Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Incomplete Ascher’s Syndrome Misdiagnosed as Eczema: A Case Report
Authors Song B ![]() , Li Q, Guo S, Li Z
, Li Q, Guo S, Li Z ![]() , Bi J
, Bi J ![]()
Received 28 October 2025
Accepted for publication 2 January 2026
Published 19 January 2026 Volume 2026:19 576697
DOI https://doi.org/10.2147/CCID.S576697
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Bendian Song, Qiuchen Li, Shitong Guo, Zhiyu Li, Jianhai Bi
Department of Burn and Plastic Surgery, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan, People’s Republic of China
Correspondence: Jianhai Bi, Department of Burn and Plastic Surgery, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan, People’s Republic of China, Tel +86 15110080702, Email [email protected]
Abstract: Ascher syndrome is a rare disorder classically characterized by blepharochalasis, double lip, and non-toxic thyroid goiter. We report a case initially diagnosed as eczema in the dermatology department, who presented with acquired double lips and blepharochalasis of the upper eyelids, without thyroid enlargement. Magnetic resonance imaging revealed uniformly increased T2-weighted signals in both the upper and lower lips, leading to a diagnosis of incomplete Ascher’s syndrome. The patient underwent oculoplastic surgery, which successfully restored the natural aesthetic contour, demonstrating the efficacy and necessity of surgical intervention. We summarize the differential diagnosis of conditions related to Ascher’s syndrome and analyze histopathological changes in the excised eyelid tissue to elucidate microscopic alterations associated with the disease.
Keywords: Ascher’s syndrome, plastic surgery, blepharochalasis, double lip, antidiastole
Introduction
Ascher syndrome, also called Laffer-Ascher syndrome, is a rare benign disorder classically characterized by the triad of blepharochalasis, double lip, and non-toxic thyroid goiter.1 This rare disorder typically manifests in young adults. Laboratory findings are often normal, with most cases showing only blepharochalasis and double lip. Consequently, patients seek consultation across multiple specialties, including ophthalmology, oral medicine, dermatology, and plastic surgery. Insufficient clinician knowledge about this disease often leads to diagnostic and treatment difficulties. This report presents a case treated with plastic surgery and highlights key differential diagnoses to improve future clinical management.
Case Presentation
A 24-year-old otherwise healthy male presented to the dermatology department with a 15-year history of progressive bilateral upper eyelid laxity and upper lip thickening. Initial symptoms, characterized by episodic upper eyelid edema and prominent thickening of the upper labial mucosa, emerged at age 9 without identifiable triggers. Over 15 years, the frequency of eyelid edema gradually diminished, resulting in progressively redundant upper eyelid skin. Concurrently, the upper labial mucosa exhibited slow, progressive hypertrophy. The patient received no systematic treatment during this period, using only topical erythromycin ointment during edematous episodes with limited benefit. His medical history was unremarkable, with no reports of trauma, surgery, allergies, or family history of genetic disorders.
Physical examination revealed bilaterally symmetrical, faintly erythematous skin with marked upper eyelid laxity, visible subcutaneous vasculature, and multiple skin folds. No proptosis, pruritus, or tenderness was observed (Figure 1A–C). Both lips appeared thickened, with a distinct double lip deformity of the upper lip featuring a central depression and inability to achieve complete lip closure (Figure 1D–F). The redundant mucosal fold became more pronounced during smiling. No thyroid enlargement was palpable.
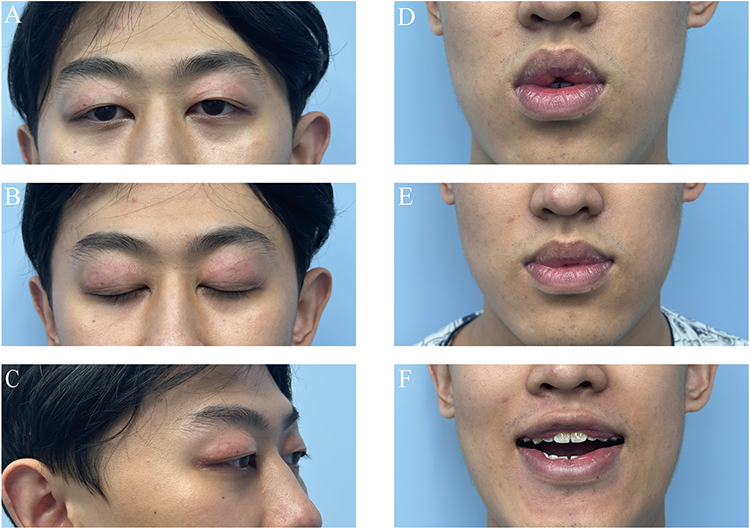 |
Figure 1 The preoperative ocular and labial images of the patient. (A) Forward gaze reveals lax and redundant upper eyelid skin. (B) Upon eyelid closure, the upper eyelid skin appears thin with visible underlying capillaries and hyperpigmentation adjacent to the eyelashes. (C) A 45-degree oblique view demonstrates lax and puffy upper eyelid skin. (D) The upper lip exhibits a double lip appearance in the natural resting state. (E) Habitual lip pursing conceals the prominent upper lip. (F) Smiling makes the upper lip double lip distinctly visible, accompanied by thickening of the lower left lip. |
Laboratory investigation showed a thyroid-stimulating hormone receptor antibody level of 2.63 IU/L (0–1.75IU/L). Thyroid ultrasonography identified a nodule in the right lobe classified as TI-RADS 3. Maxillofacial MRI demonstrated plump bilateral lacrimal glands without significant thinning of the eyelid skin. The labial mucosa and soft tissues exhibited a uniformly increased T2 signal, while DWI and ADC sequences showed no diffusion restriction (Figure 2A–D).
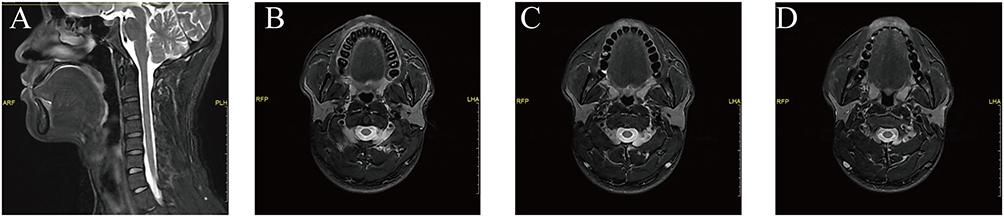 |
Figure 2 Preoperative magnetic resonance (MR) images of the patient’s maxillofacial region. (A) Sagittal view reveals hyperintensity in both the upper and lower lips on T2-weighted imaging. (B, C) Coronal views demonstrate soft tissue thickening in the upper lip. (D) Coronal view shows significant thickening and hyperintensity of the lower lip on T2-weighted imaging. |
The patient was diagnosed with incomplete Ascher syndrome by the plastic surgery team. Subsequently, he underwent corrective blepharoplasty involving excision of redundant upper eyelid skin and partial subcutaneous orbicularis oculi muscle, with fixation of prolapsed lacrimal glands to the superolateral periosteal surface (Figure 3).
 |
Figure 3 Intraoperative photograph showing the prolapsed lacrimal gland. |
Histopathological evaluation was performed on the surgical specimen using hematoxylin and eosin (H&E) staining. It revealed mild chronic inflammation in the skin tissue. Pigment was deposited in the basal layer, with scattered pigment-laden histiocytes present in the dermis. Capillary dilation and vascular endothelial hyperplasia were also observed (Figure 4A). We employed special staining techniques for further characterization. Colloid iron staining showed that in the dermis, particularly around blood vessels and skin appendages, there was a large area of bright blue, granular-like mucopolysaccharide deposition (Figure 4B). Verhoeff-Van Gieson (EVG) staining highlighted a significant reduction, thinning, and fragmentation of elastic fibers in the upper eyelid dermis, which was accompanied by marked disruption of the normal, continuous reticular network (Figure 4C).The suture was removed 6 days after the surgery. At that time, the upper eyelid skin was slightly red and swollen, but the appearance had significantly improved compared to before (Figure 5A–D).
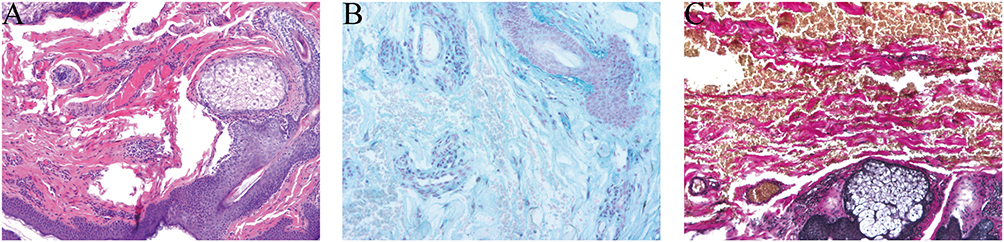 |
Figure 4 Histopathological analysis of the resected upper eyelid skin. (A) Hematoxylin and eosin (H&E) staining shows telangiectasia, inflammatory cell infiltration, and basal layer hyperpigmentation. (B) The colloid iron staining revealed a large number of dispersed, bright blue granular deposits within the dermis, indicating the presence of mucin deposition. (C) Verhoeff-Van Gieson (EVG) staining demonstrates the absence of a continuous elastic fiber layer, with fragmented and diminished elastic fibers in the dermis. |
 |
Figure 5 Preoperative and postoperative comparisons. (A) Preoperative view with the patient gazing forward. (B) Postoperative view on day 6 (after suture removal) with the patient gazing forward. (C) Preoperative view with gentle eyelid closure. (D) Postoperative view on day 6 (after suture removal) with the patient gazing forward. |
Discussion
Ascher syndrome is a rare hereditary disease with an incidence of approximately one in a million. Currently, the etiology of the disease remains unclear, though three main hypotheses have been proposed: physical trauma, autosomal dominant inheritance, and endocrine disorders. However, Fu et al found no specific gene mutations associated with eyelid laxity through whole-exome sequencing of patients and their mothers.2 Additionally, tests for rheumatoid factor and hormone levels in multiple patients revealed no significant abnormalities.
Instead, current evidence suggests that the condition may arise from abnormal enhancement of fibroblast activity and excessive deposition of extracellular matrix components such as collagen, which contribute to chronic non-neoplastic soft tissue hypertrophy.3 Notably, based on pathological findings of substantial mucin deposition observed in colloidal iron staining, we hypothesize that the accumulation of hydrophilic mucins in the patient’s eyelid tissue leads to persistent high water content, expansion, and increased tension in the dermis. Consequently, this may result in physical fatigue, rupture, and structural damage over time. Nevertheless, further research is essential to elucidate this mechanism in depth. Clinically, complete Ascher syndrome is characterized by bilateral upper eyelid skin laxity, a heavy upper lip, and non-toxic goiter.4 Yet, non-toxic goiter is reported in only 10–50% of documented cases. Thus, many scholars argue that the diagnosis of Ascher syndrome can be established based solely on the presence of relaxed upper eyelid skin and a heavy upper lip.5 In this context, the present case exhibits incomplete features of Ascher syndrome.6
The main eye symptoms include edema, pale redness, thinning, visible capillaries, sagging of the upper eyelid skin, and partial pupil coverage. These symptoms reflect the progression of eyelid lesions, which can be divided into three stages.7 The first stage is the edema phase. It is characterized by intermittent painless swelling of the upper eyelid and may be the initial manifestation of this disease.8 The frequency of eyelid edema decreases with age. The second stage involves sagging of the upper eyelid skin, causing loose, thin skin to create excess folds along the eyelid margin. The third stage is marked by atrophy of the inner fat pad, prolapse of orbital fat and lacrimal gland, resulting in more pronounced loosening of the upper eyelid skin. Surgery usually involves making a double eyelid incision, removing excess skin and the orbicularis oculi muscle, and fixing the orbital septum along with the prolapsed lacrimal gland. Our histopathological analysis confirmed previously reported findings: telangiectasia and fragmented, reduced dermal elastic fibers.9
Progressive swelling of the lips, particularly involving the lip mucosa, often occurs on the upper lip and is accompanied by dryness and cracking. This swelling becomes more noticeable during eating, speaking, or smiling. Previous reports indicate that it may also affect the patient’s pronunciation and bite,10 and that heavy lip involvement is mostly limited to the upper lip and rarely affects the lower lip.11 The patient exhibits lower lip asymmetry upon mouth opening. The patient has limited lip function and a habitual pursing of the lips with prolonged mouth closure. As a result, severe lip closure is not apparent, and the patient refuses to undergo lip repair. The formation of the lip border is attributed to the gradual widening of the horizontal groove separating the outer skin (vermilion border) from the inner mucosal area.11 There is no significant change in the middle frenulum, and usually an intraoral double elliptical incision is made to preserve the frenulum while cutting off excess tissue in a shuttle shape. In a few cases, W-shaped surgery is used.4 The pathology of excised lip tissue often suggests non-specific inflammatory cell infiltration,5 accompanied by salivary gland hyperplasia and vascular dilation.12
Thyroid enlargement often occurs many years after eyelid and lip lesions. The diagnosis of this disease mostly happens during adolescence. Changes in the thyroid gland often occur after the age of 20,1 which means the symptom often does not appear earlier. Thyroid enlargement is usually a non-toxic goiter. Parveen Rewri’s case report review indicated that only 14% (6/42) of patients had non-toxic thyroid involvement.8 It is recommended that such patients undergo regular follow-up thyroid hormone, thyroid antibody testing, and ultrasound examination.2
We have summarized the previously published data of some patients with Ascher syndrome in Table 1. Since Ascher syndrome affects multiple organs, it is necessary to distinguish it from other diseases that affect the eyelids, lips and thyroid. The diseases that require differential diagnosis are listed in the Table 2.
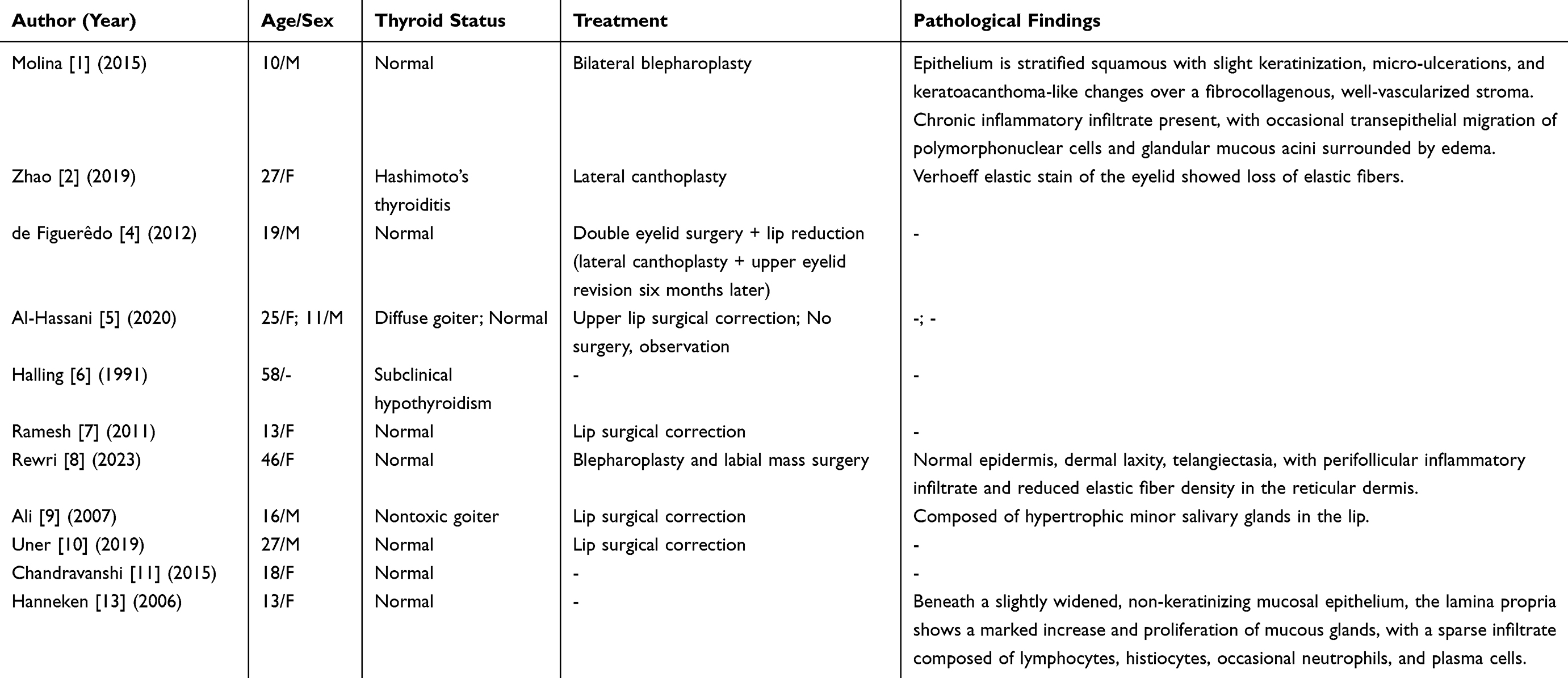 |
Table 1 The Characteristics of Ascher Syndrome as Previously Reported |
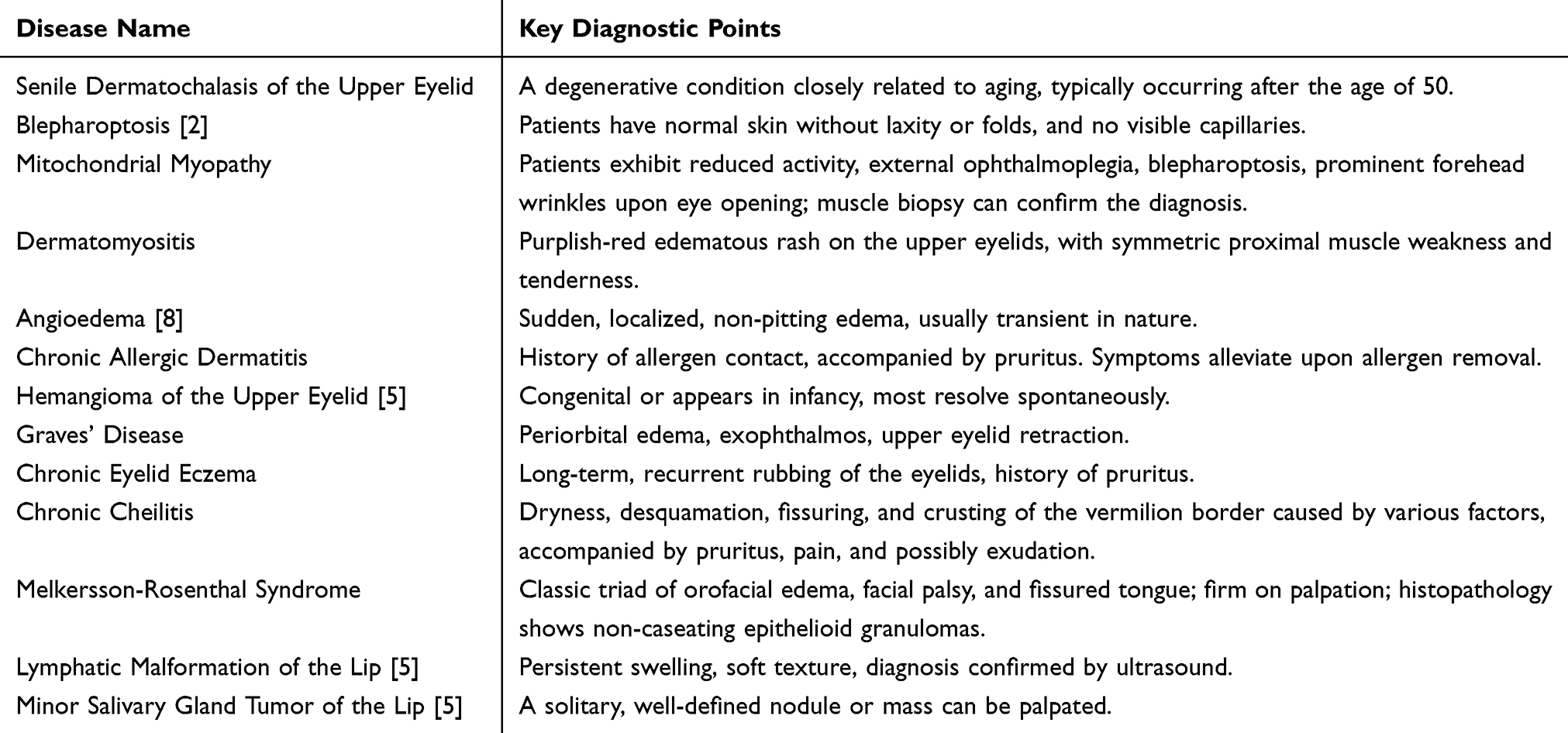 |
Table 2 Diseases and Key Points for Differential Diagnosis from Ascher Syndrome |
Currently, there are no specific drugs to treat or delay the progression of the disease. There are reports on the use of steroid shock therapy during the acute phase of upper eyelid swelling,13 and attempts to control the condition with dapsone, but the effect is not significant.8 The patient had used erythromycin eye ointment without improvement in upper eyelid redness and swelling. Therefore, surgical resection is currently the only solution to improve function and aesthetics in Ascher syndrome; however, the follow-up time for this case is relatively short, and long-term follow-up is needed to evaluate the effectiveness and necessity of plastic surgery. The follow-up period for this case is relatively short; therefore, the effectiveness and necessity of plastic surgery require evaluation through long-term follow-up.
Conclusion
This case found that the uniform high signal of the lip soft tissue in the MRI T2 image and the glycosaminoglycan deposition shown by colloid iron staining are of great value for the differential diagnosis of Ascher syndrome. Through eyelid plastic surgery, the appearance and psychological state of patients can be effectively improved, and their social adaptability can be enhanced.
Ethical Considerations
This report complies with the Helsinki Declaration of Ethical Principles. The Ethics Committee of Shandong Provincial Hospital Affiliated to Shandong First Medical University, has approved the publication of the case details.
Consent for Publication
The patient has signed a written consent form, agreeing that the details of his case and related imaging data can be publicly disclosed in this journal.
Acknowledgments
The authors would like to sincerely acknowledge the patient for consenting to share his clinical experience in this publication. We are also grateful to Dr. Jiwei Ma (Department of Pathology) and Dr. Lina Wang (Department of Radiology) of Shandong Provincial Hospital Affiliated to Shandong First Medical University for their professional support.
Funding
This work was supported by the Natural Science Foundation of Shandong Province (Grant No. ZR2022MH080).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Molina S, Medard P, Galdeano M. Ascher syndrome: report of a case with early manifestations. Craniomaxillofac Trauma Reconstr. 2015;8(2):150–7. doi:10.1055/s-0034-1395881
2. Zhao ZL, Wang SM, Shao CY, Fu Y. Ascher syndrome: a rare case of blepharochalasis combined with double lip and Hashimoto’s thyroiditis. Int J Ophthalmol. 2019;12(6):1044–1046. doi:10.18240/ijo.2019.06.26
3. Crăiţoiu Ş, Bobic AG, Manolea HO, et al. Immunohistochemical study of experimentally drug-induced gingival overgrowth. Rom J Morphol Embryol. 2019;60(1):95–102. PMID: 31263832.
4. de Figuerêdo AA, de Pochat VD, Barreto TF, Mendes RS, Alonso N, Meneses JV. Management of an unusual presentation of Ascher syndrome. J Craniofac Surg. 2012;23(6):e570–1. doi:10.1097/SCS.0b013e31825dabec
5. Al-Hassani M, Carey B, Sanderson J, Hullah E, Escudier M. Ascher’s syndrome: a rare cause of lip swelling. Ann R Coll Surg Engl. 2020;102(8):e216–e218. doi:10.1308/rcsann.2020.0161
6. Halling F, Sandrock D, Merten HA, Hönig JF. Das Ascher-Syndrom [Ascher’s syndrome]. Dtsch Z Mund Kiefer Gesichtschir. 1991;15(6):440–444.
7. Ramesh BA. Ascher syndrome: review of literature and case report. Indian J Plast Surg. 2011;44(1):147–149. doi:10.4103/0970-0358.81468
8. Rewri P, Garg S, Kumar R, Gupta G. A Century of Laffer-Ascher Syndrome. Indian J Plast Surg. 2023;56(6):540–543. doi:10.1055/s-0043-1776140
9. Ali K. Ascher syndrome: a case report and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103(2):e26–8. doi:10.1016/j.tripleo.2006.08.027
10. Uner DD, Izol BS. Ascher syndrome: a case report. Niger J Clin Pract. 2019;22(7):1029–1031. doi:10.4103/njcp.njcp_661_18
11. Chandravanshi SL, Mishra V. Ascher’s syndrome: a rare case report. Indian J Ophthalmol Mar. 2015;63(3):264–267. doi:10.4103/0301-4738.156933
12. Koutlas IG. Syndromes affecting skin and mucosa. Atlas Oral Maxillofac Surg Clin North Am. 2014;22(2):135–151. doi:10.1016/j.cxom.2014.06.001
13. Hanneken S, Reifenberger J, Homey B. Doppellippe und blepharochalasis: ascher-syndrom bei einer 13-jährigen patientin [Double-lip and blepharochalasis: ascher syndrome in a 13 year-old female patient]. Hautarzt. 2006;57(10):903–904. doi:10.1007/s00105-006-1209-5
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.