Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Improving Nursing Students’ Medication Safety Knowledge and Skills on Using the 4C/ID Learning Model
Authors Musharyanti L ![]() , Haryanti F, Claramita M
, Haryanti F, Claramita M ![]()
Received 25 November 2020
Accepted for publication 15 January 2021
Published 5 February 2021 Volume 2021:14 Pages 287—295
DOI https://doi.org/10.2147/JMDH.S293917
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Lisa Musharyanti,1 Fitri Haryanti,2 Mora Claramita3
1School of Nursing, Faculty of Medicine and Health Sciences, Universitas Muhammadiyah Yogyakarta, Yogyakarta, Indonesia; 2Department of Pediatric and Maternity Nursing, Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia; 3Department of Medical, Health Professions Education and Bioethics, Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia
Correspondence: Lisa Musharyanti
School of Nursing, Faculty of Medicine and Health Sciences, Universitas Muhammadiyah Yogyakarta, Jalan Brawijaya, Tamantirto, Kasihan, Bantul, Yogyakarta, Indonesia
Tel +62 81252126958
Email [email protected]
Introduction: Learning medication-safety has become a focus in many countries to improve medication-safety competencies in nursing students. Research on instructional design for medication-safety is still limited, especially about the use of the Four Components Instructional Design (4C/ID) model. This study aimed to compare the knowledge and skills in medication safety of nursing students after the medication-safety training using four components of instructional design known as 4C/ID.
Methods: This was a posttest-only quasi-experimental study using an intervention and control group. The participants were the third-semester students of a nursing school at Yogyakarta, Indonesia (intervention: n=55, control: n=40). The intervention group was trained for five weeks using the 4C/ID approach with interactive lectures, small group discussions, reflections, and skills simulation sessions. An observational skills evaluation and Multiple-Choice Questionnaire were administered in the last week after the training completed. Independent sample t-test and Mann Whitney tests were used to analyze the mean differences of knowledge and skills in giving oral medicine and drug injections between the two groups.
Results: The majority of respondents were female (74.1%), aged 19– 20 years (77.8%), with GPA > 3 (87.37%) and, the majority had never received instruction about patient safety (69%). There were significant mean differences in overall knowledge (p< 0.05) and also in the skills of oral drug and intramuscular drug administration (p< 0.05) between the intervention and control groups.
Conclusion: Training in medication-safety using the 4C/ID approach could improve the medication-safety knowledge and skills of the nursing students based on simple to complex learning.
Keywords: 4C/ID model, medication-safety, nursing students’ education and training
Introduction
The ability of nurses to administer drugs safely will determine the quality of service and support patient safety.1 Nurses are also the health profession, which is often considered as the last barrier in preventing medication errors to patients.2 The ability of nurses in the safe management and administration of drugs is one of the competencies that are expected to be applied in nursing care, especially in inpatient settings. Studies show that the lack of nurses’ ability to safely administer drugs will endanger patients and trigger adverse drug events.3
The lack of the quantity and quality of medication-safety during undergraduate nursing education is the main cause of the lack of ability to administer the medication safely for the patient care.3–5 In some developing countries, knowledge about medication safety has not been given on an ongoing basis curriculum and is lake of reflection in the real cases that occur in health services. Some nursing institutions may only provide pharmacological knowledge at the beginning of the year without linking this competence to the issue of patient safety.3,6
A systematic review showed that several efforts have been made to better prepare medical, nursing, and pharmacy students about medication safety by piloting various learning methods.7 However those researches were mostly coming from developed countries.8,9 Research about medication safety are important to be done in developing country because the incidence of medication error are higher in developing countries.10
Other studies have used a variety of learning methods in delivering patient safety and medication-safety to nursing students. However, research about medication safety in the nursing area was still limited compared to studies in medicine.7,8 Several studies are more focused on applying student-centered learning methods such as Problem Based Learning (PBL), case study, simulation, as methods to teach medication-safety.11 Nevertheless, the research about instructional design is still limited.7
In response to the limited research in the area of medication-safety from developing countries, in nursing education, which also highlights the use of different instructional designs in the curriculum, we aimed to fill the gap by developing and piloting a medication-safety course using the 4C/ID curriculum model in Indonesia. 4C/ID is an instructional model developed by Van Merriënboer.12 The 4C/ID model offers solutions for instructional design that are suitable for designing a course, block or module which aims to achieve complex capabilities. 4C/ID can consist of task-oriented classes with the main components, namely learning-tasks, supportive-information, procedural-information, and part-task practice.
Learning-tasks are the backbone of the 4C/ID model. Students are given learning-tasks which serve as the means for students to build their knowledge. To help students connect between the learning-tasks and the knowledge they already have, supportive-information is given to the students. The other components of 4C/ID are procedural-information and part-task practice. Procedural-information is used for routine tasks or tasks which require repetition. Procedural-information can be in the form of specific feedback and can be given before, while, and after students practice the task. The last component of 4C/ID is part-task practice, which is used to help students to achieve automation.12,13
Some previous studies that used the 4C/ID approach were in electronic engineering learning,14 pharmacotherapy learning, physiotherapy courses,15 urology learning16 and one in communication learning for nurses.17 The last study was intended for professional nurses but not focused on medication-safety. Our study was designed to improve nursing students’ comprehension in the application of medication-safety using 4C/ID instructional design.
This paper aimed to compare the knowledge and skills in medication-safety specifically for oral and intramuscular drug administration, between nursing students in the intervention and the control group.
Methods
Setting of the Study
Based on the core curriculum of undergraduate nursing in Indonesia, the topic of patient safety is covered in the second year of the program.18 Some topics included were adopted from Multi-Professional Patient Safety Curriculum Guide of World Health Organization (WHO).19 However, the implementation of this curriculum has not yet been optimal because patient safety learning is in the form of lectures instead of student-centered methods.
The skills for administering drugs are taught in the second semester. However, there is still little effort to link the skills of administering these drugs to the principles of patient safety in these skills. This gap in the curriculum makes it arduous for students to comprehend the application of safe administration of drugs, which influences their confidence and preparedness to administer safe drugs during their clinical rotation at the hospital.
Study Design
This study was a posttest quasi-experimental only with non-equivalent randomized control group design.20 Total sampling was used in this study and respondents were 106 students (Respon Rate= 89.65%). The intervention was the 4C/ID learning approach to medication-safety. Figure 1 illustrates the procedures of this study.
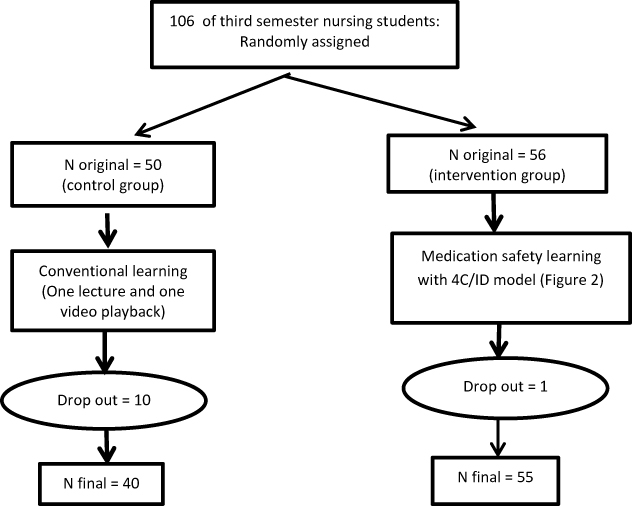 |
Figure 1 The procedures of this posttest-only quasi-experimental study. |
Participants
The respondents involved in the study were third-semester nursing students of a nursing school in Yogyakarta, Indonesia. The inclusion criteria were: 1) the students in the third semester who had learned drug administration skills, and 2) the students who have undergone early clinical exposure in health care facilities. The exclusion criteria were the students who were not attending the entire training. Table 1 shows the characteristics of the samples.
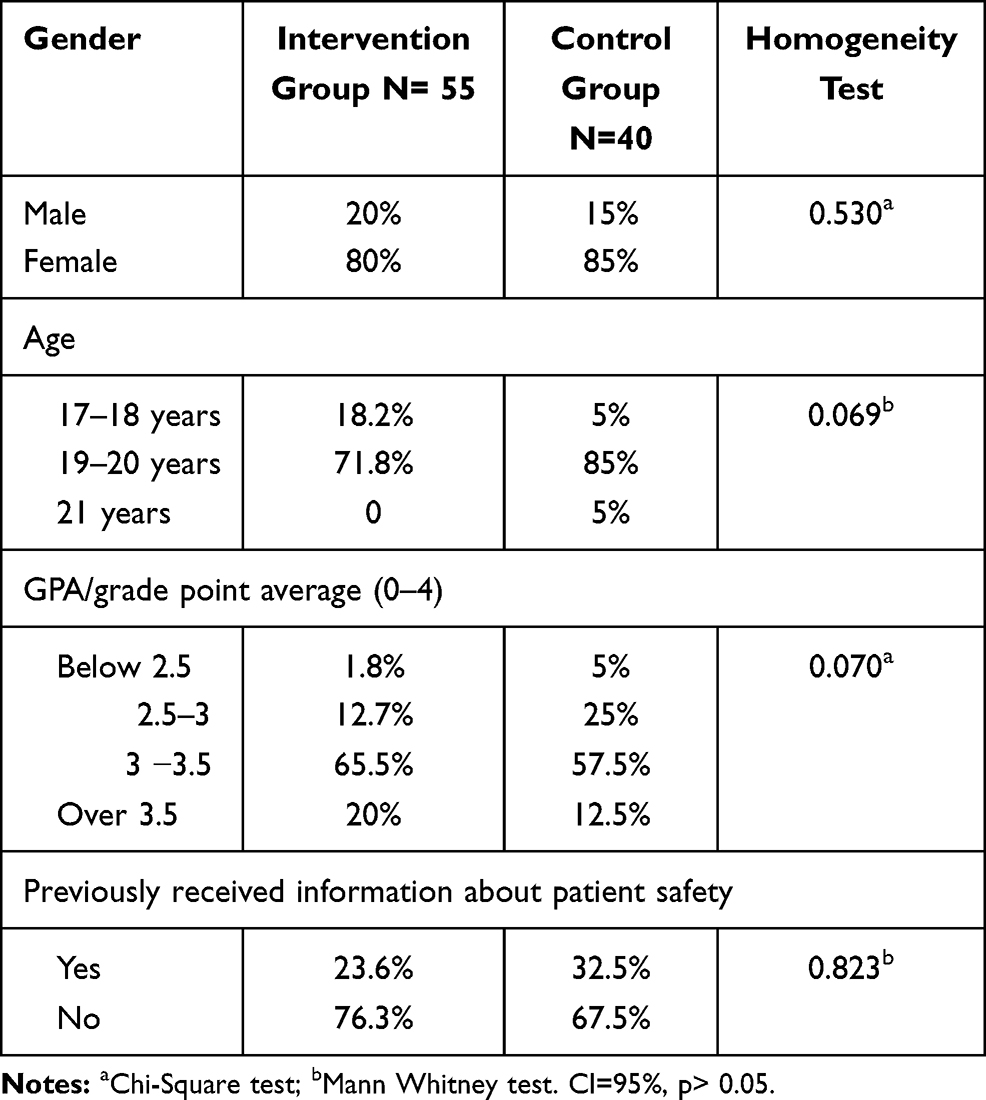 |
Table 1 Characteristics of Participants |
Instruments
Three assessment instruments used in this study were a set of Multiple-Choice Questionnaires (MCQ) and two checklists. The MCQ was used to assess student knowledge at the end of the course. The MCQ test was developed by the experts who are instructors in the courses and they made the sixty MCQ questions based on the blueprint of the learning outcomes. The blueprint were consist of aspect the patient safety and medication safety concept, the medication administration cycle in the health care, high alert medication, and the role of nurse in medication administration. Then, the questions were reviewed and revised until ready to be used for the post-test. We also do the item analysis to check the composition of difficulties questions dan medium difficulties. The MCQ questions that used were fifty number.
The instrument of skills competency includes a checklist for assessing oral medicine administration skills and a checklist for evaluating intramuscular injection skills. The two checklists used were developed from the checklists which are used in the school of nursing. First, we decided about the medication-safety and patient safety aspects which have to be included in the checklists. Then, we revised the checklists based on literature about medication-safety skills and also conducted expert consultation. We integrated the principles of patient safety and medication-safety into the checklists, and consulted with three experts. We did an interrater reliability test for the checklist items with two observers and the percent agreement of each item ranged from 77.78–100%.
The checklists contain 10 dimensions which were: patient safety application, patient identification, drug accuracy, infection control, risk of falling prevention, drug preparation, drug administration, drug monitoring, documentation, and the aspects of empathy, communicative and respectfulness.
Procedures
Respondents were divided randomly by lottery number into two groups of the intervention group (N: 56) and control group (N: 50). We overestimated the number of intervention groups to anticipate the withdrawal of participants. The intervention activity lasted for 18 hours over 5 weeks for the intervention group including the post-test session. The intervention consisted of an overview activity, then training was provided with a 4C/ID approach. Several activities that have functioned as learning- task in 4C/ID model include: real case presentation, small group discussion, reflection, and simulation of delivering oral and intramuscular medicine. Some supportive-information was given to the students in the form of interactive lecture and video playback. Procedural-information that we used involved a checklist of procedural skills that consisted of lists of oral drug administration and intramuscular drug administration. Feedback was also given by the facilitators that functioned as procedural-information during the classical session and simulation in the skills laboratory. Figure 2 illustrates the 4C/ID approach in this study.
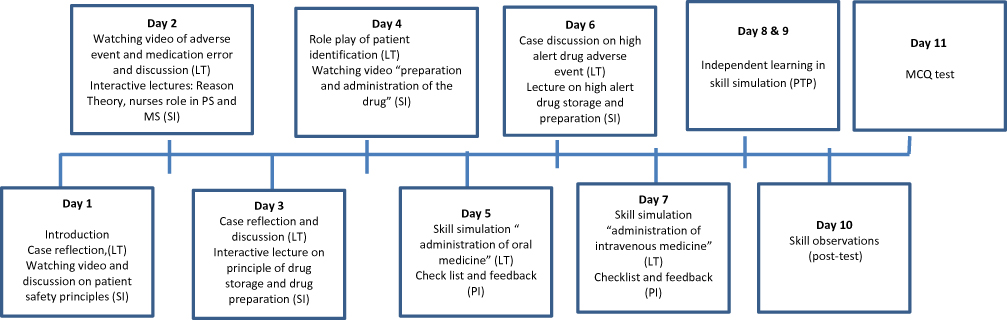 |
Figure 2 The process of medication safety course using 4C/ID approach. Abbreviations: LT, learning task; SI, supportive information; PI, procedural information; PTP, part task practice. |
In the control group, the activity took place over 2 weeks, in the form of an overview, two session of lecture and video playback, and the post-tests. Students were also given time for independent learning in a skills laboratory to practice the drug administration skills as the part-task practice implementation. At the end of the second week, the control group first took the post-test, while the intervention group received a post-test at week 5, to prevent exposure to the control group by training material from the intervention group. All of the trainers were experts in the field of patient safety.
Before the training started, the author held a briefing with the trainers and also with all of the instructors. Observers who evaluated the skills assessments were different from the instructors who trained the students. The purpose was that the observers did not know the students who were the control group and students who were the intervention group (blinding technique). The authors held a briefing with; 1) the observers to prepare them to use the checklist, 2) simulated patients, and 3) assistants who assisted the instructor when the implementation of simulation skills training and at the time of skills assessment. The observations of skills and MCQ test were held in the last week, after the training completed. The administration staff that delivered the MCQ test also did not know the students who were the control group and intervention group. At the end of the training, eleven students were considered drop-outs of the study because they did not completely join in all of the training activities.
Data Analysis
We used homogeneity test applying the Chi-Square and Mann Whitney formula that found that there were no significant differences between the characteristics of respondents in the intervention and control groups. Univariate analysis was used to describe the distribution, frequency, percentage of respondents’ characteristics of the study and to analyze the average level of knowledge, and skills of students in providing safe medication. Bivariate analysis used the independent sample t-test to analyze the mean differences of knowledge and skills in administering the oral drug and intramuscular drug because the data were normally distributed. For the data that were not normally distributed, analysis used the Mann–Whitney formula (see Tables 2 and 3).
 |
Table 2 Comparison of Knowledge of Patient Safety and Medication Safety Between Intervention and Control Group |
 |
Table 3 Comparison of Oral Drug and Intramuscular Drug Administration Skill Between Intervention Group and Control Group |
Results
The results of this study indicated that there were significant differences in the knowledge of drug administration skills of students between the intervention and the control groups with p-value 0.00 and alpha of 0.05 (5%). Intervention and control groups also have significant differences in skills, both oral drug administration, and intramuscular drug administration. Table 2 showed that there were significant differences in the majority of the knowledge aspects except for the knowledge about High Alert medicines and Look-Alike Sound-Alike (LASA) drugs. The aspect of knowledge were patient-safety concepts, general medication safety concept, storing and preparation of medicine, administration of drug, LASA and high alert drug.
Table 3 shows that there were significant differences between the overall skills of oral drug and intramuscular drug administration. Furthermore, results also showed that in the majority of aspects in oral drug administration of the intervention group, the scores were significantly higher than the control group except patient identification, documentation, and empathy, communicative and respect. Meanwhile, in the skills of intramuscular drug administration, the students in the intervention group were significantly different in all of the aspects of skills compared with the control group.
Discussions
Instructional design is very important in presenting learning material to students to achieve their learning goals. Instructional design is the art of presenting attractive learning tasks so that they are easily accepted by students. In our study, nursing students scored higher in knowledge and skills and gained more learning experience during the course with the 4C/ID approach, which can be seen from the results of knowledge and skills assessments that were significantly different from the control group. The differences can be seen in the aspects of knowledge on the concept of patient safety, the principles of drug administration, drug storage and preparation, and other aspects of knowledge. Meanwhile, the students’ skills differed significantly in the aspects of drug preparation, drug administration, and drug monitoring. In general, oral and intramuscular drug administration skills showed significant differences. In our study, nursing students scored higher in knowledge and skills and received more learning experiences during the course with the 4C/ID approach, which can be seen from the results of the assessment of knowledge and skills that were significantly different from the control group. Other studies using the 4C/ID approach for their courses in different fields.14–17
The strength of this research is the application of an innovative instructional design for complex learning with the 4C/ID approach. The 4C/ID model is suitable for use in designing substantial learning tasks or training programs in length from several weeks to several years and can also be used for a significant part of the curriculum. Learning with the 4C/ID approach places learning-tasks as the main backbone of the learning process. Learning-tasks in this course were given to facilitate students to form their knowledge with various activities in training (real case discussion and reflections, role plays of patient identification and skills simulation sessions).
At the beginning of the course, we used simpler learning-tasks, namely real case discussion and reflections (in a small group) and the students were asked to present their points in front of the class. This process managed to foster student awareness of medication-safety issues in the real practice of health services. Learning-tasks in the first two weeks were more focused on the process of reflection because student reflection is very important for the awareness of medication-safety.22 On the other hand, in conventional learning, students have not been presented with any real cases regarding medication errors and this can cause students to not appreciate the benefits of studying medication-safety and will affect their awareness.
From week 2 to week 4, students gradually engage in more complex learning-tasks, namely role play of patient identification, and simulation of drug administration with both oral drugs and intramuscular drugs. The complexity of learning-task was increased, to prepare nursing students for the real tasks of a professional nurse in medication administration that apply patient safety principles. In the later phase of the training, students have done the simulation skills of oral and intramuscular drug administration repeatedly to prepare for practical applications.13 The use of simulation methods is beneficial in achieving drug delivery competencies and connecting the students’ readiness towards actual practice and their practice in clinical education.23,24
The second component of 4C/ID is the supportive-information provided in the initial learning in the form of video playback and presentation of a real case. These two supportive-information series were used as the triggers in the learning-task activities. We also gave interactive lectures as supportive-information to help students in connecting initial knowledge with their new knowledge.16 There were several material topics chosen that answered the students’ needs for the importance of medication-safety (See Figure 2). Providing supportive-information such as the topic of the role of nurses in medication-safety was given after students were given the time to reflect about the real cases. The aim of these strategies was to better prepare the students for new information provided in response to student curiosity and in the process, the students actively construct their new knowledge.21
The third component applied from 4C/ID model in this study is procedural information. In medication-safety learning with 4C/ID, procedural-information was given in the form of check-lists of safe drug delivery skills. The checklists were used by students in guiding the steps in administering oral and intramuscular drugs administration. Aspects of patient safety and medication-safety were integrated into the check-lists. This is useful to help students to implement the supportive-information into the practice of administering drugs.12 The researchers gave the check-lists before the simulation took place so that students have time to properly prepare before the simulation activities in the skills laboratory.
The last component of 4C/ID was the task-part practice, which provided the students the opportunity to learn drug administration skills independently.13 It aims to train automation and competency in student skills. Mastery of skills from the novice stage to becoming an expert requires several steps including continuous training efforts that were facilitated by independent training and practice in the skills laboratory. Existing constraints are that while the independent training should be done several times, but at the time of this research, the researchers could only provide two scheduled opportunities for students to be able to practice independently. This lack of more practice can directly affect the ability of students to safely administer drugs because short exercises can lead to less optimal competences in safety procedures.
The results showed that there were significant differences between the overall knowledge and administration skills of the intervention and control groups. The results also showed that the majority of aspects in the knowledge and oral administration skills also have significant differences. But, there were no significant differences for the knowledge of High Alert drugs and LASA drugs between the two groups. This finding is possible because the topic of LASA drug and High Alert medicine is a reasonably difficult topic and a new concern for students. Even though they received the new information about these concerns in this course, there were not significant differences in the students’ knowledge level. Sufficient time allocation is needed to teach about High Alert medicines and LASA drugs.
In the oral drug administration skills, the aspect of documentation also showed that there were no significant differences. At the post-test of administration skills, time was extended for some students, so that those in the control group who were not applying the medication-safety principles step by step in the process still had enough time at the end of the observation to make better documentation. Whereas, the students in the intervention group had only limited time at the end of the skills observation. The lesson learned was that medication-safety skills needs enough time to be applied by the students, especially for the beginners. The instructors need to provide enough time for all students in the application of the medication-safety administration.
Limitations
We did not present the pretest value of the students because the design was posttest-only quasi-experimental design. Literature states that this design is suitable for educational research because the pretest can cause some bias in the results.20 In this study, the part-task practice was also given to the students in the limited time because of the time constraints and resources. Additionally, our study had not included a qualitative exploration of students’ perceptions of the medication-safety course. It would be interesting to hear students’ opinions about the course for improvement of further study.
Conclusion
Training of medication-safety using the 4C/ID approach could improve the medication-safety knowledge and skills of the nursing students. Training on medication-safety can be continuously given to nursing students in their preclinical education to better prepare nursing students to be competent in medication administration and patient safety.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval
The study was approved by The Research Ethics Committee, Faculty of Medicine and Health Sciences, Universitas Muhammadiyah Yogyakarta, where the research was done in the nursing study program (No. 231/EP-FKIK-UMY/VI/20160). The aim and process of the research were explained to participants. The written informed consent was obtained before they took part in this study, and informed consent also obtained for publication of anonymized responses. All procedure performed in this research were following the Declaration of Helsinki principles and the institutional research committee’s ethical standards.
Acknowledgments
We would like to thank the nursing students, nursing lecturers, and trainers, who participated in our study, and also Eric Christopher for the English-review of this paper. We also thank Professor Iwan Dwiprahasto who has given many valuable review for this manuscript.
Author Contributions
All authors (LM, FH, and MC) made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Hibah Doctoral Research SP DIPA-042.06.1.401516/2018 from The Ministry of Research, Technology and Higher Education of Republic of Indonesia.
Disclosure
The authors report no conflict of interest in this work.
References
1. Barton AJ, Armstrong G, Preheim G, Gelmon SB, Andrus LC. A national Delphi to determine developmental progression of quality and safety competencies in nursing education. Nurs Outlook. 2009;57(6):313–322. doi:10.1016/j.outlook.2009.08.003
2. Sulosaari V, Kajander S, Hupli M, Huupponen R, Leino-Kilpi H. Nurse students’ medication competence: an integrative review of the associated factors. Nurse Educ Today. 2012;32(4):399–405. doi:10.1016/j.nedt.2011.05.016
3. Vaismoradi M, Bondas T, Jasper M, Turunen H. Nursing students ’ perspectives and suggestions on patient safety: implications for developing the nursing education curriculum in Iran. Nurse Educ Today. 2014;34(2):265–270. doi:10.1016/j.nedt.2012.10.002
4. Mansour M. Examining patient safety education in pre-registration nursing curriculum: a qualitative study. J Nurs Educ Pract. 2013;3(12):157–167. doi:10.5430/jnep.v3n12p157
5. Vaismoradi M, Jordan S, Turunen H, Bondas T. Nursing students’ perspectives of the cause of medication errors. Nurse Educ Today. 2014;34(3):434–440. doi:10.1016/j.nedt.2013.04.015
6. Musharyanti L, Claramita M, Haryanti F, Dwiprahasto I. Why do nursing students make medication errors? A qualitative study in Indonesia. J Taibah Univ Med Sci. 2019;14(3):282–288. doi:10.1016/j.jtumed.2019.04.002
7. Kiersma ME, Plake KS, Darbishire PL. Patient safety instruction in US health professions education. Am J Pharm Educ. 2011;75(8):162. doi:10.5688/ajpe758162
8. Kirkman MA, Sevdalis N, Arora S, Baker P, Vincent C, Ahmed M. The outcomes of recent patient safety education interventions for trainee physicians and medical students: a systematic review. BMJ Open. 2015;5(5):e007705–e007705. doi:10.1136/bmjopen-2015-007705
9. Nguyen H-T, Nguyen T-D, van den Heuvel ER, Haaijer-Ruskamp FM, Taxis K. Medication errors in Vietnamese hospitals: prevalence, potential outcome and associated factors. Emmert-Streib F, editor. PLoS One. 2015;10(9):e0138284. doi:10.1371/journal.pone.0138284
10. Salmasi S, Khan TM, Hong YH, Ming LC, Wong TW. Medication errors in the Southeast Asian Countries: a systematic review. PLoS One. 2015;10(9):e0136545. doi:10.1371/journal.pone.0136545
11. Tella S, Liukka M, Jamookeeah D, Smith N-J, Partanen P, Turunen H. What do nursing students learn about patient safety? An integrative literature review. J Nurs Educ. 2013. doi:10.3928/01484834-20131209-04
12. Van Merriënboer JJG, Clark RE, de Croock MBM. Blueprints for complex learning: the 4C/ID-model. Educ Technol Res Dev 2002;50(2):39–61. doi:10.1007/BF02504993
13. Van Merriënboer JJG, Kirschner PA. Ten Steps to Complex Learning: A Systematic Approach to Four-Component Instructional Design.
14. Melo M, Miranda GL. Learning electrical circuits: the effects of the 4C-ID instructional approach in the acquisition and transfer of knowledge. J Inf Tech Educ Res. 2015;14:313337.
15. Verheyden G, Handgraaf M, Demirci A, Grüneberg C. The future of physiotherapy education: towards a translational model of learning complex skills: the future of physiotherapy education. Physiother Res Int. 2011;16(4):187–190. doi:10.1002/pri.519
16. Tjiam IM, Schout BMA, Hendrikx AJM, Scherpbier AJJM, Witjes JA, Van Merriënboer JJG. Designing simulator-based training: an approach integrating cognitive task analysis and four-component instructional design. Med Teach. 2012;34(10):e698–707. doi:10.3109/0142159X.2012.687480
17. Susilo AP, van Merriënboer J, van Dalen J, Claramita M, Scherpbier A. From lecture to learning tasks: use of the 4C/ID model in a communication skills course in a continuing professional education context. J Contin Educ Nurs. 2013;44(6):278–284. doi:10.3928/00220124-20130501-78
18. AINEC. The Core Curriculum of Nurse’s Education. 2015:108–111
19. World Health Organizatio n. WHO multi-professional patient safety curriculum guide; 2011
20. Gay LR, Mills GE, Airasian PW. Educational Research Competencies for Analysis and Applications. New Jersey: Pearson; 2011.
21. Vandewaetere M, Manhaeve D, Aertgeerts B, Clarebout G, Van Merriënboer JJG, Roex A. 4C/ID in medical education: how to design an educational program based on whole-task learning: AMEE Guide No. 93. Med Teach. 2015;37(1):4–20. doi:10.3109/0142159X.2014.928407
22. De Feijter JM, De Grave W, Hopmans E, Koopmans R, Scherpbier AJJA. Reflective learning in a patient safety course for final-year medical students. Med Teach. 2012;34(11):946–954. doi:10.3109/0142159X.2012.714873
23. Jarvill M, Jenkins S, Akman O, Astroth KS, Pohl C, Jacobs PJ. Effect of simulation on nursing students’ medication administration competence. Clin Simul Nurs. 2018;14:3–7. doi:10.1016/j.ecns.2017.08.001
24. Avraham R, Shor V, Hurvitz N, Shvartsur R, Kimhi E. Transferability of medication administration simulation training to clinical settings. Teach Learn Nurs. 2018;13(4):258–262. doi:10.1016/j.teln.2018.07.004
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.