Back to Journals » Journal of Asthma and Allergy » Volume 12
Impulse oscillometry reference values and bronchodilator response in three- to five-year old children living at high altitude
Authors Duenas-Meza E ![]() , Correa E, López E, Morales JC, Aguirre-Franco CE, Morantes-Ariza CF, Granados CE
, Correa E, López E, Morales JC, Aguirre-Franco CE, Morantes-Ariza CF, Granados CE ![]() , González-García M
, González-García M ![]()
Received 3 May 2019
Accepted for publication 5 August 2019
Published 19 September 2019 Volume 2019:12 Pages 263—271
DOI https://doi.org/10.2147/JAA.S214297
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Elida Duenas-Meza,1 Eliana Correa,1 Eliana López,2 Juan Carlos Morales,2 Carlos Eduardo Aguirre-Franco,1 Carlos Fabián Morantes-Ariza,3 Carlos Eduardo Granados,2 Mauricio González-García1
1Fundación Neumológica Colombiana, Bogotá, Colombia; 2Universidad De La Sabana, Chía, Colombia; 3Universidad Nacional De Colombia, Bogotá, Colombia
Correspondence: Elida Duenas-Meza
Fundación Neumológica Colombiana, Bogotá 110131, Colombia
Tel +57 1 742 8914
Fax +57 1 742 8904
Email [email protected]
Introduction: Impulse oscillometry (IOS) is used to measure airway impedance. It is an effective tool for diagnosing and treating respiratory diseases, and it has the advantage that it does not require forced respiratory maneuvers. IOS reference values are required for each population group.
Objective: This study aimed to determine the IOS reference values and bronchodilator response in healthy preschool children living in Bogotá, Colombia.
Methods: We performed a cross-sectional study in preschool children who had no history of respiratory disease; 96 children fit the parameters for testing to determine normal values according to the American Thoracic Society and European Respiratory Society criteria.
Results: Values for respiratory resistance (Rrs) and reactance (Xrs) at 5, 10, and 20 Hz, respiratory impedance (Zrs, and resonance frequency (Fres) were established. Height was the most influential independent variable for IOS values; an increase in height led to a reduction in Rrs5 and Rrs20 and an increase in Xrs5. After the administration of 400 mcg of salbutamol the values for Rrs5(−17.48%), Rrs20(−8.63%), Fres (−10.68%), and area of reactance (−35.44%) were reduced, meanwhile Xrs5 (15.35%) was increased.
Conclusions: Normal IOS values before and after the administration of 400 mcg of salbutamol were determined for a population of children aged 3–5 years at 2,640 m. Reference IOS equations for these children are presented. A relative change of up to −28% and 36% after the use of salbutamol for respiratory resistance and reactance, respectively, should be considered as an upper limit of the normal range, and possible appropriate cut-off values for defining significant response for evaluating therapeutic interventions.
Keywords: oscillometry, children, reference values, high altitude, respiratory function tests, cross-sectional studies
Introduction
Assessing pulmonary function in children is becoming increasingly important; it allows the evaluation of disease severity, confirmation of clinical diagnoses and follow-up of patients with respiratory disease. Spirometry has been the gold standard for studying asthma in children above the age of six. However, it requires active collaboration from the patient making the use difficult in preschool children This limitation has led to the implementation of other measuring techniques such as impulse oscillometry (IOS), which requires only passive cooperation to measure respiratory system impedance over a range of frequencies (5–20 Hz). This method measures both resistance and reactance of the proximal and distal airway by generating specific sound pulses into the respiratory system during spontaneous respiration.1–3 Furthermore, IOS is more sensitive than spirometry.7 in detecting reversible airway obstruction, and it can be applied to children under the age of six years.1,4,8
Proper interpretation of IOS requires one to be familiar with the specific test attributes and normal reference values (NRVs). Extrapolation of these values from different populations is not recommended as this may lead to errors when interpreting respiratory function, as well as disease evaluation and severity. Other factors such as height, respiratory system development, and geographic conditions are the main determinants of the reference values.5,6 Therefore, it is necessary to establish NRVs for IOS in a children under six years old, in whom a higher prevalence and morbidity of respiratory disease have been documented.1,4,8
The decrease of air density at high altitude can influence the values of resistance measured by IOS. Few studies have established NRVs at high altitude or assessed healthy children’s response to bronchodilators; such information is useful for evaluating children with respiratory disease.9–15 In Colombia, around 20% of the population (10 million people) live at high altitude (>2,500 meters above sea level). Colombia doesn’t have locally derived NRVs for IOS, and instead, they are extrapolated from other populations. The main objective of this study was to determine NRVs of healthy preschool children at high altitude for the total airway resistance (Rrs5 Hz), proximal airway (Rrs20 Hz), reactance at 5 Hz, resonance frequency (Fres), reactance area (AX), the difference between Rrs5 and Rrs20 (Rrs5–Rrs20) and bronchodilator response.
Materials and methods
We conducted a cross-sectional study that included preschool children aged 3 to5 from both sexes with normal weight, height and body mass index (BMI) between the range ±2 standard deviations (SDs) in accordance to the World Health Organization (WHO), who did not have respiratory disease and were attending public and private kindergarten in Bogotá. The International Study of Asthma and Allergies in Childhood (ISAAC) survey was administered to each child to determine the presence of respiratory disease.16,17
To establish the NRVs we excluded children with a personal or family history of asthma or wheezing, allergenic rhinitis or atopic dermatitis, history of premature birth (<37 weeks), low birth weight (<2500 g), obesity (BMI >2SD), bronchopulmonary dysplasia, mechanical ventilation, exposure to cigarette smoke. Respiratory infection (flu, sinusitis, pneumonia, croup) within the four weeks before the test; dyspnea, coughing, wheezing; or oxygen saturation below 90% before the IOS. Following the recommendations of the American Thoracic Society (ATS)/European Respiratory Society (ERS) for the study of normal values,18–20 children who were incapable of performing the test were also excluded.
The sample size was determined by estimating the expected population mean and SD for Rrs5, with an error of 0.05% and confidence interval (CI) of 95%. The estimated sample size was 82 children.
The protocol and informed consent were approved by the ethics committees of the University of Sabana and the Fundación Neumológica Colombiana, which are governed by the Declaration of Helsinki. The written informed consent was obtained from the parents; taking into account the age of the children, and a psychological evaluation was requested to indicate the desire to participate in the test.
Medical evaluation
On the day of the assessment, a pediatric physician performed a full physical examination and a verification of selection criteria. The physical exam comprised the following anthropometric measurements: weight, height, and pulse oximetry with a ChoiceMMed® oximeter, model Oxywatch C20.
Oscillometry
A Jaeger MasterScreen (Jaeger®) was used. The system was calibrated through a single volume of air (3 L) at difference flow rates, which were verified with a reference resistance device (0.2 kPa/l/s) supplied by the manufacturer. An impulse generator produced brief pressure pulses at intervals of 0.2 s. In this study, the mean Rrs and Xrs values were calculated over a period of 30 s in the frequency range of 5–20 Hz; the ATS/ERS recommendations for testing pulmonary function in children were also followed.20,21 Rrs5 Hz, Rrs20 Hz, Xrs5 Hz, Fres, and AX results were recorded. . We implemented the following technique: each child sat in a straight position with a nose pin. He or she was asked to inhale ambient air at a regular volume by mouth through a nozzle with a filter which was plugged into the pneumotachograph; this was continued for approximately 30 s. A parent or the child was asked to hold the child’s cheeks with both hands to prevent the pulse from escaping to the mouth walls.
We recorded measurements from three acceptable maneuvers, those that failed to fulfill the reproducibility and acceptability criteria were discarded. Salbutamol (400 µg) was administered via pressurized metered dose inhaler (Ventilan, GlaxoSmithKline) using a spacer device (aerochamber Plus®). Respiratory function measurements were repeated as describes previously 15 min after the salbutamol administration.
Tests were only considered valid if the trace was linear, ascendant, and within the system’s range of normality without interference from cough, crying, or swallowing, during measurements. Three measures were carried out, and each participant´s best test was selected. The reproducibility was validated with a variability coefficient of <10% for both Rrs5 and Rrs20, the acceptability of the test determined a coherence >0.6 for Rrs5.20
Statistical analysis
The variables of Rrs5, Rrs20, Xrs5, Fres, and Rrs5–Rrs20 were described using exploratory analyses. Normality and homogeneity tests were performed, with sex as an independent variable. A Pearson correlation matrix was obtained for all anthropometric variables. Due to the high collinearity with other variables, height was used as the main predictor for response variables in the regression models. This relationship was evaluated using generalized linear models with a Gaussian distribution and “identity” as the link function. Models with the lowest Akaike information criterion (AIC), where the intercepts and residual deviations presented significant values (α=0.05), were selected. Two-tailed CIs were estimated for each significant model (α=0.05).
Due to the specific behavior of Xrs5, the applied linear model of the first-degree accounted for a low fraction of variance. Thus, we used a third-degree polynomial model to improve the explanatory power. This model used non-orthogonal coefficients; we also used the adjusted R2 value to prevent overestimation of the coefficient’s significance. Mean differences on Rrs5 were tested for the height variable using a Student's t-test. We found significant differences between the groups at a threshold of 1.07 m in height. Furthermore, we applied an alternative second-degree model for children with a height of less than 1.07 m (Figure 1).
 |
Figure 1 Regression for Xrs5 within two height ranges. Comparison between the models which takes into account the whole sample (height range = 0.9 m–1.16 m; n=96; dotted line) and the model that takes into account individuals of height less than 1.07m (Size range = 0.9m-1.07m; n=69; continuous line), inflection point of the slope of the model with all individuals (vertical line). The graph shows the effect of reduction in slope of regression when contemplating (N=30), generating a deviation of the trend of the height group smaller than 1.07 m (n=69). Blue triangles correspond to men and red squares women. |
Results
A total of 487 respiratory disease surveys were conducted. Among the subjects, 391 children were excluded: 179 due to a family or personal history of asthma or recurrent wheeze, 67 for cigarette smoke exposure, 58 due to low birth weight or premature birth, four due to a history of mechanical ventilation, and four due to the presence of other respiratory diseases. An additional 49 children had incomplete surveys or did not meet the age requirement. Furthermore, 19 children were excluded on the test day because they showed signs of obesity or malnutrition, 11 were excluded because they exhibited symptoms of respiratory anomalies within the last four weeks (Figure 2).
 |
Figure 2 Selection for the impulse oscillometry test. |
In total, 96 oscillometries were performed. Participants’ ages ranged from 37 to 71 months, with an average of 55.7 months (4 years and 7 months); 39.6% (n=38) were male. The means and standard deviation of height, weight and BMI are shown in Table 1.
 |
Table 1 Anthropometric data from the participants |
A linear regression analysis of the IOS measurements indicated that height was the only variable that was significantly related to both resistance at 5 Hz (Rrs5) and 20 Hz (Rrs20), as well as reactance at 5 Hz (Xrs5). A linear negative relationship between height and Rrs5 and Rrs20 was shown, while a positive relationship between height and Xrs5 was exhibited. No association was found between height and Fres and AX (Figure 3). Changes in the variables after the administration of 400 mcg of salbutamol are shown in Table 2; the values for Rrs5, Rrs20, Fres, and AX were reduced, while Xrs5 was increased.
 |
Table 2 Impulse oscillometry parameters at baseline and bronchodilator responses |
 |
Figure 3 Representation of the linear regression analysis of the measures Rrs5 and Xrs5. A positive relation is observed with an increase of Xrs5 as the size increases and a negative linear relation, with decrease of Rrs5. |
Table 3 shows the multiple regression models with height as an independent variable for Rrs5, Rrs20, and Xrs5. Reference equations and values for Rrs5, Rrs20, and Xrs5 were proposed, as well as central tendency values and the 95th quantile for AX. Variation coefficients below 10% that fit the reproducibility parameters were reported in the test.
 |
Table 3 Reference equations for impulse oscillometry variables in healthy children |
When values of Rrs5, Rrs20, Xrs5, AX, and Fres in children with height below and above 1.07 m were compared, there was no significant difference for Rrs5, AX, and Fres between the two groups (Figure 1).
Discussion
This study determined the IOS reference values for preschool children living at high altitude (2,640 m). Only height exhibited a statistically significant association for Rrs5, Rrs20, and Xrs5. An inverse relationship with height was found for Rrs5 that followed a straight-line pattern; this relationship was not found between Fres and Xrs5. As expected, resistance tended to decrease as height increased.22,23
The reactance, which reflects the peripheral pulmonary compartment and elastic tissue, including the thorax, at low frequencies (Xrs5), exhibited a significant increase with height gain. This study observed significant differences between the groups below and above 1.07 m of height (Figure 1). The same pattern was observed by Nowowiejska et al for children aged 3–18 years, with a height threshold of 1.10 m. This pattern is related to the differential elastic properties of the respiratory system23 and the increased number of alveoli.24
These findings are consistent with those of previous studies of preschool children, where the height and IOS variables Rrs5, Rrs20, and Xrs5 followed a straight-line pattern.5,9,10,24–27 These straight-line patterns did not emerge in the works of Gochicoa et al,11 Dencker et al,22 and Nowowiejska et al,23 in which broader age ranges (2–15 years, 3–11 years, and 3–18 years, respectively) were used; the application of logarithmic transformations to determine the results in these models followed a curved pattern.11,22,23 Other studies have identified different anthropometric variables that influence IOS parameters, such as age for Rrs5–Rrs20 value (10) or Rrs10, a parameter not measured in this study.26
Data describing the percentage of post-bronchodilator change in healthy children are scarce.8–10,14,26,28 Establishing threshold values for the studied parameters allows the presence of reversible airway obstruction to be determined. This study found percentage changes for Rrs5 (–17.48%), Rrs20 (–8.63%), Xrs5 (+15.35%), and Fres (–10.68%), AXrs (−35.44) that were comparable to data obtained by other authors.8,9,26,29
Hellinskx et al9 reported a study of bronchodilator response in healthy and asthmatic children up to 6.5 yearsof age using the IOS. They did not find any difference between the two study groups, either in baseline or in bronchodilator responsiveness (Rrs:-12%). Lee et al26 found percentage changes after applying a bronchodilator to healthy children of –11.8% (SD: 9.5) for Rrs5, –6.05% (SD: 9.1%) for Rrs20, and –13.4% (SD: 28.3) for Xrs5. Komarow et al8 established a threshold value of −11.2% for Rrs5 and –29% for AX, the latter corresponding to a sensitivity of 67% and specificity of 69%. In Malmberg et al’s research,10 the threshold values for bronchodilator response were determined as: –19% for Rrs5, –15.2% for Rrs20, and –23.8% for Fres. Vu et al30 measured the response to a bronchodilator and calculated a Youden index, which indicates the combination of optimal sensibility and specificity. They determined a range of 20–25% change as the best threshold for bronchodilator response. Most significant responses to bronchodilator application have exhibited sensitivities of around 70%.29,31,32
A reported Rrs5 reduction value of –40%,14 has been proposed to be considered a cutoff level for a positive bronchodilator response in children. The changes in Rrs5 found in this study do not reach such limits. Differences in study populations may explain this outcome. Our study population consisted of well-defined groups of healthy subjects. Nielsen and Bisgaard found cutoff values for Rrs5 of −29%,29 that were similar to the value in the present study (−28.36%). Airway reactance, which generally remains unmodified by salbutamol in healthy children,29 exhibited an 15% change in this study. This change is was also observed bby Olaguibel et al and Klug13,33 in children with stable asthma, suggesting a slight response to salbutamol in this group of patients. Our results are in agreement with previous observations of a certain bronchomotor tone existing even in healthy.9,29
Based on these findings and previous studies, we propose a threshold for the positive response to bronchodilators within a CI of 95% or higher. Most studies have not included a threshold value with a CI, which may increase the risk of overinterpreting the response to the bronchodilator. Hence, calculating a 95% CI establishes the limits of the reference group, allowing positive and negative significance thresholds to be determined.9,10
Regression curves from this study’s analysis were similar to those described by Lai et al,24 Lee et al,26 Hellinsckx et al,9 Malmberg et al,10 de Assumpção et al,15 and Schackleton et al12 for groups of the same ages at sea level. The adjusted determination coefficient (R2; less than 20%), was lower in studies including older children.11,15 However, studies on preschool children have found low R2 values ranging from 12 to 30%.5,25,34,35
Differences in equipment characteristics or methodologies do not explain differences among Colombian reference values and those from other regions; instead, they could be due to differences in height, such as described by Quanjer et al,36 especially for preschoolers. The parameter that most influenced pulmonary function in their study was the height (Table 4, Figure 4).
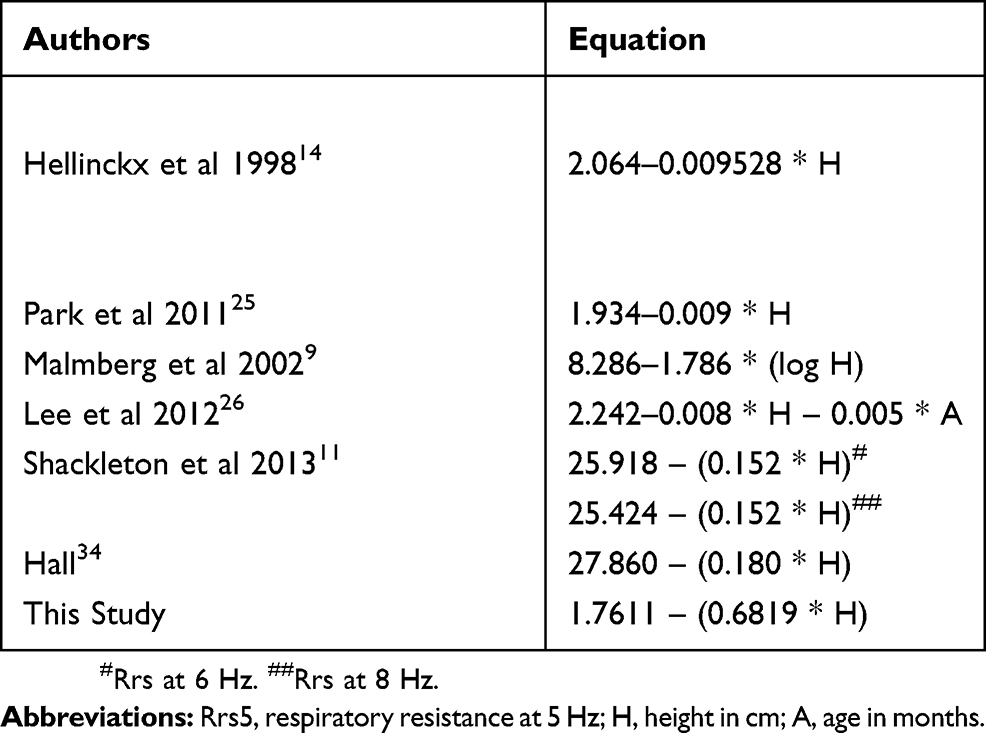 |
Table 4 Summary of equations of regression for Rrs5 in healthy children |
 |
Figure 4 Comparison of reference equations for respiratory resistance at 5Hz between this study and previous studies in young healthy children. |
This study was conducted at high altitude, a condition lacking in most IOS studies, which prevents the comparison of IOS results at sea level and high altitude. In physiological terms, the decrease in air density would result in a decline of the airway resistance; however, some studies using the interrupter technique (Rint) to assess respiratory mechanics at high altitudes37,38 have shown a lower than expected decrease of the resistance. The former may suggest that other unclear factors could modify the caliber of the respiratory system or the mechanics at high altitude. The IOS method allowes the frictional and resistance of the elastic tissue to be included. Since a control group at a different altitude was not included, conclusions cannot be made on this matter.
The main strength of this study was the estimation of normal values for pre- and post-bronchodilator conditions in a strictly and representatively selected group of children at high altitude (2,640 m), within a specific age range and including variables not measured in other studies, such a BD response. We did not have validation group. Although the ATS/ERS recommendations19,20 apply to children two and older, we did not include children between two and three years due to the difficulty they have to perform the maneuvers.
Conclusion
In summary, we stablished NRVs for IOS in pre- and post-bronchodilator application conditions for healthy children aged 3–5 years at high altitude. We found that height was the best predictor variable for most of the oscillometric parameters. Reference equations based on height were determined for both pre- and post-bronchodilator. A fall in Rrs5 of 28% or an increase in Xrs of 36% in the post-bronchodilator test could be considered as upper limit of the normal variability of resistance and reactance respectively, and the possible appropriate cut-off values for defining a significant response for evaluating therapeutic interventions.
Further studies are required to determine the clinical significance of post-BD changes in lung function in preschool children with lung disease. These values can be used for this population and populations with similar characteristics.
Acknowledgments
The authors thank the Pulmonary Function and Research Group from the Fundación Neumologica Colombiana for their support. They facilitated the availability of equipment for the tests and data collection. The authors also wish to thank the directors of the different educational institutes who allowed us to contact the children.
Author contributions
All authors contributed towards data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Al-Mutairi S, Sharma P, Al-Alawi A, et al. Impulse oscillometry: an alternative modality to the conventional pulmonary function test to categorise obstructive pulmonary disorders. Clin Exp Med. 2007;7:56–64. doi:10.1007/s10238-007-0126-y
2. Komarow HD, Myles IA, Uzzaman A, et al. Impulse oscillometry in the evaluation of diseases of the airways in children. Ann Allergy Asthma Immunol. 2011;106:191–199. doi:10.1016/j.anai.2010.11.011
3. Peirano R. Oscilometría de impulso (IOS) en niños. Neumol Pediatr. 2010;5:89–95.
4. Short PM, Williamson PA, Lipworth BJ. Sensitivity of impulse oscillometry and spirometry in beta-blocker induced bronchoconstriction and beta-agonist bronchodilatation in asthma. Ann Allergy Asthma Immunol. 2012;109:412–415. doi:10.1016/j.anai.2012.09.010
5. Komarow HD, Skinner J, Young M, et al. A study of the use of impulse oscillometry in the evaluation of children with asthma: analysis of lung parameters, order effect, and utility compared with spirometry. Pediatr Pulmonol. 2012;47:18–26. doi:10.1002/ppul.21507
6. Dennis RJ, Caraballo L, García E, et al. Prevalence of asthma and other allergic conditions in Colombia 2009–2010: a cross-sectional study. BMC Pulm Med. 2012;12:1. doi:10.1186/1471-2466-12-17
7. Frei J, Jutla J, Kramer G, et al. Impulse oscillometry: reference values in children 100 to 150 cm in height and 3 to 10 years of age. Chest. 2005;128:1266–1273. doi:10.1378/chest.128.3.1266
8. Smith H, Reinhold P, Goldman M. Forced oscillation technique and impulse oscillometry. Eur Respir Monograph. 2005;31:72–105.
9. Malmberg L, Pelkonen A, Poussa T, et al. Determinants of respiratory system input impedance and bronchodilator response in healthy Finnish preschool children. Clin Physiol Funct Imaging. 2002;22:64–71.
10. Gochicoa-Rangel L, Torre-Bouscoulet L, Martínez-Briceño D, et al. Values of impulse oscillometry in healthy mexican children and adolescents. Respir Care. 2015;60:119–127.
11. Shackleton C, Barraza-Villarreal A, Chen L, et al. Reference ranges for Mexican preschool-aged children using the forced oscillation technique. Arch Bronconeumol. 2013;49:326–329. doi:10.1016/j.arbres.2013.01.014
12. Olaguibel J, Alvarez-Puebla M, Anda M, et al. Comparative analysis of the bronchodilator response measured by impulse oscillometry (IOS), spirometry and body plethysmography in asthmatic children. J Investig Allergol Clin Immunol. 2004;15:102–106.
13. Vu LT, Demoulin B, Nguyen YT, et al. Respiratory impedance and response to salbutamol in healthy Vietnamese children. Pediatr Pulmonol. 2008;43:1013–1019. doi:10.1002/ppul.20904
14. Hellinckx J, De Boeck K, Bande-Knops J, et al. Bronchodilator response in 3–6.5 years old healthy and stable asthmatic children. Eur Respir J. 1998;12:438–443.
15. de Assumpção MS, Gonçalves RM, Martins R, et al. Reference equations for impulse oscillometry system parameters in healthy brazilian children and adolescents. Respir Care. 2016;61:1090–1099.
16. Garcia E, Aristizabal G, Vasquez C, et al. Prevalence of and factors associated with current asthma symptoms in school children aged 6–7 and 13–14 yr old in Bogota, Colombia. Pediatr Allergy Immunol. 2008;19:307–314. doi:10.1111/j.1399-3038.2007.00650.x
17. Mata Fernandez C, Fernandez-Benitez M, Perez Miranda M, et al. Validation of the Spanish version of the Phase III ISAAC questionnaire on asthma. J Investig Allergol Clin Immunol. 2005;15:201–210.
18. Taussig LM, Chernick V, Wood R, et al. Standardization of lung function testing in children. Proceedings and Recommendations of the GAP Conference Committee, Cystic Fibrosis Foundation. J Pediatr. 1980;97:668–676. doi:10.1016/s0022-3476(80)80039-4
19. Rosenfeld M, Allen J, Arets BH, et al. An official American Thoracic Society workshop report: optimal lung function tests for monitoring cystic fibrosis, bronchopulmonary dysplasia, and recurrent wheezing in children less than 6 years of age. Ann Am Thorac Soc. 2013;10:S1–S11. doi:10.1513/AnnalsATS.201301-017ST
20. Beydon N, Davis SD, Lombardi E, et al. An official American Thoracic Society/European Respiratory Society statement: pulmonary function testing in preschool children. Am J Respir Crit Care Med. 2007;175:1304–1345. doi:10.1164/rccm.200605-642ST
21. Oostveen E, MacLeod D, Lorino H, et al. The forced oscillation technique in clinical practice: methodology, recommendations and future developments. Eur Respir J. 2003;22:1026–1041.
22. Dencker M, Malmberg LP, Valind S, et al. Reference values for respiratory system impedance by using impulse oscillometry in children aged 2-11 years. Clin Physiol Funct Imaging. 2006;26:247–250. doi:10.1111/j.1475-097X.2006.00682.x
23. Nowowiejska B, Tomalak W, Radlinski J, et al. Transient reference values for impulse oscillometry for children aged 3-18 years. Pediatr Pulmonol. 2008;43:1193–1197. doi:10.1002/ppul.20926
24. Lai SH, Yao TC, Liao SL, et al. Reference value of impulse oscillometry in taiwanese preschool children. Pediatr Neonatol. 2015;56:165–170. doi:10.1016/j.pedneo.2014.09.002
25. Park JH, Yoon JW, Shin YH, et al. Reference values for respiratory system impedance using impulse oscillometry in healthy preschool children. Korean J Pediatr. 2011;54:64–68. doi:10.3345/kjp.2011.54.2.64
26. Lee JH, Haselkorn T, Borish L, et al. Risk factors associated with persistent airflow limitation in severe or difficult-to-treat asthma: insights from the TENOR study. Chest. 2007;132:1882–1889. doi:10.1378/chest.07-0713
27. Hagiwara S, Mochizuki H, Muramatsu R, et al. Reference values for Japanese children’s respiratory resistance using the LMS method. Allergol Int. 2014;63:113–119. doi:10.2332/allergolint.13-OA-0591
28. Shin YH, Jang SJ, Yoon JW, et al. Oscillometric and spirometric bronchodilator response in preschool children with and without asthma. Can Respir J. 2012;19:273–277. doi:10.1155/2012/560323
29. Nielsen KG, Bisgaard H. Discriminative capacity of bronchodilator response measured with three different lung function techniques in asthmatic and healthy children aged 2 to 5 years. Am J Respir Crit Care Med. 2001;164:554–559. doi:10.1164/ajrccm.164.4.2006119
30. Vu LT, Demoulin B, Nguyen MT, et al. Respiratory impedance and response to salbutamol in asthmatic Vietnamese children. Pediatr Pulmonol. 2010;45:380–386. doi:10.1002/ppul.21201
31. Delacourt C, Lorino H, Herve-Guillot M, et al. Use of the forced oscillation technique to assess airway obstruction and reversibility in children. Am J Respir Crit Care Med. 2000;161:730–736. doi:10.1164/ajrccm.161.3.9904081
32. Mazurek HK, Marchal F, Derelle J, et al. Specificity and sensitivity of respiratory impedance in assessing reversibility of airway obstruction in children. Chest. 1995;107:996–1002. doi:10.1378/chest.107.4.996
33. Klug B, Bisgaard H. Lung function and short-term outcome in young asthmatic children. Eur Respir J. 1999;14:1185–1189.
34. Hall GL, Sly PD, Fukushima T, et al. Respiratory function in healthy young children using forced oscillations. Thorax. 2007;62:521–526. doi:10.1136/thx.2006.067835
35. Amra B, Soltaninejad F, Golshan M. Respiratory resistance by impulse oscillometry in healthy Iranian children aged 5-19 years. Iran J Allergy Asthma Immunol. 2008;7:25–29. doi:07.01/ijaai.2529
36. Quanjer PH, Stanojevic S, Cole TJ, et al. Multi-ethnic reference values for spirometry for the 3-95-yr age range: the global lung function 2012 equations. Eur Respir J. 2012;40:1324–1343. doi:10.1183/09031936.00080312
37. Cruz JC. Mechanics of breathing in high altitude and sea level subjects. Respir Physiol. 1973;17:146–161.
38. Milic-Emily J, Kayser B. Mechanics of Breathing. In: Hornbein TSR, editor. High Altitude an Exploration of Human Adaptation. New York: Marcel Dekker, Inc.; 2001:175–198.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.