Back to Journals » Patient Preference and Adherence » Volume 16
Improving Medication Adherence in Community-Dwelling Patients with Schizophrenia Through Therapeutic Alliance and Medication Attitude: A Serial Multiple Mediation Model
Authors Hsieh WL ![]() , Yeh ST
, Yeh ST ![]() , Liu WI
, Liu WI ![]() , Li IH, Lee SK, Chien WT
, Li IH, Lee SK, Chien WT ![]()
Received 30 November 2021
Accepted for publication 19 March 2022
Published 13 April 2022 Volume 2022:16 Pages 1017—1026
DOI https://doi.org/10.2147/PPA.S351848
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Wen Ling Hsieh,1 Shin Ting Yeh,2 Wen I Liu,1 I Hsien Li,1 Shih Kai Lee,3 Wai Tong Chien4
1School of Nursing, National Taipei University of Nursing and Health Sciences, Taipei City, Taiwan; 2Department of Gerontological Health Care, National Taipei University of Nursing and Health Sciences, Taipei City, Taiwan; 3Department of Nursing, Tsaotun Psychiatric Center, Ministry of Health and Welfare, Nan-Tou, Taiwan; 4The Nethersole School of Nursing, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong, People’s Republic of China
Correspondence: Wen I Liu, School of Nursing, National Taipei University of Nursing and Health Sciences, No. 365, Ming-Te Road, Peitou District, Taipei City, 112303, Taiwan, Tel +886-2-28227101 ext. 3184, Fax +886-2-28213233, Email [email protected] Shih Kai Lee, Department of Nursing, Tsaotun Psychiatric Center, Ministry of Health and Welfare, No. 161, Yu-Pin Road, Tsaotun Township, Nan-Tou, 54249, Taiwan, Tel +886-49-2550800 ext. 2100, Email [email protected]
Background: Increased medication adherence improves patient outcomes and lowers the overall cost of care by preventing disease relapse and hospital readmission. Several systematic reviews have identified that insight, therapeutic alliance, and attitude towards medication affect medication adherence in patients with schizophrenia; however, no study has examined all the aforementioned variables together nor has discussed the chains of these mediators.
Purpose: To examine the insight–medication adherence relationship among community-dwelling schizophrenia patients through a serial multiple mediation model of therapeutic alliance and medication attitude.
Patients and Methods: This study with a cross-sectional correlational design included a convenience sample of community-dwelling schizophrenia patients from Taiwan (n = 229). From January 2017 to January 2018, data were collected by trained nurses using questionnaires. The PROCESS tool was used to analyse fine-grained chains.
Results: In serial multiple mediation, the indirect effect of insight on medication adherence through therapeutic alliance and, subsequently, alteration of medication attitude was significant. However, the direct effect changed from significant to non-significant, indicating a complete mediating effect.
Conclusion: In community-dwelling schizophrenia patients, the effects of therapeutic alliance and medication attitude on medication adherence are greater than that of insight. We recommend revising the strategy of community home visits by different psychiatrists or nurses in alternating shifts. Therapeutic alliance is the first step required to promote medication adherence. Based on this alliance, altering the patients’ medication attitude may be more effective in improving medication adherence than merely enhancing insight.
Keywords: medication adherence, insight, medication attitude, mediating effect, schizophrenia, therapeutic alliance, nursing
Introduction
Recurrent psychotic symptoms in patients with schizophrenia result in repeated hospitalisations, which costs approximately 94 million to 102 billion USD worldwide.1 Currently, Taiwan has more than 150,000 schizophrenia patients, with this number increasing by 0.7% each year. The medical expenditure for these patients is 11.2 billion NTD annually2 and is intimately associated with their medication adherence.3 Non-adherent patients have a 2.5 times higher disease recurrence rate than adherent patients.4 Risk of violence and self-injury is also higher among non-adherent patients,5 which can be immensely harmful to individuals, families, and society. Therefore, ensuring that these patients adhere to medications is crucial for psychiatric nurses. Despite researchers worldwide continuously striving to develop relevant strategies, such as psychoeducation on medication, insight establishment, and increased family support, for promoting medication adherence,6 the medication non-adherence rate among schizophrenia patients continues to be high, up to 54.5%.7 Although injection administration at the patient’s residence has been suggested as a convenient approach, implementation of this approach would incur higher medical costs and require more healthcare professionals.8 Developing interventions that help patients to autonomously and regularly self-medicate is an active strategy to effectively reduce rehospitalisations due to recurrent psychotic symptoms, thus reducing healthcare costs. Therefore, additional, cost-effective strategies must be developed to improve medication adherence.
Taking medications consistently as per the medical prescription is termed medication adherence, and patient and disease characteristics are its vital influencing factors.9 Among these factors, insight into physiopathology, diagnosis, and treatment is the most critical predictor of medication adherence.10 According to several systematic reviews, poor insight, poor therapeutic alliance, and negative attitude towards medication negatively affect medication adherence in patients with severe mental illness.10–13 Insight can explain 48% of the variation in medication adherence,14 and its lack is unfavourable for both medication adherence behaviour and quality of life of patients.15 Although numerous relevant interventions for establishing insight have been developed, insight establishment in schizophrenia patients remains a challenge. Notably, >40% of these patients are unaware of their mental illness.16 A schizophrenia patient’s poor insight affects therapeutic alliance and medication behaviours, which in turn increases psychotic symptoms and recurrence rates. However, many conditions affect insight, such as gray matter loss in an individual’s brain regions, which leads to a decline in memory, attention, and executive function. Because of a deficient metacognition, schizophrenia patients cannot integrate current and past information to influence behavioural decisions. In addition, owing to the influence of social culture, they are unable or unwilling to accept their own mental illness.17,18 Furthermore, the unwillingness to develop insight is also a defense mechanism of patients to avoid the painful mental illness-recognizing process.19 Improving insight regarding a disease is a crucial current clinical practice for community-dwelling schizophrenia patients. Numerous researchers have attempted to improve medication adherence by enhancing patient insight. However, limited disease awareness and psychological defense mechanisms have led to a lack of insight in numerous schizophrenia patients, negatively affecting medication adherence and negatively influencing recovery.16,18 Therefore, when achieving immediate improvements through insight enhancement is difficult, factors more effective than insight in promoting medication adherence among these patients must be identified.
According to WHO initiatives, a stronger collaboration between patients and Healthcare professionals (termed therapeutic alliance) contributes to better patient health.20 Therapeutic alliance refers to trust, promise, good communication, and interactions between patients and caregivers,21 and predicts rehospitalisation rates, psychological therapy and medication, and recovery.22–24 Therapeutic alliance is significantly associated with medication adherence and is the first step in nursing care.10 Studies have recently used therapeutic alliance as a mediator variable.25,26 For example, in a study involving 133 schizophrenia patients, therapeutic alliance partially mediated the cognitive impairment–recovery relationship.26 Additionally, according to the theory of planned behaviour (TPB), attitude is a critical influencing factor for behavioural change.27 Medication attitude is related to medication adherence, insight, and alliance; all these factors affect each other.10–13,28 A study examined attitude as a mediator variable in 168 inpatients with schizophrenia and found that medication attitude can mediate the insight–social functions relationship.29 However, no study has explored the relationship between medication adherence and the aforementioned mediators together nor has discussed the chain of these mediators.25,26,29 Knowledge of the chain is of more practical significance for continuous care.
In summary, medication adherence is a complex matter influenced by numerous factors, as reported in the literature. A recent systematic review found that insight was the most vital predictor of medication adherence.10 However, according to the TPB and a framework of previous studies,25–27,29 therapeutic alliance and medication attitude are important mediators of behavioural outcome. The relationship between insight and medication adherence among community-dwelling schizophrenia patients through a serial multiple mediation model of therapeutic alliance and medication attitude has rarely been investigated.25–27,29 We here therefore verified the relationship among these four variables. Our findings would subvert the current emphasis on improving the insight of patients with schizophrenia for promoting medication adherence.
Objectives and Hypothesis
The study examined a serial multiple mediation model of therapeutic alliance and medication attitude in the insight–medication adherence relationship among community-dwelling schizophrenia patients.
The serial multiple mediation model is different from a parallel mediation model. It can be used to explore the mutual association between two mediator variables and provide greater detail. This model includes two simple mediation pathways (pathway a1b1: X→M1→Y; pathway a2b2: X→M2→Y) and one serial pathway (pathway a1db2: X→M1→M2→Y). The study hypotheses about the mediating effects of pathways a1b1, a2b2, and a1db2 were significant. Pathway a1db2 is the main pathway in this study (Figure 1).
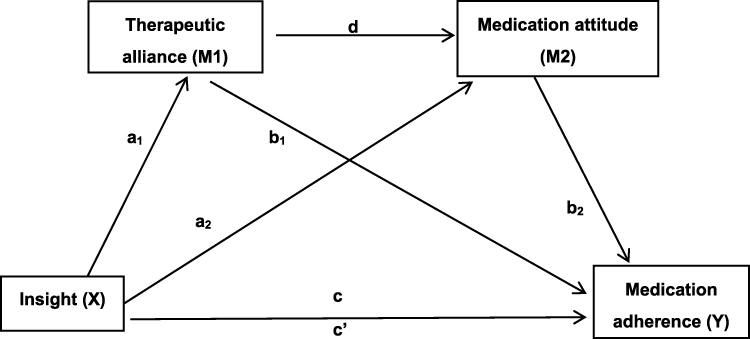 |
Figure 1 The serial mediation model in this study. Notes: X = independent variable; Y = dependent variable; M1, M2 = mediators; a1, a2, b1, b2, d, c, c’ = unstandardized regression coefficients; a1 = X on M1; a2 = X on M2; b1 =M1 on Y; b2 = M2 on Y; d = M1 on M2; c = total effect of X on Y; c’ = direct effect of X on Y. |
Methods
We adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist of items that should be included in reports of cross-sectional studies.
Design and Theoretical Framework
In this cross-sectional study, data of each participant were collected only once. The covariates included basic demographic factors and disease factors, with insight being the independent variable (X) and medication adherence being the dependent variable (Y). Therapeutic alliance (M1) and medication attitude (M2) were the mediator variables.
Setting and Participants
The study setting was the community-based psychiatric departments of two major public psychiatric hospitals having the largest number of home care clients in northern and central Taiwan. Using convenience sampling, patients who received home care services from January 2017 to January 2018 were selected as study participants. The inclusion criteria were diagnosis of schizophrenia according to the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5); age 20–64 years; treatment with at least one antipsychotic drug; received psychiatric home care services in the community; and ability to communicate in Mandarin or Taiwanese Hokkien. The exclusion criteria were diagnosis of substance use disorder, neurocognitive disorder, or intellectual disability.
G*Power, version 3.1.9.4, was used to compute the sample size and select the F-test. In the linear multiple regression, the set power was 0.80, α level was 0.05, number of predictors was 12, and medium effect size was 0.15.30 Sufficient statistical power was achieved with at least 127 participants. In total, 235 participants met the inclusion criteria, but 6 were excluded (3 were unable to communicate and 3 declined to participate). Finally, 229 participants were enrolled, and the statistical power was achieved.
Data Collection and Ethics Approval
Because the participants received home care, they were enrolled in their residences. Seven home care nurses from the study hospitals collected data during home visits; they were trained in data collection before enrolment. Inter-rater reliability was attained at an intraclass correlation (ICC) of >0.80. The trained nurses performed assessments and completed questionnaires, including the demographics questionnaire, Global Assessment of Functioning (GAF), Brief Psychiatric Rating Scale (BPRS), Schedule for Assessment Insight in Psychosis (SIP), Working Alliance Inventory-Short (WAI-S), Drug Attitude Inventory-10 (DAI-10), and Medication Adherence Rating Scale (MARS). The GAF, BPRS, and SIP tools were nurse-administered assessment questionnaires; other assessments were completed through patients’ self-reporting.
This study was reviewed and approved by the institutional review boards (IRB) of the two hospitals (Institutional Review Board of the Tri-Service General Hospital no. 1-105-05-124 and Tsaotun Psychiatric Centre, Ministry of Health and Welfare IRB no. 105026). The study was conducted according to the Declaration of Helsinki. After the investigator explained the study aim and content and the related benefits to the participants, they confirmed their willingness to participate through written informed consent. Data were collected for each patient within 15–20 min. On completing the questionnaires, the participants were encouraged to confirm that all items were completed and received appreciation gifts. Only staff members involved in this study had access to the data.
Measure Variables and Tool
Covariates
The covariates consisted of the following participant-related characteristics: age, gender, educational level, employment status, marital status, illness duration, number of hospitalisations, global function, and psychotic symptoms.
The GAF tool, proposed by the American Psychiatric Association, uses a 0–100-point scale for evaluating patient function, with higher scores indicating better global function.31 This scale has been previously used to examine the global function of 101 employees in the psychiatry Department and has demonstrated good reliability (ICC = 0.79) and validity.32 The 16-item BPRS uses a 7-point Likert scale to measure psychiatric symptoms and psychopathology, with higher scores indicating worse psychopathology. This tool has good reliability (Cronbach’s α = 0.77–0.90; test–retest reliability = 0.82) and validity (total variation explained was 68%).33,34 Chang et al translated the BPRS into Mandarin.35 The scale range was 0–96 points, with higher scores indicating more severe psychotic symptoms. For this study, the Cronbach’s α of the BPRS was 0.79.
Independent Variables and Mediators
The Scale to assess Unawareness of Mental Disorder (SUMD) is regarded as a gold standard for measuring insight, our independent variable. However, the reliability and validity of the SIP is better than those of SUMD in the Chinese version.36,37 Therefore, we used the SIP, a nine-question assessment scale developed by Yen et al, for measuring insight. A scoring scale from 1 (complete denial) to 4 points (true insight) was employed, and the total score range is 9–36 points, with higher scores indicating better insight. This tool has good reliability (Cronbach’s α = 0.92) and construct validity. SIP was significantly correlated with the scales SUMD and Schedule for the Assessment of Insight.37 In this study, the Cronbach’s α of SIP was 0.89.
WAI-S, a shortened version (12 questions) of the WAI scale (36 questions) developed by Tracey & Kokotovic (1989), is widely used to measure therapeutic alliance (our first mediator) between nurses and psychiatric patients.40–42 A scoring scale from 1 (never) to 7 (always) was employed, and the total score range is 12–84 points, with the higher score indicating better therapeutic alliance.38 This tool has good reliability (Cronbach’s α = 0.91) and construct validity (significant correlation with the California Psychotherapy Alliance Scale and Helping Alliance Questionnaire).39 In this study, the Cronbach’s α of WAI-S was 0.92.
DAI-10, a shortened version (10 questions) of the DAI scale (30 questions) developed by Nielsen et al, is used to measure medication attitude (our second mediator). This is a self-completed tool in which 1 point is given for “true” and −1 point is given for “false.” The total score range is −10 to +10 points. The higher the score, the more positive medication attitude. The scale has good test–retest reliability (r = 0.92), and the total variation explained was 54%.43 The internal consistency of the Chinese version was 0.88, the retest reliability after 2 weeks was 0.83, and the total variation explained was 43.1%.44 In this study, the Cronbach’s α of DAI-10 was 0.70.
Dependent Variable
Considering the high cost, time, and potential resistance of the participants towards these objective tools, a subjective measurement tool with a good psychometric test was also used in this study. The MARS is a self-completed tool, developed by Thompson et al based on DAI and MAQ, for measuring medication adherence. It includes 10 questions, with 1 point given for “true” and 0 point given for “false.” The total, is 0–10 points and a higher score indicates better medication adherence.45 Kao & Liu (2010) translated this scale into Mandarin. This scale has good reliability (Cronbach’s α = 0.72) and validity, and the total variation explained was 49.7% (significant correlation with objective drug concentration).46 In this study, the Cronbach’s α of MARS was 0.72.
Statistical Analysis
SPSS statistical software version 21.0 (IBM Corporation, Armonk, NY, USA) was used for the descriptive and inferential statistical analyses of the data. Categorical variables were expressed as numbers and percentages, while continuous variables were expressed as the mean and standard deviation. Independent sample t-test, one-way ANOVA, and Pearson’s correlation analysis were used for inferential statistics.
Model 6 of PROCESS version 3.5 for SPSS, which is based on ordinary least-squares regression and bootstrapping, was used to explore the fine-grained chains of the serial multiple mediation model.47 After the covariates were controlled, the serial mediation model provided three specific indirect effects that summed up to a total indirect effect. The specific indirect effects in this model were through (1) therapeutic alliance (pathway a1b1), (2) medication attitude (pathway a2b2), and (3) therapeutic alliance and medication attitude (pathway a1db2). For inference testing of the indirect effects, bootstrapping from 5000 samples of the original dataset (n = 229) was used to obtain 95% bias-corrected confidence intervals.
Results
Descriptive Statistics
In total, 229 participants aged 20–64 years (mean ± standard deviation: 46.9 ± 8.63 years) were enrolled. Table 1 presents the descriptive statistics for all study variables. Of the participants, 55.9% were men, and 64.63% were single, and 77.73% were unemployed. Overall, 47.16% of the participants had completed senior high school education. Detailed information is presented in Table 1.
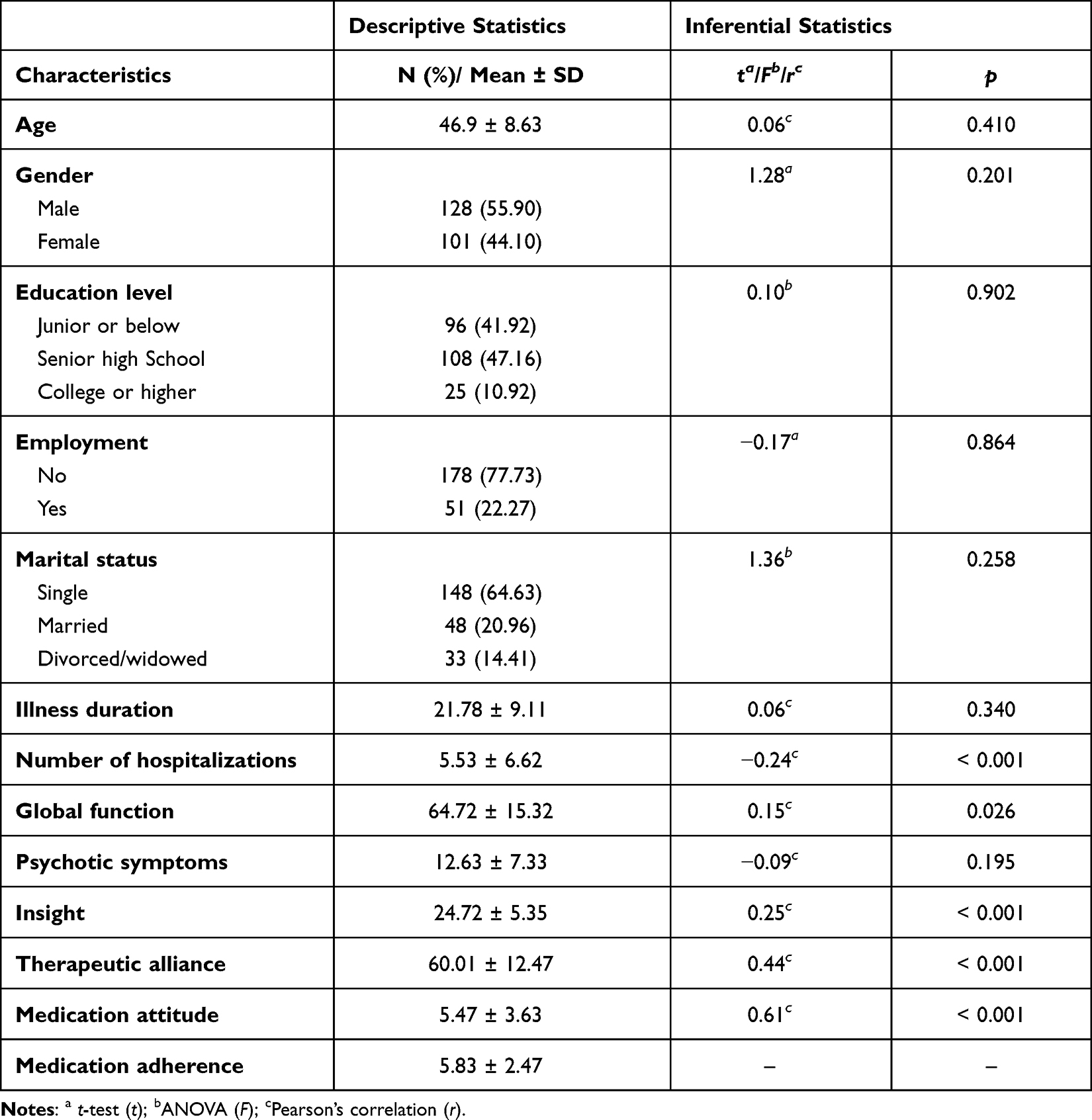 |
Table 1 Description of Patient Demographics and Main Variables (n = 229) |
Correlations Between Insight, Therapeutic Alliance, Medication Attitude, and Medication Adherence
According to bivariate associations, the factors associated with medication adherence were therapeutic alliance and medication attitude. Medication adherence was significantly related to number of hospitalisations (r = −0.24, p < 0.001), global function (r = 0.15, p = 0.026), insight (r = 0.25, p < 0.001), medication attitude (r = 0.61, p < 0.001), and therapeutic alliance (r = 0.44, p < 0.001). These correlations mostly ranged from small to moderate (r ranging from 0.24 to 0.44, p < 0.001),30 except for the positive relationship between medication attitude and medication adherence (r = 0.61, p < 0.001).
Sex (t = 1.28, p = 0.201), age (r = 0.06, p = 0.410), education level (F = 0.10, p = 0.902), employment (t = −0.17, p = 0.864), marital status (F = 1.36, p = 0.258), illness duration (r = 0.06, p = 0.340), and psychiatric symptoms (r = −0.09, p = 0.195) showed no statistically significant differences for medication adherence.
Serial Mediation Model Analysis
In this model, the variables were associated with medication adherence as covariates. Figure 2 presents the three pathways of the serial mediation model. The total effect (Bc) of insight on medication adherence was significant (Bc = 0.11, standard error [SE] = 0.03), t = 3.85, p < 0.001), indicating that the effect of insight on medication adherence was significant when therapeutic alliance and medication attitude were not considered.
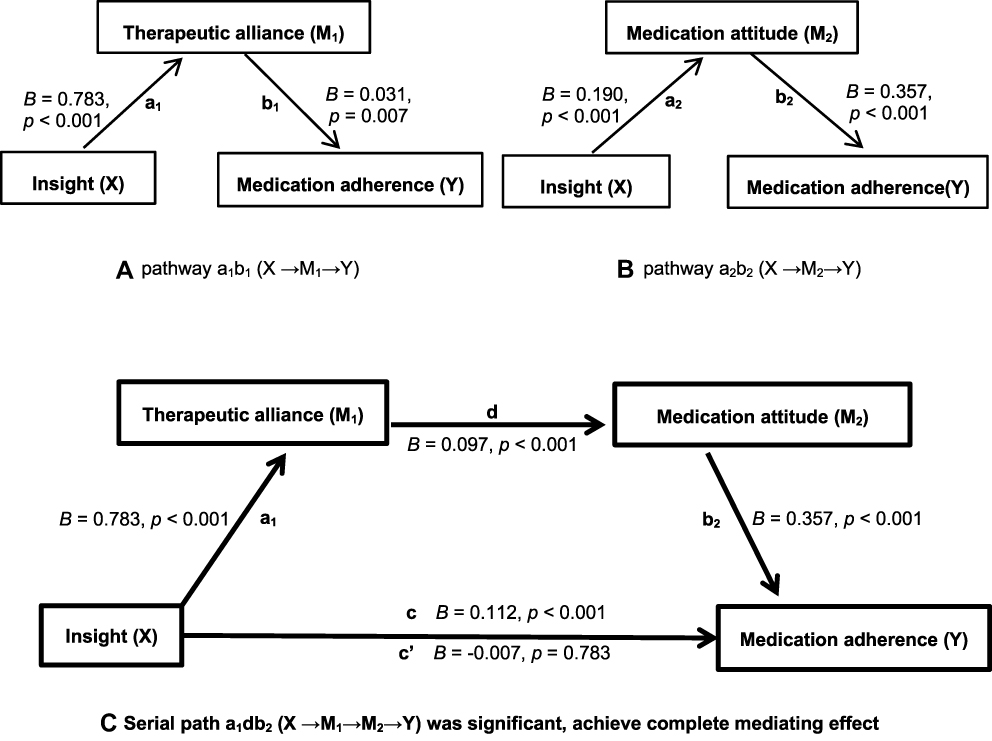 |
Figure 2 The serial mediation results in this study (A-C). Notes: X = independent variable; Y = dependent variable; M1, M2 = mediators; A is the simple mediation model (pathway a1b1: X→M1→Y). B is the simple mediatiom model (pathway a2b2: X→M2→Y). C is the serial mediation model (pathway: X→M1→M2→Y). a1, a2, b1, b2, d, c, c’ = unstandardized regression coefficients; a1 = X on M1; a2 = X on M2; b1 =M1 on Y; b2 = M2 on Y; d = M1 on M2; c = total effect of X on Y; c’ = direct effect of X on Y. The coefficient of pathway c does not consider the mediator, the total effect of insight on medication adherence. The coefficient of pathway c’ considers the mediators, the direct effect of insight on medication adherence, not including the mediating effect. If pathway c’ is not significant, after considering M1 and M2, the effect of insight on medication adherence becomes non-significant. |
In the main pathway, the sequential indirect effect of insight on medication adherence through therapeutic alliance and medication attitude was significant (pathway a1db2: point estimate = 0.027, SE = 0.007; 95% confidence interval [CI]: 0.015–0.041). In addition, the other simple mediation pathways from insight to medication adherence through therapeutic alliance (pathway a1b1: point estimate = 0.025, SE = 0.010; 95% CI: 0.006–0.047) and through medication attitude (pathway a2b2: point estimate = 0.068, SE = 0.019; 95% CI: 0.034–0.108) were significant.
When considering serial mediators, the total direct (Bc’) effect of insight on medication adherence was non-significant (Bc’ = −0.01 (0.03), t = −0.28, p = 0.783), indicating that the serial mediating model had achieved a complete mediating effect.
Discussion
The number of hospitalisations, global function, insight, medication attitude, and therapeutic alliance were significantly related to medication adherence. Higher degrees of global function, insight, medication attitude, and therapeutic alliance were associated with higher medication adherence, and vice versa. This finding is in line with that of a previous study,17,18,22,48 indicating that professionals must build a trust-based alliance relationship with patients and promote positive medication attitude, which can contribute to medication adherence.
Studies have mostly investigated these variables as a single mediating variable.25,26,29 Moreover, no study examined the serial relationship between insight and medication adherence among community-dwelling schizophrenia patients. Hence, we used a serial mediation model to investigate the potential relationship between insight and medication adherence through sequential mediation by therapeutic alliance and medication attitude. Using this model, we could determine the chain through which therapeutic alliance can predict medication attitude, which in turn can predict medication adherence. This result is consistent with those of other studies suggesting that a lack of insight is related to poorer therapeutic alliance.17,49 A possible reason is that therapeutic alliance is a fundamental factor in care and promotes behavioural changes in patients.22,50 Sincerity, active listening, understanding the interpersonal relationships of patients, and empathic life experiences in therapeutic alliance can alter medication attitude,28 improve medication adherence,21 and promote individual recovery,24,51 indicating that alliance is a vital component of promoting care outcomes. Moreover, attitude is a critical influential factor in behavioural change.27 Positive medication attitude includes an individual’s belief that the drug can treat mental illness, calm oneself, or improve personal work ability,50 which all lead to medication adherence.28 This serial relationship has been supported by previous studies.17,21,27,28,49
Our results thus offer a novel perspective for understanding the multiple effects of therapeutic alliance and medication attitude, and not the effects of a single mediator, on medication adherence. Based on the findings, we suggest that care intervention for medication adherence should establish therapeutic alliance, and subsequently focus on the individual’s attitude toward treatment or knowledge regarding Medicine rather than only on the overall insight. This result provides another clinical care perspective, which can be tailored to individual cases to promote medication adherence.
In summary, no study has included crucial variables in a serial mediation model for overall examination. Thus, this study provides novel evidence that the effects of therapeutic alliance and medication attitude on medication adherence are greater than that of insight in community-dwelling schizophrenia patients. The serial multiple model showed a complete mediating effect where pathway c’ was non-significant. Traditional care services focusing on boosting insight in patients should be improved, and an alliance relationship with patients should be developed. Based on this therapeutic alliance, interventions for developing a positive medication attitude and enhancing insight should be simultaneously performed to promote medication adherence in schizophrenia patients. Importantly, insight enhancement alone may affect the protective mechanism of the patient, causing them to face the disease without adequate psychological preparation.19
Strengths and Limitations
This may be the first study focusing on the insight––medication adherence relationship among community-dwelling schizophrenia patients through a serial multiple mediation model of therapeutic alliance and medication attitude. This result can guide clinical practice and subvert the current emphasis on enhancing the insight of schizophrenia patients for promoting medication adherence.
This study used convenience sampling; hence, sample representativeness is doubtful. However, participant recruitment was conducted at two institutions in this study, which may increase some representativeness. This is a cross-sectional study and lacks confirmation of relationships. Structured therapeutic alliance and positive attitude towards medication care protocols should be developed, and randomised controlled trials should be conducted for stringent validation of relationships. Furthermore, this study was based on existing literature and the TPB and only included therapeutic alliance and medication attitude as mediator variables. While other studies included psychotic symptoms as mediator variables,29 we included this as a control variable owing to its variability during the study process.
Concerning measurement tools, some items of MARS are similar to those of DAI-10, which may be a limitation for result interpretation. However, according to the TPB, behaviour includes the concept of attitude; thus, these tools having similar observed variables (items) is normal. Therefore, the measurement tools were chosen based on the development purpose of these tools, that is, DAI measures attitudes towards taking medication and MARS measures behaviours of taking medication. This study additionally used linear regression and considered DAI and MARS as independent variables for predicting psychiatric symptoms. The results showed no collinearity (VIF = 1.58). In addition, we only used the MARS self-completed scale. Simultaneous use of additional measurement methods for medication adherence may help to accurately determine the true status of medication adherence. However, the MARS scale is simple, cost-effective, and significantly correlated with objective blood drawing data. Hence, it offers reliability and validity for supporting the study results.
Conclusion
The study results confirmed our hypotheses, whereby the insight–medication adherence relationship through a serial multiple mediation model of therapeutic alliance and medication attitude was established, demonstrating a complete mediating effect. This study provides novel evidence that the effects of therapeutic alliance and medication attitude on medication adherence are greater than that of insight. The study findings may change traditional disease management strategies. Developing a therapeutic alliance is the first step in promoting medication adherence. Based on this alliance, altering the patients’ medication attitude may be more effective than merely enhancing insight for improving medication adherence.
Implications for Practice
We recommend revising the existing strategy of community home visits conducted by different psychiatrists or nurses in alternating shifts. Instead, the same Nursing staff or doctor should conduct the home visits. This would establish a trusting and long-lasting relationship between the healthcare professional and the community-dwelling schizophrenia patient and, subsequently, based on this therapeutic alliance, medication attitude can be altered to promote medication adherence. This sequential intervention is effective in clinical practical care and is more effective than insight enhancement alone. This study provides suggestions for clinical practice that may more effectively promote medication adherence in community-dwelling schizophrenia patients, prevent recurrence, and reduce medical costs.
Acknowledgments
The research was partly funded by the Ministry of Health and Welfare planning project of Taiwan (Grant No. 10647) and the Ministry of Science and Technology (Grant No. MOST 107-2314-B-227-006). We thank all study participants. The views and opinions expressed in this manuscript are the authors’ own.
Disclosure
The authors report no conflicts of interest in this work.
References
1. CHong HY, Teoh SL, Wu DB, Kotirum S, Chiou CF, Chaiyakunapruk N. Global economic burden of schizophrenia: a systematic review. Neuropsychiatr Dis Treat. 2016;12:357–373. doi:10.2147/NDT.S96649
2. Ministry of Health and Welfare. The disabled population by classification and locality; 2020. Available from: https://dep.mohw.gov.tw/DOS/cp-5224-62359-113.html.
3. Dilokthornsakul P, Thoopputra T, Patanaprateep O, Kongsakon R, Chaiyakunapruk N. Effects of medication adherence on hospitalizations and healthcare costs in patients with schizophrenia in Thailand. SAGE Open Med. 2016;4:1–7. doi:10.1177/2050312116637026
4. Xiao J, Mi W, Li L, Shi Y, Zhang H. High relapse rate and poor medication adherence in the Chinese population with schizophrenia: results from an observational survey in the people’s republic of China. Neuropsychiatr Dis Treat. 2015;11:1161–1167. doi:10.2147/NDT.S72367
5. Mohr P, Galderisi S, Boyer P, et al. Value of schizophrenia treatment I: the patient journey. Eur Psychiatry. 2018;53:107–115. doi:10.1016/j.eurpsy.2018.06.007
6. Dalum HS, Waldemar AK, Korsbek L, et al. Illness management and recovery: clinical outcomes of a randomized clinical trial in community mental health Centers. PLoS One. 2018;13(4):e0194027. doi:10.1371/journal.pone.0194027
7. Kretchy IA, Osafo J, Agyemang SA, Appiah B, Nonvignon J. Psychological burden and caregiver-reported non-adherence to psychotropic medications among patients with schizophrenia. Psychiatry Res. 2018;259:289–294. doi:10.1016/j.psychres.2017.10.034
8. Correll CU, Citrome L, Haddad PM, et al. The use of long-acting injectable antipsychotics in schizophrenia: evaluating the evidence. J Clin Psychiatry. 2016;77(3):1–24. doi:10.4088/JCP.15032su1
9. World Health Organization. Adherence to long-term therapies-evidence for action; 2003. Available from: https://www.who.int/chp/knowledge/publications/adherence_report/en/.
10. Velligan DI, Sajatovic M, Hatch A, Kramata P, Docherty JP. Why do psychiatric patients stop antipsychotic medication? A systematic review of reasons for nonadherence to medication in patients with serious mental illness. Patient Prefer Adherence. 2017;11:449–468. doi:10.2147/PPA.S124658
11. García S, Martinez-Cengotitabengoa M, Lopez-Zurbano S, et al. Adherence to antipsychotic medication in bipolar disorder and schizophrenic patients: a systematic review. J Clin Psychopharmacol. 2016;36(4):355–371. doi:10.1097/JCP.0000000000000523
12. Sendt KV, Tracy DK, Bhattacharyya S. A systematic review of factors influencing adherence to antipsychotic medication in schizophrenia-spectrum disorders. Psychiatry Res. 2015;225(1–2):14–30. doi:10.1016/j.psychres.2014.11.002
13. Tham XC, Xie H, Chng CM, Seah XY, Lopez V, Klainin-Yobas P. Factors affecting medication adherence among adults with schizophrenia: a literature review. Arch Psychiatr Nurs. 2016;30(6):797–809. doi:10.1016/j.apnu.2016.07.007
14. Kalkan E, Kavak Budak F. The effect of insights on medication adherence in patients with schizophrenia. Perspect Psychiatr Care. 2020;56(1):222–228. doi:10.1111/ppc.12414
15. Novick D, Montgomery W, Treuer T, Aguado J, Kraemer S, Haro JM. Relationship of insight with medication adherence and the impact on outcomes in patients with schizophrenia and bipolar disorder: results from a 1-year European outpatient observational study. BMC Psychiatry. 2015;15(1):1–8. doi:10.1186/s12888-015-0560-4
16. Ramachandran AS, Ramanathan R, Praharaj SK, Kanradi H, Sharma PS. A cross-sectional, comparative study of insight in schizophrenia and bipolar patients in remission. Indian J Psychol Med. 2016;38(3):207–212. doi:10.4103/0253-7176.183085
17. Lysaker PH, Pattison ML, Leonhardt BL, Phelps S, Vohs JL. Insight in schizophrenia spectrum disorders: relationship with behavior, mood and perceived quality of life, underlying causes and emerging treatments. World Psychiatry. 2018;17(1):12–23. doi:10.1002/wps.20508
18. Vohs JL, George S, Leonhardt BL, Lysaker PH. An integrative model of the impairments in insight in schizophrenia: emerging research on factors and treatments. Expert Rev Neurother. 2016;16(10):1193–1204. doi:10.1080/14737175.2016.1199275
19. Ogawa Y, Fukuhara K, Tanaka H, Nagata Y, Ishimaru D, Nishikawa T. Insight into illness and defense styles in schizophrenia. J Nerv Ment Dis. 2019;207(10):815–819. doi:10.1097/NMD.0000000000001038
20. World Health Organization. Stronger collaboration, better health: the global action plan for healthy lives and well-being for all; 2021. Available from: https://www.who.int/initiatives/sdg3-global-action-plan.
21. Pinto RZ, Ferreira ML, Oliveira VC, et al. Patient-centred communication is associated with positive therapeutic alliance: a systematic review. J Physiother. 2012;58(2):77–87. doi:10.1016/S1836-9553(12)70087-5
22. Browne J, Nagendra A, Kurtz M, Berry K, Penn DL. The relationship between the therapeutic alliance and client variables in individual treatment for schizophrenia spectrum disorders and early psychosis: narrative review. Clin Psychol Rev. 2019;71:51–62. doi:10.1016/j.cpr.2019.05.002
23. Shattock L, Berry K, Degnan A, Edge D. Therapeutic alliance in psychological therapy for people with schizophrenia and related psychoses: a systematic review. Clin Psychol Psychother. 2018;25(1):60–85. doi:10.1002/cpp.2135
24. Leonhardt BL, Huling K, Hamm JA, et al. Recovery and serious mental illness: a review of current clinical and research paradigms and future directions. Expert Rev Neurother. 2017;17(11):1117–1130. doi:10.1080/14737175.2017.1378099
25. Anderson SR, Tambling R, Yorgason JB, Rackham E. The mediating role of the therapeutic alliance in understanding early discontinuance. Psychother Res. 2019;29(7):882–893. doi:10.1080/10503307.2018.1506949
26. Cavelti M, Homan P, Vauth R. The impact of thought disorder on therapeutic alliance and personal recovery in schizophrenia and schizoaffective disorder: an exploratory study. Psychiatry Res. 2016;239:92–98. doi:10.1016/j.psychres.2016.02.070
27. Ajzen I. From intentions to actions: a theory of planned behavior. In: Action Control. Springer; 1985:11–39.
28. Surmann M, Falke S, von Gruchalla L, et al. Understanding the multidimensional phenomenon of medication adherence attitudes in psychosis. Psychiatry Res. 2021;295:113601. doi:10.1016/j.psychres.2020.113601
29. Zheng Y, Ning Y, She S, et al. Psychotic symptoms and attitudes toward medication mediate the effect of insight on personal-social functions in patients with schizophrenia: one-year randomized controlled trial and follow-up. Psychopathology. 2018;51(3):167–176. doi:10.1159/000486558
30. Cohen J. Statistical Power Analysis for the Behavioral Sciences. New York: Academic press; 2013.
31. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5. Washington: American psychiatric association; 2013.
32. Sonesson O, Tjus T, Arvidsson H. Reliability of a functioning scale (GAF) among psychiatric ward staff. Nord Psychol. 2010;62(1):53–64. doi:10.1027/1901-2276/a000005
33. Crippa JA, Sanches RF, Hallak JE, et al. Factor structure of Bech’s version of the brief psychiatric rating scale in Brazilian patients. Braz J Med Biol Res. 2002;35(10):1209–1213. doi:10.1590/S0100-879X2002001000014
34. Lee SM Factors associated with the results from psychiatric rehabilitation training for residents in community halfway houses in Taipei; 2013. Available from: https://hdl.handle.net/11296/drdfzc.
35. Chang T, Hwu H, Wei F. The inter-rater reliability of brief psychiatric rating scale (BPRS). Chin Soc Neurol Psychiatry Bull. 1986;12:29–36.
36. Tsai SL, Hsieh MH, Shiau SJ, Chen WJ, Hwu HG. Chinese version of the scale to assess unawareness of mental disorder: reliability, validity and clinical correlates. Taiwanese J Psychiatry. 2000;14:192–203.
37. Yen CF, Yeh ML, Chong MY, Chung HH, Chen CS. A multidimensional assessment of insights in schizophrenic patients. Kaohsiung J Med Sci. 2001;17(5):253–260.
38. Tracey TJ, Kokotovic AM. Factor structure of the working alliance inventory. J Consult Clin Psychol. 1989;1(3):207–210.
39. Paap D, Dijkstra PU. Working alliance inventory-short form revised. J Physiother. 2017;63(2):118. doi:10.1016/j.jphys.2017.01.001
40. Cookson A, Daffern M, Foley F. Relationship between aggression, interpersonal style, and therapeutic alliance during short-term psychiatric hospitalization. Int J Ment Health Nurs. 2012;21(1):20–29. doi:10.1111/j.1447-0349.2011.00764.x
41. Hegedüs A, Kozel B, Fankhauser N, Needham I, Behrens J. Outcomes and feasibility of the short transitional intervention in psychiatry in improving the transition from inpatient treatment to the community: a pilot study. Int J Ment Health Nurs. 2018;27(2):571–580. doi:10.1111/inm.12338
42. Moreno-Poyato AR, Delgado-Hito P, Suárez-Pérez R, Lluch-Canut T, Roldán-Merino JF, Montesó-Curto P. Improving the therapeutic relationship in inpatient psychiatric care: assessment of the therapeutic alliance and empathy after implementing evidence-based practices resulting from participatory action research. Perspect Psychiatr Care. 2018;54(2):300–308.
43. Nielsen RE, Lindström E, Nielsen J, Levander S. DAI-10 is as good as DAI-30 in schizophrenia. Eur Neuropsychopharmacol. 2012;22(10):747–750. doi:10.1016/j.euroneuro.2012.02.008
44. Cheng HL, Yu YW. Validation of the Chinese version of “the Drug Attitude Inventory”. Kaohsiung J Med Sci. 1997;13(6):370–377.
45. Thompson K, Kulkarni J, Sergejew AA. Reliability and validity of a new Medication Adherence Rating Scale (Mars) for the psychoses. Schizophr Res. 2000;42(3):241–247. doi:10.1016/S0920-9964(99)00130-9
46. Kao YC, Liu YP. Compliance and schizophrenia: the predictive potential of insight into illness, symptoms, and side effects. Compr Psychiatry. 2010;51(6):557–565. doi:10.1016/j.comppsych.2010.03.007
47. Hayes AF. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach. New York: Guilford publications; 2017.
48. Beck EM, Cavelti M, Kvrgic S, Kleim B, Vauth R. Are we addressing the ‘right stuff’ to enhance adherence in schizophrenia? Understanding the role of insight and attitudes towards medication. Schizophr Res. 2011;132(1):42–49. doi:10.1016/j.schres.2011.07.019
49. Pothimas N, Tungpunkom P, Kanungpiarn T, Hannes K. Experiences of medication adherence among people with schizophrenia: a qualitative systematic review. Pac Rim Int J Nurs Res. 2021;25(2):229–241.
50. Wittorf A, Jakobi U, Bechdolf A, et al. The influence of baseline symptoms and insight on the therapeutic alliance early in the treatment of schizophrenia. Eur Psychiatry. 2009;24(4):259–267. doi:10.1016/j.eurpsy.2008.12.015
51. Pec O. Stages of recovery in psychosis: converging qualitative research and psychoanalysis. Perspect Psychiatr Care. 2020;56(4):760–767. doi:10.1111/ppc.12490
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.