Back to Journals » Medical Devices: Evidence and Research » Volume 15
Improving Performance and Access to Difficult-to-Reach Anatomy with a Powered Articulating Stapler
Authors Huang ZF, Vandewalle JA ![]() , Clymer JW
, Clymer JW ![]() , Ricketts CD
, Ricketts CD ![]() , Petraiuolo WJ
, Petraiuolo WJ
Received 6 July 2022
Accepted for publication 23 August 2022
Published 2 September 2022 Volume 2022:15 Pages 329—339
DOI https://doi.org/10.2147/MDER.S379717
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Zhifan F Huang, James A Vandewalle, Jeffrey W Clymer, Crystal D Ricketts, William J Petraiuolo
Ethicon, Inc, Cincinnati, OH, USA
Correspondence: Jeffrey W Clymer, Ethicon, Inc, 4545 Creek Road, Cincinnati, OH, 45242, USA, Email [email protected]
Background: Modern surgical staplers should provide precise placement and transection, especially in tight spaces and on thick tissue. Ideally, a stapler would move to accommodate variations in the tissue and anatomy instead of having to move the tissue around to fit the stapler. This study was undertaken to evaluate the performance characteristics of the new Echelon 3000 Stapler (ECH3). Use of the ECH3 was compared to another marketed stapler, including tests for access, seal strength, staple formation in thick tissue, and end effector stability.
Methods: Pelvic anatomy measurements were used to construct a virtual model of a Low Anterior Resection (LAR). Monte Carlo simulations were performed on the staplers to compare the probability of completing a transection with one or two firings. Using water infusion of stapled porcine ileum, pressure at first leak and percentage of leaks at critical pressures were measured. Rate of malformed staples was measured in thick tissue. End effector stability while firing and under moderate pressure were compared between staplers. After use, surgeons were surveyed on the functionality of the device.
Results: ECH3 had a markedly higher probability of completing an LAR transection in one or two firings than the comparator stapler. Median initial leak pressure of stapled ileum was significantly higher, and rate of leaks was lower at 40 and 50 mmHg. ECH3 had fewer malformed staples for both 3.3- and 4.0-mm thick tissue. The end effector exhibited less angular movement during firing, and less deflection under a moderate load. Surgeons agreed the ECH3 provided precise placement and easy one-handed operation.
Conclusion: The Echelon 3000 Stapler demonstrated improved access capability, tighter seals, fewer malformed staples, and greater end effector stability. These advantages were recognized by surgeons who evaluated the use of the device preclinically.
Keywords: stapler, access, pelvis, maneuverability, powered articulation
Introduction
Increasingly complex procedures leave very little margin for error when using surgical staplers. Technological advances in surgical staplers have provided surgeons improved utility and functionality to enhance surgical care. Desired features of a surgical stapler include the ability to have precise placement and transection, especially in tight spaces and on thick tissue. Ideally, a stapler would move to accommodate variations in the tissue instead of having to move the tissue around to fit the stapler.
Fragile and variable levels of tissue thickness in patients can lead to tissue movement between the jaws of a stapler affecting the results of an intended transection. The tissue movement during firing may disrupt the integrity of the staple line, which can result in exposed tissue layers, malformed formed staples, and need for extra firings. Staple line failure can result in significant postoperative morbidity in the case of anastomotic leak or staple line bleeding. The most common problems associated with staplers, include failure to fire, malformed staples and handle lockup, that can lead to complications such as bleeding or leaks.1
The development of articulated staplers to facilitate the division of vessels and tissue deep in transection planes such as the pelvis has been useful.2,3 Maneuverability of surgical staplers into a precise position has been shown to allow a surgeon to reduce operation time due to making fine stapling position adjustments without having to remove the stapler.4
Another important feature to a surgical stapler is how wide the jaw opens. The jaw aperture needs to be wide enough to grasp or hold thick tissue. If the jaw on a stapler does not open wide enough, the stapler is unable to divide and staple thick tissue, potentially increasing the risk for inadequate staple formation with stressing or tearing of tissues.5 A wider jaw aperture can help place tissue more easily in the jaws with less manipulation of the tissue and can enable more full transections in cases where there is a desire not to force fragile tissue into the jaws past what a smaller opening would allow.
Recently, a new surgical stapler has been designed for one-handed use with improved control and access by incorporating powered continuous articulation, a wider articulation angle, and a larger jaw aperture. This study was undertaken to evaluate the performance characteristics of the Echelon 3000 Stapler (Figure 1) in bench top models. Test measures included access comparison, leak testing, staple formation in thick tissue, and end effector stability in comparison to another marketed stapler.
 |
Figure 1 The Echelon 3000 Stapler. |
Methods
Devices used in this study were the Echelon 3000 Stapler (ECH3, Model No. ECH60S/ECH45S, Ethicon, Inc., Cincinnati, OH), and Signia™ Powered Stapler with Tri-Staple Technology (SGN, Model No. EGIA60AMT, Medtronic, Fridley, MN).
Pelvic Anatomy Measurements: Anatomical measurements were derived from an earlier study6 based on Pelvic Computed Tomography and Magnetic Resonance Imaging of cadavers. Scans from 9 males with heights and weights representative of the 50th percentile were converted to 3-dimensional stereolithography files with colon and pelvic structures isolated. The subjects were in the range of 60 ± 16 years, height 175 ± 4 cm, and weight 81 ± 5 kg. The measurements obtained were similar to an independent study.7 Male patients were used because the narrowness of their pelvis creates a more challenging Low Anterior Resection (LAR) procedure than for a female patient. Pelvic anatomy of the female is round-shaped, larger, and wider, compared to the male pelvis that is heart-shaped, longer, and narrower.8
Access Comparison: The difficulty of performing procedures in the pelvis was examined via an analysis of factors affecting the outcomes of a total mesorectal excision. Both operative time and morbidity have been found to be dependent upon BMI, tumor distance from the anal verge, tumor depth and pelvic outlet.7
Predictive modeling of LAR transection was performed using virtual ECH3 and SGN staplers in the pelvic model (Figure 2). Comparisons were made on the perpendicularity of the cutline and the possibility of one or two firings completely dissecting the colon with the surgical procedure conducted at different distances above the dentate line. Optimally, when performing LAR procedures, surgeons strive to maximize the perpendicularity to the rectum, and minimize the number of firings (one firing is preferred, but no more than two).9
 |
Figure 2 Virtual placement of the stapler within the pelvis at a specific distance above the dentate line. |
The geometries of the surgical staplers’ end effectors were placed virtually within the median scan of the 9 males. The ability of the device to completely transect the colon was determined from optimal placement at each location above the dentate line given the geometry and articulation angle constraints of the devices using a 10,000-round Monte Carlo simulation.
In the simulation, rectum width and tension factor were determined via the cadaver study; angle from perpendicular and depth of device in pelvis were derived from the CT/MRI model; and device cut line length and tissue flow factor were measured from physical testing. The tissue flow factor is defined as the ratio of the longitudinal tissue flow upon stapler closure for the test stapler compared to the control stapler. The tension factor, cut line length and flow factor were assumed to be normally distributed, rectum width to be lognormally distributed, and angle from the perpendicular to follow a triangular distribution.
During device placement within the pelvic scans, placement location and shaft angle were held constant across each device. The port was placed on the abdominal wall at the iliac crest on the patient’s right side. To simulate an actual LAR procedure, the rectum model was placed at an angle within the pelvic scan. The device was placed at the target location above the dentate line. The pelvic bowl is lined with soft tissue that has some level of pliability, so a certain amount of interference, equivalent across devices, was permitted during placement.
Each device was evaluated at four different depths in the pelvic bowl: 5, 7, 9 and 11 cm from the dentate line, in correspondence with the predetermined thickness and width of the rectum. Results are provided at 7 cm from the dentate line, since this is likely the lowest location at which a 60-cm device can be used. During evaluation, shaft articulation angle did not exceed maximum capability of the device, and the end effector was positioned as perpendicularly as possible within the colon model. Once the positioning of the end effector was optimized, the angle of the end effector relative to the colon was measured.
The number of firings was calculated as:

The cutting distance was calculated as:

Results of the modeling were consistent with a study in LAR that found 50% of transections could be completed with a single firing.10
Leak Testing: Comparisons were made between the ECH3 and SGN for the pressure at which first leak occurred as fluid pressure was ramped up in sealed ileum. Staple firings were performed longitudinally on ex vivo porcine ileum of a selected tissue thickness range (1.75–2.25mm). The proximal end of the staple line was attached to a barbed Luer lock fitting and securely tied with a suture. The distal end was tied off with a suture. A computer-controlled pressure ramp-up rate of 30 mmHg/minute was utilized with dyed room-temperature water. Leaks were visually identified as originating from the staple line or the cut line. If a staple line leak occurred, testing was continued until there was a cut line leak. Statistical comparisons were performed at 30 through 60 mmHg via Fisher’s exact test.11,12
Staple Form in Thick Tissue: Comparisons of staple form were made between ECH3 60mm with Green (for thick tissue, closed staple height 2.0 mm) and Black (for extra thick tissue, 2.3 mm) reloads and SGN 60 mm with Purple (for medium/thick tissue, 1.5–2.25 mm) or Black (for extra thick tissue, 2.25–3.0 mm) reloads. Evaluations were performed on the percentage of malformed staples according to Staple Form Quality (SFQ 3–5).11 Stapling was performed on porcine stomach of target tissue thickness of 3.3 mm (Green/Purple) and 4.0 mm (Black). Statistical comparisons were made via Fisher’s exact test for percentage of malformed staples.
Closure and Firing Tissue Pressure: ECH3 with GST60B and GST60G cartridges was compared to SGN with EGIA60AMT cartridge under thick tissue conditions for tissue compression during clamping and firing of porcine gastric tissue. Comparisons were performed for uniformity and peak compression pressure. Thick tissue conditions were 2.5 ± 0.1 mm for GST60B and 3.3 ± 0.1 mm for GST60G. Twelve firings were performed for each device.
The tissue compression pressures were measured on the cartridge side, which is generally higher than the anvil side. The sensor was placed at the distal end of 6th row of staples. The tissue at this point has the full history from closure to firing. The tissue beyond this point has the history of closure and firing up to the stop of the knife. The knife stop position was set at 35 mm, ie, just over half the length of the cartridge. Staples were removed at the 7–9th positions for placement of the Tekscan sensor (Tekscan, Inc., South Boston, MA). After clamping, the tissue was held in the jaws for 15 seconds prior to firing. Firing speed was set at 12mm/s. Compression pressure was monitored until the knife was stopped at the 35mm mark. Statistical comparisons were made via Student’s t-test or Mann–Whitney for non-normally distributed data.
Tissue Grasping: Tissue grasping force was compared between ECH3 with GST60B reloads and SGN with EGIA60AMT reloads via clamping on 1.5 ± 0.3 mm thick target porcine colon tissue, cut to a length of 90 ± 5 mm. The grasping force was measured as the tissue was pulled out of the jaw, and the peak force as monitored by a 20-lbf load cell was reported as the grasping force. Tissue was grasped in the full jaw with the edge of the tissue touching the tissue stop of the jaw. Statistical comparisons were made via the Mann–Whitney test.
Shaft Stiffness: Shaft stiffness was compared between ECH3-60mm and SGN-60mm. Controlled lateral and vertical forces were applied in the middle of the jaw separately to simulate tissue manipulation forces, and the total lateral and vertical deflection of the shaft was measured. Shaft stiffness in the lateral and vertical directions was calculated from load-deflection curves. The shaft lateral and vertical stiffnesses were measured in both directions since devices were not necessarily designed to be symmetric.
A load of 1.0 lbf (4.45 N), which is considered to be a moderate manipulation force, was applied to the shaft in four directions; up, down, left, and right. For lateral forces, the joint de-articulation stiffness was included in the shaft deflection. For vertical forces, the joint vertical stiffness was included in the shaft deflection. Forces were applied to the middle of the jaw (30mm point). Statistical comparisons were made via Student’s t-test or Mann–Whitney for non-normally distributed data.
End Effector Stability: End Effector stability during firing of ECH3-60mm devices with Green or White (for vascular/thin tissue, closed staple height 1.0 mm) reloads was compared with SGN with Medium/Thick and Vascular/Medium reloads. Four devices were applied on thick tissue thickness (3.3mm) and another four on vascular tissue. Each device was fired seven times over a range of articulation angles in a bespoke fixture. Maximum angle change of the articulation angle was determined during the firing. Statistical comparisons were made via Student’s t-test or Mann–Whitney for non-normally distributed data.
Surgeon Evaluation: To evaluate the usability of the ECH3, a panel of surgeons performed simulated surgical procedures on a bench top trainer with harvested tissues. Thoracic surgeons performed a pulmonary artery transection, bronchus transection and a lung parenchyma transection. Upper GI (Bariatric, Gastric, General) surgeons performed a gastric transection and a Roux-en-Y transection. Lower GI (Colorectal, General) surgeons did an LAR transection and a jejunum-to-jejunum anastomosis transection.
Following the simulated procedures, participants answered a series of assessment questions related to the operation of the device, the placement of the device on tissue and difficulty accessing and manipulating the tissue compared to the device each participant currently uses. All participants had the opportunity to review the instructions for use prior to beginning their tasks.
Each study participant signed a consent form prior to the evaluation and interview. No procedures were performed on humans or live animals. Because this was a non-interventional study (ie, a survey), ethical approval was not required.
Results
Via metrology, ECH3 had a wider angle of articulation, larger aperture and longer joint length (Table 1). Articulation span of ECH3 is 24–27% greater than SGN, and jaw aperture is 39–57% greater. To provide the greater articulation span and jaw aperture, the joint length of ECH3 is slightly larger than SGN. Placement for lower anterior resection is feasible for both staplers.
 |
Table 1 Comparisons of ECH3 and SNG |
Access and Probability of Complete Transection: At 7 cm above the dentate line, the ECH3 60mm device had a 30% higher chance to complete a transection with one firing than SGN 60mm, while ECH3 45mm device had 2.4 times the chance as SGN 45mm (Figure 3). ECH3 devices had similar perpendicularity angles to the corresponding SGN devices, similar or longer cutline lengths and significantly less longitudinal tissue flow upon closure.
 |
Figure 3 Probability of completing transection at 7 cm above the dentate line for one and two firings. |
Leak Pressure: ECH3 exhibited a 25% greater median pressure at first leak than SGN (p = 0.014) (Figure 4). ECH3 had 88% fewer leaks below 40 mmHg (p = 0.013) and 67% fewer leaks below 50 mmHg (p = 0.023).
 |
Figure 4 Pressure at first leak cumulative failure plot for ECH3 and SGN with index lines for 50% failure. |
Staple Form: ECH3 produced 95% fewer malformed staples in 3.3 mm thick tissue and 72% fewer malformed staples in 4.0 mm thick tissue (p < 0.001 for both).
Closure and Firing Tissue Pressure: At both thicknesses, 2.5 and 3.3 mm, ECH3 had higher closure pressures than SGN, and lower firing pressures. Hence, there was less difference between closure and firing pressures for ECH3 compared to SNG, providing more uniform compression throughout the application.
Grasping Force: Average peak grasping force on 1.5mm porcine tissue was approximately two times higher for ECH3 compared to SGN.
Shaft Stiffness: Deflection of the shaft under a 1.0 lbf (4.45 N) force was greater for SGN than ECH3 both vertically and horizontally (Figure 5). In particular, deflection in the rightwards direction was over eight times greater for SGN than ECH3.
 |
Figure 5 Deflection of shaft under a 1.0 lbf (4.45 N) load. |
End Effector Control: In end effector stability testing, ECH3 display 79% less angular movement than SGN in thick tissue and 93% less movement on vessels (Figure 6).
 |
Figure 6 End effector stability of ECH3 and SGN for vascular and thick tissue. |
A total of 45 surgeons participated in the survey. Surgeons represented the areas of thoracic, bariatric, colorectal, and general surgery. Summarized results of the questionnaires are given in Table 2. Throughout the three categories of precise placement, one-handed operation and overall, surgeons agreed significantly more often than disagreed with every benefit statement. There were no dissenting opinions on the value of a larger jaw aperture or greater articulation angle of the ECH3.
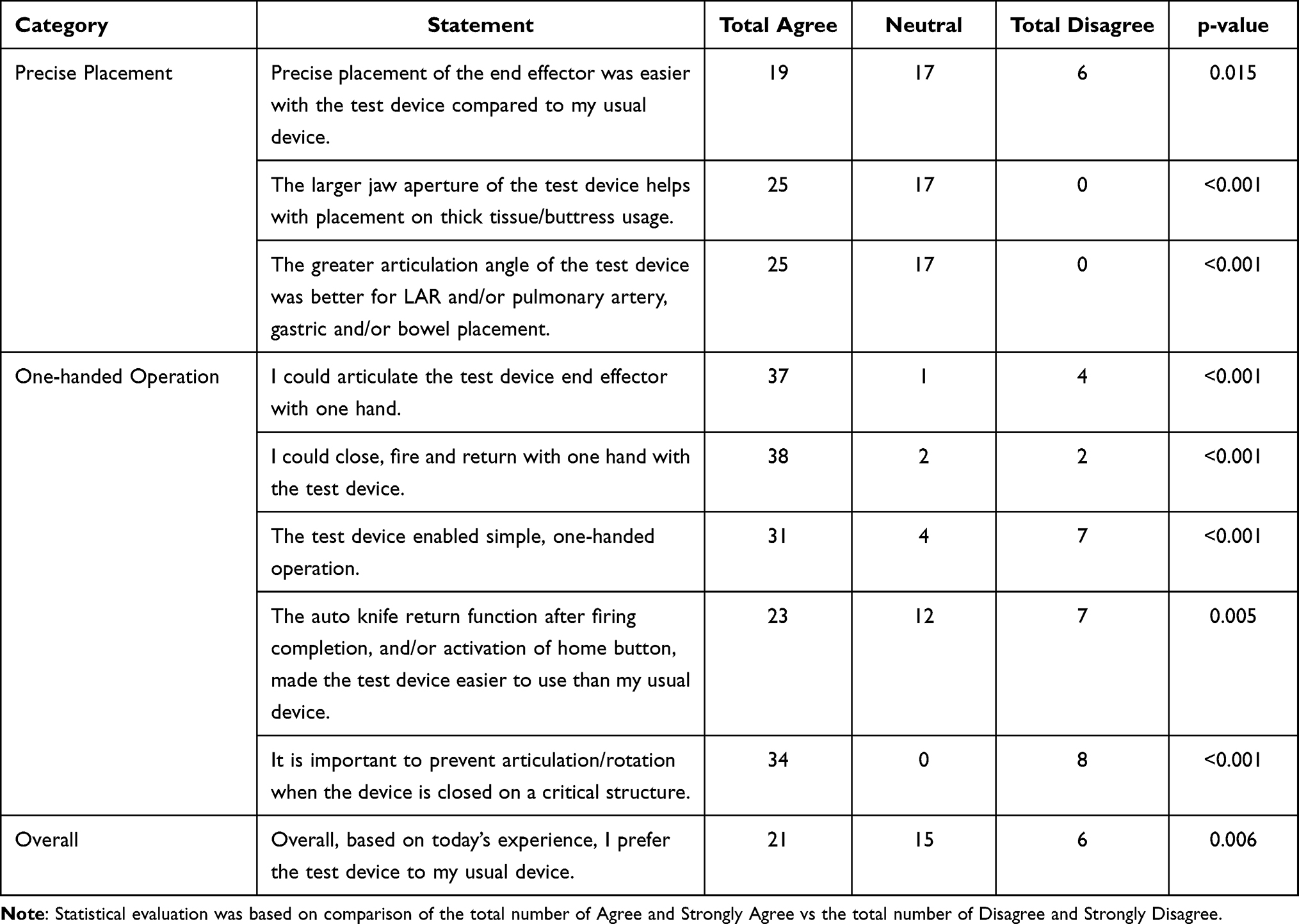 |
Table 2 Summary of Results from the Surgeon Questionnaire on the Echelon 3000 Stapler |
Discussion
Surgical staplers have become an indispensable tool in minimally invasive procedures. As technology has enabled their miniaturization, the use of staplers has been integral in the advancement of laparoscopic procedures, which provide multiple benefits over conventional open surgery.13 However, there are a number of challenges with the use of staplers in laparoscopic procedures that need to be addressed either in the design of the stapler or by its application by the surgeon.14
With open surgery, the surgeon has tactile access to the tissue and a relatively wide field, with few restrictions on the design of instrument. In laparoscopy, a stapler is necessarily limited in size in order to fit through a trocar, and compression of the staples must take place perpendicularly to the shaft axis. Because of this mechanical disadvantage, laparoscopic staplers must be designed to adapt to variable viscoelasticity within different tissues. One approach to meet these challenges is the use of powered firing, which provides the surgeon with exquisite control of the speed and strength of staple formation independent of the positioning of the device.
Previous to ECH3, the ECHELON FLEX™ Powered Plus stapler was designed to address many of the challenges that minimally invasive surgery introduced.15 With this device, dynamic firing allows the motor to slow the firing speed when the device engages thicker tissue. A refined anvil curvature as well as wider, tapered staple pockets helped to improve the capture and formation of the staples when the device is fired.
The new stapler evaluated in the current study incorporates the advances of the previous version and adds several features to improve its utility and functionality. The Echelon 3000 Stapler is designed to deliver improved access and precision with a greater articulating range and jaw aperture. Via proprietary software, ECH3 has simple haptic and audible device feedback. Articulation adjustments can be made by 1° increments, articulation can be performed with the jaws partially closed, and the left or right articulation buttons always move the end effector in the same direction even when the jaws are rotated upside down due to the inclusion of an orientation sensor.
The joint length of ECH3 (distance from the shaft pivot point to first staple) is reduced compared to the previous version and similar to SGN. This change enables a tighter/smaller turning radius in constrained conditions. In post-use surveys, surgeons agreed that the operation (placement and transection, articulation, rotation, closure, firing and opening) of ECH3 could easily be performed with one hand.
Colorectal surgeons try to minimize the number of firings when performing lower anterior resection (LAR), due to anastomotic leak factors.16,17 For restorative rectal resection, the odds ratio for anastomotic leakage was 2.71 (95% CI 1.17–6.26) when three or more firings were used.9 The greater likelihood of a single transection increases surgical efficiency that may result in reduced risks of complications caused by crossing staple lines.18
In a virtual surgery model, the ECH3 stapler was more likely to complete an LAR transection both within one and two firings compared to another marketed stapler. The three key factors in determining the number of firings are considered to be access perpendicularity, tissue flow (milking) during compression and cutline length. ECH3 achieved similar perpendicularity to SGN but had both reduced tissue flow and slightly greater cutline length. Fewer firings observed for ECH3 may be due primarily to superior tissue manipulation from Gripping Surface Technology, which limits milking during compression.
ECH3 showed higher pressures at first leak and a lower rate of leakage in the critical range between 30 and 60 mmHg.12 This may be due in part to fewer malformed staples that can compromise the integrity of the staple line and raise the risk of unexpected complications.19 The staple form for ECH3 showed fewer malformed staples both in medium and thick tissue compared to a competitive brand. Properly formed staples in laparoscopy are difficult, especially in thick tissue.14 The improved anvil and dynamic firing speed may result in improved staple form, as has been confirmed in recent studies on similar devices.15,20
In grasping the tissue, it is important that the stapler applies a consistent pressure to the tissue to achieve optimum staple formation and prevent the tissue from “milking” out of the end effector. The ECH3 Gripping Surface Technology (GST) consisting of indentations in the cartridge surface is designed to increase the ability of the stapler to grasp tissue.21–24 Manipulation of the tissue will also be aided by a robust shaft that does not deflect under moderate pressure. In this study, the ECH3 had a more uniform compression, stronger grasping force and a stiffer shaft than a competitive stapler. All these qualities help explain why the ECH3 provides greater stability of the end effector and improved access to the target tissue.
The Echelon 3000 Stapler design includes an adjustable powered articulation, a greater articulating range and wider jaw aperture. In this study, improved access capability, stronger seals, fewer malformed staples, greater grasping force and end effector stability were demonstrated. These advantages were recognized by surgeons who evaluated the use of the device preclinically. Clinical studies are needed to determine if the new features of this device confer significant patient benefits.
Disclosure
All authors are employees of Ethicon, Inc., the manufacturer of the Echelon 3000 Stapler. The authors report no other conflicts of interest in this work.
References
1. Clapp B, Schrodt A, Ahmad M., et al. Stapler malfunctions in bariatric surgery: an analysis of the MAUDE database. JSLS. 2022;26(1):
2. Gonzalez-Rivas D, Fieira E, Delgado M, Mendez L, Fernandez R, de la Torre M. Uniportal video-assisted thoracoscopic lobectomy. J Thorac Dis. 2013;5(Suppl 3):S234. doi:10.3978/j.issn.2072-1439.2013.07.30
3. Karabicak I, Karabulut K, Yuruker S, Kesicioglu T, Ozen N. Single-port laparoscopic liver resection: largest Turkish experience. Indian J Surg. 2017;79(2):111–115. doi:10.1007/s12262-015-1435-0
4. Shimada Y, Maehara S, Osawa J, Hagiwara M, Ohira T, Ikeda N. Powered articulation by the SigniaTM stapling system for stapling position adjustments: optimizing safe surgical margins in thoracoscopic sublobar resection. Surg Today. 2021;51(3):447–451. doi:10.1007/s00595-020-02109-0
5. Yamada S, Yoshino K, Inoue H. Resection and stapling technique for wide-based giant bullae in video-assisted thoracic surgery using a new end-stapler. Gen Thorac Cardiovasc Surg. 2008;56(6):306–308. doi:10.1007/s11748-008-0226-y
6. Saffarzadeh M, Eckert CE, Nagle D, et al. Pelvic and lower gastrointestinal tract anatomical characterization of the average male. Surg Innov. 2019;26(2):180–191. doi:10.1177/1553350618812317
7. Akiyoshi T, Kuroyanagi H, Oya M, et al. Factors affecting the difficulty of laparoscopic total mesorectal excision with double stapling technique anastomosis for low rectal cancer. Surgery. 2009;146(3):483–489. doi:10.1016/j.surg.2009.03.030
8. Leong A. Sexual dimorphism of the pelvic architecture: a struggling response to destructive and parsimonious forces by natural & mate selection. MJM. 2006;9(1):61.
9. Damgaard Eriksen J, Emmertsen KJ, Madsen AH, Erichsen R, Bachmann TN, Hjerrild Iversen L. The impact of multiple firings on the risk of anastomotic leakage after minimally invasive restorative rectal cancer resection and the impact of anastomotic leakage on long-term survival: a population-based study. Int J Colorectal Dis. 2022;1–14. doi:10.1007/s00384-021-04040-3
10. Yamamoto S, Fujita S, Akasu T, Inada R, Moriya Y. Risk factors for anastomotic leakage after laparoscopic surgery for rectal cancer using a stapling technique. Surg Laparosc Endosc Percutan Tech. 2012;22(3):239–243. doi:10.1097/SLE.0b013e31824fbb56
11. Henninger DD, Jones J, Clymer JW. Tighter formed staples produce stronger sealing against luminal leakage. Med Dev Diagn Eng. 2017;2:48–51.
12. Rojatkar P, Henderson CE, Hall S, et al. A novel powered circular stapler designed for creating secure anastomoses. Med Devices Diagn Eng. 2017;2(2):94–100. doi:10.15761/MDDE.1000123
13. Gaidry AD, Tremblay L, Nakayama D, Ignacio JRC. The history of surgical staplers: a combination of Hungarian, Russian, and American innovation. Am Surg. 2019;85(6):563–566. doi:10.1177/000313481908500617
14. Harris JL, Eckert CE, Clymer JW, Petraiuolo WJ. The viscoelastic behavior of soft tissues must be accounted for in stapler design and surgeon technique. Surg Technol Int. 2022;40:
15. Wise A, Rector J, Orr K, Singleton DW, Ricketts CD. Measuring staple line security and compression uniformity with an advanced endoscopic powered stapler. J Surg. 2021;7(2):1–5.
16. Toh J, Peirce C, Tou S, Chouhan H, Pfeffer F, Kim S. Robotic low anterior resection: how to maximise success in difficult surgery. Tech Coloproctol. 2020;24(7):747–755. doi:10.1007/s10151-020-02227-4
17. Otsuka K, Kimura T, Matsuo T, et al. Laparoscopic low anterior resection with two planned stapler fires. J Soc Laparoendosc Surg. 2019;23(1):
18. Silecchia G, Iossa A. Complications of staple line and anastomoses following laparoscopic bariatric surgery. Ann Gastroenterol. 2018;31(1):56. doi:10.20524/aog.2017.0201
19. DiChiacchio L, O’Neill NA, Kligman M, Bafford AC. Postoperative small bowel obstruction secondary to single malformed staple following laparoscopic total abdominal colectomy. J Surg Case Rep. 2020;2020(10):rjaa361. doi:10.1093/jscr/rjaa361
20. Kimura M, Terashita Y. Superior staple formation with powered stapling devices. Surg Obes Relat Dis. 2016;12(3):668–672. doi:10.1016/j.soard.2015.11.023
21. Kimura M, Tanaka H, Hato M, et al. Evaluation of a new stapler with unique surface gripping technology. J Adv Med Med Res. 2016;18:1–6.
22. Park SY, Kim DJ, Mo Nam C, et al. Clinical and economic benefits associated with the use of powered and tissue-specific endoscopic staplers among the patients undergoing thoracoscopic lobectomy for lung cancer. J Med Econ. 2019;22(12):1274–1280. doi:10.1080/13696998.2019.1634081
23. Rawlins L, Johnson BH, Johnston SS, et al. Comparative effectiveness assessment of two powered surgical stapling platforms in laparoscopic sleeve gastrectomy: a retrospective matched study. Med Devices. 2020;13:195.
24. Yeo E, Thompson J, Hanseman D, et al. Increased staple loading pressures and reduced staple heights in laparoscopic sleeve gastrectomy reduce intraoperative bleeding. Surgery. 2021;169(5):1110–1115. doi:10.1016/j.surg.2020.10.045
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.