Back to Journals » International Journal of Women's Health » Volume 17
In Vitro Fertilization and Dichorionic-Diamniotic Twin Pregnancies in Nulliparous Women: A Retrospective Cohort Study Comparing Pregnancy Outcomes Between Advanced and Younger Maternal Age Groups
Authors He MP, Jian WQ, Yuan CL, He SM, He MR, Yan J, Huang JC, Zhao KS ![]()
Received 23 May 2025
Accepted for publication 9 July 2025
Published 5 August 2025 Volume 2025:17 Pages 2433—2442
DOI https://doi.org/10.2147/IJWH.S538630
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Mei Ping He,* Wen Qian Jian,* Chun Lan Yuan, Shi Mei He, Mei Rong He, Jian Yan, Jian Chun Huang, Kai Sun Zhao
Department of Obstetrics, The Third Affiliated Hospital of Guangxi Medical University, The Second Nanning People’s Hospital, Nanning, Guangxi, 530031, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Kai Sun Zhao, Department of Obstetrics, The Third Affiliated Hospital of Guangxi Medical University, The Second Nanning People’s Hospital, No. 13, Dancun Road, Jiangnan District, Nanning City, Guangxi Zhuang Autonomous Region, People’s Republic of China, Tel +86 13737085418, Email [email protected] Jian Chun Huang, Department of Obstetrics, The Third Affiliated Hospital of Guangxi Medical University, The Second Nanning People’s Hospital, No. 13, Dancun Road, Jiangnan District, Nanning City, Guangxi Zhuang Autonomous Region, People’s Republic of China, Tel +86 13207801809, Email [email protected]
Objective: To compare pregnancy outcomes between advanced maternal age (AMA, ≥ 35 years) and younger maternal age (YMA, 20– 34 years) nulliparous women with IVF-conceived dichorionic-diamniotic (DCDA) twin pregnancies.
Methods: We conducted a retrospective analysis on 141 nulliparous women undergoing cesarean delivery at The Second Nanning People’s Hospital (2020– 2024). Propensity score matching (PSM, 1:1, caliper width=0.02) was conducted to balanced BMI, gravidity, and menarche age between AMA (n=47) and YMA (n=94) groups. Evaluated parameters included preterm birth (PTB), discordant twin growth, intraoperative blood loss, placental complications (previa/abruption), metabolic disorders (GDM, HDP, ICP), and postpartum hemorrhage (PPH).
Results: AMA women had significantly higher rates of discordant twin growth (P< 0.05) and greater intraoperative blood loss versus YMA. No significant intergroup differences were observed in PTB, low birth weight, placental complications, GDM, HDP, ICP, or PPH.
Conclusion: AMA nulliparous women with IVF DCDA twins face elevated risks of fetal growth discordance and surgical blood loss. However, risks of other maternal-fetal complications align with younger counterparts. Targeted prenatal surveillance for twin growth trajectories and intraoperative hemorrhage management may optimize outcomes in AMA populations. These findings support tailored clinical protocols for this high-risk demographic.
Keywords: in vitro fertilization (IVF), dichorionic-diamniotic twin pregnancy (DCDA), advanced maternal age, nulliparous women
Introduction
In recent years, the number of nulliparous women at advanced maternal age in China has steadily increased, driven by economic development and changing marital attitudes. This demographic shift, combined with the widespread use of Assisted Reproductive Technology (ART), has consequently led to a surge in twin pregnancies in nulliparous women at advanced maternal age. Advanced maternal age is defined as being 35 years or older at the time of the first delivery.1 Globally, the proportion of women delaying childbirth until their late 30s or early 40s has significantly risen.2 The literature indicates that the incidence of twin (or multiple) pregnancies resulting from assisted reproductive technology can reach as high as 21.8%.3 Twin pregnancies are associated with a higher risk of complications compared to singleton pregnancies, including hypertensive disorders, diabetes, postpartum hemorrhage, and preterm birth.4 A meta-analysis has demonstrated that, although perinatal outcomes are comparable between women of advanced maternal age and younger women with twin pregnancies, the advanced maternal age group exhibits a significantly higher incidence of gestational diabetes and cesarean deliveries.5 A study conducted in South Korea found that twin pregnancies in older mothers are associated with an increased risk of gestational diabetes, placenta previa, and higher neonatal birth weight; however, other outcomes did not show a significant correlation with maternal age.6 Additionally, a domestic study reported that twin pregnancies in women of advanced maternal age are associated with higher risks of preeclampsia, gestational diabetes mellitus (GDM), postpartum hemorrhage (PPH), and preterm birth (PTB), although the risk of adverse neonatal outcomes did not increase significantly.7 In IVF twin pregnancies, the mothers are usually older, and the proportion of nulliparous women is higher.8 Some literature studies have shown comparisons of outcomes between different age groups (such as the increased risks in advanced maternal age vs younger maternal age).9,10 Despite these findings, there remains a notable lack of research specifically focusing on the outcomes of DCDA twins pregnancies in AMA nulliparous women undergoing IVF. This gap is particularly concerning given the unique risks associated with this subgroup. This study aims to analyze the impact of advanced maternal age on the outcomes of DCDA twins achieved through IVF in nulliparous women. By focusing specifically on DCDA twins in this demographic, we aim to fill a critical gap in the literature, as existing studies predominantly focus on singleton pregnancies or mixed chorionicity twins. By providing clinical evidence, we hope to inform the perinatal management of advanced maternal age nulliparous women and potentially contribute to the development of targeted clinical guidelines for this population. Nulliparous women may have different baseline characteristics compared to multiparous women, such as no prior birth history, which reduces confounding factors. For instance, previous studies have used nulliparous women cohorts to isolate the effects of age or other variables on the outcomes of twin pregnancies.9,11 By providing clinical evidence, we hope to inform the perinatal management of advanced maternal age nulliparous women. By comparing outcomes between women of advanced maternal age and younger maternal age nulliparous women, we seek to offer more scientific guidance for clinical practice. We hypothesized that AMA nulliparous women with DCDA twins would exhibit higher rates of growth discordance and obstetric hemorrhage to younger counterparts, independent of confounders addressed through propensity matching. However, existing studies predominantly focus on singleton pregnancies or mixed chorionicity twins. The specific risks associated with DCDA twins in AMA nulliparous women undergoing IVF remain underexplored, particularly regarding growth discordance mechanisms.
Patients and Methods
General Information
Our study was conducted in a city with 13 tertiary hospitals. The center reports an annual delivery volume of approximately 3000 cases, which includes a diverse population of young primiparous women, women of advanced maternal age (AMA), and women with multiple gestation. To ensure the validity of our findings, we established strict inclusion criteria for patient enrollment. These criteria were designed to minimize selection bias and to focus on specific patient populations relevant to our research objectives. Only patients who met these criteria were included in the study, allowing us to draw meaningful conclusions from our data.
This study included nulliparous women who underwent cesarean section for IVF dichorionic-diamniotic twin pregnancies at the Second Nanning People’s Hospital from January 2020 to August 2024. All data were extracted from standardized electronic medical records, including prenatal visit logs, laboratory reports, and surgical notes. The advanced maternal age group consisted of 47 cases, while the younger maternal age group comprised 94 cases. Flowchart of Study Population Selection (Figure 1).
 |
Figure 1 Flowchart of Study Population Selection. |
Inclusion and Exclusion Criteria
Inclusion criteria: IVF; DCDA; nulliparous women; timely prenatal check-ups (defined as attending ≥8 scheduled prenatal visits with complete documentation of fetal biometry and Doppler studies, excluding preterm births). Exclusion criteria: Other types of twin pregnancies; congenital fetal abnormalities; stillbirth of one twin; heart disease; severe anemia; immune-related diseases; Suboptimally Controlled Diabetes; Suboptimally Controlled Hyperthyroidism; Suboptimally Controlled Chronic Hypertension; incomplete clinical data.
Method
Methods and Observational Indicators
Participants were divided into two groups: advanced maternal age group (≥35 years) and younger maternal age group (20–34 years). We compared BMI, pregnancies, age at menarche, gestational age at delivery, PTB, PROM, LBW, discordant twin growth, intraoperative blood loss, hemoglobin levels in early and late pregnancy (early pregnancy defined as before 13 weeks, late pregnancy as the most recent result before delivery), placenta previa, placental abruption, HDP, GDM, ICP, and PPH.
This study has received approval from the Ethics Committee of the Second Nanning People’s Hospital, which granted a waiver for informed consent from participants because the research involves retrospective analysis of anonymized clinical data and blood routine results.
This study has received approval from the Ethics Committee of the Second Nanning People’s Hospital, granting a waiver for informed consent from participants because the research involves retrospective analysis of anonymized clinical data and blood routine results, with no direct contact or intervention with the patients. The study is observational in nature and aims to analyze the clinical data and blood routine results of women with advanced and younger maternal age IVF Dichorionic-Diamniotic twin pregnancies. There are no commercial interests involved, and the study poses no harm to participants.
Data analysis will be conducted using coded information, ensuring that no personal details (such as contact information, addresses, etc.) of the participants are collected. All samples and data will be de-identified to fully protect the privacy rights of the participants. Furthermore, the data used in this study will be strictly for research purposes and will not be used for any other purposes. The publication of research results will not disclose any personal identities of the participants.
This study will comply with relevant laws and regulations, including the Declaration of Helsinki. The researchers collectively assume responsibility for maintaining confidentiality, ensuring the security and privacy of participant information throughout the study.
Diagnostic Criteria
Discordant twin growth:Estimate the weight of one twin to be less than the third percentile for gestational age; or one twin meets at least two of the following three conditions: (1) estimated weight of one twin < 10th percentile; (2) difference in estimated weight between the two fetuses ≥ 25%; (3) pulsatility index of the smaller fetus’s umbilical artery > 95th percentile.12
Additionally, clarity regarding the assessment of “discordant twin growth” is warranted; it was assessed based on birth weight.
Statistical Analysis
Statistical analysis was performed using SPSS 29.0 software (IBM Corp., Armonk, NY, USA). Propensity score matching (PSM) was conducted based on maternal BMI, pregnancies, age at menarche.The nearest neighbor matching method was applied with a 1:1 ratio and a matching tolerance 0.02.Prior to PSM, there were 47 cases in the advanced maternal age group and 94 in the younger maternal age group. Following PSM, a total of 84 cases were included in the analysis, with 42 in the advanced age group and 42 in the younger maternal age group. Data conforming to a normal distribution or approximately normal distribution were expressed as mean ± standard deviation ( ), and comparisons between groups were made using t-tests, with P < 0.05 indicating statistical significance. Count data were expressed as rates (%), analyzed using the χ2 test, and Fisher’s exact test was applied when expected counts were <5, with P < 0.05 indicating statistical significance.
), and comparisons between groups were made using t-tests, with P < 0.05 indicating statistical significance. Count data were expressed as rates (%), analyzed using the χ2 test, and Fisher’s exact test was applied when expected counts were <5, with P < 0.05 indicating statistical significance.
Results
Comparison of General Information
Prior to PSM, the advanced maternal age group had significantly higher age and pregnancies compared to the younger maternal age group (P<0.05), while BMI and age at menarche showed no significant differences (P>0.05). Following PSM, the advanced maternal age group continued to have a significantly higher mean age compared to the younger maternal age group (P<0.05), while BMI, pregnancies, and age at menarche showed no significant differences (P>0.05) (Table 1).
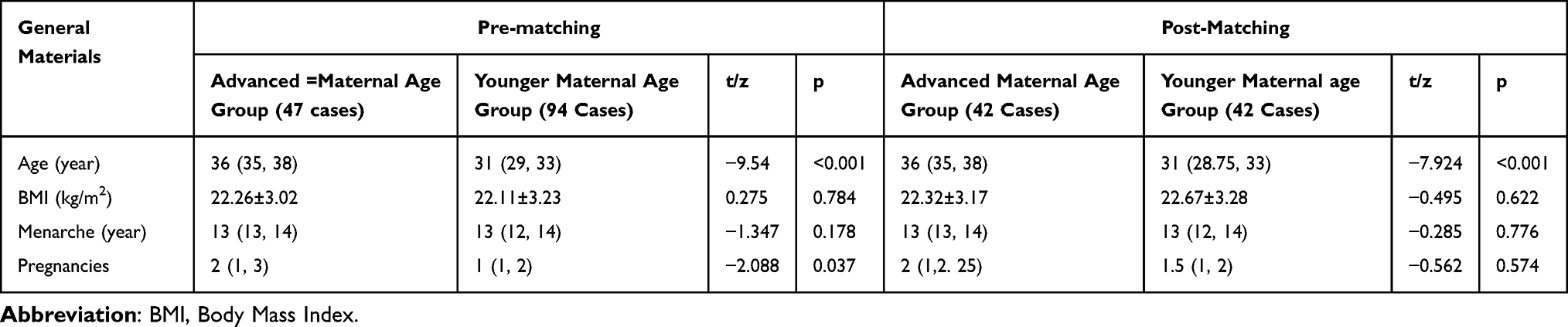 |
Table 1 Comparison of General Data Between the Two Groups of Pregnant Women Before and After Matching ( |

Comparison of Hemoglobin Levels and Pregnancy Complications
Prior to PSM, the incidence of placental abruption was higher in the advanced maternal age group compared to the younger maternal age group (P<0.05). No significant differences in hemoglobin levels during early and late pregnancy, as well as in GDM, HDP, ICP, and placenta previa (P>0.05). Following PSM, no significant differences were observed in hemoglobin levels, GDM, HDP, ICP, placenta previa, and placental abruption (P>0.05) (Table 2).
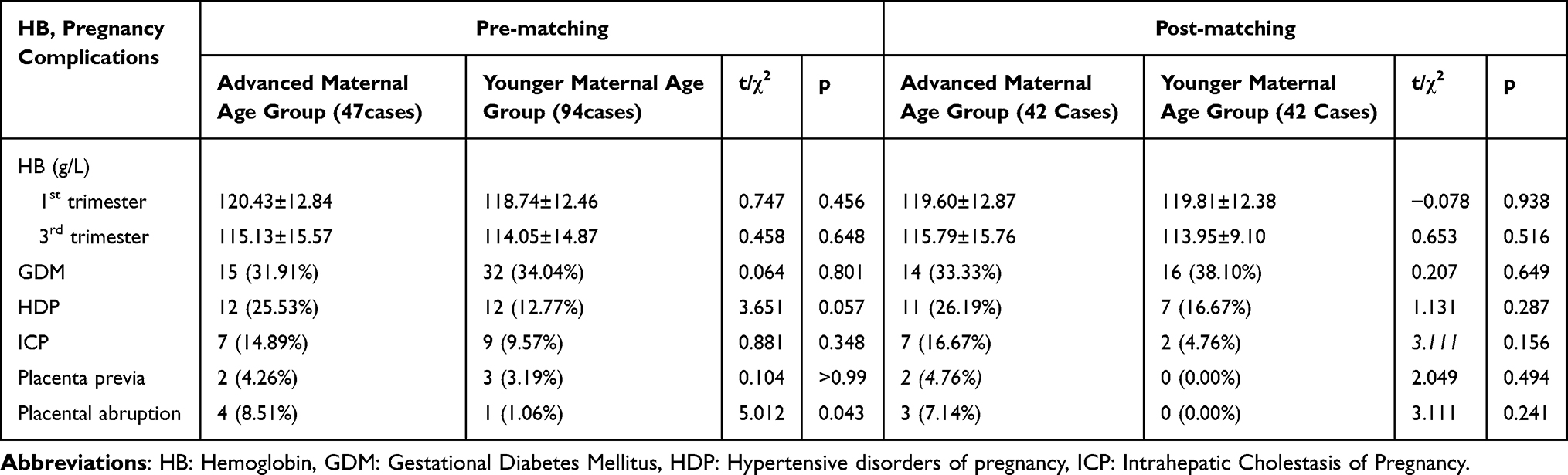 |
Table 2 Comparison of HB and Pregnancy Complications Between the Two Groups of Pregnant Women Before and After Matching ( |

Comparison of Pregnancy Outcomes
No cases of postpartum hemorrhage occurred in either group.Prior to PSM, discordant twin growth was significantly higher in the advanced maternal age group compared to the younger maternal age group (P<0.05); however, differences in fetal growth restriction, LBW, PTB, PROM, and intraoperative blood loss were not statistically significant (P>0.05). Following PSM, discordant twin growth and intraoperative blood loss were significantly higher in the advanced maternal age group compared to the younger maternal age group (P<0.05), while differences in fetal growth restriction, LBW, PTB, and PROM were not statistically significant (P>0.05) (Table 3).
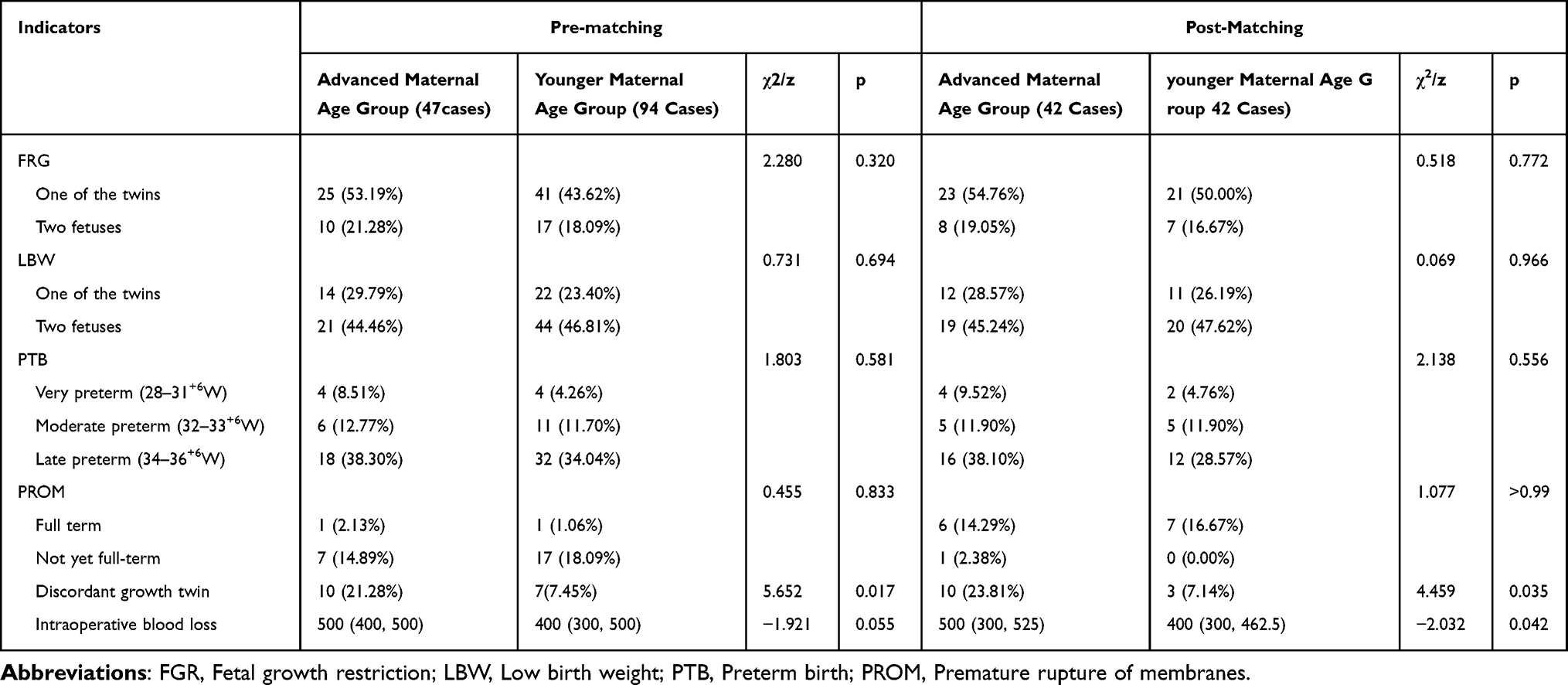 |
Table 3 Comparison of Pregnancy Outcomes Between the Two Groups of Pregnant Women Before and After Matching M(P25,P75), (n)% |
Discussion
The results indicate that advanced maternal age nulliparous women face significantly higher rates of discordant twin growth and intraoperative blood loss compared to younger maternal age primiparas, suggesting that they may encounter greater risks of fetal growth discordance and bleeding in IVF twin pregnancies. However, no significant differences were observed between the two groups regarding other pregnancy outcomes such as PTB, LBW, placenta previa, placental abruption, GDM, HDP, and ICP. This finding emphasizes the importance of individualized and close monitoring for nulliparous women at advanced maternal age to address their unique risk factors and ensure favorable outcomes in IVF-conceived dichorionic-diamniotic twin pregnancies.
Principal Findings of This Study
Comparison of Pregnancy Complications
We found no significant differences between the two groups in terms of hemoglobin (HB) levels during early and late pregnancy, preterm birth, low birth weight, placenta previa, placental abruption, gestational diabetes mellitus (GDM), hypertensive disorders of pregnancy (HDP), and intrahepatic cholestasis of pregnancy (ICP) (P>0.05). The null finding may reflect rigorous glycemic/blood pressure control in AMA women under close prenatal surveillance. The overall prevalence of placenta previa was (4–5)/1000 deliveries, although there are regional variations globally, and the reasons for these discrepancies remain unclear.13 Some studies indicate that advanced maternal age is a risk factor for developing placenta previa.14 One study showed that the prevalence of placenta previa among twin pregnancies is 40% higher than that among singleton pregnancies (3.9/1000 vs 2.8/1000).15 Our study did not find a higher incidence of placenta previa in the high-age group, which may be attributed to the limitations of our sample size; future research could consider increasing the sample size in order to further investigate this. Regarding placental abruption, assisted reproductive technology (ART) may increase its incidence.16,17 A retrospective study in China found that the risk of placental abruption increases with maternal age.18 In our study, the initial data showed a tendency for a higher incidence of placental abruption in the high-age group compared to the younger maternal age group; however, this difference became insignificant after propensity score matching (PSM), so the differences between the two groups were not significant. This may be due to the reduced sample size after PSM, which did not yield positive results. Nonetheless, we should remain vigilant about the incidence of placental abruption in the high-age population and enhance monitoring during pregnancy. Although BMI significantly impacts pregnancy outcomes among women aged 30–38 years, its effect is minimal in younger or older women.19 This aligns with our findings, suggesting that maternal age may have a limited effect on certain pregnancy outcomes. Regardless of the conception method, twin pregnancies increase morbidity and mortality for both mothers and infants; therefore, couples should be counseled about the iatrogenic risks associated with double embryo transfer. However, couples expecting twins can be informed that ART does not significantly worsen pregnancy outcomes compared to naturally conceived twin pregnancies.20 Our study further supports this notion, as we found that advanced maternal age nulliparous women undergoing ART had similar pregnancy outcomes to younger maternal age nulliparous women. Compared to younger women, older women had significantly higher incidences of gestational diabetes, cesarean delivery, and fetal growth discordance in twin pregnancies, while the incidence of preeclampsia was not influenced by maternal age.21 The advanced maternal age nulliparous women in our study also exhibited higher fetal growth discordance, but no significant differences were observed regarding GDM, HDP, or other complications. The incidence of cesarean delivery and hypertensive disorders was significantly higher in women with twin pregnancies aged over 35, increasing with maternal age, yet the incidence of neonatal complications did not rise.22 Literature suggests that when the technique for vaginal delivery in twin pregnancies is not well mastered based on training and experience, cesarean delivery is a more appropriate choice.23 We opted for cesarean delivery due to the value of IVF-conceived fetuses, as mothers and their families preferred this method.
Comparison of Pregnancy Outcomes
The results show that advanced maternal age nulliparous women exhibited significantly higher rates of discordant twin growth and intraoperative blood loss compared to younger maternal age nulliparous women (P<0.05). However, differences in fetal growth restriction, LBW, PTB, and PROM were not statistically significant (P>0.05). This suggests that maternal age may have a limited influence on certain pregnancy outcomes. Our findings suggest that, with appropriate monitoring during pregnancy, nulliparous women at advanced maternal age can achieve outcomes comparable to those of their younger counterparts. It is crucial to increase monitoring of fetal growth during pregnancy. A prospective cohort study reported that if singleton fetal growth standards are used, nearly 40% of dichorionic twins would be classified as small for gestational age near term.24 Literature indicates that singleton fetal growth curves are the best indicators for adverse outcomes in twin pregnancies and should be used for assessing fetal growth abnormalities in twin gestations.25 However, proponents of twin-specific growth curves argue that using singleton growth standards may lead to overdiagnosis of growth abnormalities, resulting in unnecessary maternal anxiety and prenatal examinations, potentially leading to preterm delivery without improving neonatal outcomes.26,27 Therefore, it is essential to select appropriate fetal growth assessment standards in twin pregnancies to avoid excessive intervention and unnecessary anxiety. Some literature suggests that many growth abnormalities in twins can be detected between 20–24 weeks, and if no abnormalities are found during this period, repeated ultrasound examinations may not be necessary.28 However, some authorities recommend routine ultrasound examinations every 2–4 weeks,29 which is also our practice. The complication rates and mortality of twin pregnancies are higher than those of singleton pregnancies, primarily due to fetal growth restriction and preterm birth, making fetal growth assessment particularly important.30–32 Our study also found that advanced maternal age nulliparas are more likely to experience fetal growth discordance in twin pregnancies. Thus, close monitoring and individualized management are critical for these high-risk pregnancies. Emerging evidence suggests that the association between mild discordant twin growth and abnormal placental pathology primarily manifests through its impact on small-for-gestational-age (SGA) status in the smaller twin.33 The increased intraoperative blood loss observed in the AMA group compared to YMA counterparts may correlate with discordant twin growth patterns. Existing literature demonstrates that growth discordance, particularly when complicated by fetal growth restriction (FGR), is associated with elevated postpartum hemorrhage risk in twin pregnancies undergoing cesarean delivery, with this association being more pronounced in dichorionic twins.34 Advanced maternal age and nulliparity can both lead to maternal vascular malperfusion (MVM), and the level of discordant twin growth in twins is significantly associated with MVM lesions.33 Deterioration of utero-placental perfusion is highly correlated with the differences in perfusion, which is closely related to discordant twin growth twins.35 While our data did not distinguish between fresh or frozen embryo transfers – a potential confounding factor in pregnancy outcomes – current evidence suggests no significant differences in perinatal outcomes between these transfer modalities.36
Conclusions
Clinical Implications of the Study
In conclusion, women of AMA who undergo IVF experience a higher risk of certain complications in DCDA twins, such as discordant twin growth and intraoperative bleeding. However, when provided with adequate prenatal care, their pregnancy outcomes are comparable to those of younger primiparous women. This finding offers reassurance to older women considering IVF for twin pregnancies, suggesting that with appropriate medical interventions and careful monitoring—including enhanced fetal growth surveillance, such as serial ultrasounds at 2–4-week intervals or ideally biweekly monitoring schedules—the potential risks can be effectively managed.
Limitations of the Study
As a retrospective single-center study, our findings are constrained by a limited sample size (post-PSM n=84), which may be underpowered to detect differences in rare outcomes like placental abruption (observed in 5 cases, pre-PSM) and placenta previa. This limitation inherently restricts the generalizability of our findings. Furthermore, while we accounted for matching variables such as BMI, menarche age, and gravidity, we did not comprehensively address potential confounding factors, including socioeconomic status, lifestyle, and genetic background. Unmeasured confounders, such as socioeconomic status and embryo quality (eg, blastocyst vs cleavage-stage transfer), could influence outcomes but were unavailable for analysis.
Prospects
To enhance the reliability and generalizability of our results, future research should adopt a multicenter, large-sample, prospective design. Moreover, it is essential to investigate specific risk factors and develop intervention strategies tailored specifically for primiparous women of advanced maternal age undergoing IVF for twin pregnancies, with the aim of optimizing prenatal management protocols. By integrating advanced monitoring technologies and personalized medical interventions, there is significant potential to substantially improve pregnancy outcomes.
In addition to the aforementioned considerations, it is crucial for future research to systematically evaluate the impact of socioeconomic factors and the type of embryo transfer (fresh vs frozen) on pregnancy outcomes. By including these variables in the study design, we can better control for potential confounding effects and improve the robustness of our findings. This comprehensive approach will not only enhance the reliability of our results but also provide deeper insights into the multifaceted nature of factors influencing twin pregnancies in primiparous women of advanced maternal age undergoing IVF.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This medical research study is a retrospective case study. Ethics review and approval in this study is required according to the Declaration of Helsinki (World Medical Association Inc, 2009), and Ethics approval for the study was obtained from the Ethics Committee of the Second Nanning People’s Hospital guidelines and national regulations.Ethics approval for the study was obtained from the Ethics Committee of the Second Nanning People’s Hospital [Y2024315].
Acknowledgments
Meiping He and Wenqian Jian are co-first authors for this study. We acknowledge the clinical support provided by the obstetric team at The Second Nanning People’s Hospital during data collection. The study received no external funding. All researchers maintained independence in study design, data analysis, and interpretation. This paper has been uploaded to ResearchSquare as a preprint: https://www.researchsquare.com/article/rs-5286618/v1‘.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There are no funding sources to be declared.
Disclosure
The authors have no conflict of interests to declare in this work.
References
1. Iams JD. Prevention of preterm parturition. N Engl J Med. 2014;370(19):1861. PMID: 24806178. doi:10.1056/NEJMc1402822
2. Seshadri S, Morris G, Serhal P, Saab W. Assisted conception in women of advanced maternal age. Best Pract Res Clin Obstet Gynaecol. 2021;70:10–20. Epub 2020 Aug 7. PMID: 32921559. doi:10.1016/j.bpobgyn.2020.06.012
3. Qin JB, Wang H, Sheng X, Xie Q, Gao S. Assisted reproductive technology and risk of adverse obstetric outcomes in dichorionic twin pregnancies: a systematic review and meta-analysis. Fertil Steril. 2016;105(5):1180–1192. Epub 2016 Jan 19. PMID: 26801066. doi:10.1016/j.fertnstert.2015.12.131
4. Yang M, Xiao L, Wang J. The relationship between maternal age and adverse pregnancy outcomes in twin pregnancies. Chin J Contemp Pediatr. 2020;22(03):238–244.
5. Zipori Y, Linder R, Khatib N, Weiner Z, Barzilay E. Advanced maternal age and perinatal outcome in twin pregnancies: a meta-analysis. J Matern Fetal Neonatal Med. 2020;33(18):3193–3199. Epub 2019 Jan 29. PMID: 30696313. doi:10.1080/14767058.2019.1570112
6. Lee YJ, Kim MN, Kim YM, et al. Perinatal outcome of twin pregnancies according to maternal age. Obstet Gynecol Sci. 2019;62(2):93–102. Epub 2019 Feb 25. PMID: 30918877; PMCID: PMC6422846. doi:10.5468/ogs.2019.62.2.93
7. Wang J, Ma X, Nan Y, et al. Analysis of pregnancy outcomes in advanced maternal age women with twin pregnancies. J Armed Forces Med Univ. 2018;39(11):968–970.
8. Barda G, Gluck O, Mizrachi Y, Bar J. A comparison of maternal and perinatal outcome between in vitro fertilization and spontaneous dichorionic-diamniotic twin pregnancies. J Matern Fetal Neonatal Med. 2017;30(24):2974–2977. Epub 2017 Jan 12. PMID: 27936998. doi:10.1080/14767058.2016.1270934
9. Pinzauti S, Ferrata C, Vannuccini S, et al. Twin pregnancies after assisted reproductive technologies: the role of maternal age on pregnancy outcome. Eur J Obstet Gynecol Reprod Biol. 2016;206:198–203. Epub 2016 Sep 21. PMID: 27723551. doi:10.1016/j.ejogrb.2016.09.019
10. Wang Y, Shi H, Chen L, et al. Absolute risk of adverse obstetric outcomes among twin pregnancies after in vitro fertilization by maternal age. JAMA Network Open. 2021;4(9):e2123634. PMID: 34505887; PMCID: PMC8433605. doi:10.1001/jamanetworkopen.2021.23634
11. Simões T, Pereira I, Gomes L, Brás S, Nogueira I, Queirós A. Higher risk of preterm twin delivery among shorter nulliparous women. J Gynecol Obstet Hum Reprod. 2024;53(1):102694. Epub 2023 Nov 21. PMID: 37992965.]. doi:10.1016/j.jogoh.2023.102694
12. Chinese Society of Perinatal Medicine, Fetal Medicine Subgroup; Chinese Society of Obstetrics and Gynecology, Obstetrics Subgroup. Clinical management guidelines for twin pregnancy (2020 Update). J Prenatal Diagn China. 2020;23(8):505–516. doi:10.3760/cma.j.cn113903-20200812-00793
13. Cresswell JA, Ronsmans C, Calvert C, Filippi V. Prevalence of placenta praevia by world region: a systematic review and meta-analysis. Trop Med Int Health. 2013;18(6):712–724. Epub 2013 Apr 1. PMID: 23551357. doi:10.1111/tmi.12100
14. Jenabi E, Salimi Z, Bashirian S, Khazaei S, Ayubi E. The risk factors associated with placenta previa: an umbrella review. Placenta. 2022;117:21–27. Epub 2021 Oct 20. PMID: 34768164. doi:10.1016/j.placenta.2021.10.009
15. Ananth CV, Demissie K, Smulian JC, Vintzileos AM. Placenta previa in singleton and twin births in the United States, 1989 through 1998: a comparison of risk factor profiles and associated conditions. Am J Obstet Gynecol. 2003;188(1):275–281. PMID: 12548229. doi:10.1067/mob.2003.10
16. Wu P, Sharma GV, Mehta LS, et al. In-hospital complications in pregnancies conceived by assisted reproductive technology. J Am Heart Assoc. 2022;11(5):e022658. Epub 2022 Feb 22. PMID: 35191320; PMCID: PMC9075081. doi:10.1161/JAHA.121.022658
17. Zhang JT, Lee R, Sauer MV, Ananth CV. Risks of placental abruption and preterm delivery in patients undergoing assisted reproduction. JAMA Network Open. 2024;7(7):e2420970. PMID: 38985469; PMCID: PMC11238021. doi:10.1001/jamanetworkopen.2024.20970
18. Li J, Yan J, Jiang W. The role of maternal age on adverse pregnancy outcomes among primiparous women with singleton birth: a retrospective cohort study in urban areas of China. J Matern Fetal Neonatal Med. 2023;36(2):2250894. PMID: 37635092. doi:10.1080/14767058.2023.2250894
19. Liu D, Li L, Sun N, et al. Effects of body mass index on IVF outcomes in different age groups. BMC Women's Health. 2023;23(1):416. PMID: 37553621; PMCID: PMC10410781. doi:10.1186/s12905-023-02540-8
20. Geisler ME, O’Mahony A, Meaney S, Waterstone JJ, O’Donoghue K. Obstetric and perinatal outcomes of twin pregnancies conceived following IVF/ICSI treatment compared with spontaneously conceived twin pregnancies. Eur J Obstet Gynecol Reprod Biol. 2014;181:78–83. Epub 2014 Aug 1. PMID: 25129152. doi:10.1016/j.ejogrb.2014.07.033
21. Toussia-Cohen S, Mohr-Sasson A, Tsur A, et al. Pregnancy and neonatal outcomes of twin pregnancies - the role of maternal age. J Perinat Med. 2021;49(5):559–565. PMID: 33596607. doi:10.1515/jpm-2020-0386
22. Gluck O, Mizrachi Y, Bar J, Barda G. The impact of advanced maternal age on the outcome of twin pregnancies. Arch Gynecol Obstet. 2018;297(4):891–895. Epub 2018 Jan 16. PMID: 29340788. doi:10.1007/s00404-018-4656-1
23. Easter SR, Taouk L, Schulkin J, Robinson JN. Twin vaginal delivery: innovate or abdicate. Am J Obstet Gynecol. 2017;216(5):484–488.e4. Epub 2017 Feb 7. PMID: 28188771. doi:10.1016/j.ajog.2017.01.041
24. Grantz KL, Grewal J, Albert PS, et al. Dichorionic twin trajectories: the NICHD fetal growth studies. Am J Obstet Gynecol. 2016;215(2):221.e1–221.e16. Epub 2016 Apr 30. PMID: 27143399; PMCID: PMC4967402. doi:10.1016/j.ajog.2016.04.044
25. Gleason JL, Yeung E, Sundaram R, et al. Developmental outcomes in small-for-gestational age twins using a singleton vs twin birthweight reference. Am J Obstet Gynecol MFM. 2021;3(6):100465. Epub 2021 Aug 18. PMID: 34416423; PMCID: PMC8630670. doi:10.1016/j.ajogmf.2021.100465
26. Shea SK, Likins BJ, Boan AD, Newman RB, Finneran MM. Dichorionic twin-specific vs singleton growth references for diagnosis of fetal growth restriction. Am J Obstet Gynecol. 2021;224(6):603.e1–603.e9. Epub 2021 Mar 23. PMID: 33771495. doi:10.1016/j.ajog.2021.03.022
27. Hiersch L, Barrett J, Fox NS, Rebarber A, Kingdom J, Melamed N. Should twin-specific growth charts be used to assess fetal growth in twin pregnancies? Am J Obstet Gynecol. 2022;227(1):10–28. Epub 2022 Jan 31. PMID: 35114185. doi:10.1016/j.ajog.2022.01.027
28. Grobman WA, Parilla BV. Positive predictive value of suspected growth aberration in twin gestations. Am J Obstet Gynecol. 1999;181(5 Pt 1):1139–1141. PMID: 10561633. doi:10.1016/s0002-9378(99)70096-7
29. Khalil A, Rodgers M, Baschat A, et al. ISUOG Practice Guidelines: role of ultrasound in twin pregnancy. Ultrasound Obstet Gynecol. 2016;47(2):247–263. Erratum in: Ultrasound Obstet Gynecol. 2018 Jul;52(1):140. doi: 10.1002/uog.19087. PMID: 26577371. doi:10.1002/uog.15821
30. Inklaar MJ, van Klink JM, Stolk TT, van Zwet EW, Oepkes D, Lopriore E. Cerebral injury in monochorionic twins with selective intrauterine growth restriction: a systematic review. Prenat Diagn. 2014;34(3):205–213. Epub 2014 Jan 13. PMID: 24338685. doi:10.1002/pd.4298
31. Yinon Y, Mazkereth R, Rosentzweig N, Jarus-Hakak A, Schiff E, Simchen MJ. Growth restriction as a determinant of outcome in preterm discordant twins. Obstet Gynecol. 2005;105(1):80–84. PMID: 15625146. doi:10.1097/01.AOG.0000146634.28459.e8
32. Blickstein I, Keith LG. Neonatal mortality rates among growth-discordant twins, classified according to the birth weight of the smaller twin. Am J Obstet Gynecol. 2004;190(1):170–174. PMID: 14749655. doi:10.1016/j.ajog.2003.07.025
33. Ashwal E, Hiersch L, Berger H, et al. Pathologic basis for the definition of discordant growth in dichorionic twins. Fetal Diagn Ther. 2021;48(4):279–287. Epub 2021 Mar 29. PMID: 33780952. doi:10.1159/000514328
34. Cao X, Luo Y, Zhou S, et al. Twin growth discordance and risk of postpartum hemorrhage: a retrospective cohort study. Front Med Lausanne. 2022;9:876411. PMID: 35692549; PMCID: PMC9174790. doi:10.3389/fmed.2022.876411
35. Zhang L, Liu X, Li J, et al. Maternal utero-placental perfusion discordance in monochorionic-diamniotic twin pregnancies with selective growth restriction assessed by three-dimensional power Doppler ultrasound. Med Sci Monit. 2020;26:e919247. PMID: 31971163; PMCID: PMC6996265. doi:10.12659/MSM.919247
36. Fattahpour SF, Hakimi P, Tabatabaei F, et al. Comparison of live birth rate and fetal outcomes between fresh embryo and frozen-thawed embryo transfers: a prospective study. BMC Pregnancy Childbirth. 2025;25(1):122. PMID: 39910459; PMCID: PMC11800545. doi:10.1186/s12884-025-07247-2
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.