Back to Journals » Neuropsychiatric Disease and Treatment » Volume 12
Influence of hypothyroidism on renal function of lithium-treated patients
Authors Lozano R ![]() , Marín R, Santacruz M
, Marín R, Santacruz M
Received 26 November 2015
Accepted for publication 28 November 2015
Published 23 December 2015 Volume 2016:12 Pages 25—27
DOI https://doi.org/10.2147/NDT.S101328
Checked for plagiarism Yes
Editor who approved publication: Dr Roger Pinder
Roberto Lozano, Reyes Marín, María-Jesús Santacruz
Pharmacy Department, Aragones Health Service, Zaragoza, Spain
Several studies have shown that lithium maintenance treatment for bipolar disorder (BD) is associated with chronic kidney disease (CKD).1–3 Three recent and large controlled studies concluded that lithium treatment, within recommended serum levels, may increase the risk of induced end-stage renal disease by twofold1,2 or, alternatively, CKD is associated with BD independent of drug treatment.3 Moreover, review of the safety data on lithium shows a 0–5 mL/min reduction in glomerular filtration rate and a clear reduction in urinary concentrating capacity, during an observation period of 1 year.4
Dear editor
Several studies have shown that lithium maintenance treatment for bipolar disorder (BD) is associated with chronic kidney disease (CKD).1–3 Three recent and large controlled studies concluded that lithium treatment, within recommended serum levels, may increase the risk of induced end-stage renal disease by twofold1,2 or, alternatively, CKD is associated with BD independent of drug treatment.3 Moreover, review of the safety data on lithium shows a 0–5 mL/min reduction in glomerular filtration rate and a clear reduction in urinary concentrating capacity, during an observation period of 1 year.4
However in any case, it should not be excluded the possibility that these associations were a result of bias. In this sense, because the risk of developing thyroid disorders, which is probably the main safety concern of lithium treatment, we would like to highlight the prevalence of hypothyroidism among BD patients as an important possible confounding variable for the associations between lithium treatment and CKD.
Indeed, we know that lithium produces thyroid dysfunction (eg, raised thyroid-stimulating hormone and decreased free thyroxine, among other alterations)4,5 in a high proportion of patients. We also know that there is a close relationship between thyroid and renal function, with hypothyroid patients displaying elevated serum creatinine levels, characterized by slower and incomplete recovery after prolonged periods of severe hypothyroidism, and reductions in glomerular filtration rate.6 These are the main thyroid-related alterations in renal function.
In summary, lithium produces renal dysfunction, which manifests diabetes insipidus and reduction of urine-concentrating ability as the most common renal complications of lithium-derived therapy. Diabetes insipidus, initially reversible upon lithium withdrawal, may become irreversible as a result of structural damage over time.4
Moreover, findings from some authors support a link between mood disorders and thyroid dysfunction, such as higher thyrotropin-releasing hormone stimulated thyroid-stimulating hormone levels observed in naïve BD-II patients, as a differential biological feature,7 among others.8–10
Finally, to continue the above described relationships between thyroid function, renal function and lithium, it is necessary to point out that overt and/or subclinical hypothyroidism and/or diabetes insipidus, two of the most important lithium-induced secondary effects, can be managed entirely by dose reduction, although combination therapy or lithium-substitution could be necessary in some cases.2
In the context of there being a close relationship between BD and thyroid-alterations, between renal and thyroid function, and between lithium treatment and hypothyroidism, we would like to raise the need to further consider the status of thyroid function in order to avoid bias when describing the effects of lithium treatment on renal function.
In fact, alterations in renal function and mood dysfunction could be related to the status of the thyroid function, particularly subclinical and/or overt hypothyroidism, and result in variability of lithium-therapy regimens (eg, cessation of treatment, changes in dosage, or combination therapy). Therapeutic variability, which we observed using data obtained from a post hoc analysis of Actur–Sur cohort, including all psychiatric outpatients referred to our Actur Sur mental health unit in Zaragoza, Spain (Table 1). The results showed that the changes in the treatment of lithium, aforementioned, are present in a high percentage of patients affected by mood disorders, including BD and schizoaffective disorder.
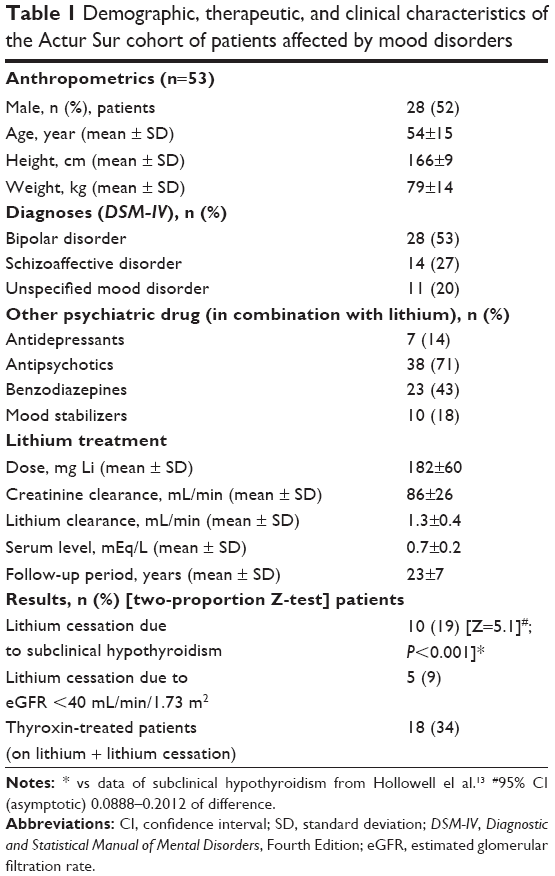 | Table 1 Demographic, therapeutic, and clinical characteristics of the Actur Sur cohort of patients affected by mood disorders |
Thus, taking into account the changes that lithium produces on the thyroid gland, and its relation to mood disorders (eg, BD, schizoaffective disorder), it is evident that to give maximum validity to any current clinical study concerning renal toxicity of lithium, the following should be considered: initial and final thyroid status of patients, use of equi-effective doses of lithium to reach a target range of 1.0–1.1 mEq/L for free thyroxin levels, and stratification of patients according to thyroid activity.11,12 In this manner, we would avoid any bias, due to the thyroid gland status present in BD patients (with or without lithium treatment).
In conclusion, there are methodological hurdles still to be overcome in the standardization of clinical study design in renal toxicity of lithium therapy, with thyroid abnormalities being one of the principal areas of variability, documented among patients with BD.
Disclosure
The author reports no conflicts of interest in this communication.
References
Close H, Reilly J, Mason JM, et al. Renal failure in lithium-treated bipolar disorder: a retrospective cohort study. PLoS One. 2014;9(3): e90169. | ||
Shine B, McKnight RF, Leaver L, Geddes JR. Long-term effects of lithium on renal, thyroid, and parathyroid function: a retrospective analysis of laboratory data. Lancet. 2015;386(9992):461–468. | ||
Kessing LV, Gerds TA, Feldt-Rasmussen B, Andersen PK, Licht RW. Use of lithium and anticonvulsants and the rate of chronic kidney disease: a nationwide population-based study. JAMA Psychiatry. 2015;1–10. | ||
McKnight RF, Adida M, Budge K, Stockton S, Goodwin GM, Geddes JR. Lithium toxicity profile: a systematic review and meta-analysis. Lancet. 2012;379(9817):721–728. | ||
Lozano R, Marín R, Santacruz MJ, Freire I, Gomez R. The efficacy of Li in bipolar disorder. Neuropsychiatr Dis Treat. 2013;9:953–954. | ||
Mariani LH, Berns JS. The renal manifestations of thyroid disease. J Am Soc Nephrol. 2012;23(1):22–26. | ||
Valle J, Ayuso-Gutierrez JL, Abril A, Ayuso-Mateos JL. Evaluation of thyroid function in lithium-naive bipolar patients. Eur Psychiatry. 1999;14(6):341–345. | ||
Hendrick V, Altshuler L, Whybrow P. Psychoneuroendocrinology of mood disorders. The hypothalamic-pituitary-thyroid axis. Psychiatr Clin North Am. 1998;21(2):277–292. | ||
Bauer M, Goetz T, Glenn T, Whybrow PC. The thyroid-brain interaction in thyroid disorders and mood disorders. J Neuroendocrinol. 2008;20(10):1101–1114. | ||
Bunevicius R, Prange AJ. Thyroid disease and mental disorders: cause and effect or only comorbidity? Curr Opin Psychiatry. 2010;23(4): 363–368. | ||
Roberto L. Lithium clearly and directly affects the activity of the thyroid gland in human. Hum Psychopharmacol. 2010;25(7–8):586. | ||
Lozano R, Marin R, Pascual A, Santacruz MJ, Lozano A, Sebastian F. Biomarkers and therapeutic drug monitoring in psychiatry. In: Kumar T, ed. Biomarker. Rijeka: InTech; 2012:155–179. | ||
Hollowell JG, Staehling NW, Flanders WD, et al. Serum TSH, T(4), and thyroid antibodies in the United States population (1988 to 1994): National Health and Nutrition Examination Survey (NHANES III). J Clin Endocrinol Metab. 2002;87(2):489. | ||
Dove Medical Press encourages responsible, free and frank academic debate. The content of the Neuropsychiatric Disease and Treatment ‘letters to the editor’ section does not necessarily represent the views of Dove Medical Press, its officers, agents, employees, related entities or the Neuropsychiatric Disease and Treatment editors. While all reasonable steps have been taken to confirm the content of each letter, Dove Medical Press accepts no liability in respect of the content of any letter, nor is it responsible for the content and accuracy of any letter to the editor. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.