Back to Journals » Risk Management and Healthcare Policy » Volume 13
Increased Blood Lipid Level is Associated with Cancer-Specific Mortality and All-Cause Mortality in Patients with Colorectal Cancer (≥65 Years): A Population-Based Prospective Cohort Study
Authors Yang Y ![]() , Gao G, Shi J, Zhang J
, Gao G, Shi J, Zhang J ![]()
Received 27 April 2020
Accepted for publication 8 July 2020
Published 23 July 2020 Volume 2020:13 Pages 855—863
DOI https://doi.org/10.2147/RMHP.S260113
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
This paper is retracted.
Yong Yang, Ge Gao, Jun Shi, Jiangnan Zhang
Department of General Surgery, The First Affiliated Hospital of Nanchang University, Nanchang 330006, Jiangxi, People’s Republic of China
Correspondence: Ge Gao; Jiangnan Zhang
Department of General Surgery, The First Affiliated Hospital of Nanchang University, No. 17 Yongwaizheng Street, Donghu District, Nanchang City, Jiangxi Province, People’s Republic of China
Tel +86 15279133591; +86 13607042729
Email [email protected]; [email protected]
Background: Hyperlipidaemia is related to the development of many cancers. The aim of this study was to explore whether blood lipid levels were associated with increased rates of cancer-specific mortality and all-cause mortality in patients with colorectal cancer (CRC).
Methods: Data on 8504 participants from The Irish Longitudinal Study on Ageing (TILDA) were analysed. A total of 304 participants with CRC who had experienced curative surgery were included. Logistic regression analysis was performed to analyse the relationship between blood lipid levels and CRC severity. Cox regression analysis was performed to assess the association between blood lipid levels and cancer-specific mortality and all-cause mortality in patients with CRC.
Results: In 304 patients with CRC, the average age was 67.8± 5.4 years. The logistic regression analysis indicated that elevated levels of total cholesterol (2.104 [1.358– 3.650]; P-trend< 0.001), triglycerides (1.665 [1.337– 2.076]; P-trend=0.005) and LDL (2.127 [1.446– 4.099]; P-trend< 0.001) but not HDL (0.688 [0.409– 1.252]; P-trend=0.124) were associated with an increased risk of higher CRC stage after adjustments were made for age, sex, marital status, BMI, drinking status, smoking status, education, physical activity, antilipidaemic medications and self-reported CVDs (≥ 2). Cox proportional hazard analysis showed that higher blood lipid levels of total cholesterol, triglycerides and LDL were independently associated with higher rates of cancer-specific mortality and all-cause mortality. Similar results persisted in the sensitivity analysis using antilipidaemic medications as an additional covariate and the stratification analysis using antilipidaemic medications as a stratified variable.
Conclusion: Increased blood lipid levels were associated with an increased risk of cancer-specific mortality and all-cause mortality in patients with CRC after adjusting for potential confounding factors. Clinicians should pay more attention to the prognostic value of increased blood lipids in patients with CRC for the risk of death.
Keywords: blood lipids, colorectal cancer, cancer-specific mortality, all-cause mortality, prognostic value
Introduction
As one of the tumours of the digestive system, colorectal cancer (CRC) is an important cause of cancer-related deaths worldwide.1,2 Compared with patients with CRC with distant metastases, the five-year survival rate is significantly higher in patients with early-stage disease (>90% vs 10–15%).3 Distant metastasis of cancer cells leads to poor prognosis and high mortality in patients with CRC, and the liver is the most important target site of CRC metastasis.4,5 Existing studies have suggested that hyperlipidaemia could exacerbate some severe diseases, such as cardiovascular diseases (CVDs), and it has already been considered a risk predictor for CVDs and CVD-related death.6,7
Epidemiologic studies have demonstrated that lipid metabolism disorders have an important impact on the progression of many cancers, such as breast and prostate cancer.8,9 Recent studies have also found the important role of blood lipids in CRC progression. For instance, reduced high-density lipoprotein cholesterol (HDL) levels or increased total cholesterol, triglycerides and low-density lipoprotein cholesterol (LDL) levels have been associated with elevated levels of pro-inflammatory cytokines, including interleukin-6 (IL-6) and tumour necrosis factor-a (TNF-a). These inflammatory cytokines can promote the growth and proliferation of CRC cells.10 Some studies have also suggested that high levels of blood lipids caused by a high-fat and/or high-sugar diet could stimulate the development of CRC.11 A lifestyle of a high-fat and/or high-sugar diet leads to increased CRC cell stemness and enhanced stemness, which stimulate the migration ability of cancer cells.12 A poor lifestyle also enhances macrophage infiltration, which promotes the migration of CRC cells to distant organs.13,14 Additionally, consumption of a high-fat and/or high-sugar diet by patients with CRC can promote more reactive oxygen species (ROS), which eventually stimulate the progression of CRC metastasis.5
Considering the role of blood lipids in the progression of CRC, we speculate that the increased lipid level is closely related to the prognosis of patients with CRC.15–17 Until now, however, few prospective clinical studies have investigated the prognostic value of hyperlipidaemia for predicting the prognosis of CRC.18 The main purpose of this study was to explore the association of blood lipid levels, including total cholesterol, triglycerides, LDL and HDL, with cancer-specific mortality and all-cause mortality in patients with CRC in a four-year cohort study. Clinical evidence has recently shown that statin use is associated with a reduced rate of CRC-related mortality.19 Therefore, we further determined whether statins could improve the prognostic value of blood lipids in patients with CRC by sensitivity and stratification analyses.
Materials and Methods
Methods
Study Sample
The Irish Longitudinal Study on Ageing (TILDA) comprising middle-aged and elderly adults (age ≥49 years) is a large prospective cohort study with repeated assessments at 2-year intervals in the Republic of Ireland. A nationally representative sample was obtained from all residential addresses in the Republic of Ireland by use of the RANSAM sampling procedure, with a response rate of 62% at wave 1 (2009–2011).20 Details on the method and design of the cohort study have been published elsewhere.20 The TILDA study mainly consisted of 1) a self-completed questionnaire; 2) a computer-aided personal interview (CAPI) performed by trained interviewers in the included subjects’ homes; and 3) a health examination performed by well-trained research nurses. All subjects who completed the CAPI and self-completed questionnaire were invited to attend one of the two health centres for health examination, including risk assessments of cancers and biochemical tests. We obtained data from TILDA so that we had enough variables to analyse the association of blood lipids with the prognosis in patients with CRC. Our study included patients with CRC who completed the CAPI, the self-completed questionnaire and the health examination at wave 1 and health examination at wave 3 (a follow-up period of 4 years). In this study, we found that 94 patients had a long history of statin use (≥12 months) from the self-completed questionnaire or CAPI. To achieve the purpose of the study, the study cohort was composed of 304 patients with CRC (aged ≥65 years) who were newly histologically diagnosed with stage I, II, or III CRC according to the “International Classification of Diseases for Oncology (Third Revision)” and had experienced curative surgery at wave 1. In addition, we included 124 subjects without CRC as healthy controls (stage 0). Patients with CRC with a history of other primary cancer types were excluded. Details on the method of inclusion of the cohort study are shown in Figure 1. The TILDA protocol was approved by the Trinity College Research Ethics Committee, and all participants gave written informed consent. We got most of TILDA’s data through a website, which is a data sharing platform for researchers to use it for free worldwide. We have obtained their consent by signing an electronic agreement. According to the Declaration of Helsinki guidelines, the Ethics Committee of The First Affiliated Hospital of Nanchang University approved this study.
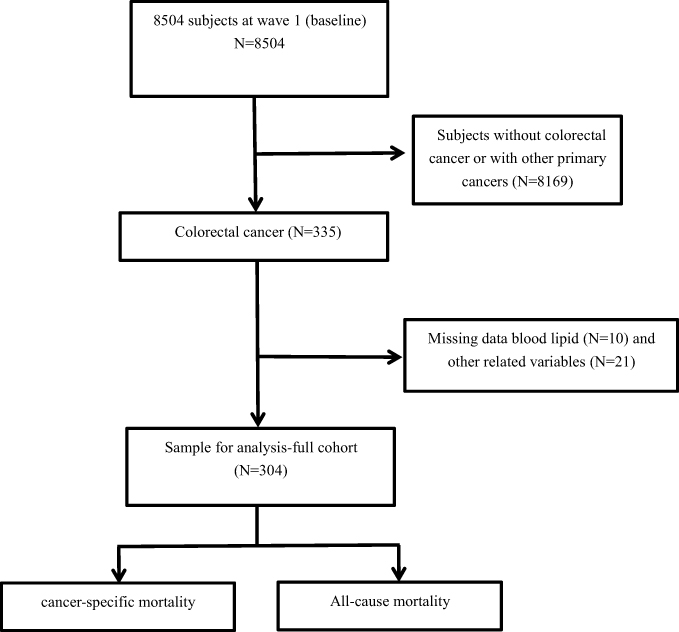 |
Figure 1 The flow chart of subjects included in the study. |
Blood Lipid Measurements
The details of blood collection, handling, storage, and lipid measurement are available elsewhere.20 In summary, serum levels of total cholesterol and triglycerides were tested by using enzymatic methods.21 Blood HDL levels were determined after precipitation of non-HDL lipoproteins.22 Blood LDL levels were calculated using the Friedewald equation.23 Blind-duplicate coefficients of variation ranged from 5% to 10%.
End Point Definitions
All included patients with CRC were followed up for 48 months. The end points were defined as cancer-specific mortality and all-cause mortality. Follow-up from the day of cancer diagnosis to the day of death from cancer for patients with CRC was performed to determine cancer-specific survival rates. Follow-up from the day of cancer diagnosis to the day of death from all causes was performed to determine overall survival rates. Patients with CRC who died of other causes were censored. These follow-up data were recorded by routine visits and telephone contacts. Details on the method and design of the follow-up were published elsewhere.20
Covariates
Sociodemographic characteristics and lifestyle factors, including age, sex, marital status, body mass index (BMI), drinking status, smoking status, education and physical activity, were obtained from the CAPI. The CAPI also collected data on self-reported CVD comorbidities, including hypertension, heart failure, myocardial infarction, diabetes mellitus and stroke. Marital status was defined as “married” or “not married”. Smoking status was classified as “current smoker, past smoker, or never smoker”. Drinking status was also classified as “current drinker, past drinker, or never drinker”. Education was defined as
primary [some primary (not complete), primary or equivalent], secondary (intermediate/junior/group certificate or equivalent or leaving certificate or equivalent or diploma/certificate) and high. (primary degree or postgraduate/higher degree)
Physical activity was divided into three levels (level 0, level 1 and level 2; the higher the level, the more exercise was performed). Self-reported CVD comorbidities were dichotomized as “yes” or “no”. Antilipidaemic medications (statin use) were also recorded by the CAPI and were dichotomized as “yes” or “no”.
Statistical Analysis
The normality of the data was analysed by the Kolmogorov–Smirnov (KS) test combined with Q-Q plots. All the continuous variables in this study are normally distributed or approximate normal distributions and are expressed as the mean ± standard deviation (M ± SD). Categorical variables are shown as n (%). CRC stage was categorized by quartiles (stage 0, stage I, stage II, and stage III). Logistic regression was performed to examine the associations between blood lipid levels (total cholesterol, triglycerides, LDL and HDL) at baseline (wave 1) and with the CRC stage, with stage 0 as the reference category. Stage 0 was defined as patients without other serious diseases. The confounding factors, including age, sex, marital status, BMI, drinking status, smoking status, education, physical activity, antilipidaemic medications and self-reported CVDs (≥2), were adjusted in the multivariate analysis. Then, multivariate Cox proportional hazard analysis was performed to identify the independent associations between blood lipid levels and cancer-specific mortality and all-cause mortality in patients with CRC.
To further examine the prognostic value of blood lipid levels for predicting cancer-specific mortality and all-cause mortality in patients with CRC, sensitivity analysis was used by adding antilipidaemic medications (statin use) as a covariate in the Cox proportional hazard model. We also analysed the associations by using self-reported CVDs (≥2) as a stratified variable. P ≤ 0.05 was considered to be statistically significant in all analyses. Data were analysed by using SPSS 24.0 and R 3.5.1.
Results
Baseline Characteristics of the Study Cohort
Of 304 participants in wave 1 (Table 1), 145 were men and 159 were women. The age (M ± SD) was 67.8 ± 5.4 years. A total of 80.2% of patients were currently married, and the BMI was 28.5 ± 3.7. Many patients were past (48.7%) or current smokers (14.8%), as well past (50.0%) or current drinkers (9.2%). A total of 22.7% of patients had higher educational levels, and 42.4% of participants had higher levels of physical activity. A total of 22.4% of the participants had self-reported CVDs (≥2).
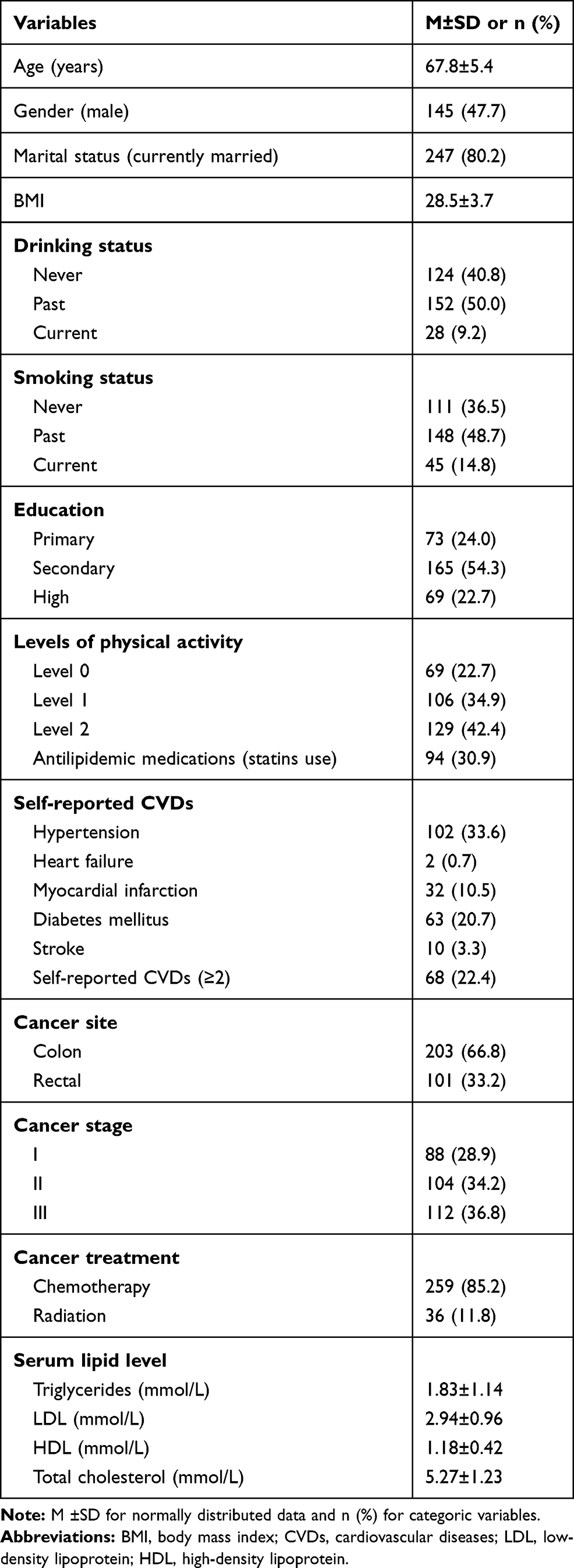 |
Table 1 Baseline Characteristics at Baseline (N=304) |
Logistic Regression Analysis for the Association Between Cancer Stage and Blood Lipid Levels in Patients with CRC at Baseline
To determine the association of blood lipid levels, including total cholesterol, triglycerides, LDL and HDL, with cancer stage (0 ~ III) in patients with CRC, multivariate logistic regression analysis was performed (Table 2). The crude model indicated that elevated levels of total cholesterol, triglycerides and LDL were associated with an increased risk of higher cancer stage after non-adjustment. After adjustments were made for age and sex, the results in Model 1 were similar to those of the crude model. This association remained statistically significant and changed little when marital status, BMI, drinking status, smoking status, education, physical activity, antilipidaemic medications and self-reported CVDs (≥2) were added to Model 1 (Model 2). For HDL, our results showed that HDL was associated with an increased risk of higher cancer stage in the crude model. However, the association did not exist in Model 1 and Model 2 after other confounding factors were adjusted.
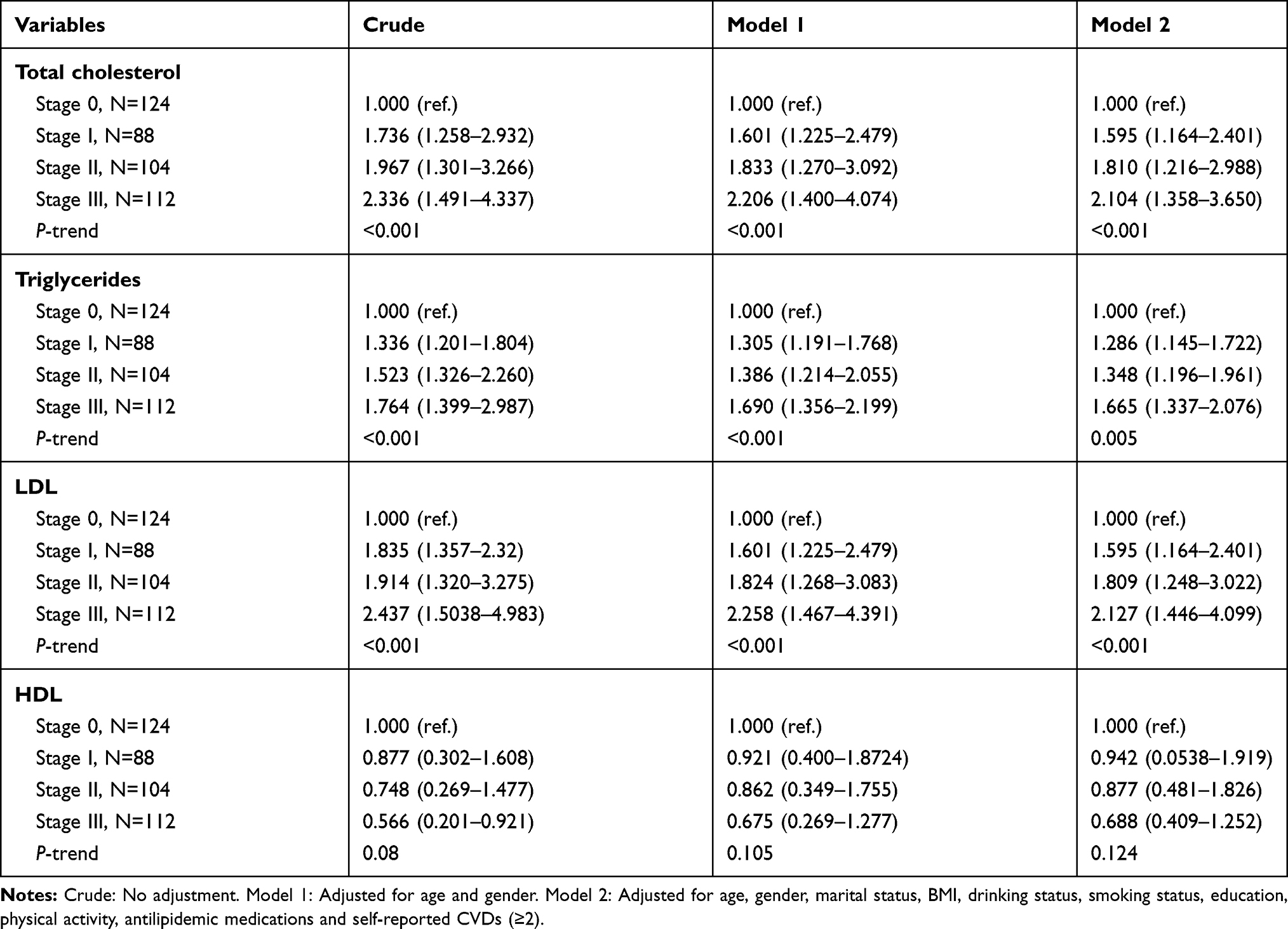 |
Table 2 Logistic Regression Analysis of the Relationship Between the Cancer Stage and Blood Lipid Levels in Patients with CRC |
Cox Proportional Hazard Model for the Association of Blood Lipid Levels with Cancer-Specific Mortality and All-Cause Mortality During the Follow-Up Period
All included patients (N=304) were followed up for a median period of 48 months. As a result, 88 patients died during the follow-up period. Seventy-three of those patients died due to CRC, and 15 deaths were caused by CVDs or diseases. In addition to HDL in this study (Table 3), we found that the increased levels of blood lipids, including total cholesterol, triglycerides and LDL, were positively correlated with higher cancer-specific mortality and all-cause mortality after adjustments were made for age, sex, marital status, BMI, drinking status, smoking status, education, physical activity, cancer stage and cancer treatment. Similarly, the Cox proportional hazard model (Table 4) also showed a significant association between blood lipid levels (total cholesterol, triglycerides and LDL) and cancer-specific mortality and all-cause mortality by sensitivity analysis using antilipidaemic medications as an additional covariate.
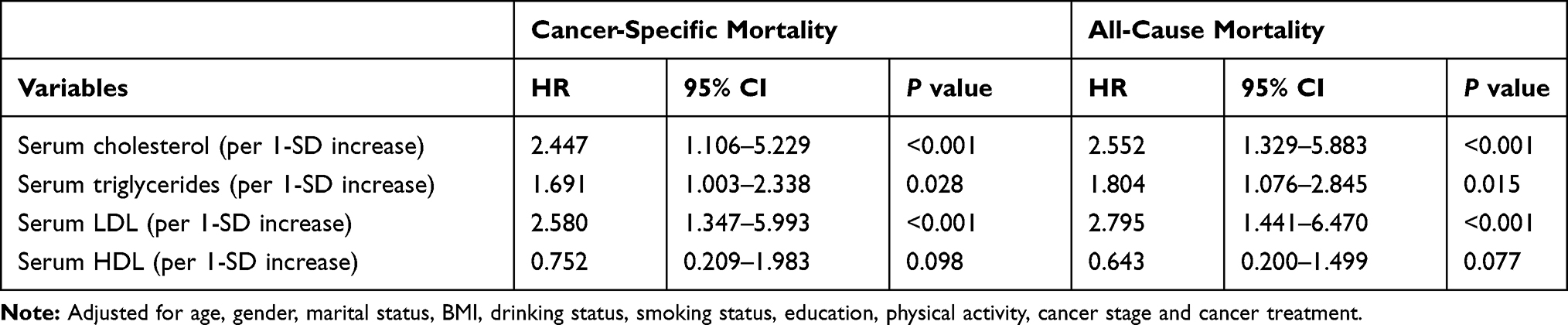 |
Table 3 Cox Proportional Hazard Model for Association of Blood Lipid Levels with Cancer-Specific Mortality and All-Cause Mortality |
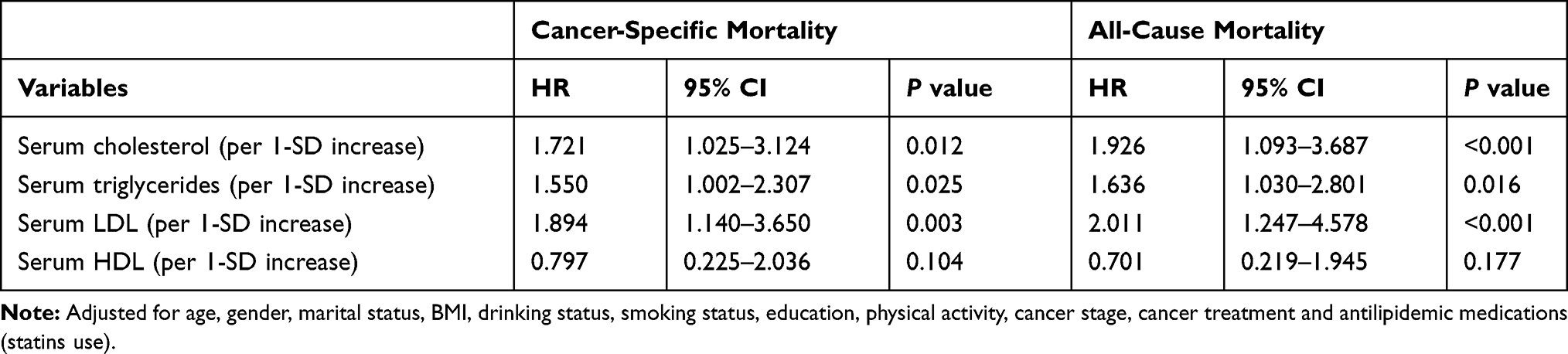 |
Table 4 Cox Proportional Hazard Model for Association of Blood Lipid Levels with Cancer-Specific Mortality and All-Cause Mortality by Sensitivity Analysis |
Cox Proportional Hazard Model for the Association of Blood Lipid Levels with Cancer-Specific Mortality and All-Cause Mortality Stratified by Self-Reported CVDs (≥2)
All patients were divided into two groups according to self-reported CVDs (≥2). Our results showed that higher blood lipid levels, including total cholesterol, triglycerides and LDL, were independently associated with a higher risk of cancer-specific mortalities and all-cause mortalities in patients without and with self-reported CVDs (≥2), respectively, after adjustments were made for age, sex, marital status, BMI, drinking status, smoking status, education, physical activity, cancer stage, cancer treatment and antilipidaemic medications (Table 5). Similarly, these blood HDL levels were still not related to cancer-specific mortalities or all-cause mortalities in the stratified analysis.
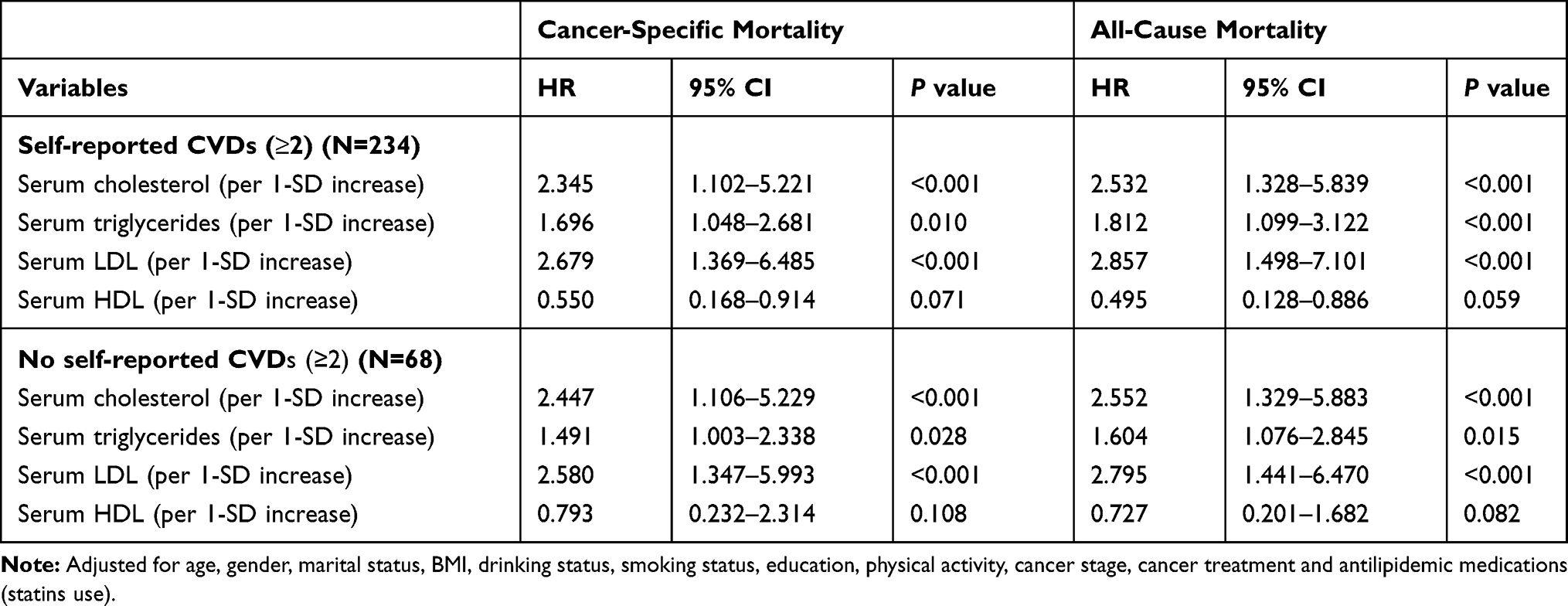 |
Table 5 Cox Proportional Hazard Model for Association of Blood Lipid Levels with Cancer-Specific Mortality and All-Cause Mortality Stratified by Self-Reported CVDs (≥2) |
Discussion
We found that elevated blood lipid levels were associated with poor prognosis for patients with CRC who underwent curative surgery after adjusting for potential confounding factors. The prognostic influence of blood lipids on patients with CRC was not mainly affected by antilipidaemic medications (statin use) or self-reported CVDs (≥2).
Recently, studies have shown that cancer and CVDs have many common risk factors and pathogenesis. Emerging evidence suggests that modifiable risk factors, including a high-fat diet, sedentary lifestyle, obesity, tobacco use and others, play a central role in the pathogenesis of both CVDs and cancers. Common mechanisms include genetics, inflammation, and ROS. As a traditional risk factor for CVDs, hyperlipidaemia has been found to be involved in the occurrence and development of tumours such as breast cancer, prostate cancer and CRC.8,9 In this study, we found that elevated blood lipid levels were associated with poor prognosis for patients with CRC who underwent curative surgery after adjusting for potential confounding factors, which is consistent with previous studies. In the field of basic research, hyperlipidaemia promotes the proliferation and metastasis of CRC cells by stimulating CRC stemness by acting on the RBP4-STRA6 pathway.12 In clinical research, however, the association between blood lipids and CRC has raised considerable controversy in recent decades. Early studies have shown that lower cholesterol levels were associated with increased mortality and incidence of CRC in the Framingham cohort24 and the Honolulu Heart Program.25 Some researchers hypothesized that patients with low serum cholesterol tend to have a more efficient hepatic clearance of cholesterol. Consequently, increased levels of bile acids can reach the colon and increase the risk for CRC because of long-term adverse effects on the colonic mucosa. Other study cohorts showed, however, that the association between dyslipidaemia and CRC was more complex or even non-existent.13,26–28 These previous findings do not seem to be in accordance with our results that elevated blood lipid levels were associated with cancer-specific mortality and all-cause mortality for patients with CRC after adjusting for potential confounding factors. The inconsistent results may be partly explained by the different study populations selected, the different study designs used, the different hypotheses being investigated, the different confounding factors included and the inherent difficulties in obtaining epidemiologic measurements. First, our study population was obtained from patients aged ≥65 years, and age-related factors are complex and diverse, which may lead to the partial deviation of results. Then, we aimed to assess the relationship between blood lipids and mortality in patients with CRC, whereas previous studies have only explored the relationship between blood lipids and the CRC incidence rate. Additionally, sensitivity analysis showed that total cholesterol, LDL and triglycerides were still associated with cancer-specific mortality and all-cause mortality for patients with CRC when we added antilipidaemic medications (statin use) as an additional covariate in the Cox proportional hazard model (Table 4), which is more precise and persuasive than previous studies.19,29 Statin use is an important confounding factor but is not adjusted for in some previous studies. In our study, the HR value was significantly lower after antilipidaemic medications (statin use) were added in the sensitivity analysis, although significant correlations between blood lipids and the mortality of CRC still existed. Similar results existed in the stratification analysis, and the association of blood lipids with cancer-specific mortality and all-cause mortality of patients with CRC was not affected by self-reported CVDs (≥2) (Table 5). Interestingly, we found that HDL was not related to the poor prognosis of patients with CRC. A reasonable explanation may be that HDL is an anti-atherosclerotic lipoprotein that has been considered a protective factor against CVDs.
Our study had some strengths. The results of the study mainly contribute to the literature in three different aspects. First, the data of this study are from TILDA, a longitudinal study of a national (US) sample.27 Data analysis proved that higher blood lipid levels are closely related to increased mortality and all-cause mortality for patients with CRC, which expands rare longitudinal research on the associations between blood lipid levels and CRC. Second, our study results showed that patients with statin use and self-reported CVDs (≥2) had almost no effect on the association of blood lipids with the risk of CRC death. Finally, we were able to conduct a robust and accurate calibration analysis to remove the adverse effects of potential confounding factors, including sociodemographic characteristics and lifestyle factors (smoking, drinking, exercise and others), which have been known to be associated with multiple primary cancers.
In conclusion, the population-based prospective study revealed that blood lipid levels were associated with increased mortality and all-cause mortality of CRC. Clinicians should pay more attention to the predictive value of increased blood lipid levels in patients with CRC for the risk of death. Statin use may reduce the risk of death and improve the prognosis for patients with CRC. Blood lipids may be a reliable prognostic factor for predicting mortality and all-cause mortality in patients with CRC.
The limitation of the study is the small sample size. It is necessary that more studies be implemented to identify the value of blood lipids (total cholesterol, triglycerides, and LDL) for predicting prognosis in patients with CRC. Additionally, our study only included a certain group of patients and lacked a definition of surgical treatment and other clinical parameters, which were also important confounding factors that may affect our results.
Acknowledgments
We thank all individuals who were responsible for the planning and administering of TILDA and making the datasets of TILDA available on their website.
Disclosure
All of the authors declare no conflicts of interest and have nothing to disclose for this work.
References
1. Angeli JPF, Garcia CCM, Sena F, et al. Lipid hydroperoxide-induced and hemoglobin-enhanced oxidative damage to colon cancer cells. Free Radic Biol Med. 2011;51(2):503–515. doi:10.1016/j.freeradbiomed.2011.04.015
2. Siegel R, DeSantis C, Jemal A. Colorectal cancer statistics, 2014. CA Cancer J Clin. 2014;64(2):104–117. doi:10.3322/caac.21220
3. Geng L, Chaudhuri A, Talmon G, et al. MicroRNA-192 suppresses liver metastasis of colon cancer. Oncogene. 2014;33(46):5332–5340. doi:10.1038/onc.2013.478
4. Lambert AW, Pattabiraman DR, Weinberg RA. Emerging Biological Principles of Metastasis. Cell. 2017;168(4):670–691. doi:10.1016/j.cell.2016.11.037
5. Wang C, Li P, Xuan J, et al. Cholesterol Enhances Colorectal Cancer Progression via ROS Elevation and MAPK Signaling Pathway Activation. Cell Physiol Biochem. 2017;42(2):729–742. doi:10.1159/000477890
6. Nordestgaard BG, Varbo A. Triglycerides and cardiovascular disease. Lancet. 2014;384(9943):626–635. doi:10.1016/S0140-6736(14)61177-6
7. Rosamond W, Flegal K, Furie K, et al.; Writing Group Members. Heart disease and stroke statistics—2008 update a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2008;121(121):e46–e215.
8. Nelson ER, Wardell SE, Jasper JS, et al. 27-hydroxycholesterol links hypercholesterolemia and breast cancer pathophysiology. Science. 2013;342(6162):1094–1098. doi:10.1126/science.1241908
9. His M, Zelek L, Deschasaux M, et al. Prospective associations between serum biomarkers of lipid metabolism and overall, breast and prostate cancer risk. Eur J Epidemiol. 2014;29(2):119–132. doi:10.1007/s10654-014-9884-5
10. van Duijnhoven FJB, Bueno-De-Mesquita HB, Calligaro M. Blood lipid and lipoprotein concentrations and colorectal cancer risk in the European Prospective Investigation into Cancer and Nutrition. Gut. 2011;60(8):1094–1102. doi:10.1136/gut.2010.225011
11. Day SD, Enos RT, Mcclellan JL, et al. Linking inflammation to tumorigenesis in a mouse model of high-fat-diet-enhanced colon cancer. Cytokine. 2013;64(1):454–462. doi:10.1016/j.cyto.2013.04.031
12. Karunanithi S, Levi L, Devecchio J, et al. RBP4-STRA6 pathway drives cancer stem cell maintenance and mediates high-fat diet-induced colon carcinogenesis. Stem Cell Rep. 2017;9(2):438–50.
13. Liu Z, Brooks RS, Ciappio ED, et al. Diet-induced obesity elevates colonic TNF-α in mice and is accompanied by an activation of Wnt signaling: a mechanism for obesity-associated colorectal cancer. J Nutr Biochem. 2012;23(10):1207–1213. doi:10.1016/j.jnutbio.2011.07.002
14. Qian BZ, Pollard JW. Macrophage diversity enhances tumor progression and metastasis. Cell. 2010;141(1):39–51. doi:10.1016/j.cell.2010.03.014
15. Peng F, Hu D, Lin X, et axl. An in-depth prognostic analysis of baseline blood lipids in predicting postoperative colorectal cancer mortality: the FIESTA study. Cancer Epidemiol. 2018;52:148–157. doi:10.1016/j.canep.2018.01.001
16. Shu X, Xiang YB, Rothman N, et al. Prospective study of blood metabolites associated with colorectal cancer risk. Int J Cancer. 2018;143(3):527–534.
17. Katzke VA, Sookthai D, Johnson T, et al. Blood lipids and lipoproteins in relation to incidence and mortality risks for CVD and cancer in the prospective EPIC–Heidelberg cohort. BMC Med. 2017;15(1):218. doi:10.1186/s12916-017-0976-4
18. Da-Qing D, Bing-Qing LI, Pei-Yuan HE. Study on the value of blood lipids in colorectal cancer. World Latest Med Inf. 2019(6):24-27.
19. None. Statin use and reduced cancer-related mortality. N Engl J Med. 2013;x. doi:10.1056/NEJMc1214827
20. Whelan BJ, Savva GM. Design and methodology of the irish longitudinal study on ageing. J Am Geriatr Soc. 2013;61:S265–S268. doi:10.1111/jgs.12199
21. Siedel J, Hägele EO, Ziegenhorn J, et al. Reagent for the enzymatic determination of serum total cholesterol with improved lipolytic efficiency. Clin Chem. 1983;29(6):1075–1080.
22. Patsch W, Brown SA, Morrisett JD, et al. A dual-precipitation method evaluated for measurement of cholesterol in high-density lipoprotein subfractions HDL2 and HDL3 in human plasma. Clin Chem. 1989;35(2):265–270.
23. Mcnamara JR, Cohn JS, Wilson PWF, et al. Calculated values for low-density lipoprotein cholesterol in the assessment of lipid abnormalities and coronary disease risk. Clin Chem. 1990;36(1):36–42. doi:10.1093/clinchem/36.1.36
24. Williams RR, Sorlie PD, Feinleib M, et al. Cancer incidence by levels of cholesterol. JAMA. 1981;245(3):247–252. doi:10.1001/jama.1981.03310280023021
25. Stemmermann GN, Nomura AM, Heilbrun LK, et al. Serum cholesterol and colon cancer incidence in Hawaiian Japanese men. J Natl Cancer Inst. 1981;67(6):1179.
26. Nomura AMY, Stemmermann GN, Po-Huang C. Prospective Study of Serum Cholesterol Levels and Large-Bowel Cancer. J Natl Cancer Inst. 1991;83:1403–1407.
27. Huang Y, Su Y, Jiang Y, Zhu M. Sex differences in the associations between blood pressure and anxiety and depression scores in a middle-aged and elderly population: the Irish Longitudinal Study on Ageing (TILDA) [published online ahead of print, 2020 May 23]. J Affect Disord. 2020;274:118–125. doi:10.1016/j.jad.2020.05.133
28. Pekkanen J, Nissinen A, Punsar S, et al. Short- and long-term association of serum cholesterol with mortality. The 25-year follow-up of the Finnish cohorts of the seven countries study. Am J Epidemiol. 1992;135(11):1251. doi:10.1093/oxfordjournals.aje.a116231
29. Shao Y, Hsu CH, Yeh KH, et al. Statin use is associated with improved prognosis of colorectal cancer in Taiwan. Clin Colorectal Cancer. 2015;14(3):
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.