Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 11
Incidence, Risk and Protective Factors for Unintentional, Nonfatal, Fall-Related Injuries at Home: A Community-Based Household Survey from Ujjain, India
Authors Pathak A ![]() , Agarwal N, Mehra L
, Agarwal N, Mehra L ![]() , Mathur A
, Mathur A ![]() , Diwan V
, Diwan V
Received 12 December 2019
Accepted for publication 11 February 2020
Published 20 February 2020 Volume 2020:11 Pages 65—72
DOI https://doi.org/10.2147/PHMT.S242173
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Ashish Pathak,1– 4 Nitin Agarwal,5 Love Mehra,1 Aditya Mathur,1 Vishal Diwan3,6,7
1Department of Pediatrics, R. D. Gardi Medical College, Ujjain 456006, India; 2Department of Women and Children’s Health, International Maternal and Child Health Unit, Uppsala University, Uppsala SE-751 85, Sweden; 3Department of Global Public Health, Health Systems and Policy-Karolinska Institutet, Stockholm, SE-171 76, Sweden; 4International Centre for Health Research, Ujjain Charitable Trust Hospital and Research Centre, Ujjain 456006, MP, India; 5Department of Pediatric Surgery, R. D. Gardi Medical College, Ujjain, 456006, India; 6Department of Public Health & Environment, R. D. Gardi Medical College, Ujjain 456006, India; 7ICMR- National Institute for Research in Environmental Health (NIREH), Bhopal, India
Correspondence: Ashish Pathak Tel +91 930-223-9899
Email [email protected]
Background: Childhood injury is an increasing public health burden and considered a major cause of childhood morbidity and mortality worldwide. In this study, we identified the distribution and risk factors for fall-related child injuries at home in Ujjain, India.
Methods: A community-based, cross-sectional study was conducted in 2017 in Ujjain, India, which included 6308 children up to 18 years of age living in 2518 households. Data were collected using a pretested, semi-structured, proforma from the parents of the included children.
Results: The overall incidence of home injury was 7.78% (95% confidence interval [CI]: 7.12– 8.84) in the last 1 year, ie, 2015– 16. The incidence was significantly higher at 5– 10 years of age (odds ratio [OR]: 2.91, 95% CI: 1.75– 4.85; P < 0.001), followed by 1– 5 years (OR: 2.66, 95% CI: 1.59– 4.45; P < 0.001). The incidence of injuries was higher in boys than in girls (adjusted odds ratio [aOR]: 1.73, 95% CI: 1.43– 2.10; P < 0.001). Other risk factors associated with unintentional fall injuries at home were residence (rural vs urban; aOR: 1.25, 95% CI: 1.03– 1.51; P = 0.018), number of family members (≤ 4 vs 5– 10 and ≤ 4 vs > 10; aOR: 0.69, 95% CI: 0.56– 0.86; P < 0.001 and aOR: 0.67, CI: 0.48– 0.94; P < 0.023, respectively), cooking area (combined vs separate; aOR: 0.82, 95% CI: 0.68– 1.00; P = 0.057), and whether mother is alive vs not alive (aOR: 2.09, 95% CI: 1.10– 3.94; P = 0.023).
Conclusion: The incidence of fall injuries among children at home in Ujjain, India, was similar to other resource constraint settings. The incidence was higher in rural areas, in the age group of 5– 10 years, and in families in which the mother was not alive. By contrast, large and combined families had a lower incidence of falls.
Keywords: childhood, epidemiology, nonfatal injuries, home injuries, India
Background
Unintentional childhood injuries in and around home are a major public health problem and the second leading cause of death due to injuries after road traffic accidents.1–5 However, most of these injuries are preventable.6–8 Such injuries have a major impact on the education, family relationship, and emotional and psychological well-being of the child and cause economic and social burden on the families; therefore, preventing these injuries is paramount.9 The spectrum of fall-related home injuries varies from minor injuries requiring first aid or those requiring outpatient health care visits that can lead to hospitalizations, such as burns and scalds, to major injuries such as choking, strangulation, and drowning, which are often fatal.2,4,10 However, establishing a global spectrum of unintentional fall-related injuries is difficult because of the lack of valid data, particularly for nonfatal injuries, from low-and-middle-income countries (LMICs).4,6,7
Childhood unintentional falls are associated with various factors such as age; sex; geographical area; child development; parental literacy; overcrowding at home; home environment including unsafe building designs such as stairs, windows, and roofs without safety grills; unsafe storage of potentially hazardous substances such as kerosene and medicine; unsafe kitchen with access to stove and knives; and insufficient household lighting.2–4,10,11
Despite a relatively high burden of injuries and falls, with 92% of all Disability-Adjusted Life Years (DALYs) lost due to falls, policy-makers in LMICs including India have considered injuries and falls as low priority.4 Furthermore, population-based studies on this topic are lacking due to poorly maintained death registers, inappropriate coding of causes of death, lack of standard definitions of home accidental mortality and morbidity, and lack of hospital-based injury surveillance.2,4,12,13 This lack of data on local injury problems hampers appropriate resource allocation to prevent and treat fall-related injuries in LMICs. Therefore, this study aimed to determine the burden, anatomical distribution, risk and protective factors, and outcomes of unintentional, nonfatal childhood fall-related injuries at home through a community-based survey in Ujjain, India.
Methods
Study Site and Population
The study was conducted by the Department of Pediatrics, RD Gardi Medical College (RDGMC), in Ujjain district in the western part of Madhya Pradesh, India.14 The district has a population of 1.9 million with a sex ratio (females per thousand males) of 958 in urban areas and 975 in rural areas.14 Approximately 61% of the population lives in rural areas.14 The key population and household profiles, such as population below 15 years; sex ratio; literacy rates; fertility rates; households with safe drinking water, cooking fuel, and electricity; and maternal and child characteristics are described in National Family Health Survey-4.15
The Multidimensional Poverty Index 2018 indicated that Madhya Pradesh ranked third among all states with a Multidimensional Poverty Index of 0.180 against a national average of 0.121, indicating higher acute poverty than the national average.16 The household survey was conducted in both rural and urban areas. From the rural area, seven villages were randomly selected from the Demographic Surveillance Site of RDGMC.17 Out of these 7 villages, 1214 households including 3401 children were included in the survey. From the urban area, 10 geographically contiguous slums in Ujjain city, having 2,000 households including 10,000 individuals, around the Urban Health Centre of RDGMC were selected. Out of these urban slums, 1304 households including 2907 children were included in the survey. The number of individuals per household is approximately 5.1 in Ujjain district,15 which is comparable with the population included in the study. Ujjain is a typical regional city of India having 30–50% of new middle-class population, which spends between US $2 and US $10 per capita per day.18
Recruitment of Participants and Data Collection
According to the WHO guidelines for sample size calculation for community surveys of injuries, the minimum sample size was calculated as 1173 children each for the rural and urban areas.19 Accordingly, the survey included 3401 and 2907 children from urban and rural areas, respectively, with a response rate of 98%. The details of sample size calculation and sampling frame have been published previously.20
A total of 2846 households in the sampling frame were approached, of which, 2514 households were identified as having children aged 1 month to 18 years old. From these households, 6308 children were recruited in the study after obtaining signed informed consent from the household head. Three trained study assistants interviewed the female head of the households, along with two team leaders who supervised the data collection. Information on fall-related injuries was collected using a questionnaire developed using WHO Training Educating and Advancing Collaboration in Health on Violence and Injury Prevention (TEACH-VIP 2) guidelines for injury survey.19 Another structured questionnaire was used to interview caregivers to collect household demographic data.20
Field Definitions of Unintentional Home-Related Injuries
This study included only unintentional, nonfatal, fall-related injuries occurring at home that were recalled and reported by the female household head and/or the participants or the male household heads (n = 7), during the last 1-year period, ie, 2015–16. Participants could report multiple injuries for each episode of fall and also multiple falls in the last 1-year period. Injuries were correlated with the mechanism of injury and classified as unintentional and nonfatal according to the International Classification for External Causes of Injuries.9
A fall in the injury cases was defined according to the Preventions of Falls Network Europe Consensus as “a sudden and unintentional change in position resulting in an individual landing at a lower level such as on an object, the floor, or the ground, with or without injury”.21 Only falls associated with injuries are reported in the present study. The details of place, height, and time of fall, first aid provided, and hospitalizations following falls were also noted. In a household cooking area was considered separate if it was outside the house or was located at a height of at least one meter from the floor.
Data Management and Data Analysis
The data were coded and entered in Epi InfoTM (Version 7.2). Data analysis was done using Stata (Version 13.0, StataCorp, College Station, TX, USA). Proportions of fall injuries were reported with corresponding 95% confidence intervals (CIs). Bivariate analysis was done using Chi-square test to compare proportions of fall injuries by gender (girls versus boys), age (1 month to 1 year versus more than 1 year to 5 years, more than 5 years to 10 years, more than 10 years to 18 years), rural versus urban residence, family type (nuclear versus joint), number of family members (3–4 versus 5–10 versus more than 10), number of siblings (up to 2 versus 3 or more), mother live versus not, father alive versus not, cooking area combined versus separate. Crude odds ratios (OR) were calculated from two-by-two tables. Adjusted odds ratios (aOR) of falls for various covariates having P value <0.1 were calculated with a backward multivariate logistic regression model. A P value <0.001 was considered statistically significant. For the final model, model discrimination was done using a concordance-statistics-receiver-operating-characteristics (ROC) curve, while model calibration was done using the Hosmer–Lemeshow “goodness-of-fit” test.22,23 The Institutional Ethics Committee of R. D. Gardi Medical College, Ujjain, approved the study (Approval No.-354/2014)
Results
Incidence of Falls
In the survey, 6308 children reported a total of 491 unintentional, nonfatal, fall-related injuries at home, indicating an overall incidence rate of 7.78% (95% CI: 7.12–8.84). A total of 338 (69%, 95% CI: 64.51–72.91) fall injuries received first aid and 40 (8%, 95% CI: 5.91–10.95) falls resulted in hospital admissions. The overall incidence of falls that required first aid was 68.84% (95% CI: 64.61–72.78) and that of those requiring hospitalization was 8.15% (95% CI: 6.04–10.9).
The commonest places of injury were the streets in front of home, veranda, rooms, terrace, agriculture fields, stairs, and bathroom with incidence rates of 32%, 22%, 14%, 10%, 10%, 5%, and 4%, respectively.
Types and Anatomical Distribution of Fall Injuries
The most common type of injury was abrasions (n = 356), followed by cuts (n = 176) and contusions (n = 144). The age and gender-related distribution of fall injuries is shown in Table 1. The most common anatomical site of injury was the head (n = 300), followed by lower extremities (n = 257; Figure 1). Table 2 provides the age and gender-related distribution of anatomical sites of injury.
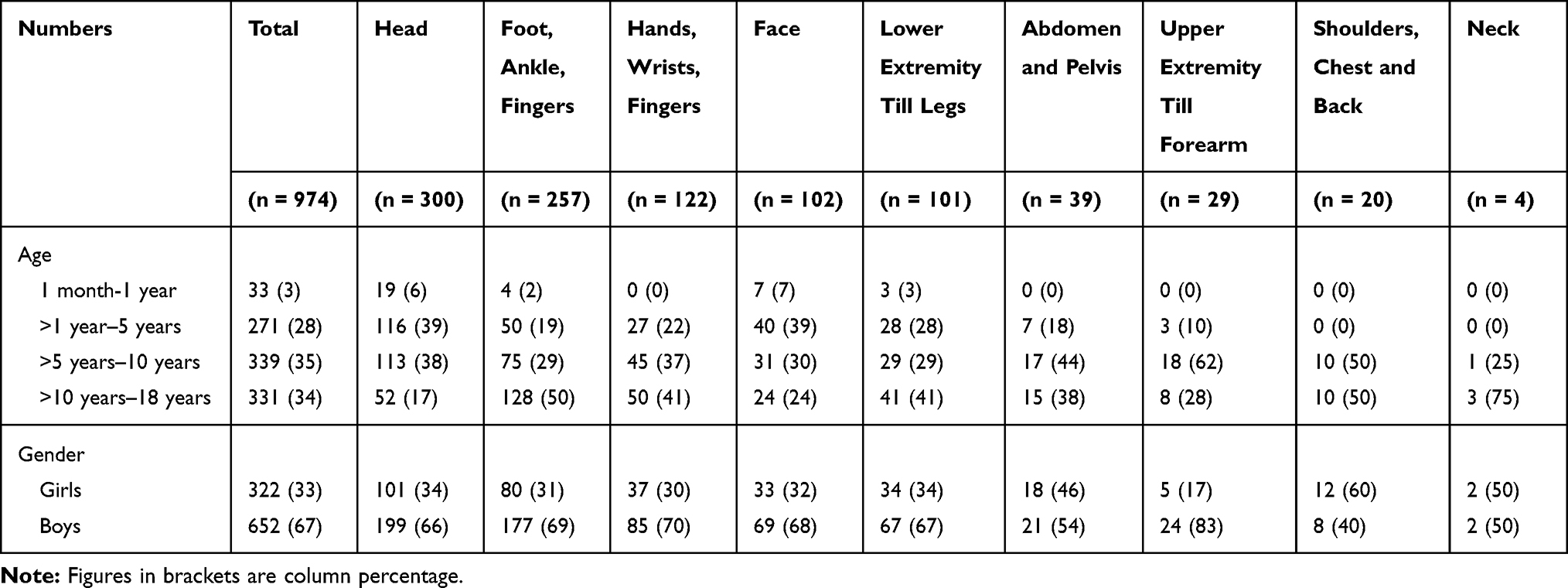 |
Table 1 Anatomical Distribution of 974 Fall-Related Injuries According to Age and Gender in 491 Children from the Community Survey in Ujjain, India |
 |
Table 2 Distribution of Types of Injury of 974 Falls According to Age and Gender in 491 Children from the Community Survey in Ujjain, India |
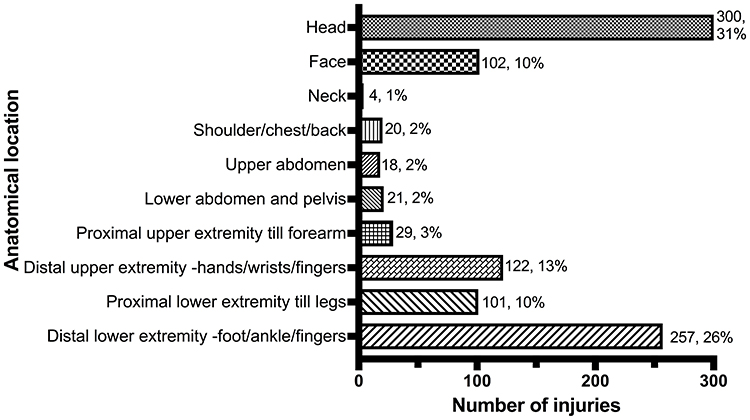 |
Figure 1 Anatomical location of 974 injuries resulting from 491 falls in the study. |
Bivariate Analysis
In bivariate analysis, boys were more likely to sustain falls than girls (OR: 1.83, 95% CI: 1.52–2.30; P < 0.001). In addition, falls were significantly correlated with age (Table 3). Children aged between 5 and 10 years had a maximum incidence of fall-related injuries (OR: 2.91, 95% CI: 1.75–4.85; P < 0.001). Children living in urban locations and orphans had a higher incidence of falls compared with those living in rural areas (Table 3). Children living in joint families (OR: 0.82; 95% CI: 0.68–1.45; P = 0.044), with more than five family members (OR: 0.64; 95% CI: 0.519–0.796; P < 0.001), and with three or more siblings (OR: 0.73; 95% CI: 0.611–0.886; P = 0.001) had a lower incidence of falls (Table 4).
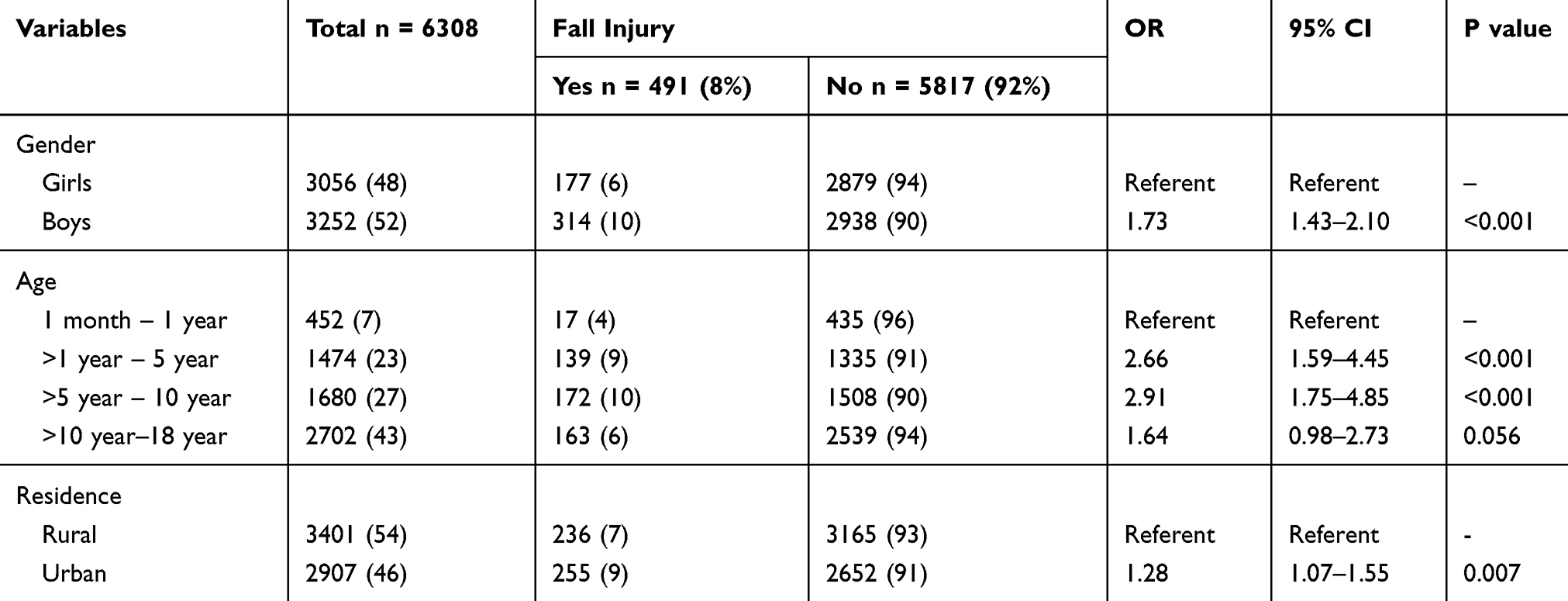 |
Table 3 Demographic Characteristics of 6308 Children and 491 Children with Fall Included in the Community Survey in Ujjain, India |
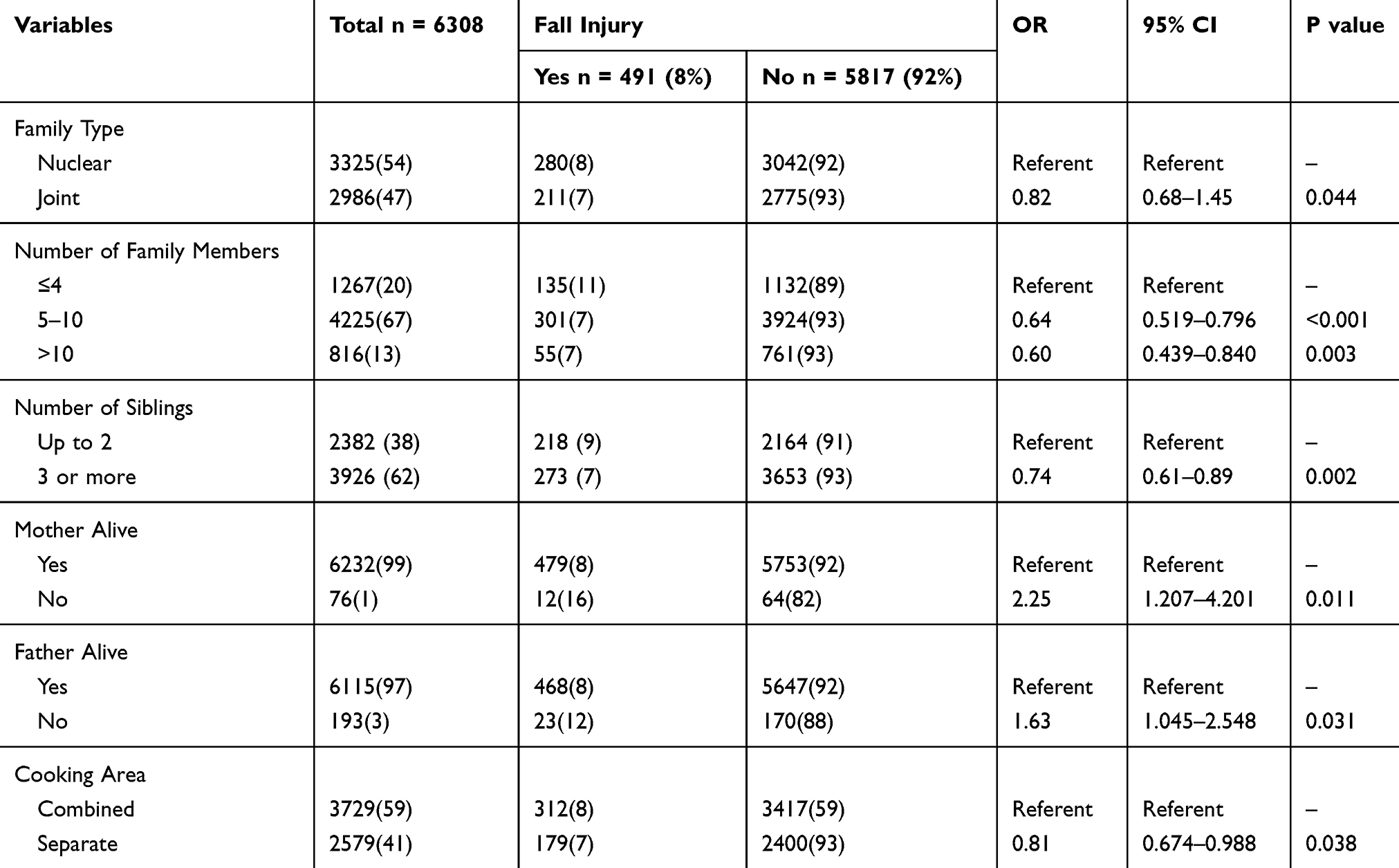 |
Table 4 Family Related Characteristics of 6308 Children and 491 Children with Fall Included in the Community Survey in Ujjain, India |
The majority (n = 339, 69%) of falls occurred from 12 p.m. to 6 p.m. Moreover, the majority (n = 248, 51%) of falls occurred at the ground level. The height of fall was more than 2 m in 52 (11%) injuries.
Multivariate Analysis
Multivariate logistic regression showed that falls were associated with gender (higher incidence in boys versus girls); age (greatest in age group of 5–10 years); place of residence (urban greater than rural), number of members in the family (less falls in larger families), separate cooking area; and if mother was not alive (Table 5).
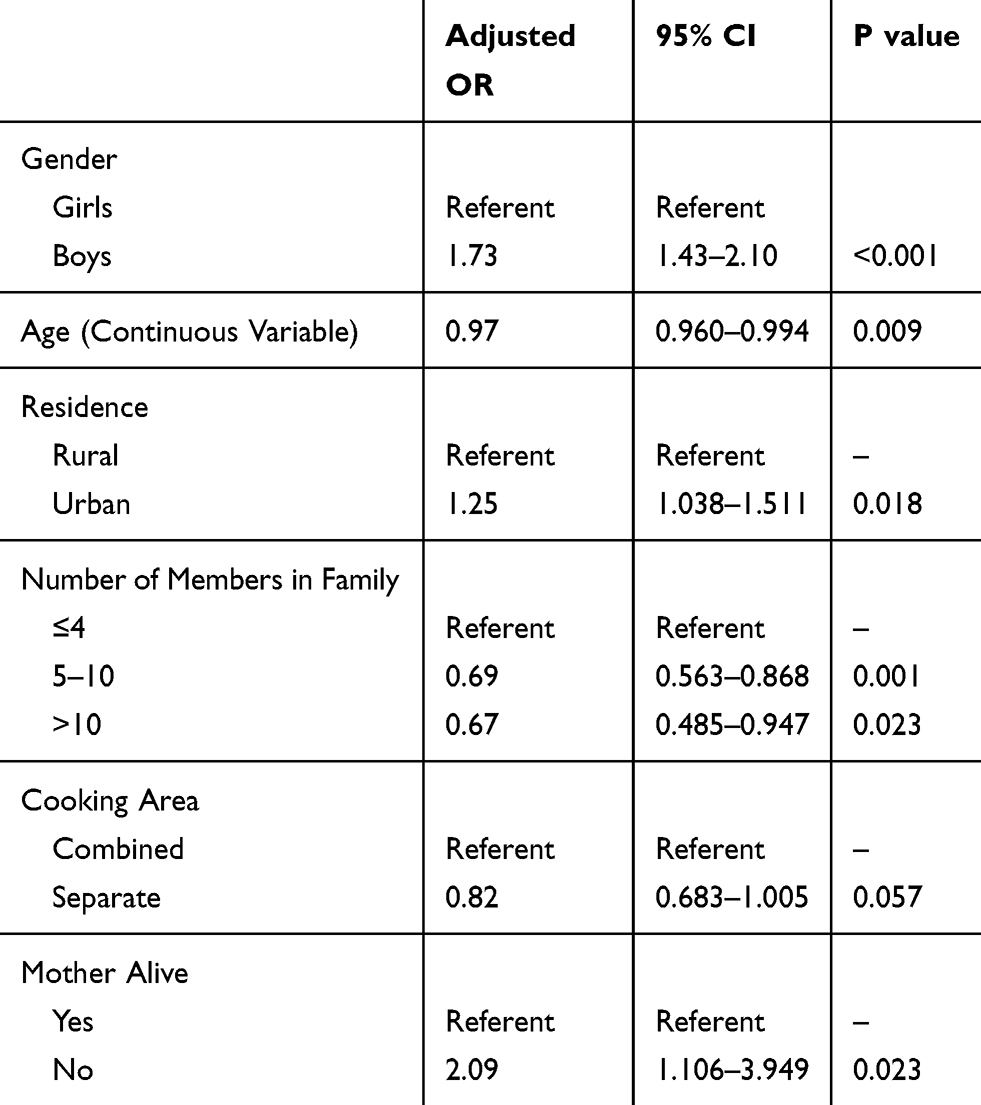 |
Table 5 Adjusted Odds Ratios of Sociodemographic Risk Factors for 491 Children with Fall Included in the Community Survey in Ujjain, India |
Model Performance
The ROC of the final model was 0.7092 showing an excellent model fit. The Hosmer–Lemeshow test showed that chi-square was 11.12 (P = 0.295) showing good model calibration.
Discussion
To our knowledge, this is the first study to report the incidence and risk factors associated with home-related falls in children and adolescents ≤18 years of age in central India. An injury incidence of 7.78% translates into an estimated 60 million nonfatal childhood and adolescent fall injuries in India. The findings of the study add to the evidence that childhood nonfatal fall injuries are an important public health problem and should be incorporated in injury prevention programs. Falls are the most common injuries that occur at home. Our study reports a higher incidence of injuries in Ujjain than that reported by other studies from India20,24–27 and Nepal, which reported an incidence of 5.72% among children between 0 and 14 years of age.28 Other LMICs also reported a high incidence of childhood fall injuries.29–32
A total of 338 (69%) fall injuries received first aid and 40 (8%) falls resulted in hospital admissions. Of the total of 974 injuries, the commonest injury was abrasions (37%), followed by cuts (18%) and contusions (15%). Abrasions and cuts are considered the commonest outcome of fall injuries, which may lead to scars over bony prominences such as the knees, shins, and forehead. These injuries are considered minor and treatable at home and hence are most frequently neglected.33 The most common anatomical site of injury in this study was the head (31%), followed by lower extremities (26%). A systematic review reported that the head is the most common anatomical site of injury after a fall.33 In a study in Bangladesh, head, face, and chest injuries were frequent in younger children (<4 years); upper limb injuries were frequent in older children (5–9 years old); and lower limb injuries were frequent in young adults (10–24 years old).34
Boys were more likely to sustain falls than girls and children aged between 5 and 10 years had a maximum incidence of fall-related injuries in the study. Worldwide, multiple studies have shown that boys have a higher incidence of fall than girls.6,11,13,25,27,28,33
The majority (n = 248, 51%) of falls occurred at the ground level, which is similar to that reported earlier.11,27,28 Results of a multivariate logistic regression demonstrated that type of residence, number of members in the family, type of cooking area, and whether the mother was alive were significantly associated with fall injuries. Moreover, the surrounding environment plays a crucial role in the occurrence of injuries; rural outmigration has resulted in overcrowded cities, which makes children living in urban areas more prone to unintentional fall-related injuries.6 Accordingly, in the present study, children living in crowded urban areas experienced more injuries compared with children living in rural areas. Moreover, according to WHO, overcrowded housing and living conditions are critical risk factors for fall-related injuries.5 Furthermore, children living in families, with more than five members, and with three or more siblings experienced less falls in the present study, which is similar to the results reported by other studies from India and China.26,35 Most injuries to young children are preventable and can happen due to lapses in caregiver attention.36 Large families can have more adults to supervise. This could explain the protective effect of large families on unintentional fall-related injuries in our study. However, other studies from resource-rich settings have shown that a large number of siblings at home can increase the risk of all types of injuries.36 However, in many resource-constrained settings, elder siblings act as caregivers and provide supervision for their younger siblings.37 Increased risk of falls among children whose mothers were not alive further substantiates this point. However, what defines and quantifies supervision and how to measure it, remains elusive.36 A separate and inaccessible cooking area in the household had a protective effect on fall-related injuries. This may be because of the Indian tradition of cooking at ground level. WHO report on injury prevention also reported a protective effect of separate cooking area on injuries including fire injuries.4
Strengths and Limitations
The survey was done in both rural and urban areas using the standard and validated WHO survey tools. To minimize potential biases the interview was carried out with the mother by trained interviewers. However, the study certain limitations. The responses of the mothers might have varied according to their health awareness in general and of injuries in particular. The recall period of 1 year used in the study for nonfatal falls might be too long especially, if the fall did not result in a significant injury. As Ujjain is a typical regional city of India with the rising new middle class of India, which is quite diverse geographically and socially,18 we feel the results are generalizable to similar regional cities of India and other middle-income countries. However, to substantiate these results, a nationwide survey through multi-centre survey project is needed in India.
Conclusions
The incidence of fall injuries among children occurring at home in Ujjain, India is high, similar to other resource constraint settings. The incidence was higher in rural areas, in the age group of 5–10 years and in families where mother was not alive. Large and combined families had a lower incidence of falls. These findings will form the basis of future intervention studies to prevent unintentional fall injuries among children in India and in similar resource-constrained settings.
Acknowledgments
The authors thank all the students and schools for participating in the study. The authors thank the Dean Dr MK Rathore and the Medical Director Dr VK Mahadik, R. D. Gardi Medical College, Ujjain, for their administrative support. This manuscript was edited by editingindia.
Author Contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This study is part of a project funded by the Indian Council of Medical Research (ICMR), New Delhi, India (Grant number 2013-1253).
Disclosure
The authors declare that they have no competing interests.
References
1. Faruque AV, Mateen Khan MA. Unintentional injuries in children: are our homes safe? J Coll Physicians Surg Pak. 2016;26(5):445–446.
2. Gielen AC, McDonald EM, Shields W. Unintentional home injuries across the life span: problems and solutions. Annu Rev Public Health. 2015;36:231–253. doi:10.1146/annurev-publhealth-031914-122722
3. Osborne JM, Davey TM, Spinks AB, McClure RJ, Sipe N, Cameron CM. Child injury: does home matter? Soc Sci Med. 2016;153:250–257. doi:10.1016/j.socscimed.2016.02.017
4. WHO. World Report on Child Injury Prevention; 2008. Available from: https://www.who.int/violence_injury_prevention/child/injury/world_report/en/.
5. WHO. Falls; 2018. Available from: https://www.who.int/news-room/fact-sheets/detail/falls.
6. Alonge O, Hyder AA. Reducing the global burden of childhood unintentional injuries. Arch Dis Child. 2014;99(1):62–69. doi:10.1136/archdischild-2013-304177
7. Hyder AA, Sugerman D, Ameratunga S, Callaghan JA. Falls among children in the developing world: a gap in child health burden estimations? Acta Paediatr. 2007;96(10):1394–1398. doi:10.1111/j.1651-2227.2007.00419.x
8. ICECI Coordination and Maintenance Group. International Classification of External Causes of Injuries (ICECI), Version 1.2. Consumer Safety Institute, Amsterdam and AIHW National Injury Surveillance Unit, Adelaide; 2018. Available from: http://www.iceci.org.
9. Public Health England. Child Accident Prevention Trust, Royal Society for the Prevention of Accidents-Reducing unintentional injuries in and around the home among children under five; 2018. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/696646/Unintentional_injuries_under_fives_in_home.pdf.
10. Kassebaum NJ, Smith AGC, Bernabe E, et al. Global, Regional, and National Prevalence, Incidence, and Disability-Adjusted Life Years for Oral Conditions for 195 Countries, 1990–2015: a Systematic Analysis for the Global Burden of Diseases, Injuries, and Risk Factors. J Dent Res. 2017;96(4):380–387. doi:10.1177/0022034517693566
11. Bhatti JA, Farooq U, Majeed M, Khan JS, Razzak JA, Khan MM. Fall-related injuries in a low-income setting: results from a pilot injury surveillance system in Rawalpindi, Pakistan. J Epidemiol Glob Health. 2015;5(3):283–290. doi:10.1016/j.jegh.2015.01.003
12. Borse NN, Hyder AA. Call for more research on injury from the developing world: results of a bibliometric analysis. Indian J Med Res. 2009;129(3):321–326.
13. Balan B, Lingam L. Unintentional injuries among children in resource poor settings: where do the fingers point? Arch Dis Child. 2012;97(1):35–38. doi:10.1136/archdischild-2011-300589
14. Census of India, Office of the Registrar General & Census Commissioner, India, Ministry of Home Affairs, Government of India. District profile; 2011. Available from: http://www.census2011.co.in/census/district/302-ujjain.html.
15. International Institute for Population Sciences-National Family Health Survey-4 2015-16 District Fact Sheet Ujjain, Madhya Pradesh; 2016. Available from: http://rchiips.org/NFHS/FCTS/MP/MP_FactSheet_435_Ujjain.pdf.
16. Oxford Poverty and Human Development Initiative. Global multidimensional poverty index report. Chapter 2 Madhya Pradesh A case study; 2018. Available from: https://ophi.org.uk/wp-content/uploads/G-MPI_2018_2nd_INDIA_ch.pdf.
17. Fochsen G, Deshpande K, Diwan V, Mishra A, Diwan VK, Thorson A. Health care seeking among individuals with cough and tuberculosis: a population-based study from rural India. Int J Tuberc Lung Dis. 2006;10(9):995–1000.
18. Krishnan S, Hatekar N. Rise of the new middle class in India and its changing structure. Econ Political Weekly. 2017;52(22):40–48.
19. WHO. Training Educating and Advancing Collaboration in Health on Violence and Injury Prevention (TEACHVIP) users’ manual; 2012. Available from: https://apps.who.int/iris/bitstream/handle/10665/44865/9789241503464_eng.pdf;jsessionid=EBC9443D4B39EB85565FC62E84522EB0?sequence=1.
20. Mathur A, Mehra L, Diwan V, Pathak A. Unintentional childhood injuries in Urban and Rural Ujjain, India: a community-based survey. Children (Basel). 2018;5(2). doi:10.3390/children5020023
21. Lamb SE, Jorstad-Stein EC, Hauer K, Becker C. Prevention of Falls Network E, Outcomes Consensus G. Development of a common outcome data set for fall injury prevention trials: the Prevention of Falls Network Europe consensus. J Am Geriatr Soc. 2005;53(9):1618–1622. doi:10.1111/j.1532-5415.2005.53455.x
22. Hosmer DW, Lemeshow S. Goodness of fit tests for the multiple logistic regression model. Commun Stat - Theory Methods. 1980;9(10):1043–1069. doi:10.1080/0361092800882794
23. Cook NR. Use and misuse of the receiver operating characteristic curve in risk prediction. Circulation. 2007;115(7):928–935. doi:10.1161/CIRCULATIONAHA.106.672402
24. Mohan D, Kumar A, Varghese M. Childhood injuries in rural north India. Int J Inj Contr Saf Promot. 2010;17(1):45–52. doi:10.1080/17457300903524862
25. Bhamkar R, Seth B, Setia MS. Profile and risk factor analysis of unintentional injuries in children. Indian J Pediatr. 2016;83(10):1114–1120. doi:10.1007/s12098-016-2159-2
26. Parmeswaran GG, Kalaivani M, Gupta SK, Goswami AK, Nongkynrih B. Unintentional childhood injuries in Urban Delhi: a community-based study. Indian J Community Med. 2017;42(1):8–12. doi:10.4103/0970-0218.199791
27. Bhuvaneswari N, Prasuna JG, Goel MK, Rasania SK. An epidemiological study on home injuries among children of 0–14 years in South Delhi. Indian J Public Health. 2018;62(1):4–9. doi:10.4103/ijph.IJPH_428_16
28. Gupta S, Gupta SK, Devkota S, et al. Fall injuries in Nepal: a countrywide population-based survey. Ann Glob Health. 2015;81(4):487–494. doi:10.1016/j.aogh.2015.07.004
29. Chowdhury SM, Rahman A, Mashreky SR, et al. The horizon of unintentional injuries among children in low-income setting: an overview from Bangladesh Health and Injury Survey. J Environ Public Health. 2009;2009:435403. doi:10.1155/2009/435403
30. Ahmed B, Fatmi Z, Siddiqui AR. Population attributable risk of unintentional childhood poisoning in Karachi Pakistan. PLoS One. 2011;6(10):e26881. doi:10.1371/journal.pone.0026881
31. Lafta R, Al-Shatari S, Cherewick M, et al. Injuries, death, and disability associated with 11 years of conflict in Baghdad, Iraq: a randomized household cluster survey. PLoS One. 2015;10(8):e0131834. doi:10.1371/journal.pone.0131834
32. Saadat S, Hafezi-Nejad N, Ekhtiari YS, et al. Incidence of fall-related injuries in Iran: a population-based nationwide study. Injury. 2016;47(7):1404–1409. doi:10.1016/j.injury.2016.05.001
33. Fuglkjaer S, Dissing KB, Hestbaek L. Prevalence and incidence of musculoskeletal extremity complaints in children and adolescents. A systematic review. BMC Musculoskelet Disord. 2017;18(1):418. doi:10.1186/s12891-017-1771-2
34. Wadhwaniya S, Alonge O, Ul Baset MK, Chowdhury S, Bhuiyan AA, Hyder AA. Epidemiology of fall injury in rural Bangladesh. Int J Environ Res Public Health. 2017;14(8):900. doi:10.3390/ijerph14080900
35. Zhang H, Li Y, Cui Y, Song H, Xu Y, Lee SY. Unintentional childhood injury: a controlled comparison of behavioral characteristics. BMC Pediatr. 2016;16:21. doi:10.1186/s12887-016-0558-1
36. Morrongiello BA. Caregiver supervision and child-injury risk: I. Issues in defining and measuring supervision; II. Findings and directions for future research. J Pediatr Psychol. 2005;30(7):536–552. doi:10.1093/jpepsy/jsi041
37. Ruiz-Casares M, Nazif-Munoz JI, Iwo R, Oulhote Y. Nonadult supervision of children in low- and middle-income countries: results from 61 national population-based surveys. Int J Environ Res Public Health. 2018;15(8):1564. doi:10.3390/ijerph15081564
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.