Back to Archived Journals » Open Access Surgery » Volume 13
Indications and Postoperative Outcomes of Pediatric Adenotonsillectomy at a Private Hospital in Dar es Salaam, Tanzania
Authors Abraham ZS ![]() , Kahinga AA
, Kahinga AA ![]() , Mapondella KB, Massawe ER, Ntunaguzi D
, Mapondella KB, Massawe ER, Ntunaguzi D
Received 14 February 2020
Accepted for publication 28 April 2020
Published 19 May 2020 Volume 2020:13 Pages 35—38
DOI https://doi.org/10.2147/OAS.S249844
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Luigi Bonavina
Zephania Saitabau Abraham,1 Aveline Aloyce Kahinga,2 Kassim Babu Mapondella,2 Enica Richard Massawe,2 Daudi Ntunaguzi2
1Department of Surgery, University of Dodoma, College of Health and Allied Sciences, Dodoma, Tanzania; 2Department of Otorhinolaryngology, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania
Correspondence: Zephania Saitabau Abraham Email [email protected]
Aim: We aimed to describe indications and postoperative outcomes of adenotonsillectomy among pediatric patients at a private hospital that serves the largest number of patients with otorhinolaryngological complaints seeking treatment in private health facilities in Tanzania’s largest city.
Introduction: Adenotonsillectomy is one of the commonest surgical procedures in otorhinolaryngology, and indications reported, though scarce in the literature, are infections and sleep-disordered breathing (SDB). Some studies in the last few decades have documented SDB superseding infection. There have been no studies in Tanzania documenting indications and postoperative outcomes of adenotonsillectomy, despite this being a commonly performed surgical procedure.
Methods: A hospital-based descriptive cross-sectional study was conducted from January to December 2018, where children aged 0– 18 years who had undergone adenotonsillectomy at a private hospital were recruited. Data were analyzed using SPSS version 21.
Results: A total of 350 patients aged 0– 18 years were recruited: 60% were children aged < 5 years, 35% 6– 11 years, and 5% 12– 17 years. SDB accounted for a total of 247 (70.5%) indications, while infection accounted for only 60 (17.1%), and when both indications were combined, it accounted for 43 (12.4%) cases. SDB as an indication was proportionally higher in younger children, while infection was higher in older children. Postoperative hemorrhage was encountered in five patients (1.4%). Secondary hemorrhage predominated in four cases (80%), whilst one patient (20%) had primary hemorrhage. Sepsis at the surgical site was found to be the cause for all four patients (100%) with secondary hemorrhage, and the patient with primary hemorrhage had isolated thrombocytopenia as the underlying cause of hemorrhage.
Conclusion: SDB was the commonest indication for adenotonsillectomy and postoperative complications were rare encounter, with secondary hemorrhage being predominant.
Keywords: indications, outcomes, pediatric, adenotonsillectomy, Tanzania
Introduction
(Adeno)tonsillectomy refers to the surgical removal of tonsils and/or adenoids. This surgical procedure remains a commonly performed surgery in otorhinolaryngology practice across the globe in both developed and developing countries. This surgical procedure is considered an ancient one and is well known to be a life-saving procedure for patients if indications are clearly set.1 Through prevention of recurrent infections, significant resolution of enuresis, and elimination of upper-airway obstruction, (adeno)tonsillectomy has resulted in marked improvement in quality of life.2–4 When indications are well set while adhering to known guidelines, adenotonsillectomy has been reported to be curative in >50% of cases by eliminating obstructive sleep apnea.1,5–8 The current primary indication for (adeno)tonsillectomy has generally shifted from recurrent/chronic throat infections to upper-airway obstruction.3,6,8–10
There is a paucity of literature that characterizes the clinical course of patients who have undergone (adeno)tonsillectomy in our country, despite it being the commonest surgical procedure performed in otolaryngology. We aimed to describe indications and postoperative outcomes of adenotonsillectomy among pediatric patients at a private health facility serving the largest number of patients with otorhinolaryngological complaints seeking treatment in private health facilities in Tanzania’s largest city — Dar es Salaam.
Methods
A hospital-based descriptive cross-sectional study was conducted from January to December 2018 at Ekenywa Specialized Hospital, where children aged 0–18 years who had undergone adenotonsillectomy at a private hospital were recruited. Data were analyzed using SPSS version 21. Using a 95% CI for judging significance, association between variables was explored with two-tailed χ2. These procedures were carried out by two qualified otorhinolaryngologists according to the indications laid down by the American Academy of Otolaryngology–Head and Neck Surgery. Tonsillectomy was done principally by cold dissection, though diathermy was at times used to achieve hemostasis by cauterization, whereas adenoidectomy was performed mainly by conventional techniques (blind curettage). These patients were divided into three age ranges: 0–5 years, 6–11 years, and 12–17 years. Analysis of information obtained included basic information: date of birth, indication(s), type of procedure and date, sex, age-group, and outcome. indications were then divided into two broad groups: infections, which included chronic tonsillitis or recurrent tonsillitis, ie, three or more attacks of tonsillitis within a 12-month period; and sleep-disordered breathing (SDB), comprising tonsil and/or adenoid hypertrophy causing sleep disturbances. Diagnosis of obstructive sleep apnea/SDB was made entirely clinically by history-taking, since sleep study/laboratory records were not available. Patients with co-morbid conditions, eg, syndromic and neoplastic cases, were excluded. Ethical approval to conduct the study was sought from the Ekenywa Specialized Hospital Research Ethics Committee and written informed consent obtained from participants’ parents/legal guardians prior to recruitment into the study, with adherence to the Declaration of Helsinki.
Results
Age and Sex Distribution of Study Participants
A total of 350 patients aged 0–18 years were recruited: 60% were children aged <5 years, 35.1% 6–11 years, and 4.9% 12–17 years. Patient ages ranged from 9 months to 17 years. The mean age was 5.02±2.04 years, with a median age of 5 years. There were 260 males (74.3%) and 90 females (25.7%), with a male:female ratio of 2.9:1 (Table 1).
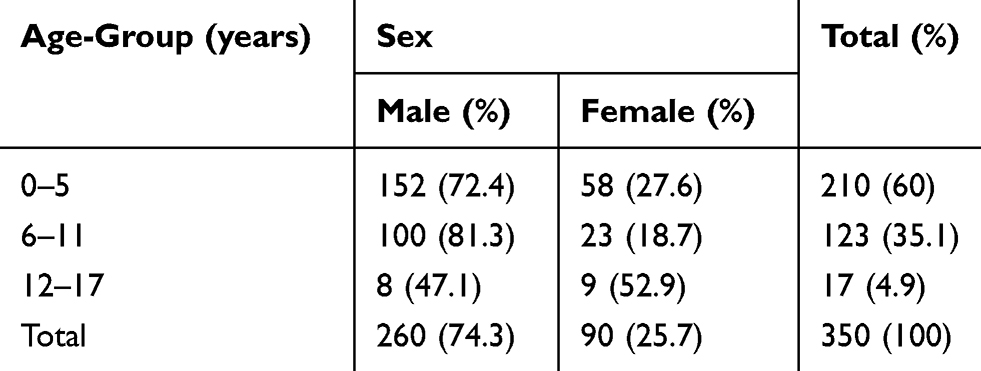 |
Table 1 Age and Sex Distribution of pediatric Patients who had Undergone Adenotonsillectomy |
Association Between Type of Surgical Procedure and Indications
Adenoidectomy (47, 94%) and tonsillectomy (110, 73.3%) were performed predominantly due to SDB. Similarly, the main indication for adenotonsillectomy was SDB (90, 60%). Fisher’s exact test revealed a strong association between type of procedure and given indication for adenotonsillectomy (P=0.001) (Table 2).
 |
Table 2 Association Between Type of Surgical Procedure and Indications |
Indications for Adenotonsillectomy by Age-Group
SDB accounted for a total of 247 (70.5%) and infection only 103 (29.5%) for these procedures. SDB as an indication was proportionally higher in younger children (<5 years of age — 200, 96.2%), while infection was higher in older children (12–17 years — 50, 74.6%). Fisher’s exact test revealed a significant association between age-groups and indications for adenotonsillectomy (P=0.001, Table 3).
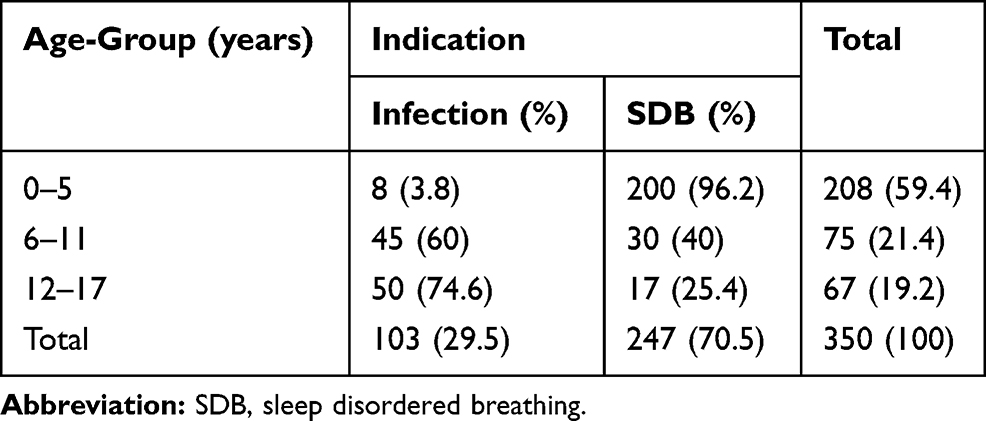 |
Table 3 Indications for Adenotonsillectomy by Age-group |
Postoperative Outcomes of Adenotonsillectomy
Postoperative hemorrhage was encountered in five patients (1.4%). Secondary hemorrhage predominated in four cases (80%), while one patient (20%) had primary hemorrhage (Table 4).
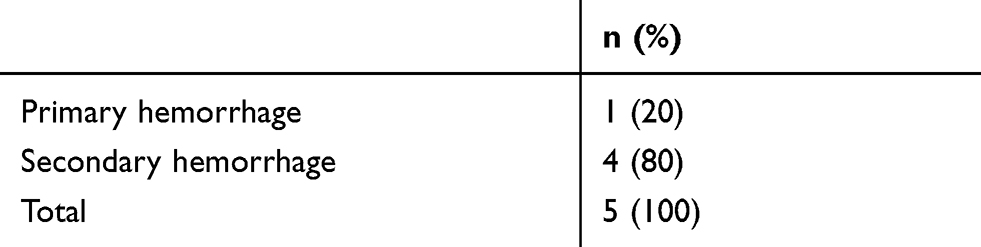 |
Table 4 Postoperative Outcomes of Adenotonsillectomy |
Etiology of Postadenotonsillectomy Hemorrhage among Pediatric Patients
Sepsis at the surgical site was found to be the cause for all four patients with secondary hemorrhage, and the patient who had primary hemorrhage was found to have isolated thrombocytopenia as the underlying cause of hemorrhage (Table 5).
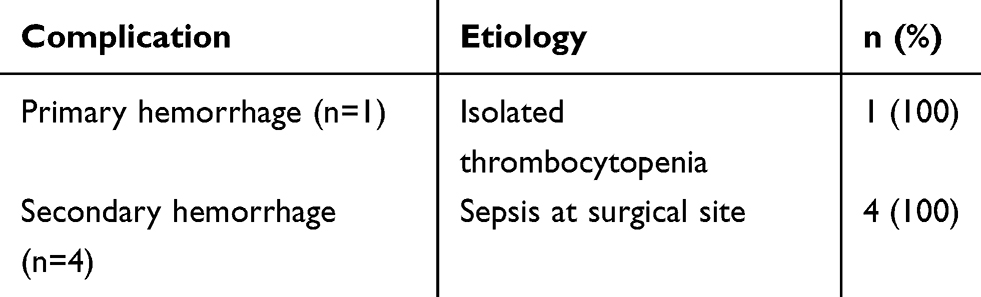 |
Table 5 Etiology of Postadenotonsillectomy Hemorrhage |
Discussion
SDB, which may be caused by obstructive adenotonsillar hypertrophy, has emerged as the leading indication for adenotonsillectomy, and may range from primary snoring to obstructive sleep apnea.3,7–12 The aim of this study was to determineindications and postoperative outcomes of adenotonsillectomy at a private health facility serving the largest number of patients with otorhinolaryngological complaints in private practices in our country.
In our study, comprising 350 patients aged 0–18 years with adenotonsillar hypertrophy who had undergone (adeno)tonsillectomy, it was found that SDB accounted for 70.5% while infection accounted for 29.5% of indications over a 1-year period. Our results are in line withParker and Walner.11 With increasing age, SDB was found to increase steadily, showinging a significant decline after the age of 10 years and receding at 18 years. Similarly, infection as indication for adenotonsillectomy was found to be more prevalent in children aged 0–5 years, with a decline after this age (Table 3).
In children aged <5 years, SDB was the leading indication for (adeno)tonsillectomy, at 59.4% (Table 3). This shows similarity to the findings of Tom et al in a 2-year survey, where 91.5% of indications were due to SDB.13 Several studies in Nigeria also back these findings of tonsillectomy and adenoidectomy being performed predominantly due to SDB.7,14 A study in North America also reported findings that agree with ours,where SDB was found to be the predominant indication for (adeno)tonsillectomy. Contrary to what has been seen in recent studies, 90% of adenotonsillectomies in the 1970s were due to infections, but this has decreased gradually to 30% by 2005.5–7,10–12 These findings appear to be dissimilar to what was found in our study, and this may be due to different approaches to patient selection and a smaller sample compared to our study.
Postoperative hemorrhage may occur as a complication of (adeno)tonsillectomy, and in this study it was found to account for 1.4% of cases. Secondary hemorrhage (80%) was found to supersede primary hemorrhage (20%, Table 4). All cases of secondary hemorrhage were due to sepsis at the surgical site, and one patient with primary hemorrhage had isolated thrombocytopenia (Table 5). Similar findings emerged in a meta-analysis by Canto et al, where hemorrhage was found to be one of the commonest complications after adenotonsillectomy and secondary hemorrhage accounted for 2.6% of cases.15
The main limitations for this study include the fact that while indications for (adeno)tonsillectomy are clear enough, it is common for infected tonsils and/or adenoids that are either chronically or acutely infected to be enlarged and thus to end up with some degree of obstruction. This may account for some degree of overlap in some patients with both infection and obstruction as indications for the surgical procedure under consideration.
Conclusion
This study has validated recent findings that SDB has risen greatly as an indication for (adeno)tonsillectomy, rather than infections that were once predominant prior the era where antibiotics were not widely available to people, even with a doctor’s prescription. Postoperative complications after adenotonsillectomy are rare, and sepsis at the surgical site was found to be the leading cause of postoperative hemorrhage in our hospital setting.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Younis RT, Lazar RH. History and current practice of tonsillectomy. Laryngoscope. 2002;112:3–5.
2. Sargi Z, Younis RT. Tonsillectomy and adenoidectomy techniques: past, present and future. Otolaryngology. 2007;33136:331–335.
3. Manickavasagam J, Ali S, Quraishi MS. General practitioners ’ versus consultants ’ perspective on indications for paediatric tonsillectomy: current trends. J Laryngol Otol. 2012;126:163–167.
4. Piessens P, Hens G, Lemkens N, Schrooten W, Debruyne F, Lemkens P. International Journal of Pediatric Otorhinolaryngology Effect of adenotonsillectomy on the use of respiratory medication §. Int J Pediatr Otorhinolaryngol. 2012;76(6):906–910. doi:10.1016/j.ijporl.2012.02.069
5. Wong BY, Ng YW, Hui Y. A 10 year review of tonsillectomy in a tertiary centre. HK J Paediatr. 2007;12:297–299.
6. Silva S, Ouda M, Mathanakumara S, Ridyard E, Morar P. Tonsillectomy under threat: auditing the indications for performing tonsillectomy. J Laryngol Otol. 2012;126:609–611.
7. Ahmed AO, Aliyu I, Kolo ES. Indications for tonsillectomy and adenoidectomy: our experience. Niger J Clin Pract. 2014;17(1):1–5.
8. Investigation O. Indications, clinical course, and postoperative outcomes of urgent adenotonsillectomy in children. JAMA Otolaryngol Head Neck Surg. 2015;141(3):236–244.
9. Indications C. Tonsillectomy and changing indications. Pediatr Clin North Am. 1996;43(6):1319–1338.
10. Erickson BK, Larson DR, Sauver JLS, Meverden RA, Orvidas LJ. Changes in incidence and indications of tonsillectomy and adenotonsillectomy, 1970–2005. YMHN. 2009;140(6):894–901. doi:10.1016/j.otohns.2009.01.044
11. Parker NP, Walner DL. International Journal of Pediatric Otorhinolaryngology Trends in the indications for pediatric tonsillectomy or adenotonsillectomy §. Int J Pediatr Otorhinolaryngol. 2011;75(2):282–285. doi:10.1016/j.ijporl.2010.11.019
12. Gates GA, Folbre TW. Indications for adenotonsillectomy. Archives of Otolaryngology-Head & Neck Surgery. 1986 May 1;112(5):501–2
13. Tom LW, Dedio RM, Cohen DE, Wetmore RE, Handler SD, Potsic WP. Is outpatient tonsillectomy appropriate for young children?. The laryngoscope. 1992 Mar;102(3):277–80
14. Afolabi OA, Alabi BS, Ologe FE, Dunmade AD. International Journal of Pediatric Otorhinolaryngology Parental satisfaction with post-adenotonsillectomy in the developing world. Int J Pediatr Otorhinolaryngol. 2009;73:1516–1519.
15. Canto GDL, Pachêco-pereira C, Aydinoz S, Bhattacharjee R. Adenotonsillectomy Complications. Pediatrics. 2019;136(4):702–718.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.