Back to Journals » Clinical Interventions in Aging » Volume 21
Individualized Perioperative PEEP in Older Surgical Patients: A Three-Dimensional Titration Framework
Authors Hu K, Han X, Guo J, Gan S, He W, Luo C, Yao W ![]()
Received 23 January 2026
Accepted for publication 27 May 2026
Published 4 June 2026 Volume 2026:21 598503
DOI https://doi.org/10.2147/CIA.S598503
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Kexin Hu,1,* Xue Han,2,* Jinyan Guo,1 Shulin Gan,1 Weijie He,1 Chenfang Luo,1 Weifeng Yao1
1Department of Anesthesiology, the Third Affiliated Hospital of Sun Yat-sen University, Guangzhou, Guangdong, 510630, People’s Republic of China; 2Department of Anesthesiology, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, Guangzhou, Guangdong, 510120, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chenfang Luo, Email [email protected] Weifeng Yao, Email [email protected]
Abstract: Postoperative pulmonary complications (PPCs) remain a major determinant of morbidity, delayed functional recovery, and long-term outcomes in older surgical patients. While positive end-expiratory pressure (PEEP) is a cornerstone of lung-protective ventilation, fixed or uniformly high PEEP strategies have yielded inconsistent benefits in the elderly and are frequently limited by hemodynamic intolerance. Accumulating evidence suggests that the optimal PEEP in older patients lies within a narrow therapeutic window defined by competing risks of atelectasis, overdistension, and circulatory compromise. This narrative review synthesizes current evidence linking individualized perioperative PEEP to PPCs and functional recovery in older adults, with a particular focus on the limitations of one-size-fits-all approaches. We propose a pragmatic three-dimensional titration framework that integrates respiratory mechanics (driving pressure and compliance), regional lung imaging (lung ultrasound and electrical impedance tomography), and hemodynamic tolerance to guide PEEP selection. By mapping physiological endpoints to clinical and functional outcomes, we highlight how individualized PEEP strategies may improve perioperative safety and recovery trajectories in the aging population. Finally, we discuss translational pathways, implementation challenges, and key research gaps to inform future trials and clinical adoption.
Keywords: individualized PEEP, older surgical patients, postoperative pulmonary complications, driving pressure, functional recovery
Introduction
Postoperative pulmonary complications (PPCs), commonly including atelectasis, hypoxemia, pneumonia, respiratory failure, bronchospasm, pleural effusion, and the need for unplanned postoperative respiratory support, remain among the most frequent and consequential adverse events following surgery, particularly in older patients. In this review, older patients generally refer to adults aged 65 years or above, while recognizing that age thresholds vary across perioperative studies and that frailty, cardiopulmonary reserve, and baseline functional status may be more clinically informative than chronological age alone. Beyond their immediate respiratory manifestations, PPCs are increasingly recognized as a central driver of prolonged hospitalization, delayed mobilization, increased readmission rates, and long-term functional decline in the aging surgical population. Compared with the general adult surgical population, older patients are more susceptible to PPCs and their downstream consequences because of reduced pulmonary reserve, impaired airway clearance, frailty, a higher burden of comorbidities, and diminished physiological compensation during the perioperative period. With the rapid global expansion of elderly patients undergoing major surgery, optimizing perioperative respiratory management has become a critical priority not only for reducing morbidity but also for preserving postoperative independence and quality of life.1,2
PEEP constitutes a cornerstone of lung-protective ventilation by preventing anesthesia-induced atelectasis, stabilizing alveolar units, and reducing cyclic opening and closing of lung tissue.3 However, despite its widespread use, the optimal perioperative PEEP strategy in older patients remains controversial. Large randomized trials applying fixed low or uniformly high PEEP levels, often combined with recruitment maneuvers, have yielded inconsistent results with respect to PPC reduction. Importantly, these strategies have frequently been accompanied by hemodynamic compromise, including hypotension and increased vasopressor requirements, and these effects are particularly pronounced in older adults with limited cardiovascular reserve.4
The elderly represent a uniquely vulnerable population in whom the therapeutic window for PEEP is markedly narrowed. Age-related increases in closing capacity, reductions in functional residual capacity, and greater regional ventilation heterogeneity predispose older lungs to dependent atelectasis even under modest anesthetic exposure.5 At the same time, age-associated diastolic dysfunction, reduced preload reserve, and impaired right ventricular adaptability render older patients more susceptible to PEEP-induced reductions in venous return and cardiac output.6 As a result, identical PEEP levels may produce fundamentally different and sometimes opposing physiological effects across individuals. In one patient, a given PEEP level may improve aeration and oxygenation, whereas in another it may promote overdistension, dead-space ventilation, hypotension, or increased vasopressor dependence. These differences highlight the limitations of one-size-fits-all ventilation strategies in the aging surgical population.
In recent years, growing attention has shifted toward individualized approaches to PEEP titration that account for interpatient heterogeneity in lung mechanics, regional aeration, and circulatory tolerance. Among proposed physiological targets, driving pressure (ΔP) has emerged as a robust surrogate of global lung stress and a strong predictor of postoperative pulmonary outcomes. However, driving pressure alone cannot capture regional phenomena such as dependent recruitment or nondependent overdistension.7 Advances in bedside imaging, particularly lung ultrasound (LUS) and electrical impedance tomography (EIT), may help refine PEEP selection beyond global mechanical indices. LUS is a radiation-free bedside technique that can identify dependent atelectasis, pleural abnormalities, and changes in lung aeration during recruitment or PEEP adjustment. EIT is a noninvasive monitoring technique that provides continuous, real-time assessment of regional ventilation distribution and can help identify the balance between collapse and overdistension during PEEP titration8. Nevertheless, even physiologically optimal PEEP from a respiratory perspective may not be clinically acceptable if it exceeds an individual patient’s hemodynamic tolerance. Therefore, circulatory safety should be treated not as a secondary observation, but as a defining constraint in PEEP selection for older patients.
Despite these advances, current evidence remains fragmented. Studies vary widely in titration methods, timing, and outcome selection, and few have focused specifically on older patients or incorporated functional recovery as a clinically meaningful endpoint.8 Moreover, most approaches rely on a single physiological dimension, failing to integrate respiratory mechanics, regional lung behavior, and circulatory safety into a unified decision-making framework.9 This lack of integration may partially explain why individualized PEEP strategies often improve physiological parameters but do not consistently translate into reductions in PPCs or improvements in postoperative recovery.
Importantly, the framework proposed in this review is not intended to suggest that experienced clinicians have not previously considered driving pressure, lung aeration, or hemodynamic stability when adjusting ventilator settings. In routine practice, many anesthesiologists already use these parameters, either formally or informally, to guide intraoperative ventilation. Rather, the value of the proposed framework lies in providing a protocol-based, reproducible, and teachable integration of these selected parameters. By converting clinical judgment into a structured pathway, such a framework may improve standardization, support clinician training, facilitate documentation and audit, and provide a clearer basis for future comparative research.
Against this background, we propose that individualized perioperative PEEP in older patients should be conceptualized within a three-dimensional titration framework. This framework integrates (1) driving pressure and compliance to screen for global lung stress, (2) regional lung imaging to validate recruitment and avoid overdistension, and (3) hemodynamic tolerance to define safe upper limits. Operationally, this framework can be translated into a stepwise workflow that includes establishing baseline lung-protective ventilation, identifying candidate PEEP levels through mechanical screening, validating regional aeration when imaging is available, and applying hemodynamic safety limits to determine the final clinically acceptable PEEP. By aligning physiological optimization with clinical feasibility, such a multidimensional approach may better balance lung protection and circulatory safety, thereby reducing PPCs while supporting faster and more complete functional recovery.
In this narrative review, we synthesize current evidence linking individualized perioperative PEEP strategies to PPCs and postoperative functional outcomes in older patients. We critically examine the limitations of fixed PEEP approaches, review available titration tools, and introduce a pragmatic three-dimensional framework for PEEP optimization. Finally, we discuss translational pathways, implementation challenges, and key research gaps to inform future clinical trials and guide perioperative respiratory care in the aging population.
Methods
This narrative review was supported by a structured literature search to inform the development of a pragmatic framework for individualized perioperative PEEP titration in older surgical patients. PubMed, Web of Science, and Embase were searched from database inception to December 2025 using combinations of terms related to PEEP, individualized PEEP titration, driving pressure, lung ultrasound, electrical impedance tomography, transpulmonary pressure, postoperative pulmonary complications, older patients, aging, and perioperative ventilation.
Relevant articles included studies addressing perioperative or intraoperative PEEP strategies, individualized ventilation, respiratory mechanics, imaging-guided titration, hemodynamic effects of PEEP, and postoperative pulmonary outcomes in adult or older surgical populations. Studies involving patients aged ≥65 years were prioritized when available; however, adult studies with mechanistic or clinical relevance to older patients were also considered because age-specific evidence remains limited.
Articles focused exclusively on pediatric or neonatal populations, non-perioperative intensive care settings without relevance to surgical ventilation, or topics unrelated to PEEP titration were excluded. Reference lists of key articles and reviews were manually screened. Findings were synthesized narratively because of heterogeneity in study design, populations, titration methods, and outcomes. The selection process was guided by PRISMA principles where applicable, but no meta-analysis was performed because the review aimed to develop a conceptual and clinically implementable framework rather than estimate pooled effects.
Rationale and Tools for Individualized Perioperative PEEP
Core Objectives of Perioperative PEEP
The primary physiological rationale for applying PEEP during general anesthesia is to counteract anesthesia-related loss of lung volume and prevent the formation of dependent atelectasis.10 Induction of anesthesia rapidly reduces functional residual capacity, promotes airway closure—particularly in dependent lung regions-and impairs ventilation-perfusion matching. These effects are further amplified by surgical positioning, such as Trendelenburg or lateral decubitus positions, and by pneumoperitoneum during laparoscopic procedures, all of which disproportionately affect older patients due to age-related reductions in lung elastic recoil and increased closing capacity.11
Beyond preventing atelectasis, perioperative PEEP aims to stabilize alveoli throughout the respiratory cycle, thereby minimizing cyclic recruitment–derecruitment injury. Repeated opening and closing of unstable lung units generates shear stress at the alveolar interface and contributes to ventilator-induced lung injury, even in patients without pre-existing lung disease.12 However, the application of PEEP entails an inherent trade-off: while insufficient PEEP fails to maintain alveolar stability, excessive PEEP risks alveolar overdistension, impaired pulmonary perfusion, and adverse hemodynamic effects.13 This balance is particularly delicate in older patients, in whom both pulmonary and cardiovascular reserves are reduced.
Therefore, the overarching goal of perioperative PEEP is not the maximization of lung recruitment per se, but the identification of a patient-specific pressure range that maintains alveolar stability, minimizes global and regional lung stress, and preserves circulatory function. This conceptual shift-from applying PEEP as a fixed intervention to titrating it as a dynamic physiological therapy—underpins the rationale for individualized PEEP strategies.
Limitations of Fixed PEEP Strategies
Despite the central role of PEEP in lung-protective ventilation, large clinical trials employing fixed low or high PEEP levels have demonstrated inconsistent effects on postoperative pulmonary complications.14 These mixed results reflect a fundamental limitation of uniform PEEP strategies: identical airway pressures do not translate into equivalent lung or circulatory effects across individuals.
Interpatient heterogeneity is particularly pronounced in older adults. Variations in chest wall compliance, body habitus, and spinal curvature alter the transmission of airway pressure to the lung parenchyma, meaning that the same PEEP may produce under-recruitment in one patient and overdistension in another. Increases in intra-abdominal pressure-whether due to obesity, pneumoperitoneum, or surgical retraction-further modify pleural pressure and shift the pressure–volume relationship of the lung.15,16 As a result, airway pressure alone becomes an unreliable surrogate for lung stress.
In addition, the aging lung is characterized by increased regional heterogeneity, with dependent regions prone to collapse and nondependent regions susceptible to overinflation.12 Fixed PEEP levels cannot accommodate this spatial complexity and may simultaneously under-recruit some lung regions while overdistending others. Importantly, the cardiovascular consequences of PEEP are also highly individualized. Older patients frequently exhibit impaired diastolic filling, reduced preload reserve, and limited right ventricular adaptability, rendering them vulnerable to PEEP-induced reductions in venous return and cardiac output.17 Thus, a PEEP level that appears “lung protective” based on respiratory mechanics alone may be clinically unacceptable due to hemodynamic intolerance.
Together, these factors explain why fixed PEEP strategies have failed to consistently improve outcomes in heterogeneous surgical populations and highlight the need for approaches that explicitly account for individual lung mechanics, regional aeration, and circulatory reserve.
Tools and Operational Considerations for Individualized PEEP
To move beyond uniform strategies, individualized PEEP titration requires tools capable of capturing relevant physiological dimensions at the bedside.18 These tools can be broadly categorized into mechanical indices, imaging-based assessments, and safety boundaries that define acceptable limits of intervention.
Mechanical indices provide an initial, global assessment of lung stress. Driving pressure (ΔP), defined as the difference between plateau pressure and PEEP, has emerged as a particularly informative parameter, as it reflects the cyclic stress applied to the respiratory system and has been consistently associated with pulmonary outcomes.19 Static and dynamic respiratory compliance offer complementary information regarding lung recruitability and overdistension, while transpulmonary pressure—estimated using esophageal manometry—allows partitioning of airway pressure into lung and chest wall components, which is especially relevant in older patients with altered chest wall mechanics.20
Imaging-based tools enable regional validation of mechanical findings. Computed tomography remains the reference standard for assessing lung recruitment and overdistension but is impractical for routine perioperative use. Lung ultrasound (LUS) offers a bedside, radiation-free alternative for detecting dependent atelectasis and monitoring recruitment dynamics, whereas electrical impedance tomography (EIT) provides continuous, real-time visualization of regional ventilation distribution and changes in lung impedance during PEEP titration. These modalities help identify the point at which additional PEEP yields diminishing recruitment or induces nondependent overdistension—information not discernible from global mechanics alone.21
Timing of assessment is a critical yet often underappreciated aspect of individualized PEEP. Lung mechanics and aeration are dynamic during surgery and should be reassessed at key perioperative transitions, including immediately after induction, following major position changes, after establishment of pneumoperitoneum, and prior to emergence.22 Failure to re-evaluate PEEP under changing conditions may negate the benefits of initial titration.
Finally, safety boundaries must be explicitly defined to ensure clinical feasibility. These include limits on plateau pressure and driving pressure to prevent excessive lung stress, as well as hemodynamic thresholds such as mean arterial pressure, cardiac output surrogates, and vasopressor requirements. In older patients, even modest hemodynamic deterioration may have disproportionate consequences, reinforcing the need to integrate circulatory tolerance into PEEP decision-making rather than treating it as a secondary consideration.23
An overview of commonly used PEEP titration tools, their physiological targets, advantages, and limitations in older patients is summarized in Table 1, highlighting that no single modality is sufficient in isolation. Instead, meaningful individualization emerges from the integration of complementary information across mechanical, imaging, and hemodynamic domains.
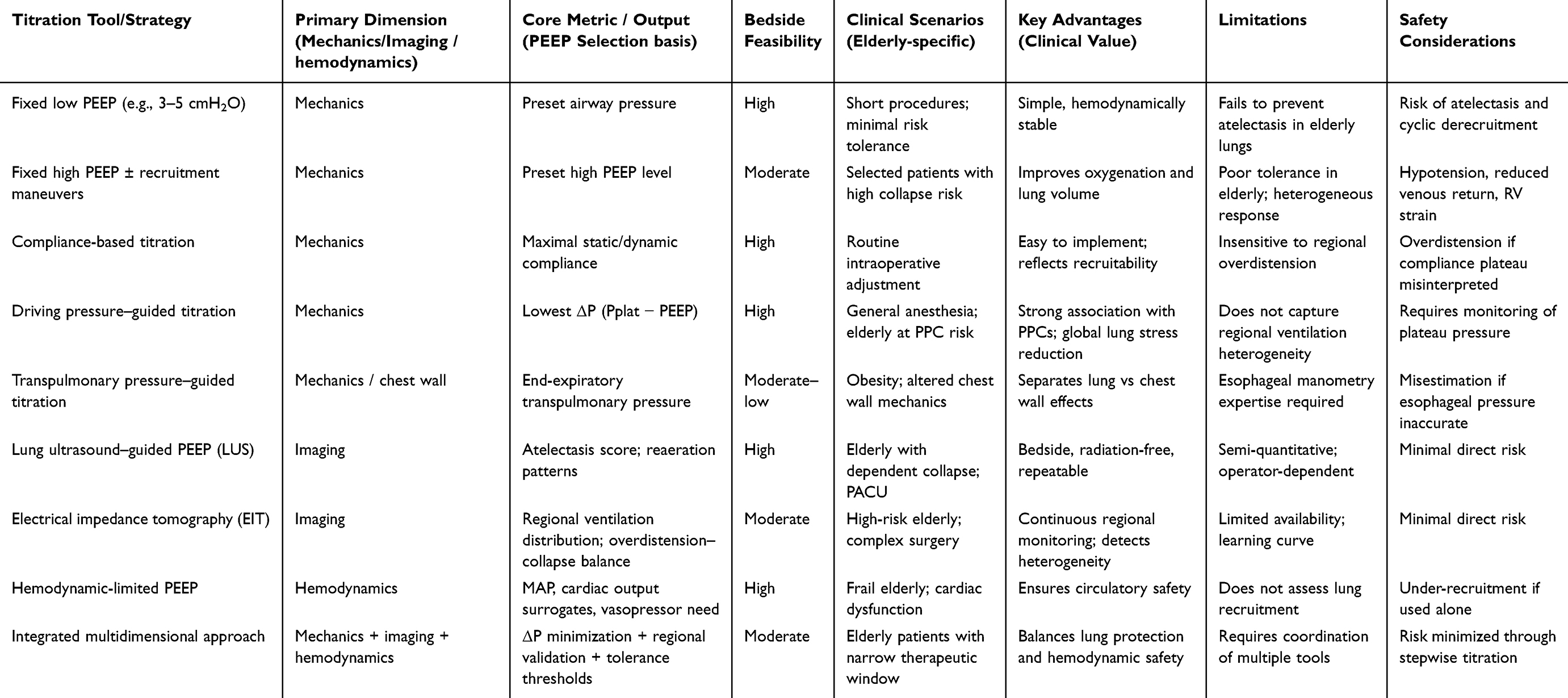 |
Table 1 Comparison of PEEP Titration Tools and Strategies in Older Patients |
The Aging Lung and Circulation: Why a Three-Dimensional Framework Is Needed
Structural and Functional Features of the Aging Lung
Older patients in this review primarily refer to adults aged ≥65 years, although age thresholds vary across perioperative studies and physiological vulnerability is not determined by chronological age alone. Frailty, cardiopulmonary reserve, baseline functional status, and comorbidity burden may also influence PEEP tolerance and PPC risk. Older patients enter the perioperative period with a respiratory system that is predisposed to collapse and heterogeneity even before anesthesia is administered. A hallmark of pulmonary aging is the progressive increase in closing capacity, driven by loss of elastic recoil and altered small-airway mechanics.24 When closing capacity approaches or exceeds functional residual capacity (FRC)—a scenario that becomes more common with age—airway closure can occur during normal tidal breathing, particularly in dependent regions. General anesthesia further reduces FRC and blunts tonic diaphragmatic activity, making airway closure and atelectasis more likely and more extensive in older adults than in younger patients.25
In parallel, aging increases the spatial non-uniformity of ventilation. The combination of altered lung compliance, changes in chest wall mechanics, and gravitational effects promotes a pattern in which dependent lung units collapse while nondependent units remain relatively well aerated and thus more vulnerable to overdistension when airway pressures rise. This “recruitment-overdistension asymmetry” is clinically important: oxygenation may improve with higher PEEP even while regional stress concentrates in already open lung regions.26,27 As a result, global mechanical improvements can mask regional injury risk, underscoring the need for regional assessment rather than reliance on single global indices.
A further contributor to perioperative vulnerability is reduced mucociliary clearance and cough effectiveness in older patients, which together impair secretion handling and increase susceptibility to postoperative infections and atelectasis persistence. Sedation, opioids, pain-related splinting, and limited mobility compound these age-related changes, creating a physiologic milieu in which minor intraoperative derecruitment can progress to clinically meaningful PPCs during recovery. Collectively, these features explain why the aging lung is not merely a “smaller reserve” version of the young lung but a qualitatively different system in which the balance between collapse prevention and overdistension avoidance is more fragile.28,29
Mechanistically, these age-related changes create a direct pathway from perioperative derecruitment to PPCs. Loss of elastic recoil and altered small-airway mechanics increase closing capacity, and when closing capacity approaches or exceeds functional residual capacity, airway closure may occur during normal tidal breathing, particularly in dependent lung regions.24,25 General anesthesia and neuromuscular blockade further reduce functional residual capacity, impair diaphragmatic activity, and promote rapid formation of dependent atelectasis, thereby aggravating ventilation–perfusion mismatch and perioperative hypoxemia.22,29 In older patients, these intraoperative changes are more likely to persist into the postoperative period because mucociliary clearance, cough effectiveness, respiratory muscle performance, and early mobilization are frequently impaired.25,28,29 Consequently, even modest atelectasis or derecruitment may progress to clinically relevant PPCs, including hypoxemia, pneumonia, respiratory failure, and delayed postoperative recovery.29
Hemodynamic Vulnerability in Older Patients
The circulatory consequences of PEEP are magnified in older adults because cardiovascular aging reduces the ability to buffer abrupt changes in intrathoracic pressure and venous return. Age-associated declines in cardiac reserve—often accompanied by diastolic dysfunction and increased ventricular stiffness—make preload dependence more pronounced. When PEEP increases mean intrathoracic pressure, venous return may fall, left ventricular filling becomes impaired, and systemic blood pressure can decline. In older patients, this sequence may occur at PEEP levels that are well tolerated in younger adults, particularly in the presence of anesthetic-induced vasodilation, relative hypovolemia, or pre-existing antihypertensive therapy.30,31
PEEP can also increase right ventricular (RV) afterload by elevating transpulmonary pressure and altering pulmonary vascular resistance, especially if overdistension occurs in nondependent lung regions. Older patients may have limited RV–pulmonary vascular coupling reserve, rendering them vulnerable to RV strain, reduced pulmonary blood flow, and downstream impairment of left-sided filling. Importantly, these hemodynamic perturbations are not simply “side effects” but can directly influence organ perfusion, delirium risk, renal outcomes, and overall recovery trajectories onal constraint but a central determinant of whether a given PEEP strategy is clinically viable in the elderly.
Taken together, age-related cardiac and vascular changes mean that PEEP titration cannot focus solely on optimizing lung mechanics or oxygenation. In older patients, a physiologically “best” PEEP from a respiratory standpoint may be unacceptable if achieved at the cost of hypotension, escalated vasopressor exposure, or RV stress. This reinforces the need to incorporate circulatory endpoints into PEEP decision-making.
The “Narrow Therapeutic Window” of PEEP in Older Adults
The coexistence of an atelectasis-prone lung and a hemodynamically vulnerable circulation creates a narrow therapeutic window for PEEP in older patients. On one side of this window, insufficient PEEP permits airway closure, dependent atelectasis, and cyclic recruitment–derecruitment, promoting ventilation-perfusion mismatch, inflammatory injury, and downstream PPCs. On the other side, excessive PEEP may shift lung units into overdistension, increase transpulmonary stress, worsen pulmonary perfusion distribution, and precipitate hemodynamic compromise through reduced venous return and RV loading. In older adults, the distance between these two failure modes is often small, and the location of the optimal point varies markedly among individuals and across perioperative stages (eg, after positioning or pneumoperitoneum).32,33
Within this narrow therapeutic window, appropriately selected PEEP may provide several mechanistic benefits for older patients. By increasing end-expiratory lung volume and maintaining small-airway patency, PEEP can partially counteract anesthesia-induced reductions in functional residual capacity and limit dependent atelectasis.22,29 Stabilization of recruited alveolar units may reduce cyclic recruitment–derecruitment, improve ventilation–perfusion matching, and attenuate atelectasis-related lung injury, thereby providing a plausible mechanism for reducing PPC risk.12,13,33 This protective effect is particularly relevant in older adults, in whom postoperative atelectasis may persist because of impaired cough, reduced secretion clearance, opioid-related respiratory depression, pain-limited deep breathing, and delayed mobilization.25,28,29 Clinical studies further support this physiological rationale, showing that individualized PEEP strategies guided by respiratory mechanics or lung ultrasound can improve intraoperative respiratory mechanics and reduce postoperative atelectasis in elderly surgical patients.34,35
This narrow window also explains why single-parameter approaches can underperform. If PEEP selection relies only on global mechanics (eg, compliance or driving pressure), it may overlook regional overdistension or persistent dependent collapse. If it relies only on imaging markers of recruitment, it may inadvertently push PEEP beyond a patient’s hemodynamic tolerance.18 Conversely, if PEEP titration is guided primarily by blood pressure or vasopressor use, clinicians may accept clinically meaningful derecruitment that later manifests as PPCs. Accordingly, a robust approach in older patients must explicitly manage three competing objectives: minimizing global lung stress, ensuring regional recruitment without overdistension, and maintaining hemodynamic stability.36
These interlocking vulnerabilities are schematically summarized in Figure 1, which illustrates how aging shifts the balance toward collapse, amplifies ventilation heterogeneity, and reduces circulatory buffering capacity, thereby narrowing the safe and effective PEEP range. This mechanistic context provides the rationale for a three-dimensional framework integrating driving pressure-based mechanical screening, imaging-based regional validation, and hemodynamic tolerance as complementary constraints for individualized perioperative PEEP titration in older adults.
 |
Figure 1 Physiological vulnerability to PEEP in older patients. |
Therefore, the benefit of PEEP in older patients is conditional rather than absolute. The same pressure that prevents dependent collapse in one patient may overdistend already aerated nondependent regions or exceed cardiovascular tolerance in another patient. This conditional benefit provides the physiological justification for integrating mechanical screening, imaging-based regional validation, and hemodynamic safety limits into a unified titration strategy.
Construction of a Three-Dimensional PEEP Titration Framework
Clinical Background and Objectives
The inconsistent benefits of uniform perioperative PEEP strategies in heterogeneous surgical populations—together with the heightened hemodynamic vulnerability of older adults—suggest that the “optimal PEEP” cannot be defined as a single universal value. Rather, PEEP should be treated as a titratable therapy whose net benefit depends on the balance between three competing risks: dependent atelectasis and cyclic derecruitment, nondependent overdistension and lung stress, and PEEP-induced circulatory compromise.14,37 In older patients, this balance is particularly precarious because the safe and effective range of PEEP is narrow and may shift rapidly with changes in position, pneumoperitoneum, anesthetic depth, and fluid–vasopressor management.
Accordingly, the objective of an individualized approach is not simply to improve oxygenation or maximize recruitment, but to maximize lung protection while preserving circulatory safety. This requires a pragmatic framework that (i) uses readily available bedside signals to identify candidate PEEP levels, (ii) validates that these levels achieve recruitment without harmful overdistension, and (iii) explicitly incorporates hemodynamic tolerance as a decisive constraint. To achieve these goals in a manner that is feasible in routine perioperative practice, we propose a three-dimensional PEEP titration framework that integrates respiratory mechanics, regional lung imaging, and hemodynamic “brakes” into a stepwise decision pathway.38,39
Three Core Dimensions of the Framework
Dimension 1: Mechanical Screening to Reduce Global Lung Stress
The first dimension uses global respiratory mechanics to screen for PEEP levels that minimize overall lung stress. Driving pressure (ΔP) and compliance provide a pragmatic readout of how much cyclic strain is being imposed on the respiratory system under a given PEEP. In the perioperative setting, mechanical screening serves two functions: it identifies PEEP ranges where recruitment likely improves compliance, and it avoids excessive plateau pressures that may reflect overdistension. Importantly, mechanical indices are most effective as an initial “coarse filter” rather than a definitive endpoint, because they cannot distinguish regional collapse from regional overinflation.40
Dimension 2: Imaging-Based Validation of Regional Recruitment and Overdistension
The second dimension introduces regional assessment to address the key limitation of global mechanics: the inability to detect spatial heterogeneity.41 Lung ultrasound (LUS) can detect dependent atelectasis and track reaeration during PEEP adjustments, whereas electrical impedance tomography (EIT) offers continuous monitoring of regional ventilation distribution and can quantify trade-offs between collapse and overdistension. Imaging thus functions as a “fine-tuning” layer: among mechanically acceptable PEEP candidates, it helps select the level that achieves the best regional balance—recruiting dependent units while avoiding nondependent overdistension.
Dimension 3: Hemodynamic Tolerance as a Safety ceiling42,43
The third dimension defines the hemodynamic safety boundaries that constrain PEEP escalation. In older patients, even modest increases in intrathoracic pressure may reduce venous return, impair cardiac output, and precipitate hypotension or increased vasopressor requirements. Hemodynamic tolerance therefore acts as an explicit “brake”: it sets an individualized upper limit for PEEP, beyond which physiological lung optimization becomes clinically unsafe.44,45 Importantly, hemodynamic assessment should go beyond a single blood pressure reading and incorporate trends in mean arterial pressure, vasopressor dose, heart rate, and—when available—cardiac output surrogates or echocardiographic indicators of right ventricular strain.46
Taken together, these three dimensions form a complementary triad: mechanics provides global screening, imaging provides regional validation, and hemodynamics provides a patient-specific safety ceiling. Their integration is particularly suited to older adults, in whom the trade-offs between recruitment, overdistension, and perfusion compromise are amplified.
A Four-Step Titration Workflow
To translate these dimensions into an operational clinical pathway, we propose a four-step titration workflow that can be applied during general anesthesia and repeated at key perioperative transitions.47 The process is designed to be pragmatic: it relies first on widely available mechanical signals, adds imaging when feasible for refinement, and always incorporates hemodynamic tolerance as a non-negotiable constraint.
Step 1: Establish Baseline Lung-Protective Ventilation
Titration should begin from a standardized protective baseline to ensure comparability across subsequent adjustments. This includes low tidal volume ventilation based on predicted body weight, avoidance of excessive plateau pressures, and optimization of respiratory rate to maintain adequate ventilation.48 Baseline PEEP should be set according to the “minimum effective pressure” principle rather than as a fixed high PEEP level. In routine practice, an initial PEEP of 3–5 cmH2O may be applied after induction to prevent early derecruitment while preserving hemodynamic stability and allowing subsequent upward or downward titration.14 When clinically appropriate and hemodynamically tolerated, a recruitment maneuver may then be performed, followed by stepwise PEEP titration using best respiratory compliance, lowest driving pressure, and/or oxygenation response to identify candidate PEEP levels for subsequent validation.
Step 2: Initial PEEP Screening Using Mechanical Indices
A brief PEEP trial, often performed as a decremental or stepwise titration, can be used to identify a mechanically favorable PEEP range. Driving pressure (ΔP) minimization and/or maximal compliance are typical selection criteria.32 In a pragmatic bedside procedure, after stabilization under baseline lung-protective ventilation and, when appropriate, after a recruitment maneuver, clinicians may test a limited number of PEEP levels using small stepwise changes, such as 2 to 3 cmH2O increments or decrements, to reduce workflow burden.49 At each PEEP level, airway pressures and respiratory mechanics should be allowed to stabilize briefly, after which plateau pressure, driving pressure, static or dynamic compliance, oxygenation, and basic hemodynamic variables should be recorded. PEEP levels associated with plateau pressure ≥30 cmH2O, increased driving pressure, reduced compliance, impaired oxygenation, sustained MAP reduction, increased vasopressor requirement, or signs of RV strain should be excluded. The mechanically favorable range is then defined as the level or narrow range associated with the lowest driving pressure, the highest compliance, or both, while remaining within these respiratory and hemodynamic safety limits. This step yields one or two candidate PEEP levels rather than a final decision, which should subsequently undergo imaging-based validation and hemodynamic safety assessment.
Step 3: Imaging-Based Validation and Fine-Tuning
Among mechanically acceptable candidates, regional imaging is used to verify that the chosen PEEP produces meaningful dependent recruitment and does not induce nondependent overdistension. With LUS, improvements in dependent aeration scores and reduction of consolidation patterns support recruitment. With EIT, the target is a regional ventilation distribution that minimizes collapse while limiting overdistension, often conceptualized as a “best compromise” point. Oxygenation should be assessed concurrently as a functional endpoint, including SpO2, FiO2 requirement, and PaO2/FiO2 when arterial blood gas data are available. If oxygenation remains difficult to maintain despite mechanically acceptable PEEP, clinicians should reassess for residual atelectasis, ventilation–perfusion mismatch, airway obstruction, position- or pneumoperitoneum-related derecruitment, and hemodynamic impairment. When imaging suggests persistent recruitable collapse without overdistension, PEEP may be cautiously increased within predefined mechanical and hemodynamic safety limits. Imaging thus refines PEEP selection by ensuring that global mechanical optimization aligns with regional lung protection and clinically adequate oxygenation.50,51
Step 4: Final Decision Under a Hemodynamic “Brake” Mechanism
The final PEEP should satisfy hemodynamic tolerance criteria. If imaging and mechanics suggest higher PEEP but hemodynamics deteriorate (eg, sustained MAP reduction, rising vasopressor requirement, signs of RV strain), the PEEP should be reduced to the highest level that remains hemodynamically acceptable In older patients, this safety step is decisive: a slightly less recruited lung may be preferable to clinically significant circulatory compromise. This step also emphasizes reassessment, as hemodynamic tolerance may change with anesthetic depth, fluid shifts, and surgical phase.52,53
This four-step process is schematically illustrated in Figure 2, which summarizes the clinical workflow and the decision points at which each dimension of the framework is applied.
 |
Figure 2 Three-dimensional PEEP titration framework and clinical workflow. |
Adaptations for Special Perioperative Scenarios
Laparoscopic Surgery and Trendelenburg Positioning
Pneumoperitoneum and Trendelenburg positioning increase pleural pressure and promote dependent collapse, often shifting the mechanically optimal PEEP upward. However, these same conditions may also increase intrathoracic pressure transmission and worsen venous return. In this context, the framework emphasizes repeated reassessment after pneumoperitoneum establishment and major positional changes, with imaging used to confirm recruitment and hemodynamics used to prevent excessive circulatory burden.54
Obesity in Older Adults
Obesity increases chest wall elastance and intra-abdominal pressure, making airway pressure a poor proxy for transpulmonary pressure. Older obese patients may therefore require higher airway PEEP to achieve adequate transpulmonary end-expiratory pressure, but they are simultaneously at high risk of hemodynamic compromise.55 When available, transpulmonary pressure guidance or imaging-based validation becomes particularly valuable, while hemodynamic thresholds should be applied conservatively.
Cardiothoracic Surgery
Cardiothoracic surgery represents another high-risk scenario in which perioperative ventilatory management is closely related to postoperative pulmonary outcomes. In thoracic surgery, particularly during one-lung ventilation, regional ventilation heterogeneity may increase the competing risks of dependent atelectasis and overdistension of the ventilated lung. Although protective ventilation with low tidal volume and PEEP has been shown to reduce major postoperative complications after lung cancer surgery,56 the PROTHOR trial found that a higher PEEP strategy combined with recruitment maneuvers during one-lung ventilation did not reduce postoperative pulmonary complications compared with lower PEEP.57 Similarly, in on-pump cardiac surgery, the PROVECS trial showed that an open-lung strategy incorporating higher PEEP, recruitment maneuvers, and ventilation during cardiopulmonary bypass did not significantly reduce postoperative pulmonary complications and required more frequent intraoperative adjustments due to arterial hypotension or surgical requirements.58 These findings suggest that older cardiothoracic patients may require cautious, individualized PEEP adjustment based on driving pressure, regional aeration when available, oxygenation response, and hemodynamic tolerance rather than routine use of fixed high-pressure strategies.
Older Patients with Compromised Lung Function or Prior Lung Resection
In older patients with impaired baseline lung function, such as emphysema or COPD, PEEP should be adjusted cautiously because airflow limitation, dynamic hyperinflation, and intrinsic PEEP may increase the risk of overdistension, air trapping, and hemodynamic compromise.59,60 External PEEP should therefore be titrated in small increments, with close attention to expiratory flow limitation, auto-PEEP, plateau pressure, driving pressure, oxygenation response, and circulatory tolerance.61 In patients with a history of pulmonary lobectomy or other lung resection, reduced lung volume and limited pulmonary reserve may further narrow the safe PEEP range; thus, low tidal volume ventilation, conservative PEEP escalation, imaging-based confirmation of recruitable atelectasis, and strict mechanical and hemodynamic safety limits are particularly important.62
Evidence Linking Individualized PEEP to PPCs and Functional Recovery
Specific PPCs Addressed and Their Mechanistic Links to PEEP
In this review, PPCs mainly refer to postoperative atelectasis, hypoxemia, pneumonia, respiratory failure, and the need for unplanned postoperative respiratory support, while broader composite definitions may also include bronchospasm and pleural effusion.29 Among these complications, atelectasis and hypoxemia are the most directly related to perioperative PEEP. Insufficient PEEP may promote end-expiratory airway closure, dependent alveolar collapse, ventilation–perfusion mismatch, and cyclic recruitment–derecruitment, whereas appropriately titrated PEEP may preserve end-expiratory lung volume and stabilize recruitable lung units. However, excessive PEEP may cause regional overdistension, increase driving pressure, impair pulmonary perfusion, or reduce venous return and cardiac output, thereby offsetting potential pulmonary benefits. This interpretation is supported by evidence showing that perioperative atelectasis can contribute to gas-exchange impairment, pneumonia, and postoperative respiratory insufficiency,1 while high PEEP combined with recruitment maneuvers has not consistently reduced PPCs and may increase intraoperative hypotension or vasoactive drug use.14 In addition, increased driving pressure during intraoperative ventilation is associated with a higher risk of PPCs, suggesting that PEEP titration should avoid increasing global lung stress even when oxygenation improves.35
Pneumonia, respiratory failure, and unplanned postoperative respiratory support are more distal PPCs. They may arise from persistent atelectasis, impaired secretion clearance, hypoxemia, or increased work of breathing, particularly in older patients with reduced cough efficiency, impaired mucociliary clearance, opioid-related hypoventilation, pain-limited deep breathing, and delayed mobilization. Bronchospasm and pleural effusion are clinically relevant components of some PPC definitions, but their relationship with intraoperative PEEP is less direct and may be more strongly influenced by airway reactivity, fluid balance, cardiac function, or pre-existing pulmonary disease. Therefore, when interpreting evidence on individualized PEEP, atelectasis and hypoxemia should be regarded as the most immediate PEEP-sensitive outcomes, whereas pneumonia, respiratory failure, and postoperative respiratory support represent downstream outcomes influenced by both intraoperative ventilation and postoperative care. This distinction may partly explain why individualized or high-PEEP strategies improve intraoperative physiology in some studies but do not always translate into consistent reductions in composite PPC endpoints.63,64
Evidence Stratified by PEEP Titration Strategy
An expanding body of perioperative literature has explored individualized PEEP strategies using different physiological targets and titration modalities. Although study designs and endpoints vary, most approaches demonstrate superior physiological optimization compared with fixed PEEP strategies, with emerging—though heterogeneous—signals of benefit for PPCs and early recovery, particularly in high-risk and older patients.64
Lung Ultrasound–Guided PEEP
Lung ultrasound (LUS)–guided approaches rely on semiquantitative aeration scores or reaeration patterns to detect dependent atelectasis and guide PEEP adjustments. Perioperative studies consistently show that LUS-guided PEEP improves lung aeration and reduces radiographic or ultrasound-defined atelectasis compared with conventional ventilation.41,50 In older patients, this strategy is especially relevant because dependent collapse is common and often poorly captured by global mechanics. While most studies emphasize physiological endpoints, some report reductions in early PPCs or surrogate markers of impaired recovery, suggesting potential clinical relevance.34
Electrical Impedance Tomography (EIT)-Guided PEEP
EIT enables continuous, bedside visualization of regional ventilation distribution and allows identification of PEEP levels that best balance alveolar collapse and overdistension. Surgical studies employing EIT-guided titration demonstrate improved ventilation homogeneity and reduced regional overdistension compared with fixed PEEP strategies. Given the pronounced ventilation heterogeneity observed in older lungs, EIT offers a mechanistically appealing tool.65 However, evidence linking EIT-guided PEEP to reductions in PPCs or improvements in functional recovery remains limited, partly due to small sample sizes and variability in outcome definitions.
Transpulmonary Pressure-Guided Strategies
Titration based on transpulmonary pressure aims to maintain a positive end-expiratory transpulmonary pressure to prevent collapse while avoiding excessive lung stress. This approach is particularly relevant in patients with altered chest wall mechanics, including obese older adults. Perioperative trials have shown improved oxygenation and reduced atelectasis compared with airway pressure-based strategies, but effects on PPCs are inconsistent.66,67 Practical limitations, including the need for esophageal pressure monitoring and uncertainty regarding optimal targets in older patients, have constrained widespread adoption.
Driving Pressure-Guided Strategies
Driving pressure (ΔP) has emerged as a robust global marker of lung stress and a predictor of postoperative pulmonary outcomes. Strategies targeting ΔP minimization often result in improved compliance and reduced mechanical strain. In older patients, ΔP-guided titration is attractive due to its simplicity and bedside feasibility.35,40 However, ΔP reflects global respiratory mechanics and may fail to detect persistent dependent collapse or emerging nondependent overdistension, limiting its reliability when used as a sole decision criterion.
Compliance-Based Titration
Compliance-guided PEEP selection remains one of the most commonly applied individualized approaches. Improvements in static or dynamic compliance are typically interpreted as evidence of recruitment. While this strategy frequently improves oxygenation and global mechanics, its impact on PPCs has been inconsistent. In older patients with heterogeneous lung units, increases in compliance may reflect overdistension of already open regions rather than true recruitment, underscoring the limitations of compliance as a standalone guide.63 Across these modalities, individualized PEEP strategies consistently improve intraoperative physiological parameters compared with fixed approaches. However, translation into consistent reductions in PPCs or improvements in functional recovery has been variable, suggesting that physiological optimization alone is insufficient unless aligned with patient-specific tolerance and perioperative context.
Why Have Study Results Been Inconsistent?
Several factors help explain the heterogeneity of findings across studies evaluating individualized PEEP, particularly in older surgical populations.First, differences in titration methods and timing play a critical role. Some studies perform PEEP titration only once after induction, whereas others reassess after changes in position, pneumoperitoneum, or surgical phase.68 Given the dynamic nature of lung mechanics during surgery-especially in older adults with limited reserve-single-time-point titration may fail to maintain optimal conditions throughout the perioperative period.
Second, variation in perioperative co-interventions complicates interpretation. Fluid management, vasopressor use, recruitment maneuvers, analgesic strategies, and postoperative respiratory care all interact with PEEP effects. Differences in these co-interventions can attenuate or exaggerate the apparent benefits of individualized PEEP, making it difficult to isolate the contribution of the titration strategy itself.69 Third, heterogeneity among older patients is often underestimated. Chronological age alone does not capture physiological vulnerability. Frailty, baseline functional status, cardiac reserve, and pre-existing pulmonary disease substantially influence tolerance to PEEP and susceptibility to PPCs. Trials that treat older adults as a homogeneous group may therefore dilute benefits in high-risk subgroups while exposing others to unnecessary hemodynamic risk.70 Finally, outcome selection contributes to apparent inconsistency. Many studies prioritize short-term physiological endpoints, such as oxygenation or compliance, rather than clinically meaningful outcomes including PPCs, length of stay, or postoperative functional recovery. Because PPCs and delayed recovery reflect cumulative perioperative insults, modest intraoperative physiological improvements may not translate into detectable clinical benefits unless embedded within a broader, integrative strategy.71
Taken together, these considerations suggest that divergent results across individualized PEEP studies are not contradictory but reflect differences in physiological targets, timing, patient selection, and contextual factors. As schematically illustrated in Figure 3, existing titration strategies predominantly optimize isolated dimensions-global lung stress, regional aeration, or circulatory safety—without fully integrating their competing effects. This evidence synthesis underscores the need for multidimensional approaches capable of aligning physiological optimization with patient-specific tolerance to improve PPCs and functional recovery in older surgical patients.
 |
Figure 3 Evidence map linking individualized PEEP strategies to physiological outcomes, PPCs, and functional recovery. |
Clinical Translation and Future Research Directions
Implementable Clinical Pathways
For individualized perioperative PEEP to move from physiological concept to routine practice in older patients, implementation must be workflow-compatible, reproducible, and auditable A feasible pathway begins with standardized bedside steps embedded into existing anesthesia routines rather than adding complex protocols that depend on expert operators.72 In practice, this requires a structured checklist covering (i) baseline lung-protective ventilation settings, (ii) the trigger points for reassessment (eg, after induction, after major positioning, after pneumoperitoneum, and before emergence), (iii) the titration method selected for that case (mechanics-only vs imaging-assisted), and (iv) predefined stopping rules based on respiratory and hemodynamic safety boundaries.73 Importantly, the pathway should explicitly document the final selected PEEP and the physiological rationale supporting it (eg, lowest ΔP within safety constraints; LUS-confirmed recruitment without overdistension; hemodynamic tolerance maintained).
More specifically, the pathway should begin with a baseline lung-protective ventilation bundle after induction of anesthesia. This may include low tidal volume ventilation, typically 6–8 mL/kg predicted body weight, together with an initial modest PEEP of approximately 5 cmH2O, rather than routine application of uniformly high PEEP. Respiratory rate should be adjusted according to end-tidal CO2 or arterial blood gas analysis to maintain adequate ventilation, while plateau pressure, driving pressure, and respiratory compliance should be monitored to avoid excessive global lung stress.14,48 Inspired oxygen concentration should also be titrated according to oxygenation requirements rather than fixed at a high level. In general, FiO2 should be adjusted to maintain clinically acceptable oxygenation according to the patient’s baseline pulmonary status, while avoiding unnecessary prolonged exposure to very high FiO2.74 Persistent oxygenation deterioration or an increasing FiO2 requirement should prompt reassessment rather than simple escalation of oxygen delivery. Reassessment should be both time-based and event-triggered. In addition to predefined time points such as after induction, after major positional changes, after pneumoperitoneum establishment, and before emergence, ventilation and PEEP settings should be re-evaluated when intraoperative oxygenation deteriorates, FiO2 requirement increases, respiratory compliance decreases, plateau pressure or driving pressure rises, or hemodynamic instability develops, including sustained mean arterial pressure reduction or escalating vasopressor requirement.14,35,48
To reduce variability and facilitate adoption, a documentation template is essential. At minimum, the record should capture: tidal volume per predicted body weight; plateau pressure, PEEP, and driving pressure at baseline and after titration; oxygenation and ventilation indices; and hemodynamic variables (mean arterial pressure, vasopressor dose, and if available, cardiac output surrogates). When imaging is used, a brief categorical result (eg, LUS aeration improvement; EIT collapse–overdistension balance point) should be documented rather than extensive narrative.75 Such templates support both clinical decision-making and later quality review.
At the departmental level, translation requires quality control indicators that reflect both fidelity to the process and patient safety. Process metrics may include the proportion of eligible older patients receiving protocolized reassessment at predefined time points, completion of documentation fields, and adherence to plateau pressure and driving pressure thresholds. Outcome metrics should include PPC incidence, unplanned postoperative respiratory support, and hemodynamic adverse events such as sustained intraoperative hypotension or high vasopressor exposure. Because older patients are sensitive to systemic effects of hypotension, integrating safety metrics into quality dashboards is critical to prevent unintended harm from aggressive PEEP escalation.
Perioperative Continuity of Care
A key limitation of many intraoperative ventilation strategies is that their effects can be transient if postoperative care does not preserve lung recruitment. In older adults, derecruitment can occur rapidly after extubation due to residual anesthetic effects, pain-related hypoventilation, impaired cough, and reduced mobility. Therefore, individualized PEEP should be conceptualized as part of a continuum of perioperative respiratory support, extending beyond the operating room into the post-anesthesia care unit (PACU) and ward.76
In the PACU, the priority is to maintain adequate lung aeration while minimizing sedation and enabling effective ventilation. Practical measures include early assessment for residual atelectasis risk (eg, clinical signs, oxygen requirement, or bedside LUS where available), timely initiation of noninvasive respiratory support when indicated, and avoidance of prolonged supine immobility. For high-risk older patients, short-term application of CPAP or high-flow nasal oxygen may help preserve recruitment achieved intraoperatively.77 Pain control strategies should be optimized to support deep breathing and early mobilization while minimizing excessive opioid exposure that can suppress respiratory drive.
On the ward, preventing recurrent collapse depends on reinforcing physiologic “anti-atelectasis”behaviors-early ambulation, incentive spirometry where appropriate, head-of-bed elevation, and structured respiratory physiotherapy-together with targeted monitoring for early signs of PPCs. For older patients, perioperative respiratory continuity should be aligned with broader recovery pathways, such as enhanced recovery protocols, because mobilization and feeding interact with respiratory mechanics and overall functional recovery. Conceptually, the intraoperative three-dimensional titration framework provides a starting point, but sustained benefit likely requires postoperative strategies that prevent re-collapse and preserve functional reserve.78
Research Gaps and Future Directions
Despite increasing physiological evidence supporting individualized PEEP, several gaps limit confident translation into older-patient–centered outcomes. First, there is a need for randomized controlled trials stratified by frailty and cardiac function, rather than chronological age alone. Frailty captures reduced physiologic resilience and may identify older patients most likely to benefit from recruitment-focused strategies, while cardiac function stratification may identify those most vulnerable to hemodynamic harm.79 Such stratification would reduce dilution of treatment effects and improve safety.
Second, future studies should adopt harmonized outcome sets that integrate pulmonary morbidity with recovery and safety. PPCs remain essential, but older-patient–relevant endpoints should also include functional recovery measures (time to ambulation, discharge readiness, length of stay, postoperative mobility trajectories) and safety endpoints (hypotension burden, vasopressor exposure, markers of right ventricular strain). Without standardized outcome reporting, comparisons across studies remain difficult and meta-analytic synthesis remains limited.80
Third, there is a major methodological need for head-to-head comparisons between the three-dimensional framework and single-modality titration strategies. While driving pressure-guided, LUS-guided, and EIT-guided approaches each offer value, their isolated use may not address the competing risks that define the narrow PEEP therapeutic window in older adults.38 Trials that directly test integrative frameworks against single-parameter strategies-while controlling for co-interventions and ensuring postoperative continuity-would provide the most informative evidence for clinical adoption.
Finally, implementation science questions remain underexplored: which settings (high-risk surgical services, PACU protocols, ICUs) derive the greatest benefit, what training level is needed for imaging-based titration, and how workflow constraints influence adherence.81 Addressing these pragmatic considerations will be essential for moving individualized PEEP from expert centers to broader perioperative practice.
Conclusions and Perspectives
Optimal perioperative PEEP in older patients, generally referring to adults aged 65 years or above, cannot be defined as a fixed value or a uniform protocol. Instead, it represents a dynamic and individualized balance shaped by age-related changes in lung structure, ventilation heterogeneity, reduced cardiovascular reserve, frailty, comorbidity burden, and evolving intraoperative conditions such as positioning, pneumoperitoneum, surgical type, and anesthetic depth. These factors collectively narrow the therapeutic window within which PEEP may prevent atelectasis and cyclic derecruitment while avoiding regional overdistension and hemodynamic compromise. Therefore, approaches that apply identical airway pressures across heterogeneous older populations are unlikely to achieve consistent clinical benefit.
The clinical relevance of individualized PEEP lies in its potential association with specific postoperative pulmonary complications, including atelectasis, hypoxemia, pneumonia, respiratory failure, and the need for unplanned postoperative respiratory support. Insufficient PEEP may promote airway closure, dependent alveolar collapse, ventilation–perfusion mismatch, and persistent postoperative atelectasis, whereas excessive PEEP may increase driving pressure, impair pulmonary perfusion, reduce venous return, aggravate right ventricular loading, and increase vasopressor requirements. Thus, perioperative PEEP management in older patients should not focus solely on oxygenation or recruitment, but should simultaneously consider global lung stress, regional aeration, and circulatory tolerance.
The three-dimensional PEEP titration framework proposed in this review offers a pragmatic pathway to address this complexity. By integrating mechanical screening based on driving pressure and compliance, imaging-based validation using lung ultrasound or electrical impedance tomography when available, and hemodynamic tolerance as a non-negotiable safety constraint, this framework aligns physiological optimization with clinical feasibility. Importantly, its value lies not in replacing clinical judgment or relying on a single technology, but in providing a structured, reproducible, and teachable approach for integrating key physiological signals into perioperative decision-making.
Looking forward, the value of individualized PEEP should be judged not only by improvements in intraoperative oxygenation or respiratory mechanics, but also by its ability to reduce clearly defined PPCs, preserve functional reserve, and support timely recovery in older adults. Future studies should validate this multidimensional framework in well-designed, stratified clinical trials that account for frailty, cardiopulmonary reserve, surgical risk, and perioperative care pathways. Outcomes should include PPC incidence, unplanned postoperative respiratory support, hemodynamic adverse events, length of stay, and functional recovery. With further validation and thoughtful integration into perioperative workflows, individualized PEEP guided by a three-dimensional titration strategy may help improve respiratory safety and recovery-oriented outcomes in the growing population of older surgical patients.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author Weifeng Yao upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Guangdong Provincial Foundation and Applied Basic Research Fund (2025A1515012585, 2026A1515012759, 2024A1515220097) and the National Natural Science Foundation of China (82372193, 82572513).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Lagier D, Zeng C, Fernandez-Bustamante A, Vidal Melo MF. Perioperative pulmonary atelectasis: Part II. Clinical implications. Anesthesiology. 2022;136(1):206–19. doi:10.1097/ALN.0000000000004009
2. Wysham WZ, Kim KH, Roberts JM, et al. Obesity and perioperative pulmonary complications in robotic gynecologic surgery. Am J Obstet Gynecol. 2015;213(1):33.e31–33.e37. doi:10.1016/j.ajog.2015.01.033
3. Wang SH, Wang Y, Li SY, et al. Effect of individualized PEEP titrated by EIT on postoperative atelectasis in children undergoing laparoscopy: a randomized controlled trial. Int J Med Sci. 2025;22(12):3007–3013. doi:10.7150/ijms.112280
4. Liu T, Huang J, Wang X, Tu J, Wang Y, Xie C. Effect of recruitment manoeuvres under lung ultrasound-guidance and positive end-expiratory pressure on postoperative atelectasis and hypoxemia in major open upper abdominal surgery: a randomized controlled trial. Heliyon. 2023;9(2):e13348. doi:10.1016/j.heliyon.2023.e13348
5. Neuman MD, Feng R, Carson JL, et al. Spinal anesthesia or general anesthesia for hip surgery in older adults. N Engl J Med. 2021;385(22):2025–2035. doi:10.1056/NEJMoa2113514
6. Bernhard W. Lung surfactant: function and composition in the context of development and respiratory physiology. Ann Anat. 2016;208:146–150. doi:10.1016/j.aanat.2016.08.003
7. Pérez J, Dorado JH, Accoce M, Plotnikow GA. Airway and transpulmonary driving pressure by end-inspiratory holds during pressure support ventilation. Respir Care. 2023;68(11):1483–1492. doi:10.4187/respcare.10802
8. Rahaman U. Mathematics of Ventilator-induced Lung Injury. Indian J Crit Care Med. 2017;21(8):521–524. doi:10.4103/ijccm.IJCCM_411_16
9. Canet J, Gallart L, Gomar C, et al. Prediction of postoperative pulmonary complications in a population-based surgical cohort. Anesthesiology. 2010;113(6):1338–1350. doi:10.1097/ALN.0b013e3181fc6e0a
10. Reinius H, Jonsson L, Gustafsson S, et al. Prevention of atelectasis in morbidly obese patients during general anesthesia and paralysis: a computerized tomography study. Anesthesiology. 2009;111(5):979–987. doi:10.1097/ALN.0b013e3181b87edb
11. Tusman G, Böhm SH. Prevention and reversal of lung collapse during the intra-operative period. Best Pract Res Clin Anaesthesiol. 2010;24(2):183–197. doi:10.1016/j.bpa.2010.02.006
12. Mead J, Takishima T, Leith D. Stress distribution in lungs: a model of pulmonary elasticity. J Appl Physiol. 1970;28(5):596–608. doi:10.1152/jappl.1970.28.5.596
13. Gattinoni L, Tonetti T, Cressoni M, et al. Ventilator-related causes of lung injury: the mechanical power. Intensive Care Med. 2016;42(10):1567–1575. doi:10.1007/s00134-016-4505-2
14. Anaesthesiology P, Hemmes SN, Gama de Abreu M, Pelosi P, Schultz MJ. High versus low positive end-expiratory pressure during general anaesthesia for open abdominal surgery (PROVHILO trial): a multicentre randomised controlled trial. Lancet. 2014;384(9942):495–503.
15. Gattinoni L, Giosa L, Bonifazi M, et al. Targeting transpulmonary pressure to prevent ventilator-induced lung injury. Expert Rev Respir Med. 2019;13(8):737–746. doi:10.1080/17476348.2019.1638767
16. Runck H, Schumann S, Tacke S, Haberstroh J, Guttmann J. Effects of intra-abdominal pressure on respiratory system mechanics in mechanically ventilated rats. Respir Physiol Neurobiol. 2012;180(2–3):204–210. doi:10.1016/j.resp.2011.11.007
17. Mahmood SS, Pinsky MR. Heart-lung interactions during mechanical ventilation: the basics. Ann Transl Med. 2018;6(18):349. doi:10.21037/atm.2018.04.29
18. Sella N, Pettenuzzo T, Zarantonello F, et al. Electrical impedance tomography: a compass for the safe route to optimal PEEP. Respir Med. 2021;187:106555. doi:10.1016/j.rmed.2021.106555
19. Grieco DL, Chen L, Brochard L. Transpulmonary pressure: importance and limits. Ann Transl Med. 2017;5(14):285. doi:10.21037/atm.2017.07.22
20. Somhorst P, Mousa A, Jonkman AH. Setting positive end-expiratory pressure: the use of esophageal pressure measurements. Curr Opin Crit Care. 2024;30(1):28–34. doi:10.1097/MCC.0000000000001120
21. Deng BY, Li N, Wu WS, et al. Use of neonatal lung ultrasound for the early detection of pneumothorax. Am J Perinatol. 2020;37(9):907–913. doi:10.1055/s-0039-1688999
22. Hedenstierna G, Edmark L. The effects of anesthesia and muscle paralysis on the respiratory system. Intensive Care Med. 2005;31(10):1327–1335. doi:10.1007/s00134-005-2761-7
23. Amato MB, Meade MO, Slutsky AS, et al. Driving pressure and survival in the acute respiratory distress syndrome. N Engl J Med. 2015;372(8):747–755. doi:10.1056/NEJMsa1410639
24. Leblanc P, Ruff F, Milic-Emili J. Effects of age and body position on “airway closure” in man. J Appl Physiol. 1970;28(4):448–451. doi:10.1152/jappl.1970.28.4.448
25. Sharma G, Goodwin J. Effect of aging on respiratory system physiology and immunology. Clin Interv Aging. 2006;1(3):253–260. doi:10.2147/ciia.2006.1.3.253
26. Janssens JP, Pache JC, Nicod LP. Physiological changes in respiratory function associated with ageing. Eur Respir J. 1999;13(1):197–205. doi:10.1183/09031936.99.14614549
27. Gattinoni L, Quintel M, Marini JJ. Volutrauma and atelectrauma: which is worse? Crit Care. 2018;22(1):264. doi:10.1186/s13054-018-2199-2
28. Davis MP, DiScala S, Davis A. Respiratory depression associated with opioids: a narrative review. Curr Treat Options Oncol. 2024;25(11):1438–1450. doi:10.1007/s11864-024-01274-5
29. Miskovic A, Lumb AB. Postoperative pulmonary complications. Br J Anaesth. 2017;118(3):317–334. doi:10.1093/bja/aex002
30. Pinsky MR. Cardiopulmonary interactions: physiologic basis and clinical applications. Ann Am Thorac Soc. 2018;15(Suppl 1):S45–s48. doi:10.1513/AnnalsATS.201704-339FR
31. Lakatta EG, Levy D. Arterial and cardiac aging: major shareholders in cardiovascular disease enterprises: part I: aging arteries: a “set up” for vascular disease. Circulation. 2003;107(1):139–146. doi:10.1161/01.CIR.0000048892.83521.58
32. Gattinoni L, Caironi P, Cressoni M, et al. Lung recruitment in patients with the acute respiratory distress syndrome. N Engl J Med. 2006;354(17):1775–1786. doi:10.1056/NEJMoa052052
33. Slutsky AS, Ranieri VM. Ventilator-induced lung injury. N Engl J Med. 2013;369(22):2126–2136. doi:10.1056/NEJMra1208707
34. Feng D, Zhao Y, Wu Z, et al. Ultrasound guided individualized PEEP reduces postoperative atelectasis in elderly patients undergoing laparoscopic radical rectal cancer surgery. Sci Rep. 2025;15(1):39585. doi:10.1038/s41598-025-17862-w
35. Neto AS, Hemmes SN, Barbas CS, et al. Association between driving pressure and development of postoperative pulmonary complications in patients undergoing mechanical ventilation for general anaesthesia: a meta-analysis of individual patient data. Lancet Respir Med. 2016;4(4):272–280. doi:10.1016/S2213-2600(16)00057-6
36. Vieillard-Baron A, Matthay M, Teboul JL, et al. Experts’ opinion on management of hemodynamics in ARDS patients: focus on the effects of mechanical ventilation. Intensive Care Med. 2016;42(5):739–749. doi:10.1007/s00134-016-4326-3
37. Vistisen ST, Enevoldsen JN, Greisen J, Juhl-Olsen P. What the anaesthesiologist needs to know about heart-lung interactions. Best Pract Res Clin Anaesthesiol. 2019;33(2):165–177. doi:10.1016/j.bpa.2019.05.003
38. Tsumura H, Harris E, Brandon D, Pan W, Vacchiano C. Review of the mechanisms of ventilator induced lung injury and the principles of intraoperative lung protective ventilation. Aana J. 2021;89(3):227–233.
39. Cylwik J, Buda N. Lung ultrasonography in the monitoring of intraoperative recruitment maneuvers. Diagnostics. 2021;11(2):276. doi:10.3390/diagnostics11020276
40. Gattinoni L, Tonetti T, Quintel M. Intensive care medicine in 2050: ventilator-induced lung injury. Intensive Care Med. 2018;44(1):76–78. doi:10.1007/s00134-017-4770-8
41. Bouhemad B, Brisson H, Le-Guen M, Arbelot C, Lu Q, Rouby JJ. Bedside ultrasound assessment of positive end-expiratory pressure-induced lung recruitment. Am J Respir Crit Care Med. 2011;183(3):341–347. doi:10.1164/rccm.201003-0369OC
42. Volpicelli G, Elbarbary M, Blaivas M, et al. International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012;38(4):577–591. doi:10.1007/s00134-012-2513-4
43. Frerichs I, Amato MB, van Kaam AH, et al. Chest electrical impedance tomography examination, data analysis, terminology, clinical use and recommendations: consensus statement of the TRanslational EIT developmeNt stuDy group. Thorax. 2017;72(1):83–93. doi:10.1136/thoraxjnl-2016-208357
44. Pinsky MR. Why knowing the effects of positive-pressure ventilation on venous, pleural, and pericardial pressures is important to the bedside clinician?*. Crit Care Med. 2014;42(9):2129–2131. doi:10.1097/CCM.0000000000000364
45. Chang HY, Cheng KS, Lung HL, et al. Hemodynamic effects of nasal intermittent positive pressure ventilation in preterm infants. Medicine. 2016;95(6):e2780. doi:10.1097/MD.0000000000002780
46. Gali B, Goyal DG. Positive pressure mechanical ventilation. Emerg Med Clin North Am. 2003;21(2):453–473. doi:10.1016/S0733-8627(03)00006-3
47. Ladha KS, Bateman BT, Houle TT, et al. Variability in the use of protective mechanical ventilation during general anesthesia. Anesth Analg. 2018;126(2):503–512. doi:10.1213/ANE.0000000000002343
48. Young CC, Harris EM, Vacchiano C, et al. Lung-protective ventilation for the surgical patient: international expert panel-based consensus recommendations. Br J Anaesth. 2019;123(6):898–913. doi:10.1016/j.bja.2019.08.017
49. Saguil A, Fargo MV. Acute respiratory distress syndrome: diagnosis and management. Am Fam Physician. 2020;101(12):730–738.
50. Mojoli F, Bouhemad B, Mongodi S, Lichtenstein D. Lung ultrasound for critically ill patients. Am J Respir Crit Care Med. 2019;199(6):701–714. doi:10.1164/rccm.201802-0236CI
51. Songsangvorn N, Xu Y, Lu C, et al. Electrical impedance tomography-guided positive end-expiratory pressure titration in ARDS: a systematic review and meta-analysis. Intensive Care Med. 2024;50(5):617–631. doi:10.1007/s00134-024-07362-2
52. Joseph A, Petit M, Vieillard-Baron A. Hemodynamic effects of positive end-expiratory pressure. Curr Opin Crit Care. 2024;30(1):10–19. doi:10.1097/MCC.0000000000001124
53. Delle Femine FC, D’Arienzo D, Liccardo B, et al. Echocardiography in the ventilated patient: what the clinician has to know. J Clin Med. 2024;14(1):77. doi:10.3390/jcm14010077
54. Bigatello L, Pesenti A. Respiratory physiology for the anesthesiologist. Anesthesiology. 2019;130(6):1064–1077. doi:10.1097/ALN.0000000000002666
55. Pelosi P, Croci M, Ravagnan I, et al. The effects of body mass on lung volumes, respiratory mechanics, and gas exchange during general anesthesia. Anesth Analg. 1998;87(3):654–660. doi:10.1213/00000539-199809000-00031
56. Marret E, Cinotti R, Berard L, et al. Protective ventilation during anaesthesia reduces major postoperative complications after lung cancer surgery: a double-blind randomised controlled trial. Eur J Anaesthesiol. 2018;35(10):727–735. doi:10.1097/EJA.0000000000000804
57. Writing C, Steering C, Group PC. Anaesthesiology PRVNftCTNotESo, Intensive C. Effects of intraoperative higher versus lower positive end-expiratory pressure during one-lung ventilation for thoracic surgery on postoperative pulmonary complications (PROTHOR): a multicentre, international, randomised, controlled, Phase 3 trial. Lancet Respir Med. 2026;14(1):17–28.
58. Lagier D, Fischer F, Fornier W, et al. Effect of open-lung vs conventional perioperative ventilation strategies on postoperative pulmonary complications after on-pump cardiac surgery: the PROVECS randomized clinical trial. Intensive Care Med. 2019;45(10):1401–1412. doi:10.1007/s00134-019-05741-8
59. Jubran A. Setting positive end-expiratory pressure in the severely obstructive patient. Curr Opin Crit Care. 2024;30(1):89–96. doi:10.1097/MCC.0000000000001131
60. Roesthuis LH, van der Hoeven JG, Guerin C, Doorduin J, Heunks LMA. Three bedside techniques to quantify dynamic pulmonary hyperinflation in mechanically ventilated patients with chronic obstructive pulmonary disease. Ann Intensive Care. 2021;11(1):167. doi:10.1186/s13613-021-00948-9
61. Luo LF, Lin YM, Liu Y, et al. Effect of individualized PEEP titration by ultrasonography on perioperative pulmonary protection and postoperative cognitive function in patients with chronic obstructive pulmonary disease. BMC Pulm Med. 2023;23(1):232. doi:10.1186/s12890-023-02471-y
62. Park M, Yoon S, Nam JS, et al. Driving pressure-guided ventilation and postoperative pulmonary complications in thoracic surgery: a multicentre randomised clinical trial. Br J Anaesth. 2023;130(1):e106–e118. doi:10.1016/j.bja.2022.06.037
63. Ferrando C, Soro M, Unzueta C, et al. Individualised perioperative open-lung approach versus standard protective ventilation in abdominal surgery (iPROVE): a randomised controlled trial. Lancet Respir Med. 2018;6(3):193–203. doi:10.1016/S2213-2600(18)30024-9
64. Writing Committee for the PCGotPVNftCTNotESoA, Bluth T, Serpa Neto A, et al. Effect of Intraoperative High Positive End-Expiratory Pressure (PEEP) With Recruitment Maneuvers vs Low PEEP on Postoperative Pulmonary Complications in Obese Patients: a Randomized Clinical Trial. JAMA. 2019;321(23):2292–2305. doi:10.1001/jama.2019.7505
65. Brabant OA, Byrne DP, Sacks M, et al. Thoracic electrical impedance tomography–The 2022 Veterinary Consensus Statement. Front Vet Sci. 2022;9:946911. doi:10.3389/fvets.2022.946911
66. Yoshida T, Brochard L. Esophageal pressure monitoring: why, when and how? Curr Opin Crit Care. 2018;24(3):216–222. doi:10.1097/MCC.0000000000000494
67. Bazurro S, Ball L, Pelosi P. Perioperative management of obese patient. Curr Opin Crit Care. 2018;24(6):560–567. doi:10.1097/MCC.0000000000000555
68. Denny JT, Mungekar SS, Landgraf BR, et al. An unusual cause of failure to ventilate. J Investig Med High Impact Case Rep. 2018;6:2324709618781174. doi:10.1177/2324709618781174
69. Anselmi A, Verhoye JP. Prevention of postoperative pulmonary complications and aggregation of marginal gains. J Thorac Cardiovasc Surg. 2017;153(3):735–736. doi:10.1016/j.jtcvs.2016.10.049
70. Verwijmeren L, Noordzij PG, Daeter EJ, et al. Preoperative frailty and one-year functional recovery in elderly cardiac surgery patients. J Thorac Cardiovasc Surg. 2023;166(3):870–878.e876. doi:10.1016/j.jtcvs.2022.01.032
71. Kotta PA, Ali JM. Incentive spirometry for prevention of postoperative pulmonary complications after thoracic surgery. Respir Care. 2021;66(2):327–333. doi:10.4187/respcare.07972
72. Mazda Y, Aoyama K. An introductory guide to quality improvement in perioperative medicine. J Anesth. 2021;35(5):606–610. doi:10.1007/s00540-021-02913-z
73. Kokotovic D, Berkfors A, Gögenur I, Ekeloef S, Burcharth J. The effect of postoperative respiratory and mobilization interventions on postoperative complications following abdominal surgery: a systematic review and meta-analysis. Eur J Trauma Emerg Surg. 2021;47(4):975–990. doi:10.1007/s00068-020-01522-x
74. Jiang Z, Liu S, Wang L, et al. Effects of 30% vs. 60% inspired oxygen fraction during mechanical ventilation on postoperative atelectasis: a randomised controlled trial. BMC Anesthesiol. 2023;23(1):265. doi:10.1186/s12871-023-02226-6
75. Ahrens TS. Effects of mechanical ventilation on hemodynamic waveforms. Crit Care Nurs Clin North Am. 1991;3(4):629–639. doi:10.1016/S0899-5885(18)30690-7
76. Zeng C, Lagier D, Lee JW, Vidal Melo MF. Perioperative pulmonary atelectasis: Part I. Biology and mechanisms. Anesthesiology. 2022;136(1):181–205. doi:10.1097/ALN.0000000000003943
77. Monastesse A, Girard F, Massicotte N, Chartrand-Lefebvre C, Girard M. Lung ultrasonography for the assessment of perioperative atelectasis: a pilot feasibility study. Anesth Analg. 2017;124(2):494–504. doi:10.1213/ANE.0000000000001603
78. Grant MC, Crisafi C, Alvarez A, et al. Perioperative care in cardiac surgery: a Joint Consensus Statement by the Enhanced Recovery After Surgery (ERAS) Cardiac Society, ERAS International Society, and The Society of Thoracic Surgeons (STS). Ann Thorac Surg. 2024;117(4):669–689. doi:10.1016/j.athoracsur.2023.12.006
79. Alviar CL, Miller PE, McAreavey D, et al. Positive pressure ventilation in the cardiac intensive care unit. J Am Coll Cardiol. 2018;72(13):1532–1553. doi:10.1016/j.jacc.2018.06.074
80. Williamson PR, Altman DG, Blazeby JM, et al. Developing core outcome sets for clinical trials: issues to consider. Trials. 2012;13:132. doi:10.1186/1745-6215-13-132
81. Serpa Neto A, Hemmes SN, Barbas CS, et al. Protective versus conventional ventilation for surgery: a systematic review and individual patient data meta-analysis. Anesthesiology. 2015;123(1):66–78. doi:10.1097/ALN.0000000000000706
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.