Back to Journals » International Journal of Women's Health » Volume 18
Improved Outcomes with Nerve-Sparing Technique: A Retrospective Comparison of Colorectal Surgeries for Bowel Endometriosis
Authors Ji L, Jin L, Shao M ![]() , Hu M
, Hu M
Received 13 December 2025
Accepted for publication 19 February 2026
Published 10 March 2026 Volume 2026:18 588653
DOI https://doi.org/10.2147/IJWH.S588653
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vinay Kumar
Limei Ji,1,2 Lanying Jin,1,2 Mingjun Shao,1,2 Min Hu2
1Department of Gynecology, Jinhua Maternity and Child Health Care Hospital, Jinhua, People’s Republic of China; 2Department of Gynecology, Jinhua Hospital of Zhejiang University, Jinhua, People’s Republic of China
Correspondence: Min Hu, Department of Gynecology, Department of Obstetrics and Gynecology, Jinhua Maternal and Child Health Care Hospital, No. 266 Hou Shan Road, Jinhua, Zhejiang, 321000, People’s Republic of China, Tel +86 579 82552733, Email [email protected]
Study Objective: The aim of this study was to describe surgical outcomes after different types of colorectal surgery for bowel endometriosis and to present the feasibility of LscPR in bowel endometriosis.
Design: Retrospective analysis.
Setting: Gynecological department at the Jinhua Maternity and Child Health Care Hospital.
Interventions and Measurements: From January 2014 to November 2024, we recruited 320 patients with bowel endometriosis who underwent LscShR (n=108), LscDR (n=70), LscSgR (n=73), or LscPR (n=69).
Main Results: Over a median follow-up of 4.6 years (range: 1– 10 years), one patient rejected subsequent treatment in the LscShR and LscSgR groups, respectively, and two patients were lost to follow-up in the LscDR group; a total of 316 women completed the follow-up questionnaire. The total complication rate was highest in the LscSgR group (16.67%), followed by the LscDR (5.88%), LscPR (4.35%), and LscShR (1.87%) groups, with a statistically significant difference (P = 0.002). BE recurrence was seen only in the LscShR (12.15%) and LscDR (7.35%) groups (P < 0.001). DIE recurrence rates were low and similar across all groups (P = 0.810), ranging from 1.45% (LscPR) to 4.41% (LscDR). The incidence of low anterior rectal resection syndrome in the LscPR group was similar to that of the LscShR and LscDR (P > 0.05) groups, and the parameter was significantly lower than that in the LscSgR group (P < 0.05);.The LscPR surgical method was associated with the most comprehensive postoperative symptom improvement, achieving the best overall BENS scores. The rectal sensory parameters (FRS, CRS, MRTS) and the operation time of the balloon extraction test in the LscPR group were similar to those in the LscDR and LscShR groups (P > 0.05), and significantly lower than those in the LscSgR group (P < 0.05).
Conclusion: Within the limitations of a retrospective study, our data suggest that LscPR is an effective approach for bowel endometriosis, associated with significant symptom improvement and fewer complications.
Keywords: bowel endometriosis, deep endometriosis, LARS, preservation of mesentery segmental intestinal resection
Introduction
Endometriosis represents a chronic inflammatory oestrogen-dependent condition, with an estimated incidence of approximately 10–20% of women of reproductive age worldwide, rising to 30–35% in infertile women.1 Deep endometriosis (DE) is the most aggressive form, and is defined as endometriosis lesions spreading and infiltrating more than 5 mm beneath the peritoneal layer; it represents 48% of all cases of endometriosis.2 DE leads to inflammation, the two most characteristic manifestations of which are infertility and pelvic pain.3 Deep infiltrating endometriosis (DIE) usually localizes in the posterior compartment and involves the bowel in 3.8–37% of cases,4 with the rectum and/or sigmoid colon involved in approximately 70–93% of all cases.5 Bowel endometriosis (BE) is a challenging disease often involving a fibrotic reaction causing anatomic distortion and dense adhesions, which are associated with intestinal complaints such as dyspareunia, dysmenorrhea, progressive dyschezia, constipation, rectorrhagia and tenesmus, all of which negatively impact patients’ health.6,7
Medical treatment should be considered the first line of therapy. Symptoms may temporarily improve with medical therapies; however, prolonged medical treatment cannot eradicate the disease and can be associated with side effects.8 Deep infiltrating lesions are less likely to resolve and the progression of endometriosis may negatively affect women’s quality of life and their fertility.9 In these situations, surgery is preferred. Three conventional colorectal surgeries may be employed in the surgical treatment of bowel DE: nodule excision without opening the rectum (shaving), resection of the nodule with excision of the anterior rectal wall (disc excision), and segmental rectosigmoidectomy. Procedures are carried out according to the depth, extent, and location of lesions; however, there is no consensus regarding the optimal surgical strategy.10
The rate of recurrence has been related to the completeness of surgical excision.11 Segmental bowel resection is preferred in many cases; however, the radical nature of the surgery carries the risk of postoperative complications, including rectovaginal fistulae, anastomosis dehiscence, pelvic abscess and peritonitis,12 and intestinal dysfunction is increased significantly.13 The segmental bowel resection procedure shares technical similarities with the segmental resections performed in rectal cancer surgery. The primary goal of oncologic surgery is radical resection to achieve a cure, for which a certain degree of risk of nerve injury may be accepted to ensure oncologic safety. In contrast, the core objective of surgery for endometriosis is to maximally alleviate symptoms, preserve organ function, and maintain patients’ long-term quality of life.14 The classical trans-mesorectal excision, while pursuing complete mesorectal resection, is likely to damage the hypogastric plexus and splanchnic nerves embedded within the mesorectum.15 For benign conditions, iatrogenic autonomic nerve injury may lead to urinary, defecatory, and sexual dysfunction.16 Therefore, there is an urgent need for a surgical strategy that achieves a better balance between thorough lesion excision and maximal preservation of pelvic nerve function. The nerve-sparing and refined mesenteric dissection technique evaluated in this study was developed precisely to address this specific need.
Materials and Methods
Patient Selection
This was a single-center, observational, indication-based cohort study. We retrospectively analyzed patients with bowel endometriosis (BE) who underwent surgery at Jinhua Maternity and Child Health Care Hospital between January 2014 and November 2024 (Figure 1). The inclusion criteria were as follows: (1) patients underwent basic clinical evaluations, including physical examination, transvaginal ultrasonography, and magnetic resonance imaging (MRI) to confirm the precise characteristics of bowel nodules (size, depth of rectal wall invasion, and extent of circumferential involvement); (2) the lesion should be >15 cm from the anus; and (3) patients should have no desire to be pregnant. The exclusion criteria were: (1) patients with severe pelvic and intrauterine inflammatory disease; (2) BE involving only rectal serosa; and (3) a postoperative diagnosis of gynecologic malignancy. All eligible patients were informed of the benefits and degree of risk of postoperative complications and outcomes associated with the four specific types of surgery and the possible conversion from MIS to laparotomy. The choice of procedure was decided preoperatively in most cases, and the specific surgical method could be changed based on the concrete size of the BE lesion detected during the procedure. Postoperative continuous medical therapy such as GnRH analogs and dienogest was recommended for patients to reduce the risk of postoperative recurrences. The colorectal procedures would be performed by a colorectal surgeon from the same surgical team. During the follow-up period, the following data would be recorded by a clinical research technician. This research was approved by the Ethics Committee of Jinhua Maternity and Child Health Care Hospital and all patients provided written informed consent before recruitment. Questionnaires were answered postoperatively by patients to evaluate their health status: low anterior rectal resection syndrome score (LARS),17 Bowel Endometriosis Syndrome (BENS),18 rectal sensation test,19 and rectal manometry test.20,21 Operating time was determined from the first skin incision to closure. Operative blood loss was estimated by gathering the blood in suction bottles during the surgery.
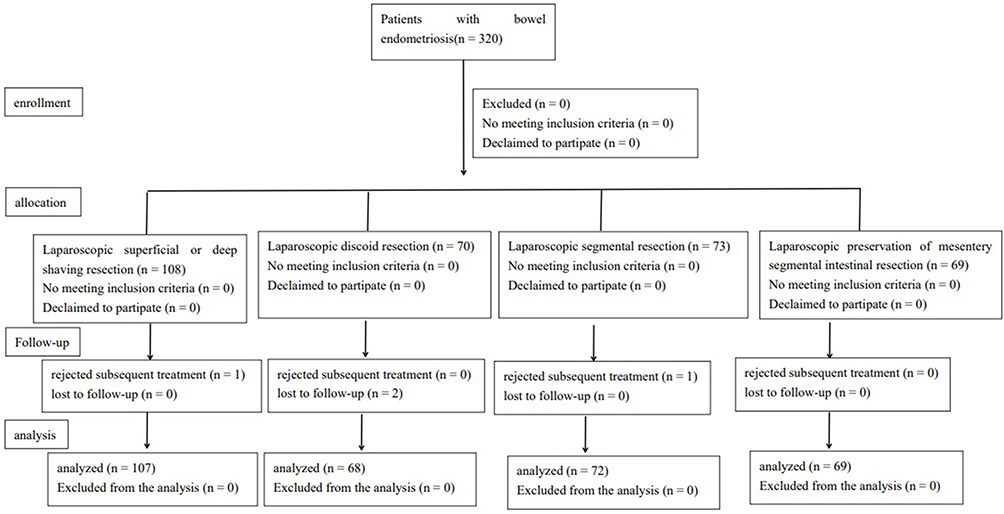 |
Figure 1 CONSORT flow diagram. |
Surgical Technique
All of the cases recruited in this study were operated on by the same five proficient gynecologists. All patients were scheduled for bowel preparation before the procedure. The patients were placed in the Trendelenburg position at 30 degrees. After general anesthesia, all visible endometriosis in pelvic sites were performed using ultrasonic scalpel (Ethicon Endo-surgery Inc., Cincinnati, OH, USA). BE lesions involving at least the muscularis propria layer of the intestinal wall were considered eligible for surgical resection. Rectal surgery, when required, was conducted by a specialized proctologist.
Laparoscopic superficial or deep shaving resection (LscShR) (Figure 2) was indicated for BE nodules meeting all of the following criteria: (1) a diameter of <3 cm; (2) a depth of rectal wall invasion of <7 mm; and (3) involvement of <50% of the bowel circumference. The shaving resection technique involved removing the nodule on the anterior face of the rectum. Laparoscopic discoid resection (LscDR) (Figure 3) was chosen when the intestinal endometriotic nodule was solitary and less than 3 cm, at a distance of more than 10 cm from the anus, had fully invaded the intestinal wall, affected no more than one-third of the total circumference of the segment, and did not cause major distortion. The laparoscopic segmental resection (LscSgR) technique (Figure 4) and laparoscopic preservation of mesentery segmental intestinal resection (LscPR) technique (Figure 5) were described in our previous study.22
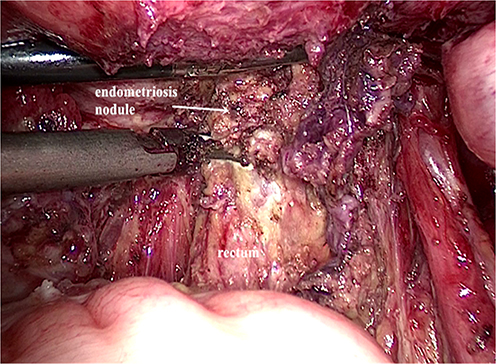 |
Figure 2 Laparoscopic shaving resection. |
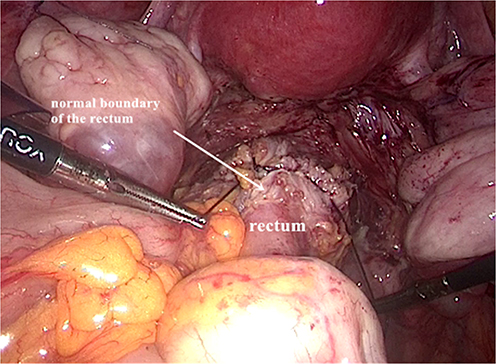 |
Figure 3 Laparoscopic discoid resection. |
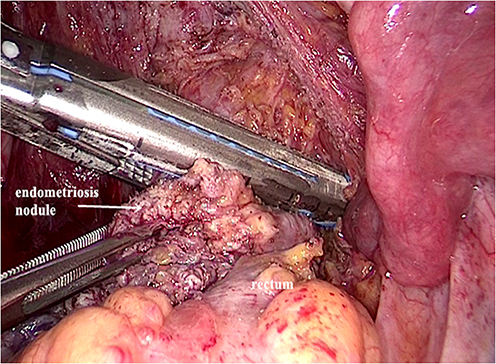 |
Figure 4 Laparoscopic segmental resection. |
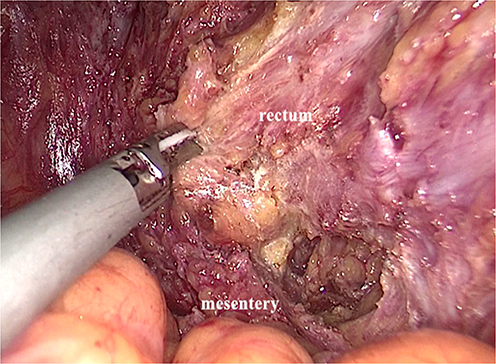 |
Figure 5 Laparoscopic preservation of mesentery segmental intestinal resection. |
Assessment
Rectal Manometry Test
Three months after surgery, the patient was instructed to administer a glycerin enema two hours prior to the procedure. A single Foley catheter was taken, and its tip lubricated with mineral oil. The catheter was then inserted slowly into the rectal ampulla (approximately 10 cm from the anal verge). The balloon was inflated with 50 mL of normal saline. The distal end of the catheter was clamped with a hemostat. The patient was then instructed to assume a sitting defecation posture and to attempt to expel the balloon.
Rectal Sensation Test
For the sensory assessment, using the method described above, three months after surgery, the balloon was positioned within the rectal ampulla. The balloon was initially inflated with 20 mL of air, with subsequent increments up to a maximum volume of 340 mL. During the inflation process, the patient was instructed to describe three distinct sensory thresholds: the initial sensation of rectal distention (FRS) or a fleeting desire to defecate; a sustained sensation of needing to defecate (CRS), which may be accompanied by a feeling of abdominal pressure or discomfort; and the intense sensation just prior to unbearable discomfort (MRTS), which may be accompanied by significant abdominal cramping or pain.
Statistical Analysis
SPSS version 17.0 (SPSS, Inc., IBM, Chicago, IL) was used to perform all statistical analyses. Data are presented as mean ± standard deviation (SD), median (range), or absolute number (%). The difference in means between the two groups was tested by analysis of variance (ANOVA). All P-values were two-tailed, and a P-value of <0.05 was considered statistically significant.
Results
From January 2012 to November 2024, 320 patients underwent laparoscopy for symptomatic deep endometriosis infiltrating the rectosigmoid. Patient characteristics are shown in Table 1. All patients agreed to provide written informed consent to undergo DE surgery, including bowel resection when necessary. One patient rejected subsequent treatment the in LscShR and LscSgR groups, respectively, and two patients were lost to follow-up in the LscDR group. Finally, there were 107, 68, 72, and 69 cases of LscShR, LscDR, LscSgR, and LscPR, respectively. No patients experienced hemorrhage and conversion to laparotomy during the perioperative period. The specific follow-up rates were comparable across all groups (97.14–100%), and a chi-square test confirmed no significant differences in loss to follow-up (P = 0.617).
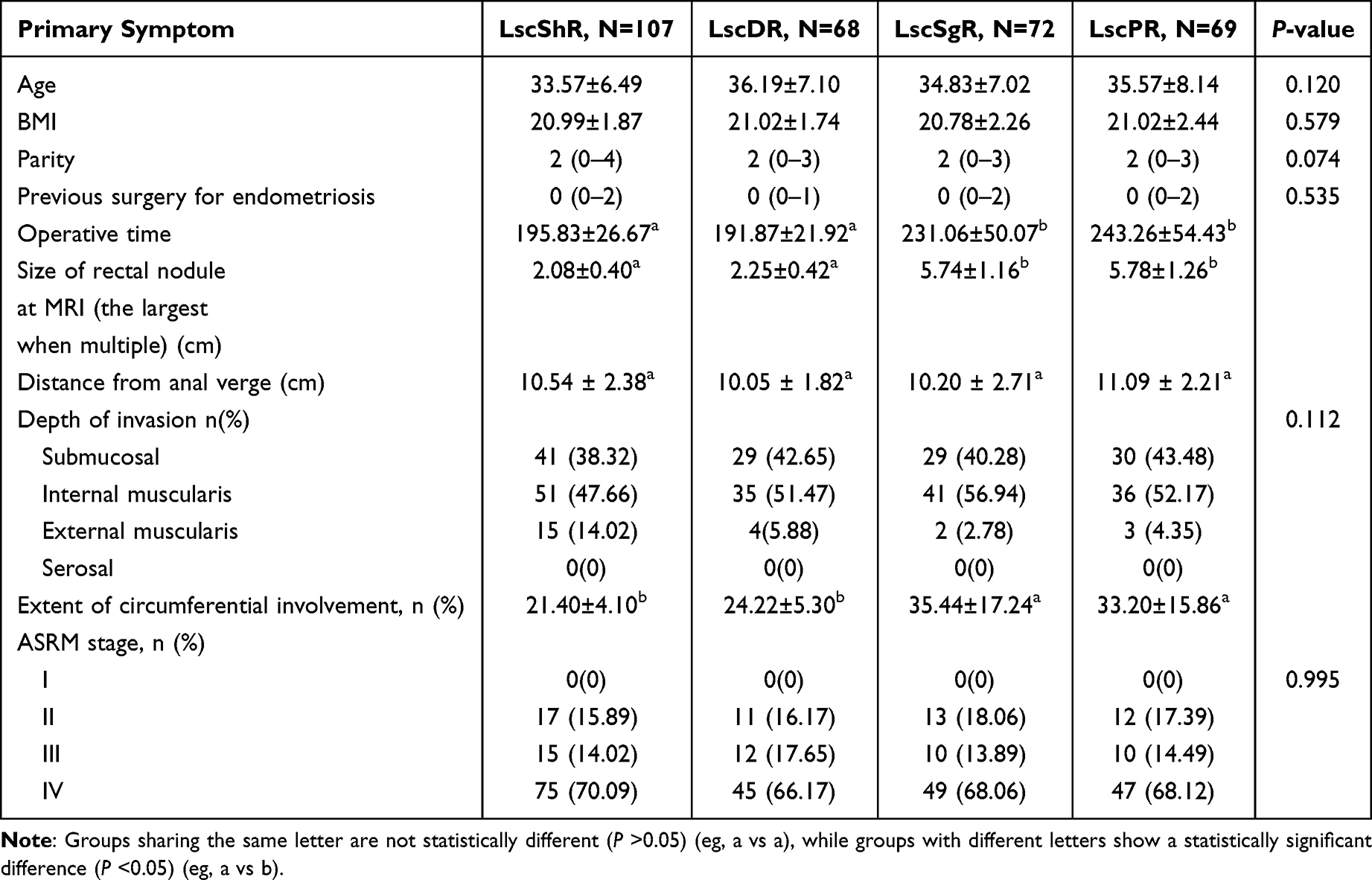 |
Table 1 Baseline Clinical Characteristics of Patients in Four Groups |
Postoperative complications and recurrence of DE and BE are described in Table 2. The overall incidence of postoperative complications of LscPR was lower than that of LscSgR, and similar to that of LscShR and LscDR. There was no BE recurrence in the LscSgR and LscPR groups. DIE recurrence rates were similar across all groups (P = 0.810).
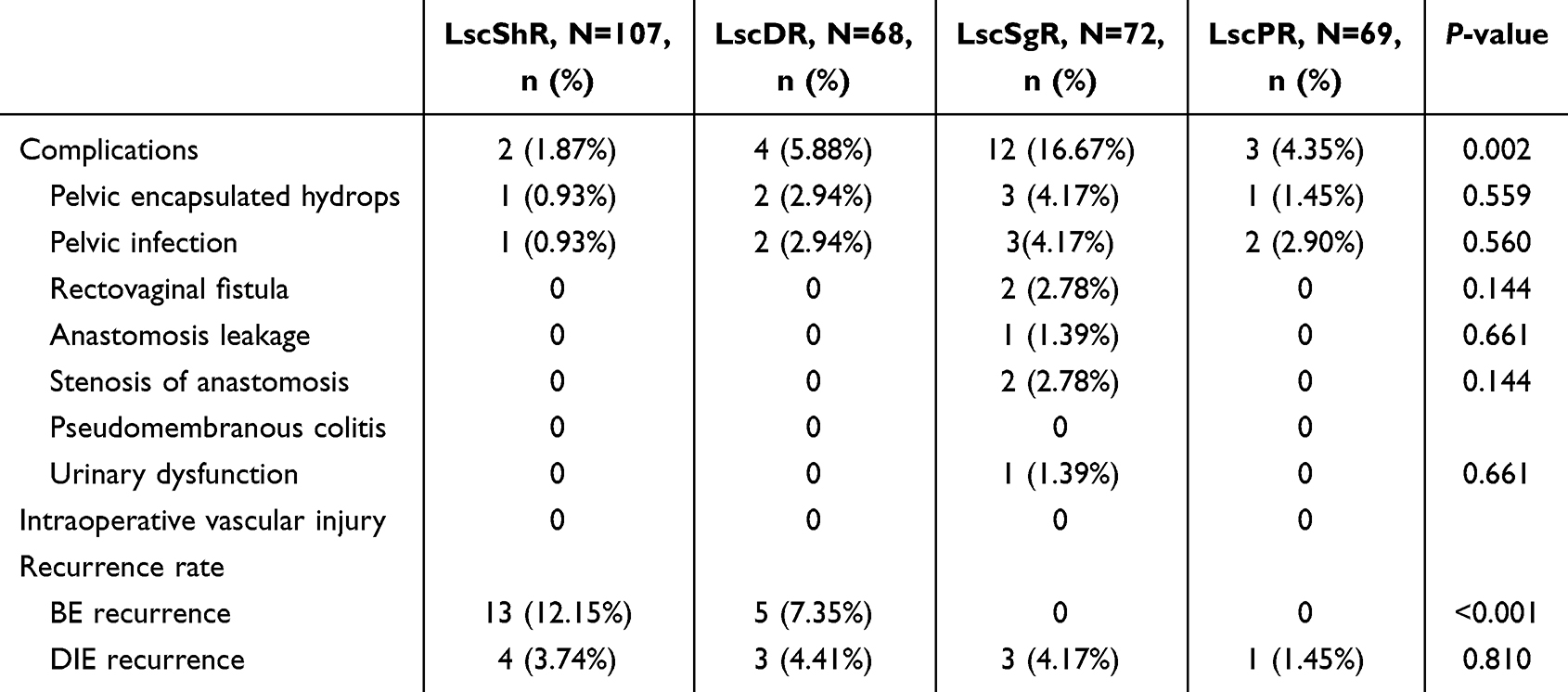 |
Table 2 Postoperative Complications and Recurrence Following Use of Four Surgical Methods |
The LARS scores after surgery are shown in Table 3, and the incidence of LARS in the LscPR groups was similar to that in the LscShR and LscDR groups (P > 0.05), and significantly less than that in the LscSgR group (P < 0.05).
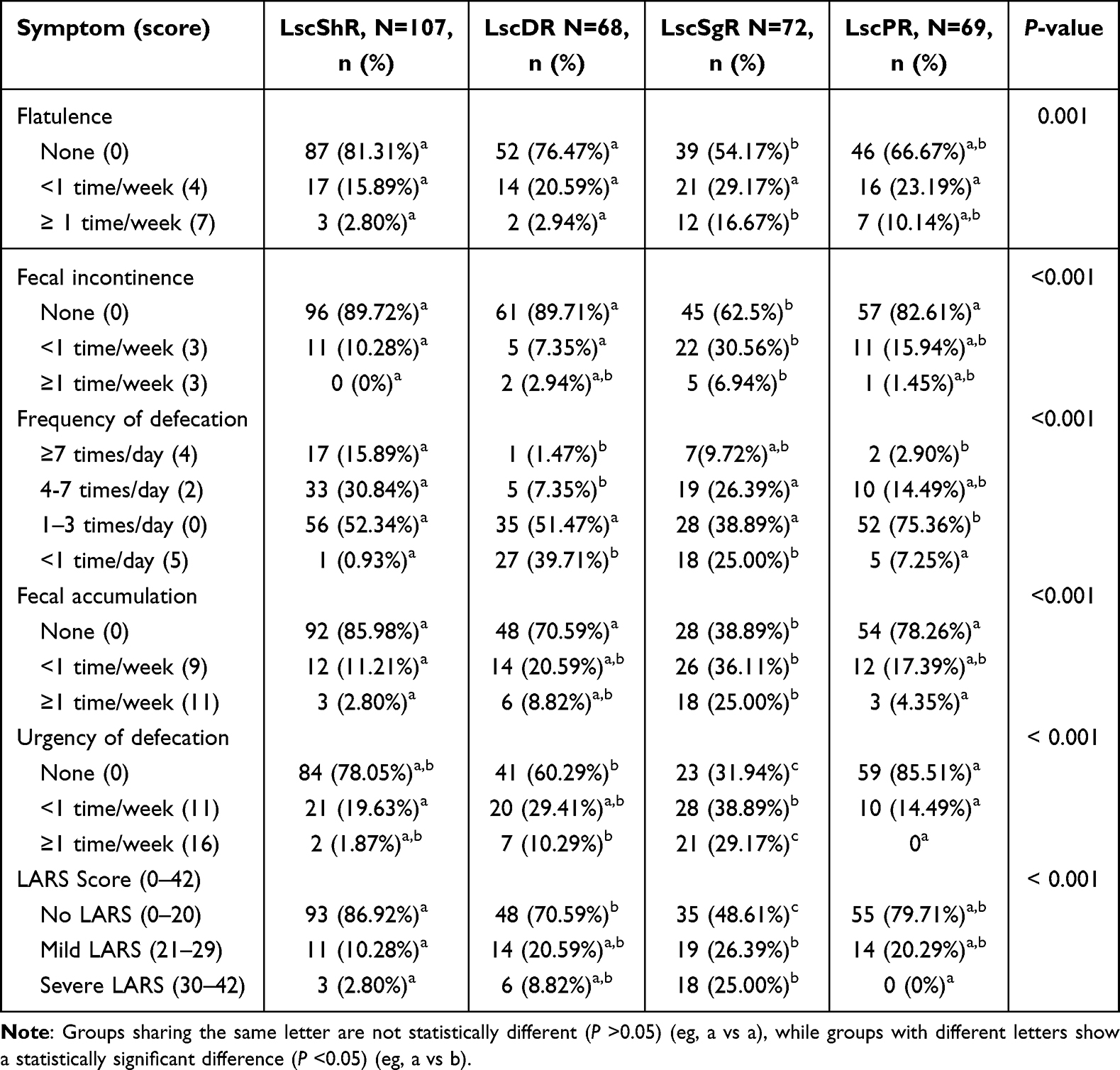 |
Table 3 LARS Score and Symptoms After Different Types of Surgery |
The LscPR was associated with the most comprehensive postoperative symptom improvement, achieving the best overall BENS scores in 4 groups, and the most favorable outcomes in defecation and fecal urgency urination (Table 4).
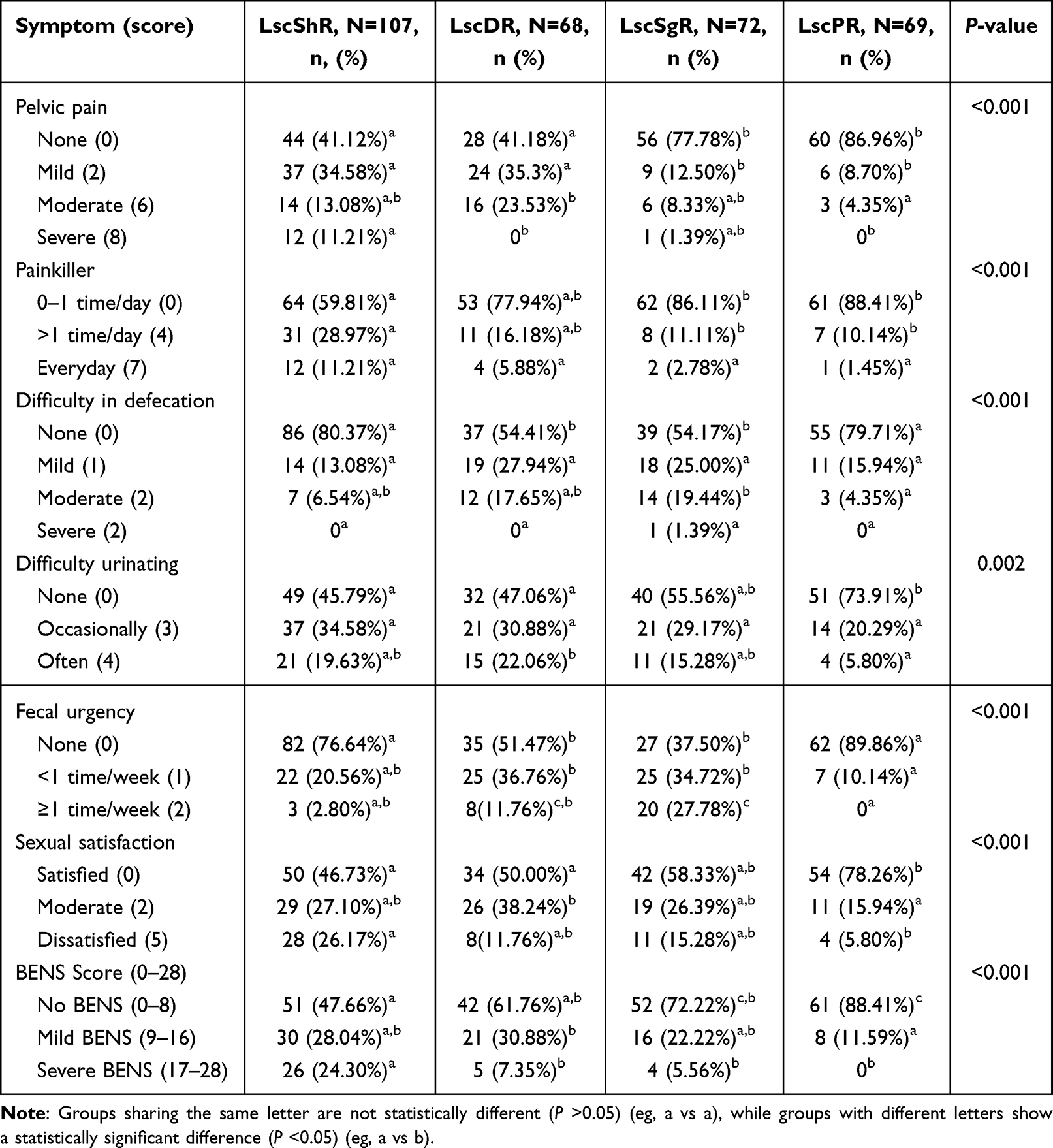 |
Table 4 Improvement in BENS Score Following Different Types of Surgery |
The FRS, CRS, and MRTS parameters and the operation time of the balloon extraction test in the LscPR group were similar to those in the LscDR and LscShR groups (P > 0.05), and were significantly lower than those in the LscSgR group (P < 0.05) (Table 5). Compared to the other three surgical approaches, the nerve-sparing technique of LscPR helped to recover rectal sensory and motor function.
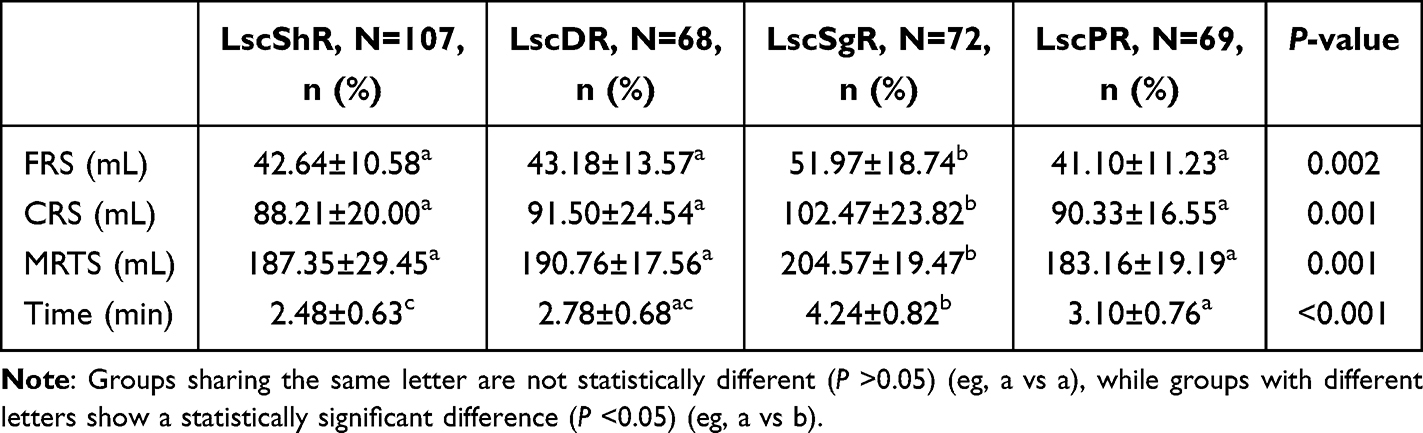 |
Table 5 Results of Rectal Manometry and Sensation Tests Following Different Types of Surgery |
Discussion
The main therapeutic strategies for endometriosis were medication and surgery.8,9 BE presents a therapeutic dilemma for the surgeon.23,24 Surgical treatment of bowel DE depends primarily on the size and the number of lesions, location, depth of infiltration, and extent of bowel lumen involvement.25 Different surgical techniques have been proposed. Adverse events are closely linked to the complexity of the surgical procedure itself, and the optimal treatment approach to BE is still controversial.26
The present review produces an overview of 10 years’ assessment of postoperative complications following surgical treatment of DE in our department. Before 2017 we mainly performed LscSgR (lesions of >3cm) to provide microscopically complete removal of digestive nodules and ensure a decrease in the risk of BE recurrences.
However, conventional LscSgR was associated with postoperative anastomotic leakage and compromised rectal sensory function, which we attributed to inadvertent injury to the autonomic pelvic nerves. This led us to adopt and refine a nerve-sparing technique, focusing on the preservation of the hypogastric plexus and splanchnic nerves, with the aim of reducing these functional sequelae.
The diagnosis of recurrent BE and DIE is based on symptoms combined with clinical signs. MRI have relatively high detection rates for endometriosis (sensitivity 88%, specificity 98%, accuracy 96%);27 however, the cost prohibits routine use in follow-up protocols. Instead, transvaginal ultrasound (TVUS) is the conventional follow-up technique, achieving a sensitivity of 87.2% and a specificity of 96.8% in detecting rectosigmoid endometriosis.28 MRI is reserved for cases where recurrence is suspected but cannot be confirmed by TVUS.
We noticed the high number of digestive symptoms following LscSgR in our department, such as increased frequency of bowel movements and fecal incontinence. These unpleasant functional digestive symptoms may last for a long time and even be accompanied by postoperative complications seriously affecting patients’ quality of life. For lesions of less than 3 cm, we applied LscShR so that the surgery could avoid risk of postoperative complications, in particular rectovaginal fistulas; however, preoperative symptoms are prone to recurrence. Optimum clearance of the endometriosis is key, and the main risk factor for recurrent disease reported in the literature is incomplete surgery.29 Anaf et al30 reported that deep endometriotic lesions invade the rectal wall along the nerves, sometimes even at a distance from the palpated lesion. The LscShR may be microscopically incomplete. Vercellini et al31 reported a significantly higher recurrence rate of 20% at one-year follow-up and an additional procedure was required in 25% of patients within five years after LscShR.
In subsequent surgeries, we reconsidered the risk of complications and significant outcomes. We adopted LscDR, which is considered only for lesions smaller than 3 cm. Nezhat et al11 first proposed discoid resection in BE and subsequently Roman et al32 improved the technique by using a stapler instead of manual suturing. LscDR does not require section of the mesorectum to reduce denervation and the special suturing is less likely to lead to rectal stenosis and dysfunction.33,34 Mabrouk et al35 reported a risk of recurrence after LscDR of 1.8–8%. A significant reduction in recurrence rate was observed compared to LscShR, a finding that is also in line with our outcomes.
However, use of a transanal stapler for BE may lead to progressive stenosis of the bowel. Additionally, when the nodules affect more than 50% of rectal circumference and LscDR is not an overly complex procedure for BE, colorectal resection is inevitable.36 Malzoni et al37 performed laparoscopic segmental rectosigmoid resection with the preservation of mesentery and achieved complete excision of endometriosis with no postoperative complications during the follow-up period. Preserving the mesentery is better in terms of re-establishing the anastomotic site and has less impact on postoperative intestinal function.
For these reasons, we linked LscPR to organ preservation in our study in the subsequent period; that is, stay as close as possible to the external muscularis propria on the shortest possible segment, with short healthy margins. This technique preserves the vascularity of the segments and innervation.38 Fanfani et al39 described a case control study with 88 patients who underwent segmental rectosigmoid resection for BE; the rectovaginal fistula complication rate was 3.4%, which was similar with LscSgR in our study. In our study, there was no rectovaginal and anastomotic fistula, anastomotic stenosis, or urinary dysfunction in the LscPR group, and no differences were shown regarding total postoperative complications with LscShR and LscDR. This is attributable to two details: our close postoperative monitoring of patients’ clinical symptoms and inflammatory markers such as C-reactive protein; and taking nerve-sparing techniques into account to avoid rectal innervation, that is, preservation of the inferior mesenteric artery may improvehealing of the incision. These results are in line with our expectations. Our study provided good perioperative outcomes and improved digestive functional outcomes more in the LscPR group than in the LscSgR group. There was also significant improvement in BENS score and recovery of rectal motor and sensory function was better in the LscPR than in the LscSgR group (P < 0.05).
A strength of the present study is that it is the first to report on the use of LscPR rather than the three conventional procedures concerning the management of BE and postoperative functional recovery. There are, however, some limitations to our study. First, selection bias is a major limitation because the observed differences in outcomes (eg, recurrence, LARS) may be confounded by the baseline severity and extent of the lesion for which each procedure was chosen. We selected patients over a long time period and those managed during the initial period were more likely to undergo shave and radical resection than patients enrolled in the subsequent arm. In the subsequent stage, the evolving expertise of the surgical team may have lead to greater surgical proficiency and resulted in more favorable outcomes. While the outcomes reflect a real-world learning curve, the study design inherently limits comparability between patients treated in the earlier and later phases of the study. Another limitation of this study was that it was conducted at a single center. In order to clarify the optimal procedure for BE, further research is needed to investigate multi-institutional prospective studies in order to construct a standardized diagnosis and long-term treatment process for BE.
Conclusion
LscPR promises to be a useful approach to treating deep pelvic endometriosis. For patients with bowel endometriosis who are not prioritizing fertility preservation, our findings indicate that LscPR can be an effective treatment, allowing for complete nodule resection, alleviation of digestive symptoms, and significant quality-of-life improvement.
Data Sharing Statement
All data analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Statement of Ethics
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki. The study protocol was reviewed and approved by the Jinhua Maternity and Child Health Care Hospital Ethics Committee (approval no: 2022-KY064), and written informed consent was obtained from all participants.
Acknowledgment
We thank Zhang Jing for her insightful discussions on surgical anatomy relevant to mesenteric preservation, which helped refine the technical description of the procedure.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received fees from Zhejiang Province Medical and Health Science and Technology (2024KY1754).
Disclosure
The authors declare that there are no conflicts of interest related to this research.
References
1. Alabiso G, Alio L, Arena S, et al. How to manage bowel endometriosis: the ETIC approach. J Minim Invasive Gynecol. 2015;22:517–11. doi:10.1016/j.jmig.2015.01.021
2. de Paula Andres M, Borrelli GM, Kho RM, Abrao MS. The current management of deep endometriosis: a systematic review. Minerva Ginecol. 2017;69:587–596. doi:10.23736/S0026-4784.17.04082-5
3. Chen Y, Li T. Unveiling the mechanisms of pain in endometriosis: comprehensive analysis of inflammatory sensitization and therapeutic potential. Int J Mol Sci. 2025;26:1770. doi:10.3390/ijms26041770
4. Hur C, Falcone T. Robotic treatment of bowel endometriosis. Best Pract Res Clin Obstet Gynaecol. 2021;71:129–143. doi:10.1016/j.bpobgyn.2020.05.012
5. Ruffo G, Scopelliti F, Manzoni A, et al. Long-term outcome after laparoscopic bowel resections for deep infiltrating endometriosis: a single-center experience after 900 cases. BioMed Res Int. 2014;2014:463058. doi:10.1155/2014/463058
6. Jiao H, Feng W, Liu H. Clinical diagnosis and treatment of bowel endometriosis and the distribution characteristics of lesions.BMC WOMENS HEALTH. BMC Women’s Health. 2025;26:62. doi:10.1186/s12905-025-04248-3
7. Wickramasekera D, Hay DJ, Fayz M. Acute small bowel obstruction due to ileal endometriosis: a case report and literature review. JR Coll Surg Edinb. 1999;59–60.
8. Vercellini P, Buggio L, Borghi A, et al. Medical treatment in the management of deep endometriosis infiltrating the proximal rectum and sigmoid colon: a comprehensive literature review. Acta Obstet Gynecol Scand. 2018;97:942–955. doi:10.1111/aogs.13328
9. Chapron C, Fauconnier A, Dubuisson JB, et al. Deep infiltrating endometriosis: relation between severity of dysmenorrhea and extent of disease. Hum Reprod. 2003;18:760–766. doi:10.1093/humrep/deg152
10. Donnez O, Roman H. Choosing the right surgical technique for deep endometriosis:shaving, disc excision, or bowel resection? Fertile Steril. 2017;108:931–942. doi:10.1016/j.fertnstert.2017.09.006
11. Nezhat C, Nezhat F, Pennington E, et al. Laparoscopic disk excision and primary repair of the anterior rectal wall for the treatment of full-thickness bowel endometriosis. Surg Endosc. 1994;8:682–685. doi:10.1007/BF00678566
12. Minelli L, Fanfani F, Fagotti A, et al. Laparoscopic colorectal resection for bowel endometriosis: feasibility, complications, and clinical outcome. Arch Surg Chicago. 2009;144:234–239. doi:10.1001/archsurg.2008.555
13. Soto E, Catenacci M, Bedient C, et al. Assessment of long-term bowel symptoms after segmental resection of deeply infiltrating endometriosis: a matched cohort study. J Minim Invasive Gynecol. 2016;23(753):–759. doi:10.1016/j.jmig.2016.03.004
14. Pecorella G, Morciano A, Sparic R, et al. Endometriosis and reproductive sparing surgery: a narrative review and agree ii-s-based evaluation of international guidelines. J CLIN MED. 2026;15:380. doi:10.3390/jcm15010380
15. Cui WQ, Hu QX, Zhang F, et al. Application status and progress of intraoperative nerve monitoring in pelvic autonomic nerve preserving radical resection of rectal cancer. Zhonghua Wei Chang Wai Ke Za Zhi. 2023;26:1202–1209. doi:10.3760/cma.j.cn441530-20221212-00520
16. Matsui T, Kiuchi J, Kuriu Y, et al. Deep pelvis and low visceral fat mass as risk factors for neurogenic bladder after rectal cancer surgery. BMC Gastroenterol. 2024;24:323. doi:10.1186/s12876-024-03433-2
17. Emmertsen KJ, Laurberg S. Low anterior resection syndrome score: development and validation of a symptom-based scoring system for bowel dysfunction after low anterior resection for rectal cancer. Ann Surg. 2012;255:922–928. doi:10.1097/SLA.0b013e31824f1c21
18. Riiskjær M, Egekvist AG, Hartwell D, et al. Bowel Endometriosis Syndrome: a new scoring system for pelvic organ dysfunction and quality of life. Hum Reprod. 2017;32:1812–1818. doi:10.1093/humrep/dex248
19. Kritasampan P, Lohsiriwat S, Leelakusolvong S. Manometric tests of anorectal function in healthy adult. Thai Subjects J Med Assoc Thai. 2004;87:536–542.
20. Prichard DO, Lee T, Parthasarathy G, et al. High-resolution anorectal manometry for identifying defecatory disorders and rectal structural abnormalities in women. Clin Gastroenterol Hepatol. 2017;15:412–420. doi:10.1016/j.cgh.2016.09.154
21. Chiarioni G, Whitehead WE. Anorectal physiology in health: a randomized trial to determine the optimum catheter for the balloon expulsion test. Neurogastro-Enterol Motil. 2019;31:e13582. doi:10.1111/nmo.13582
22. Ji L, Shao M, Hu M. Optimizing outcomes in laparoscopic segmental resection for bowel endometriosis. Int J Gynecol Obstet. 2025;1–8.
23. Jacobson TZ, Duffy JM, Barlow D, et al. Laparoscopic surgery for pelvic pain associated with endometriosis. Cochrane Database Syst Rev. 2009;001300.
24. Ruffo G, Sartori A, Crippa S, et al. Laparoscopic rectal resection for severe endometriosis of the mid and low rectum: technique and operative results. Surg Endosc. 2012;26:1035–1040. doi:10.1007/s00464-011-1991-8
25. Barretto R, da Silva RCM, Filho RPG, et al. Does age influence surgical technique in bowel endometriosis? A multicenter analysis of 1547 cases. J Robot Surg. 2025;19:665. doi:10.1007/s11701-025-02861-w
26. Ceccaroni M, Ceccarello M, Clarizia R, et al. Nerve-sparing laparoscopic disc excision of deep endometriosis involving the bowel: a single-center experience on 371 consecutives cases. Surg Endosc. 2021;35:5991–6000. doi:10.1007/s00464-020-08084-4
27. Bazot M, Kermarrec E, Bendifallah S, et al. MRI of intestinal endometriosis. Best Pract Res Clin Obstet Gynaecol. 2021;71:51–63. doi:10.1016/j.bpobgyn.2020.05.013
28. Ferrero S, Barra F, Perrone U, et al. Ultrasound diagnosis of bowel endometriosis. Gynecol Obstet Invest. 2025;90:268–278. doi:10.1159/000542563
29. Habib N, Centini G, Lazzeri L, et al. Bowel endometriosis: current perspectives on diagnosis and treatment. Int J Womens Health. 2020;12:35–47. doi:10.2147/IJWH.S190326
30. Anaf V, El Nakadi I, Simon P, et al. Preferential infiltration of large bowel endometriosis along the nerves of the colon. Hum Reprod. 2004;19:996–1002. doi:10.1093/humrep/deh150
31. Vercellini P, Crosignani PG, Abbiati A, et al. The effect of surgery for symptomatic endometriosis: the other side of the story. Hum Reprod Update. 2009;15:177–188. doi:10.1093/humupd/dmn062
32. Roman H, Tuech JJ. New disc excision procedure for low and mid rectal endometriosis nodules using combined transanal and laparoscopic approach. Colorectal Dis. 2014;16:253–256. doi:10.1111/codi.12605
33. Lee WY, Takahashi T, Pappas T, et al. Surgical autonomic denervation results in altered colonic motility: an explanation for low anterior resection syndrome? Surgery. 2008;143:778–783. doi:10.1016/j.surg.2008.03.014
34. Roman H, Bridoux V, Tuech JJ, et al. Bowel dysfunction before and after surgery for endometriosis. Am J Obstet Gynecol. 2013;209:524–530. doi:10.1016/j.ajog.2013.04.015
35. Mabrouk M, Raimondo D, Altieri M, et al. Surgical, clinical, and functional outcomes in patients with rectosigmoid endometriosis in the gray zone: 13-year long-term follow-up. J Minim Invas Gyn. 2019;26:1110–1116. doi:10.1016/j.jmig.2018.08.031
36. B BVRHK, Roman H, Kianifard B, et al. Combined transanal and laparoscopic approach for the treatment of deep endometriosis infiltrating the rectum. Hum Reprod. 2012;27:418–426. doi:10.1093/humrep/der422
37. Malzoni M, Iuzzolino D, Rasile M, et al. Surgical principles of segmental rectosigmoid resection and reanastomosis for deep infiltrating endometriosis. J Min Invas Gyn. 2020;27:258. doi:10.1016/j.jmig.2019.06.018
38. Puntambekar SP, Venkateswaran S, Naidu S, et al. Endometriosis resection using nerve sparing versus non-nerve sparing surgical techniques. J Obstet Gynaecol India. 2023;73:421–427. doi:10.1007/s13224-023-01794-4
39. Fanfani F, Fagotti A, Gagliardi ML, et al. Discoid or segmental rectosigmoid resection for deep infiltrating endometriosis: a case-control study. Fertil Steril. 2010;94:444–449. doi:10.1016/j.fertnstert.2009.03.066
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.