Back to Journals » International Medical Case Reports Journal » Volume 12
Imported Brucellosis In The Era Of Dramatically Increasing Immigrants And Foreign Travelers From Endemic Areas: Occupational Hazards Of Secondary Infection Among Laboratory Technicians In A Nonendemic Country
Authors Fukuchi T ![]() , Yanagihara N, Imaoka K
, Yanagihara N, Imaoka K ![]() , Sugawara H
, Sugawara H ![]()
Received 26 July 2019
Accepted for publication 8 October 2019
Published 21 October 2019 Volume 2019:12 Pages 313—317
DOI https://doi.org/10.2147/IMCRJ.S224831
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ronald Prineas
Takahiko Fukuchi,1,2 Nobue Yanagihara,3 Koichi Imaoka,4 Hitoshi Sugawara1
1Division of General Medicine, Jichi Medical University Saitama Medical Center, Omiya, Saitama, Japan; 2Division of General Internal Medicine, Fukaya Red Cross Hospital, Fukaya, Saitama, Japan; 3Department of Clinical Laboratory, Fukaya Red Cross Hospital, Fukaya, Saitama, Japan; 4Laboratory of Reservoir Control of Zoonoses, Department of Veterinary Science, National Institute of Infectious Diseases, Shinjuku, Tokyo, Japan
Correspondence: Takahiko Fukuchi
Jichi Medical University Saitama Medical Center, Division of General Medicine, 1-847, Amanumacho, Omiya-ku, Saitama 330-8503, Japan
Tel +81 48 647 2111
Fax +81 48 644 8617
Email [email protected]
Background: Brucellosis, an important zoonotic disease, is endemic in various parts of the world. Patients diagnosed with brucellosis in developed countries are often travelers and immigrants from endemic areas. This pathogen is listed as biosafety level 3, which means that it is highly contagious and therefore a risk to clinical laboratory technicians.
Case presentation: A 43-year-old Chinese man, who could not understand Japanese, visited our hospital because of an intermittent fever that had persisted for 5 months. Associated symptoms included muscle pain whenever he had a fever. He reported currently working as a welder in Japan. However, his previous employment working in animal husbandry in Heilongjiang, mainland China was not determined at the initial visit owing to language barriers. Two sets of blood culture showed nonfermenting gram-negative bacilli, initially misidentified as Ochrobactrum anthropi and subsequently identified as Brucella abortus. Six-week doxycycline and rifampicin were administered, with intravenous gentamicin for the initial 1 week. The patient recovered without relapse, confirmed by the negative result of a Brucella agglutination test. The patient’s wife and three laboratory technicians were required to undergo blood examinations, which revealed no evidence of infection; however, they received prophylaxis with 3 weeks’ doxycycline and rifampicin.
Conclusion: In nonendemic countries, immigrants with imported brucellosis can be treated, to prevent secondary brucellosis infection, an occupational hazard among laboratory technicians. Greater attention is needed for positive findings of blood cultures, which may initially be misidentified as O. anthropi. When providing medical care for immigrants with fever of unknown origin, it is especially important for primary care physicians to overcome language barriers so as to assess pertinent information regarding their home country, such as previous employment, to prevent the spread the imported zoonoses in the era of a dramatically increasing number of immigrants and foreign travelers.
Keywords: imported brucellosis, Brucella abortus, zoonosis, Ochrobactrum anthropi, laboratory exposure, laboratory-acquired infection
Introduction
Brucellosis is a zoonotic infectious disease distributed worldwide, which is caused by intracellular gram-negative bacteria and requires long-term antibiotic therapy. Brucellosis is mainly present in developing and pastoral countries with low to moderate incomes.1 However, the disease is encountered sporadically among immigrants and travelers in developed countries.2 Japan reported the elimination of Brucella abortus in 1973. This pathogen must immediately be registered with the Ministry of Health, Labour and Welfare if diagnosed by a doctor or veterinarian. This pathogen is highly contagious and therefore a risk to laboratory workers because exposure to only a few bacteria can lead to the development of clinical symptoms.3 This fact requires physicians to inform laboratory scientists or clinical laboratory technicians about the possibility of brucellosis, to avoid the risk of infection with this pathogen.
Herein, we report our experience with a patient who developed brucellosis after emigrating from an endemic country to Japan. He did not initially report his previous occupation in his country of origin; therefore, the physician did not presume the pathogen to be Brucella spp. Brucella species include B. melitensis and its biovars: B. abortus in cattle, B. melitensis in sheep and goats, B. suis in pigs, and B. canis in dogs. This patient’s treatment course included a routine bacteriological investigation, which exposed laboratory technicians to the risk of bacterial infection. We describe this case in the hopes of drawing the attention of health care practitioners to this important issue.
Case Presentation
A 43-year-old man visited our hospital owing to intermittent fever. He could not speak or understand Japanese language. His past medical history included urolithiasis, for which he was not treated. His social history was notable as he had emigrated from mainland China; he was currently employed as a metallic welder in Japan. He was a current smoker (1 pack per day) and occasionally drank alcohol.
The patient had previously worked in animal husbandry in Heilongjiang on mainland China where he had a herd of cows (approximately 60 heads). Ten months prior to his first visit to our hospital, two cows had spontaneous abortions; however, the patient did not consult a veterinarian at the time. He emigrated to Japan after selling all of his cows, 7 months prior to his first visit to our hospital. Unfortunately, information about his previous job was not determined at the initial visit owing to language barriers.
Two months after emigrating, the patient developed a sudden fever with chills, general malaise, a bitter taste in his mouth, mild constipation, and myalgia. The symptoms resolved spontaneously within 2 or 3 days. without any treatment. The patient’s body temperature was not measured. This course of fever developed once or twice a month for 5 months. He visited our hospital to check his medical condition. Because he could only understand and speak Chinese, he was accompanied by a relative with moderate understanding of Japanese.
We found the following on physical examination of the patient. Consciousness, alert; blood pressure, 121/73 mmHg; heart rate, 90 bpm; respiration rate, 18 bpm; body temperature, 37.3°C; no abnormal findings on examination of the head, neck, chest, abdomen, back, joints, and skin. There were no palpable lymph nodes and no obvious splenomegaly.
Laboratory findings were as follows: white blood cells 4,400/μL; alkaline phosphatase 389 IU/L; and C-reactive protein 4.56 mg/dL. There were no other abnormalities. A computed tomography scan revealed mild splenomegaly.
On the first visit day, the physician took two sets of blood culture samples and closely followed the man as an outpatient because of his good general condition. Three days later, the blood cultures revealed nonfermenting gram-negative bacilli. Using a Phoenix system 100 (Japan Becton Dickinson, Tokyo, Japan), Ochrobactrum anthropi was identified in an initial report on day 8. The patient’s general condition was still good at his second visit to the hospital. Transthoracic echocardiography revealed no evidence of endocarditis. Under the provisional diagnosis of bacteremia of unknown origin, ciprofloxacin 400 mg bid was prescribed, which relieved his symptoms. Laboratory technicians were unable to identify the bacteria because of contradictory results between automatic and biochemical identification; therefore, the technicians sent samples to the National Institute of Infectious Diseases for accurate identification. The patient had not mentioned his previous occupation during his first visit to the hospital, meaning that the physician was unable to determine the possibility of infection with Brucella spp. Consequently, laboratory technicians managed the patient’s samples following the usual procedures, such as smearing, vortexing, and sniffing the colonies outside of a biosafety cabinet. The pathogen was subsequently identified as B. abortus using polymerase chain reaction. A serum agglutination test was positive for Brucella spp. (B. abortus ≥160, B. canis 1280). Doxycycline 100 mg bid and rifampicin 600 mg qd were administered for 6 weeks, as well as additional intravenous gentamicin 5 mg/kg div for the initial 1 week (Figure 1). Repeated blood cultures revealed negative results and Brucella agglutination tests showed positive but gradually decreasing positivity 6 months after the initiation of treatment (B. abortus 80, B. canis 160). There was no sign of relapse for 1 year after treatment; however, the patient declined another blood test at this point. The patient did not complain of any vertebral or joint pain throughout the clinical course. The patient’s wife and three laboratory technicians at our hospital were required to undergo physical and blood examinations, which revealed no evidence of infection. Most serum agglutination tests for these individuals were negative for Brucella spp. (B. abortus <40, B. canis <160); however, one laboratory technician had a slightly elevated B. canis titer at 320, which was considered asymptomatic infection with B. canis; around 3% of dogs are infected with B. canis in Japan. Doxycycline and rifampicin were administered for 3 weeks as prophylaxis, under guidelines of the Centers for Disease Control and Prevention.4 After exposure, these individuals did not develop brucellosis for at least 12 months.
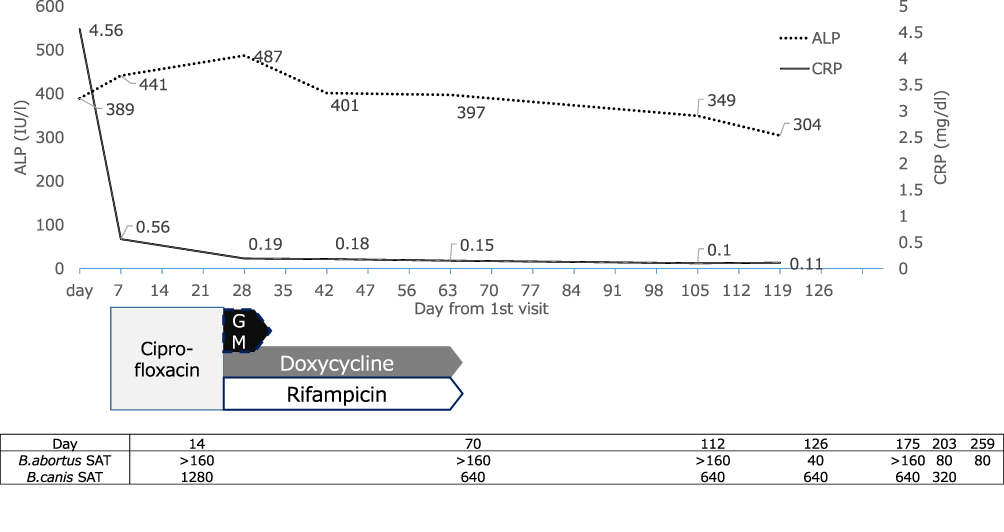 |
Figure 1 Clinical course. Abbreviations: ALP, alkaline phosphatase; CRP, C-reactive protein; GM, gentamicin. |
Discussion
In nonendemic countries, it is possible to treat immigrant patients with imported brucellosis, to prevent secondary brucellosis infection, an occupational hazard for laboratory technicians. As part of routine diagnostic services, positive blood culture findings should be carefully noted and scrutinized, to avoid initial misidentification of O. anthropi. The present report highlights that it is especially important for primary care physicians to assess information regarding a patient’s home country, such as previous employment, to avoid the spread of imported zoonoses. In the present era of a dramatically increasing number of immigrants and foreign travelers, language barriers must be overcome when providing medical care to immigrants or foreigners with fever of unknown origin.
Initially, a result of O. anthropi led to confusion about the patient’s etiology among the medical team because this pathogen is related to nosocomial infection among immunosuppressed patients.5 Therefore, the physicians carefully took a second history from the patient and his relative, upon notification of the similarity between O. anthropi and Brucella spp. by a well-trained laboratory technician. Owing to concerns about laboratory-acquired infections, some technicians underwent routine bacteriological testing. Brucella spp. can be transmitted via the respiratory mucosa, conjunctivae, gastrointestinal tract, or abraded skin.3 Formerly, laboratory technicians were trained to sniff bacterial colonies in the laboratory setting. In nonendemic countries such as Japan, some experts continue to advise technicians in training as well as in real-world settings to sniff bacterial colonies. However, there are differing opinions related to this procedure.6 Aerosolization is the main source of Brucella spp. transmission;5 therefore, samples suspected of being Brucella spp. and O. anthropi should be handled inside a biosafety cabinet, and sniffing examination by laboratory workers should be prohibited. In our case, the physician could not know about the risk of brucellosis because the patient did not mention his previous occupation as a stock breeder. The patient’s current occupation alerted the physician to possible occupational risks such as febrile illness caused by inhalation of zinc fumes (known as metal fume fever), which resulted in a misleading differential diagnoses. The long duration of incubation, from 1 week to several months,1 can cause a delay in recognizing brucellosis. Our patient had a relatively long incubation period of 1 month. The initial result misidentifying O. anthropi was shared among the medical team, which may have reduced transmission. More careful history-taking and more discerning judgment are necessary when dealing with patients who have a fever of unknown origin, especially if a language barrier exists.
The treatment for brucellosis is controversial. A meta-analysis published in 2008 recommended triple therapy with doxycycline, rifampicin, and gentamicin.7 In contrast, a later meta-analysis did not support triple therapy because it lacks substantial evidence and there is a concern about the high cost of treatment.8 In our patient, we selected the triple regimen because cost was not a restrictive factor under the national health insurance, which covers most medical costs. In addition, the high relapse rate, rather than the cost of treatment, should be the most important factor in choosing the treatment regimen. This patient declined to receive inpatient treatment because of his work; therefore, initial intravenous gentamicin was administered as outpatient parenteral antibiotic therapy.
The incidence of brucellosis differs worldwide, from the highest rate at 1603 per 1 million population in Syria,9 to nonendemic status in Japan, with only 14 human patients infected with livestock Brucella spp. (ie, B.melitensis and B. abortus) reported during 1999–2018. In contrast, mainland China has a rising prevalence of human brucellosis; the brucellosis prevalence is particularly high in northern regions of China bordering Mongolia and is expanding southward.10 Heilongjiang Province, where our patient formerly lived, has a relatively high prevalence rate of human brucellosis (4861 cases/100,000 population in 2010).10 In addition, a sporadic outbreak among livestock workers and veterinarians has been reported in South Korea, which was previously a nonendemic country but has been making efforts to control the spread of animal and human brucellosis infection.11,12 Over 1 million workers originally from foreign countries are currently working in Japan, of which the largest proportion (31.8%) are from China.13 A literature review of 505 imported cases of brucellosis included immigrants and foreign travelers.14 That review illustrated that most imported cases were associated with traditional risk factors, such as travel and/or consumption of unpasteurized dairy products in or from endemic countries. Our patient had strong exposure to risk factors owing to living in an endemic country and his involvement with diary production. In comparison with developing countries, pastoral Mediterranean countries have a higher potential risk of brucellosis. A case report from Japan also showed that consumption of natural cheeses in France may cause B. melitensis infection.15 Physicians should consider the possibility of brucellosis in patients from countries or areas with a higher prevalence of this disease.
Brucella spp. are highly contagious bacteria, and appropriate identification is important in public health practice. The highest incidence of infection associated with Brucella spp. is among laboratory technicians, with 641 cases per 100,000, as compared with 0.08 cases per 100,000 in the general population.3
Conclusion
We successfully treated a patient in which brucellosis was not initially suspected, which led to inadvertent exposure of laboratory technicians to this pathogen. In the present era of an increasing number of foreign travelers as well as workers entering Japan owing to revision of the immigration control law, primary care physicians in nonendemic areas must be vigilant regarding this pathogen. Close communication among physicians and laboratory technicians and careful assessment of factors related to a patient’s home country, which may require dealing with language barriers, are required to treat and prevent infection with this pathogen.
Consent For Publication
Written informed consent was obtained from the patient for publication of this case report.
Availability Of Data And Material
The authors agree to make the raw data and materials described in our manuscript freely available upon request.
Acknowledgments
We appreciate the contribution of the laboratory workers at Fukaya Red Cross Hospital, Shunsuke Watanabe, Shoya Watanabe, and Kazuhiko Nose. We also thank Analisa Avila of Edanz Group for editing a draft of this manuscript.
Author Contributions
TF clinically followed the patient and drafted the manuscript. NY and KI contributed to identifying the pathogen and advised as to the treatment of the patient. HS reviewed the manuscript. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pappas G, Akritidis N, Bosilkovski M, Tsianos E. Brucellosis. New Engl J Med. 2005;352:2325–2336. doi:10.1056/NEJMra050570
2. Norman FF, Monge-Maillo B, Chamorro-Tojeiro S, Perez-Molina JA, Lopez-Velez R. Imported brucellosis: a case series and literature review. Travel Med Infect Dis. 2016;14:182–199. doi:10.1016/j.tmaid.2016.05.005
3. Singh K. Laboratory-acquired infections. Clin Infect Dis. 2009;49:142–147. doi:10.1086/599104
4. Centers for Disease Control and Prevention. Brucellosis Reference Guide: Exposures, Testing and Prevention. Atlanta, GA: CDC; 2017. Available from: https://www.cdc.gov/brucellosis/pdf/brucellosi-reference-guide.pdf.
5. Gul HC, Brucellosis EH. Brucella species. In: Bennett JE, Dolin R, Blaser MJ, editors. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases.
6. Barkham T. Taylor MB Sniffing bacterial cultures on agar plates: a useful tool or a safety hazard? J Clin Microbiol. 2002;40:3877. doi:10.1128/JCM.40.10.3877.2002
7. Skalsky K, Yahav D, Bishara J, Pitlik S, Leibovici L, Paul M. Treatment of human brucellosis: systematic review and meta-analysis of randomised controlled trials. BMJ. 2008;336:701–704. doi:10.1136/bmj.39497.500903.25
8. del Pozo JSG, Solera J. Systematic review and meta-analysis of randomized clinical trials in the treatment of human brucellosis. PLoS One. 2012;7:e32090. doi:10.1371/journal.pone.0032090
9. Pappas G, Papadimitriou P, Akritidis N, Christou L, Tsianos EV. The new global map of human brucellosis. Lancet Infect Dis. 2006;6:91–99. doi:10.1016/S1473-3099(06)70382-6
10. Zhong Z, Yu S, Wang X, et al. Human brucellosis in the people’s republic of china during 2005–2010. Int J Infect Dis. 2013;17:e289–e292. doi:10.1016/j.ijid.2012.12.030
11. Mi-Yeoun Park C-SL, Choi Y-S, Park S-J, Lee J-S, Lee H-B. A sporadic outbreak of human brucellosis in korea. J Korean Med Sci. 2005;20:941–946. doi:10.3346/jkms.2005.20.6.941
12. Kim EK, Hwang JH, Hwang JH, Lee CS. Human Brucellosis Endemics in Korea? Yonsei Med J. 2017;58:259–260. doi:10.3349/ymj.2017.58.1.259
13. Ministry of Health, Labour and Welfare. http://www.mhlw.go.jp/stf/houdou/0000148933.html.
14. Norman FF, Monge-Maillo B, Chamorro-Tojeiro S, Pérez-Molina J-A, López-Vélez R. Imported brucellosis: a case series and literature review. Travel Med Infect Dis. 2016;14:182–199. doi:10.1016/j.tmaid.2016.05.005
15. Ikeda H, Nagamine K. [A case of Brucellosis with intermittent fever in a patient returning from France]. Kansenshogaku Zasshi.2016;90:138–141. Article in Japanese. doi:10.11150/kansenshogakuzasshi.90.138
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.