Back to Journals » Journal of Asthma and Allergy » Volume 15
Impulse Oscillometry System for the Diagnosis of Wheezing Episode in Children in Office Practice
Authors Kulkarni S ![]() , Kurane A, Sakate D
, Kurane A, Sakate D
Received 21 October 2021
Accepted for publication 21 February 2022
Published 16 March 2022 Volume 2022:15 Pages 353—362
DOI https://doi.org/10.2147/JAA.S344643
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Suhas Kulkarni,1 Anil Kurane,1 Deepak Sakate2
1Department of Pediatrics, D.Y. Patil Medical College, Kolhapur, Maharashtra, India; 2Department of Statistics and Applied Mathematics, Central University of Tamil Nadu, Thiruvarur, Tamil Nadu, India
Correspondence: Suhas Kulkarni, D.Y. Patil Medical College, Kolhapur, Maharashtra, India, Tel +91 231 2601235, Fax +91 231260138, Email [email protected]
Background and Objective: Objectively differentiating between wheezing episodes and other respiratory disorders will be helpful in treatment in office practice. The impulse oscillometry system has been useful in assessing airway resistance in children 3– 6 years old. As the reference values are different in geographical regions the use of the impulse oscillometry is still limited. Comparison between the percent change in IOS parameters as compared to reference standards and changes in actual IOS parameters was done to diagnose wheezing episodes.
Methodology: Three to six years old children with a history of fever, cough, cold, and/or breathlessness with noisy breathing and who were not on any regular medications, whose parents gave consent were recruited in the study. The children underwent an impulse oscillometry system examination as per the guidelines. The test was repeated after they were given nebulization by salbutamol (2.5 mg) (before COVID 19 pandemic). Final diagnosis was done by following patients for 7 days.
Results: About 106 children were recruited in the study. Five children could not perform the IOS test. Eighteen children did not complete the follow-up. Hence, 83 children were analyzed. There were 47 males and 36 female patients. The change in actual values of AX, R5, and X20 showed statistically significant difference in wheezing episode group (p-value< 0.001). The percentage change as compared to predicted values of R5 and X20 also showed a statistically significant difference in the wheezing episode group and the others group (p-value< 0.001).
Conclusion: The change in actual values of AX, R5, X20, and resonant frequency may help to differentiate wheezing episode from other respiratory diseases.
Keywords: impulse oscillometry system, respiratory disorders, wheezing episode
Introduction
Wheezing in infants and children is a common problem presented to pediatric primary care offices. Approximately 25–30% of infants will have at least one episode of wheezing.1 By 3 years of age, an episode of wheezing will have occurred in 30% of children and by 6 years of age, almost half of children will have had at least one episode of wheezing.2
Wheezing occurs during the prolonged expiratory phase by the rapid passage of air through airways that are narrowed to the point of closure. Children wheeze more often than adults because of physical differences. In infants and young children bronchi are small, resulting in higher peripheral airway resistance. As a result, diseases that affect the small airways have a proportionately greater impact on total airway resistance in these patients. Infants also have less elastic tissue recoil and fewer collateral airways, resulting in easier obstruction and atelectasis. The rib cage, trachea, and bronchi are also more compliant in infants and young children, and the diaphragm inserts horizontally instead of obliquely. All of these factors increase the likelihood of wheezing and respiratory distress in infants and chidren.3
It is important for clinicians and epidemiologists to recognize that there are distinct types of audible respiratory noises in early life with characteristic acoustic properties.4 The assessment of airway obstruction in very young children is difficult because of the lack of objective lung function measurements and definitive biomarkers.5 Thus, an objective tool for recognition of wheezing in the outpatient department is of clinical value.6,7
Intra-observer variation is modest, but inter-observer variation is large for most clinical examination findings in children with dyspnea. The measurement error induced by this variation is too large to distinguish potentially clinically relevant changes in dyspnea after treatment in two-thirds of observations. The poor inter-observer reliability of clinical dyspnea assessment in children limits its usefulness in clinical practice and research, and highlights the need to use more objective measurements in these patients.8
Mild episodes of wheeze in preschoolers are characterized by enhanced airway inflammation, reversible airflow limitation, and asthma-related symptoms. FeNO values increase significantly during the first 48 hours and return to personal baseline within 10 days from the initiation of the episode. Longitudinal follow-up suggests that symptoms, inflammation, and lung function correlate well in this phenotype of asthma.9 Thus, there is a need for objective measurement of airway resistance to make a diagnosis of wheezing episode. The impulse oscillometry system (IOS) has been shown to be useful in assessing airway resistance in children 3–6 years old.10–12 The impulse oscillometry system parameters are; Zrs, Rrs, Xrs, AX, and resonant frequency. Zrs is total impedance. It is sum of all the forces opposing the pressure impulses (the oscillations)(Rrs plus Xrs). Rrs is the resistance of airways. Multiple frequency oscillations provide further information about resistance. R at 5 Hz is resistance at 5 Hz frequency. It measures total resistance of the airway. R at 20 Hz is resistance at 20 Hz frequency. It represents resistance of large airways. Xrs is reactance. It is the imaginary part of Zrs. It has two parts. I: Inertance, C: Capacitance. It can be seen as rebound resistance. It represents compliance. X5 reflects elastic recoil of peripheral airways. Resonant frequency is the frequency at which inertance and capacitance are equal. AX is integrated low frequency reactance between 5 Hz and resonant frequency.13 Impulse oscillometry has been shown to be useful in diagnosis of asthma and monitoring of lung function in children.14
As the reference values are different in geographical regions the use of the impulse oscillometry is still limited. To overcome this it was suggested by Konstantinou et al15 to use actual values, baseline values, and change in R at 5 Hz after bronchodilation of the patient to diagnose wheezing episode. Thus a study was designed to assess the usefulness of the impulse oscillometry system in office practice to diagnose wheezing episodes in 3–6 years old children. An attempt was made to compare the change in percentage of IOS parameters as compared to reference standard provided by the manufacturer and actual IOS parameters and change in IOS parameters after bronchodilation to diagnose wheezing episodes.
Methodology
Study Design
A prospective diagnostic cohort study was conducted in the pediatrics department of a tertiary care hospital from December 2016–December 2019. The study was approved by the Institutional Ethics Committee, D. Y. Patil Medical College, Kolhapur (2016/35/PA-F dated September 16, 2016). This study was conducted in accordance with the Declaration of Helsinki. Study population: D. Y. Patil medical college is situated in the city and caters to almost half the population of the district of Kolhapur, the population of which is around two million. The hospital provides free of cost services to the patients in an outpatient department and, as is centrally placed in the city, the population can be said to be representing the community. The children with fever, cough, cold, and/or breathlessness and noisy breathing who were not on any regular medications and whose parents gave consent for the study were recruited in the study. The purpose and details of methods used in the study were explained to all the parents. The weight was taken with minimal clothes on an electronic weighing machine and the height was taken with a stadiometer. Written informed consent was obtained prior to the study. A validated pre-designed data collection form was used to collect demographic and clinical information such as symptoms, duration, severity, and details of clinical examination (cough, cold, breathlessness, fever, heart rate, respiratory rate, examination of respiratory system, and oxygen saturation). The symptoms cough, cold, fever, and breathlessness were graded by the parents on scales of 1–4. Indicating nil as 1 and severe as 4. A diagnostic cohort study was done which may avoid spectrum bias. It also avoids misinformation bias.
Sample size calculation was done considering the prevalence of wheezing episodes (40%). The alpha of 0.05 and 95% confidence level were considered for the calculation. The following formula (Pourhoseingholi et al16 2013) was used to calculate the sample size,
 where
where  is the critical value of the Normal distribution at α (ie, for a confidence level of 95%, the critical value
is the critical value of the Normal distribution at α (ie, for a confidence level of 95%, the critical value  ),
),  is the expected prevalence and
is the expected prevalence and  is the precision. The calculated sample size was 92.
is the precision. The calculated sample size was 92.
A total of 110 children within 3–6 years of age with the above symptoms and the fulfilling inclusion criteria were evaluated in the study. Four children were excluded due to the presence of chronic respiratory disease, congenital heart disease, or having undergone ventilation after birth. In total, 106 children were recruited in the study. Five children did not perform the IOS diagnostic test and 18 children did not come for follow-up, hence they were excluded (Figure 1). These children underwent an impulse oscillometry system (IOS) test (Masterscreen Impulse Oscillometry system, Care fusion Germany 234 GmbH Hochberg). The impulse oscillometry was performed according to European respiratory Society (ERS)/American Thoracic Society (ATS) guidelines.17 Values of parameters R5, R20, X5, X20, AX, and resonant frequency were measured. The measurements were done again 20 minutes after nebulization with salbutamol (2.5 mg) (before the COVID pandemic with due precautions). The system was calibrated by a 3-L syringe provided by the manufacturer once daily. The system was also calibrated for temperature and atmospheric pressure. All the patients underwent IOS using nose clips and parents or guardians were advised to gently hold the sides of the patient’s face. The predicted values given by the manufacturer were used for calculation.18 The coherence function given by the machine was used to assess the acceptability of the recordings. The IOS data was not used for care of the patients. Final diagnosis was done by following the patient clinically for up to 7 days. Patients with an increased respiratory rate and the presence of rhonchi and those showing improvement after a bronchodilator were considered to have a clinically wheezing episode. The case definitions were made appropriately and the same test was done in all the patients to avoid misclassification bias. Work up bias was avoided by doing tests in all the subjects. The detection bias was avoided as the test was not used to diagnose cases and its management. It is accepted that clinical examination before the test can lead to some bias.
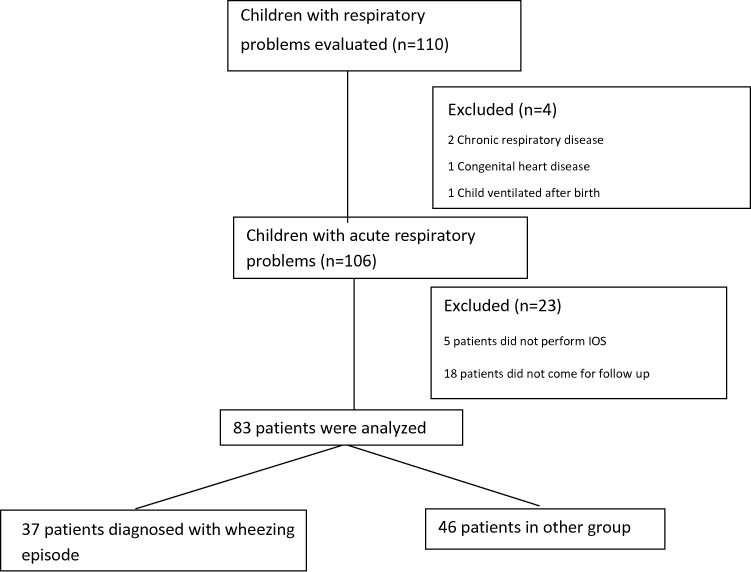 |
Figure 1 Study flowchart. |
Statistical Analysis
Collected data was analysed in R software (3.6.1). Difference of respiratory resistance between pre- and post-IOS test was assessed; mean and standard deviation were determined by paired t-test, and Wilcoxon-Sign-Rank test as some parameters happened to be non-normal. Odds ratio was used to assess the strength of IOS parameters in differentiating wheezing episode from other respiratory disorders. The ROC curves were plotted for each parameter. The specificity, sensitivity, positive predictive value, and negative predictive value were calculated for the parameters having ROC values of more than 0.70.
Results
Eighty-three patients were analyzed in the study. There were 47 males and 36 female patients. The weight was lower in the other group as compared to the wheezing group. The height was similar in both groups. The symptoms cough, cold, fever, and breathlessness, as told by parents, did not differentiate between the wheezing episode and other respiratory diseases. The respiratory rate and respiratory system examination could differentiate between the wheezing episode and other respiratory disorders (p-value less than <0.001). The hematological parameters did not show a significant difference between both the groups (Table 1).
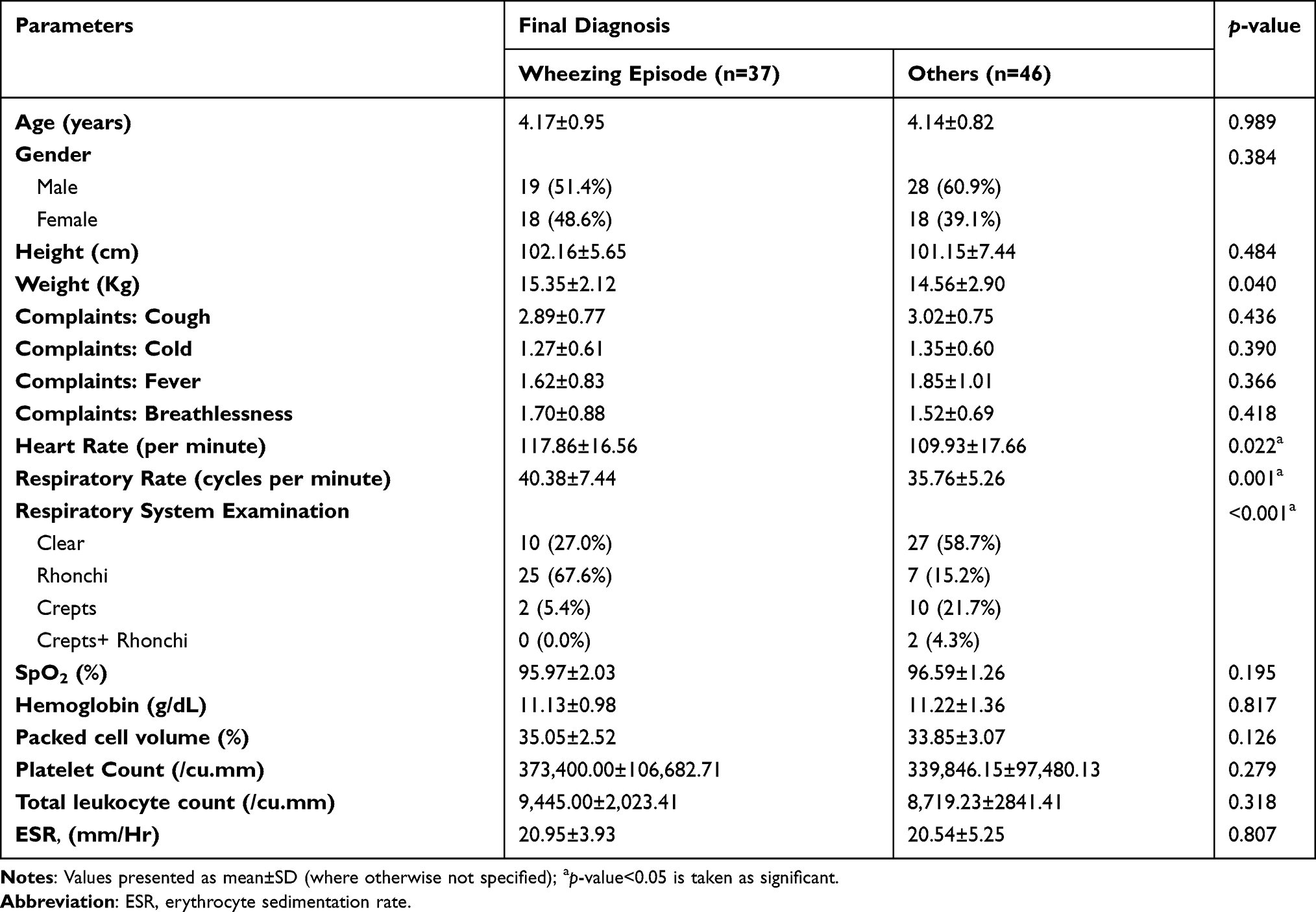 |
Table 1 Association Between Final Diagnosis and Demographic and Clinical Parameters |
The pre-nebulization values of AX, R5, X20, and resonant frequency were significantly higher in the wheezing group. After nebulization the values of AX, R5, X20, and resonant frequency did not show a significant difference when compared with the other group. The actual change in values of AX, R5, X20, and resonant frequency showed a statistically significant difference in the wheezing episode group. The percent change in R5 observed (post-nebulization) showed a significant difference. The percent change as compared to predicted values of R5 and X20 also showed a statistically significant difference in the wheezing episode group (Table 2).
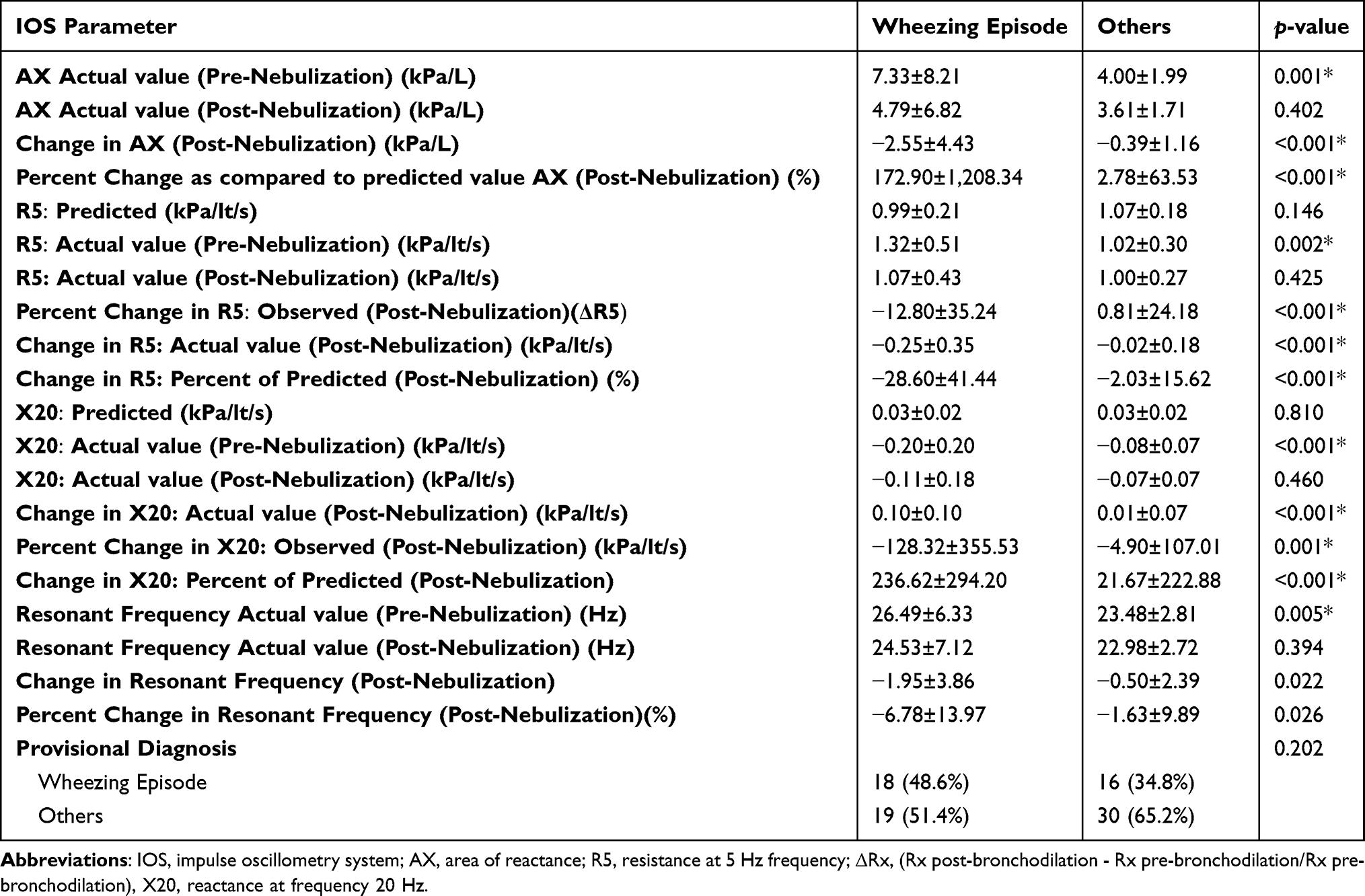 |
Table 2 Significance of Impulse Oscillometry Parameters in Wheezing Episode and Others |
The sensitivity of the impulse oscillometry parameters AX, R5, X20, and resonant frequency was 60–80%. The specificity varied from 56–93%. The change in pre- and post-nebulization values for R5 showed a maximum specificity of 93.5% (for the cutoff 0.24, ROC value=0.785). The positive predictive value for change in R5 was 88.5% (range=70–98%) and the negative predictive value was 75.4% (range=62–86%) (Table 3).
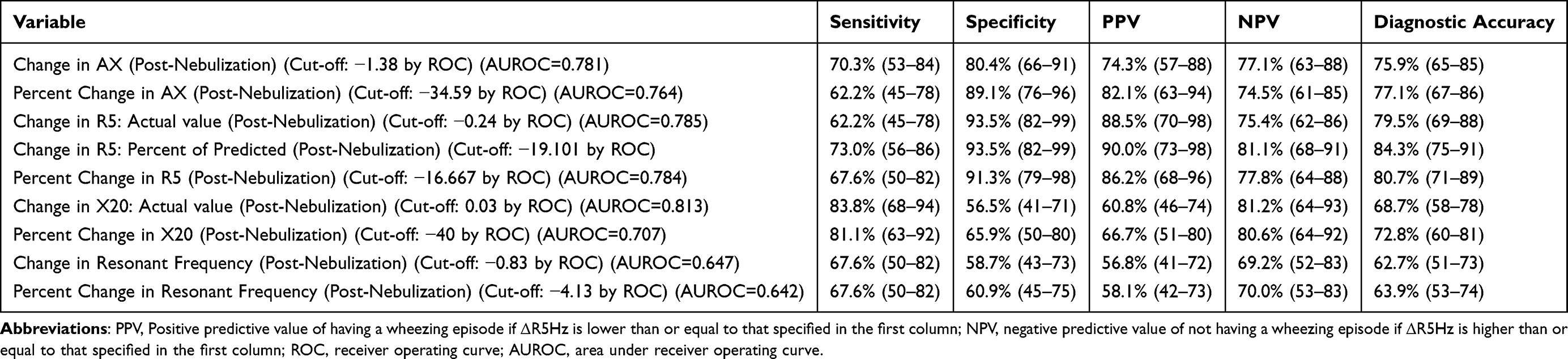 |
Table 3 Sensitivity, Specificity, Positive Predictive Value, and Negative Predictive Value of Significant IOS Parameters |
The percentage change in R at 5 Hz (observed post-nebulization ie Δ5) at cut-off 16.67 has a 67.6% sensitivity and a specificity of 91.3% and a positive predictive value of 86.2% and a negative predictive value of 77.8% (ROC value=0.784). The confidence intervals for these values were narrow, indicating the strength of these values. At a cut-off of Absolute Change in R5: Percent of Predicted R5 (Post-Nebulization) ≤-19.101, it predicts a final diagnosis of wheezing episode with a sensitivity of 73%, and a specificity of 93.5% (ROC value=0.801). Change in AX 4.5 had an ROC value of 0.781. The sensitivity 73%, specificity 67.4%, PPV 64.3%, and NPV 69.9% were good. The resonant frequency had an ROC value of 0.647. The sensitivity, specificity, PPV, and NPV values were moderately good.
The odds ratios were calculated for these IOS parameters. The odds ratio for change in R5 was 23.55 and it was 21.88 for percent change of R5 and change in R5% of predicted (post-nebulization) was 38.7. The odds ratios were 9.7 for change in AX values and 13.47 for the percent change in AX value (Table 4).
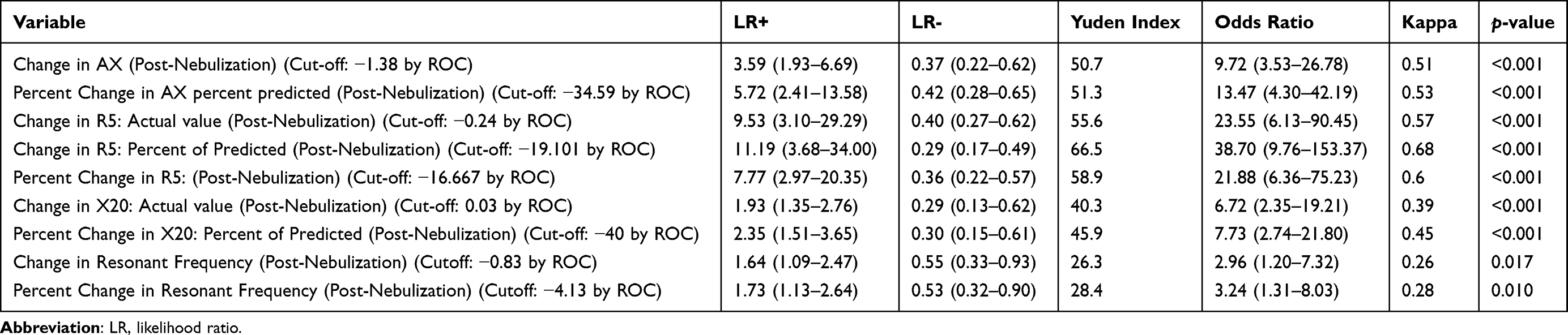 |
Table 4 The Odds Ratio for Significant Parameters of Impulse Oscillometry |
Discussion
Respiratory problems are the commonest cause of morbidity and mortality in children. Wheezing episodes remain the common cause of morbidity in children.6 The diagnosis of these conditions is objectively difficult due to the unavailability of a test which can be performed easily in children. Spirometry is the currently performed test for assessing pulmonary function in clinical practice and is considered to be the gold standard for diagnosing asthma. However, spirometry is not easy to perform in children younger than 5 years, since it requires good patient co-operation. Batmaz et al19 and Knitillha et al20 conducted a study in children with impulse oscillometry and spirometry and concluded that IOS values correlated with spirometry. DuBois et al21 discovered the forced oscillation technique (FOT), a tool that measures pulmonary function using sound waves of the same frequency generated by a loud speaker and which pass into the lungs at the time of tidal breathing. This test was modified by Michaelson et al,22 and named the impulse oscillometry system (IOS). In this test, resistance is measured. Children perform this test easily as minimum cooperation is needed. In our study, five children did not perform the test, which could be because of initial fear about a test in the hospital. More familiarity probably could resolve this issue. IOS parameters such as reactance (R), impedance (X), and total resistance (Z) at low frequency (5 Hz) were more likely to differentiate wheezing from other respiratory disorders than at higher frequencies. This can be attributed to easy penetration of low frequency into peripheral bronchial tree (diameter <2 mm) and, hence, reflects obstruction in both the peripheral and the central airways, whereas higher frequencies do not transmit to the peripheral airways of lungs.
This study was designed to find the usefulness of an impulse oscillometry system in routine pediatric office practice. Hence the population of children with symptoms fever, cough, cold, and breathlessness as told by the parents was included in the study. In a diagnostic study rather than a healthy control group the children with similar symptoms form a better comparative group. The idea was to differentiate the wheezing episode with a history and clinical examination and a test in the outpatient department. The children with mild-to-moderate disease severity were included as the diagnosis is likely to be difficult in these children. A coherence value above 0.9 was taken as an acceptable record. It was found to be feasible in the routine outpatient department. The impulse oscillometry can be used for longitudinal assessment of airway resistance, which has been shown in a study by Konstantinou et al.15 Various reference equations have been derived at various geographic regions and in various age groups.23–26 But they cannot be used at other geographical areas. As has been shown by Konstantinou et al,15 actual values and percent change in actual values of IOS parameters can be used instead of reference values for children below 6 years. In this study it is seen that the percent change in predicted value as well as percent change in actual value both have almost similar sensitivity and specificity. In a region where the reference values are not available, values before and after bronchodilation can help in the diagnosis. The mean value of R at 5 Hz in the study by Konstantinou et al15 was 1.114±0.280 kPa/lt/sec at the time of wheezing episode, the mean value in this study was 1.32 ± 0.51kPa/lt/sec. This difference may be because the age group in our study was 3–6 years and the age group in the study by Konstantinou et al15 was 4–6 years. The lower the age group the higher is the value of resistance. The confidence interval in this study was larger than the other study because there was a large range of age group. In this study, percent change in R at 5 Hz if taken as −16.6%, sensitivity was 67.6%, specificity was 91.3%, and diagnostic accuracy was 80.7%. In the study by Konstantinou et al,15 a cut-off of −20.5% had a sensitivity of 69.7% and specificity of 74.41% and at −46.4% the specificity increased to 100% but sensitivity decreased to 4.3%. Klug et al27 in their study had values of R at 5 Hz 1.48±0.25 pre-bronchodilation and 1.25±0.22 post-bronchodilation in age group 2–5 years. The higher R at 5 Hz values could be because children selected were stable asthmatic children and with the lower age group than in this study.
The odds ratio calculated shows that actual change in R5, percent change in actual value of R5, or percentage change as compared to predicted value are the significant parameters with discriminating ability and, hence, it may help in practice in the diagnosis of wheezing episode. In addition, the parameters AX and resonant frequency can also be used. X20 shows similar good prediction but how inertia of the lung or airways is affected by bronchodilation needs further research.
The measurement of airway resistance not only helps in differentiating the wheezing episode from other diseases but it will help in quantifying the resistance at each episode and measuring the response to bronchodilators after treatment. This will help in detecting borderline cases and it will help in proper diagnosis and treatment of the patients.
Limitations
The limitations of the study are the small sample size and the study of IOS parameters was done only twice on one single day. One observer of clinical severity may contribute bias to the drawbacks. All the stringent criteria of within-subject variability were not followed.
Conclusion
Using percent change in actual values of R at 5 Hz and percent change in R at 5 Hz as compared to reference standard after nebulization with salbutamol may help in arriving at the diagnosis of wheezing episode along with history and examination of the patient. It requires the least cooperation from children. Hence, it can be considered for the same among 3–6 years old children.
Acknowledgments
We acknowledge the support and encouragement from all the members of the Department of Pediatrics, D Y Patil Medical College, Kolhapur.
Funding
No funding was given by any agency to this research.
Disclosure
None of the authors has any conflict of interest for this work.
References
1. Weiss LN. The diagnosis of wheezing in children. Am Fam Physician. 2008;77(8):1109–1114. PMID: 18481558.
2. Martinez FD, Wright AL, Taussig LM, Holberg CJ, Halonen M, Morgan WJ. Asthma and wheezing in the first six years of life. The Group Health Medical Associates. N Engl J Med. 1995;332(3):133–138. PMID: 7800004. doi:10.1056/NEJM199501193320301
3. Sarnaik AP, Heidemann SM, Clark JA. Chest wall. In: Kliegman B, Stanton J, Geme S, Schor N, editors. Nelson Textbook of Pediatrics.
4. Elphick HE, Ritson S, Rodgers H, Everard ML. When a “wheeze” is not a wheeze: acoustic analysis of breath sounds in infants. Eur Respir J. 2000;16(4):593–597. doi:10.1034/j.1399-3003.2000.16d04.x
5. Tenero L, Tezza G, Cattazzo E, Piacentini G. Wheezing in preschool children. Early Hum Dev. 2013;89(Suppl 3):S13–S17. PMID: 24001476; PMCID: PMC7130726. doi:10.1016/j.earlhumdev.2013.07.017
6. Brand PL, Baraldi E, Bisgaard H, et al. Definition, assessment and treatment of wheezing disorders in preschool children: an evidence-based approach. Eur Respir J. 2008;32(4):1096–1110. doi:10.1183/09031936.00002108
7. Bokov P, Mahut B, Flaud P, Delclaux C. Wheezing recognition algorithm using recordings of respiratory sounds at the mouth in a pediatric population. Comput Biol Med. 2016;1(70):40–50. doi:10.1016/j.compbiomed.2016.01.002
8. Bekhof J, Reimink R, Bartels I, et al. Large observer variation of clinical assessment of dyspneic wheezing children. Arch Dis Child. 2015;100:649–653. doi:10.1136/archdischild-2014-307143
9. Konstantinou GN, Xepapadaki P, Manousakis E, et al. 2013 Assessment of airflow limitation, airway inflammation, and symptoms during virus-induced wheezing episodes in 4-to 6-year-old children. J Allergy Clin Immunol. 2013;131(1):87–93. doi:10.1016/j.jaci.2012.10.033
10. Marotta A, Klinnert MD, Price MR, Larsen GL, Liu AH. Impulse oscillometry provides an effective measure of lung dysfunction in 4-year-old children at risk for persistent asthma. J Allergy Clin Immunol. 2003;112(2):317–322. doi:10.1067/mai.2003.1627
11. Komarow HD, Skinner J, Young M, et al. A study of the use of impulse oscillometry in the evaluation of children with asthma: analysis of lung parameters, order effect, and utility compared with spirometry. Pediatr Pulmonol. 2012;47(1):18–26. doi:10.1002/ppul.21507
12. de Oliveira Jorge PP, de Lima JH, Chong e Silva DC, Medeiros D, Solé D, Wandalsen GF. Impulse oscillometry in the assessment of children’s lung function. Allergologia et Immunopathologia. 2019;47(3):295–302. doi:10.1016/j.aller.2018.03.003
13. Brashier B, Salvi S. Measuring lung function using sound waves: role of the forced oscillation technique and impulse oscillometry system. Breathe. 2015;11(1):57–65. doi:10.1183/20734735.020514
14. Burman J, Malmberg LP, Remes S, Jartti T, Pelkonen AS, Mäkelä MJ. Impulse oscillometry and free-running tests for diagnosing asthma and monitoring lung function in young children. Ann Allergy Asthma Immunol. 2021;127(3):326–333. doi:10.1016/j.anai.2021.03.030
15. Konstantinou GN, Papadopoulos NG, Manousakis E, Xepapadaki P. Virus-induced asthma/wheeze in preschool children: longitudinal assessment of airflow limitation using impulse oscillometry. J Clinl Med. 2019;8(9):1475. doi:10.3390/jcm8091475
16. Pourhoseingholi MA, Vahedi M, Rahimzadeh M. Sample size calculation in medical studies. Gastroenterol Hepatol Bed Bench. 2013;6(1):14–17.
17. Beydon N, Davis SD, Lombardi E, et al. An official American Thoracic Society/European Respiratory Society statement: pulmonary function testing in preschool children. Am J Respir Crit Care Med. 2007;175(12):1304–1345. doi:10.1164/rccm.200605-642ST
18. Dencker M, Malmberg LP, Valind S, et al. Reference values for respiratory system impedance by using impulse oscillometry in children aged 2–11 years. Clin Physiol Funct Imaging. 2006;26(4):247–250. PMID: 16836699. doi:10.1111/j.1475-097X.2006.00682.x
19. Batmaz SB, Kuyucu S, Arıkoglu T, Tezol O, Aydogdu A. Impulse oscillometry in acute and stable asthmatic children: a comparison with spirometry. J Asthma. 2016;53(2):179–186. doi:10.3109/02770903.2015.1081699
20. Knihtilä H, Kotaniemi‐Syrjänen A, Mäkelä MJ, Bondestam J, Pelkonen AS, Malmberg LP. Preschool oscillometry and lung function at adolescence in asthmatic children. Pediatr Pulmonol. 2015;50(12):1205–1213. doi:10.1002/ppul.23188
21. DuBois AB, Botelho SY, Comroe JH
22. Michaelson ED, Grassman ED, Peters WR. Pulmonary mechanics by spectral analysis of forced random noise. J Clin Invest. 1975;56(5):1210–1230. doi:10.1172/JCI108198
23. Amra B, Soltaninejad F, Golshan M. Respiratory resistance by impulse oscillometry in healthy Iranian children aged 5–19 years. Iran J Allergy Asthma Immunol. 2008;7(1):25–29.
24. De Assumpção MS, Gonçalves RM, Martins R, Bobbio TG, Schivinski CI. Reference equations for impulse oscillometry system parameters in healthy Brazilian children and adolescents. Respir Care. 2016;61(8):1090–1099. doi:10.4187/respcare.04226
25. Gochicoa-Rangel L, Torre-Bouscoulet L, Martínez-Briseño D, Rodríguez-Moreno L, Cantú-González G, Vargas MH. Values of impulse oscillometry in healthy Mexican children and adolescents. Respir Care. 2015;60(1):119–127. doi:10.4187/respcare.03374
26. Duenas-Meza E, Correa E, López E, et al. Impulse oscillometry reference values and bronchodilator response in three-to five-year old children living at high altitude. J Asthma Allergy. 2019;12:263. doi:10.2147/JAA.S214297
27. Klug B, Bisgaard H. Lung function and short-term outcome in young asthmatic children. Eur Respir J. 1999;14(5):1185–1189. doi:10.1183/09031936.99.14511859
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.