Back to Journals » Journal of Asthma and Allergy » Volume 15
Infectious Asthma: An Easily Identified Clinical Presentation with Implications for Diagnosis, Prognosis, Treatment, and Prevention of Asthma
Authors Hahn DL ![]() , Schultek NM
, Schultek NM ![]()
Received 24 June 2022
Accepted for publication 25 August 2022
Published 9 September 2022 Volume 2022:15 Pages 1269—1272
DOI https://doi.org/10.2147/JAA.S379890
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Amrita Dosanjh
David L Hahn, Nikki M Schultek
Intracell Research Group, Wake Forest, NC, USA
Correspondence: David L Hahn, Intracell Research Group, Wake Forest, NC, USA, Tel +1 608 234-3212, Email [email protected]
Asthma is recognized as a syndrome with multiple underlying etiologies requiring tailored treatments, yet the basic principles of asthma anti-inflammatory therapy remain largely unchanged. An emerging body of epidemiological and clinical evidence points to the possibility that acute infections and their chronic sequelae may be important underlying etiologic and pathophysiologic factors in asthmagenesis for some patients. In this Research Letter we focus on the evidence for and clinical implications of an easily recognizable and surprisingly common asthma clinical presentation that we call Infectious Asthma (IA), defined as asthma that first becomes symptomatic during or after an acute respiratory illness. It is important to emphasize that IA is different from and does not include the well documented propensity for acute (mostly viral) respiratory infections to precipitate asthma exacerbations in people with pre-existing asthma. Nor does IA refer to transient wheezing episodes associated with respiratory illnesses that do not develop into chronic asthma. Our definition for IA refers exclusively to the observation or report of an acute respiratory illness in close proximity to the first symptomatic episode of de novo chronic asthma. This clinical presentation says nothing about any pre-existing or underlying asymptomatic biological characteristics that may also contribute to asthmagenesis. Microbiological diagnoses and inflammatory manifestations of infections in asthma are beyond the scope of this Letter and have been reviewed elsewhere.1
Estimates of IA prevalence are imprecise because clinicians have not been trained to take a history of IA systematically and, with few exceptions, researchers have dismissed IA as either exacerbations of previously unrecognized asthma or as asthma symptoms mistaken as infection. Nevertheless, large, well designed, population-based studies describe temporal associations of clinical infectious illnesses and new-onset asthma. A large 1999 retrospective epidemiologic study of random samples of schoolchildren aged 5–7 years (n=7,545) and 9–11 years (n=7,498) were studied using the International Study of Asthma and Allergies in Childhood (ISAAC) Phase II protocol.2 Children of parents reporting that the child had had ≥5 fever episodes during the first year of life were at increased risk of asthma at up to 11 years of age, suggesting that repeated early childhood infections either “triggered or induced” asthma symptoms. The increased odds of asthma in the children whose parents reported frequent infections was 2.3 (1.4–3.7) when allergy was present and 11.5 (6.0–22.1) when allergy was absent. The report did not provide data allowing derivation of the proportion (prevalence) of children whose asthma was “triggered or induced” by infection. Such prevalence data are available from a 2011 population-based incident case-control study of all new clinically diagnosed cases of asthma (n=521) during a 2.5-year study period and randomly selected controls (n=932) in a geographically defined area of Finland.3 This study reported that a wide variety of respiratory illnesses were strongly associated with the onset of asthma within the following year. The increased odds of asthma after lower respiratory illnesses (acute bronchitis and pneumonia) was 7.2 (5.2–10.0) and after upper respiratory illnesses (common colds, sinusitis, tonsillitis, otitis media) was 2.3 (1.7–3.0). In contrast to the results of the ISAAC study, the odds of developing asthma after lower respiratory illness in this study were greater when allergy was present (11.4, 7.3–17.9) compared to when allergy was absent (8.5, 5.2–14.0). Of those who developed asthma, 35.8% had experienced acute bronchitis or pneumonia in the year prior to asthma onset. This prevalence of ~1/3 is in rough agreement with the prevalence of IA reported in a 1995 clinical descriptive study of 97 primary care outpatients encountered between 1988–1993 with asthma diagnosed according to American Thoracic Society (ATS) criteria.4 The treating clinician systematically recorded whether patients recalled that the very first symptoms of asthma began after an acute respiratory illness. Sufficient history was available to classify 41 (45%) of 92 patients with IA. Compared with the non-IA patient group, those with IA had a significantly shorter asthma duration (5.6 versus 13.3 years, P<0.001), yet significantly worse percentages of predicted FEV1 and FEF25–75% both before and after bronchodilator therapy (P-values ranged from 0.02–0.04). The association of IA and decreased pulmonary function is also suggested by results of a case series of 101 adults with asthma and coexisting COPD (the “overlap syndrome”) in which 77% reported they had IA.5 This high prevalence of IA in overlap syndrome patients suggests a predilection for IA to lead to irreversible airflow limitation. These epidemiologic and clinical studies indicate that IA characterizes a significant amount of asthma and may be associated with the development of fixed airflow limitation. More precise estimates of the population prevalence of IA await better data.
Respiratory viral infections, particularly rhinovirus, are associated with subsequent asthma in children. Fungal infection and sensitization are well recognized contributors to acute exacerbations and asthma severity in both bronchopulmonary Aspergillosis and Severe Asthma with Fungal Sensitization (SAFS), but evidence that these fungal infections present as IA is not available to our knowledge. Perhaps the most impactful potential therapeutic implications of IA relate to associations of IA and the atypical respiratory bacterial pathogens Mycoplasma pneumoniae and Chlamydia pneumoniae in both children and adults (Table 1).
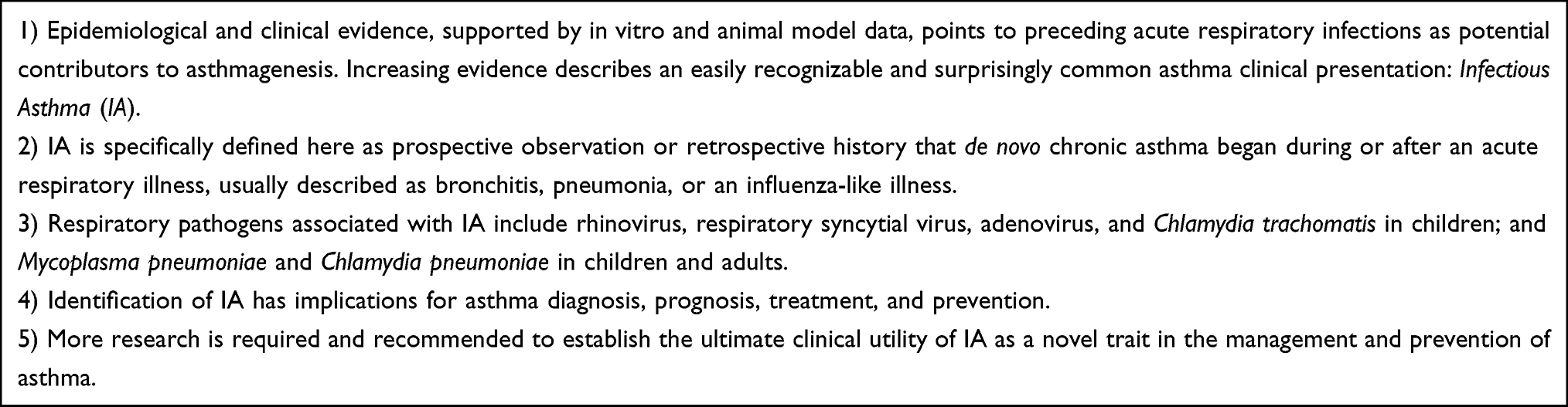 |
Table 1 Infectious Asthma (IA), a Novel Asthma Trait |
M. pneumoniae. A 2016 nationwide historical cohort study performed in Taiwan between 2000–2008 identified 1,591 patients with M. pneumoniae infection (cases) and compared results to 6,364 patients without M. pneumoniae infection (controls) matched on age, sex, and index year.6 Incident cases of both early-onset and late-onset asthma were closely related to prior M. pneumoniae infection, irrespective of age, sex, comorbidity, and atopic status. Over 8 years post-infection ~11% of infected cases developed asthma compared to ~4% of controls. The incident rate ratios, IRRs (95% confidence interval) decreased steadily from 7.3 (6.3–8.4) during the 6-month period after infection to 1.96 (1.7–2.3) ≥2 years after infection. The fact that prior M. pneumoniae infection was associated with new-onset asthma irrespective of age, sex, comorbidity, and atopic status suggests that the primacy of these currently accepted “phenotypes” should be critically re-evaluated in the context of IA.
C. pneumoniae. A 2005 nested case-control study within a 15-year prospective cohort study designed for other purposes measured baseline and follow up C. pneumoniae antibodies (IgG/IgM and IgA) in 83 Finnish adults who developed subsequent incident asthma (cases) and 162 matched controls without asthma.7 High titer C. pneumoniae antibody suggestive for chronic infection (IgG≥1:128 and IgA≥1:32) was significantly associated with greater loss of lung function (FEV1 change, mL/yr) in subjects who contracted new non-atopic asthma compared to other groups (median change in FEV1, 89.6 versus 55.9 mL/y, P=0.032). This study did not detect a significant association of C. pneumoniae antibody and incident asthma. High background antibody prevalence in the general population (~70%) likely decreased power to detect an association of antibody and incident asthma. Furthermore, the study was not designed to diagnose acute infection at the time of new asthma onset. A more sensitive approach is to test for acute infection at the time of a first wheezing episode and then to follow tested participants for the development of de novo asthma. This approach was implemented in a prospective clinical and microbiologic study that evaluated for acute C. pneumoniae infection in 163 outpatients presenting with an acute wheezing illness.8 The study identified a subgroup of 10 adults without any prior history of wheezing symptoms or diagnosis of asthma. At the time of the first acute wheezing illness, all 10 met diagnostic criteria for acute primary (n=8) or secondary (n=2) C. pneumoniae infection. In four patients the wheezing resolved without treatment, in five the wheezing persisted and developed into chronic asthma, and one patient developed chronic bronchitis with chronic sputum production that was culture positive for C. pneumoniae 6 months after the acute infection resolved, confirming chronic infection. Long-term anti-chlamydial antimicrobial treatment resulted in elimination of asthma symptoms in those patients with a prospectively documented C. pneumoniae infection prior to the onset of IA.
The magnitude of the contribution of C. pneumoniae infection to IA is unknown but may be significant based on two observations. First, ecologic data from Finland show that countrywide epidemics of C. pneumoniae infections during the latter part of the 20th century were associated with significant increases in population prevalence of asthma in all age groups and both sexes.9 Second, a 2021 systematic review and meta-analysis found that the population attributable risk (PAR, a measure of the proportion of a disease that may be impacted by removal of the risk factor) of C. pneumoniae-specific IgE in chronic asthma was 47% (95% confidence interval 39–55%) for all levels of asthma severity combined and was even higher for severe asthma.10
Chlamydia trachomatis can cause a protracted, afebrile, eosinophilic pneumonitis in infants that is associated with subsequent asthma. A 1986 retrospective clinical study of 18 African-American infants hospitalized with well documented C. trachomatis pneumonia of infancy (cases) were evaluated 7–8 years later and results were compared to 19 control children.11 To avoid confounding by co-infections, only cases that were culture negative for adenovirus and RSV during the initial hospitalization were selected for evaluation. Despite the small sample sizes, the case group had significantly worse pulmonary function and significantly more reversible airway obstruction compared to controls. Cases were also more likely to cough for ≥3 months per year or to have been diagnosed with asthma by a physician (33% of cases versus 5% of controls, P<0.03, for each condition). C. trachomatis and C. pneumoniae lung infections have been directly confirmed by microbiologic testing of bronchoalveolar lavage fluid in a significant proportion of children with severe asthma and also in other children with non-asthma severe obstructive lung diseases. A prospective, consecutive cohort of 182 children and adolescents (mean age=8.7, range <6 months to 17 years) with severe chronic lung conditions (128 asthma, 54 non-asthma) from a pediatric pulmonology practice underwent bronchoscopy indicated for accepted clinical indications.12 Culture of bronchoalveolar lavage (BAL) fluid for C. trachomatis and/or C. pneumoniae was positive in 59 (46.1%) of 128 patients with asthma and 16 (29.6%) of 54 patients without asthma (P<0.05).
We believe that identification of IA may have important implications for diagnosis, prognosis, treatment, and prevention. The presence of IA should motivate a search for chronic atypical infection as a potentially treatable cause for the asthma syndrome.1 IA may have important prognostic value because evidence suggests that IA is a risk factor for development of reduced lung function and the overlap syndrome.4,5 Regarding treatment, IA is associated with infection by the atypical bacteria M. pneumoniae and C. pneumoniae that are prone to chronic infection.1 Macrolides are now a guideline-recommended option for severe asthma but whom to treat and whether macrolides are directly anti-inflammatory or act via their antimicrobial activities are not established. Further research is warranted into whether IA predicts a positive macrolide treatment response. Another impactful research question is whether early empiric antibiotic treatment of IA can prevent the development of future chronic asthma and the overlap syndrome which is associated with severity, morbidity, and mortality.
Funding
None for manuscript preparation, Atopic LLC has agreed to pay the Open Access fee.
Disclosure
Ms Nikki M. Schultek reports a patent 16923729 issued; and also reports that she previously served as an advisor to Atopic, Corp. The authors report no other conflicts of interest in this work.
References
1. Webley WC, Hahn DL. Infection-mediated asthma: etiology, mechanisms and treatment options, with focus on Chlamydia pneumoniae and macrolides. Respir Res. 2017;18(1). doi:10.1186/s12931-017-0584-z
2. von Mutius E, Illi S, Hirsch T, Leupold W, Keil U, Weiland SK. Frequency of infections and risk of asthma, atopy and airway hyperresponsiveness in children. Eur Respir J. 1999;14(1):4–11. doi:10.1034/j.1399-3003.1999.14a03.x
3. Rantala A, Jaakkola JJ, Jaakkola MS. Respiratory infections precede adult-onset asthma. PLoS One. 2011;6(12):e27912. doi:10.1371/journal.pone.0027912
4. Hahn DL. Infectious asthma: a reemerging clinical entity? J Fam Pract. 1995;41:153–157.
5. Wagshul FA, Brown DT, Schultek NM, Hahn DL. Outcomes of antibiotics in adults with “difficult to treat” asthma or the overlap syndrome. J Asthma Allergy. 2021;14:703–712. doi:10.2147/JAA.S313480
6. Yeh JJ, Wang YC, Hsu WH, Kao CH. Incident asthma and Mycoplasma pneumoniae: a nationwide cohort study. J Allergy Clin Immunol. 2016;137(4):1017–1023. doi:10.1016/j.jaci.2015.09.032
7. Pasternack R, Huhtala H, Karjalainen J. Chlamydophila (Chlamydia) pneumoniae serology and asthma in adults: a longitudinal analysis. J Allergy Clin Immunol. 2005;116(5):1123–1128. doi:10.1016/j.jaci.2005.08.030
8. Hahn DL, McDonald R. Can acute Chlamydia pneumoniae infection initiate chronic asthma? Ann Allergy Asthma Immunol. 1998;81:339–344. doi:10.1016/S1081-1206(10)63126-2
9. Hahn DL. Chlamydia/Mycoplasma: do they cause new-onset asthma in adults? In: Johnston SL, Papadopoulos NG, editors. Respiratory Infections in Allergy and Asthma. Vol. 178. New York Basel: Marcel Dekker, Inc; 2003:645–662.
10. Hahn DL. Chlamydia pneumoniae and chronic asthma: updated systematic review and meta-analysis of population attributable risk. PLoS One. 2021;16(4):e0250034. doi:10.1371/journal.pone.0250034
11. Weiss SG, Newcomb RW, Beem MO. Pulmonary assessment of children after chlamydial pneumonia of infancy. J Pediatr. 1986;108(5 Pt 1):659–664. doi:10.1016/S0022-3476(86)81037-X
12. Webley WC, Tilahun Y, Lay K, et al. Occurrence of Chlamydia trachomatis and Chlamydia pneumoniae in paediatric respiratory infections. Eur Respir J. 2009;33(2):360–367. doi:10.1183/09031936.00019508
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.