Back to Journals » OncoTargets and Therapy » Volume 8
Increased risk of developing lung cancer in Asian patients carrying the TERT rs2736098 G>A polymorphism: evidence from 3,354 cases and 3,518 controls
Authors Yang Z, Zhang X, Fang S, Tan Y, Yan H, Gu W, Wang J
Received 28 April 2015
Accepted for publication 3 August 2015
Published 30 September 2015 Volume 2015:8 Pages 2757—2765
DOI https://doi.org/10.2147/OTT.S87534
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Faris Farassati
Zhenhua Yang,1,* Xunlei Zhang,2,* Surong Fang,1 Yan Tan,1 Haijun Yan,1 Wei Gu,1 Jianhong Wang2
1Department of Pneumology, Nanjing First Hospital, Nanjing Medical University, Nanjing, 2Department of Medical Oncology, Nantong University Affiliated Tumor Hospital, Nantong, People’s Republic of China
*These authors contributed equally to this work
Background: The association between telomerase reverse transcriptase (TERT) rs2736098 G>A and risk of lung cancer (LC) remains inconclusive. To explore the association more precisely, we performed a comprehensive search and conducted a meta-analysis on all eligible case–control studies involving 3,354 cases and 3,518 controls.
Methods: The 95% confidence interval (95% CI) and the pooled odds ratio (OR) were calculated using a random or fixed effect model. Publication bias, heterogeneity, and sensitivity analysis were also explored.
Results: All studies were case–control studies on LC in patients of Asian descent, consisting of one Korean study and five Chinese studies. Overall, the variant A allele of TERT rs2736098 G>A was found to significantly increase the risk of LC in all genetic models (GA vs GG: OR =1.13, 95% CI =1.02–1.25, P=0.017; AA vs GG: OR =1.78, 95% CI =1.53–2.07, P<0.001;GA/AA vs GG: OR =1.25, 95% CI =1.14–1.38, P<0.001; AA vs GA/GG: OR =1.66, 95% CI =1.45–1.92, P<0.001). In the subgroup analysis, significant associations were found in Chinese group and hospital-based studies. Different genotype test methods showed no influence on the final results.
Conclusion: Our study identified that TERT rs2736098 G>A polymorphism significantly increased the risk of LC in Asian populations.
Keywords: genetic polymorphism, TERT, rs2736098 G>A, lung cancer, meta-analysis
Introduction
Worldwide, lung cancer (LC) is one of the most frequent cancers and the leading cause of cancer-related death.1 It has been estimated that there would be nearly 224,210 newly diagnosed cases and 159,260 deaths caused by LC in United States in 2014.2 The rates of LC are increasing in People’s Republic of China and several other countries in Asia and Africa, where smoking is becoming more prevalent.1 Approximately 80% of the 1.3 billion current smokers worldwide live in low- and middle-income countries, with over 300 million in People’s Republic of China alone.3 Far and away, the greatest cause of LC is the exposure to tobacco smoke through active or passive smoking.1 However, some nonsmokers can also develop LC, suggesting that other risk factors, such as genetic susceptibility, might be of tremendous importance in the development of the disease.4,5
Recently, independent genome-wide association studies (GWAS)6–11 have identified that single nucleotide polymorphisms (SNPs) in some chromosomal regions (such as 15q25, 5p15, and 6p21), which contain genes that regulate nicotinic acetylcholine receptor (nAChR) and telomerase production, are significantly associated with the risk of LC. In addition, 5p15.33, a crucial genomic region for telomere biology, was recently identified as a susceptibility region for LC, where telomerase reverse transcriptase (TERT) and cleft lip and palate transmembrane 1-like gene (CLPTM1L) are located.6,12–17
A common genetic variant, TERT rs2736098, which is located on chromosome 5p15.33, was identified as a susceptibility locus for LC recently in a combined analysis of Icelandic and European sample sets.15 Moreover, several GWAS have investigated the role of the TERT rs2736098 polymorphism in the etiology of LC among Asians, but the results were inconclusive.
Hence, a meta-analysis of six eligible studies18–23 involving 3,354 cases and 3,518 controls was performed to derive a more precise estimation of the overall risk of rs2736098 polymorphism associated with the risk of LC in Asians.
Materials and methods
Identification and eligibility of relevant studies
We searched PubMed, Embase, and MEDLINE (updated to April 30, 2015) using the following search terms: “rs2736098”, “TERT”, “5p15.33”, “genetic susceptibility”, “SNP”, “polymorphism” or “variation”, and “lung cancer”. The literature search was limited to published English manuscripts. The studies selected for our meta-analysis met the following criteria: 1) evaluated the TERT rs2736098 polymorphism and LC risk, 2) the use of a case–control design, and 3) available genotype frequency. We also manually reviewed the reference lists to identify additional relevant studies. This study was a meta-analysis; all the studies we explored provided ethics statements and a statement of informed consent.
Data extraction
Two investigators independently extracted the published data according to the following subjects and reached a consensus on all the items in cases of discordance: the first author’s name, year, country, ethnicity, source of controls, and numbers of genotyped cases and controls. Data were extracted separately whenever possible.
Statistical analysis
All analyses were performed using the Stata software (Version 10.0; StataCorp LP, College Station, TX, USA) using two-sided P-values. The strength of the association between the TERT rs2736098 polymorphism and the risk of LC was assessed by the odds ratio (OR) and the 95% confidence interval (95% CI). The significance of the pooled ORs was determined using the Z-test. The pooled ORs were obtained from the combination of individual studies by heterozygote comparison (GA vs GG), homozygote comparison (AA vs GG), a dominant model (GA/AA vs GG), and a recessive model (AA vs GA/GG). A P-value lesser than 0.05/4 (0.0125) was accepted for statistical significance after Bonferroni correction; multiple comparisons were made four times. Both the I2-statistic for quantifying the proportion of the total variation due to heterogeneity and Cochran’s Q-statistic for testing heterogeneity were calculated to estimate heterogeneity among the selected studies.24,25 If the P-value (Q-test) was >0.05, indicating a lack of heterogeneity across studies, the summary ORs were calculated using the fixed effects model (the Mantel–Haenszel method).26 Otherwise, the random effects model (DerSimonian–Laird method) was used.27 Stratified analyses were also performed by country, source of controls, and genotyping method. Egger’s linear regression test and Funnel plots were used to assess the potential publication bias.28 To evaluate the stability of the results, we performed the sensitivity analyses by deleting one single study each time of the meta-analysis to show the influence of the individual data to the summary ORs.
Results
Characteristics of studies
Figure 1 illustrates the study selection process. A total of six eligible studies that met all inclusion criteria, involving 3,354 cases and 3,518 controls, were included in the pooled analyses. The main characteristics of these studies are shown in Table 1. All studies were case–control studies on LC in patients of Asian descent, consisting of one Korean study and five Chinese studies. Controls in four studies were hospital-based, and other two were population-based. The TERT SNP rs2736098 was genotyped by the TaqMan methodology in three studies and by polymerase chain reaction (PCR) in others.
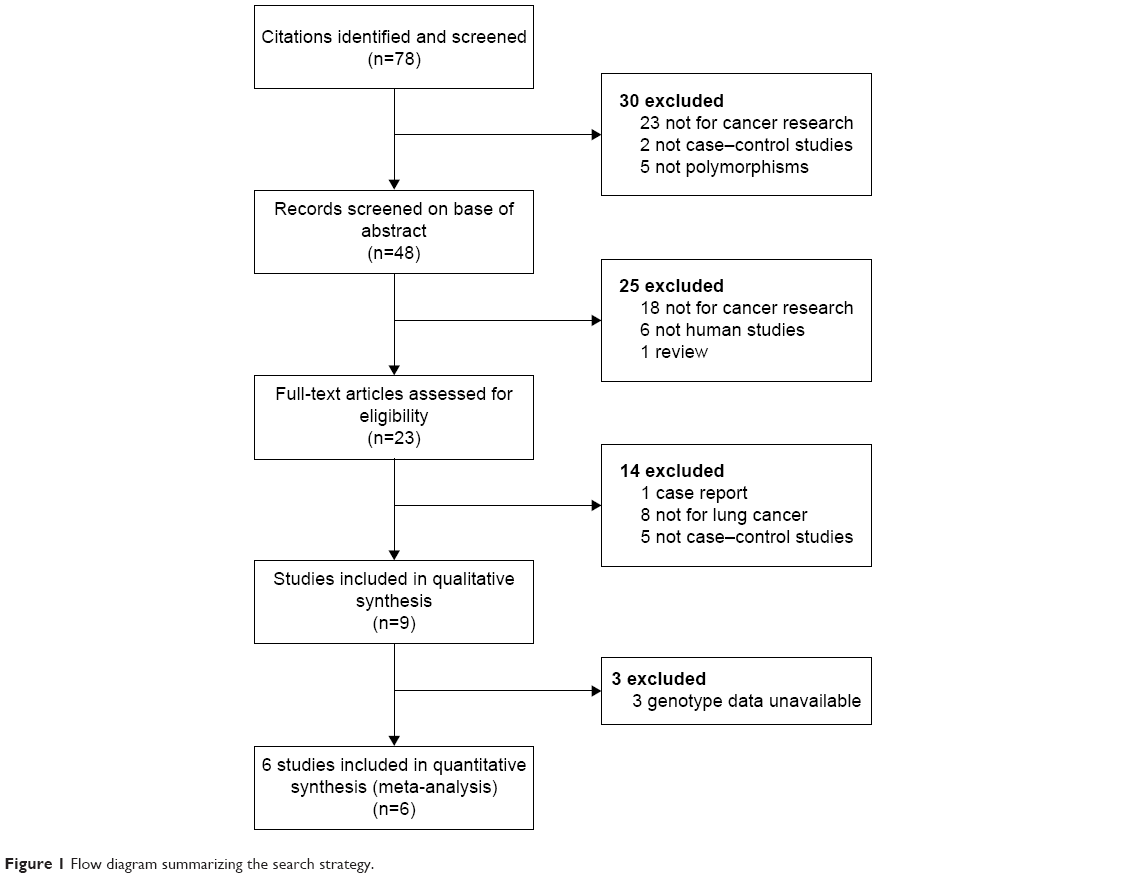 | Figure 1 How diagram summarizing the search strategy |
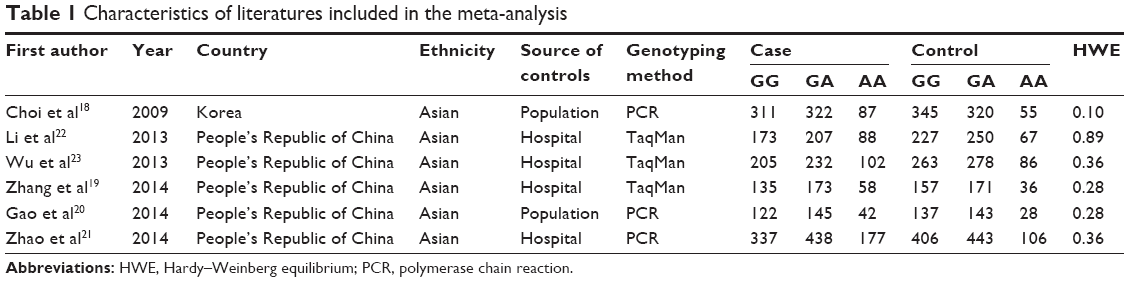 | Table 1 Characteristics of literatures included in the meta-analysis |
Quantitative synthesis
The evaluation of the associations between the TERT rs2736098 polymorphism and the susceptibility to LC are presented in Table 2. Overall, the variant A allele of TERT rs2736098 G>A could significantly increase the risk of LC in all genetic models (heterozygote comparison, GA vs GG: OR =1.13, 95% CI =1.02–1.25, P=0.017, I2=0%; homozygote comparison, AA vs GG: OR =1.78, 95% CI =1.53–2.07, P<0.001, I2=0%; dominant model, GA/AA vs GG: OR =1.25, 95% CI =1.14–1.38, P<0.001, I2=0%; recessive model, AA vs GA/GG: OR =1.66, 95% CI =1.45–1.92, P<0.001, I2=0%) (Figures 2, S1–S3).
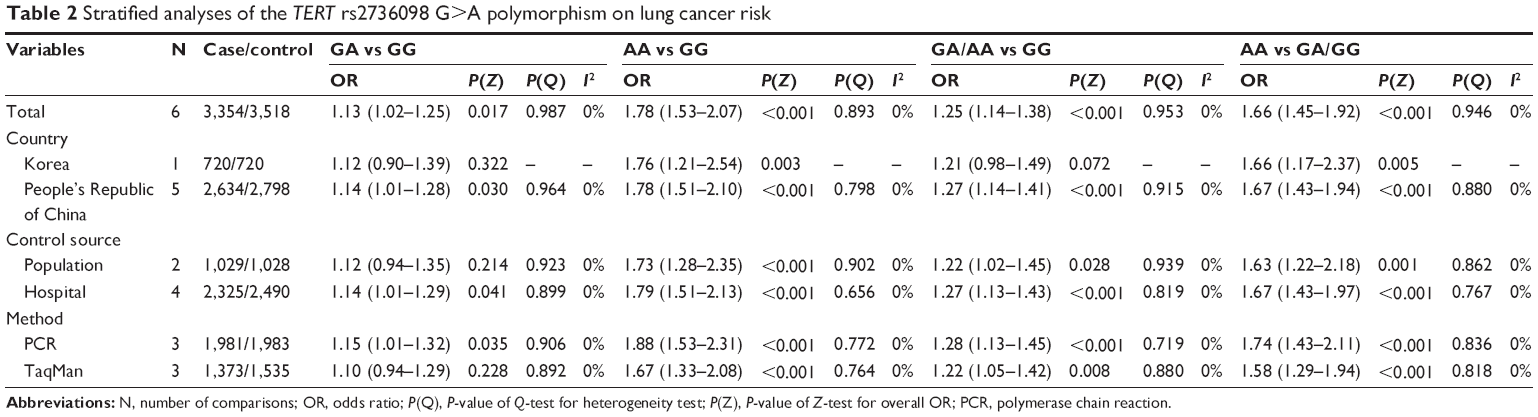 | Table 2 Stratified analyses of the TERT rs2736098 G>A polymorphism on lung cancer risk |
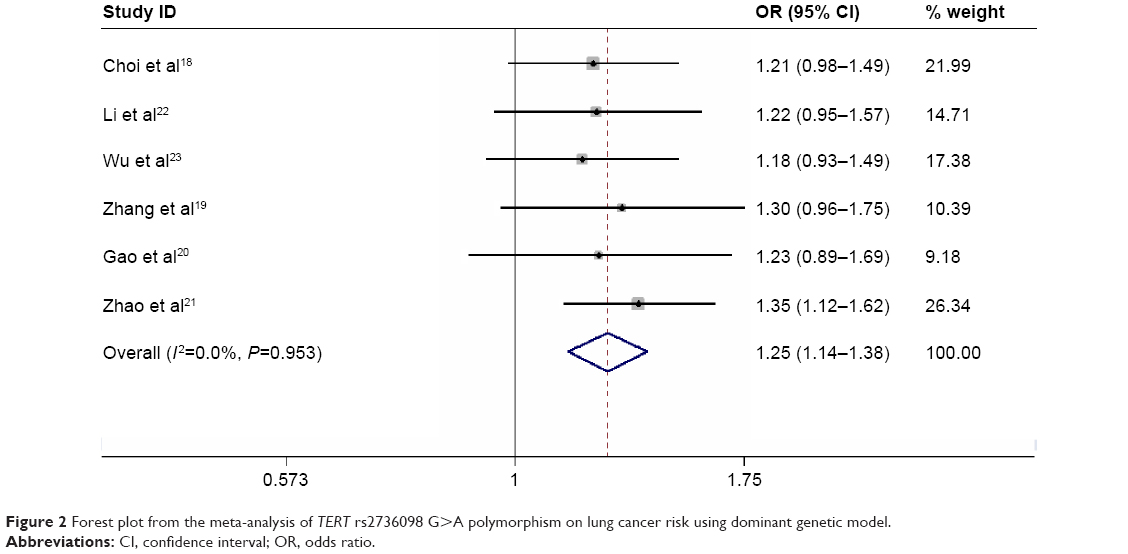 | Figure 2 Forest plot from the meta-analysis of TERT rs2736098 G>A polymorphism on lung cancer risk using dominant genetic model. |
Additionally, in the analysis stratified by countries, all genetic comparison except heterozygote comparison produced significantly increased risks in the Chinese group (GA vs GG: OR =1.14, 95% CI =1.01–1.28, P=0.030, I2=0%; AA vs GG: OR =1.78, 95% CI =1.51–2.10, P<0.001, I2=0%; GA/AA vs GG: OR =1.27, 95% CI =1.14–1.41, P<0.001, I2=0%; AA vs GA/GG: OR =1.67, 95% CI =1.43–1.94, P<0.001, I2=0%). However, significant results were detected only in homozygote comparison and recessive model among Korean group (GA vs GG: OR =1.12, 95% CI =0.90–1.39, P=0.322; AA vs GG: OR =1.76, 95% CI =1.21–2.54, P=0.003; GA/AA vs GG: OR =1.21, 95% CI =0.98–1.49, P=0.072; AA vs GA/GG: OR =1.66, 95% CI =1.17–2.374, P=0.005). Considering the control source, studies with hospital-based controls showed elevated risks in three genetic comparisons (AA vs GG: OR =1.79, 95% CI =1.51–2.13, P<0.001, I2=0%; GA/AA vs GG: OR =1.27, 95% CI =1.134–1.43, P<0.001, I2=0%; AA vs GA/GG: OR =1.67, 95% CI =1.43–1.97, P<0.001, I2=0%). In the studies with population-based controls, significant associations were observed in homozygote comparison (AA vs GG: OR =1.73, 95% CI =1.28–2.35, P<0.001, I2=0%) and recessive model (AA vs GA/GG: OR =1.63, 95% CI =1.22–2.18, P=0.001, I2=0%), but not in dominant model (GA/AA vs GG: OR =1.22, 95% CI =1.02–1.45, P=0.028, I2=0%) and heterozygote comparison (GA vs GG: OR =1.12, 95% CI =0.94–1.35, P=0.214, I2=0%). In the subgroup analysis by genotype test methods, we observed significant association in three genetic comparisons (homozygote comparison, dominant model, and recessive model) in both groups using the TaqMan and PCR method (Table 2).
Test of heterogeneity
When evaluating the association between the TERT rs2736098 polymorphism and the risk of LC, we found that there was no significant heterogeneity for the heterozygote comparison (GA vs GG: Pheterogeneity=0.987, I2=0%), homozygote comparison (AA vs GG: Pheterogeneity=0.893, I2=0%), dominant model comparison (GA/AA vs GG: Pheterogeneity=0.953, I2=0%), and recessive model comparison (AA vs GA/GG: Pheterogeneity=0.946, I2=0%), which indicated that the ethnicity, control source, and genotype test methods in these six studies were similar and equilibrium.
Sensitivity analysis
To evaluate the stability of the results, we performed sensitivity analyses by deleting one single study each time in the meta-analysis, but the corresponding pooled ORs were not altered materially, suggesting that the results of our meta-analyses were statistically stable and reliable (data not shown).
Publication bias
Egger’s test and Begg’s funnel plot were carried out to assess the publication bias of our meta-analyses. Egger’s test was used to provide statistical evidence of funnel plot symmetry. Results did not show any obvious publication bias (GA/AA vs GG: P=0.491). The shape of the funnel plots revealed no evidence of obvious asymmetry (Figure 3 shows the funnel plot of the overall GA/AA vs GG comparisons).
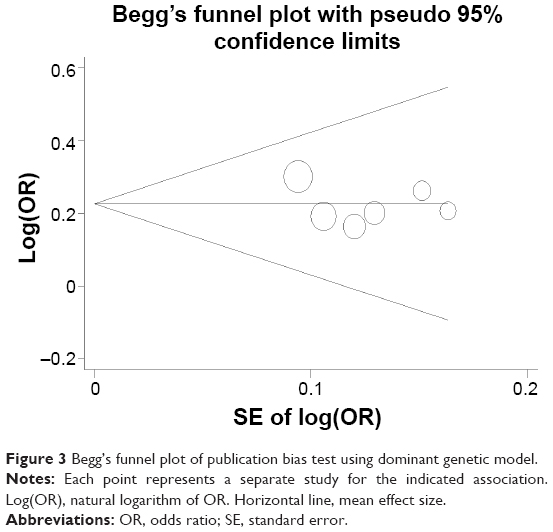 | Figure 3 Begg’s funnel plot of publication bias test using dominant genetic model. |
Discussion
In the current meta-analysis, we ascertained, first, that the TERT rs2736098 G>A polymorphism was significantly associated with increased risk of LC in Asians. In the subgroup analysis, significant associations were found in Chinese group and hospital-based studies. Different genotype test methods showed no influence to the final results.
The TERT gene has been mapped to chromosome 5p15.33, which consists of 16 exons and 15 introns spanning 35 kb of genomic DNA.15 TERT is the rate-limiting catalytic subunit of the telomerase enzyme required for maintenance of telomere DNA length.29 The length of telomeres gradually decreases with each cell division, increasing age, or mutations in structural proteins. It has been known that telomere is essential for the preservation of chromosomal integrity and stability, cellular immortality, and various carcinogeneses.30–32 Human telomerase activity is suppressed in most somatic tissues during differentiation but strongly upregulated in tumors. Additionally, telomerase may drive tumor progression and metastasis by activation of the glycolytic pathway.33 Telomere dysfunction is an essential feature in carcinogenesis, implicating the involvement of in multiple cancers, including that of breast, head and neck, bladder, cervical, colorectal, glioma, and hepatocellular carcinoma.18,34–39
TERT rs2736098 is localized to the second exon of the telomerase gene TERT. Zhang et al40 found that the rs2736098 A allele contributed significantly to hepatocellular carcinoma risk. In a Polish study of 1,995 breast cancer cases and 2,296 controls, Savage et al38 found no evidence that the TERT rs2736098 polymorphism at 5p15.33 was associated with breast cancer risk. Recently, independent GWAS1,3,6,18,19,23 have focused on the association between TERT rs2736098 and LC risk. This SNP was first identified as a susceptibility locus for LC in a combined analysis of Icelandic and European sample sets.18 More recently, a study of 501 cancer cases in Chinese women and 576 cancer-free controls also found that the variant allele of rs2736098 was significantly associated with increased risk of LC, especially in lung adenocarcinomas.22
Although several studies have investigated the role of rs2736098 polymorphism in LC risk, the clinical relevance of this polymorphic gene remains inconclusive. Thus, this meta-analysis of the association between the TERT rs2736098 G>A polymorphisms and risk of LC was performed. The present meta-analysis, comprising 3,354 cases and 3,518 controls, explored the association between TERT rs2736098 polymorphisms and LC risk. It was observed that the TERT rs2736098 polymorphism was significantly correlated with increased risk of LC. In the stratified analysis by countries, control groups, and genotype test methods, similar results were found in these subgroups. Our meta-analysis proved that A allele of TERT rs2736098 G>A variant was a low-penetrant risk factor for the development of LC.
As with all meta-analyses, some limitations of our analysis might have affected the objectivity of the conclusions, which must be considered when interpreting the results. First, further evaluation of the potential interactions was limited because of the lack of original data in some studies, such as pathological subtypes of cancer. Second, unadjusted estimates were applied in our meta-analysis owing to the lack of adjusted estimates, which might have caused serious confounding bias. A more precise evaluation should be conducted if more detailed individual data become available, such as age, sex, smoking states, and histological types. Third, because all the patients in the six studies were Asians, we could not infer the risk in Europeans due to the differences in genetic backgrounds and environmental and lifestyle contexts (such as dietary habits and tobacco smoke).12
In spite of certain limitations, the present meta-analysis provided significant information. First, we estimated the association conclusively between the TERT rs2736098 G>A polymorphism and LC risk, and further showed the significant association especially among Chinese rather than Korean population. This study may also provide a potential genetic marker and new insight into the etiology of LC. Second, substantial numbers of cases and controls were pooled from different studies, which significantly increased the statistical power of the analysis and made our meta-analysis more comprehensive and persuasive. Third, no heterogeneity and publication biases were detected, indicating that the results were likely reliable and unbiased.
Conclusion
In conclusion, our meta-analysis suggests that the TERT rs2736098 G>A polymorphism is associated with increased risk of LC among Asians. The insight from this study predicts the TERT rs2736098 G>A polymorphism as a potential genetic marker in the etiology of LC and will probably be a potential therapeutic target for new drugs. Nevertheless, we suggest that larger and well-designed multicentric studies including samples stratified by a genetic–environmental interaction should be carried out to fully clarify the roles of the TERT rs2736098 polymorphisms in the etiology of LC.
Acknowledgments
This work was supported by the Science and Technology Commission of Nanjing, People’s Republic of China (grant number 2014048) and the Health and Family Planning Commission of Nantong, People’s Republic of China (grant number WQ2015052).
Disclosure
The authors report no conflicts of interest in this work.
References
Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. | ||
Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014;64:9–29. | ||
Brawley OW. Avoidable cancer deaths globally. CA Cancer J Clin. 2011;61:67–68. | ||
Brennan P, Hainaut P, Boffetta P. Genetics of lung-cancer susceptibility. Lancet Oncol. 2011;12:399–408. | ||
Baba H, Muro K, Yasui H. Updated results of the FIRIS study: a phase II/III trial of 5-FU/l-leucovorin/irinotecan (FOLFIRI) versus irinotecan/S-1 (IRIS) as second-line chemotherapy for metastatic colorectal cancer (mCRC) [abstract]. J Clin Oncol. 2011;29:3562. | ||
McKay JD, Hung RJ, Gaborieau V, et al. Lung cancer susceptibility locus at 5p15.33. Nat Genet. 2008;40:1404–1406. | ||
Landi MT, Chatterjee N, Yu K, et al. A genome-wide association study of lung cancer identifies a region of chromosome 5p15 associated with risk for adenocarcinoma. Am J Hum Genet. 2009;85:679–691. | ||
Wang Y, Broderick P, Webb E, et al. Common 5p15.33 and 6p21.33 variants influence lung cancer risk. Nat Genet. 2008;40:1407–1409. | ||
Thorgeirsson TE, Geller F, Sulem P, et al. A variant associated with nicotine dependence, lung cancer and peripheral arterial disease. Nature. 2008;452:638–642. | ||
Hung RJ, McKay JD, Gaborieau V, et al. A susceptibility locus for lung cancer maps to nicotinic acetylcholine receptor subunit genes on 15q25. Nature. 2008;452:633–637. | ||
Amos CI, Wu X, Broderick P, et al. Genome-wide association scan of tag SNPs identifies a susceptibility locus for lung cancer at 15q25.1. Nat Genet. 2008;40:616–622. | ||
Hirschhorn JN, Lohmueller K, Byrne E, Hirschhorn K. A comprehensive review of genetic association studies. Genet Med. 2002;4:45–61. | ||
Jin G, Xu L, Shu Y, et al. Common genetic variants on 5p15.33 contribute to risk of lung adenocarcinoma in a Chinese population. Carcinogenesis. 2009;30:987–990. | ||
Kang JU, Koo SH, Kwon KC, Park JW, Kim JM. Gain at chromosomal region 5p15.33, containing TERT, is the most frequent genetic event in early stages of non-small cell lung cancer. Cancer Genet Cytogenet. 2008;182:1–11. | ||
Rafnar T, Sulem P, Stacey SN, et al. Sequence variants at the TERT-CLPTM1L locus associate with many cancer types. Nat Genet. 2009;41:221–227. | ||
Zienolddiny S, Skaug V, Landvik NE, et al. The TERT-CLPTM1L lung cancer susceptibility variant associates with higher DNA adduct formation in the lung. Carcinogenesis. 2009;30:1368–1371. | ||
Hsiung CA, Lan Q, Hong YC, et al. The 5p15.33 locus is associated with risk of lung adenocarcinoma in never-smoking females in Asia. PLoS Genet. 2010;6:e1001051. | ||
Choi JE, Kang HG, Jang JS, et al. Polymorphisms in telomere maintenance genes and risk of lung cancer. Cancer Epidemiol Biomarkers Prev. 2009;18:2773–2781. | ||
Zhang Y, Zhao M, Shen L, et al. Genetic polymorphisms of TERT and CLPTM1L and risk of lung cancer: a case-control study in northeast Chinese male population. Med Oncol. 2014;31:18. | ||
Gao L, Thakur A, Liang Y, et al. Polymorphisms in the TERT gene are associated with lung cancer risk in the Chinese Han population. Eur J Cancer Prev. 2014;23:497–501. | ||
Zhao MM, Zhang Y, Shen L, et al. Genetic variations in TERT-CLPTM1L genes and risk of lung cancer in a Chinese population. Asian Pac J Cancer Prev. 2014;15:2809–2813. | ||
Li C, Yin Z, Wu W, Li X, Ren Y, Zhou B. Genetic variations in TERT-CLPTM1L genes and risk of lung cancer in Chinese women nonsmokers. PLoS One. 2013;8:e64988. | ||
Wu H, Qiao N, Wang Y, et al. Association between the telomerase reverse transcriptase (TERT) rs2736098 polymorphism and cancer risk: evidence from a case-control study of non-small-cell lung cancer and a meta-analysis. PLoS One. 2013;8:e76372. | ||
Cochran WG. The comparison of percentages in matched samples. Biometrika. 1950;37:256–266. | ||
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–560. | ||
Mantel N, Haenszel W. Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst. 1959;22:719–748. | ||
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177–188. | ||
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–634. | ||
Lantuejoul S, Salon C, Soria JC, Brambilla E. Telomerase expression in lung preneoplasia and neoplasia. Int J Cancer. 2007;120:1835–1841. | ||
Weinrich SL, Pruzan R, Ma L, et al. Reconstitution of human telomerase with the template RNA component hTR and the catalytic protein subunit hTRT. Nat Genet. 1997;17:498–502. | ||
Feldser DM, Hackett JA, Greider CW. Telomere dysfunction and the initiation of genome instability. Nat Rev Cancer. 2003;3:623–627. | ||
Rodier F, Kim SH, Nijjar T, Yaswen P, Campisi J. Cancer and aging: the importance of telomeres in genome maintenance. Int J Biochem Cell Biol. 2005;37:977–990. | ||
Bagheri S, Nosrati M, Li S, et al. Genes and pathways downstream of telomerase in melanoma metastasis. Proc Natl Acad Sci U S A. 2006;103:11306–11311. | ||
Chen H, Chen Y, Zhao Y, et al. Association of sequence variants on chromosomes 20, 11, and 5 (20q13.33, 11q23.3, and 5p15.33) with glioma susceptibility in a Chinese population. Am J Epidemiol. 2011;173:915–922. | ||
Gago-Dominguez M, Jiang X, Conti DV, et al. Genetic variations on chromosomes 5p15 and 15q25 and bladder cancer risk: findings from the Los Angeles-Shanghai bladder case-control study. Carcinogenesis. 2011;32:197–202. | ||
Hofer P, Baierl A, Bernhart K, et al. Association of genetic variants of human telomerase with colorectal polyps and colorectal cancer risk. Mol Carcinog. 2012;51(suppl 1):E176–E182. | ||
Liu Z, Li G, Wei S, et al. Genetic variations in TERT-CLPTM1L genes and risk of squamous cell carcinoma of the head and neck. Carcinogenesis. 2010;31:1977–1981. | ||
Savage SA, Chanock SJ, Lissowska J, et al. Genetic variation in five genes important in telomere biology and risk for breast cancer. Br J Cancer. 2007;97:832–836. | ||
Wang S, Wu J, Hu L, et al. Common genetic variants in TERT contribute to risk of cervical cancer in a Chinese population. Mol Carcinog. 2012;51(suppl 1):E118–E122. | ||
Zhang C, Tian YP, Wang Y, Guo FH, Qin JF, Ni H. hTERT rs2736098 genetic variants and susceptibility of hepatocellular carcinoma in the Chinese population: a case-control study. Hepatobiliary Pancreat Dis Int. 2013;12:74–79. |
Supplementary materials
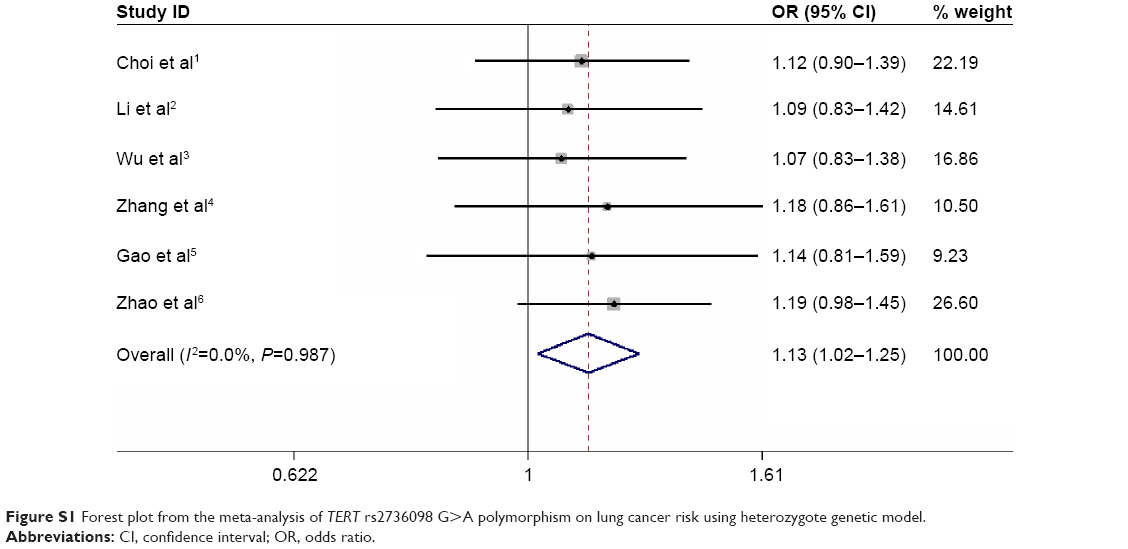 | Figure S1 Forest plot from the meta-analysis of TERT rs2736098 G>A polymorphism on lung cancer risk using heterozygote genetic model. |
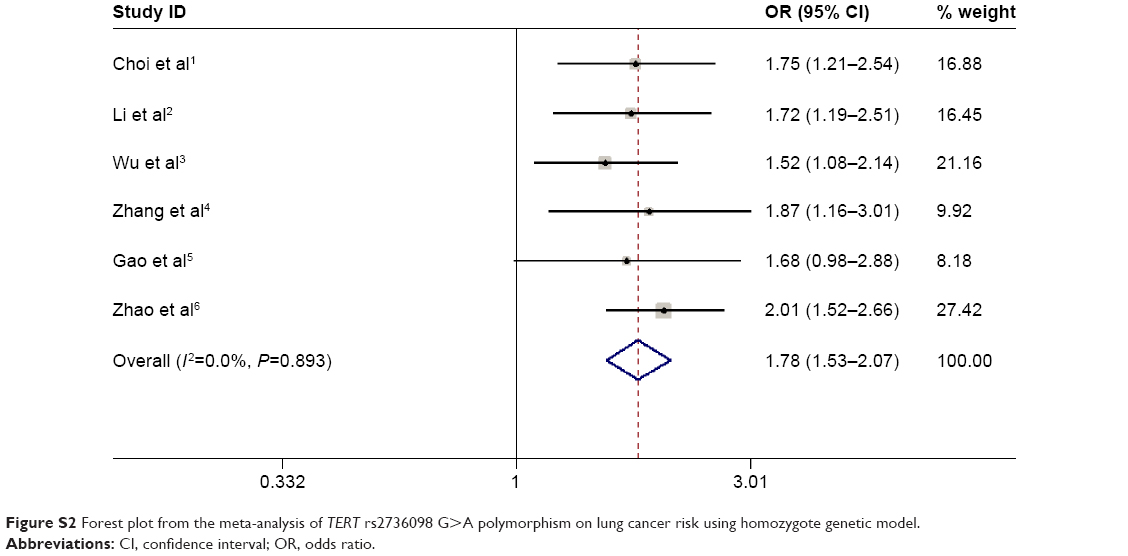 | Figure S2 Forest plot from the meta-analysis of TERT rs2736098 G>A polymorphism on lung cancer risk using homozygote genetic model. |
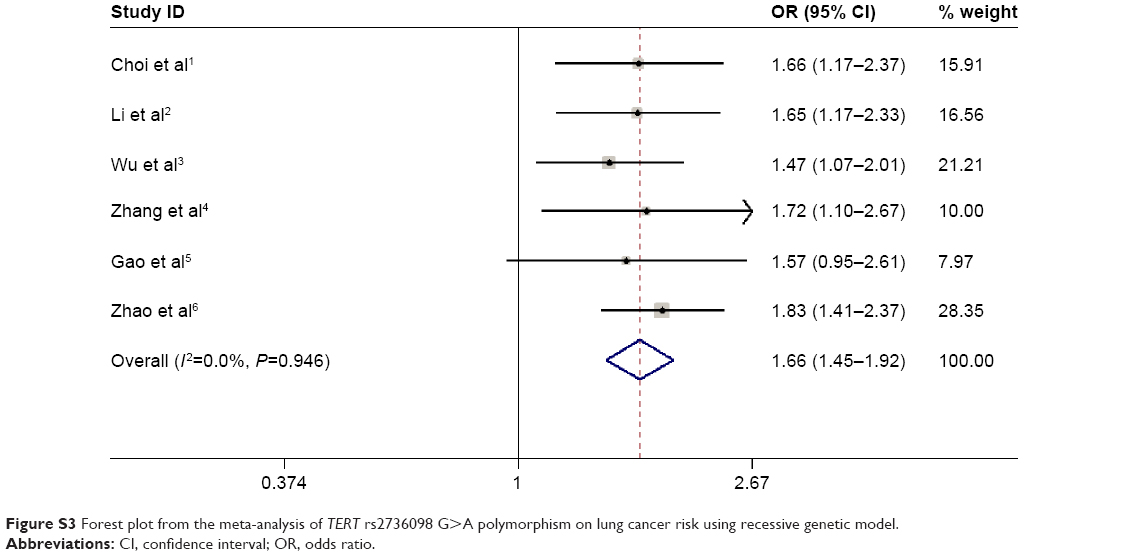 | Figure S3 Forest plot from the meta-analysis of TERT rs2736098 G>A polymorphism on lung cancer risk using recessive genetic model. |
References
Choi JE, Kang HG, Jang JS, et al. Polymorphisms in telomere maintenance genes and risk of lung cancer. Cancer Epidemiol Biomarkers Prev. 2009;18:2773–2781. | ||
Li C, Yin Z, Wu W, Li X, Ren Y, Zhou B. Genetic variations in TERT-CLPTM1L genes and risk of lung cancer in Chinese women nonsmokers. PLoS One. 2013;8:e64988. | ||
Wu H, Qiao N, Wang Y, et al. Association between the telomerase reverse transcriptase (TERT) rs2736098 polymorphism and cancer risk: evidence from a case-control study of non-small-cell lung cancer and a meta-analysis. PLoS One. 2013;8:e76372. | ||
Zhang Y, Zhao M, Shen L, et al. Genetic polymorphisms of TERT and CLPTM1L and risk of lung cancer: a case-control study in northeast Chinese male population. Med Oncol. 2014;31:18. | ||
Gao L, Thakur A, Liang Y, et al. Polymorphisms in the TERT gene are associated with lung cancer risk in the Chinese Han population. Eur J Cancer Prev. 2014;23:497–501. | ||
Zhao MM, Zhang Y, Shen L, et al. Genetic variations in TERT-CLPTM1L genes and risk of lung cancer in a Chinese population. Asian Pac J Cancer Prev. 2014;15:2809–2813. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.