Back to Journals » Clinical Interventions in Aging » Volume 15
Inertial Training Improves Strength, Balance, and Gait Speed in Elderly Nursing Home Residents
Authors Naczk M ![]() , Marszalek S, Naczk A
, Marszalek S, Naczk A
Received 26 October 2019
Accepted for publication 20 December 2019
Published 7 February 2020 Volume 2020:15 Pages 177—184
DOI https://doi.org/10.2147/CIA.S234299
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Video abstract presented by Mariusz Naczk.
Views: 920
Mariusz Naczk,1 Slawomir Marszalek,2 Alicja Naczk3
1Institute of Health Sciences, Collegium Medicum, University of Zielona Gora, Zielona Gora, Poland; 2Department of Physiotherapy, Poznan University of Medical Sciences, Poznan, Poland; 3Department of Physical Education and Sport, Faculty of Physical Culture in Gorzow Wielkopolski, University School of Physical Education in Poznan, Gorzow Wielkopolski, Poland
Correspondence: Mariusz Naczk
Institute of Health Sciences, Collegium Medicum, University of Zielona Gora, 28 Zyty St., Zielona Gora 65-046, Poland
Tel/Fax +48 68 328 31 05
Email [email protected]
Purpose: The aim of the study was to evaluate the impact of inertial training on upper and lower extremity strength in the elderly. The study also assessed the influence of inertial training on their independence, balance, and speed and quality of gait.
Methods: Twenty physically inactive older residents of a nursing home (6 women and 14 men; age, 76.7 ± 8.77 years) were randomized to a training (T; n = 10) or control group (C; n = 10). The T group performed inertial training twice a week for 6 weeks using a Cyklotren inertial device. Each training session included 12 exercise sets involving the elbow and knee flexor and extensor muscles (3 sets per single muscle group). The training loads were 10 and 20 kg for the upper and lower extremities, respectively. Before and after training, the maximum force of trained muscles was evaluated under training conditions. Functional tests were also completed.
Results: Participants from the T group had significantly increased (37.1– 69.1%) elbow and knee flexor and extensor muscle strength. Improvement in upper and lower limb strength in non-specific conditions was also noted; 23.3% and 40.6%, respectively. Functional abilities improved significantly in the T group (Tinetti balance test: 29%, Tinetti gait tests: 18.6%, and gait speed (8-Foot Up-and-Go): 12.8%), while remaining unchanged in C.
Conclusion: We strongly recommend a daily routine of inertial training for older adults. Benefits from inertial training can reduce the risk of falls and increase the safety and independence of the elderly.
Keywords: strength training, elderly, balance, gait, eccentric
Introduction
Many negative functional changes occur as a result of aging. Among these are a decrease in muscle strength, sarcopenia, and deterioration in neuromuscular coordination.1,2 Older people also have higher levels of body fat and many have overly high Body Mass Index.3 These changes limit their independence, as daily activities become difficult to perform. As a result of physiological changes with aging, locomotory abilities decline, balance deteriorates, and the risk of falling increases: 30–40% of all people age 65 years and older are reported to fall at least once per year.4 Elderly who are unable to live independently are quite often placed in nursing homes, which provide good living conditions, medical care, and physiotherapy. Unfortunately, the author’s own experience shows that the level of physical activity of residents of nursing homes is low. Participation in exercise programs is voluntary and often not very attractive for the elderly. Moreover, the number of physiotherapy classes is not adequate to the need, because of staffing and technical restrictions. As a result of aging and low physical activity, the functional efficiency of residents deteriorates quickly. Strength training is one of the best workouts for older adults to improve quality of life, increase independence, and prevent falls.5
One of the many strength-training methods is inertial training. It is not very well known, especially in older adults. Inertial training is performed with a specialized device that uses inertial resistance, which differs from more traditional resistance modalities. During inertial exercises, short episodes of eccentric overload occur, and the peak value of strength noted during inertial exercise is greater than during standard weight training.6 These brief episodes of eccentric overload are probably responsible for the high effectiveness of inertial training noted in young men.6 Inertial training is used mainly by young men and athletes. However, some studies showed significant increases in muscle strength over relatively short times in older adults following inertial training. Older women tested by Brzenczek-Owczarzak et al7 improved their shoulder muscle strength from 3.5% to 21.9% after 4 weeks of inertial training. However, the authors did not measure functional changes following training. Onambele et al8 stated that inertial training leads to a greater increase in quadriceps power and gastrocnemius muscle-tendon stiffness than traditional weight training.
To date, there are no studies concerning the influence of inertial training on the strength of different muscle groups in elderly persons who have major musculoskeletal limitations. Moreover, there are little data regarding the usefulness of inertial training in enhancing functionality in the elderly, especially with regard to improving balance and gait quality.
According to current knowledge regarding the impact of training on muscle strength, we hypothesized that inertial training will increase muscles strength and the functional capacity in elderly nursing home residents.
The aim of the study was to evaluate the impact of inertial training on elbow and knee flexor and extensor strength in elderly residents of a nursing home. The study assessed the impact of inertial training on independence and its influence on balance, speed, and quality of gait.
Materials and Methods
Subjects
A group of 68 elderly residents of a nursing home attended an initial meeting and 34 agreed to participate in the study. However, 14 subjects were excluded after the following criteria were applied: bone fractures in the prior 3 months, tendon and ligament injuries in the prior 2 months, serious heart disease, cerebral palsy, and limb amputations. The study finally included 20 physically inactive older people (6 women and 14 men; age, 76.7 ± 8.77 years, range 65–91 years; body mass, 78.3 ± 8.91 kg; height, 174.2 ± 6.72 cm). The participants were randomly allocated into two groups: a training group (T; n = 10) and a control group (C; n = 10) using the chit method. Each group included three women and seven men. The T group participated in 6 weeks of inertial training while the control group maintain their normal daily activity. Details are presented in the participant’s flow diagram (Figure 1). All participants gave written informed consent to take part in the study. Moreover, the participants showed in Figure 2 provided written informed consent for their images to be published. All procedures were approved by the Ethics Committee of Poznan University of Medical Science in Poland, with approval based on the Declaration of Helsinki.
 |
Figure 1 Flow diagram for study participants. |
 |
Figure 2 Subject position during inertial training. (A) elbow flexors exercise. (B) knee flexors exercise. |
Testing
All procedures and training were provided in the nursing home where the participants lived.
The influence of inertial training on each participant’s functional abilities before and after training was evaluated using the following tools:
Activities of Daily Living (ADL) Questionnaire
This concerned bathing and showering, personal hygiene and grooming, dressing, toilet hygiene (getting to the toilet, cleaning oneself, and getting back up), functional mobility, and self-feeding. Participants were rated 1 to 3 points for each task; 1 point when the elderly cannot perform the task, 2 points when he can with help and 3 points when he can do it alone, without help.
The Chair Stand Test
Participants had to repeatedly stand up from and sit down on a chair for 30 s with their arms folded across their chests. The number of stands was recorded.9
The Biceps Curl Test
The participants had to repeatedly lift a 5 lb. (2.27 kg) (women) or 8 lb. (3.63 kg) (men) weight for 30 s. The number of lifts was recorded.9
8-Foot Up-and-Go
The participants were asked to get up from a seated position, walk 8 feet (2.44 m), turn, and return to a seated position. The time required was measured in seconds.9
Tinetti Test for Gait and Balance Evaluation
The Tinetti Assessment Tool is a simple test that measures a participant gait and balance. The participant performs a total of 16 tasks (during 9 tests the researcher assesses the balance of the participant and during 7 subsequent tests the researcher assesses the gait of the participant). Scoring of the Tinetti Assessment Tool is done on a two or 3-point ordinal scale (depend on the task) with a range of 0 to 1 or 0 to 2. A score of 0 represents the most impairment, while a score of 1 or 2 represents independence. The individual scores are then combined to form three measures; an overall gait assessment score, and overall balance assessment score, ad a combined gait and balance score. The maximum score for the gait component is 12 points. The maximum score for the balance component is 16 points. The maximum total score is 28 points. The full description of the test is presented by Tinetti10 and Vaught.11
Strength Measurement Under Inertial Conditions
The maximal force applied using the Cyklotren was measured under the training conditions. The first measurement session was preceded by two trial sessions, where the elderly learned how to perform the exercise properly. The Cyklotren is a new functional cybernetic device for inertial training.12 After warm-up, each participant performed a 10-s maximal test of the flexors and extensors of the elbow and knee joints, separately, with a 1-min break between measurements. All tests were performed while seated in a rehabilitation chair (Figure 2A and B). Different loads were set for the upper and lower extremities; 10 kg for elbow flexors and extensors and 20 kg for knee flexors and extensors. The range of motion for each exercise was approximately 60 degrees. All measured parameters (force, range of motion, etc.) were recorded using a computer and displayed on-line on the screen. The maximal value of force (in newtons) achieved during one full cycle was used for further analysis. The Cyklotren measurements exhibit high reproducibility (interclass correlation coefficient [ICC] consistency ≥0.945, ICC agreement ≥0.932). The absolute error of the measurement system is smaller than 0.5 N.
Training
Inertial training was performed twice a week (Monday and Thursday, between 8:30 a.m. and 4:30 p.m.) for 6 weeks. Training was conducted by the same two researchers. Before each training session, a standardized warm-up comprising 5 mins of submaximal cycling on the lower body ergometer and a few slow cycles with the Cyklotren was performed. Similar to the testing, each exercise was performed in seated position in a rehabilitation chair (Figure 2A and B). Each session trained four muscle groups: the flexors and extensors of the elbow and knee joints. Each exercise included 3 sets, with the right and left extremities worked separately. The work time was 15 s per set. A 2-mins break occurred between consecutive sets. During elbow flexor training in the starting position, the active arm was flexed approximately 100 degrees at the elbow joint. Participant held the handle connected to the rope, which was fully extended and tensed (hand in supination). To begin the exercise, participant flexed the elbow. During elbow extensor training in the starting position the handle was held in pronation, the active arm was flexed approximately 50 degrees at the elbow joint. To begin the exercise, participant extended the elbow. During knee flexor training in the starting position, the active leg was flexed at the knee joint to approximately 120 degree. To begin exercise, participants flexed the knee moving the device handle. During knee extensors training in the starting position, the active leg was flexed at the knee joint to approximately 60 degree. To begin exercise, participants straightened the knee moving the device handle. The range of motion for all exercises was approximately 60 degrees.
Throughout the training period, the loads were constant and were 10 kg for the upper limbs and 20 kg for the lower limbs; however, the number of cycles was progressively increased over the weeks of training.
Statistical Analysis
To confirm a normal distribution of the data, the Shapiro–Wilk test was used. Descriptive statistics, including means and standard deviations, were calculated. Paired t-tests were used to test for significant changes within groups, comparing values before and after training. The simple effect of training for each participant was defined as a relative increase in an analyzed variable after training compared with the before-training value, using the following formula:
where RI is the relative increase and x is the measured value before (pre) and after (post) training. Lower and upper borders of 95% confidence intervals for relative increase were calculated.
Differences in relative increases between groups were tested with one-way ANOVA. If differences were detected, the Scheffé post hoc procedure was used to determine where the differences occurred. The level of significance was set at P ≤ 0.05. The effect size (ES) of the training was calculated using the independent two-sample t-test, and Cohen’s d was determined. The scale presented by Cohen13 indicates that d < 0.41 represents a small ES, 0.41–0.70 a moderate ES, and higher than 0.70 a large ES.
Results
None of the analysed parameters significantly differed between tested groups at the beginning of the experiment.
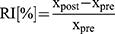
The training group showed statistically significant percentage changes (from 37.1% to 69.1%) in maximal force between pre- and post-training for all trained muscles. Relative increases in maximal force were also significantly greater in the T group compared with the C group. The effect sizes expressed by Cohen’s d value for all strength tests ranged from 1.14 to 3.95 (Table 1). The absolute values of analyzed parameters before and after training are presented in Table 2.
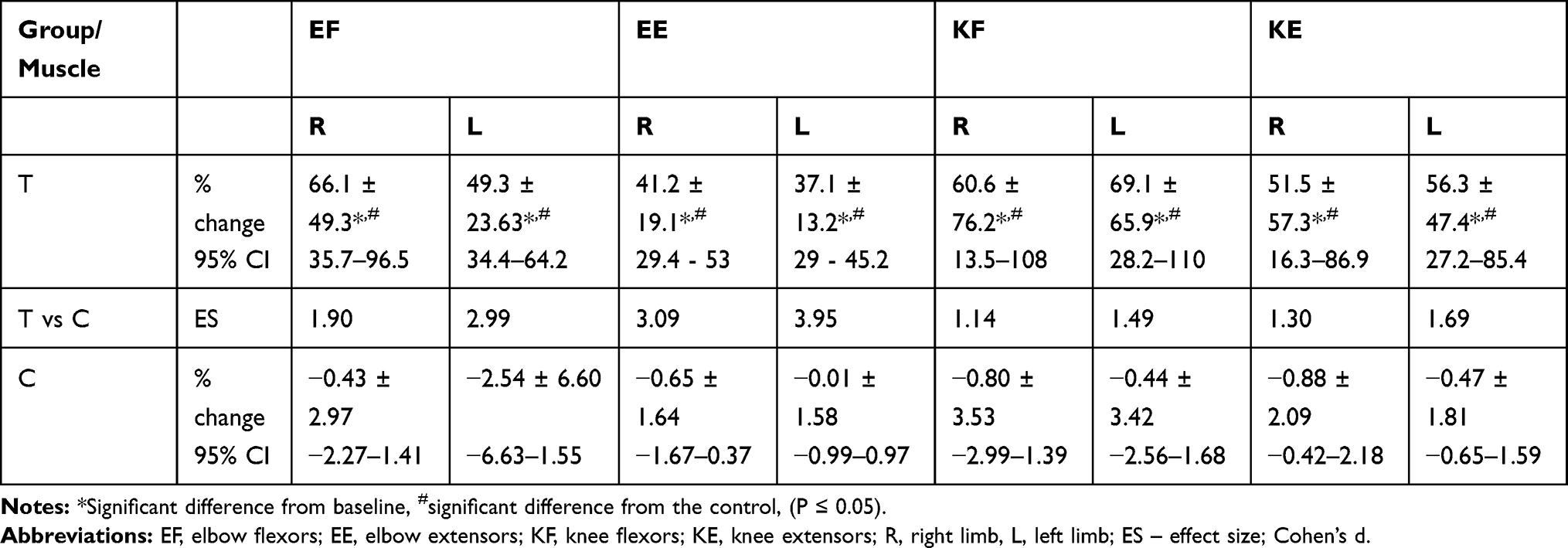 |
Table 1 Mean Percentage Changes, Standard Deviations, 95% Confidence Intervals, and Effect Sizes for Force Measured Using Cyklotren |
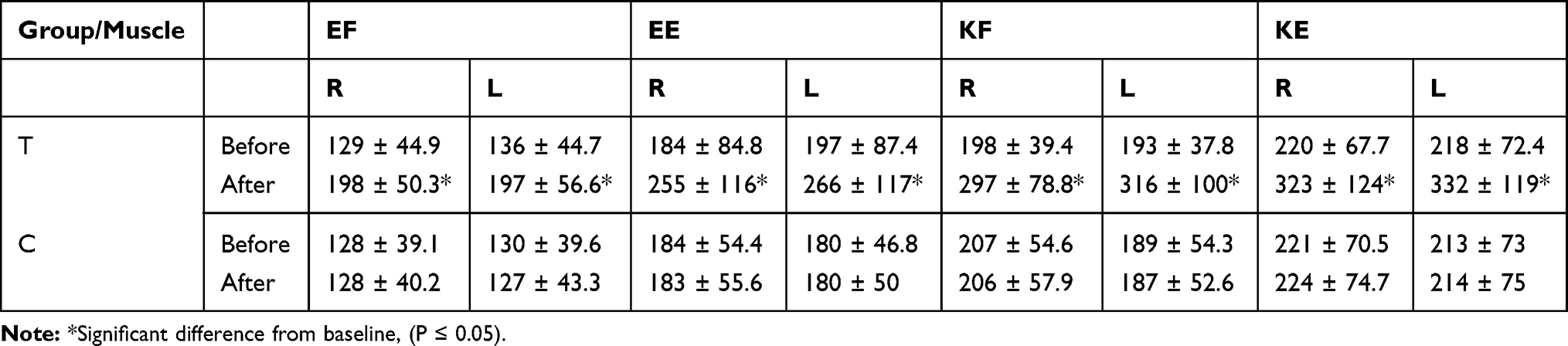 |
Table 2 Mean and Standard Deviations for Absolute Values of Force Measured Using Cyklotren |
Strength measured during the biceps curl test and chair stand test increased significantly in the T group, while it was unchanged in C. Moreover, relative changes in both tests noted in T were significantly greater than those observed in C (Table 3). The time to complete the 8-Foot Up-and-Go test decreased by 12.8% and 1.87% in T and C, respectively. The changes noted in T were significantly greater than those in C. However, ADL was unchanged. Both groups achieved similar numbers of points before and after the training period.
 |
Table 3 Mean Percentage Changes, Standard Deviations, 95% Confidence Intervals, and Effect Sizes for Analyzed Functional Parameters |
The post-training points values on the Tinetti test were significantly higher than the pre-training values in T, while no significant change occurred in C. Gait and balance improvements in T were 18.6% and 29%, respectively, and were significantly greater than those in C, which were 2.1% and 5.55%, respectively (Table 3).
The absolute results of tested functionalities before and after training are presented in Table 4.
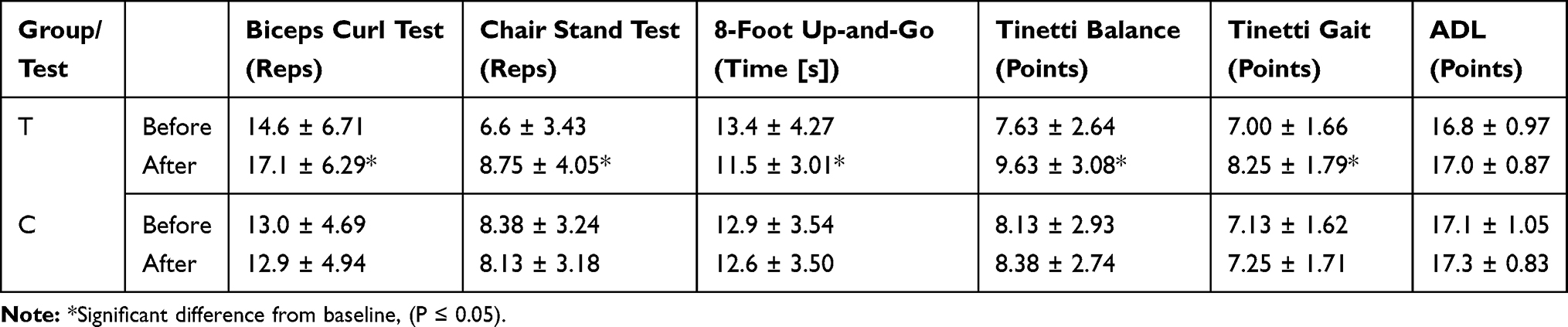 |
Table 4 Mean and Standard Deviations for Absolute Values of Analyzed Functional Parameters |
Discussion
The results of our study indicate that inertial training is highly effective in the elderly who live in nursing homes. Despite their age, participants from the training group increased their elbow and knee flexor and extensor muscle strength significantly. Effect size magnitudes strongly confirmed this observation. Using the Cohen scale,13 we found a high effect size for our training. Moreover, Cohen’s d value for the upper extremities (1.90–3.95) was higher than that for the lower extremities (1.14–1.69). Strength improvement noted in the T group was greater than that observed by Brzenczek-Owczarzak et al,7 who reported a 3.5–21.9% increase in shoulder abductor strength in elderly women following 5 weeks of inertial training. Our participants achieved greater improvements in knee extensor muscle strength than those observed by Onambele et al8 (about 50% vs 8%, respectively). However, the elderly persons trained by Onambele et al8 were tested under a non-specific condition (isometric force) while in our study participants were tested under training conditions. On the other hand, it should be noted that the strength increase noted in our participants in a non-specific condition also increased significantly. Upper and lower body strength evaluated by the Biceps Curl Test and Chair Stand Test improved by 23% and 41%, respectively. To date, the influence of inertial training on muscle strength has been tested mainly in healthy subjects and athletes, and the studies showed that relatively short inertial training periods promote skeletal muscle adaptations in strength, power, and size.14–17 Our results indicate that inertial training can be used by the elderly to enhance their muscle strength. To the best of our knowledge, the improvement in strength (from 37% to 69% for different muscles) achieved by the elderly persons tested in the present study was extremely high. The efficacy of inertial training in the elderly can be greater than that obtained during traditional resistance training. Older women tested by Valour et al18 increased their strength by 11–19% after 7 weeks of elbow-flexor eccentric training. Furthermore, Cannon et al19 reported that 10 weeks of resistance training performed by older women led to significant improvement (18%) in knee extensor strength.
The results of several previous studies showed that strength and power training can reduce the negative effects of aging and help to maintain functional capacity.5,20 There is a lack of knowledge concerning the influence of inertial training on independence and functional abilities in the elderly. Only Onambele et al8 reported an improved balance in elderly persons following inertial training (balance was tested using a piezo-electric force platform). Our study shows that 6 weeks of inertial training enhanced the mobility of elderly persons. Both the 8-Foot Up-and-Go and Tinetti gait tests indicated that confidence and speed of gait improved significantly. Therefore, we recommend using inertial training in the elderly to improve gait quality. Similar to Onambele’s observation, our results showed that a 6-week inertial training can lead to a 29% balance improvement in elderly individuals, as evaluated by the Tinetti test. This is important information for fall prevention in the elderly. Other functional tests (the Biceps Curl Test and Chair Stand Test) showed that inertial training can be useful to improve independence in this population. The American College of Sports Medicine and the American Heart Association suggest that older adults should perform resistance exercises involving the major muscle groups at least twice per week.21 Strength training improves the quality of life and prevents falls. Our study indicates that inertial training can be a good tool to achieve these benefits.
In contrast, responses to the ADL questionnaire did not change following training. In our opinion, this was the result of a ceiling effect. Our participants achieved 16.8 points out of a possible 18. The use of the Instrumental Activities of Daily Living scale rather than the basic ADL scale would probably have been more appropriate in our study.
It would be interesting to know what physiological changes occurred in our participants; we focused only on the mechanical and functional aspects of inertial training. Previous studies showed that increased strength observed after inertial training results from neuromuscular improvement and muscle hypertrophy.8,16,22 It is also possible that activation of agonist muscles increases while antagonist coactivation decreases. However, most studies have been done on young subjects. Future studies are needed to describe and explain physiological changes in the elderly following inertial training.
It is noteworthy that all subjects in the training group enjoyed participating and no one had an injury or a health problem following training (except for DOMS). Seeing the level of their strength displayed on the screen was especially attractive for them. We called it the “competition factor”—participants compared their strength at every training session with the value obtained at the previous one, and they very often compared their strength with that achieved by other participants.
Limitations of the Study
The study was conducted on a small group of participants. A small sample size limits the possibility of drawing strong conclusions. Moreover, physiological and biochemical parameters have not been studied. Physiological tests may indicate mechanisms responsible for changes in muscle strength and improvement of functionality. Biochemical tests may show changes in the health status of the respondents. Another limitation of the research is the lack of data regarding longitudinal effects. We could not test the participant when the project was completed. It was interesting how long the training effect has been maintained.
Clinical Implications
Six-week inertial training performed by elderly nursing home residents:
- caused a great, significant strength increase in trained muscles
- increased gait speed and gait quality
- improved balance
- was well tolerated - no injury was noted
- was an attractive form of exercise
Considering the fact that the availability of inertial devices is better and better, we recommend to include inertial exercises to the rehabilitation process in elderly nursing home residents to improve their safety and quality of life. However, it should be noted, that this study included a small group of participants, therefore future study is needed.
Conclusion
Inertial training led to great improvement in upper and lower limb muscle strength in elderly residents of a nursing home. A 6-week training program produced functional benefits: balance, and confidence and speed of gait improved significantly. These changes lessen the risk of falls and enhance the safety and independence of the elderly. We strongly recommend the addition of inertial training to the daily routines of older adults.
Acknowledgments
We thank all the elderly who participated in this study. The authors also wish to express their appreciation to the Head of Nursing Home in Gorzow Wielkopolski, who cooperated with the researchers. This work was supported by the 2.0 Innovation Voucher (grant no. RPLB.01.02.00-08-0002/17).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bazzucchi I, Marchetti M, Rosponi A, et al. Differences in the force/endurance relationship between young and older men. Eur J Appl Physiol. 2005;93:390–397. doi:10.1007/s00421-004-1277-0
2. Walston JD. Sarcopenia in older adults. Curr Opin Rheumatol. 2012;24:623–627. doi:10.1097/BOR.0b013e328358d59b
3. St-Onge MP, Gallagher D. Body composition changes with aging: the cause or the result of alterations in metabolic rate and macronutrient oxidation? Nutrition. 2010;26:152–155. doi:10.1016/j.nut.2009.07.004
4. Hill K, Vrantsidis F, Haralambous B, et al. An Analysis of Research on Preventing Falls and Falls Injury in Older People: Community, Residential Care and Hospital Settings. Australia, Canberra; 2004. Available from: https://www1.health.gov.au/internet/main/publishing.nsf/Content/health-pubhlth-publicat-document-falls_community-cnt.htm.
5. Persch LN, Ugrinowitsch C, Pereira G, Rodacki ALF. Strength training improves fall-related gait kinematics in the elderly: A randomized controlled trial. Clin Biomech (Bristol, Avon). 2009;24:819–825. doi:10.1016/j.clinbio-mech.2009.07.012
6. Norrbrand L, Pozzo M, Tesch PA. Flywheel resistance training calls for greater eccentric muscle activation than weight training. Eur J Appl Physiol. 2010;110:997–1005. doi:10.1007/s00421-010-1575-7
7. Brzenczek-Owczarzak W, Naczk M, Arlet J, Forjasz J, Jedrzejczak T, Adach Z. Estimation of inertial training efficacy in older women. J Aging Phys Act. 2013;21:433–443. doi:doi.10.1123/japa.21.4.433
8. Onambele GL, Maganaris CN, Mian OS, et al. Neuromuscular and balance responses to flywheel inertial versus weight training in older persons. J Biomech. 2008;41:3133–3138. doi:10.1016/j.jbiomech.2008.09.004
9. Jones CJ, Rikli RE. Measuring functional fitness in older adults. J Active Aging. 2002;2:25–30.
10. Tinetti ME. Performance-oriented assessment of mobility problems in elderly patients. J Am Geriatr Soc. 1986;34:119–126. doi:10.1111/j.1532-5415.1986.tb05480.x
11. Vaught SL. Gait, balance, and fall prevention. Ochsner J. 2001;3:94–97.
12. Naczk M, Naczk A, Brzenczek-Owczarzak W, Arlet J, Adach Z. Inertial training: from the oldest devices to the newest Cyklotren technology. Trends Sport Sci. 2015;22:191–196.
13. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
14. Maroto-Izquierdo S, García-López D, Fernandez-Gonzalo R, Moreira OC, González-Gallego J, de Paz JA. Skeletal muscle functional and structural adaptations after eccentric overload flywheel resistance training: a systematic review and meta-analysis. Sci Med Sport. 2017;20:943–951. doi:10.1016/j.jsams.2017.03.004
15. Nuñez Sanchez FJ, Sáez de Villarreal E. Does Flywheel paradigm training improve muscle volume and force? A meta-analysis. J Strength Cond Res. 2017;31:3177–3186. doi:10.1519/JSC.0000000000002095
16. Naczk M, Naczk A, Brzenczek-Owczarzak W, Arlet J, Adach Z. Impact of inertial training on strength and power performance in young active men. J Strength Cond Res. 2016;30:2107–2113. doi:10.1097/JSC.0000000000000217
17. Naczk M, Lopacinski A, Brzenczek-Owczarzak W, Arlet J, Naczk A, Adach Z. Influence of short-term inertial training on swimming performance in young swimmers. Eur J Sport Sci. 2017;17:369–377. doi:10.1080/17461391.2016.1241304
18. Valour D, Rouji M, Pousson M. Effects of eccentric training on torque-angular velocity-power characteristics of elbow flexor muscles in older women. Exp Gerontol. 2004;39:359–368. doi:10.1016/j.exger.2003.11.007
19. Cannon J, Kay D, Tarpenning KM, Marino FE. Comparative effects of resistance training on peak isometric torque, muscle hypertrophy, voluntary activation and surface EMG between young and elderly women. Clin Physiol Funct Imaging. 2007;27:91–100. doi:10.1111/j.1475-097X.2007.00719.x
20. Hunter GR, McCarthy JP, Bamman MM. Effects of resistance training on older adults. Sports Med. 2004;34:329–348. doi:10.2165/00007256-200434050-00005
21. Nelson ME, Rejeski WJ, Blair SN, et al. Physical activity and public health in older adults: recommendation from the American College of Sports Medicine and the American Heart Association. Circulation. 2007;116:1094–1105. doi:10.1161/CIRCULATIONAHA.107.185650
22. Seynnes OR, de Boer M, Narici MV. Early skeletal muscle hypertrophy and architectural changes in response to high-intensity resistance training. J Appl Physiol. 2007;102:368–373. doi:10.1152/japplphysiol.00789.2006
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.