Back to Journals » Clinical Ophthalmology » Volume 16
Incidence and Clinical Characteristics of Postoperative Endophthalmitis After Ab-Interno Canaloplasty
Authors Khan A, Riaz KM ![]() , Rangu N, Shah VA, Hussain ZS, Khaimi MA
, Rangu N, Shah VA, Hussain ZS, Khaimi MA
Received 7 October 2022
Accepted for publication 15 November 2022
Published 22 November 2022 Volume 2022:16 Pages 3875—3882
DOI https://doi.org/10.2147/OPTH.S392322
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Asher Khan,1,2 Kamran M Riaz,2 Neal Rangu,1,2 Vinay A Shah,2 Zain S Hussain,2,3 Mahmoud A Khaimi2
1College of Medicine, University of Oklahoma, Oklahoma City, OK, USA; 2Dean McGee Eye Institute, University of Oklahoma, Oklahoma City, OK, USA; 3University of Medicine and Health Sciences, Basseterre, Saint Kitts and Nevis
Correspondence: Kamran M Riaz, Dean McGee Eye Institute, University of Oklahoma, 608 Stanton L. Young Blvd, Oklahoma City, OK, 73104, USA, Tel +1 405-271-1095, Fax +1 405-271-3680, Email [email protected]
Introduction: Postoperative endophthalmitis (POE) is a rare but devastating complication of ophthalmic surgeries. Microinvasive glaucoma surgery (MIGS) procedures have become increasingly utilized for the surgical reduction of intraocular pressure (IOP). Ab-interno canaloplasty (ABiC) is a popular MIGS procedure, but POE rates and clinical effects following ABiC have not been studied.
Methods: This study conducted a retrospective review of all consecutive cases of either standalone ABiC or combined ABiC with phacoemulsification performed at a tertiary care academic referral center from 2015 to 2021. Exclusion criteria included a history of incisional glaucoma surgery, retinal surgery, or additional concurrent microinvasive glaucoma surgery (MIGS) at the time of ABiC. The rates of POE after ABiC were calculated with 95% confidence intervals (CI) based on the Clopper-Pearson exact method.
Results: Of 3256 cases of ABiC, one case (0.03%, 1/3256, 95% CI: 0.00– 0.17%) of post-ABiC endophthalmitis was identified. The rate of POE in standalone ABiC was 0.00% (0/1332 cases, 95% CI: 0.00– 0.28%), whereas the rate in combined ABiC with phacoemulsification was 0.05% (1/1924 cases, 95% CI: 0.00– 0.29%). Additionally, the rate of POE following stand-alone cataract surgery, 0.10%, 11/11,470 cases, 95% CI: 0.05– 0.17%), total cataract surgeries, 0.06% (17/28,013 cases, 95% CI: 0.04– 0.10%), total MIGs, excluding ABiC, surgeries, 0.08%, (3/3845 cases, 95% CI: 0.02– 0.23%) portray non-inferiority of ABiC in the risk of POE. The case of ABiC-POE presented four days after surgery and required a vitreous tap with intraocular injection of antibiotics and pars plana vitrectomy. No causative organism was identified. A final 1-year follow-up revealed a corrected distance visual acuity of 20/40 and stable glaucoma.
Conclusion: The rate of POE after ABiC (1 per 3256 cases) is statistically non-inferior to the reported incidence of POE after other MIGS and incisional glaucoma surgeries.
Keywords: ab-interno canaloplasty, canaloplasty, endophthalmitis, post-operative infections
Plain Language Summary
Ocular infections after eye surgeries are undesirable events that can have visually significant consequences, including loss of vision. Surgeries for glaucoma have historically involved procedures with large incisions and significant complication rates, including infections. Recently, a new class of glaucoma surgeries known as “microinvasive glaucoma surgeries” (MIGS) has emerged as techniques offering smaller incisions, faster healing times, and more effectiveness than historically performed procedures. However, postoperative infections (known as postoperative endophthalmitis (POE)) remain an area of interest and concern among ophthalmic surgeons. Ab-interno canaloplasty (ABiC) is a procedure with some similarities to other MIGS procedures but also has notable differences in surgical approach and tissue manipulation. In this paper, we report the rates of POE after ABiC at our tertiary-care referral center across 3256 cases. We observed only one case of POE after ABiC, which is lower than the POE rates reported for other MIGS procedures. While the purpose of our paper is not to dictate practice patterns for ophthalmologists, we believe the information presented in this manuscript is of interest to surgeons as they decide which MIGS procedure is most suitable and indicated for their respective patient populations.
Introduction
In recent years, numerous microinvasive glaucoma surgery (MIGS) procedures have been introduced within ophthalmology. Some MIGS procedures can be performed as standalone surgeries, while others may be combined with cataract surgery, and can effectively reduce elevated intraocular pressures (IOP), especially when topical medications are insufficient. Within the spectrum of MIGS procedures, ab-interno canaloplasty (ABiC) is an angle-based procedure involving 360-degree catheterization and viscodilation of Schlemm’s canal to treat mild to moderate primary open-angle glaucoma (POAG).1,2 Similar to other MIGS procedures, ABiC offers advantages such as minimal tissue disruption and rapid recovery times.3 ABiC may be performed as a standalone procedure or combined with phacoemulsification. Whereas most currently utilized MIGS procedures primarily work on local or regional locations of the anterior chamber angle and cause an increased focal aqueous outflow, ABiC affects the entire canal and distal collector channels. In contrast to other MIGS procedures, ABiC does not involve any device placement, allowing for the preservation of angle anatomy for future angle-based treatments if needed.1
Postoperative endophthalmitis (POE) is characterized by marked infection and inflammation of intraocular tissues following ophthalmic surgery.4 POE is a relatively rare complication, with incidence rates ranging from 0.02%–0.71% after cataract surgery and 0.2–6.3% after glaucoma surgery.5,6 POE therapeutic approaches, such as intracameral antibiotic injections, have contributed to the relatively rare occurrence of POE.7 Following cataract surgery, Bhatta et al reported that the administration of intracameral antibiotics reduced POE occurrence from 0.144% to 0.025%.8 Recently, the incidence rates of POE after several MIGS procedures were reported by Starr et al: 0.13% (4/3055 cases, 95% CI: 0.04–0.30%).9 However, ABiC was not included and remains an understudied MIGS procedure, especially regarding its safety profile, clinical efficacy, and POE rates. To our knowledge, no previous studies have reported the rate and clinical features of the complication POE after ABiC.9 We report our experience of POE after ABiC over the last six years among multiple surgeons at a large tertiary care academic medical center.
Materials and Methods
This was a retrospective chart review of all consecutive cases of either standalone ABiC or ABiC combined with phacoemulsification performed at the study institution from October 1, 2015 to May 31, 2021. This study adhered to the tenets of the Declaration of Helsinki and its later amendments. Ethics approval was obtained from the University of Oklahoma Institutional Review Board (IRB: 6173), and HIPAA regulations were followed. The IRB determined that informed consent was not necessary for this study, given the retrospective chart review; thus, this was waived for this specific study.
Concomitant cataract surgery at the time of ABiC was allowed, as ABiC is most frequently performed in conjunction with phacoemulsification.1 For combined cases, phacoemulsification was completed before the ABiC procedure. Inclusion criteria were standalone ABiC cases and cases of ABiC combined with phacoemulsification performed in patients at least 18 years of age with an established history of POAG. Only cases in which both the ABiC procedure and POE diagnosis and treatment were performed at the study institution were included in the final analysis. If patients did not complete a follow-up visit, their data were treated as missing. Exclusion criteria included history of incisional glaucoma surgery, retinal surgery, or additional concurrent MIGS performed at the time of ABiC. Cases associated with preexisting endophthalmitis, systemic infection, angle-closure glaucoma, or mixed-mechanism glaucoma were also excluded.
Data were presented descriptively using mean, standard deviation (SD), count, and percentage, and analyzed using Microsoft Excel 365 for Windows (v. 2205, Microsoft Corp, Redmond, Washington, USA) and the SAS (v9.4) software. Due to binomial nature of POE occurrences, the rates of POE after ABiC were calculated together with 95% confidence intervals (CI) using the Clopper-Pearson exact method via normal approximation.
All ABiC cases were performed using the iTrack microcatheter (Nova Eye Medical, Fremont, California, USA) in the manner previously described.1,2 All surgeries were performed by one of 28 surgeons (4 attending surgeons, 6 fellows, and 20 residents) at our institution. All ABiC patients underwent pre- and postoperative evaluations, which included assessments of pain, lid edema, history of glaucoma, ocular surgical history, ocular medication use, IOP, corrected distance visual acuity (CDVA), gonioscopy, slit lamp examination (including evaluation of anterior chamber reaction), and posterior segment evaluation when indicated. Postoperative examinations were performed 1 day, 1 week, 1 month, 6 months, and 12 months after surgery. All patients routinely received postoperative topical antibiotics (ofloxacin 0.3%) dosed four times a day for one week and topical steroids (loteprednol 0.5% suspension) dosed four times a day for three days, followed by a reduction to once a day for three days. Of note, our single-center institutional protocol does not permit use of intracameral antibiotics. Topical hypotensive medications were discontinued postoperatively and reintroduced in instances where IOP rose above the target value determined for each patient. Cases of POE were diagnosed clinically based on history and exam findings, including reduced vision, pain, and hypopyon. Only patients who received vitreous tap with intraocular injection of antibiotics, independent of microbiology results, were diagnosed with POE.
Results
Patient demographic data are summarized in Table 1. During the 6-year study period, 3256 consecutive ABiC procedures were performed in 2123 patients. The mean age of patients included in the study was 70.6 years (SD 10.3). Of these patients, 1111 were male and 1012 were female. POE rates are portrayed in Table 2. Of the 3256 cases, 1924 had combined phacoemulsification. One case of POE was identified from 3256 ABiC cases (1/3256 eyes; 0.03%, 95% CI: 0.00–0.17%). The rate of POE in standalone ABiC was 0.00% (0/1332 cases, 95% CI: 0.00–0.28%), and the rate in combined ABiC with phacoemulsification was 0.05% (1/1924 cases, 95% CI: 0.00–0.29%). POE rate following cataract surgery alone was 0.01% (11/11,470 cases, 95% CI: 0.05–0.17%) and the POE rate following total cataract surgeries was 0.04% (17/28,013 cases, 95% CI: 0.04–0.10%). The rate of POE in total MIGS excluding ABiC was 0.08% (3/3845 cases, 95% CI: 0.02–0.23%), and the rate of POE in MIGS surgeries alone, excluding ABiC, was 0.00% (0/1692 cases, 95% CI: 0.00–0.22%).
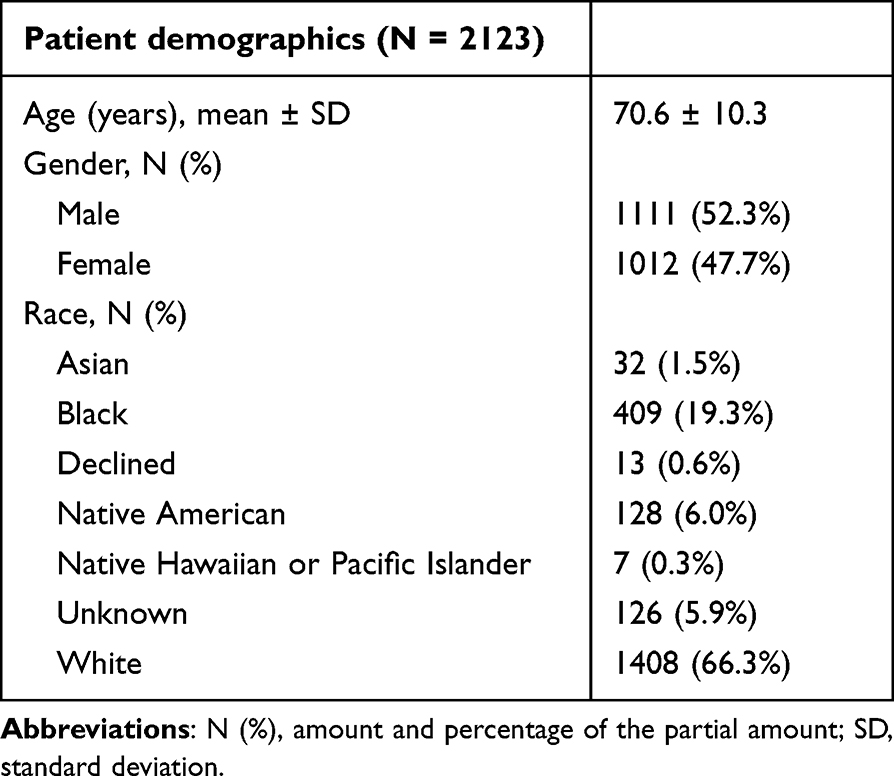 |
Table 1 Patient and Case Demographic Data for All ABiC Cases |
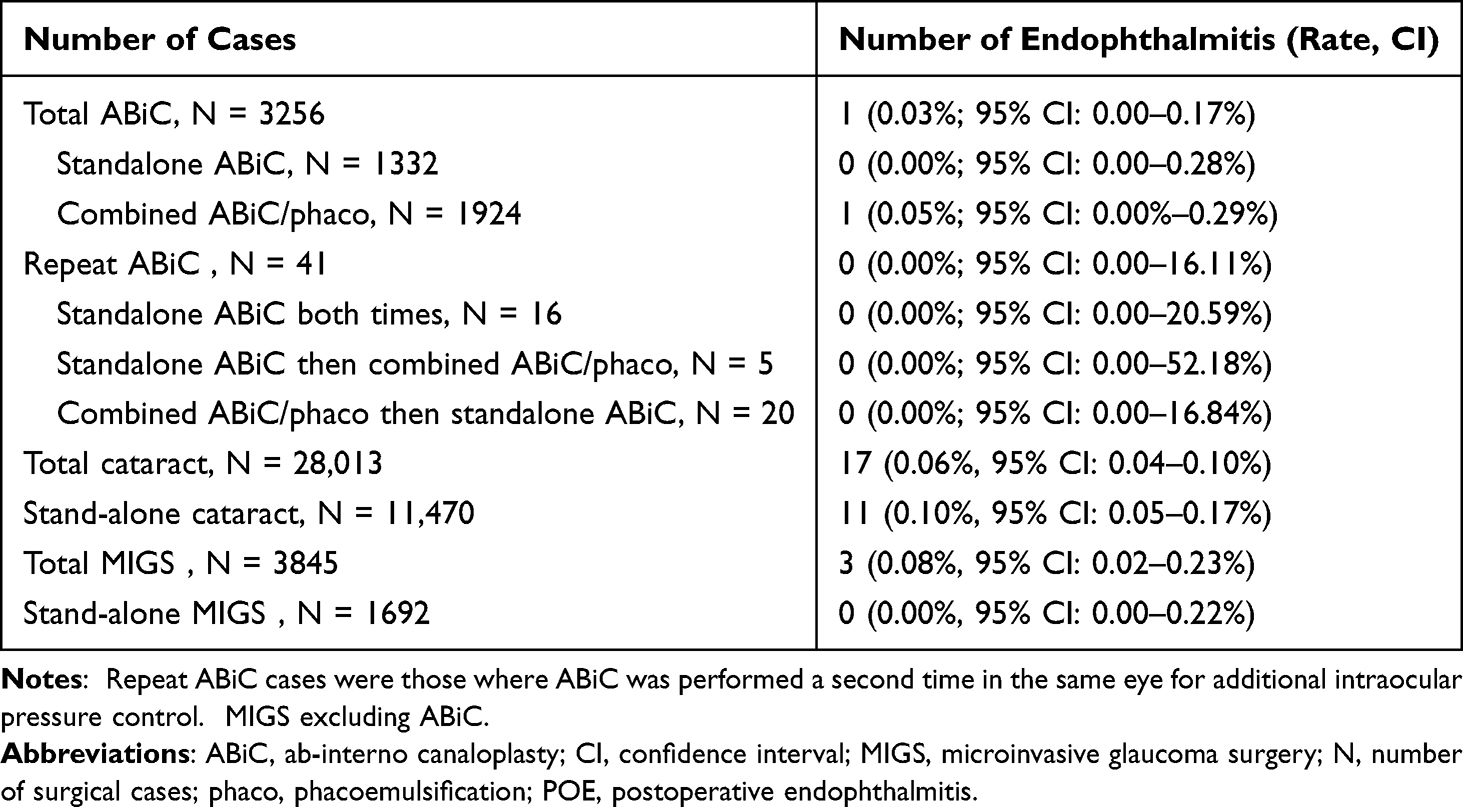 |
Table 2 POE Rates Following Ocular Surgeries at the Study Institution |
Of note, there were 21 cases of POE, inclusive of all ocular surgeries, at our institution during the study period. Of these, three were associated with non-ABiC MIGS procedures: 2 cases after endocyclophotocoagulation combined with micro-bypass stent (iStent; Glaukos Corp, Aliso Viejo, California) and phacoemulsification; and 1 case after trabeculectomy using the Ex-PRESS Glaucoma Filtration Device (Alcon Inc., Geneva, Switzerland) combined with phacoemulsification. The other 18 POE cases occurred after cataract surgery alone or retinal surgeries in nonglaucomatous eyes.
Clinical characteristics of POE after ABiC case are summarized in Table 3. This patient presented with blurred vision and ophthalmalgia four days after undergoing ABiC combined with phacoemulsification. Clinical examination was notable for hand motion CDVA, IOP 40 mm Hg, and profound anterior and posterior segment inflammation. Based on the history and exam findings, a clinical diagnosis of POE was made, and the patient received an immediate vitreous tap with intraocular injection of 1 mg vancomycin and 2.25 mg ceftazidime. Due to a worsening clinical course, the patient underwent pars plana vitrectomy with a repeat injection of 1 mg vancomycin and 2.25 mg ceftazidime in the operating room. No causative organism was identified. The patient’s condition subsequently improved, and a 2-year follow-up demonstrated a maintained CDVA of 20/40 and IOP 8 mm Hg, without requiring additional intraocular surgeries. Throughout the follow-up period, the patient’s IOP measurements remained below target levels without needing topical hypotensive medications.
 |
Table 3 Clinical Characteristics of Post-ABiC Endophthalmitis Case |
Discussion
POE is a vision-threatening complication that can occur after intraocular surgery, with incidence rates varying depending on the type of surgery performed.5,6 MIGS procedures have recently gained significant interest among anterior segment surgeons and glaucoma specialists. Smaller incisions, avoidance of antimetabolites,10 combination with phacoemulsification,11 and less surgical manipulation of intraocular tissues in MIGS procedures may partially explain their increased popularity. Surgeons may adopt MIGS procedures as these advantages may translate to a lower risk of POE, especially when compared to traditional incisional glaucoma surgeries. In the present study, we report one case of POE in a consecutive, multi-surgeon series of 3256 ABiC cases.
We observed that the rate of POE after ABiC remains statistically non-inferior compared to other MIGS procedures,9 even though ABiC is most frequently performed in conjunction with cataract surgery at our institution, as seen in our case of POE discussed earlier (Table 2). This patient eventually reached a stable visual outcome and controlled IOP after additional treatment. We also note that the rate of POE after ABiC is similar to POE after cataract surgery.5,6,12 It is plausible that the incision size (ranging from 1.8 to 2.4 mm, depending on surgeon preference) utilized for phacoemulsification may be an independent risk factor for POE. Thus, the ABiC procedure itself likely does not impose a significant added risk for infection.13 For the bulk of the procedure, ABiC utilizes the initial incision created for phacoemulsification and does not require making any additional large-sized incisions that may further increase the risk for POE.14–19 Notably, no cases of POE were observed after standalone ABiC (0/1332 cases, 0.00%; 95% CI: 0.00–0.28%). However, we emphasize that the purpose of this study was to characterize the rate and clinical features of POE cases after ABiC. Extrapolating whether our case of post-ABiC endophthalmitis resulted from the cataract surgery or the ABiC component is outside the scope of this study; however, the rate of POE secondary to ABiC is not statistically significantly greater than the risk of POE secondary to cataract surgery from our high surgical-volume, tertiary care referral center nor from previously published literature.5,6,12 More granularly, this study presents useful information regarding the safety profile of ABiC against POE development from cataract surgery alone (rate = 0.10%, 95% CI 0.05–0.17%) and all cataract surgery groups (rate = 0.06%, 95% CI 0.04–0.10%). Additional information is provided in Table 2.
Published reports in the literature regarding POE after MIGS procedures are limited at this time. A report from another tertiary-care referral institution reviewed numerous MIGS procedures among multiple surgeons and found a prevalence of bacterial endophthalmitis after MIGS procedures of 0.13%.9 The authors reported 13 total cases of POE, with 9 cases after the micro-bypass stent (iStent; Glaukos Corp, Aliso Viejo, California) combined with phacoemulsification; 3 cases, one of which was combined with phacoemulsification, associated with the ab-interno gel stent (Xen Gel stent; Allergan Plc, Dublin, Ireland); and 1 case after a standalone suprachoroidal micro-stent (CyPass Microstent; Alcon Inc., Geneva, Switzerland). Of note, this study included the OMNI surgical system (Sight Sciences, Inc., Menlo Park, CA, USA), which utilizes a combined canaloplasty-trabeculotomy approach.
Among currently utilized MIGS procedures,20–24 ABiC has notable differences, such as comprehensively addressing blockages in the collector channels with a pressurized, volumetric, and circumferential delivery of viscoelastic.1,2 Instead of cutting or removing portions of the trabecular meshwork, as performed in trabeculotomy procedures including the OMNI device, ABiC involves only a small perforation of the trabecular meshwork followed by 360-degree cannulation and viscodilation of Schlemm’s canal. Additionally, ABiC does not require the implantation of devices or hardware but instead restores natural outflow channels with no significant amount of tissue damage.1,14–19 In our study, we noted a statistically non-inferior POE rate after ABiC, factoring in the lengthy time period and multiple surgeons of variable experience levels. The differences mentioned above of ABiC regarding anatomical approach and surgical technique may partially explain the lower rate of POE after ABiC seen at our institution compared to the higher rates of POE after MIGS procedures observed elsewhere.5,9 Additionally, 41 repeat ABiC cases for additional IOP control were performed during the study period, none of which resulted in POE. This suggests that ABiC may be safely repeated in recalcitrant cases while simultaneously conferring a statistically non-inferior risk of POE.
We propose that while many MIGS procedures may effectively reduce IOP, the safety profile, especially concerning POE risk, is not similar across all procedures. For example, previous authors reported that tube exposure with glaucoma drainage devices (GDDs) was the most significant risk factor associated with aqueous shunt-related endophthalmitis.25–28 This may also partially explain the increased risk and rates of POE associated with the ab-interno gel stent, as its subconjunctival location leads to the potential for tube exposure.29,30 It is also plausible that procedures involving higher amounts of iatrogenic tissue manipulation or destruction may increase the risk of POE, reflected by the higher POE rates observed with incisional glaucoma surgeries.31,32 Additionally, GDDs involve an implanted device in the eye; we note that in the series by Starr et al, most POE cases were associated with device-based MIGS procedures, namely the micro-bypass stent and suprachoroidal micro-stent.9 Further research, including multivariate analysis of MIGS procedures and potential risk factors, is needed for future study.
The strengths of this study include a lengthy time period, a relatively high number of cases at a single center, and standardized surgical techniques among multiple surgeons. However, this study is not without limitations. First, the calculated rates in this study assume that all patients with POE after ABiC performed at our institution were also managed by our retina service; thus, if a patient developed POE and sought treatment elsewhere, this study may underreport the true rate. Second, some inaccuracies may result from the inherently low event rate of POE after ABiC, though the rate is comparable with rates of POE after other intraocular surgeries.9 In summary, while this study represents the largest to-date review of POE in eyes that underwent ABiC, a larger, prospective, comparative, multi-center study of commonly utilized MIGS procedures and their relative risk for POE is warranted.
Conclusions
The purpose of this study was not to comment on the efficacy or superiority of a given MIGS procedure over another nor promote ABiC over other MIGS procedures. Ultimately, the decision for which MIGS procedure to perform is per the clinical judgment and surgical experience of the treating surgeon. Although POE after MIGS procedures remains a rare, sentinel event, these cases merit interest among anterior segment and glaucoma surgeons who may perform a multitude of MIGS procedures. As MIGS procedures continue to gain popularity, we offer that ABiC is a procedure with an excellent infection safety profile consistent with other MIGS procedures and should be considered in surgeons’ armamentarium for IOP reduction.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are not publicly available due to institutional policies regarding data sharing outside of approved researchers within the university. Upon reasonable written request, interested researchers may submit a request for de-identified, anonymized data to our administration team which we can relay to the institutional data monitoring board (IRB) for further review.
Ethics Approval and Informed Consent
This study adhered to the tenets of the Declaration of Helsinki and its later amendments. Ethics approval was obtained from the university’s Institutional Review Board (IRB: 6173), and HIPAA regulations were followed.
Acknowledgments
The authors would like to thank Joel Scott, health-care analyst at Dean McGee Eye Institute, for assistance in providing surgical data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
The authors report no funding support for this study.
Disclosure
Mahmoud A. Khaimi is Chief Medical Consultant for Nova Eye Medical (iTrack). The other authors report no conflicts of interest in this work.
References
1. Khaimi MA. Canaloplasty: a minimally invasive and maximally effective glaucoma treatment. J Ophthalmol. 2015;2015:1–5. doi:10.1155/2015/485065
2. Gallardo MJ. 24-month efficacy of viscodilation of schlemm’s canal and the distal outflow system with iTrack ab-interno canaloplasty for the treatment of primary open-angle glaucoma. Clin Ophthalmol. 2021;15:1591–1599. doi:10.2147/OPTH.S272506
3. Vinod K, Gedde SJ. Safety profile of minimally invasive glaucoma surgery. Curr Opin Ophthalmol. 2021;32:160–168. doi:10.1097/ICU.0000000000000731
4. Hanscom TA. Postoperative endophthalmitis. Clin Infect Dis. 2004;38:542–546. doi:10.1086/381262
5. Zheng CX, Moster MR, Khan MA, et al. Infectious endophthalmitis after glaucoma drainage implant surgery: clinical features, microbial spectrum, and outcomes. Retina. 2017;37:1160–1167. doi:10.1097/IAE.0000000000001329
6. Nowak MS, Grzybowski A, Michalska-Małecka K, et al. Incidence and characteristics of endophthalmitis after cataract surgery in Poland, during 2010–2015. Int J Environ Res Public Health. 2019;16:2188. doi:10.3390/ijerph16122188
7. Shorstein NH, Winthrop KL, Herrinton LJ. Decreased postoperative endophthalmitis rate after institution of intracameral antibiotics in a Northern California eye department. J Cataract Refract Surg. 2013;39:8–14. doi:10.1016/j.jcrs.2012.07.031
8. Bhatta S, Pant N, Poudel M. Postoperative endophthalmitis with and without intracameral moxifloxacin prophylaxis in a high volume surgery setting. BMJ Open Ophthalmol. 2021;6:e000609. doi:10.1136/bmjophth-2020-000609
9. Starr MR, Huang D, Israilevich RN, et al. Endophthalmitis after minimally invasive glaucoma surgery. Ophthalmology. 2021;128:1777–1779. doi:10.1016/j.ophtha.2021.06.004
10. Higginbotham EJ, Stevens RK, Musch DC, et al. Bleb-related endophthalmitis after trabeculectomy with mitomycin c. Ophthalmology. 1996;103:650–656. doi:10.1016/S0161-6420(96)30639-8
11. Lee GA, Porter AJ, Vincent RA, Makk J, Vincent SJ. Combined phacoemulsification and microinvasive glaucoma surgery in comparison to phacoemulsification alone for open angle glaucoma. Eye. 2020;34:312–318. doi:10.1038/s41433-019-0459-2
12. Oshika T, Ohashi Y. Endophthalmitis after cataract surgery: effect of behind-the-lens washout. J Cataract Refract Surg. 2017;43:1399–1405. doi:10.1016/j.jcrs.2017.08.009
13. Cao H, Zhang L, Li L, Lo S. Risk factors for acute endophthalmitis following cataract surgery: a systematic review and meta-analysis. PLoS One. 2013;8:e71731.
14. Khaimi MA. Long-term medication reduction in controlled glaucoma with iTrack ab-interno canaloplasty as a standalone procedure and combined with cataract surgery. Ther Adv Ophthalmol. 2021;13:25158414211045751.
15. Riaz KM, Gill MS, Murphy DA, Ding K, Khaimi MA. Surgical management of intraocular pressure with ab interno canaloplasty in postkeratoplasty patients: 12-month results. Cornea. 2022. doi:10.1097/ICO.0000000000003009
16. Harvey BJ, Khaimi MA. A review of canaloplasty. Saudi J Ophthalmol. 2011;25:329–336. doi:10.1016/j.sjopt.2011.08.003
17. Khaimi MA, Dvorak JD, Ding K. An analysis of 3-year outcomes following canaloplasty for the treatment of open-angle glaucoma. J Ophthalmol. 2017;2017:1–7. doi:10.1155/2017/2904272
18. Khaimi MA. A retrospective analysis of the use of loteprednol etabonate ophthalmic suspension 0.5% following canaloplasty. Clin Ophthalmol. 2018;12:319–329. doi:10.2147/OPTH.S153912
19. Khaimi MA. Canaloplasty using iTrack 250 microcatheter with suture tensioning on Schlemm’s canal. Middle East Afr J Ophthalmol. 2009;16:127–129. doi:10.4103/0974-9233.56224
20. Lavia C, Dallorto L, Maule M, Ceccarelli M, Fea AM. Minimally-invasive glaucoma surgeries (MIGS) for open angle glaucoma: a systematic review and meta-analysis. PLoS One. 2017;12:e0183142.
21. Brandão LM, Grieshaber MC. Update on minimally invasive glaucoma surgery (MIGS) and new implants. J Ophthalmol. 2013;2013:1–12. doi:10.1155/2013/705915
22. Pillunat LE, Erb C, Jünemann AG, Kimmich F. Micro-invasive glaucoma surgery (MIGS): a review of surgical procedures using stents. Clin Ophthalmol. 2017;11:1583–1600. doi:10.2147/OPTH.S135316
23. Nichani P, Popovic MM, Schlenker MB, Park J, Ahmed IIK. Microinvasive glaucoma surgery: a review of 3476 eyes. Surv Ophthalmol. 2021;66:714–742. doi:10.1016/j.survophthal.2020.09.005
24. Shalaby WS, Jia J, Katz LJ, Lee D. iStent inject: comprehensive review. J Cataract Refract Surg. 2021;47:385–399. doi:10.1097/j.jcrs.0000000000000325
25. Li A, Conti TF, Singh RP, Challa P. Infectious and sterile endophthalmitis in eyes with glaucoma drainage device from two large ophthalmic institutions. Ophthalmol Glaucoma. 2021;4:193–200. doi:10.1016/j.ogla.2020.09.003
26. Robbins CB, Feng HL, Fekrat S. Management patterns and visual outcomes of endophthalmitis after glaucoma drainage device placement: a case series. J Glaucoma. 2021;30:5–7. doi:10.1097/IJG.0000000000001679
27. Gedde SJ, Scott IU, Tabandeh H, et al. Late endophthalmitis associated with glaucoma drainage implants. Ophthalmology. 2001;108:1323–1327. doi:10.1016/S0161-6420(01)00598-X
28. Levinson JD, Giangiacomo AL, Beck AD, et al. Glaucoma drainage devices: risk of exposure and infection. Am J Ophthalmol. 2015;160:516–521. doi:10.1016/j.ajo.2015.05.025
29. Olgun A, Imamoğlu S, Karapapak M, Düzgün E, Kaçar H. Endophthalmitis after XEN gel stent implantation: 2 cases. J Glaucoma. 2018;27:191–194. doi:10.1097/IJG.0000000000001076
30. Lim R, Lim KS. XEN implant-related endophthalmitis. Ophthalmology. 2018;125(209):30. doi:10.1016/j.ophtha.2017.10.019
31. Poulsen EJ, Allingham RR. Characteristics and risk factors of infections after glaucoma filtering surgery. J Glaucoma. 2000;9:438–443. doi:10.1097/00061198-200012000-00004
32. Simonett JM, Choi RY, Flaxel CJ. Filtering-associated endophthalmitis after trabeculectomy or tube-shunt implant. Ophthalmol Retina. 2021;5:279–284. doi:10.1016/j.oret.2020.07.013
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.