Back to Journals » International Medical Case Reports Journal » Volume 15
Infantile Bowel Obstruction in a Patient with Situs Inversus Totalis and Polysplenia: A Case Report
Authors Yusuf Ali A ![]() , Biyikli A, Abdi AM
, Biyikli A, Abdi AM ![]() , Guler I
, Guler I
Received 10 August 2022
Accepted for publication 19 October 2022
Published 28 October 2022 Volume 2022:15 Pages 605—609
DOI https://doi.org/10.2147/IMCRJ.S385808
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Abdullahi Yusuf Ali,1 Ahmet Biyikli,1 Abdishakur Mohamed Abdi,1 Ilkay Guler2
1Department of Pediatric Surgery, Somalia Turkish Training and Research Hospital, Mogadishu, Somalia; 2General Directorate of Public Hospitals, Ministry of Health of Republic of Turkiye, Ankara, Turkey
Correspondence: Abdullahi Yusuf Ali, Tel +252615474485, Email [email protected]
Abstract: The infantile intestinal obstruction associated with situs inversus totalis and polysplenia is extremely rare, with only a few cases reported in the literature. Furthermore, the management of this association is complicated. We report a case of a 2-month-old boy with intestinal obstruction due to malrotation and volvulus with thin translucent omentum sac encasing the small intestine associated with situs inversus totalis, polysplenia, and pulmonary hypertension. To the best of our knowledge, this is the first case of situs inversus totalis with polysplenia, pulmonary hypertension, and intestinal obstruction due to malrotation and volvulus with thin translucent omentum sac encasing the small intestine.
Keywords: situs inversus, polysplenia, dextrocardia, malrotation, midgut volvulus
Introduction
Situs inversus is a rare condition in which body organs are reversed from their normal position.1
Situs inversus totalis is a rare genetic abnormality that has been estimated to happen 1 in 10,000 to 1 in 50,000. In situ inversus totalis rotation is clockwise, but the normal embryonic rotation of the midgut is counter-clockwise direction.6
The abdominal-thoracic viscera are mirrored images and are transposed in situs inversus totalis.2
It can be isolated or associated with other congenital abnormalities, the most common of which is intestinal malrotation, which affects 40–90% of patients.3
On the other hand, polysplenia is identified by the existence of multiple spleens. In approximately 20% of cases, polysplenia is associated with situs inversus.1
We report here a case of situs inversus totalis, polysplenia, and pulmonary hypertension in which intestinal obstruction due to malrotation and volvulus with thin translucent omentum sac encasing the small intestine was the initial presentation.
Case Presentation
A 2-month-old boy was referred to our pediatric surgery department with bilious vomiting and mild abdominal distention since birth.
The baby was born at term by cesarean section to a 25-year-old primigravida mother. On examination, the infant was afebrile and moderately dehydrated.
The abdomen was soft and distended, and the nasogastric aspirate was bilious. Plain radiographs revealed dextrocardia, liver opacity on the left side of his abdomen, and a stomach bubble on the right side suggestive of situs inversus totalis (Figure 1).
 |
Figure 1 X-ray abdomen showing few dilated bowel loops, paucity of distal gas shadow, and dextrocardia. |
In addition, there were a few dilated bowel loops in his upper abdomen with an absence of distal gas shadows. Echocardiography demonstrated dextrocardia and pulmonary hypertension with a systolic pulmonary arterial pressure of 54 mmHg.
The patient was stabilized and resuscitated. After optimization, an abdominal exploration confirmed the situs inversus totalis with the liver and a C-loop of the duodenum on the left side. During the exploration, we also detected that our patient had twelve spleens of different sizes (Figure 2).
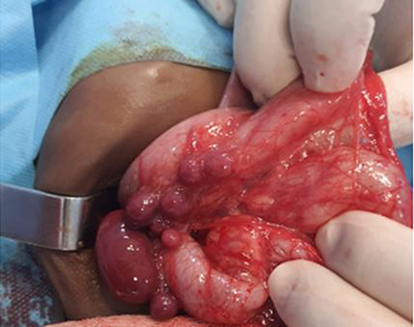 |
Figure 2 Multiple spleens in the upper-right quadrant along the greater curvature of the stomach. |
The entire small bowel was healthy but enclosed in a thin transparent sac containing jelly-like material in the left half of the abdomen (Figure 3).
 |
Figure 3 Intra-operative view of the transparent membrane enclosing the small intestine. |
Several Ladd’s bands crossed the second part of the duodenum with a narrow-base mesentery.
The Ladd’s procedure was performed; the bowel was derotated after excising the thick Ladd’s bands. Subsequently, the sac was excised, and an inversion appendectomy was performed.
The child was referred to the newborn intensive care unit in an intubated state, but the next day, the child was extubated.
The immediate postoperative period was uneventful, and oral feeding started on day five after passing stool. Subsequently, hematemesis and rectal bleeding started for an unknown reason on the eighth postoperative day, and the patient died.
Discussion
Situs inversus totalis (SIT) is a rare autosomal recessive congenital anomaly in which the abdominal organs are fully transposed.4
Therefore, there is a mirror-image transposition of all abdominal organs. The first known case in humans was reported by Fabricius.4
Situs inversus is estimated to occur in 1 in every 8000 to 25,000 live births. The condition is equally distributed among males and females, while boys predominate when there are concurrent splenic anomalies, similarly to the present case.5
Polysplenia syndrome is characterized by the presence of two or more spleens, usually detected during childhood.1
It can be associated with congenital anomalies of the other organs. The position of spleens is variable, and their number can vary from 2 to 16. Approximately 20% of these cases have situs inversus, while more than 40% have cardiac anomalies.1
Our patient had situs inversus totalis with dextrocardia and polysplenia; however, we did not detect any cardiac anomalies.
The midgut’s embryonic rotation is usually counterclockwise, but in situs inversus totalis, the rotation is clockwise.6
Due to this erroneous rotation, the visceral organs are inverted like a mirror image. In almost all cases, situs inversus totalis is diagnosed during a routine check-up or while performing imaging studies for another illness.
Abdominal and chest X-rays, computerized tomography (CT) scans, and barium X-rays can all be used to diagnose this condition. Our case was diagnosed after the referral for an erect abdominal x-ray and an upper gastrointestinal contrast study.
Differential diagnosis includes multiple organ malrotation syndrome.2 Intussusception is commonly present at age 6 and 36 months, and the male-to-female ratio is approximately 3:1. The most common type is ileocolic and others include ileo-ileal, jejuno-jejunal, jejuno-ileal, or colo-colic.9
The case has excluded intussusception according to age, radiologically and intra operative finding as reported (Mulita F, Tchabashvili L, Liolis E, Maroulis I).
Surgical management of neonatal intestinal obstruction associated with situs inversus totalis should follow the same surgical principles as performed for classical cases.2
In addition, the direction of rotation should be examined since transposition of the viscera can lead to midgut volvulus. Ladd’s procedure is the standard corrective surgery for intestinal malrotation in children.7
Notably, Ladd’s procedure involves division of the peritoneal bands (ie, Ladd’s bands) traversing the posterior abdomen, reduction of volvulus, appendectomy, and functional positioning of the intestine with or without fixation.
To the best of our knowledge, there is only one published case of a thin translucent membrane sac encasing the small intestine in the literature.8
Mahalik et al presented a 2-year-old boy with situs inversus totalis, polysplenia, ventricular septal defect, and malrotation with volvulus.8
These authors reported that they removed the sac and thick Ladd’s bands, derotated the bowel and performed an inverted appendectomy.
This child recovered uneventfully and was discharged on the sixth postoperative day. During a two-year follow-up, he was asymptomatic and thriving well.
In our case, although a thin translucent omental sac enveloped the small intestine, the entire small bowel was healthy, and there were no cardiac anomalies.
Subsequently, the patient underwent Ladd’s procedure due to intestinal malrotation with volvulus. Unfortunately, on the eighth postoperative day, hematemesis and rectal hemorrhage began for an unclear reason, and the patient died.
To the best of our knowledge, this is the first case of situs inversus totalis with polysplenia, pulmonary hypertension, and intestinal obstruction due to malrotation and volvulus with thin translucent omentum sac encasing the small intestine.
Conclusion
All newborns should undergo a physical examination in the delivery room for the early detection of situs inversus totalis, and the possibility of encountering life-threatening complications should always be kept in mind.
In situs inversus, due to the transposition of viscera, midgut volvulus may occur in an anticlockwise direction, hence derotation is carried out clockwise.
Ethics Approval
Based on the regulations of the review board of the Mogadishu Somali Turkish Training and Research Hospital, is not required institutional review board approval for the case reports.
Consent for Publication
Written informed consent had obtained by the patient’s parents to have the case details and any accompanying images published.
Acknowledgments
Many thanks to Assoc. Prof. Dr Sertac Cimen and Dr. Mohamed Farah Yusuf Mohamud from the Education Department of Somalia Turkish Training and Research Hospital for their significant contributions while writing this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare no financial support for this study.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Chinya A, Naranje K, Mandelia A. Situs inversus abdominalis, polysplenia, complex jejunal atresia and malrotation in a neonate: a rare association. Int J Surg Case Rep. 2019;56:93–95. doi:10.1016/j.ijscr.2019.02.016
2. Gupta R, Soni V, Valse PD, Goyal RB, Gupta AK, Mathur P. Neonatal intestinal obstruction associated with situs inversus totalis: two case reports and a review of the literature. J Med Case Rep. 2017;11(1):4–9. Doi:10.1186/s13256-017-1423-z
3. Report C. A snared loop on top of malrotation in association with situs inversus, a report of rare presentation; 2022.
4. Alshaikh MA, Al Ghadeer HA, Alabad H, Almohsin M, Al Ali RA. Situs inversus totalis in association with duodenal atresia. Cureus. 2021;13(9). doi:10.7759/cureus.17764
5. Ben Ahmed Y, Ghorbel S, Chouikh T, et al. Combination of partial situs inversus, polysplenia and annular pancreas with duodenal obstruction and intestinal malrotation. Jbr Btr. 2012;95(4):257–260.
6. Bostanci ME, Atabey M, Bozkurt B, Ozel I, Karadayi K. Co-existence of cecal volvulus with situs inversus totalis: a case report. Turkish J Emerg Med. 2016;16(3):134–135. doi:10.1016/j.tjem.2015.01.004
7. Tashjian DB, Weeks B, Brueckner M, Touloukian RJ. Outcomes after a Ladd procedure for intestinal malrotation with heterotaxia. J Pediatr Surg. 2007;42(3):528–531.
8. Mahalik SK, Khanna S, Menon P. Malrotation and volvulus associated with heterotaxy syndrome. J Indian Assoc Pediatr Surg. 2012;17(3):138–140.
9. Mulita F, Tchabashvili L, Liolis E, Maroulis I. Transient small bowel intussusception in a 30-year-old male. Gastroenterol Rev/Przeglad Gastroenterologiczny. 2021;16(3):252–253.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.