Back to Journals » Clinical Ophthalmology » Volume 17
Incidence and Pattern of Neuro-Ophthalmological Disorders Presenting to Vitreoretinal Clinics in Bhutan: A 3-Year National Study
Authors Rai BB ![]() , Sarac O, van Kleef JP
, Sarac O, van Kleef JP ![]() , Maddess T
, Maddess T
Received 9 November 2022
Accepted for publication 19 December 2022
Published 6 January 2023 Volume 2023:17 Pages 107—114
DOI https://doi.org/10.2147/OPTH.S396879
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Bhim B Rai,1,2 Ozge Sarac,3,4 Joshua P van Kleef,1 Ted Maddess1
1John Curtin School of Medical Research, Australian National University, Canberra, ACT, Australia; 2Department of Ophthalmology, Jigme Dorji Wangchuck National Referral Hospital, Thimphu, Bhutan; 3Department of Ophthalmology, AYBU Ankara City Hospital, Ankara, Turkey; 4Wills Eye Hospital Neuro-Ophthalmology Department, Philadelphia, PA, USA
Correspondence: Bhim B Rai, John Curtin School of Medical Research, Australian National University, 131 Garran Road, Acton, Canberra, ACT, 2607, Australia, Tel +61 2 6125 9253, Email [email protected]
Purpose: To inform national health policy, we quantified the pattern of neuro-ophthalmological disorders (NODs) presenting to the national vitreoretinal clinics in Bhutan.
Study Design: Retrospective cross-sectional study.
Methods: We reviewed all new NODs patients over three years. Demographic data, presenting complaints, treatment history, systemic diseases, diagnostic procedures, and diagnoses were quantified. Logistic regression examined the odds of factors linked to more common NODs.
Results: Of 226 patients, the majority were males (54.0%), farmers (60.2%), and urbanites (55.8%). Loss of vision was the most common presenting complaint (57.9%), followed by head or orbital trauma (19.5%). The best corrected visual acuity (BCVA) of 216 eyes (47.8%) was ≤ 6/60. Hypertension was the most common systemic disease (16.4%), followed by diabetes (3.5%), and intracranial space-occupying lesions (3.5%). Neuroimaging (37.6%) was the most common diagnostic test performed, followed by visual field testings (VFTs) (22.9%). With a NOD incidence of 7.8% p.a. (226/2913), optic atrophy (OA) was diagnosed in 134 patients (59.3%). Other common NODs were optic neuritis (15.5%), papilloedema (9.3%), and traumatic optic neuropathy (8.4%). Female gender increased the odds for glaucomatous OA by 2.65× (p = 0.044), and age by 1.09× per year (p < 0.001). Being female increased the odds of optic neuritis by 2.57× (p = 0.03).
Conclusion: Over half of the NODs were OA, which could be curable with timely treatment. Improved treatment of glaucoma and non-communicable diseases would reduce the risk of NODs-induced visual loss in Bhutan. The need for improved neuro-ophthalmological assessment and a coordinated multidisciplinary approach to NODs are the highest priorities.
Keywords: Bhutan eye diseases, neuro-ophthalmological disorders, optic atrophy, optic neuritis, papilloedema
Introduction
Neuro-ophthalmological disorders (NODs) are the diseases of the central nervous system (CNS) that manifest in the visual system.1 NODs may cause visual disturbances due to the involvement of the optic nerve, CNS, ocular motility, and pupillary responses.2 There is lack of precise epidemiological data and structured management protocols for NODs, and many NODs fall in the grey area between neuro-ophthalmologists, neuro-surgeons, and neurologists.3 Hospital-based studies reported that the annual incidence of NODs was 9.81 per 100,000 per year in Singapore, with incidence increasing with age,3 and in Thailand it was 1.2%.1
The 2009 Rapid Assessment of Avoidable Blindness (RAAB) survey in Bhutan reported that 22.1% of the blindness/visual impairment were due to posterior segment disorders.4 A hospital-based study reported that NODs involving the optic nerve were the fifth most common disorder among vitreoretinal (VR) disorders.5 Despite this, Bhutan does not possess a neuro-ophthalmologist and therefore NODs are mostly managed by VR specialist who had set up a national referral system. The cases of neuropathies affecting third, fourth and sixth cranial nerves resulting strabismus are managed by a paediatric ophthalmologist, and orbital disorders are managed by an oculoplastic surgeon. The current study is the first to report on NODs presenting to the VR services in Bhutan and is designed to inform national and regional health policies.
Materials and Methods
Study Design and Ethics
This retrospective cross-sectional study was approved by the Research Ethics Board of Health (REBH), Royal Government of Bhutan, Thimphu, and adhered to the principles in the Declaration of Helsinki. Informed consent was waived by the REBH because this retrospective study collected only de-identified data.
Setting and Participants
The study sites included all VR Sub-speciality clinics (VRSCs) in Bhutan. The Jigme Dorji Wangchuck National Referral Hospital (JDWNRH) in Thimphu in western region was the main site, other sites included the eastern regional referral hospital (ERRH) and central regional referral hospital (CRRH). All patients with NODs presenting to the VRSCs for the first time over 3 years (01 May 2013 until 30 April 2016) were included. We did not set any inclusion or exclusion criteria, except 6 cases which were excluded due to incomplete data.
Clinical Examination and Data Collection
The data collected included demography, presenting complaints and duration, treatments received before presenting to the VRSC, and associated systemic diseases, diagnostic tests and the diagnoses. Best corrected visual acuities (BCVA) at presentation were measured using a Snellen chart, Tumbling E for illiterate patients, and the Sheridan Gardners 3 m vision chart for children. Intraocular pressure (IOP) was measured by Goldmann applanation tonometry or iCare tonometry. Anterior and posterior segments were examined under slit-lamp biomicroscopy (BM 900, Haag-Streit, Switzerland), 90D bio-microscopy and indirect ophthalmoscope (Model 125, Welch Allyn, USA). Optical coherence tomography (OCT) scans were performed to confirm retinal and optic disk lesions using a Spectral Domain OCT (Cirrus-HD 4000, Carl Zeiss Germany). Fundus photographs were taken by a VISUCAM-524 (Carl Zeiss, Germany). When indicated, imaging diagnostics such as magnetic resonance imaging (MRI) and computerised tomography (CT) scans were performed to diagnose or rule out intracranial and orbital pathologies. The results of these imaging diagnostics were provided by the qualified radiologists. Lumbar puncture (LP) was also performed when indicated and interpreted by the departments of internal medicine, neuro-surgery, or pathology. Visual field tests (VFTs) were performed with Humphrey Field Analyzer (HFA 3, Carl Zeiss, Germany), and Frequency Doubling Technology (FDT) perimetry (Carl Zeiss Meditec, Dublin, California USA). In paediatric patients, the diagnoses were confirmed by examination under anaesthesia (EUA). Intracranial pathologies such as causes of papilloedema and other intracranial space occupying lesions (ISOL) were confirmed by working collaboratively with the medical internists, neuro-physician and neuro-surgeon. When necessary, imaging technology such as MRI and CT scanning, and LP were sought with results interpreted by qualified radiologists and pathologists respectively. There was overlapping optic neuritis (papillitis) and retrobulbar neuritis. Therefore, for clarity optic neuritis cases include papillitis with or without retrobulbar neuritis, while retrobulbar neuritis has only retrobulbar involvement but no papillitis.
Statistical Analysis
The data were analysed using MATLAB (2020b, The MathWorks, Natick, MA). Comparisons of the expected and observed frequencies employed Chi-squared tests, other factors were examined with t-tests. Logistic regression was used to examine the odds of independent factors linked to the more commonly encountered diseases. A value of p < 0.05 was considered statistically significant.
Results
Demography
A total of 226 new NOD cases attended the VRSC in 3 years. The majority of patients were males (122 patients, 54.0%), and 152 patients (67.3%) were of working age (18–65 years). The mean age of presentation was 44.6 ± 21.7 years, ranging from 7 months to 85 years. Females presented earlier than males: 40.9 ± 22.0 vs 47.8 ± 20.9 years (p = 0.014, Wilcoxon/Rank sum test). Farmers/housewives constituted the biggest group (136 patients, 60.2%), followed by the working-class population (48 patients, 21.3%) namely employees in the private (22 patients, 9.7%), government (21 patients, 9.3%) and corporate (5 patients, 2.2%) sectors. Majority of patients lived in an urban setting (126, 55.8%). Half of the study cohort did not attend modern schooling (Table 1).
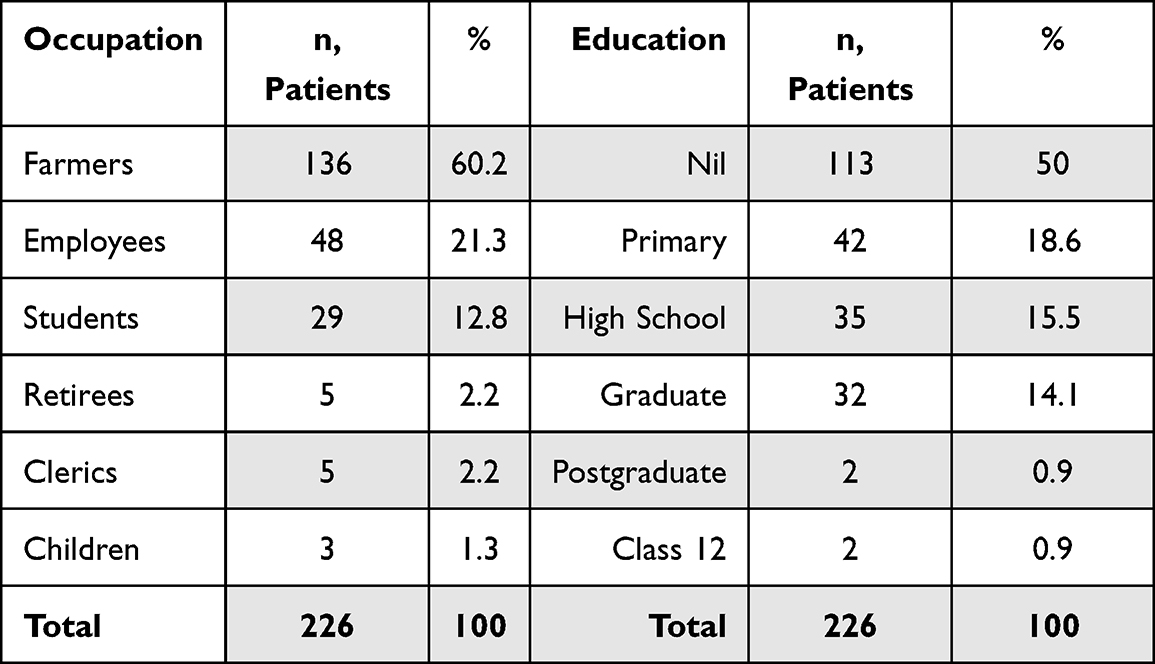 |
Table 1 Demographic Characteristics of Patients |
Presenting Complaints
Eighty-one patients (35.8%) presented with gradually impaired vision, and 50 patients (22.1%) presented with a sudden loss of vision. Forty-four patients (19.5%) presented with trauma such as road traffic accidents (RTAs), fist fights, falls from height, wooden implements, and iron nails or rods. Nineteen patients (8.5%) had received unsatisfactory cataract surgery, so they sought further consultation to find OA in 12 patients (10 unilateral and 2 bilateral); glaucomatous OA (GOA) in 6 patients (4 unilateral and 2 bilateral), and traumatic optic neuropathy (TON) in one patient (Table 2).
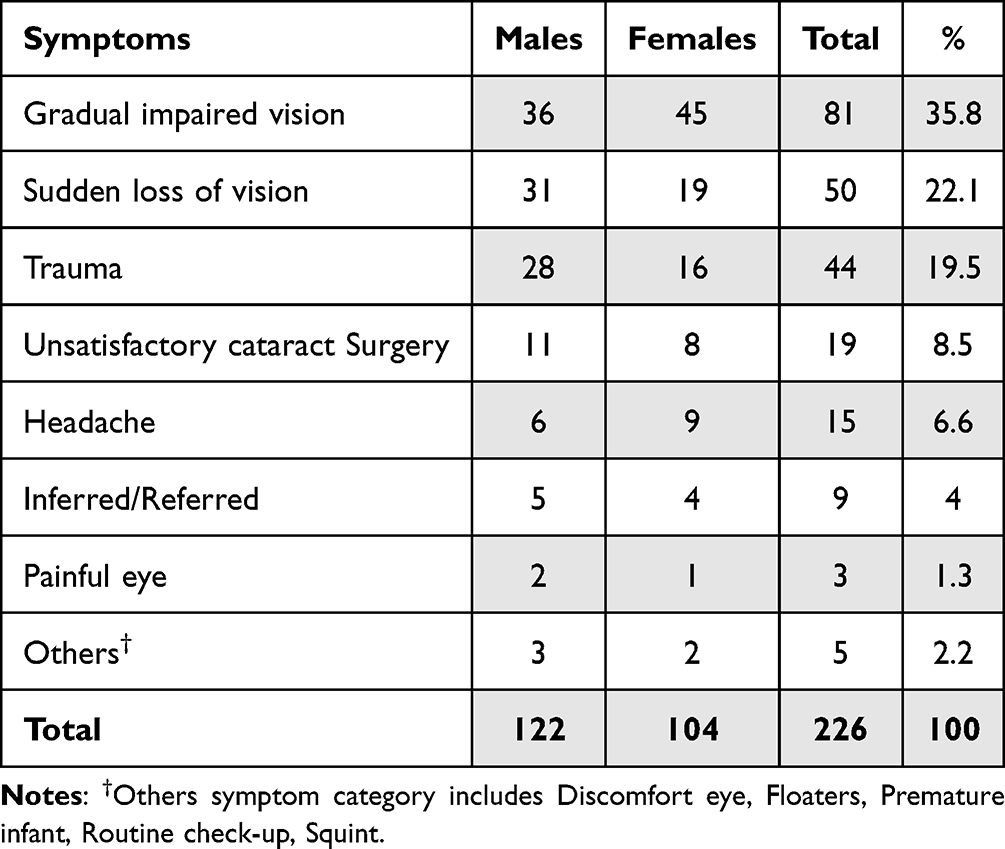 |
Table 2 Presenting Complaints |
The mean duration of symptoms at which the patients sought consultation was 23 months, ranging from a day to 38 years. The median was 3 months, and the interquartile range 0.5 to 24 months.
Systemic Diseases
Hypertension was the most common systemic disorder (37 patients, 16.4%), followed by diabetes mellitus (8 patients, 3.5%), and brain tumour (8 patients, 3.5%). Other systemic co-morbidities were pituitary tumours (3 patients, 1.3%), and pheochromocytoma, chronic kidney disease, and systemic lupus erythematosus in one patient each (0.4%).
Prior Interventions
Cataract operations were the most common intervention (17 patients, 7.5%), followed by ISOL surgery (6 patients, 2.7%), retinal detachment surgery (4 patients, 1.8%), trabeculectomy (2 patients, 0.9%), and peripheral laser iridotomy, intravenous methylprednisolone and parotid tumour operation in one patient each (0.4%).
Visual Acuities
In terms of decimal visual acuity, the mean ± SD across the eyes was 0.32 ± 0.36. The standard conversion to decimal acuities was used for 6/6 to 1/60, while CF was converted to 0.01, HM to 0.005, and NA, NPL, and PL to 0. The BCVA of 216 eyes (47.8%) was ≤6/60 (Figure 1A), 105 patients (46.5%) had binocular vision ≤6/12, while 56 (24.8%) patients had binocular vision ≤6/60 (Figure 1B). Only 26 subjects had BCVA ≥ 6/12 bilaterally.
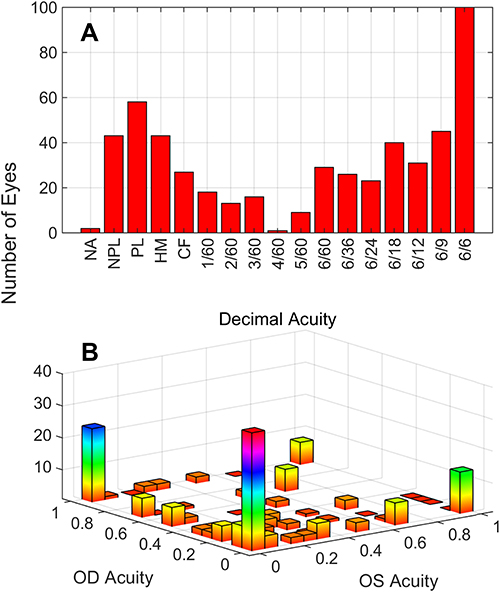 |
Figure 1 Visual acuities. (A) The distribution of visual acuities across the 452 eyes. (B) The distribution of decimal acuities in the two eyes. |
Diagnostic Procedures
Diagnoses were made using an inter-disciplinary approach seeking cross-consultation with radiologists, medical internists, and a neuro-surgeon. MRI of the brain and orbit was the most common diagnostic procedure performed (135 patients, 35.5%) to confirm or rule out intracranial and orbital pathologies, followed by OCT (79 patients, 20.5%), VFT (88 patients, 22.9%) including the HFA (64, 16.6%) and FDT tests (24, 6.3%), haematological tests (23 patients, 6.0%), B-scan ultrasound (10 patients, 2.6%), CT-scan (8 patients, 2.1%), chest X-ray (2 patients, 0.5%), and EUA (1 patient, 0.3%).
Neuro-Ophthalmological Disorders
A total of 226 NOD patients were seen among 2913 VR patients over three years, providing an incidence rate of 7.8% per annum. The most common NOD was OA (134 patients, 59.3%). Among them, 31 patients (13.7%) had GOA. In other cases, the causes included previously diagnosed ON, trauma, and papilloedema. ON was the second most common disease, seen in 35 patients (15.5%). Of them, 31 patients (13.7%) had papillitis and 4 patients (1.8%) had retrobulbar neuritis. Papilloedema was diagnosed in 21 patients (9.3%), TON was seen in 19 patients (8.4%). Malignant hypertensive retinopathy was diagnosed in 9 patients (4.0%). Other details are shown in Table 3.
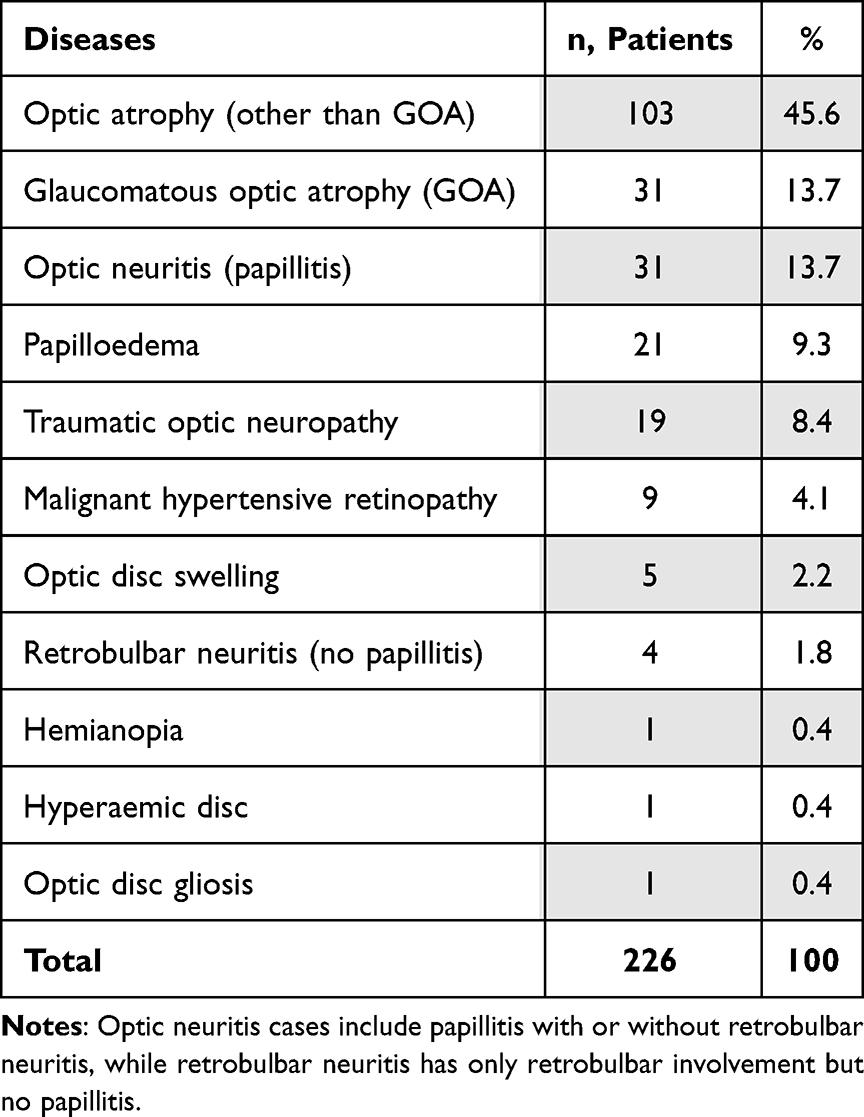 |
Table 3 Neuro-Ophthalmological Disorders/Findings Presenting to the Vitreoretinal Clinics in Bhutan |
Unfortunately, a total of 95 patients (42.0%) had bilateral NODs at initial presentation. To break down by disease, 17 of 31 GOA patients (54.8%), 32 of 103 patients (31.1%) of OA with other causes, 21 of 21 patients (100%) with papilloedema, 12 of 31 patients with ON (38.7%), and 2 of 4 patients (50.0%) with retrobulbar neuritis were bilateral. A total of 49 patients (36.6%) had bilateral OA, combined GOA and OA with other causes, and were deemed blind.
Logistic Regression
We used logistic regression to quantify any factors determining the odds of having some of the more common diseases. Possible contributing factors included age, sex, education, urban vs rural setting, and unilateral disease.
In these models, we examined age relative to mean age so as to minimise the effect on the intercept. Table 4 presents the outcomes for GOA against other diseases. Female gender and age increased the odds of GOA significantly by 2.65x (p ˂ 0.0001), and 1.09x (p = 0.044) per year respectively, while unilateral disease decreased the odds by 0.24x (lower and upper SE 0.15x and 0.39x) (p = 0.003). Not shown are the outcomes for ON, for which being female increased the odds by 2.57x (p = 0.03, SE 1.63x and 4.29x), and age decreased them by 0.97x per year (p = 0.014, SE 0.96x and 0.98x). For OA, only unilateral disease was a significant factor with increased odds by 2.53x (p < 0.002, lower and upper SE 1.90x and 3.36x).
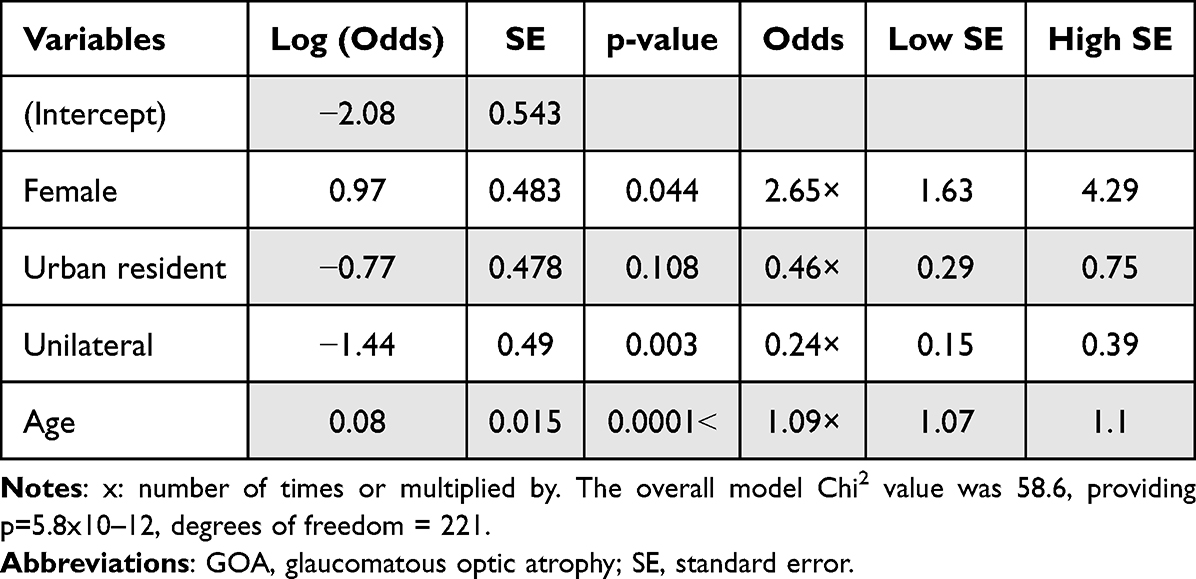 |
Table 4 Logistic Regression Analysis for Diagnosis of GOA |
Discussion
NODs should be of high concern with the rising incidence of inflammatory diseases such as multiple sclerosis, neuro-syphilis, and ISOL.6 In the present study, 67.3% of patients were of working age. At least 19 NODs patients were diagnosed incidentally following unsatisfactory cataract surgery, which hinted that NODs might be more prevalent in the community. OA was the most common NOD (59.3%), 36.6% of which was bilateral, followed by ON (15.5%), papilloedema (9.3%), TON (8.4%), and malignant hypertensive retinopathy (4.1%). Female gender and age increased the odds for GOA by 2.65 times. Being female increased the odds of ON by 2.57 times. The BCVAs were rather poor, with just 32.5% of eyes better than or equal to 6/12, while 47.8% were ≤6/60. In terms of bilateral outcomes, 46.5% of subjects were ≤6/12 in both eyes, and 24.8% ≤6/60. The persons with bilateral BCVAs of ≤6/60 were not significantly older than other subjects.
The occupational breakdown of patients also showed that the farmers were the most affected group, followed by employees of the government, private and corporate sectors. This will affect the already strained Bhutanese human resources immensely. Although modern schooling was introduced in Bhutan in 1961, the monastic system of education is still embraced by Bhutanese people.7 As a result, majority of the elderly patients had not attended modern schooling. This finding agreed with similar studies in Bhutan.5,8
The majority of patients had symptoms for a mean duration of 23 months when they presented for the first time, while only 22.1% presented with sudden loss of vision. This might be a reflection of lower level of education and poor knowledge about the diseases and treatment options, which is typical behaviour of low- to middle-income countries. Alternatively, they might have sought traditional or indigenous healing methods, which are practised commonly in Bhutan. TON was also a common reason for consultation. The details of the modes of injuries were described elsewhere.5 Incidental diagnosis of TON or OA from other causes was common among the patients who received unsatisfactory cataract surgery. The prior interventions some patients had received were for diseases other than the NODs such as cataract, ISOL, retinal detachment and glaucoma. Only one patient had received intravenous methylprednisolone for ON (in India). The main reason for such poor management of NODs was the lack of any neuro-ophthalmologist in the country. Prior to the establishment of VR services in Bhutan NOD cases were either managed by general ophthalmologists or referred to India. However, these patients were very reluctant to travel out of country for treatment, and many of them sought traditional or local healers. ISOL was the second most common systemic disease, which was only fourth in the previous study on the VR diseases.5 This disparity is likely because ISOL causes further diseases within the nervous system.
Neuroimaging, mostly MRI rather than CT-scans of brain and orbit, was required to confirm or rule out ON, TON, and ISOL which directly or indirectly caused NODs. Therefore, it was the most common diagnostic procedure performed. Comparatively, the diagnostic yield of neuroimaging in neuro-ophthalmology is high and cost-effective.9 OCT has revolutionised diagnostic possibilities in ophthalmology including neuro-ophthalmology with its relatively high resolution.10 Similarly, in our study the OCT was used frequently to diagnose NODs. The assessment of VFTs is fundamental to neuro-ophthalmological functional diagnosis including topodiagnostic considerations in case of unexplained visual loss and suspected lesions of the visual pathway non-invasively.11 Likewise, the VFT was performed frequently to diagnose glaucomatous visual field loss or disorders the brain.
OA topped the list of NODs, and unfortunately 49 of these patients had bilateral disease, with consequent poor outcomes (Figure 1). This finding perhaps is a tell-tale sign of the many limitations of the health services and social and developmental milestones in Bhutan: poor availability and accessibility of health facilities, poor referral systems, peoples’ reliance on local healers, and poor health knowledge of the public. There is significant room for improvement. The common causes of OA were glaucoma, trauma, ON and secondary to ISOL, either directly or as part of management complications. Trauma was mainly due to RTA, activities related to agriculture, falls from height and domestic violence.5 Over 57% of Bhutan’s livelihood depends on agriculture, livestock and the forestry sector.12 Bhutan therefore needs to introduce stricter RTA laws to prevent RTA-related injuries, safer agricultural and construction practices, and more stringent laws against the domestic violence.
Malignant hypertensive retinopathy was a significant cause of NOD, which was expected because the hypertensive retinopathy is the most common VR disease.5 Another study reported that 54.1% of hypertensives also had co-existent diabetes with overall prevalence of hypertension and diabetes at 26.0% and 8.2%, respectively.13 Retinal vein occlusion, for which both the hypertensive retinopathy and diabetes are risk factors, was the second most common reason for retinal laser therapy, only next to diabetic retinopathy in Bhutan.8 WHO has reported that 28% of total mortality in Bhutan was due to cardiovascular disease, and another 17% due to other non-communicable diseases.14 The risk factors include harmful use of alcohol, high salt intake, unhealthy diet, physical inactivity, and tobacco use.15 So Bhutan would benefit by controlling non-communicable diseases including dietary modifications, increasing physical activity and intensifying complications screening programs.
We have found that the female gender increased the odds of GOA and ON. Increased level of interleukin-8 (IL-8) is secreted in response to female hormone estradiol, is a significant risk for glaucoma including failure of filtering glaucoma surgery.16 The collagen vascular disease is more common in women is a risk factor for many systemic and ocular diseases, including ON.17
To reduce GOA and glaucoma-related blindness, screening for glaucoma at the community level is critical. Transporting conventional perimeters to remote Bhutanese communities is challenged both geographically and economically. A portable perimeter would aid in this task. The multifocal pupillographic objective perimeter (mfPOP) has been found effective in diagnosing not only glaucoma, but also early diabetic retinopathy prior to the onset of classical signs,18 and AMD.19 Newer mfPOP tests assess both eyes in 82-seconds.20 A rapid objective and portable version of mfPOP would be convenient for screening program in remote areas.21
The study is limited by the small number of participants and by its retrospectivity. Potential neuro-ophthalmological cases such as cranial nerve palsies, and orbital disorders managed by the paediatric ophthalmologists and oculoplastic surgeons were not included. We also lack data on ischaemic optic neuropathy, giant cell arteritis, migraine, transient ischaemic attack and stroke, which will be included in future studies. Critical diagnostic data on serology is missing as this test was noted only with the umbrella term of haematological tests in the registers that we referred for data collection. In some NOD cases, we did not have definitive diagnoses, so we have mentioned only the NOD findings such as papilloedema, hyperaemic disc, or optic disc gliosis. This was due to the loss of patients to follow up after being referred to other departments such as internal medicine and neuro-surgery.
Conclusions
The current study reported only on the NODs presenting to the VR services in Bhutan to inform national and regional health policies. Other cases of neuropathies affecting third, fourth and sixth cranial nerves resulting strabismus managed by a paediatric ophthalmologist, and orbital disorders managed by an oculoplastic surgeon are not reported here. We found 59.3% of all NOD patients already had OA that was beyond being treatable Due to lack of Neuro-ophthalmologists, NODs were managed by a VR specialist who was already overworked with VR diseases. Proper coordination among treating physicians and their eye-care team with a multidisciplinary approach was missing. There is an urgent need for addressing limited human resources, particularly a neuro-ophthalmologist, and developing a multidisciplinary approach to manage NODs to reduce NOD-related blindness and visual impairment.
Funding
This is an Australian Government funding agency awarded to the Australian National University. This agency supplied 50% of the funding for this grant. As required by the grant the other 50% was matched funding 25% from our university (the Australian National University) and 25% from a potential commercial partner, which for this grant was Konan Medical USA.
Disclosure
BBR reports scholarship provided by the Australian National University that supported the study. JPvK and TM report grants from the MRFF Biotechnology Bridge (BTB) Program – research grant number: BTBR100196, during the conduct of the study; grants from Konan Medical USA, outside the submitted work; In addition, they have a patent application (P0040304AU) on novel analysis methods for mfPOP/OFA pending to Konan Medical USA. TM owns shares from EyeCo Pty Ltd. The authors report no other conflicts of interest in this work.
References
1. Mekhasingharak N, Koohasawad S, Chirapapaisan N. Neuro-ophthalmic diseases in a tertiary hospital in Thailand: a prospective study. Thai J Ophthalmol. 2019;33(2):92–100.
2. Rucker JC, Kennard C, Leigh RJ. The neuro-ophthalmological examination. Handb Clin Neurol. 2011;102:71–94.
3. Lim SA, Wong WL, Fu E, et al. The incidence of neuro-ophthalmic diseases in Singapore: a prospective study in public hospitals. Ophthalmic Epidemiol. 2009;16(2):65–73. doi:10.1080/09286580902737516
4. Lepcha NT, Chettri CK, Getshen K, et al. Rapid assessment of avoidable blindness in Bhutan. Ophthalmic Epidemiol. 2013;20(4):212–219. doi:10.3109/09286586.2013.794902
5. Rai BB, Morley MG, Bernstein PS, et al. Pattern of vitreo-retinal diseases at the national referral hospital in Bhutan: a retrospective, hospital-based study. BMC Ophthalmol. 2020;20(1). doi:10.1186/s12886-020-01335-x
6. Walton C, King R, Rechtman L, et al. Rising prevalence of multiple sclerosis worldwide: insights from the Atlas of MS, third edition. Mult Scler. 2020;26(14):1816–1821. doi:10.1177/1352458520970841
7. United Nations Organisations. Bhutan - Education; 2019. Available from: https://www.nationsencyclopedia.com/Asia-and-Oceania/Bhutan-EDUCATION.html.
8. Rai BB, Morley MG, Zangmo P, et al. Retinal laser services in Bhutan: a 3-year national survey. BMC Ophthalmol. 2020;20(1):404. doi:10.1186/s12886-020-01675-8
9. Mehta S, Loevner LA, Mikityansky I, et al. The diagnostic and economic yield of neuroimaging in neuro-ophthalmology. J Neuroophthalmol. 2012;32(2):139–144. doi:10.1097/WNO.0b013e31824e3753
10. Kernstock C, Friebe K, Tonagel F. Anwendungsgebiete für die Optische Kohärenztomografie (OCT) in der Neuroophthalmologie [Applications of optical coherence tomography (OCT) in neuro-ophthalmology]. Klin Monbl Augenheilkd. 2013;230(11):1097–1105. German. doi:10.1055/s-0033-1350786
11. Ungewiss J, Schiefer U. Perimetrie in der neuroophthalmologischen Funktionsdiagnostik: Indikation – Methoden – Topodiagnostik [Perimetry in neuro-ophthalmological function diagnostics: indication - methods - topodiagnostic aspects]. Klin Monbl Augenheilkd. 2018;235(11):1218–1228. German. doi:10.1055/a-0668-5971
12. Climate-Smart Agriculture in Bhutan. International centre for tropical agriculture (CIAT); 2017. Available from: http://sdwebx.worldbank.org/climateportal/doc/agricultureProfiles/CSA-in-Bhutan.pdf.
13. Giri BR, Sharma KP, Chapagai RN, et al. Diabetes and hypertension in urban Bhutanese men and women. Indian J Community Med. 2013;38(3):138–143. doi:10.4103/0970-0218.116349
14. WHO. Non-Communicable Diseases: Country Profile 2018. World Health Organization; 2018.
15. Pelzom D, Isaakidis P, Oo MM, et al. Alarming prevalence and clustering of modifiable noncommunicable disease risk factors among adults in Bhutan: a nationwide cross-sectional community survey. BMC Public Health. 2017;17(1). doi:10.1186/s12889-017-4989-x
16. Chono I, Miyazaki D, Miyake H, et al. High interleukin-8 level in aqueous humor is associated with poor prognosis in eyes with open angle glaucoma and neovascular glaucoma. Sci Rep. 2018;8(1):14533. doi:10.1038/s41598-018-32725-3
17. Sharma SK, Sharma AL, Mahajan VK. Ophthalmic manifestations in patients with collagen vascular disorders: a hospital-based retrospective observational study. Int Ophthalmol. 2021;41(8):2765–2775. doi:10.1007/s10792-021-01833-x
18. Rai BB, Maddess T, Carle CF, et al. Comparing objective perimetry, matrix perimetry, and regional retinal thickness in early diabetic macular oedema. Trans Vis Sci Tech. 2021;10(32):1–12. doi:10.1167/tvst.10.13.32
19. Rai BB, Essex RW, Sabeti F, et al. An objective perimetry study of central versus peripheral sensitivities and delays in age-related macular degeneration. Transl Vis Sci Technol. 2021;10(14):24. doi:10.1167/tvst.10.14.24
20. Rai BB, Sabeti F, Carle CF, et al. Rapid objective testing of visual function matched to the ETDRS grid and its diagnostic power in age-related macular degeneration. Ophthalmol Sci. 2022;2(2):100143. doi:10.1016/j.xops.2022.100143
21. Maddess T, van Kleef JP, Rohan EMF, et al. Rapid, non-contact multifocal visual assessment in multiple sclerosis. Neurol Sci. 2022. doi:10.1007/s10072-022-06387-z
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.