Back to Journals » Clinical Interventions in Aging » Volume 14
Improvements in oral functions of elderly after simple oral exercise
Authors Kim HJ, Lee JY ![]() , Lee ES, Jung HJ, Ahn HJ, Kim BI
, Lee ES, Jung HJ, Ahn HJ, Kim BI ![]()
Received 13 February 2019
Accepted for publication 6 April 2019
Published 16 May 2019 Volume 2019:14 Pages 915—924
DOI https://doi.org/10.2147/CIA.S205236
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Hyo-Jung Kim,1 Joo-Young Lee,1 Eun-Song Lee,1 Hyo-Jung Jung,2 Hyung-Joon Ahn,2 Baek-Il Kim1
1Department of Preventive Dentistry & Public Oral Health, Brain Korea 21 PLUS Project, Yonsei University College of Dentistry, Seoul, Republic of Korea; 2Department of Orofacial pain & Oral medicine, Yonsei University College of Dentistry, Seoul, Republic of Korea
Purpose: Conventional oral exercises in previous studies are considered impractical for continuous use in the elderly because of the extended duration needed for effective outcomes. Therefore, in the present study, a simple oral exercise (SOE) was developed to reduce performance time, focusing on improvements in mastication, salivation, and swallowing functions. The aim of this study was to determine the short-term effects of the SOE with respect to improving mastication, salivation, and swallowing function in elderly subjects ≥65 years of age.
Patients and methods: The study included 84 subjects, all of whom performed the SOE 2 times per day for 1 week. Masticatory performance was assessed using the mixing ability index (MAI). Unstimulated saliva and the degree of moisture of the tongue/buccal mucosa were evaluated, and the repetitive saliva swallowing test was performed. On the basis of each of these four measurements, subjects were dichotomized into two groups with high (good) and low (poor) conditions. The same evaluations were conducted before and immediately after intervention, as well as after 1 week of intervention. A subjective evaluation with questionnaires was performed after 1 week of intervention. The changes were analyzed using repeated-measures ANOVA, Cochran’s Q test, and McNemar’s test.
Results: The mean MAI increased by 6% immediately after the intervention, and by 16% in the poor-chewing group. Similarly, the amount of unstimulated saliva increased by 0.1 ml/min immediately after the SOE, and by 29% in the poor-salivation group. The degree of tongue moisture increased by 3% and was maintained. In the poor-swallowing group, 25% and 40% of the subjects were upgraded to the good-swallowing group immediately after intervention, as well as after 1 week of intervention, respectively. The subjects experienced less discomfort as their oral function improved.
Conclusion: The SOE was effective in immediately improving oral functions, and improvement was maintained for 1 week.
Keywords: deglutition disorders, elderly, mastication, oral exercise, salivation, xerostomia
Introduction
Oral health is closely related to systemic health, and poor oral health can lead to deterioration of systemic disease.1 Impaired oral health affects dietary habits, nutrition, sleep, mental status, and social relationships.2 It is important for elderly individuals to improve and/or maintain oral function because this population exhibits various risk factors that threaten oral function; moreover, such individuals are susceptible to various diseases based on aging-related changes in bodily functions.3
Among oral symptoms, decreased salivation in the elderly may cause various diseases, such as oral soft tissue disease, dental caries, periodontal disease, and oral candidiasis.4 In addition, xerostomia—the subjective sensation of dry mouth—can cause speech and mastication problems, as well as dysphagia, thus reducing quality of life.5,6 Therefore, measures to alleviate hyposalivation and xerostomia should be implemented to improve quality of life and overall health in old age. However, chemical agents used to relieve dry mouth may cause side effects and often require a prescription.7
Furthermore, masticatory and swallowing functions in the elderly are closely related to general nutritional status and quality of life. As the first step in the digestive process, mastication has been reported to affect both physical and mental health, and is a major factor in maintaining a healthy diet.8–10 A decline in swallowing function may lead to severe pneumonia or respiratory disease.11 However, masticatory and swallowing functions can be restored through muscle-strengthening activities and rehabilitation.11,12 Several previous studies have reported that restoration of masticatory function can be achieved by improving muscular strength; notably, the effects of physical oral exercises (similar to those proposed by Hakuta et al13) have been described.13–16
Thus, oral exercise has been introduced to improve weakened oral function in the elderly. Oral exercise is part of a rehabilitation strategy initiated in Japan in 2002.17 The program is easy to teach and follow, and includes oral stretching and exercise. The program was introduced in Korea by Cho et al17 in 2012, with some modifications based on Korean situation; subsequently, it has been widely used to improve oral health in the elderly, both in public health and in dental clinics. Several previous studies have reported improvements in salivation, relief of oral dryness, swallowing function, subjective chewing ability, and oral health-related quality of life, on the basis of follow-up 3–6 months later.13,16–19 Most studies have evaluated only the long-term effects of the program because they were performed in community-based programs at senior citizens’ centers. However, individuals experiencing mouth discomfort may expect that their oral function will recover rapidly after any intervention. Therefore, continuous progress can be facilitated by short-term improvement of oral function through oral exercise, which then further motivates patients. Second, time can an important factor in the maintenance of continuous engagement in oral exercises. Notably, the oral exercise programs that were used in previous studies involved only physical exercise, without oral health education, for ≥20 min.17 Therefore, there may have been practical limitations that impacted the abilities of elderly individuals to continuously perform these exercises.
Accordingly, in the present study, a simple oral exercise (SOE) was developed to reduce oral exercise performance time to and be completed in approximately 2 min, focusing on improvement in mastication, salivation, and swallowing functions. We attempted to design the SOE intervention to produce immediate improvements in oral functions; this would enable it to be used as a preparatory exercise before meals, thereby providing elderly subjects with adequate nutrition by reducing their discomfort during eating. We also expect that the SOE might be useful as an early intervention to prevent aspiration pneumonia, which is the most common cause of death in the elderly population.19,20 In the present study, oral functions related to nutrition intake in the elderly were classified into three factors: mastication, salivation, and swallowing; each was evaluated using objective measurements. In particular, we aimed to evaluate masticatory function more precisely and objectively using a wax cube, which aids in simulation of the actual masticatory process. The primary aim of this study was to evaluate the immediate effects of the SOE on mastication, salivation, and swallowing function in elderly individuals ≥65 years of age.
Material and methods
Participants
This was a short-term interventional study of elderly individuals ≥65 years of age who were recruited from a senior citizens’ center located in a metropolitan area of Korea between April 2017 and June 2017. The number of subjects at baseline was 116, and denture wearers were included. Edentulous individuals who did not wear dentures and those who had been diagnosed with severe periodontal disease through oral examinations were excluded. Those who received dental treatment during the study period, or who had incomplete data collection, were also excluded from the analysis. A total of 84 subjects were included in the final analysis. The average number of present teeth in the subjects was 18.1±8.4 at baseline. No patients were treated for Sjögren’s syndrome, had received therapeutic irradiation, or were on medications, such as antidepressants, psycholeptics, or those used to treat urinary incontinence; all of these factors have been related to suppression of salivation.21
All subjects received written and oral explanations describing the purpose and methods of the study, as well as confidentiality practices and their ability to withdraw from the study; they all then provided written informed consent. This study was conducted in compliance with the Declaration of Helsinki and approved by the Institutional Review Board of Yonsei University (Seoul, Korea; No. 2–2016-0034).
Simple oral exercise (SOE)
SOE training was provided by one trained dental hygienist. The SOE intervention was performed for approximately 2 min after simple oral health education. The SOE intervention included only exercises for mastication, salivation, and swallowing from among the exercises modified by Cho et al17 which included lip stretching, tongue stretching, cheek stretching, masticatory muscle exercise, and swallowing movements. Subjects were instructed to perform the SOE intervention as preparation before meals at home each day. A leaflet illustrating the motion was distributed to all subjects, who performed the SOE intervention 2 times per day. The training was conducted in groups of five subjects.
Study protocol
The study was performed at the Dental Hospital of Yonsei University of College of Dentistry. Evaluations of oral functions were conducted before the intervention. The same assessments of oral functions were performed immediately after the intervention, as well as after 1 week of intervention, to examine both temporary effect and short-term effects of the SOE intervention. After 1 week of home-care, subjective assessment was measured along with evaluation of oral functions.
Subjective measurement
Sociodemographic characteristics were surveyed. In addition, modified questionnaires described by Torres et al22 and Fox et al23 were implemented using “yes“ and ”no” nominal scales, in order to assess discomfort in mastication, swallowing, and dry mouth. Two researchers reviewed the details of each questionnaire to ensure comprehension among subjects.
Objective measurement
Subjects were divided into one of two groups―good and poor function―using appropriate criteria for each oral function (mastication, salivation, and swallowing function). Each oral function was evaluated according to the degree of change in each group.
Evaluation of masticatory performance
The mixing ability index (MAI), which is an objective evaluation of masticatory function previously described by Sato et al,24 was calculated using a modified method described by Jeong et al25 MAI was significantly correlated with the sieving method, which has been used as a “gold standard” assessment of masticatory performance.26 Two-color wax cubes (12×12×12 mm3 [made from red and green utility wax rods]) were used as artificial food. Each subject was provided with two wax cubes and required to chew one cube for 10 strokes in a habitual manner. The chewed wax samples were rinsed with water and dried at room temperature.
Dried specimens were photographed on both sides using a digital single-lens reflex camera (D80, Nikon Co., Tokyo, Japan) under standardized conditions of distance and light. All images were saved as JPEG files and analyzed using an image analysis program (Image-Pro plus® version 6.0, Media Cybernetics Inc., Bethesda, MD, USA). In each image, the total area of the specimen, area with ≤50 μm thickness, the maximum length and the maximum width, and area without color mixing were calculated. Using the above variables, the MAI was determined, in accordance with the method used in previous studies:25,27 namely, MAI was analyzed for each specimen and calculated.27 The average MAI of two specimens was then used as a representative value. The MAI score was calculated on a scale of 0–100 points. A higher score indicated better chewing performance. Specimens that were excessively crushed or torn were excluded from analysis. Only 73 of 84 subjects were evaluated. To compare relative masticatory performance among subjects, they were classified into good and poor chewing groups, based on median MAI.
Evaluation of oral dryness
Moisture of the tongue and buccal mucosa was measured using an oral moisture-checking device (Moisture Checker Mucus®, Life Co, Ltd, Tokyo, Japan), which has good sensitivity and specificity.28 A disposable polyethylene cover was applied to the sensor and replaced for each subject. For accurate measurement, one trained examiner manually applied the device to measurement sites at a pressure of approximately 200 g, in accordance with the manufacturer’s instructions. The measurement sites were the lingual mucosa, approximately 10 mm from the tip of the tongue, and the right buccal mucosa, approximately 10 mm from the mouth corner; these sites were described by Fukushima et al29 To reduce error in measurement, the same areas were measured three times and the median value was used as the representative value.
According to a previous publication by the American Dental Association, the ideal method to diagnose hyposalivation is measurement of salivary flow.30 Unstimulated saliva was collected by spitting naturally collected saliva once per minute for 5 min into a test tube; during collection, subjects remained in a stable sitting position. Eating, drinking, and smoking were prohibited 1 h before unstimulated saliva collection. Evaluation after intervention was measured immediately after the SOE intervention. To compare the degree of change according to salivation status, a flow rate of ≤0.2 ml of unstimulated saliva per minute was defined as hyposalivation and used to distinguish between good and poor salivation groups.31
Repetitive Saliva Swallowing Test (RSST)
RSST is a method to evaluate swallowing ability, which has demonstrated good accuracy.32 Subjects were seated comfortably and asked to swallow their saliva continuously and as much as possible for 30 s. During this swallowing task, one trained dentist palpated the laryngeal prominence and elevations of the hyoid bone, and recorded the number of movements. In accordance with criteria reported in previous studies,11,16 < 3 times was defined as swallowing hypofunction and used to distinguish between good and poor swallowing groups.
Statistical methods
Changes in oral function immediately after intervention, as well as after 1 week of intervention, were analyzed using one-way repeated measures ANOVA. The Bonferroni post hoc test was performed to determine differences among the time points. Cochran’s Q test was used to compare changes in the proportions of good- and poor-swallowing subjects after interventions in the poor- and good-swallowing groups, respectively. Subjective changes after 1 week of intervention were analyzed using McNemar’s test.
Results
Participant characteristics
The mean age of the subjects was 74.43 years (Table 1). The subjects were grouped on the basis of their use of removable partial dentures and complete dentures; notably, most (65.5%) of the subjects did not wear dentures. Based on the Asia-Pacific standard for body mass index (BMI),33 most subjects were obese (≥25 kg/m2); most non-obese subjects had a normal BMI (≤22.9 kg/m2).
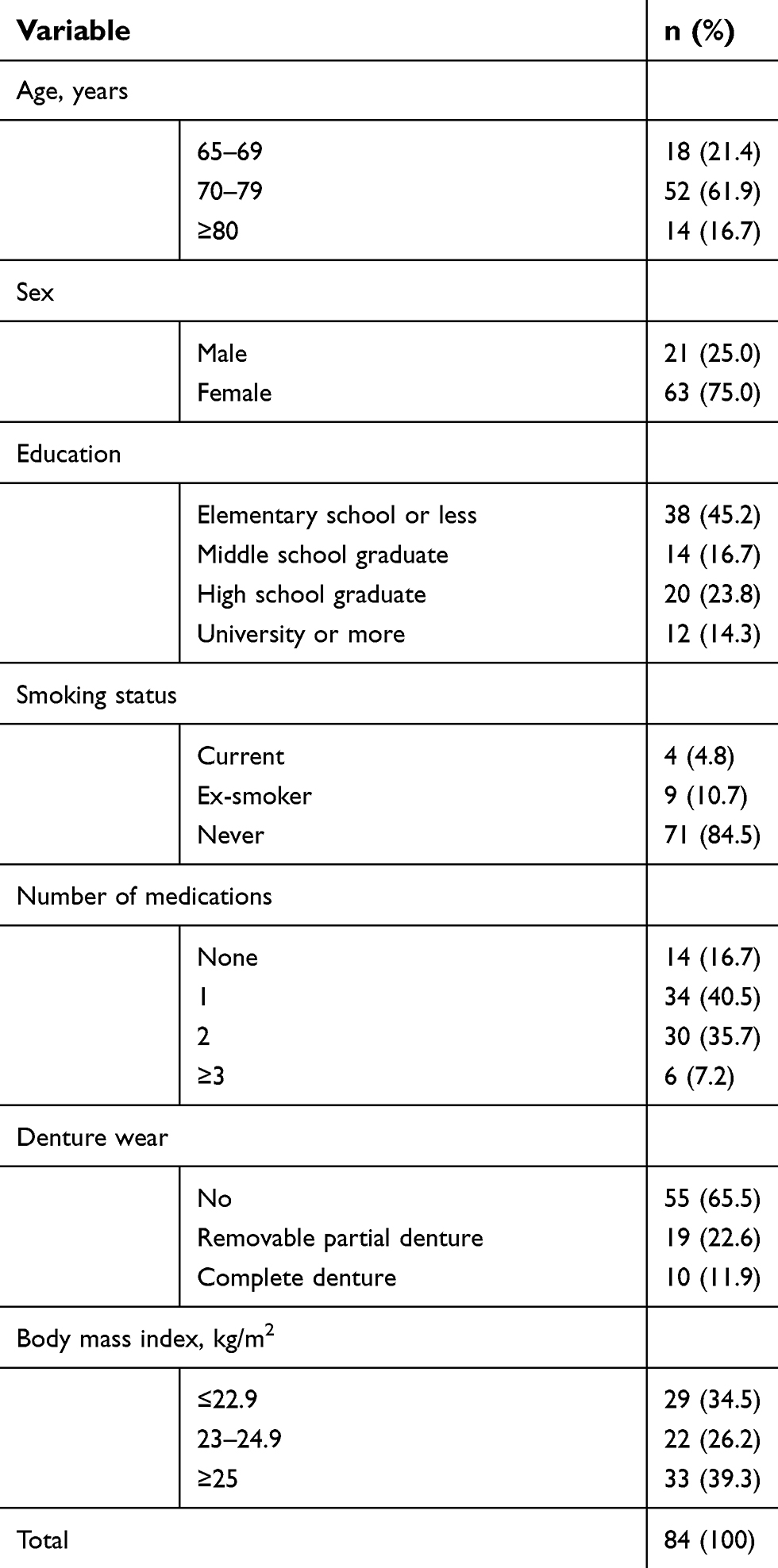 | Table 1 Participant characteristics |
Changes immediately after intervention and after 1 week of intervention in all subjects
In total, 45.2% or 16.7% of subjects completed the SOE intervention over 7 or 6 days, respectively. In addition, 4.8% of the subjects performed the SOE intervention for <4 days. The MAI increased by approximately 6%, immediately after the intervention (Table 2). Although there was no statistically significant increase in unstimulated saliva flow rate immediately after the SOE intervention, it increased by approximately 0.1 ml/min after 1 week of intervention. The degree of tongue moisture increased significantly (by approximately 3%), immediately after the intervention; this increase was maintained after 1 week of intervention (P=0.005). The degree of buccal mucosa moisture also increased significantly, immediately after the SOE intervention (P=0.023). The proportion of subjects that comprised the good-swallowing group significantly increased by approximately 9% and 15%, immediately after and after 1 week of SOE, respectively (P=0.003).
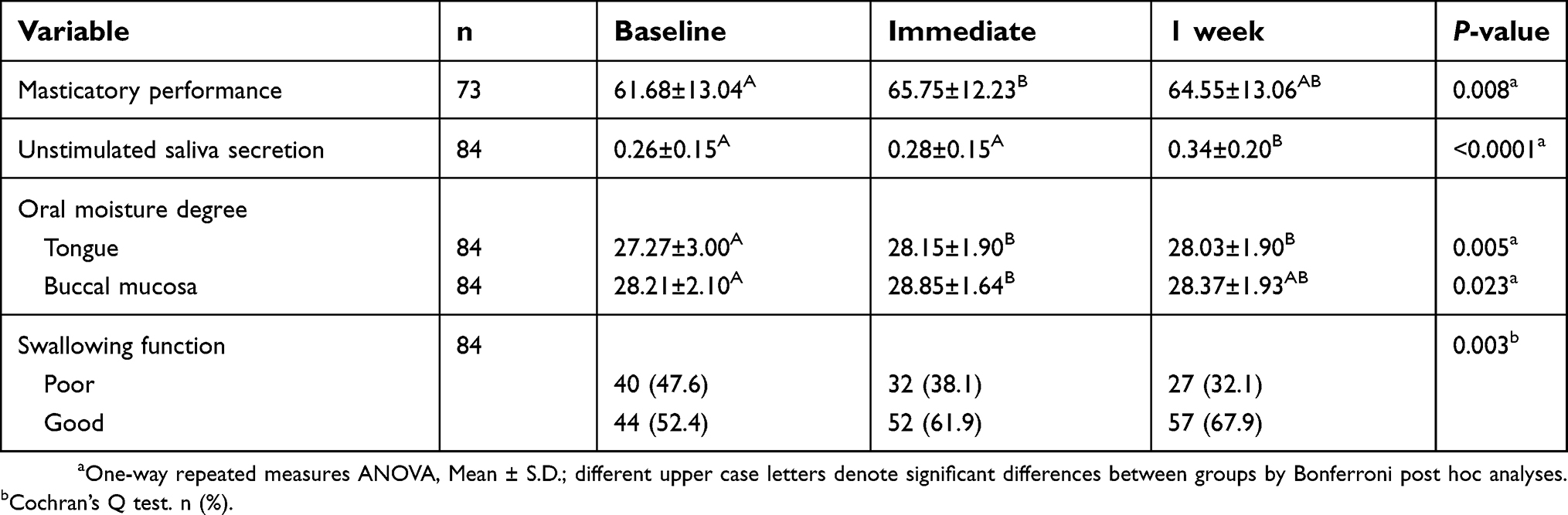 | Table 2 Changes in oral functions across all subjects after simple oral exercise intervention |
Changes immediately after and after 1 week of intervention in the good- and poor- groups
In a comparison between good- and poor- chewing groups, the average number of teeth at baseline significantly differed between the good-chewing group (21.5±6.9) and poor-chewing group (16.4±8.2). Masticatory performance did not change significantly after the intervention in the good-chewing group (n=36), whereas it increased by 16% immediately after the intervention in the poor-chewing group (n=37); this increase was maintained after 1 week of intervention (P<0.05) (Table 3). The volume of unstimulated saliva was the same before and immediately after SOE in the good-salivation group (n=48), whereas it increased by approximately 29% immediately after the intervention, and by 78% after 1 week of intervention in the poor-salivation group (n=36). The intervention had no effect on the degree of tongue moisture in the good-salivation group; however, tongue moisture was significantly improved by approximately 5% immediately after SOE in the poor-salivation group. In total, 93.2% of subjects in the good-swallowing group retained their good-swallowing function after SOE (Table 3). Additionally, 25% and 40% of those initially in the poor-swallowing group improved to the normal range immediately after, and after 1 week of SOE, respectively.
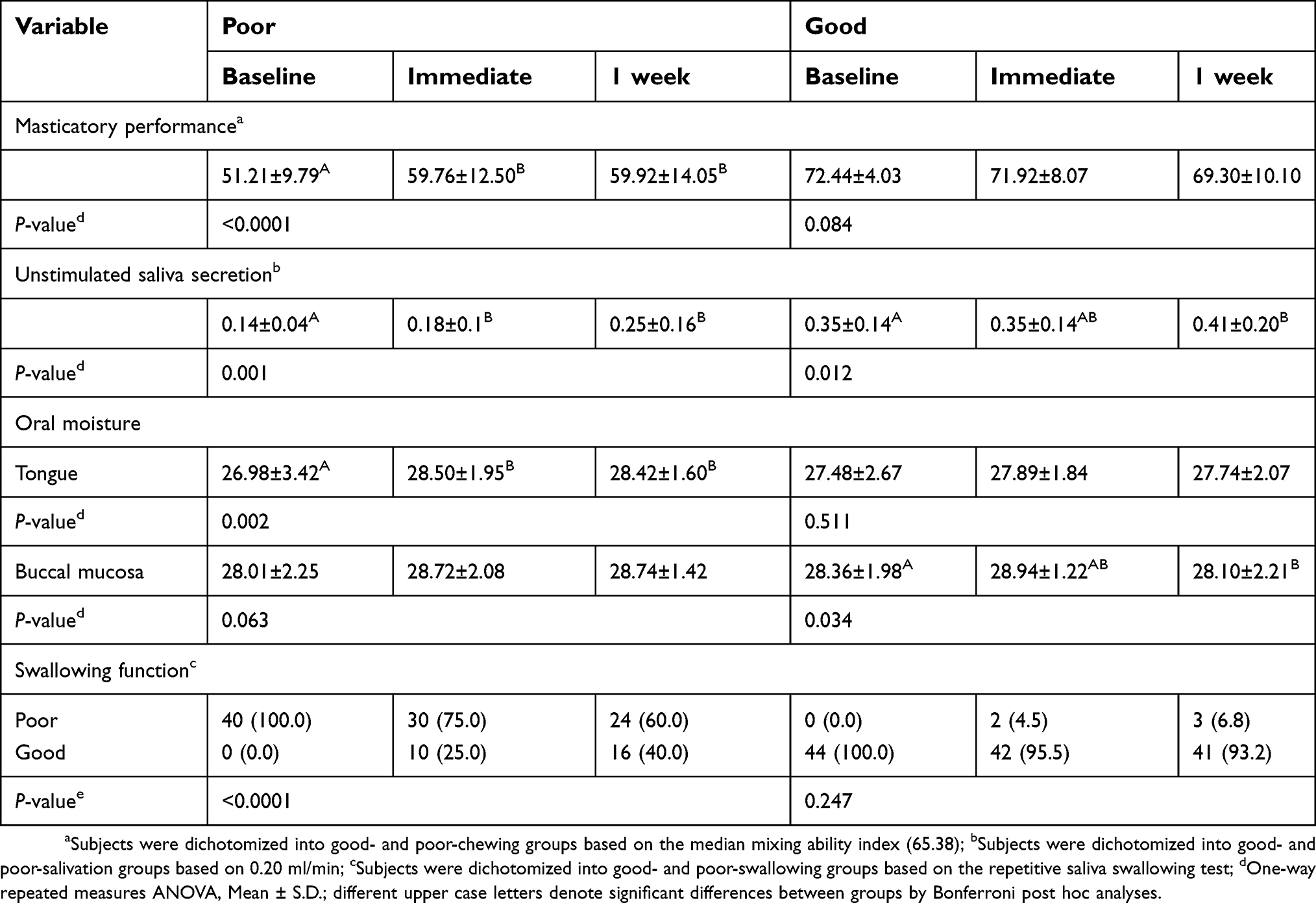 | Table 3 Changes in oral functions after performing simple oral exercise intervention, according to oral functional abilities |
Changes in subjective discomfort
Before SOE intervention, 46.4% of subjects answered “yes” to subjective difficulties in chewing hard food (Table 4). After 1 week, however, only 22.6% of the subjects answered “Yes” to this question; this difference was statistically significant (P<0.0001). The number of the subjects who answered “yes” to “Aspiration when drinking liquid” decreased by approximately 20% (P=0.002). With respect to oral dryness, subjects who experienced difficulties with swallowing food due to oral dryness and those who needed liquids to swallow dry foods were reduced by approximately 4% and 10%, respectively; however, these differences were not statistically significant. In contrast, there was a statistically significant decrease in the feeling of mouth dryness when eating a meal (P=0.049).
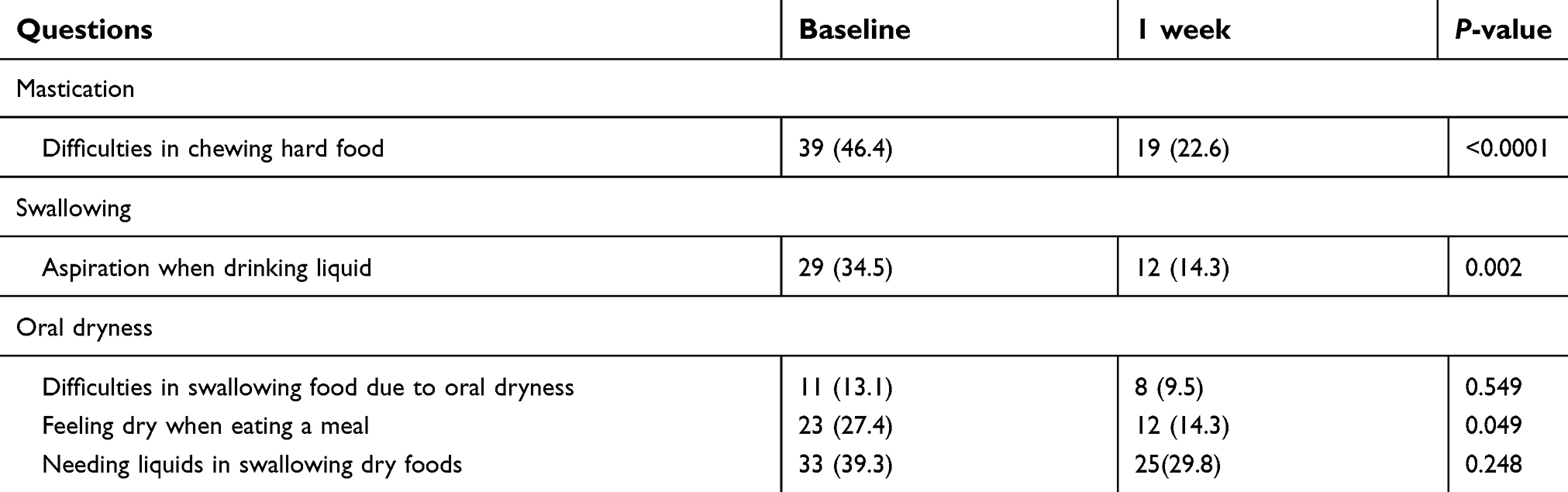 | Table 4 Changes in the numbers of subjects who experienced discomfort after performing simple oral exercise intervention |
Discussion
In this study, the SOE intervention focused on enhancing mastication, salivation, and swallowing function; notably, the intervention was immediately effective in improving oral function. We confirmed that improved oral functions were maintained over the short study period of 1 week. In general, it is not recommended to provide a large amount of information to elderly individuals in a single session because this population often requires additional time to comprehend instructions and recall information, due to aging.34 Therefore, an SOE intervention with several key motions is preferred over a conventional, complex oral exercise method; moreover, the new method can be performed continuously because it is easier for elderly individuals to remember, and appears to be highly utilized.
Most previous studies have been limited to evaluation of changes in subjective masticatory ability after oral exercise. However, the evaluation of subjective chewing abilities is affected by other factors, such as adaptational and psychological factors; thus, subjective evaluations are generally optimistic.35 In the present study, we evaluated changes in objective masticatory performance by using the MAI, as well as by simultaneous assessment of subjective masticatory ability. The MAI reflected changes in masticatory performance with high sensitivity, similar to several previous studies that successfully evaluated masticatory function in patients with temporomandibular disorder, botulinum toxin injection, orthodontic patients, and those receiving implants.27,36–38 In the present study, the mean MAI of all subjects was 61.68, which was similar to the MAI in the 20–30-year-old age group in a previous study.25 However, the prior study may have included only healthy individuals who could travel to the hospital alone, because it was conducted at a dental hospital. In addition, the poor-chewing group, which was classified as below the median in this study, was also in the relatively poor group, such that the baseline mean MAI was similar to that of subjects who were ≥60 years of age or those who had 1–2 lost teeth in a previous study.25
The present study demonstrated that masticatory performance in the poor-chewing group immediately improved by approximately 16% after SOE intervention. Approximately 64–69 MAI was the normal range of masticatory performance through the occlusion of all molars, based on previous studies using the MAI. The subjects with increased masticatory performance after the intervention did not reach the normal range. However, the increased values were higher than those in subjects without 1–2 molars; this change may be sufficient for robust oral intake. There was also a nine-point difference in MAI between healthy subjects and those without 1–2 molars, which was similar to the increase in MAI after the SOE intervention.25 The number of teeth plays a major role in the masticatory system and is known to be closely related to chewing ability.35 Although there was no increase in the number of functional teeth during the intervention period, the SOE intervention yielded a similar improvement in function in the short-term, compared with the group with all posterior teeth.25
In contrast, there was little change after SOE in the good-chewing group. Painter et al39 reported that the effect of the exercise might be particularly noticeable in low functioning subjects because the intervention was designed to address physical functioning. Some previous studies reported that exercise was ineffective or less effective in normal subjects than in the low functioning subjects.40,41 Similarly, in the present study, the good-chewing group, which exhibited the reference score of the general population (64–69) showed only a slight increase or decrease. However, we could not determine whether an effect occurred because we did not include a control group in the present study. Thus, our results should be interpreted carefully because the observed effects could be caused by statistical errors (eg, regression to the mean effect).
Previous studies have reported that repeated tooth-clenching tasks or short-term oral sensorimotor tasks can cause neuroplastic changes in corticomotor control of the masseter muscles over a short period of time, resulting in increased precision of task performance.42,43 These results suggest that SOE may induce neuroplastic changes and improve masticatory performance by improvement of dexterity. Furthermore, Simona et al15 observed an increase in masseter muscle activity enhanced by physical exercise over a 6-month period. In addition, maximum mouth-opening distance and bite force were increased after oral exercise at 3 months and 6 months, respectively.17,29 These results suggest that the SOE intervention can improve masticatory function through enhancement of masticatory muscle activity over a longer period of time.
In the present study, we observed a significant increase in the unstimulated saliva flow rate after the SOE intervention. The rate of unstimulated saliva production in all subjects increased to 0.26 ml/min immediately after the intervention and to 0.34 ml/min at 1 week after the intervention. These results are very similar to those reported in a previous study by Sugiyama et al,11 in which the rate of unstimulated saliva increased from 0.25 ml/min to 0.37 ml/min after a 3-month period of oral exercise. The present study was the first to reveal the unique phenomenon that salivation could be improved to a level similar to long-term performance of approximately 3 months, even during a short-term period of 1 week when the SOE intervention was performed every day. The motions for salivation in the SOE intervention included stretching the tongue up and down, as well as right and left, along with stimulation of the buccal mucosa and oral vestibule. The sublingual ducts and parotid papilla were stimulated by performing these motions; thus, saliva secretion was immediately increased. The interesting result observed in this study was that the amount of unstimulated saliva did not increase immediately after the SOE intervention in the good-salivation group, whereas it increased by approximately 29% in the poor-salivation group. In addition, the amount of unstimulated saliva increased by approximately 39% upon re-evaluation after 1 week of intervention, which was consistent with the increase in the 3-month oral exercise described by Ohara et al.19 Moreover, the increase after 1 week of the SOE intervention was in the normal range of the rate of unstimulated saliva production (0.2–0.5 ml/min).44 In addition, the number of subjects who experienced discomfort with oral dryness during food intake was markedly decreased in the subjective symptom survey, suggesting that the SOE intervention proposed in the present study was effective in improving salivation in elderly individuals with decreased salivation. Therefore, the amount of saliva can be temporarily increased by the SOE intervention as a preparatory exercise immediately before food intake, which may help to relieve masticatory and swallowing discomfort.
The degree of moisture in both the tongue and buccal mucosa also exhibited a statistically significant increase immediately after the intervention, with a greater effect on the tongue mucosa. This is consistent with the findings of a previous study by Hakuta et al,13 in which tongue dryness was relieved by oral exercise over a 3-month period. In the present study, the degree of tongue moisture in the poor-salivation group was increased immediately after intervention, while there was no significant change in the good-salivation group. This tendency was consistent with improvement in other oral functions, as mentioned above. Conversely, the degree of moisture in the buccal mucosa was not affected in the poor-salivation group. This may be because the measurement site of the buccal mucosa was located near the parotid papilla, and recorded values may vary depending on the measurement site. According to a previous study, the tongue mucosa is more suitable for measurement using an oral moisture-checking device than the buccal mucosa;29 therefore, results addressing the degree of moisture in the tongue mucosa in the present study may be more reliable than those collected in the buccal mucosa. After 1 week of intervention, many subjects reported that their mouth (ie, oral mucosa) had become soft. The results of the subjective evaluation suggest that moisture in the oral mucosa increased slightly with an increase in unstimulated saliva after the SOE intervention.
RSST assessment indicated that 25% and 40% of the subjects in the poor-swallowing group experienced improvements in swallowing function to within the normal range (RSST >3) immediately after, and after 1 week of intervention, respectively. The present study found that swallowing function in elderly individuals with poor swallowing ability could improve to within the normal range after a short period of time, both immediately after and after 1 week of intervention. Ibayashi et al18 reported that the baseline RSST score in subjects with good-swallowing ability was 4 points, and that this increased to 5 points by the end of a 6-month intervention. In the present study, swallowing function did not improve after 1 week in the good-swallowing group. Nevertheless, if the SOE intervention is performed for an extended period, improvements in swallowing ability may also occur in elderly individuals with good swallowing function. There was a statistically significant reduction in subjective discomfort during eating, with respect to mastication, salivation, and swallowing function, in responses to most interview questions. There was a possibility that false positives were recorded because the same questionnaire was administered after a short interval of 1 week. Nevertheless, objective numerical changes were observed according to test results of oral function; therefore, an actual relaxation in oral function may have occurred. In addition, approximately 70% of subjects were asked about their feelings regarding the SOE intervention with an open question. Most subjects responded positively, and most responses were “the motion was not difficult,” followed by “the mouth was softened and the saliva is well secreted.” Therefore, many subjects appeared to have experienced a salivation effect after performing the SOE intervention. It is expected that the SOE intervention will be performed continuously in the future because it was regarded as highly favorable.
The SOE intervention instruction in this study had the advantage of not being affected by multiple educators; therefore, educator differences were minimized, if not eliminated. The purpose of this study was to investigate the feasibility of using the SOE intervention as a pre-meal exercise; we acknowledge that the 1-week follow-up period was relatively short, compared with other studies involving periods of at least 3–6 months of intervention. Nevertheless, our results were clinically meaningful. In addition, there was no control group because all oral functions were evaluated immediately after the intervention. Therefore, it was not possible to directly compare the oral function of subjects who performed the SOE intervention and those who did not perform any intervention. In the future, a study is needed to overcome those limitations.
All oral functions involving mastication, salivation, and swallowing were particularly more effective in the relatively poor groups than in the relatively good groups. Therefore, it will be necessary to evaluate the effect of the SOE intervention in a target group with weak oral function in the future.
Conclusion
In conclusion, the SOE intervention was immediately effective in improving oral functions, and the increased functions were maintained after 1 week of intervention. It is recommended that elderly people with poor oral functions perform the SOE intervention before each meal.
Acknowledgments
This work was supported by the Korea Institute of Planning and Evaluation for Technology in Food, Agriculture, Forestry and Fisheries (IPET) through the High Value-added Food Technology Development Program, funded by the Ministry of Agriculture, Food and Rural Affairs (MAFRA) (316071031HD020).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tavares M, Lindefjeld Calabi KA, San Martin L. Systemic diseases and oral health. Dent Clin North Am. 2014;58(4):797–814. doi:10.1016/j.cden.2014.07.005
2. Helgeson MJ, Smith BJ, Johnsen M, Ebert C. Dental considerations for the frail elderly. Spec Care Dentist. 2002;22(3 Suppl):40s–55s.
3. De Rossi SS, Slaughter YA. Oral changes in older patients: a clinician‘s guide. Quintessence Int. 2007;38(9):773–780.
4. Turner MD, Ship JA. Dry mouth and its effects on the oral health of elderly people. J Am Dent Assoc. 2007;138:S15–S20. doi:10.14219/jada.archive.2007.0358
5. Anil S, Vellappally S, Hashem M, Preethanath RS, Patil S, Samaranayake LP. Xerostomia in geriatric patients: a burgeoning global concern. J Investig Clin Dent. 2016;7(1):5–12. doi:10.1111/jicd.12120
6. Gerdin EW, Einarson S, Jonsson M, Aronsson K, Johansson I. Impact of dry mouth conditions on oral health‐related quality of life in older people. Gerodontology. 2005;22(4):219–226.
7. Han P, Suarez-Durall P, Mulligan R. Dry mouth: a critical topic for older adult patients. J Prosthodont Res. 2015;59(1):6–19. doi:10.1016/j.jpor.2014.11.001
8. Kwon SH, Park HR, Lee YM, et al. Difference in food and nutrient intakes in Korean elderly people according to chewing difficulty: using data from the Korea national health and nutrition examination survey 2013 (6th). Nutr Res Pract. 2017;11(2):139–146. doi:10.4162/nrp.2017.11.2.139
9. Kim EK, Lee SK, Choi YH, et al. Relationship between chewing ability and cognitive impairment in the rural elderly. Arch Gerontol Geriatr. 2017;70:209–213. doi:10.1016/j.archger.2017.02.006
10. Miura H, Miura K, Mizugai H, Arai Y, Umenai T, Isogai E. Chewing ability and quality of life among the elderly residing in a rural community in Japan. J Oral Rehabil. 2000;27(8):731–734.
11. Sugiyama T, Ohkubo M, Honda Y, et al. Effect of swallowing exercises in independent elderly. Bull Tokyo Dent Coll. 2013;54(2):109–115.
12. Argolo N, Sampaio M, Pinho P, Melo A, Nobrega AC. Do swallowing exercises improve swallowing dynamic and quality of life in parkinson‘s disease? NeuroRehabilitation. 2013;32(4):949–955. doi:10.3233/NRE-130918
13. Hakuta C, Mori C, Ueno M, Shinada K, Kawaguchi Y. Evaluation of an oral function promotion programme for the independent elderly in Japan. Gerodontology. 2009;26(4):250–258. doi:10.1111/j.1741-2358.2008.00269.x
14. Sakayori T, Maki Y, Ohkubo M, Ishida R, Hirata S, Ishii T. Longitudinal evaluation of community support project to improve oral function in Japanese elderly. Bull Tokyo Dent Coll. 2016;57(2):75–82. doi:10.2209/tdcpublication.2015-0035
15. Tecco S, Baldini A, Mummolo S, et al. Frenulectomy of the tongue and the influence of rehabilitation exercises on the sEMG activity of masticatory muscles. J Electromyogr Kinesiol. 2015;25(4):619–628. doi:10.1016/j.jelekin.2015.04.003
16. Sakayori T, Maki Y, Hirata S, Okada M, Ishii T. Evaluation of a Japanese “Prevention of long-term care” project for the improvement in oral function in the high-risk elderly. Geriatr Gerontol Int. 2013;13(2):451–457. doi:10.1111/j.1447-0594.2012.00930.x
17. Cho EP, Hwang SJ, Clovis JB, Lee TY, Paik DI, Hwang YS. Enhancing the quality of life in elderly women through a programme to improve the condition of salivary hypofunction. Gerodontology. 2012;29(2):e972–980. doi:10.1111/j.1741-2358.2011.00594.x
18. Ibayashi H, Fujino Y, Pham T-M, Matsuda S. Intervention study of exercise program for oral function in healthy elderly people. Tohoku J Exp Med. 2008;215(3):237–245.
19. Ohara Y, Yoshida N, Kono Y, et al. Effectiveness of an oral health educational program on community-dwelling older people with xerostomia. Geriatr Gerontol Int. 2015;15(4):481–489. doi:10.1111/ggi.12301
20. Bowerman TJ, Zhang J, Waite LM. Antibacterial treatment of aspiration pneumonia in older people: a systematic review. Clin Interv Aging. 2018;13:2201–2213. doi:10.2147/CIA.S183344
21. Tan EC, Lexomboon D, Sandborgh‐Englund G, Haasum Y, Johnell K. Medications that cause dry mouth as an adverse effect in older people: a systematic review and metaanalysis. J Am Geriatr Soc. 2018;66(1):76–84. doi:10.1111/jgs.15151
22. Torres SR, Peixoto CB, Caldas DM, et al. Relationship between salivary flow rates and Candida counts in subjects with xerostomia. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;93(2):149–154.
23. Fox PC, Busch KA, Baum BJ. Subjective reports of xerostomia and objective measures of salivary gland performance. J Am Dent Assoc. 1987;115(4):581–584.
24. Sato H, Fueki K, Sueda S, et al. A new and simple method for evaluating masticatory function using newly developed artificial test food. J Oral Rehabil. 2003;30(1):68–73.
25. Jeong SH, Kang SM, Ryu JH, Kwon HK, Kim BI. Subjective food intake ability in relation to the mixing ability index in Korean adults. J Oral Rehabil. 2010;37(4):242–247. doi:10.1111/j.1365-2842.2009.02050.x
26. Sato S, Fueki K, Sato H, et al. Validity and reliability of a newly developed method for evaluating masticatory function using discriminant analysis. J Oral Rehabil. 2003;30(2):146–151.
27. Kang SM, Lee SS, Kwon HK, Kim BI. Short-term improvement of masticatory function after implant restoration. J Periodontal Implant Sci. 2015;45(6):205–209. doi:10.5051/jpis.2015.45.6.205
28. Fukushima Y, Yoda T, Araki R, et al. Evaluation of oral wetness using an improved moisture-checking device for the diagnosis of dry mouth. Oral Sci Int. 2017;14(2):33–36. doi:10.1016/S1348-8643(17)30017-4
29. Fukushima Y, Yoda T, Kokabu S, et al. Evaluation of an oral moisture-checking device for screening dry mouth. Open J Stomatology. 2013;3(8):7. doi:10.4236/ojst.2013.38073
30. Wiener RC, Wu B, Crout R, et al. Hyposalivation and xerostomia in dentate older adults. J Am Dent Assoc. 2010;141(3):279–284.
31. Furumoto EK, Barker GJ, Carter‐Hanson C, Barker BF. Subjective and clinical evaluation of oral lubricants in xerostomic patients. Spec Care Dentist. 1998;18(3):113–118.
32. Persson E, Wardh I, Ostberg P. Repetitive saliva swallowing test: norms, clinical relevance and the impact of saliva secretion. Dysphagia. 2018. doi:10.1007/s00455-018-9937-0
33.
34. Harris NO, García-Godoy F, Nathe CN. Primary preventive dentistry. Boston: Pearson; 2014.
35. Van der Bilt A. Assessment of mastication with implications for oral rehabilitation: a review. J Oral Rehabil. 2011;38(10):754–780. doi:10.1111/j.1365-2842.2010.02197.x
36. Ahn HJ, Lee YS, Jeong SH, Kang SM, Byun YS, Kim BI. Objective and subjective assessment of masticatory function for patients with temporomandibular disorder in Korea. J Oral Rehabil. 2011;38(7):475–481. doi:10.1111/j.1365-2842.2010.02179.x
37. Park HU, Kim BI, Kang SM, Kim ST, Choi JH, Ahn HJ. Changes in masticatory function after injection of botulinum toxin type A to masticatory muscles. J Oral Rehabil. 2013;40(12):916–922. doi:10.1111/joor.12111
38. Choi TH, Kim BI, Chung CJ, et al. Assessment of masticatory function in patients with non-sagittal occlusal discrepancies. J Oral Rehabil. 2015;42(1):2–9. doi:10.1111/joor.12227
39. Painter P, Carlson L, Carey S, Paul SM, Myll J. Low-functioning hemodialysis patients improve with exercise training. Am J Kidney Dis. 2000;36(3):600–608. doi:10.1053/ajkd.2000.16200
40. Oh JC, Park JW, Cha TH, Woo HS, Kim DK. Exercise using tongue-holding swallow does not improve swallowing function in normal subjects. J Oral Rehabil. 2012;39(5):364–369. doi:10.1111/j.1365-2842.2011.02274.x
41. Keens TG, Krastins IR, Wannamaker EM, Levison H, Crozier DN, Bryan AC. Ventilatory muscle endurance training in normal subjects and patients with cystic fibrosis. Am Rev Respir Dis. 1977;116(5):853–860. doi:10.1164/arrd.1977.116.5.853
42. Iida T, Komiyama O, Obara R, Baad-Hansen L, Kawara M, Svensson P. Repeated clenching causes plasticity in corticomotor control of jaw muscles. Eur J Oral Sci. 2014;122(1):42–48. doi:10.1111/eos.12101
43. Zhang H, Kumar A, Kothari M, et al. Can short-term oral fine motor training affect precision of task performance and induce cortical plasticity of the jaw muscles? Exp Brain Res. 2016;234(7):1935–1943. doi:10.1007/s00221-016-4598-4
44. Fejerskov O, Nyvad B, Kidd E. Dental Caries: The Disease and Its Clinical Management.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.