Back to Journals » Journal of Healthcare Leadership » Volume 17
Implicit Leadership Theories and Traits: A Qualitative Study of Managers in a Medical Sciences University
Authors Amini S ![]() , Rahati M
, Rahati M ![]() , Atash-Parvar S
, Atash-Parvar S ![]() , Panahi M
, Panahi M ![]() , Shahpari M
, Shahpari M
Received 17 June 2025
Accepted for publication 11 October 2025
Published 14 October 2025 Volume 2025:17 Pages 549—563
DOI https://doi.org/10.2147/JHL.S544837
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Zhanming Liang
Saeed Amini, Meghdad Rahati, Shabnam Atash-Parvar, Mahdieh Panahi, Marzieh Shahpari
Department of Health and Management Sciences, Khomein University of Medical Sciences, Khomein, Iran
Correspondence: Saeed Amini, Email [email protected]
Background: Understanding how healthcare professionals conceptualize leadership is vital for developing effective leadership development programs in medical universities. However, little is known about Implicit Leadership Theories (ILTs) within the unique context of Iranian medical universities, where education and healthcare service provision intersect.
Aim: This study explored implicit leadership expectations among faculty and staff in a medical university setting, emphasizing the novelty of examining ILTs in Iran’s academic health system and its potential relevance for similar institutions globally.
Methods: A qualitative phenomenological approach was employed to investigate ILTs among faculty and managers at Khomein University of Medical Sciences, a regional institution integrating healthcare services with clinical education. Fifteen participants were purposively sampled and interviewed using a semi-structured guide, drawn from twenty invited individuals. Data were analyzed using Colaizzi’s method with support from MAXQDA. Ethical approval was obtained, and informed consent was secured from all participants.
Results: Four domains of ILTs were identified: (1) ethical and personal traits such as honesty, justice, and humility; (2) managerial and organizational competencies and capabilities, including planning, decision-making, and accountability; (3) communication and relational behaviors emphasizing respect, empathy, and participation; and (4) structural and cultural conditions shaping leader effectiveness.
Conclusion: Findings highlight the need to align leadership behaviors with follower expectations to foster trust, strengthen leadership development, and enhance institutional performance. Situating ILTs in a non-Western academic health setting expands the global literature on leadership and followership, offering insights for medical universities in Iran and comparable systems internationally.
Keywords: implicit leadership theories, medical university, qualitative research, healthcare leadership
Introduction
Effective leadership is critical for the performance, resilience, and ethical functioning of academic health institutions, which must simultaneously deliver clinical services, educate future health professionals, and respond to evolving public health demands.1,2 While abundant research has examined formal leadership models and competencies, less is known about followers’ unconscious expectations, so-called Implicit Leadership Theories (ILTs), that shape how leaders are perceived and accepted in practice.3 In contexts such as medical universities, where clinical priorities, academic norms, and socio-political influences intersect, misalignment between leader behavior and follower expectations can undermine trust, hamper collaboration, and reduce institutional effectiveness.
ILTs are shaped by cultural, organizational, and professional norms, and studies show that expectations of leadership differ across societies. For example, research in Western contexts highlights autonomy, vision, and transformational qualities as central to ILTs,4–6 while Asian and Middle Eastern studies emphasize relational trust, ethical integrity, and collectivist values.7–9 Cross-cultural evidence suggests that while certain prototypes such as honesty and competence are widely recognized, the weight and expression of leadership expectations vary by context.10,11 This underscores the need to study ILTs in diverse healthcare and educational systems to clarify both universal and context-specific features.
Within healthcare organizations, ILTs have been linked to critical outcomes including teamwork, staff morale, patient safety, and the acceptance of clinical leaders.2,12,13 Epitropaki and Martin showed that congruence between leader behaviors and follower ILTs predicts higher satisfaction and effectiveness; similar findings in healthcare highlight that ethical credibility and effective communication strengthen trust and commitment.4 However, reviews also note that most ILT research in healthcare has been conducted in hospitals or corporate health settings, with limited focus on the academic medical environment where education and service provision intersect.14,15
Although ILTs have been studied in multiple organizational settings internationally,3–5 and a few Iranian studies have examined ILTs or followership prototypes in industrial or corporate contexts,16–18 there is a notable lack of empirical research exploring ILTs in the academic medical environment in Iran. Existing local studies have not specifically investigated how ILTs operate at the intersection of healthcare delivery and higher education, nor have they integrated individual ethical traits, managerial competencies, and structural/cultural conditions into a single, context-sensitive framework for medical universities. This absence of targeted investigation is significant because academic health institutions combine hierarchical clinical cultures, academic autonomy, and public sector governance—conditions that likely shape distinct ILTs and leadership expectations.
Filling this gap provides value on multiple levels. Theoretically, it extends ILT research into a complex institutional domain where leader legitimacy is not determined solely by managerial skill but also by ethical credibility, clinical understanding, and cultural fit. Practically, understanding ILTs can guide recruitment, selection, and leadership development tailored to academic health organizations, helping institutions design programs and appointment processes that align leader behaviors with follower expectations. Explicit attention to ILTs can also strengthen organizational trust, reduce the risks of disengagement or resistance, and ultimately improve institutional performance in medical universities. Addressing this gap additionally offers policy-relevant guidance for promoting meritocratic appointments and limiting adverse external influences that erode leadership legitimacy.
Accordingly, this study aims to:
- Explore the implicit leadership expectations (ILTs) held by faculty, clinical staff, and managers within a medical university;
- Identify the personal traits, managerial competencies, and relational behaviors that followers associate with effective leadership in this context; and
- Develop an integrated, context-sensitive leadership framework that links ILTs to organizational conditions and practical recommendations for leadership selection, development, and policy.
By empirically investigating ILTs in a medical university and proposing an integrated leadership framework for medical universities, this paper advances ILT scholarship into a novel institutional domain and offers actionable insights for leadership practice.
Materials and Methods
Research Procedure and Sample
This qualitative study was conducted in 2024 at Khomein University of Medical Universities in Iran, which is a regional Iranian institution offering healthcare services and clinical education. The research population consisted of middle and senior managers across clinical, educational, and administrative units. Participants were selected using purposive sampling, which was appropriate for exploring ILTs by engaging individuals with relevant managerial experience and direct involvement in leadership interactions.
To enhance diversity and representativeness, participants were drawn from different organizational domains (education, research, treatment, and administration), professional backgrounds (clinical and non-clinical), and hierarchical levels. This approach was intended to capture a wide range of perspectives reflective of the larger medical university context.
Inclusion criteria were: (i) at least three years of managerial or supervisory experience within the medical university system, (ii) willingness to participate voluntarily, and (iii) the ability to articulate experiences related to leadership expectations. Exclusion criteria included temporary or short-term administrative positions and individuals unwilling to provide informed consent.
A total of 12 individuals were invited, of whom 15 consented. From these, twelve were ultimately interviewed. The first twelve participants were selected to maximize variation across managerial domains, gender, and professional background. Data saturation was reached during the twelfth interview, at which point no new themes or codes emerged. The three additional volunteers were respectfully informed that their participation was not required once saturation had been confirmed. They were thanked for their willingness, and the decision was communicated clearly to avoid any perception of exclusion or devaluation of their consent. While purposive sampling does not allow for strict statistical generalization, the deliberate diversification of participants strengthens the transferability of findings to similar academic health institutions in Iran and comparable contexts internationally.
Research Instruments and Data Collection
Data were collected through semi-structured, in-depth interviews guided by an interview protocol developed from the literature on ILTs and leadership in healthcare. The guide included open-ended questions exploring participants’ expectations of effective leadership, perceived legitimacy of leaders, and experiences of alignment or misalignment between leader behaviors and institutional needs. Probing questions further examined ethical traits, managerial competencies, and contextual influences. All interviews were conducted by two members of the research team (SAP and MP) who were trained in qualitative interviewing and familiar with phenomenological methods. The interview guide was developed based on prior ILT literature4,6,15 and phenomenological research principles.19–21 To refine clarity and flow, the guide was pilot tested with two participants from a neighboring institution; no substantial modifications were required.
Interviews were conducted either face-to-face in participants’ offices or via secure online platforms (Microsoft Teams or Skype for Business), depending on participant preference and scheduling feasibility. Both platforms provided password-protected access and end-to-end encryption, ensuring confidentiality and data security during virtual interviews. Each session lasted between 45 and 75 minutes. Prior to data collection, informed consent was obtained, and confidentiality was assured. Recruitment was facilitated through formal invitations distributed by the university administration, followed by individual contacts. To ensure participants understood that their involvement was completely voluntary and that there would be no negative consequences for non-participation, the invitation emphasized the voluntary nature of the study. Participants were explicitly informed that declining or withdrawing from the study at any stage would not affect their professional standing or relationship with the institution. Additionally, verbal and written consent forms reinforced this, and participants were encouraged to ask any questions regarding the study before making their decision.
The interview guide was initially drafted in English and then translated into Persian (Farsi) for participant use. A forward–backward translation process was applied: two bilingual experts independently translated the guide into Persian, and an independent bilingual reviewer back-translated it into English. Any discrepancies were resolved through discussion within the research team, ensuring both semantic accuracy and cultural appropriateness.
All interviews were audio-recorded with participant permission and transcribed verbatim in Persian. Transcripts were anonymized and imported into MAXQDA 2022 for coding and thematic analysis using Colaizzi’s phenomenological method. The Colaizzi’s seven-step method is widely used in phenomenological health research to ensure systematic theme extraction.19,22 For clarity we used the following operational definitions: skills = discrete learned abilities; competencies = observable combinations of knowledge, skills and attitudes applied to tasks and measurable by performance; capabilities = broader adaptive capacity to integrate and deploy competencies in complex or novel contexts.
To enhance the rigor of the analysis, two members of the research team independently coded all transcripts. Initial codes were compared and discussed until consensus was achieved, ensuring inter-coder reliability and consistency of interpretation. Discrepancies were resolved through iterative discussion with the full research team, and the coding framework was refined accordingly. In addition, researcher reflexivity was addressed by maintaining reflective journals and analytic memos throughout the study, which allowed the team to document assumptions, monitor potential biases, and ensure that interpretations were grounded in participants’ accounts rather than researchers’ preconceptions. These strategies contributed to the credibility, dependability and trustworthiness of the findings.
Results
Participant Demographics
A total of 12 university managers were interviewed, including faculty members, clinical managers, and administrative leaders. The sample included both male and female participants, with an age range of 36–58 years and managerial experience ranging from three to over 20 years. Participants were drawn from diverse organizational domains—educational, clinical, and administrative units, ensuring a broad perspective on implicit leadership expectations in the medical university (Table 1).
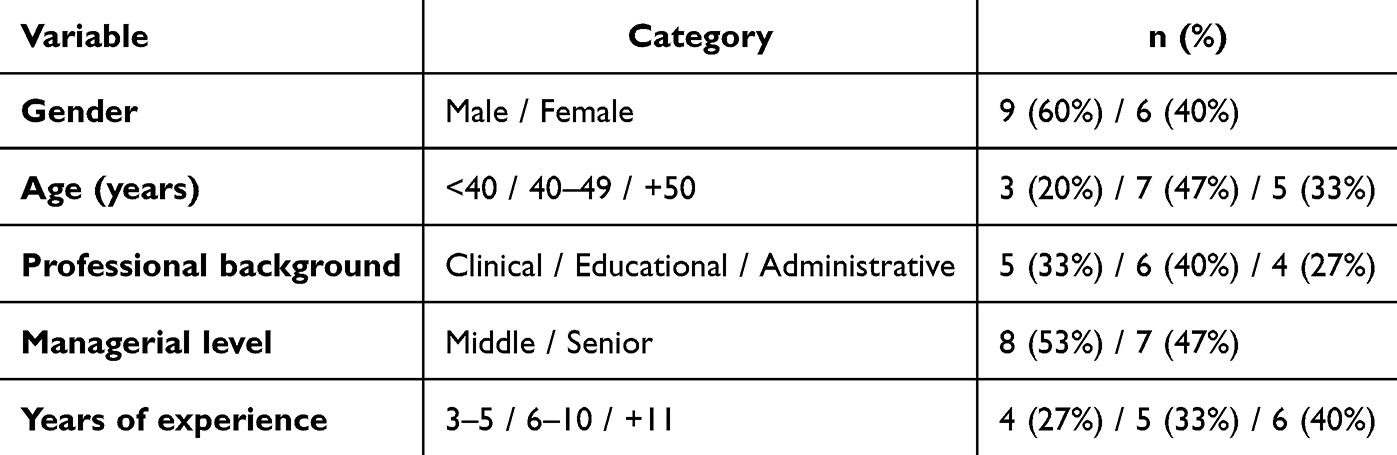 |
Table 1 Demographic Characteristics of University Managers Participating in the Study (N = 15) |
Emergent Themes
Data were analyzed using Colaizzi’s seven-step phenomenological method, which involved: (1) reading all transcripts to acquire a sense of the whole, (2) extracting significant statements, (3) formulating meanings, (4) clustering meanings into themes, (5) developing an exhaustive description, (6) producing the fundamental structure, and (7) validating findings with participants (member checking). Analysis of interviews revealed a rich array of perspectives regarding effective and ineffective leadership in a medical academic context. Data were organized into four major thematic domains: (1) Personal and Ethical Leadership Traits, (2) Managerial and Organizational Competencies, (3) Communication and Relationship-Oriented Behaviors and (4) Structural and Cultural Conditions. These domains were derived using Colaizzi’s phenomenological method, ensuring that recurring themes across the data were systematically categorized. The domains reflect the key patterns identified from participants’ responses, which were cross-checked and validated by multiple team members to ensure consistency and representativeness of the findings. Each domain encompassed multiple subcategories derived from repeated patterns in the data (Table 2).
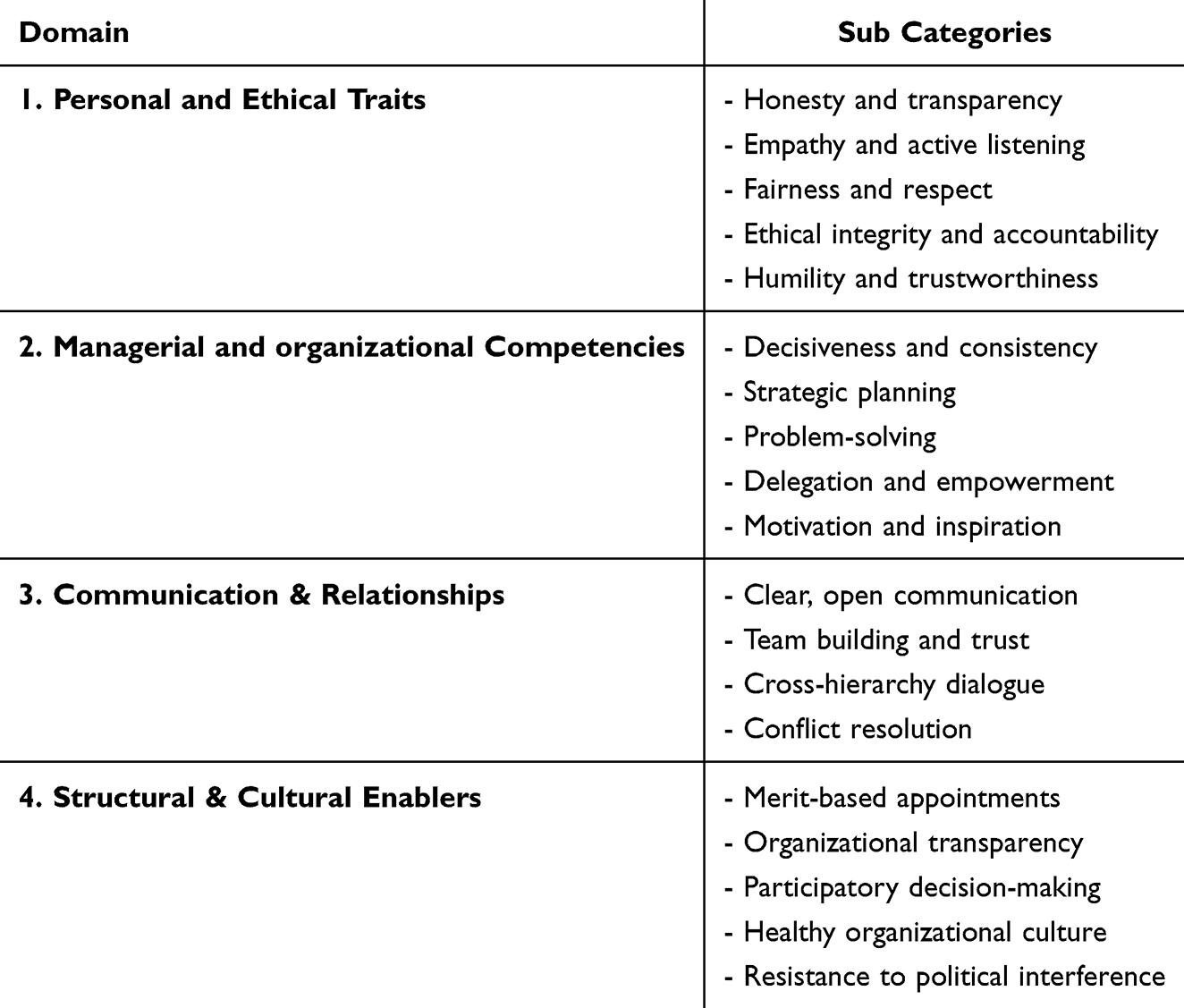 |
Table 2 Key Domains and Subcategories of Implicit Leadership Theories in Medical Universities |
Personal and Ethical Leadership Traits
Participants overwhelmingly emphasized that effective leadership begins with strong personal and ethical foundations. Traits such as honesty, transparency, fairness, respect, humility, and organizational commitment were repeatedly cited as essential to building trust and sustaining ethical behavior within the institution. These qualities were seen not only as moral imperatives but also as practical tools for building cohesive teams and reducing organizational conflict.
Honesty and transparency were considered the cornerstone of leadership credibility. Leaders who openly communicated decisions—especially difficult ones—were more likely to gain long-term trust. Fairness and respectful treatment were described as indicators of emotional maturity, with several participants emphasizing the impact of perceived injustice on morale.
One participant noted:
Even when our supervisor had to make difficult decisions, their honesty made us trust the process. Transparency and fairness really set the tone for the whole department.
Another added:
Listening with empathy and giving everyone a chance to speak made us feel valued, even when the outcome didn’t go our way.
The concept of organizational commitment also emerged as a vital trait, with leaders described as role models who work beyond formal obligations and embody a strong sense of institutional loyalty. Participants valued leaders who “put the organization first” in both routine matters and during crises.
A manager explained:
I saw our dean staying late many times to solve staff issues—he didn’t have to do it, but he cared. It made us care more too.
Another reflected:
He never made us feel small. Whether you were a janitor or a professor, he treated you with the same respect—and that respect motivated everyone to work harder.
These narratives demonstrate that personal and ethical leadership traits are not just idealized values but active, daily behaviors that shape workplace culture. Participants made clear that leaders who embody ethical principles through consistent action generate loyalty, emotional commitment, and psychological security within the organization.
Managerial and Organizational Competencies
Beyond personal integrity, participants emphasized the need for leaders to demonstrate high-level managerial competencies and strategic organizational capabilities. These included the ability to make timely and effective decisions, manage crises, plan strategically, delegate appropriately, and guide teams through complex institutional challenges.
A strong emphasis was placed on decisiveness—leaders were expected to make informed decisions confidently, without hesitation or favoritism, particularly in resource-limited or politically sensitive environments. Participants also described the value of systems thinking and macro-level planning, noting that leaders must not only solve immediate problems but also align actions with broader institutional goals. In addition, the transfer of knowledge and experience was described as a critical function of effective leadership. Leaders were seen as mentors who should coach their subordinates, build internal capacity, and develop future leaders. Understanding personality types, managing interpersonal dynamics, and customizing communication styles were also valued as signs of a mature and competent leader.
One participant shared:
A capable leader doesn’t just tell people what to do—they show them how, pass on experience, and grow others around them. That’s what builds sustainable leadership.
Another remarked:
You could see the difference in his crisis management. He stayed calm, assessed the situation, and quickly involved the right people. That’s when you realize who’s fit to lead.
Participants stressed that problem-solving is a core expectation, particularly in the healthcare and academic setting, where operational obstacles are frequent. Leaders who could analyze complex problems, propose feasible solutions, and adapt quickly to changing circumstances were perceived as highly effective.
As one manager put it:
Our former director always had a plan B. If something failed, he didn’t blame people—he pivoted fast. That flexibility saved us many times.
Another explained:
Strategic vision isn’t just about long documents; it’s about daily decisions that align with long-term goals. A good leader keeps that vision alive in every meeting.
Taken together, these perspectives illustrate that in addition to moral character, a successful academic leader must possess practical competencies that support execution, resilience, and team empowerment. Participants viewed leadership as both a human and technical competency set, one that must balance emotional intelligence with tactical ability.
Communication and Relationship-Oriented Behaviors
A distinct and recurrent theme in participants’ narratives was the importance of communication and relational competence in leadership. Effective leaders were described as those who engage in transparent, respectful, and inclusive communication with all levels of staff. This includes the ability to listen actively, provide constructive feedback, manage interpersonal dynamics, and build trust-based relationships across the organization.
Participants emphasized that strong communication was not merely a soft skill but a core competency and strategic asset, central to fostering collaboration, reducing misunderstandings, and promoting a positive workplace climate. Several participants linked poor leadership communication to organizational disengagement and inefficiency.
One manager described:
When I spoke to him, it felt like I was the only person that mattered. He gave his full attention and listened without interrupting—it really encouraged me to be more engaged in my work.
Another noted:
A good leader communicates not only with superiors but also with the team on the ground. They don’t just give orders—they explain, involve, and respond. That’s how you build trust.
A third participant explained:
Our department only started functioning properly when the new head came in and opened up communication channels—suddenly people felt heard and valued. It made a real difference.
These statements reflect a strong consensus that relational leadership fosters psychological safety and promotes mutual respect. Leaders who prioritize listening, approachability, and interpersonal awareness are seen as catalysts for team cohesion and professional growth.
Structural and Cultural Conditions
Participants highlighted that effective leadership is not solely a function of individual traits or competencies, but is also significantly influenced by the structural and cultural environment in which leadership occurs. Leaders operate within systems shaped by policies, institutional traditions, and socio-political dynamics, factors that can either support or hinder their effectiveness. A transparent and merit-based selection process was repeatedly emphasized as a foundational condition for cultivating trust and legitimacy. Participants expressed concern that political appointments, favoritism, and informal power networks undermine the credibility of leadership and diminish staff morale.
One participant explained:
When leaders are appointed based on connections rather than competence, everyone notices. It demotivates those who’ve worked hard, and people lose faith in the system.
A healthy organizational culture, characterized by fairness, teamwork, and openness, was considered essential. Participants noted that leaders have the power to shape culture through their behaviors and decisions. In contrast, a toxic culture, marked by rivalry, backbiting, or secrecy, was seen as a major barrier to collaboration and performance.
Another participant shared:
You can have a capable leader, but if the environment encourages division and distrust, even the best efforts will fail. Leadership and culture have to work together.
Cultural alignment emerged as a recurring issue:
We need leaders who understand the organizational culture—what motivates staff, what creates conflict, and how to build a fair, unified environment.
Additionally, delegation of authority and participatory management were viewed as structural supports that enhance leadership impact. Participants expressed that when leaders encourage staff input, create space for dialogue, and distribute responsibilities appropriately, employees feel more invested and productive. This inclusivity not only improves performance but also strengthens the social fabric of the institution.
Moreover, resistance to political interference and clear boundaries between leadership and external power structures were considered critical for safeguarding institutional integrity. Participants suggested that even competent leaders often struggle under pressure from political actors, especially in public institutions. These views reinforce the idea that leadership in academic medical settings must be supported by systemic fairness, cultural coherence, and organizational transparency. Without these enabling conditions, even well-intentioned leaders may find their efforts constrained or derailed.
Impact of Leadership Traits on Organizational Outcomes
In addition to identifying essential leadership traits and competencies, participants consistently linked these characteristics to tangible organizational outcomes. These effects were discussed in relation to employee morale, operational efficiency, institutional credibility, and long-term success.
For instance, ethical integrity—including honesty, fairness, and transparency—was closely associated with trust-building, team cohesion, and a sense of psychological safety. Participants described how ethical leaders reduce internal conflict and set a cultural tone that promotes accountability. Similarly, strategic and operational competencies, such as decision-making, crisis management, and systems thinking, were viewed as crucial to ensuring goal alignment, resource optimization, and organizational resilience. Leaders who could manage uncertainty while maintaining long-term vision were seen as catalysts for progress and adaptability.
Empathy and active listening were often connected with higher levels of employee engagement, loyalty, and reduced burnout. Participants emphasized that leaders who genuinely listened to concerns and responded thoughtfully created environments where staff felt valued and motivated to contribute. Furthermore, transparency in communication and decision-making was linked to a greater perception of organizational justice. This reduced ambiguity and speculation, and in turn fostered higher morale and trust in leadership.
One participant noted:
When our leader was open about challenges and decisions, it felt like we were all in it together. It made us more committed—not just to the leader, but to the whole institution.
Another added:
Respectful leadership isn’t just nice to have—it’s productive. People don’t waste energy dealing with politics or fear. They focus on their work.
The findings also highlight the critical role of institutional structure, including merit-based appointments and participatory practices, in reinforcing leadership legitimacy. Leaders seen as fair and competent—particularly those chosen transparently—garnered stronger organizational support and fostered long-term engagement among staff. These linkages are summarized in Table 2, which maps key leadership traits to their perceived organizational effects, based on participant narratives (Table 3).
 |
Table 3 Impact of Leadership Traits on Organizational Outcomes |
Discussion
This study explored ILTs among managers in a medical sciences university, identifying four overarching categories: personal and ethical characteristics, managerial competencies, communication and relationship-building skills, and structural–cultural conditions. The findings emphasize that leadership in this context is perceived as an integrative phenomenon shaped not only by individual attributes but also by organizational culture and external expectations. These results are consistent with previous studies highlighting the significance of ethics, integrity, and trust in leadership.6,23,24 At the same time, they extend the literature by showing how context-specific cultural norms, such as favoritism or hierarchical decision-making, influence perceptions of leadership effectiveness.25,26 Compared with prior research, the present study underlines the role of structural and cultural conditions in shaping ILTs, which are often underexplored in existing models. While leadership theories developed in Western contexts emphasize individual competence and vision,2,8 our findings suggest that in medical universities, relational trust, organizational justice, and context-based ethics play equally critical roles.10,19,27 These insights support the view that leadership is socially constructed and contingent upon cultural and institutional settings.
Theoretical Implications
The study contributes to ILTs theory by integrating both individual and contextual dimensions of leadership. Specifically, it highlights how ethical orientation, humility, and fairness—elements deeply rooted in cultural values, shape implicit expectations of effective leaders. This extends prior models that have largely centered on cognitive schemas of individual traits.7,28
The findings also contribute to the broader healthcare leadership literature by situating ILTs within the organizational and cultural realities of medical universities. While earlier frameworks emphasize transformational or transactional leadership styles,12,29 our data reveal that managers implicitly value leaders who balance ethical responsibility with managerial competencies, such as resource allocation and policy compliance. This suggests that leadership in health education systems requires both moral legitimacy and administrative expertise. Moreover, the proposed integrated leadership framework advances theoretical understanding by showing that leadership effectiveness cannot be understood solely through personal traits but must account for systemic factors such as organizational justice, favoritism, and participatory culture. These insights refine existing ILT perspectives and contribute to a deeper understanding of leadership in non-Western and healthcare-specific contexts.
Proposed Conceptual Model: The Integrated Leadership Framework for Medical Universities
Based on the thematic synthesis of participant insights, this study proposes a contextually grounded, three-tiered leadership model tailored to the complexities of academic health institutions (Figure 1). The Integrated Leadership Framework for Medical Universities is designed to bridge individual, organizational, and systemic levels of leadership, reflecting the dynamic interplay between personal values, strategic action, and institutional culture.
 |
Figure 1 Integrated Leadership Framework for Medical Universities. |
Core Leadership Identity (Individual Level)
At the foundation of the model lies the personal and ethical identity of the leader. Participants consistently described effective leaders as those who embody integrity, emotional intelligence, humility, and authenticity. These traits are not just character attributes—they serve as the ethical compass that guides behavior, decision-making, and interpersonal relationships. In healthcare academia, where leaders operate within high-stakes, emotionally charged environments, personal credibility and trustworthiness are indispensable. Leaders who possess a strong moral core foster respect, inspire loyalty, and model ethical conduct for others to emulate.
Strategic and Operational Capacities (Organizational Level)
The second tier of the framework emphasizes the managerial and strategic competencies necessary for effective leadership in complex, resource-constrained academic environments. These include the ability to plan and prioritize, delegate responsibilities, manage crises, build high-functioning teams, and lead organizational change. Participants emphasized that leaders must move beyond day-to-day administrative duties and instead think systemically—aligning immediate actions with long-term institutional goals. Importantly, effective leaders must not only possess these competencies but also be able to transfer them to others, building organizational capabilities and resilience through mentorship and empowerment.
Contextual and Cultural Alignment (Institutional Level)
At the highest level, leadership must be attuned to the organizational structure, socio-cultural norms, and political realities of the academic institution. Participants underscored that leadership effectiveness is deeply influenced by external and internal contexts—including institutional history, cultural expectations, and political interference. Leaders who navigate these challenges with wisdom, uphold meritocratic principles, and actively resist favoritism or unethical influence contribute to a healthy organizational culture. They build legitimacy not by asserting power but by aligning leadership behavior with collective values and institutional needs.
This tripartite framework moves beyond generic leadership models by explicitly addressing the interdependencies between personal ethics, operational skill, and contextual intelligence. It recognizes that academic medical leaders must be both morally grounded and strategically agile, while also culturally responsive and politically aware. Leaders who integrate these three domains are more likely to earn the trust of their teams, maintain organizational coherence, and sustain long-term institutional progress. In summary, the Integrated Leadership Framework for Medical Universities offers a roadmap for identifying, developing, and evaluating leaders who are equipped to meet the demands of today’s academic healthcare landscape. It encourages institutions to view leadership not as a static role but as a dynamic, multi-level function that must be cultivated across individual, operational, and systemic domains.
Clarifying Terms: Skills, Competencies, and Capabilities
To avoid conceptual ambiguity, we explicitly distinguish three commonly conflated terms because our participants used related language that we initially reported interchangeably. Skills are the discrete, teachable abilities or proficiencies an individual possesses (for example: active listening, minute-taking, conflict-mediation). Competencies are observable, measurable combinations of knowledge, skills, and attitudes (KSAs) applied to achieve specific professional tasks or outcomes (for example: “strategic decision-making competency” combines knowledge of systems, analytical skills, and relevant judgment). Capabilities refer to broader adaptive capacity: the ability of an individual (or organization) to integrate and deploy multiple competencies under changing, complex, or novel conditions (for example: the capacity to lead through political pressure, resource scarcity, or crisis). This distinction, skills = building blocks; competencies = KSAs applied to tasks and measurable performance; capabilities = adaptive, integrative capacity, aligns with recent syntheses of leadership and management literature and competency frameworks in health contexts.30–33
Implication for Interpreting Our Findings
When participants emphasized honesty, transparency, and humility they were primarily referring to personal traits that underpin competency in ethical leadership (ie, the set of KSAs that generate ethical decision-making and fair practices). When they emphasized decision-making, planning, and crisis management they were describing leadership competencies (measurable combinations of KSAs). References to flexibility, systems-level thinking, and navigating political pressures point to capability, the leader’s adaptive capacity to integrate competencies across novel institutional constraints. Interpreting our themes with this terminology increases conceptual precision and helps translate qualitative insights into concrete selection, training, and evaluation strategies (eg, measurable competency assessments versus capability-building exercises).
Why These Distinctions Matter in a Medical-University Setting
Medical universities combine two interdependent missions—education and clinical service—creating work demands that differ from single-mission organizations. In such hybrid settings, a candidate may demonstrate required skills (eg, teaching or a particular clinical technique) yet lack the competencies to align departmental goals with institutional strategy, or the capabilities to adapt when clinical service demands shift rapidly (for example, during service surges or regulatory change). Our data show that followers do not evaluate leaders on skills alone: they assess whether leaders demonstrate integrated competencies (fair resource allocation, evidence-based decision processes) and, crucially, whether those competencies cohere into capability when the system is stressed (eg, political interference, sanctions, or resource constraints). This explains why ethical credibility and contextual savvy emerged as central expectations alongside technical managerial skills.
Transferability & Implications for Other Iranian and International Medical Universities
Although our study is single-site, the dual-mission character of medical universities is common across Iran and some other countries; similar features (hierarchical clinical cultures, public governance, and competing academic and service priorities) have been documented in recent studies of academic medicine and medical education leadership.33,34 Therefore:
- Selection and appointment: Selection processes should assess not only discrete skills or credentials but validated competencies (measurable KSAs) and indicators of capability (past performance in complex or politically constrained environments). This suggests use of multi-source assessments (behavioral interviews, situational judgment tests, and portfolio review) rather than only CV review.
- Leadership development: Training curricula should be twofold, (1) competency-based modules that teach and measure task-specific KSAs (eg, strategic planning, financial stewardship), and (2) capability-building experiences (action learning, cross-unit rotations, crisis simulations, mentoring) that foster adaptability, systems thinking, and political navigation.
- Organizational design and policy: Institutional safeguards (transparent appointment procedures, merit-based promotion, and protected decision-making spaces) are important system-level enablers that allow competencies to translate into capability. Our participants’ concerns about favoritism and political appointment indicate that system design mediates whether an otherwise competent leader can exercise capability effectively; thus, policy reforms that strengthen meritocracy and participatory governance are likely to improve leader legitimacy across similar institutions.
Practical Relevance for International Medical Universities
For institutions outside Iran the distinction remains relevant: in resource-rich settings capability may look different (eg, digital transformation leadership), but the three-tier logic is portable — teach skills, measure competencies, and design experiences that build capability. Recent global leadership frameworks emphasize the same multilevel approach to leadership preparation (competency taxonomies combined with adaptive, practice-based development).33,34 Thus our model (ethical identity → managerial competencies → contextual capability) can guide tailored interventions in diverse academic health systems while encouraging local adaptation to cultural and governance contexts.
Practical Implications
The findings carry important implications for leadership development and policy in medical universities. First, leadership training programs should emphasize ethical leadership, fairness, and trust-building, as these were consistently identified as core expectations by participants. Embedding ethics and integrity into leadership curricula can strengthen legitimacy and organizational cohesion.
Second, recruitment and promotion systems should prioritize managerial competencies aligned with the ILTs identified in this study. For example, selection processes can include assessments of strategic planning, problem-solving, and communication competencies, alongside evaluations of ethical commitment and fairness. This approach can reduce the risk of favoritism and increase transparency in leadership appointments.
Third, the results underscore the importance of cultivating a participatory and supportive organizational culture. Policies that encourage open communication, teamwork, and reduced hierarchical barriers may enhance leadership effectiveness and employee engagement.14,35 Concrete initiatives such as structured mentoring, peer feedback mechanisms, and ethics-based performance reviews can operationalize these recommendations in practice.
The final domain, structural and cultural conditions, represents a unique extension of ILT frameworks. While ILTs are typically conceptualized as cognitive schemas residing within followers,3,4 our findings suggest that contextual conditions, such as bureaucratic structures, external political influences, and cultural expectations, shape which prototypes become salient in practice. This emphasizes the dynamic interaction between individual schemas and institutional environments.
Importantly, while our study interviewed managers, their views should not be interpreted solely as leaders’ self-perceptions. Rather, these managers articulated the leadership qualities they expect and value in others, which indirectly reflects their own followership prototypes. This distinction highlights the interconnectedness of implicit leadership and implicit followership theories, reinforcing the argument that leadership perceptions are co-constructed through leader–follower interactions.5
A further contribution of this study lies in extending ILTs research into a non-Western academic health context. Most ILTs literature originates from Western, corporate, or hospital settings.3–5,12 By focusing on an Iranian medical university, this research provides insights from a system that combines higher education, clinical care, and public governance, illustrating how ILTs are shaped in environments marked by different cultural and institutional logics. Such contributions expand the global relevance of ILT scholarship by demonstrating both universal prototypes and context-specific expectations.
At the same time, the generalizability of these findings must be considered with caution. Iran’s academic health system operates under conditions shaped by international sanctions, resource constraints, and unique socio-political dynamics. These conditions may amplify expectations of ethical integrity, justice, and accountability in leaders, while also constraining opportunities for leadership development. Although these features limit direct transferability, they also offer valuable lessons for other low- and middle-income countries facing structural challenges in academic health leadership.
Another contextual consideration is the organizational form of medical education. In countries such as Iran, Turkey, and China, medical universities are established as standalone institutions directly managing both academic and healthcare services. In contrast, in many Western countries, medical schools are embedded within comprehensive universities, where governance and leadership structures differ. This global distinction underscores why ILTs in Iranian medical universities may emphasize competencies related to dual missions of clinical service delivery and academic training more strongly than in embedded medical schools.
Limitations and Future Research Recommendations
This study is not without limitations. The qualitative design and focus on a single medical university limit the generalizability of findings. While rich insights were obtained, the results may not fully represent other institutions or cultural settings. Future studies should apply the framework to multiple universities and cross-cultural contexts to enhance transferability. Additionally, the reliance on participants’ narratives means that the findings reflect perceived rather than directly observed leadership behaviors. Future research could adopt mixed-methods approaches, combining qualitative insights with surveys or longitudinal assessments to validate and expand upon the present results. Finally, while this study highlighted faculty managers’ perspectives, future investigations could include other stakeholders such as students, clinical staff, and policymakers. This broader lens would provide a more comprehensive understanding of ILTs in healthcare education.
In summary, this study contributes to ILT scholarship by integrating ethical, managerial, relational, and contextual dimensions into an Integrated Leadership Framework for Medical Universities. By situating the analysis in Iran, it adds to the growing body of non-Western ILT literature and demonstrates the importance of cultural and structural conditions in shaping leadership expectations. Future research could compare ILTs across different medical universities globally, exploring how institutional forms and cultural settings moderate the salience of leadership prototypes.
Conclusion
This study revealed that effective leadership in academic medical institutions is perceived through a combination of ethical integrity, strategic competency, and contextual alignment. Managers value traits such as honesty, fairness, decisiveness, and cultural sensitivity, which shape implicit expectations of ideal leadership. The proposed Integrated Leadership Framework highlights three essential domains—individual character, operational capacity, and institutional alignment—offering a practical model for leadership development in medical universities. Institutions aiming to enhance leadership effectiveness should prioritize merit-based appointments, ethical conduct, and culturally responsive practices. Aligning leadership behavior with these implicit expectations can strengthen organizational trust, improve performance, and foster a more cohesive institutional culture. Further research across diverse academic health settings is recommended to validate and refine the model.
Ethical Considerations
The study protocol was approved by the Ethics Committee of Khomein University of Medical Sciences (Approval No: IR.KHOMEIN.REC.1402.014). All participants provided written informed consent after receiving detailed information about the study’s purpose, procedures, confidentiality, and the voluntary nature of participation. Anonymity was maintained in all transcripts and reports. In addition, participants granted explicit consent for the publication of anonymized direct quotes from their interviews.
Acknowledgments
The authors would like to thank the participants of this study and the Department of Health and Management Sciences, Khomein University of Medical Sciences, for their support.
Funding
This research was funded by Khomein University of Medical Sciences.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Yukl G. Leadership in Organizations.
2. West M, Armit K, Loewenthal L, Eckert R, West T, Lee A. Leadership and leadership development in health care: the evidence base. 2015.
3. Shondrick SJ, Dinh JE, Lord RG. Developments in implicit leadership theory and cognitive science: applications to improving measurement and understanding alternatives to hierarchical leadership. Leadersh Q. 2010;21(6):959–978. doi:10.1016/j.leaqua.2010.10.004
4. Epitropaki O, Martin R. Implicit leadership theories in applied settings: factor structure, generalizability, and stability over time. J Appl Psychol. 2004;89(2):293. doi:10.1037/0021-9010.89.2.293
5. Lord RG, Maher KJ. Leadership and Information Processing: Linking Perceptions and Performance. Routledge; 2002.
6. Ling Q, Liu F, Wu X. Servant versus authentic leadership: assessing effectiveness in China’s hospitality industry. Cornell Hospitality Q. 2017;58(1):53–68. doi:10.1177/1938965516641515
7. Ardichvili A, Kuchinke KP. Leadership styles and cultural values among managers and subordinates: a comparative study of four countries of the former Soviet Union, Germany, and the US. Human Res Dev Int. 2002;5(1):99–117. doi:10.1080/13678860110046225
8. Brodbeck FC, Chhokar JS, House RJ. Culture and leadership in 25 societies: integration, conclusions, and future directions. In: Culture and Leadership Across the World. Psychology Press; 2007:1057–1118.
9. Silverthorne C. Leadership effectiveness and personality: a cross cultural evaluation. Pers Individ Dif. 2001;30(2):303–309. doi:10.1016/S0191-8869(00)00047-7
10. Den Hartog DN, House RJ, Hanges PJ, et al. Culture specific and cross-culturally generalizable implicit leadership theories: are attributes of charismatic/transformational leadership universally endorsed? Leadersh Q. 1999;10(2):219–256. doi:10.1016/S1048-9843(99)00018-1
11. Javidan M, Dorfman PW, De Luque MS, House RJ. In the eye of the beholder: cross cultural lessons in leadership from project GLOBE. Acad Manag Perspectives. 2006;20(1):67–90. doi:10.5465/amp.2006.19873410
12. Al-Amin M, Makarem SC, Rosko M. Efficiency and hospital effectiveness in improving Hospital Consumer Assessment of Healthcare Providers and Systems ratings. Health Care Manag Rev. 2016;41(4):296–305. doi:10.1097/HMR.0000000000000076
13. Wong C, Cummings G. Authentic leadership: a new theory for nursing or back to basics? J Health Organiz Manage. 2009;23(5):522–538. doi:10.1108/14777260910984014
14. West MA, Eckert R, Steward K, Pasmore WA. Developing Collective Leadership for Health Care. London:King’s Fund;2014.
15. Daly J, Jackson D, Mannix J, Davidson PM, Hutchinson M. The importance of clinical leadership in the hospital setting. J Healthcare Leadership. 2014;75–83. doi:10.2147/JHL.S46161
16. Akhavan Tabassi A, Ramli M, Hassan Abu Bakar A, Hamid Kadir Pakir A. Transformational leadership and teamwork improvement: the case of construction firms. J Manag Dev. 2014;33(10):1019–1034. doi:10.1108/JMD-01-2012-0003
17. Akhavan Tabassi A, Hassan Abu Bakar A. Towards assessing the leadership style and quality of transformational leadership: the case of construction firms of Iran. J Technol Manag China. 2010;5(3):245–258. doi:10.1108/17468771011086256
18. Gil-Cordero E, Ledesma-Chaves P, Ortega-Gutierrez J, Han H. Organizational value and participatory leadership for sustaining the competitive advantages of hospitality and tourism companies. Humanit Soc Sci Commun. 2023;10(1):1–17. doi:10.1057/s41599-023-01881-x
19. Groenewald T. A phenomenological research design illustrated. Int J Qual Methods. 2004;3(1):42–55. doi:10.1177/160940690400300104
20. Moustakas C. Phenomenological Research Methods. Sage;1994.
21. Giorgi A. The theory, practice, and evaluation of the phenomenological method as a qualitative research procedure. J Phenomenolog Psychol. 1997;28(2):235–260.
22. Morrow R, Rodriguez A, King N. Colaizzi’s descriptive phenomenological method. Psychologist. 2015;28(8):643–644.
23. Engelbrecht AS, Heine G, Mahembe B. Integrity, ethical leadership, trust and work engagement. Leadership Org Dev J. 2017;38(3):368–379. doi:10.1108/LODJ-11-2015-0237
24. Brown ME, Treviño LK. Ethical leadership: a review and future directions. Leadersh Q. 2006;17(6):595–616. doi:10.1016/j.leaqua.2006.10.004
25. Farh J-L, Cheng B-S. A cultural analysis of paternalistic leadership in Chinese organizations. In: Management and Organizations in the Chinese Context. Springer; 2000:84–127.
26. Hofstede G, Hofstede GJ, Minkov M. Cultures and Organizations: Software of the Mind.
27. Aina OA, Verma KK, editors. Effect of leadership style on organizational commitment. In: 2017 Pan Pacific Microelectronics Symposium (Pan Pacific). IEEE; 2017:1–15.
28. Schyns B, Hansbrough T. When Leadership Goes Wrong: Destructive Leadership, Mistakes, and Ethical Failures. IAP; 2010.
29. Bass BM, Riggio RE. Transformational Leadership. Psychology press; 2006.
30. Kakemam E, Liang Z. Guidance for management competency identification and development in the health context: a systematic scoping review. BMC Health Serv Res. 2023;23(1):421. doi:10.1186/s12913-023-09404-9
31. Heinen M, van Oostveen C, Peters J, Vermeulen H, Huis A. An integrative review of leadership competencies and attributes in advanced nursing practice. J Adv Nurs. 2019;75(11):2378–2392. doi:10.1111/jan.14092
32. Burke EM, Fox JA, Tager K, McDowell S, Phelps F, Koh H. Toward a public health leadership national training agenda: a review of conceptual frameworks and core competencies. Front Public Health. 2025;13:1630046. doi:10.3389/fpubh.2025.1630046
33. Dash NR, Koutaich R, Al Khalaf HA, Hani MJ, Koutaich R, Guraya SY. The Framework of Leadership in Academic Medicine (FLAM); a mixed-methods study to develop leadership skills and competence. 2023.
34. Collins IIRT, Purkey NJ, Singh M, DeSantis AD, Sanford RA. The four Cs of physician leadership: a key to academic physician success. Qual Res Med Healthcare. 2024;8(2):11519. doi:10.4081/qrmh.2024.11519
35. Burke CS, Sims DE, Lazzara EH, Salas E. Trust in leadership: a multi-level review and integration. Leadersh Q. 2007;18(6):606–632. doi:10.1016/j.leaqua.2007.09.006
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
What It Takes to Manage Change: A Qualitative Study of Healthcare Managers’ Role Perceptions in Supporting and Sustaining TeamSTEPPS Implementation
Lüchinger R, Blondon K, Junod Perron N, Audétat MC
Journal of Healthcare Leadership 2026, 18:584769
Published Date: 30 April 2026