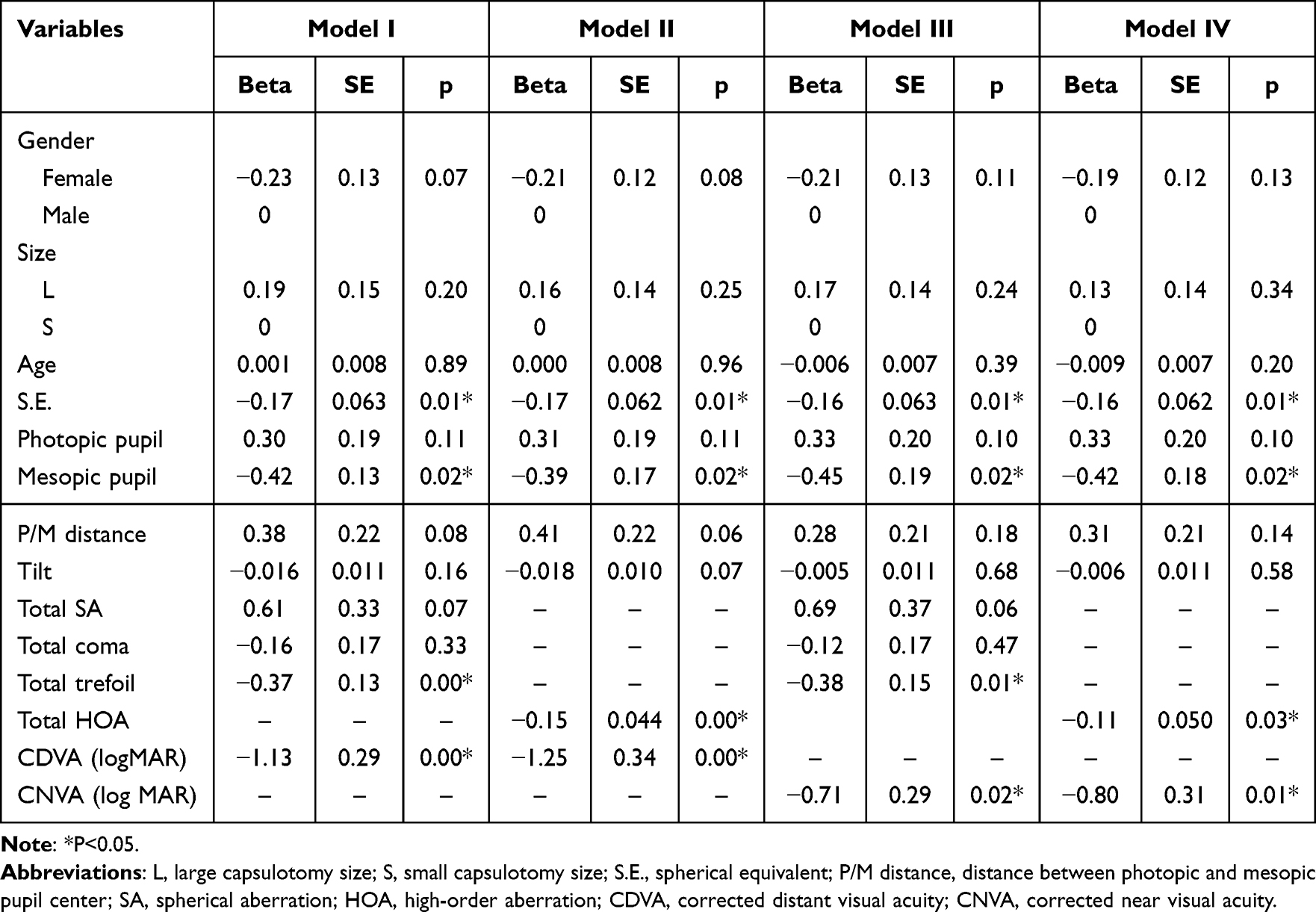 |
Table 4 Factors Associated with Changes in Rasch-Transformed Catquest-9SF-CN Scores: Generalized Estimating Equations (GEE) Multiple Regression Model |
Discussion
This study investigated the impact of posterior capsulotomy size on visual acuity, optical quality, and HOAs in eyes implanted with EDOF IOLs. While Nd:YAG capsulotomy improved vision in both groups, capsulotomy size influenced specific optical parameters and subjective symptoms.
Both small and large capsulotomy groups showed visual acuity improvement, reaffirming the efficacy of Nd:YAG laser in managing visually significant PCO.4,14,15 The L group exhibited a slightly greater gain in CDVA, limited to distance vision, while near visual acuity outcomes were similar between groups. Thus, although statistically significant, the CDVA difference should be interpreted cautiously. Previous literature has recommended capsulotomy sizes of ≤3.5 mm to maintain capsular stability;5 however, our findings suggest that such conservative sizing may be less suitable for EDOF lenses, where small openings may leave central opacities or generate unwanted aberrations.
Objective optical quality, as assessed by Strehl ratio and MTF, improved in both groups, consistent with earlier findings.16 Although between-group differences were not significant, the L group showed a trend toward better optical metrics. These measures—particularly under real-world intermediate or low-contrast conditions—reflect visual function beyond acuity alone.
Given the minimal acuity difference, especially in near vision, capsulotomy size may more strongly influence postoperative HOA profiles. Notably, trefoil aberration increased more in the S group, while SA decreased to a greater extent—highlighting a trade-off between minimizing asymmetric versus symmetric HOAs. These aberration shifts may have greater clinical relevance for subjective vision than acuity measures alone. In EDOF IOLs, which extend depth of focus via echelette optics and manipulation of spherical and chromatic aberrations,8 even small optical disturbances can impact quality. Our findings suggest that larger capsulotomies may help preserve symmetrical light transmission and reduce aberration-related distortion.
Prior studies have shown reductions in total, coma, spherical, and trefoil aberrations after Nd:YAG capsulotomy in various PCO types.17 While some wavefront metrics improve, coma often remains unchanged.18 Though data specific to EDOF IOLs remain limited, the literature supports the procedure’s role in improving acuity, contrast sensitivity, and satisfaction.19,20 Larger capsulotomies in particular have been linked to less intraocular scatter and better outcomes, supporting the idea that asymmetric HOAs play a key role in postoperative quality, especially in EDOF eyes.6,7,21
Our wavefront analysis further clarifies this. Both groups showed reduced total HOAs postoperatively, but differences emerged at the component level. SA decreased more in the S group, potentially enhancing contrast and depth of focus. However, this was offset by a greater rise in trefoil aberration—an asymmetric HOA that compromises clarity and induces photic symptoms like starbursts.
The pronounced increase in trefoil in the S group suggests that small, cruciate-shaped capsulotomies may create irregular posterior capsule edges, resulting in asymmetric light scatter. Previous studies have associated non-circular capsulotomies with greater scatter and aberration.22 Such effects may be more pronounced in small capsulotomies, where tight crossing angles and incomplete openings disrupt wavefront symmetry and degrade visual quality.
Our patient-reported outcomes support this interpretation. In the APPLES questionnaire, the L group reported significant improvement in starburst symptoms, whereas the S group showed a slight decline in satisfaction. Regression analysis further identified postoperative trefoil aberration as a significant predictor of poorer subjective visual quality, aligning with prior studies linking trefoil to increased glare and starbursts, particularly under mesopic conditions.23,24
The marked reduction in SA in the S group may reflect an aperture effect, where smaller capsulotomies limit peripheral light entry, thereby excluding SA from oblique rays. This highlights a clinical trade-off: reducing symmetric aberrations like SA may come at the expense of increased asymmetric HOAs such as trefoil, depending on capsulotomy size.
These results emphasize the importance of individualized surgical planning. For patients with higher preoperative trefoil, larger capsulotomies may minimize irregularities and enhance subjective satisfaction. Conversely, if SA predominates, a smaller capsulotomy may help filter peripheral aberrations without introducing asymmetry. Tailoring capsulotomy size to preoperative HOA profiles may thus optimize visual outcomes.
Defocus curve analysis showed broadly similar performance between groups, with both maintaining a wide range of functional vision (logMAR ≤ 0.2) from +1.0 D to –3.0 D. Although the L group demonstrated a slight numerical trend toward better acuity at intermediate vergences (around –1.50 to –2.00 D), these differences did not reach statistical significance and should be interpreted cautiously.
Catquest-9SF-CN Rasch scores improved in both groups. Although post-treatment scores were slightly better in the L group, the magnitude of improvement from baseline did not differ significantly between groups, consistent with the questionnaire’s focus on global daily-function over a short (1-month) horizon. However, multivariate regression identified postoperative trefoil, mesopic pupil size, and CDVA/CNVA as significant predictors of satisfaction. Notably, capsulotomy size itself was not a direct predictor, suggesting its effect is mediated by optical aberrations rather than surgical geometry alone.
The APPLES results support this conclusion. Starburst symptoms—commonly reported with EDOF IOLs—improved only in the L group, indicating that larger capsulotomies may more effectively reduce photic phenomena. This underscores that minimizing aberration-induced symptoms may be more impactful for patient satisfaction than maximizing acuity alone.
Several limitations should be acknowledged. This was a single-center study with short-term follow-up (1 month), which may not capture delayed effects such as fibrosis or IOL decentration. Wavefront analyses were conducted under controlled conditions, possibly underestimating real-world variability. Although surgical technique and energy settings were standardized, minor differences in centration or capsule morphology could have influenced results. Lastly, these results apply to a specific IOL and may not be generalizable to other EDOF or multifocal lens designs.
Conclusion
While both small and large capsulotomies improved visual acuity after Nd:YAG laser in EDOF IOL patients, the large capsulotomy group showed advantages in CDVA, more stable trefoil aberration, and reduced starburst symptoms. These benefits likely stem not from size alone, but from the optical effects of capsulotomy geometry. A personalized approach—favoring larger openings for trefoil-dominant eyes and smaller ones for SA-dominant profiles—may optimize both visual outcomes and patient satisfaction. Further studies with longer follow-up and broader populations are warranted to validate these findings and refine laser strategies for advanced IOL recipients.
Acknowledgments
The authors acknowledge the support of the Department of Health, Taipei City Government (Project No. 11201-62-022).
Disclosure
The authors received no financial support for the research, authorship, and /or publication of this article. No public or private support was received.
References
1. Chen X, Xu J, Chen X, et al. Cataract: advances in surgery and whether surgery remains the only treatment in future. Adv Ophthalmol Pract Res. 2021;1(1):100008. doi:10.1016/j.aopr.2021.100008
2. Awasthi N, Guo S, Wagner BJ. Posterior capsular opacification: a problem reduced but not yet eradicated. Arch Ophthalmol. 2009;127(4):555–562. doi:10.1001/archophthalmol.2009.3
3. Chan E, Mahroo OA, Spalton DJ. Complications of cataract surgery. Clin Exp Optom. 2010;93(6):379–389. doi:10.1111/j.1444-0938.2010.00516.x
4. Karahan E, Er D, Kaynak S. An overview of Nd:YAG laser capsulotomy. Med Hypothesis Discov Innov Ophthalmol. 2014;3(2):45–50. PMID: 25738159; PMCID: PMC4346677.
5. Cetinkaya S, Cetinkaya YF, Yener HI, et al. The influence of size and shape of Nd:YAG capsulotomy on visual acuity and refraction. Arq Bras Oftalmol. 2015;78(4):220–223. doi:10.5935/0004-2749.20150057
6. Hayashi K, Nakao F, Hayashi H. Influence of size of neodymium:yttrium-aluminium-garnet laser posterior capsulotomy on visual function. Eye. 2010;24(1):101–106. doi:10.1038/eye.2009.41
7. Goble RR, O’Brart DP, Lohmann CP, et al. The role of light scatter in the degradation of visual performance before and after Nd:YAG capsulotomy. Eye. 1994;8(Pt 5):530–534. doi:10.1038/eye.1994.131
8. Kanclerz P, Toto F, Grzybowski A, et al. Extended depth-of-field intraocular lenses: an update. Asia Pac J Ophthalmol. 2020;9(3):194–202. doi:10.1097/APO.0000000000000296
9. Chang DH, Janakiraman DP. Smith PJ, et al. Visual outcomes and safety of an extended depth-of-focus intraocular lens: results of a pivotal clinical trial. J Cataract Refract Surg. 2022;48(3):288–297. doi:10.1097/j.jcrs.0000000000000747
10. Miret JJ, Camps VJ, García C, et al. Analysis of the optical performance of intraocular lenses using profilometric measurements. Graefes Arch Clin Exp Ophthalmol. 2025;263(2):451–465. doi:10.1007/s00417-024-06628-1
11. Congdon N, Fan H, Choi K, et al. Impact of posterior subcapsular opacification on vision and visual function among subjects undergoing cataract surgery in rural China: Study of Cataract Outcomes and Up-Take of Services (SCOUTS) in the caring is hip project, report 5. Br J Ophthalmol. 2008;92(5):598–603. doi:10.1136/bjo.2007.126714
12. Lundström M, Pesudovs K. Catquest-9SF patient outcomes questionnaire: nine-item short-form Rasch-scaled revision of the catquest questionnaire. J Cataract Refract Surg. 2009;35(3):504–513. doi:10.1016/j.jcrs.2008.11.038
13. Grzybowski A, Kanclerz P, Muzyka-Woźniak M. Methods for evaluating quality of life and vision in patients undergoing lens refractive surgery. Graefes Arch Clin Exp Ophthalmol. 2019;257(6):1091–1099. doi:10.1007/s00417-019-04270-w
14. Yotsukura E, Torii H, Saiki M, et al. Effect of neodymium:YAG laser capsulotomy on visual function in patients with posterior capsule opacification and good visual acuity. J Cataract Refract Surg. 2016;42(3):399–404. doi:10.1016/j.jcrs.2015.11.042
15. LoBue SA, Martin CR, Benson KK, et al. The role of early Nd:YAG laser capsulotomy in improving visual performance in mild to moderately symptomatic trifocal patients. Clin Ophthalmol. 2023;17:3991–4000. doi:10.2147/OPTH.S448784
16. McMillin JC, Rocha KM, Barnwell EL, et al. Objective evaluation of vision quality in pseudophakic patients with posterior capsular opacification using double-pass retinal imaging. ARQ Bras Oftalmol. 2019;82(3):189–194.
17. Prasad RS, Koshy TA, Sankarananthan R, et al. Effect of Nd:YAG laser posterior capsulotomy on higher order aberrations in different types of posterior capsule opacification: a prospective study. Indian J Ophthalmol. 2025;73(3):370–376. doi:10.4103/IJO.IJO_3162_23
18. Levy J, Lifshitz T. Klemperer I, et al. The effect of Nd:YAG laser posterior capsulotomy on ocular wave front aberrations. Can J Ophthalmol. 2009;44(5):529–533. doi:10.3129/i09-160
19. Montenegro GA, Marvan P. Dexl A, et al. Posterior capsule opacification assessment and factors that influence visual quality after posterior capsulotomy. Am J Ophthalmol. 2010;150(2):248–253. doi:10.1016/j.ajo.2010.02.026
20. Magno BV, Datiles MB, Lasa MS, et al. Evaluation of visual function following neodymium:YAG laser posterior capsulotomy. Ophthalmology. 1997;104(8):1287–1293.
21. Holladay JT, Bishop JE, Lewis JW. The optimal size of a posterior capsulotomy. J Am Intraocul Implant Soc. 1985;11(1):18–20. doi:10.1016/s0161–6420(97)30146–8.
22. Li J, Yu Z, Song H. The effect of capsulotomy shape on intraocular light-scattering after Nd:YAG laser capsulotomy. J Ophthalmol. 2020;2020:4153109. doi:10.1155/2020/4153109
23. Watson AB, Yellott JI. A unified formula for light-adapted pupil size. J Vis. 2012;12(10):12. doi:10.1167/12.10.12
24. McKelvie J, McArdle B, McGhee C. The influence of tilt, decentration, and pupil size on the higher-order aberration profile of aspheric intraocular lenses. Ophthalmology. 2011;118(9):1724–1731. doi:10.1016/j.ophtha.2011.02.025
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.