Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 13
Indacaterol acetate/mometasone furoate provides sustained improvements in lung function compared with salmeterol xinafoate/fluticasone propionate in patients with moderate-to-very-severe COPD: results from a Phase II randomized, double-blind 12-week study
Authors Beeh KM ![]() , Kirsten AM
, Kirsten AM ![]() , Tanase AM
, Tanase AM ![]() , Richard A, Cao W, Hederer B
, Richard A, Cao W, Hederer B ![]() , Beier J
, Beier J ![]() , Kornmann O, van Zyl-Smit RN
, Kornmann O, van Zyl-Smit RN ![]()
Received 6 July 2018
Accepted for publication 25 October 2018
Published 6 December 2018 Volume 2018:13 Pages 3923—3936
DOI https://doi.org/10.2147/COPD.S179293
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Richard Russell
Kai Michael Beeh,1 Anne-Marie Kirsten,2 Ana-Maria Tanase,3 Alexia Richard,3 Weihua Cao,4 Bettina Hederer,3 Jutta Beier,1 Oliver Kornmann,5 Richard N van Zyl-Smit6
1Insaf Respiratory Research Institute Wiesbaden, Wiesbaden, Germany; 2Pulmonary Research Institute at Lung Clinic Grosshansdorf, Airway Research Center North, German Center for Lung Research, Grosshansdorf, Germany; 3Novartis Pharma AG, Basel, Switzerland; 4Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA; 5IKF Pneumologie, Clinical Research Centre Respiratory Diseases, Frankfurt, Germany; 6Division of Pulmonology and UCT Lung Institute, University of Cape Town, Cape Town, South Africa
Background and purpose: Fixed-dose combinations of a long-acting beta agonist and an inhaled corticosteroid are more effective than the individual components in COPD. The primary study objective was to demonstrate that the combination indacaterol acetate/mometasone furoate (IND/MF [QMF149]) was non-inferior to the twice-daily combination salmeterol xinafoate/fluticasone propionate (Sal/Flu) in terms of trough FEV1 at week 12 (day 85). Secondary objectives were to compare the efficacy of IND/MF (QMF149) vs Sal/Flu with respect to other lung function parameters, COPD exacerbations, symptoms and dyspnea, health status/health-related quality of life, and rescue medication use.
Materials and methods: This was a 12-week multicenter, randomized, double-blind, double-dummy, parallel-group, Phase II study in patients with moderate-to-very-severe COPD, who were randomized (1:1) to IND/MF (QMF149) (150/160 µg once daily; n=316) or Sal/Flu (50/500 µg twice daily; n=313).
Results: Over 90% of patients completed the study: 94.6% in the IND/MF (QMF149) group and 92.0% in the Sal/Flu group. The primary objective of non-inferiority of IND/MF (QMF149) to Sal/Flu for trough FEV1 at week 12 (day 85) was met: the lower limit of the CI (95% CI: 27.7, 83.3 mL) was greater than -60 mL. The analysis for superiority of IND/MF (QMF149) to Sal/Flu demonstrated superiority of IND/MF (QMF149), with a difference of 56 mL (P<0.001). In addition, IND/MF (QMF149) treatment significantly improved COPD exacerbation-related parameters during the 12-week period. Other significant improvements with IND/MF (QMF 149) vs Sal/Flu were noted for dyspnea at week 12 and other COPD symptoms and COPD rescue medication use over the 12 weeks. The safety and tolerability profiles of both the treatments were similar.
Conclusion: IND/MF (QMF149) (150/160 µg once daily) offered superior lung function and symptom efficacy and a favorable safety profile compared with Sal/Flu (50/500 µg twice daily) in patients with moderate-to-very severe COPD.
Keywords: COPD, once-daily inhalers, fixed-combination inhalers, indacaterol, mometasone, LABA/ICS combinations
Plain language summary
For the treatment of COPD, long-acting bronchodilators are the cornerstone of therapy, as recommended by the Global Initiative for Chronic Obstructive Lung Disease. For those with marked symptoms, particularly breathlessness and frequent exacerbations (increased cough and sputum), a combination of bronchodilators and/or adding an inhaled steroid is recommended. Inhaled steroids have been long-known to reduce exacerbations compared with a bronchodilator alone. This study assessed the efficacy of a once-daily long-acting bronchodilator/inhaled steroid (indacaterol acetate/mometasone furoate) compared with a twice-daily combination (salmeterol xinafoate/fluticasone propionate [Sal/Flu]) for the treatment of COPD. The study conclusively showed that once-daily indacaterol acetate/mometasone furoate combination improved lung function and reduced symptoms and exacerbations compared with twice-daily Sal/Flu combination.
Introduction
COPD is a major cause of chronic morbidity and mortality worldwide,1 and its management imposes a substantial economic burden, mainly due to the costs associated with managing exacerbations, especially hospitalizations.2–5 The main goals of treatment are to control symptoms and reduce the future risk of exacerbations;6–8 Current treatment recommendations suggest the use of inhaled corticosteroids (ICSs) as an add-on treatment for those patients who continue to exacerbate on effective bronchodilation.8
Most available long-acting beta agonist (LABA)/ICS combinations are formulated as twice-daily (bid) treatments based on the use of bid LABA formulations (salmeterol and formoterol). Vilanterol/fluticasone furoate is a LABA/ICS fixed-dose combination (FDC) that is suitable for once-daily (qd) dosing.4,9 Compared with vilanterol alone, the addition of fluticasone furoate to vilanterol has been shown to be associated with a decreased rate of moderate and severe exacerbations of COPD in patients with a history of exacerbation.10
QMF149, delivered via the Concept1 (Breezhaler®) device, is the combination of an investigational, inhaled qd FDC of the LABA indacaterol (IND) acetate (150 μg) and the ICS mometasone furoate (MF) (160 μg), initially developed for the maintenance treatment of COPD and asthma. Both the components of this LABA/ICS combination have shown clinical benefits in patients with COPD or asthma.11,12 Previous research demonstrated that 80, 160, and 320 μg doses of MF in the Concept1 (Breezhaler®) device were comparable with 200, 400, and 2×400 μg doses of MF, respectively, in the Twisthaler® device; these findings were based on pharmacokinetic data in healthy volunteers, in vitro fine particle mass adjustments, and subsequent confirmation in a clinical study.13
MF is an on-target ICS due to its very high affinity for the glucocorticoid receptor.14,15 The efficacy of MF in COPD was demonstrated in a 52-week randomized controlled trial (RCT) comparing qd and bid administration in patients with moderate-to-severe COPD. This study reported that both MF 800 μg qd and MF 400 μg bid (administered via Twisthaler®) significantly increased post-bronchodilator trough FEV1 from baseline vs placebo (50 and 53 mL, respectively, vs a 19 mL decrease for placebo; P<0.001); in addition, health status, as measured by the St George’s Respiratory Questionnaire (SGRQ), improved significantly in all domains (total, activity, impacts, and symptoms) in the pooled MF groups vs placebo (P≤0.031).16 MF was generally well-tolerated, with incidence rates of any treatment-emergent adverse event (AE) comparable with placebo.16
Indacaterol is an ultra-LABA, the first approved for the treatment of COPD that allows qd administration,17 with a stronger affinity for the beta2-adrenergic receptors vs a low intrinsic activity at the beta1-receptor,4,18 which improves the cardiovascular safety profile;18 it has a fast onset of action (within 5 minutes)17,19 coupled with a sustained bronchodilator effect (24 hours). When compared with salbutamol (200 μg) and salmeterol/fluticasone propionate (50/500 μg) in patients with moderate-to-severe COPD, single doses of 150 and 300 μg indacaterol demonstrated a fast onset of action, similar to that of salbutamol and faster than that of salmeterol/fluticasone propionate;20 FEV1 at 5 minutes post-dose was significantly higher with 150 and 300 μg indacaterol than it was with salmeterol/fluticasone propionate (50 mL, P=0.003; 70 mL, P<0.001, for the 150 and 300 μg dose, respectively).20
In clinical studies with a duration ranging from 12 weeks to 1 year, qd indacaterol 150 or 300 μg significantly improved lung function vs placebo in patients with moderate-to-severe COPD.17
In relation to safety, indacaterol has been reported to be well tolerated at all doses, with rates of AEs characteristic of beta2-agonists, such as headache, muscle spasm, and tremor, comparable with placebo.17,21
The primary objective of the current study was to demonstrate that the investigational qd combination IND/MF (QMF149) is at least non-inferior to the bid combination salmeterol xinafoate/fluticasone propionate (Sal/Flu) in terms of trough FEV1 at week 12 (day 85). Sal/Flu (50/500 μg, bid) is a marketed, FDC product comprising a LABA and ICS and is indicated for the maintenance treatment of airflow obstruction and reducing exacerbations in patients with COPD. The secondary objectives were to compare the efficacy of IND/MF (QMF149) vs Sal/Flu with respect to other lung function parameters, COPD exacerbations, dyspnea (transitional dyspnea index [TDI]), health status/health-related quality of life (SGRQ; COPD assessment test [CAT]), rescue medication use and COPD symptoms, and to evaluate the safety and tolerability of study treatments during the treatment period.
Materials and methods
Study design
This was a multicenter, randomized, double-blind, double-dummy, parallel-group, Phase II study (NCT01636076), conducted between November 2, 2012, and September 25, 2013, at 117 study centers in Europe, Asia, Australia, South Africa, and the Middle East (see the list of all participating centers in Supplementary materials).
The study consisted of 1-week screening and 2-week run-in phase, followed by a double-blind, parallel-group treatment phase (12 weeks) and a 30-day safety follow-up (Figure 1). Written informed consent was obtained from all patients who participated, and the study was approved by the independent ethics committee/institutional review board of each study center. The study was conducted according to the ethical principles of the Declaration of Helsinki.
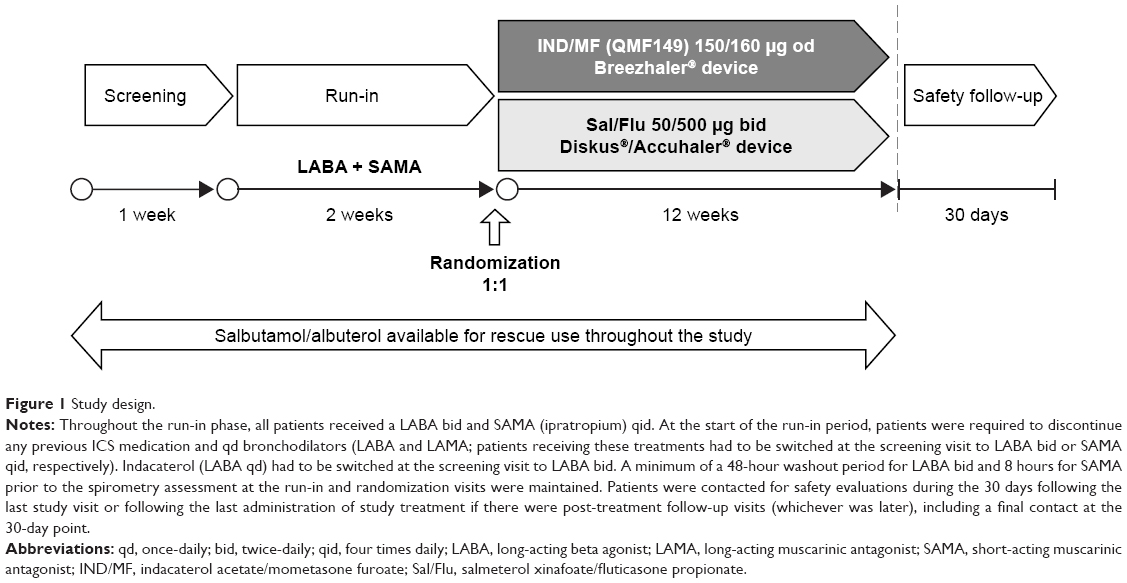 | Figure 1 Study design. |
Patients
Patients were eligible for inclusion in the study if they were: male or female patients aged ≥40 years with moderate-to-very-severe COPD, as defined by the Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2011 guidelines,22 had a post-bronchodilator FEV1 of <70% of the predicted normal value,23,24 and a post-bronchodilator FEV1/FVC of <0.70 at run-in (post-bronchodilator refers to within 30 minutes after inhalation of 400 μg salbutamol/360 μg albuterol [or equivalent dose]); current or ex-smokers with a smoking history of ≥10 pack years (number of packs of 20 cigarettes smoked per day multiplied by number of years the patient smoked, an ex-smoker was defined as a subject who had quit smoking ≥6 months prior to screening).
Key exclusion criteria included any COPD exacerbation that required treatment with antibiotics and/or oral corticosteroids and/or hospitalization in the 6 weeks before screening or developing a COPD exacerbation between screening and randomization, any respiratory tract infection within 4 weeks prior to the screening visit or between the screening and baseline visits, concomitant pulmonary disease (eg, lung fibrosis, sarcoidosis, interstitial lung disease, pulmonary hypertension), a history of asthma or onset of respiratory symptoms before the age of 40 years. Patients who required the use of >8 inhalations of short-acting β2-agonist (SABA) (90 μg albuterol/100 μg salbutamol via metered dose inhaler) on any 3 consecutive days or >12 inhalations of SABA on any 2 consecutive days from screening to randomization were also excluded from the study.
Treatments
At the start of the run-in period, patients were required to discontinue any previous ICS medication and bronchodilators (LABA and LAMA); patients receiving these treatments were switched to a LABA bid and short-acting muscarinic antagonist (SAMA; ipratropium) four times daily. Following the run-in period, eligible patients were randomized (1:1), using Interactive Response Technology, to one of the two treatment groups: IND/MF (QMF149) (150/160 μg qd), delivered via the Concept1 (Breezhaler®) device as a single dose dry powder inhaler, or Sal/Flu (50/500 μg bid), delivered via the Diskus®/Accuhaler® device.
Randomization was stratified by smoking history (ex-smoker, current smoker) and COPD severity (moderate, severe, very severe). IND/MF (QMF149) was supplied by Novartis Drug Supply Management (Novartis International AG, Basel, Switzerland) as dry powder FDC formulation.
As IND/MF (QMF149) and Sal/Flu are delivered via different inhaler devices, a double-dummy design was used for dosing, whereby patients received two inhalers. They were instructed to take both morning and evening doses at approximately the same time of day (both in the morning and evening). The morning dosing consisted of sequential single inhalations from each of the two devices: one inhalation from the Concept1 (Breezhaler®) device containing IND/MF (QMF149) or placebo plus one inhalation from the Diskus®/Accuhaler® device containing Sal/Flu or placebo. The evening dosing consisted of only a single inhalation from the Diskus®/Accuhaler® device containing Sal/Flu or placebo.
All patients, physicians, and other study staff were blinded to the assigned treatment for the duration of the study.
Outcomes and assessments
Spirometry was performed using standard methodology.24 The primary endpoint was trough FEV1 after 12 weeks of treatment (day 85). For IND/MF (QMF149), trough FEV1 refers to the mean of the two FEV1 values measured at 23 hours 10 minutes and 23 hours 45 minutes after the previous morning dose. For Sal/Flu, trough FEV1 is defined as the mean of the two FEV1 values measured at 11 hours 10 minutes and 11 hours 45 minutes after the previous evening dose.
Secondary endpoints included absolute value of trough FEV1 value at week 12, area under the curve (AUC) (5 minutes to 4 hours) for FEV1 on day 1, COPD exacerbation-related parameters (time to first COPD exacerbation during the 12-week treatment, the annual rate of COPD exacerbations, duration [total days] of COPD exacerbations over the 12-week treatment period), TDI25 focal score and the proportion of responders at week 12 (day 84), SGRQ26 total score and the proportion of responders at week 12 (day 84), CAT27 frequencies of categories of clinical impact on COPD (mild, moderate, severe, or very severe) at week 12 (day 84), COPD rescue medication use over 12 weeks of treatment (electronic diary [e-diary]), COPD symptoms (e-diary) over 12 weeks (daily respiratory symptoms [change from baseline in the mean daily respiratory symptom scores], percentage of days “able to perform usual daily activities,” percentage of nights with “no night-time awakenings,” percentage of days with “no daytime symptoms”), and safety assessments.
A COPD exacerbation was defined as a worsening of two or more of the following major symptoms for at least 2 consecutive days: dyspnea, sputum volume, sputum purulence, or a worsening of any one major symptom together with an increase in any one of the following minor symptoms for at least 2 consecutive days: sore throat, colds (nasal discharge and/or nasal congestion), fever without other cause, cough, wheeze. A COPD exacerbation was considered of moderate severity if treatment with systemic corticosteroids and/or antibiotics was required; it was considered severe if the patient was hospitalized.
Other exacerbation-related parameters are presented in the Supplementary materials, Table S1.
The degree of impairment due to dyspnea was assessed at baseline, using the Baseline Dyspnea Index, and over the treatment period using the TDI, which captures changes from baseline;25 a TDI focal score of ≥1 is considered to be a clinically significant improvement from baseline.28 Health status/health-related quality of life was assessed with the SGRQ26 and CAT;27 for SGRQ, a 4-unit change is classed as a minimally clinical important difference (MCID).29 At the run-in visit (day 14), all patients were provided with an e-diary to record morning and evening daily clinical symptoms and rescue medication (salbutamol/albuterol) use. The patient was instructed to routinely complete the diary twice daily, in the morning and evening, considering events over the previous 12 hours.
Statistical analysis
The sample size was determined to demonstrate the non-inferiority of IND/MF over Sal/Flu with regard to trough FEV1 after 12 weeks of treatment. With a non-inferiority margin of −60 mL, an SD of 210 mL, and dropout rate of 10%, ~288 patients were needed per arm to yield 90% power for the testing of non-inferiority with a one-sided significance level of 2.5%. nQuery (V7.0) was used to calculate the sample sizes.
The full analysis set (FAS) was used for the primary efficacy analysis and included all randomized patients who received at least one dose of the study drug (intent-to-treat principle).
Primary and most of the secondary endpoint analyses were performed using a mixed model for repeated measures (MMRM). The model comprised treatment, country, visit, treatment-by-visit interaction, smoking status, and COPD severity as fixed effects, and baseline FEV1 and SABA FEV1 reversibility components as covariates.
The between-treatment comparisons for AUC (5 minutes to 4 hours) for FEV1 on day 1 were analyzed with analysis of covariance (ANCOVA) mixed model.
The time to first COPD exacerbation was displayed with a Kaplan–Meier curve and analyzed using a Cox regression model stratified by baseline smoking status and COPD severity. The rate of COPD exacerbations over the 12-week treatment period was analyzed using a negative binomial regression model displaying 95% CI of the estimated rate difference. The duration and total number of exacerbation days were summarized by treatment using subjects with at least one exacerbation.
Logistic regression was conducted for TDI focal score on the proportion of patients achieving clinically meaningfulness as ≥1 unit and SGRQ for the proportion of subjects who achieved a clinically important improvement of at least 4 units in the SGRQ total score after 12 weeks of treatment. The CAT frequencies of categories of clinical impact on COPD (mild, moderate, severe, or very severe) were summarized by treatment.
Between-treatment comparisons for change from baseline in the mean daily total and mean daily individual symptom scores over the 12 weeks of treatment were analyzed with ANCOVA mixed model.
Non-inferiority of IND/MF (QMF149) to Sal/Flu would be claimed if the 95% CI for the adjusted mean FEV1 difference of IND/MF (QMF149) minus Sal/Flu lay entirely to the right (higher than) of the non-inferiority margin of −60 mL. If non-inferiority of IND/MF (QMF149) with respect to trough FEV1 after 12 weeks treatment (ie, at day 85) was met, IND/MF (QMF149) was then tested for superiority using the FAS at the (two-sided) 5% significance level by the same MMRM used for the primary analysis.
The exploratory subgroup analyses of trough FEV1 after 12 weeks of treatment were performed for FAS by using the MMRM analysis in the following subgroups of interest: age group (<65 years, 65 to <75 years, ≥75 years), gender (male, female), race (Caucasian, non-Caucasian), severity of airflow limitation (moderate or less, severe or worse, based on the classification defined by the GOLD 2011 guidelines),22 smoking status at baseline (current smoker, ex-smoker), and SABA FEV1 reversibility (≤5% increase, >5% and ≤12% increase, >12% increase).
The safety set included all patients who received at least one dose of study drug.
SAS (V9.3) was used for all the statistical analyses conducted in this study.
Results
Patients
Of the 982 patients screened, 629 with moderate-to-very severe COPD were randomized (1:1) to one of the two treatment groups: IND/MF (QMF149), n=316; Sal/Flu, n=313 (Figure 2). Over 90% of patients in both the treatment groups completed the study: 94.6% in the IND/MF (QMF149) group and 92.0% in the Sal/Flu group. Overall, the most common reasons for treatment discontinuation were patient/guardian decision (n=17, 2.7%) and AEs (n=17, 2.7%). Patient demographics and baseline characteristics were similar between the two treatment groups (Table 1). The average age of the study population was 64.5 years, and over 90% of patients were aged between 40 and 75 years.
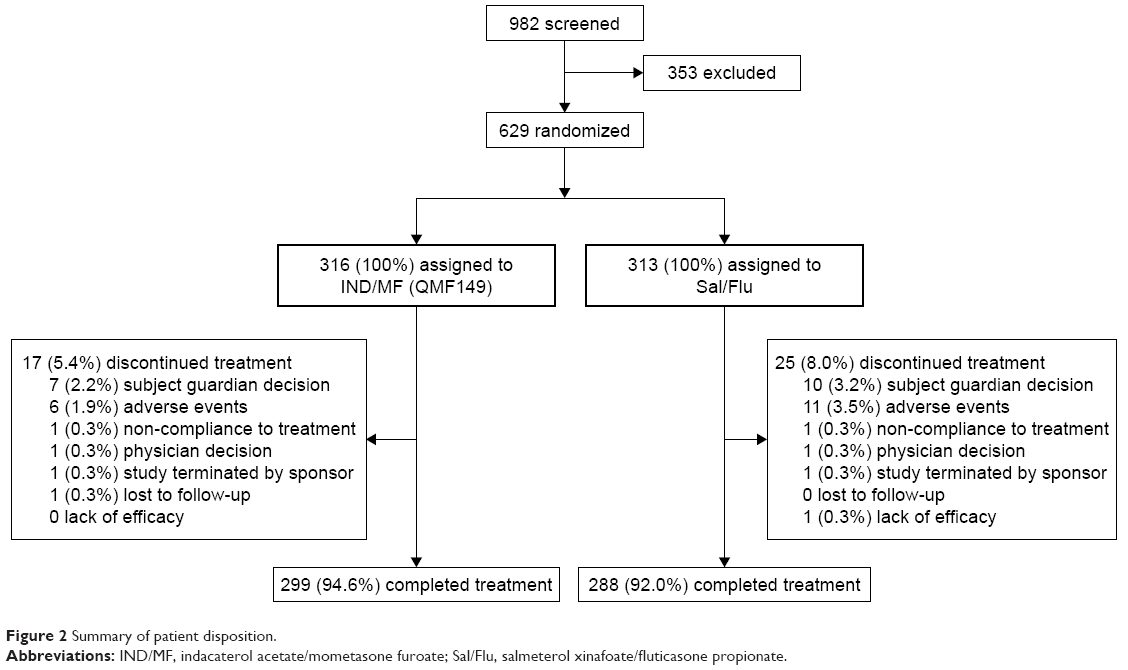 | Figure 2 Summary of patient disposition. |
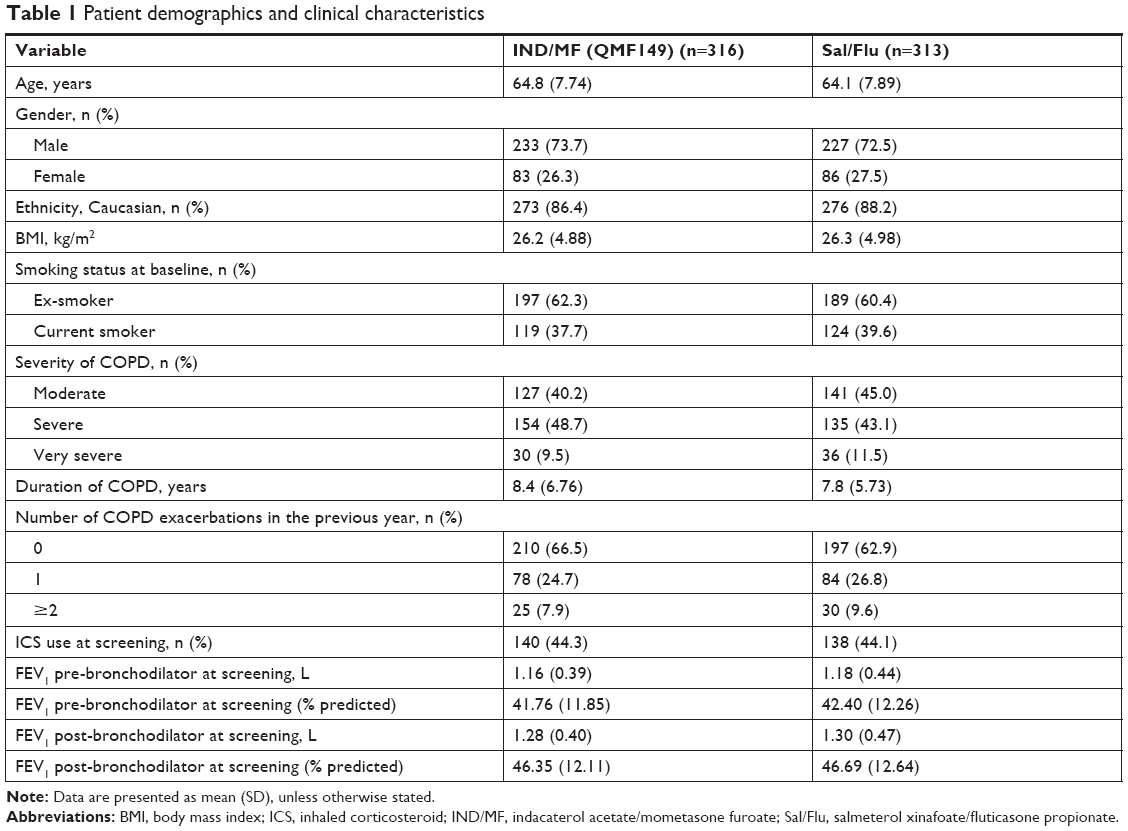 | Table 1 Patient demographics and clinical characteristics |
The numbers of patients using ICS (either as an FDC or monotherapy) at screening were comparable between the treatment groups: IND/MF (QMF149), n=140 (44.3%); Sal/Flu, n=138 (44.1%). Most of the patients had severe (IND/MF [QMF149], 48.7%; Sal/Flu, 43.1%) or very severe (IND/MF [QMF149], 9.5%; Sal/Flu, 11.5%) disease; 40.2% of patients in the IND/MF (QMF149) group and 45.0% in the Sal/Flu group were categorized as moderate severity (GOLD 2011),22 with a mean duration of COPD of ~8 years in both the groups. As per protocol, all patients were smokers or ex-smokers (mean 45 pack years).
FEV1 at screening was balanced across the two groups, with a mean post-bronchodilator FEV1 of 1.28 L in the IND/MF (QMF149) group and 1.30 L in the Sal/Flu group and a mean percent predicted FEV1 of 46.3% and 46.7% of the predicted normal, respectively. The majority of patients had no COPD exacerbations in the previous year since this was not a study inclusion criterion. Similar numbers of patients in each treatment group had at least one COPD exacerbation in the previous year (103 patients [32.6%] in the IND/MF [QMF149] group, 114 [36.4%] in the Sal/Flu group).
Efficacy
Lung function
Trough FEV1
At week 12 (day 85), the least squares (LS) mean trough FEV1 for IND/MF (QMF149) was 1.270 L (± standard error 0.0124) and for Sal/Flu, it was 1.215 L (±0.0124). As the lower limit of the treatment difference (IND/MF – Sal/Flu =56 mL; 95% CI: 27.7, 83.3 mL) was greater than −60 mL at week 12 (day 85), the primary end point was met: IND/MF (QMF149) was shown to be non-inferior to Sal/Flu with respect to trough FEV1. Because the study met its primary objective of non-inferiority to Sal/Flu, testing for superiority of IND/MF (QMF149) to Sal/Flu was conducted. This analysis demonstrated superiority of IND/MF (QMF149) to Sal/Flu, with a treatment difference of 56 mL (P<0.001).
IND/MF (QMF149) provided greater and sustained trough FEV1 improvements compared with Sal/Flu increasing from day 2 onwards, over the 12-week period (Figure 3). Mean FEV1 on days 28, 29, and 84 was significantly greater with IND/MF (QMF149) vs Sal/Flu: day 28, 44 mL (95% CI 18.4, 70.2; P<0.001); day 29, 30 mL (95% CI 3.8, 56.1; P=0.025); and day 84, 62 mL (95% CI 32.4, 90.6; P<0.001). There was a small, but significant, efficacy difference in the mean trough FEV1 in favor of Sal/Flu observed at day 2 (−27 mL; 95% CI −47.2, −6.3; P=0.011).
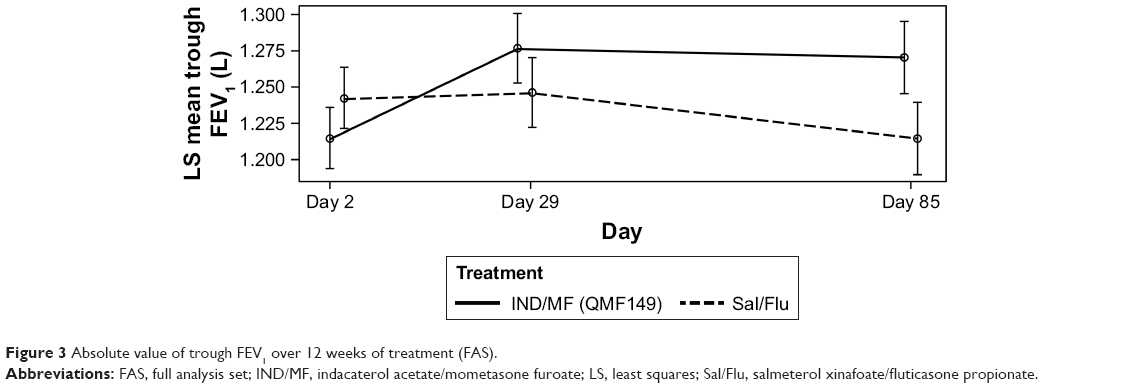 | Figure 3 Absolute value of trough FEV1 over 12 weeks of treatment (FAS). |
Exploratory subgroup analyses
Subgroup analyses results for trough FEV1 were consistent and further supported the primary endpoint in terms of age, gender, race, COPD severity, smoking status, and FEV1 reversibility, with IND/MF (QMF149) demonstrating significant improvements in trough FEV1 at week 12 (day 85) in the subgroups of interest (Table 2).
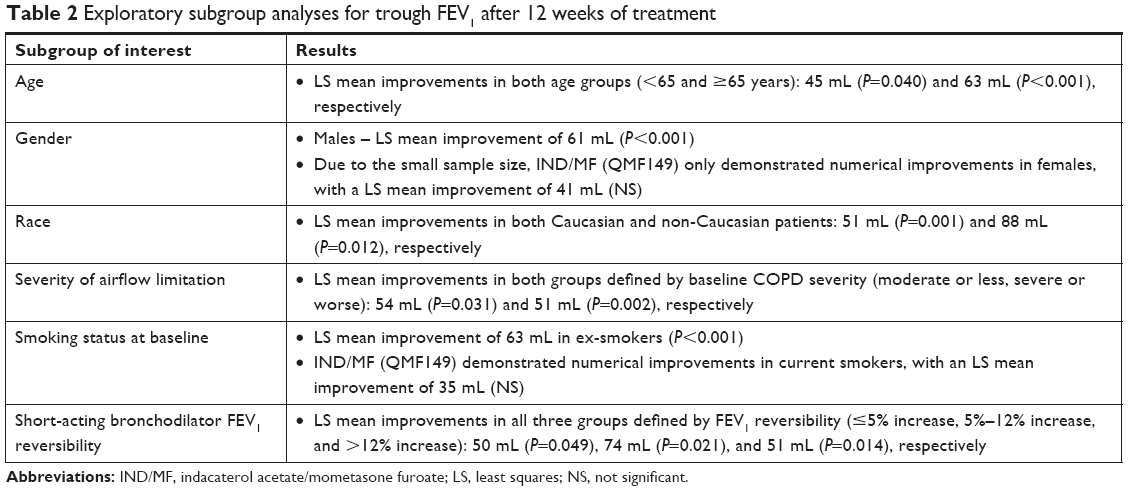 | Table 2 Exploratory subgroup analyses for trough FEV1 after 12 weeks of treatment |
AUC (5 minutes to 4 hours) for FEV1 on day 1
There was a significant treatment difference between IND/MF (QMF149) and Sal/Flu in FEV1 AUC (5 minutes to 4 hours) on day 1, in favor of IND/MF (QMF149), with LS mean of 17 mL (95% CI 0.9, 33.8 mL; P=0.039). IND/MF (QMF149) showed faster onset of bronchodilation effect, as evidenced by greater LS mean FEV1 values in the IND/MF (QMF149) group vs the Sal/Flu group at 5 minutes, 30 minutes, and 1 hour post-dose on day 1; the treatment differences (56, 31, and 24 mL) were significant at all these time points (P<0.001 at 5 and 30 minutes; P<0.0061 at 1 hour post-dose); at 4 hours after dosing, a similar improvement in lung function was observed in LS mean FEV1 in both the treatment groups (Figure 4).
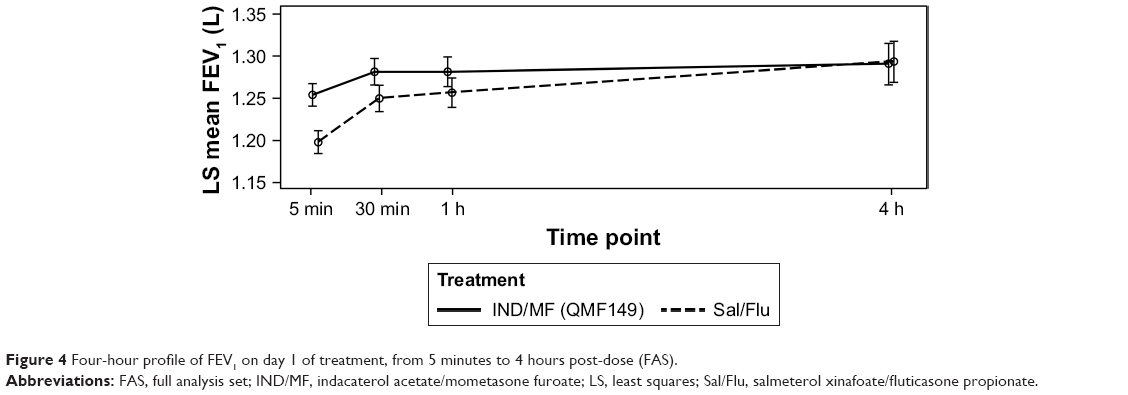 | Figure 4 Four-hour profile of FEV1 on day 1 of treatment, from 5 minutes to 4 hours post-dose (FAS). |
Exacerbations
Exacerbation rates were low in both the groups, with a mean of 0.25, 0.11, and 0.36 for moderate, severe, and moderate or severe exacerbations, per patient per year, respectively, in the IND/MF (QMF149) group vs 0.59, 0.07, and 0.66, respectively, in the Sal/Flu group. For all the COPD exacerbation-related parameters reported below, no significant differences between treatment groups were noted for severe COPD exacerbations.
Time to first COPD exacerbation during the 12-week treatment
Patients in the IND/MF (QMF149) group demonstrated a significantly longer time to first moderate, and first moderate or severe exacerbation compared with patients in the Sal/Flu group: HR =0.45 (95% CI 0.250, 0.815; P=0.008); HR =0.51 (95% CI 0.298, 0.855; P=0.011; Figure 5), with reductions in HR of 55% and 49%, respectively.
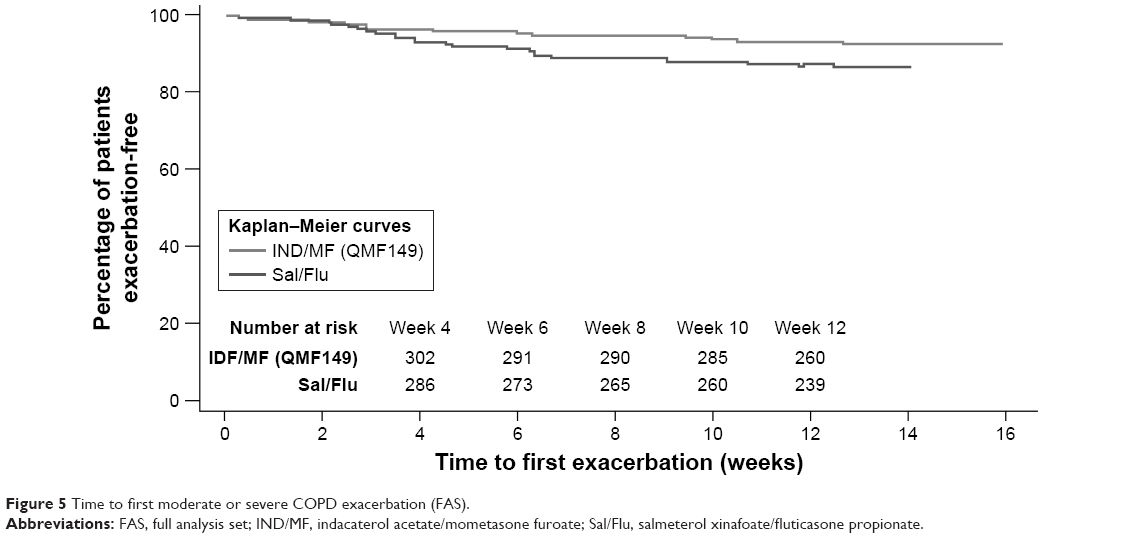 | Figure 5 Time to first moderate or severe COPD exacerbation (FAS). |
The IND/MF (QMF149) group demonstrated higher event-free rates (HR <1) at week 12 than did the Sal/Flu group for moderate, and moderate or severe exacerbations (Table 3).
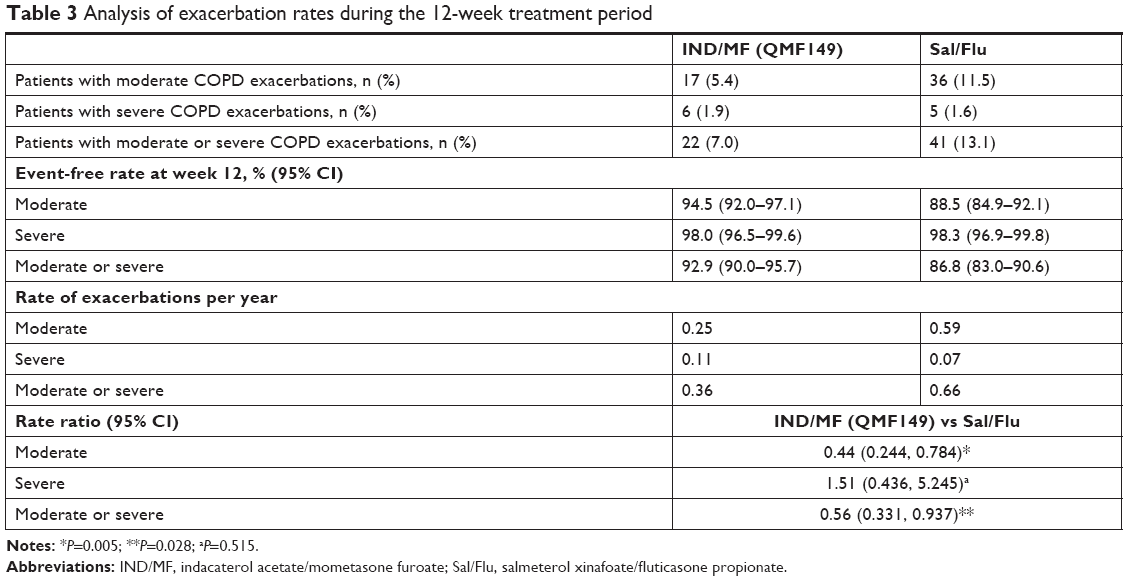 | Table 3 Analysis of exacerbation rates during the 12-week treatment period |
Annual rate of COPD exacerbations
The annualized exacerbation rates were compared between groups and the reductions in annual rate of moderate (56%; P=0.005), and moderate or severe (44%; P=0.028) COPD exacerbations were significantly in favor of IND/MF (QMF149) (Table 3).
Duration (total days) of COPD exacerbations over the 12-week treatment period
Most patients did not experience a COPD exacerbation during the treatment period. IND/MF (QMF149) significantly reduced the mean (±SD) number of exacerbation days per patient compared with Sal/Flu for moderate (0.9±4.40 vs 1.5±5.05, P=0.003), and for moderate or severe (1.4±6.57 vs 1.7±5.29, P=0.015) COPD exacerbations.
Dyspnea
IND/MF (QMF149) significantly improved TDI focal score at week 12 (least squares mean for treatment difference [LSMTD] =0.501; 95% CI 0.0601, 0.9414; P=0.026) vs Sal/Flu. There was no significant difference between groups in the percentage of patients who achieved MCID >1 point from baseline in TDI focal score at week 12, although this was numerically in favor of IND/MF (QMF149): 52.6% in the IND/MF (QMF149) group vs 45.9% in the Sal/Flu group.
Health status/health-related quality of life
There were no significant differences in health status/health-related quality of life between the two treatment groups after 12 weeks of treatment.
SGRQ
Treatment with IND/MF (QMF149) was associated with numerical improvements in health status (SGRQ total score) after 12 weeks of treatment compared with treatment with Sal/Flu (LSMTD −1.66; 95% CI −3.6001, 0.2777; NS). Unlike the Sal/Flu group (−1.94 units), the IND/MF (QMF149) group approached a clinically meaningful improvement in patient health status from baseline (−3.6 units) in the SGRQ total score.
There was no significant difference between groups in the percentage of patients achieving MCID ≥4 units in the SGRQ score at week 12 (day 84), although a numerically higher proportion of patients (42.7%) in the IND/MF (QMF149) group achieved this compared with the Sal/Flu group (37.5%).
CAT
CAT scores of 0–10, 11–20, 21–30, and 31–40 represent a “mild,” “moderate,” “severe”, or “very severe” clinical impact of COPD on the patient, respectively. At week 12 (day 84), fewer patients in the IND/MF (QMF149) group than in the Sal/Flu group were in the “severe” (23.4% vs 24.3%) or “very severe” (1.6% vs 4.5%) clinical impact of COPD categories.
COPD rescue medication use
The reduction in rescue medication use over 12 weeks was significantly in favor of IND/MF (QMF149) vs Sal/Flu (Table 4): mean daily number of puffs (LSMTD −0.47, P=0.003), mean daytime number of puffs (LSMTD −0.325, P=0.001), mean nighttime number of puffs (LSMTD −0.143, P=0.044), and percentage of days with no rescue medication use (LSMTD 6.26, P=0.007).
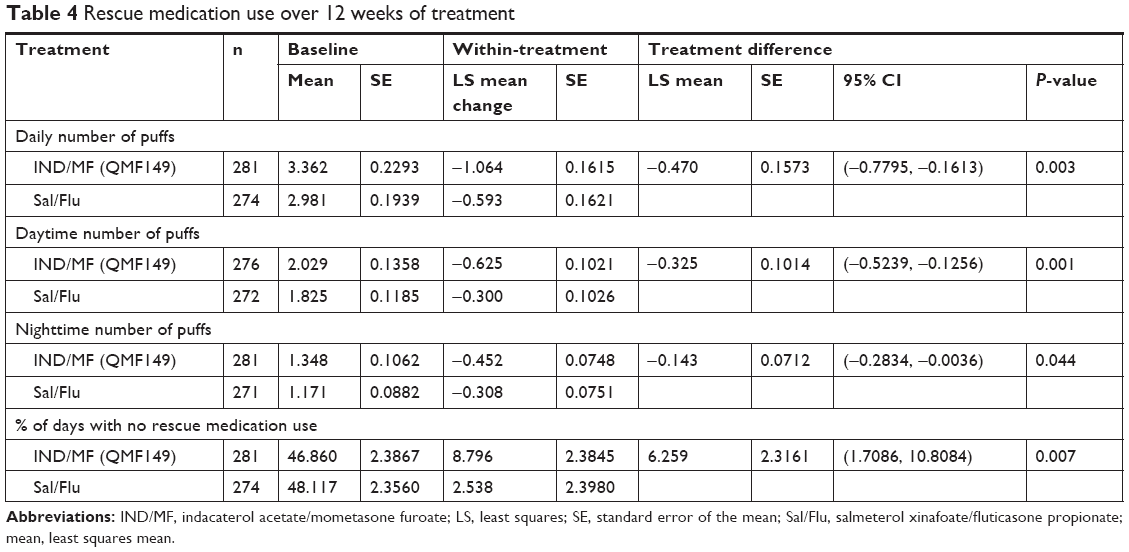 | Table 4 Rescue medication use over 12 weeks of treatment |
COPD symptoms
Compared with Sal/Flu treatment, IND/MF (QMF149) therapy significantly reduced the mean daily respiratory symptoms score (LSMTD −0.122; 95% CI −0.2108, −0.0339; P=0.007), the percentage of days “able to perform usual daily activities” (LSMTD 7.537%; 95% CI 3.8326, 11.2424; P<0.001) and the percentage of nights with “no nighttime awakenings” (LSMTD 3.507%; 95% CI 0.0121, 7.0022; P=0.049) over 12 weeks (Table 5). There was no significant difference in terms of percentage of days with “no daytime symptoms” over 12 weeks of treatment (Table 5).
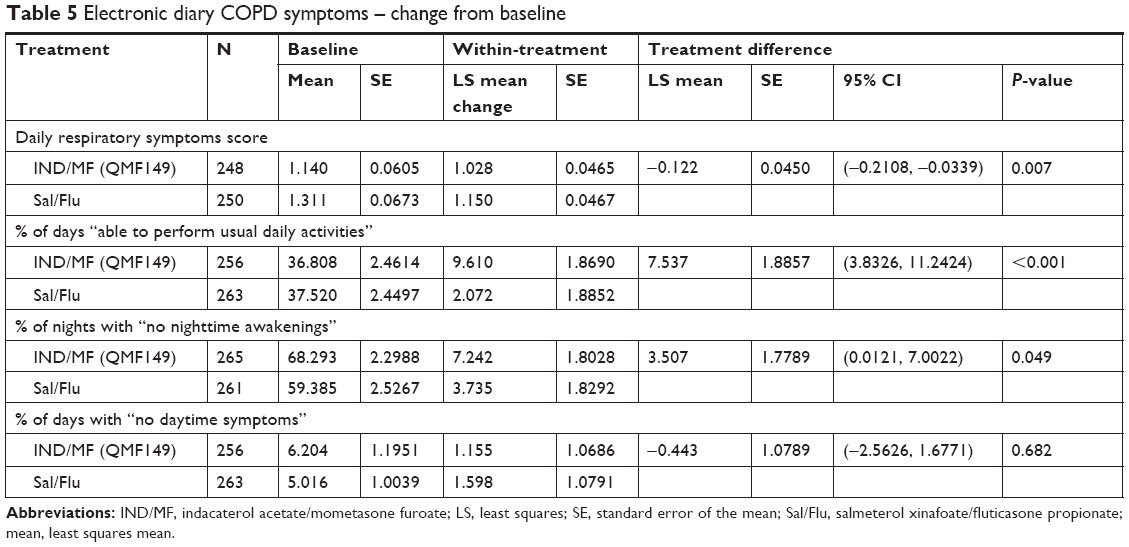 | Table 5 Electronic diary COPD symptoms – change from baseline |
Safety and tolerability
Overall, both the treatments were well-tolerated, with a low incidence of AEs. No deaths were reported in this study. Most of the reported AEs were of mild to moderate intensity and were resolved by the last follow-up visit. IND/MF (QMF149)-treated patients experienced fewer serious adverse events (SAEs), AEs, and AEs related to COPD exacerbations, as well as discontinuations due to AEs, compared with Sal/Flu-treated patients (Table 6).
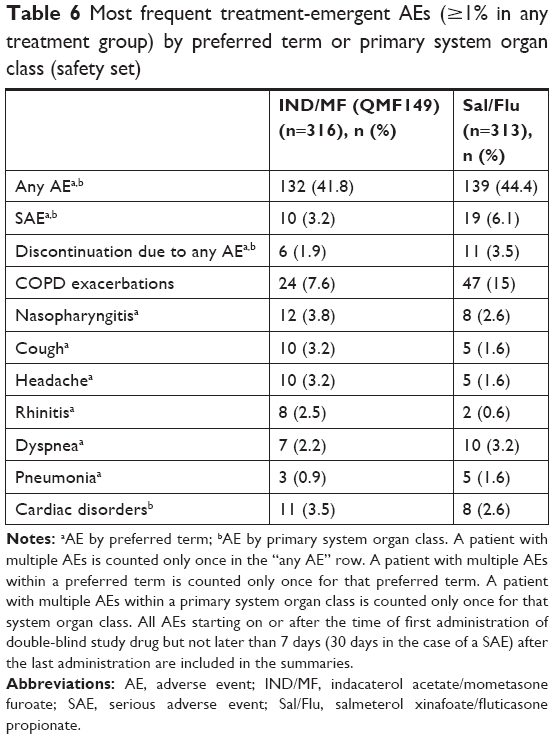 | Table 6 Most frequent treatment-emergent AEs (≥1% in any treatment group) by preferred term or primary system organ class (safety set) |
The most common SAE was COPD exacerbation: 1.9% (n=6) in the IND/MF (QMF149) group and 1.6% (n=5) in the Sal/Flu group. COPD exacerbation was also the most common AE leading to discontinuation in either treatment group: 0.6% (n=2) in the IND/MF (QMF149) group and 0.3% (n=1) in the Sal/Flu group. The incidence of pneumonia (any reported AE or SAE of pneumonia confirmed by chest X-ray) was low and similar between the two treatment groups: IND/MF (QMF149) (n=3; 0.9%); Sal/Flu (n=5; 1.6%). Likewise, the incidence of AEs related to cardiac disorders was comparable: IND/MF (QMF149) (n=11; 3.5%); Sal/Flu (n=8; 2.6%). The incidences of rhinitis, cough, and headache were low but slightly higher in the IND/MF vs Sal/Flu treatment arms (2.5% vs 0.6%, 3.2% vs 1.6%, and 3.2% vs 1.6%, respectively). No major effects of treatment on pulse or blood pressure were observed, and no clinically meaningful treatment differences were noted between the treatment groups for routine laboratory parameters.
Discussion
This randomized, parallel-group, 12-week study of the qd combination of IND/MF (QMF149) delivered via the Concept1 (Breezhaler®) device demonstrated significant improvements in lung function, as measured by the primary endpoint of trough FEV1, compared with bid Sal/Flu delivered via the Diskus®/Accuhaler® device, in patients with moderate-to-very-severe COPD. Secondary endpoints, including exacerbations, dyspnea, rescue medication use, COPD symptoms, showed superior efficacy of IND/MF over Sal/Flu.
For the primary endpoint of trough FEV1 at week 12 (day 85), treatment with IND/MF (QMF149) resulted in a 56 mL improvement over Sal/Flu. An increased improvement in trough FEV1 for IND/MF (QMF149) over Sal/Flu was observed after day 2 of treatment. The exploratory subgroup analyses, which were conducted for several subgroups of interest (age, gender, race, COPD severity, smoking status, and FEV1 reversibility), showed similar results to those of the primary analysis for trough FEV1 after 12 weeks of treatment, further supporting the superiority of IND/MF (QMF149) to Sal/Flu.
Importantly, the fast onset of action of the LABA component of QMF149, indacaterol20 was confirmed in favor of IND/MF (QMF149) over Sal/Flu, as significant treatment differences were observed for LS means of FEV1 at 5 minutes, 30 minutes, and 1 hour post-dose on day 1. Indacaterol provides 24-hour bronchodilation,17,30 and when compared with other LABAs, such as salmeterol and formoterol, it has shown superior improvements in lung function, dyspnea, and rescue medication use in patients with COPD.30–32
The treatment difference in trough FEV1 observed in the current study with the FDC combination of IND/MF (QMF149) vs Sal/Flu is similar to findings in previous studies comparing indacaterol monotherapy with salmeterol monotherapy. Specifically, indacaterol (150 μg qd) was significantly superior to salmeterol 50 μg bid at week 12 in patients with moderate-to-severe COPD: trough FEV1 (adjusted mean difference [95% CI] 60 [37, 83] mL; P<0.001).31 Similarly, an earlier study that compared indacaterol (150 μg qd) with salmeterol (50 μg bid) and placebo in moderate-to-severe COPD found that indacaterol increased trough FEV1 at week 12 by 170 mL over placebo (P<0.001) and by 60 mL over salmeterol (P<0.001).32 The present study evaluated COPD patients with moderate (42%), severe (46%), and very severe (11%) disease (GOLD categories B, C, and D; GOLD 2014);33 so compared with patients in the previous studies of indacaterol vs salmeterol,31,32 the patients in the current study had generally more advanced disease. However, they were comparable with the population in the INVIGORATE study, where indacaterol alone was less effective than tiotropium for reducing exacerbations.34
In patients with more severe disease and persistent exacerbations, treatment with a single bronchodilator (LABA or LAMA) may not be sufficient; hence, those patients may benefit from dual bronchodilation or a combination of LABA and ICS, the latter preferred for patients with a history of or concomitant asthma.8 Support for the contribution of the ICS MF to the lung function efficacy of a LABA/ICS combination is provided by the pooled analysis of two 52-week RCTs of formoterol fumarate/mometasone furoate (FF/MF) FDC combination in patients with moderate-to-very-severe COPD.35 This study found that the improvements in trough FEV1 were significantly greater for FF/MF 10/400 μg compared with FF 10 μg (P≤0.008) and placebo (P<0.001) at the week 13 primary endpoint and at all other time points (eg, week 26).
An important aspect of COPD management is reducing or preventing COPD exacerbations,2,4 due to their substantial and potentially prolonged negative impact on patients, the possible acceleration in disease progression and considerable healthcare expenditure.36 Limitations of the current study, in terms of the secondary endpoint of exacerbations, include its short duration of 12 weeks and the fact that the inclusion criteria did not require a history of exacerbations, resulting in low exacerbation rates, which prevent firm conclusions on long-term exacerbation outcomes. Nevertheless, IND/MF (QMF149) treatment significantly improved COPD exacerbation-related parameters for moderate, and moderate or severe exacerbations during the 12-week treatment period. These findings should be interpreted with caution, but may show a trend for long-term outcomes. An earlier study in patients with moderate COPD who were at low risk of exacerbations – the Indacaterol: Switching Non-exacerbating Patients with Moderate COPD From Salmeterol/Fluticasone to Indacaterol (INSTEAD) trial – demonstrated non-inferiority in terms of trough FEV1 after 12 weeks of indacaterol 150 μg qd monotherapy to the combination of Sal/Flu 50/500 μg bid; this study also found no significant differences between the monotherapy to the combination treatment group on TDI or the SGRQ at weeks 12 or 26, or rescue medication use or COPD exacerbation rates over 26 weeks.37
Other significant improvements with IND/MF (QMF 149) vs Sal/Flu were noted for dyspnea (TDI focal score) at week 12, COPD rescue medication use (number of puffs of salbutamol/albuterol) over the 12 weeks, as well as COPD symptoms (daily respiratory symptoms score, the percentage of days “able to perform usual daily activities” and the percentage of nights with “no nighttime awakenings”) over 12 weeks.
Although health status/health-related quality of life (as determined by the SGRQ total score and the CAT overall score) did not show clinically significant improvements with either treatment after 12 weeks, the IND/MF (QMF149) group approached the meaningful clinical improvement difference (MCID) of ≥4 units29 in patient health status from baseline (3.6 units) in the SGRQ total score. There was also no significant difference between groups in the proportion of patients who achieved MCID >1 point from baseline in TDI focal score or MCID ≥4 units in the SGRQ score at week 12.
Overall, the efficacy findings of the present study are in agreement with those from systematic reviews, which have supported the use of LABA/ICS combination therapies in COPD.2,9,38,39
In patients with moderate-to-very-severe COPD and exacerbations, an ICS combined with a LABA is more effective than either component alone in improving lung function and health status and reducing exacerbations.8
The safety and tolerability profiles of both the treatments were similar. Both the treatments were generally well-tolerated, with COPD exacerbations, nasopharyngitis, and cough being the most commonly reported AEs. AEs related to COPD exacerbation occurred nearly twice as frequently in the Sal/Flu group compared with the IND/MF (QMF149) group: 47 (15%) and 24 (7.6%), respectively.
Lastly, in addition to the superior efficacy of qd IND/MF (QMF 149) vs bid Sal/Flu, the qd dosing of the IND/MF (QMF149) combination offers greater patient convenience.
Conclusion
In summary, this Phase II study showed that the LABA/ICS FDC treatment, IND/MF (QMF149) (150/160 μg qd, delivered via Concept1 [Breezhaler®]), offered superior efficacy and a similar safety profile compared with Sal/Flu (50/500 μg bid, delivered via Diskus®/Accuhaler®) in patients with moderate-to-very severe COPD. IND/MF (QMF149) could potentially represent an improvement in ICS-based treatment for COPD, as it combines the rapid onset of action and “best in class” efficacy of the LABA indacaterol, along with the anti-inflammatory activity of the ICS MF.
In line with GOLD recommendation, LABA/ICS would benefit a rather limited group of COPD patients (eg, who may have a history of asthma and/or findings suggestive of asthma–COPD overlap) while in asthma ICS-based treatment is the cornerstone therapy and therefore IND/MF (QMF149) is currently developed for asthma.
Data sharing
Novartis is committed to sharing access to patient-level data with qualified external researchers and supporting clinical documents from eligible studies. These requests are reviewed and approved by an independent review panel on the basis of scientific merit. All data provided are anonymized to respect the privacy of patients who have participated in the trial in line with applicable laws and regulations. Result summaries have been posted on the Novartis clinical trial database and other online public databases. More information on Novartis’ position on access to clinical trial results and patient-level data is available here: https://www.novartis.com/our-science/clinical-trials/clinical-trial-information-disclosure.
Acknowledgments
The authors were assisted in the preparation of the manuscript by Delia Randall (Novartis Product Lifecycle Services), who provided writing and editorial support, funded by Novartis Pharma AG in accordance with Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3). Novartis was responsible for the conception and design of the study and analysis and interpretation of data. The authors thank the patients who took part in the study and the staff at the participating clinical centers. This study was published as an abstract and presented at the British Thoracic Society Winter Meeting 2014, London, UK, December 3–5, 2014. Insaf Respiratory Research Institute has received compensation for services on advisory boards or consulting for Ablynx, Almirall, AstraZeneca, Berlin Chemie, Boehringer, Chiesi, Cytos, Mundipharma, Novartis, Pohl Boskamp, and Zentiva. The institution has received compensation for speaker activities in scientific meetings supported by Almirall, AstraZeneca, Berlin Chemie, Boehringer, Cytos, ERT, GSK, Novartis, Pfizer, Pohl Boskamp, and Takeda. The institution has further received compensation for design and performance of clinical trials from Almirall, Altana/Nycomed, AstraZeneca, Boehringer, Cytos, GSK, Infinity, Medapharma, MSD, Mundipharma, Novartis, Parexel, Pearl Therapeutics, Pfizer, Revotar, Teva, Sterna, and Zentiva. The Pulmonary Research Institute at LungClinic Grosshansdorf received reimbursement from Novartis for conducting this study. The Pulmonary Research Institute at Lung Clinic Grosshansdorf, Airway Research Center North, German Center for Lung Research received compensation for participation in clinical studies from AstraZeneca, Bayer Healthcare, Boehringer Ingelheim, GSK, Novartis, Roche, Sanofi, and Takeda. IKF Pneumologie, Clinical Research Centre Respiratory Diseases received reimbursement from Novartis for conducting this study. Division of Pulmonology and UCT Lung Institute, University of Cape Town received reimbursement from Novartis for conducting this clinical trial.
Author contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
AMT, BH and AR are employees of Novartis Pharma AG. WC is an employee of Novartis Pharmaceuticals Corporation. KMB declares that no personal payments were received from any pharmaceutical entity in the past 5 years. KMB and JB are full-time employees of Insaf Respiratory Research Institute. AMK is an employee of the Pulmonary Research Institute at LungClinic Grosshansdorf. AMK received speaking honoraria, honoraria for participation in advisory board meetings, and travel support for attending congresses in respiratory medicine from Boehringer Ingelheim, AstraZeneca, and Novartis. RNVZS has received honoraria for academic work from Novartis, AZ, CIPLA, ASPEN, Pfizer, GSK, and MSD. The authors report no other conflicts of interest in this work.
References
Collaborators GBDCRD, Soriano JB, Abajobir AA, et al. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir Med. 2017;5(9):691–706. | ||
Kew KM, Dias S, Cates CJ. Long-acting inhaled therapy (beta-agonists, anticholinergics and steroids) for COPD: a network meta-analysis. Cochrane Database of Systematic Reviews. 2014;(3):CD010844. | ||
Hutchinson A, Brand C, Irving L, Roberts C, Thompson P, Campbell D. Acute care costs of patients admitted for management of chronic obstructive pulmonary disease exacerbations: contribution of disease severity, infection and chronic heart failure. Intern Med J. 2010;40(5):364–371. | ||
Barjaktarevic IZ, Arredondo AF, Cooper CB. Positioning new pharmacotherapies for COPD. International Journal of Chronic Obstructive Pulmonary Disease. 2015;10:1427–1442. | ||
Guarascio AJ, Ray SM, Finch CK, Self TH. The clinical and economic burden of chronic obstructive pulmonary disease in the USA. ClinicoEconomics and Outcomes Research: CEOR. 2013;5:235–245. | ||
Wedzicha JA, Seemungal TA. COPD exacerbations: defining their cause and prevention. Lancet (London, England). 2007;370(9589):786–796. | ||
Seemungal TA, Donaldson GC, Paul EA, Bestall JC, Jeffries DJ, Wedzicha JA. Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;157(5 Pt 1):1418–1422. | ||
GOLD. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management and prevention of chronic pulmonary disease; 2017. Available from: https://goldcopd.org/gold-2017-global-strategy-diagnosis-management-prevention-copd/. Accessed November 05, 2018. | ||
Stynes G, Svedsater H, Wex J, et al. Once-daily fluticasone furoate/vilanterol 100/25 mcg versus twice daily combination therapies in COPD – mixed treatment comparisons of clinical efficacy. Respiratory Research. 2015;16:25. | ||
Dransfield MT, Bourbeau J, Jones PW, et al. Once-daily inhaled fluticasone furoate and vilanterol versus vilanterol only for prevention of exacerbations of COPD: two replicate double-blind, parallel-group, randomised controlled trials. Lancet Respir Med. 2013;1(3):210–223. | ||
Kosoglou T, Hubbell J, Xuan F, et al. Comparison of the systemic bioavailability of mometasone furoate after oral inhalation from a mometasone furoate/formoterol fumarate metered-dose inhaler versus a mometasone furoate dry-powder inhaler in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2013;8:107–116. | ||
Cazzola M, Matera MG. Novel long-acting bronchodilators for COPD and asthma. Br J Pharmacol. 2008;155(3):291–299. | ||
Vaidya SS, Khindri S, Calder N, et al. Pharmacokinetics of indacaterol and mometasone furoate delivered alone or in a free or fixed dose combination in healthy subjects. Pulm Pharmacol Ther. 2016;37:30–36. | ||
Tan RA, Corren J. Mometasone furoate in the management of asthma: a review. Ther Clin Risk Manag. 2008;4(6):1201–1208. | ||
Crim C, Pierre LN, Daley-Yates PT. A review of the pharmacology and pharmacokinetics of inhaled fluticasone propionate and mometasone furoate. Clinical Therapeutics. 2001;23(9):1339–1354. | ||
Calverley PM, Rennard S, Nelson HS, et al. One-year treatment with mometasone furoate in chronic obstructive pulmonary disease. Respiratory Research. 2008;9:73. | ||
Cazzola M, Bardaro F, Stirpe E. The role of indacaterol for chronic obstructive pulmonary disease (COPD). J Thorac Dis. 2013;5(4):559–566. | ||
Battram C, Charlton SJ, Cuenoud B, et al. In vitro and in vivo pharmacological characterization of 5-[(R)-2-(5,6-diethyl-indan-2-ylamino)-1-hydroxy-ethyl]-8-hydroxy-1H-quinolin-2-o ne (indacaterol), a novel inhaled beta(2) adrenoceptor agonist with a 24-h duration of action. J Pharmacol Exp Ther. 2006;317(2):762–770. | ||
Slack RJ, Barrett VJ, Morrison VS, et al. In vitro pharmacological characterization of vilanterol, a novel long-acting beta2-adrenoceptor agonist with 24-hour duration of action. J Pharmacol Exp Ther. 2013;344(1):218–230. | ||
Balint B, Watz H, Amos C, Owen R, Higgins M, Kramer B. Onset of action of indacaterol in patients with COPD: comparison with salbutamol and salmeterol-fluticasone. Int J Chron Obstruct Pulmon Dis. 2010;5:311–318. | ||
Cazzola M, Proietto A, Matera MG. Indacaterol for chronic obstructive pulmonary disease (COPD). Drugs Today (Barc). 2010;46(3):139–150. | ||
GOLD. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management and prevention of chronic pulmonary disease. 2011. Available from: www.goldcopd.org. Accessed November 14, 2018. | ||
Hankinson JL, Odencrantz JR, Fedan KB. Spirometric reference values from a sample of the general U.S. population. Am J Respir Crit Care Med. 1999;159(1):179–187. | ||
Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. European Respiratory Journal. 2005;26(2):319–338. | ||
Mahler DA, Weinberg DH, Wells CK, Feinstein AR. The measurement of dyspnea. Contents, interobserver agreement, and physiologic correlates of two new clinical indexes. Chest. 1984;85(6):751–758. | ||
Jones PW, Quirk FH, Baveystock CM, Littlejohns P. A self-complete measure of health status for chronic airflow limitation. The St. George’s Respiratory Questionnaire. American Review of Respiratory Disease. 1992;145(6):1321–1327. | ||
Jones PW, Harding G, Berry P, Wiklund I, Chen WH, Kline Leidy N. Development and first validation of the COPD Assessment Test. European Respiratory Journal. 2009;34(3):648–654. | ||
Mahler DA, Witek TJ Jr. The MCID of the transition dyspnea index is a total score of one unit. COPD. 2005;2(1):99–103. | ||
Jones PW. St. George’s respiratory questionnaire: MCID. COPD. 2005;2(1):75–79. | ||
Dahl R, Chung KF, Buhl R, et al. Efficacy of a new once-daily long-acting inhaled beta2-agonist indacaterol versus twice-daily formoterol in COPD. Thorax. 2010;65(6):473–479. | ||
Korn S, Kerwin E, Atis S, et al. Indacaterol once-daily provides superior efficacy to salmeterol twice-daily in COPD: a 12-week study. Respir Med. 2011;105(5):719–726. | ||
Kornmann O, Dahl R, Centanni S, et al. Once-daily indacaterol versus twice-daily salmeterol for COPD: a placebo-controlled comparison. Eur Respir J. 2011;37(2):273–279. | ||
GOLD. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management and prevention of chronic pulmonary disease; 2014. Available from: www.goldcopd.org. Accessed November 12, 2018. | ||
Decramer ML, Chapman KR, Dahl R, et al. Once-daily indacaterol versus tiotropium for patients with severe chronic obstructive pulmonary disease (INVIGORATE): a randomised, blinded, parallel-group study. Lancet Respir Med. 2013;1(7):524–533. | ||
Tashkin DP, Doherty DE, Kerwin E, et al. Efficacy and safety characteristics of mometasone furoate/formoterol fumarate fixed-dose combination in subjects with moderate to very severe COPD: findings from pooled analysis of two randomized, 52-week placebo-controlled trials. Int J Chron Obstruct Pulmon Dis. 2012;7:73–86. | ||
Celli BR, Barnes PJ. Exacerbations of chronic obstructive pulmonary disease. Eur Respir J. 2007;29(6):1224–1238. | ||
Rossi A, van der Molen T, del Olmo R, et al. INSTEAD: a randomised switch trial of indacaterol versus salmeterol/fluticasone in moderate COPD. Eur Respir J. 2014;44(6):1548–1556. | ||
Nannini LJ, Lasserson TJ, Poole P. Combined corticosteroid and long-acting beta(2)-agonist in one inhaler versus long-acting beta(2)-agonists for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;(9):CD006829. | ||
Nannini LJ, Poole P, Milan SJ, Holmes R, Normansell R. Combined corticosteroid and long-acting beta(2)-agonist in one inhaler versus placebo for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2013;(11):CD003794. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.