Back to Journals » Research and Reports in Urology » Volume 14
Implementation of a Standardized Renal Trauma Protocol at a Level 1 Trauma Center: 7-Year Protocol and 10-Year Institutional Review
Authors Werner Z, Haffar A ![]() , Bacharach E, Knight-Davis J, Hajiran A, Luchey A
, Bacharach E, Knight-Davis J, Hajiran A, Luchey A
Received 24 November 2021
Accepted for publication 3 January 2022
Published 17 March 2022 Volume 2022:14 Pages 79—85
DOI https://doi.org/10.2147/RRU.S349504
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Guglielmo Mantica
Zachary Werner,1 Ahmad Haffar,2 Emma Bacharach,1 Jennifer Knight-Davis,3 Ali Hajiran,1 Adam Luchey1
1Department of Urology, West Virginia University, Morgantown, WV, USA; 2School of Medicine, West Virginia University, Morgantown, WV, USA; 3Department of Surgery, West Virginia University, Morgantown, WV, USA
Correspondence: Ahmad Haffar, School of Medicine, West Virginia University, Suite 6300 Health Sciences Center Morgantown, Morgantown, WV, 26505, USA, Tel +304 993-2237, Fax +304 293-2807, Email [email protected]
Objective: Current urologic renal trauma guidelines favor conservative management. In 2012, we implemented an institution-wide renal trauma protocol to standardize management. This protocol details initiation of DVT (deep vein thrombosis) prophylaxis, cessation of bed rest, and frequency of laboratory studies. We hypothesized that low-grade injuries (grade I–III) could be managed without urologic consultation and that our chemical DVT prophylaxis regimen would not pose an increased risk of hemorrhage requiring transfusion.
Methods: We performed a cross-sectional analysis of a prospectively maintained database containing all renal trauma at our institution from 2009 to 2019. We segregated injuries based on grade, presence of multi-organ trauma, and evaluated the presence and types of intervention, initiation of chemical DVT prophylaxis, and post-DVT prophylaxis hemorrhage requiring transfusion.
Results: We identified 295 cases of renal trauma, of which 62 were isolated injuries. Forty-three of the isolated renal injuries were transferred from outside facilities, 70% of which were classified as low-grade injuries. There were 220 low-grade lacerations and 75 high-grade lacerations. No grade I or II lacerations required any interventions. Two (2.5%) grade III lacerations required IR embolization. Twenty-five (41%) grade IV lacerations required intervention, of which five were nephrectomy. Seven (54%) grade V lacerations required intervention, of which 5 were nephrectomies. Upon review of our protocol with early ambulation and DVT prophylaxis, there were no cases of isolated renal injury where initiation of either treatment resulted in delayed hemorrhage requiring transfusion or surgical intervention.
Conclusion: Only 2/220 low-grade renal lacerations required intervention. Our data suggest that grade I and II renal lacerations can be managed safely without urologic consultation. Consultation is warranted for grade III injuries given the possibility of initial understaging. Furthermore, we believe our renal laceration protocol in our admittedly small, isolated sample has shown our DVT prophylaxis initiation to not pose increased risk.
Keywords: renal, trauma, review, protocol, thromboembolic
Introduction
The management of acute renal trauma has undergone a paradigm shift since the 1980s, toward increasingly conservative management. The validity of the non-operative approach has been bolstered by technological advances that allow for better risk stratification and by the development of minimally invasive procedures such as selective angioembolization. Multiple guidelines, such as the Association of Urology (EAU) and American Urological Association (AUA) guidelines for blunt genitourinary trauma, recommend an initially conservative approach in hemodynamically stable patients.1,2 However, due to the paucity of prospective clinical trials regarding management, there remains a lack of clarity regarding optimal treatment protocols for these patients, including criteria for admission, frequency of hematologic parameters and vital signs, timing of ambulation and chemoprophylaxis initiation, and activity restrictions. Thus, significant heterogeneity is present in the approach to renal injuries among different healthcare centers.3,4
At our level-one trauma center, a renal trauma protocol was developed and instituted in 2012 to help streamline patient management and address heterogeneity among trauma surgery and urology services. The protocol addressed issues such as initial and repeat imaging, laboratory draw frequency, deep vein thrombosis prophylaxis (DVT), and ambulation, amongst other considerations. We referenced the American Association for the Surgery of Trauma (AAST) organ injury grading system to better manage our patients based on associated risk. Of particular interest was the timing of chemical DVT prophylaxis because trauma patients are known to be at increased risk for venothrombotic events.5–7 However, given the highly vascular nature of the kidney, there exists the possibility of inadvertently causing a significant hemorrhagic event after initiation of prophylaxis.
In this study, our objective was to evaluate our institutional renal trauma protocol to determine opportunities to better manage patients with low grade renal injuries. We further desired to characterize the risk of hemorrhage associated with early implementation of DVT prophylaxis in renal injuries. Patients with isolated low-grade injuries are an ideal population to evaluate risk as other multi-organ injuries could confound any derived conclusions. It is our belief that examining renal trauma at our institution could potentially help improve patient outcomes, decrease the need for transfer, reduce unnecessary cost, and act as a model for other institutions or clinicians.
Methods
After approval by our institutional review board (Protocol # 1307059849R007), a renal trauma database was developed extending to patients treated since 2009. An institution-wide renal trauma protocol was developed in 2012 and is available below in Table 1. The patients’ renal injury was classified based on the American Association for the Surgery of Trauma (AAST) renal injury scale, where severity is assessed according to the depth of renal parenchymal damage and involvement of the urinary collection system and renal vessels. Patients were managed according to the grade of injury following the protocol, as shown in Table 1. The database was prospectively maintained as a collaborative effort between the Departments of Urology and Trauma Surgery. We retrospectively reviewed all graded renal injuries at our institution from 2009 to the most recent data in 2019. Isolated injuries were distinguished by the absence of any other concomitant solid bone or organ injuries. For all injuries, we characterized demographic data, injury grade, need for interventions and type of intervention. Interventions in our study included “minimally invasive” techniques such as angioembolization. For isolated renal trauma, we additionally characterized initiation of DVT prophylaxis, post-DVT prophylaxis hemorrhage requiring transfusion, length of stay, and hemoglobin upon discharge. Advanced statistical analyses beyond this characterization did not yield statistically meaningful results given the confounding effects of management of multi-organ trauma and the small sample size of isolated renal trauma.
 |
Table 1 West Virginia University Hospital’s Renal Injury Protocol (2012–2019) |
Results
Patient demographics are shown in Table 2. A total of 295 cases of renal laceration were identified with 74.6% (n = 220) low grade (grades I–III) renal injuries and 25.4% (n = 75) high grade (grades IV–V) lacerations. Blunt injuries constituted 270 of these injuries. The majority of patients were male with a median age of 28.5 years. Of the 295 injuries, a total of 62 were isolated injuries. Interestingly, 43 of these 62 isolated injuries were transferred to our institution for elevation of care, the majority of which were low-grade injuries (30/43). Overall, the rate of intervention was low (34/295) with only 2 interventions performed on low-grade injuries, both of which were IR embolization of grade III injuries. The characterization of interventions performed is shown in Table 3. Of the isolated renal injuries only 18 of the 62 received chemical DVT prophylaxis as shown in Table 4. In many cases, this was due to the patient being discharged home on the day of or prior to initiation of DVT prophylaxis. However, within this population, none of the patients required post-DVT prophylaxis transfusion. Urologic follow-up was limited with 30 of 62 isolated patients returning, 13 of whom were children.
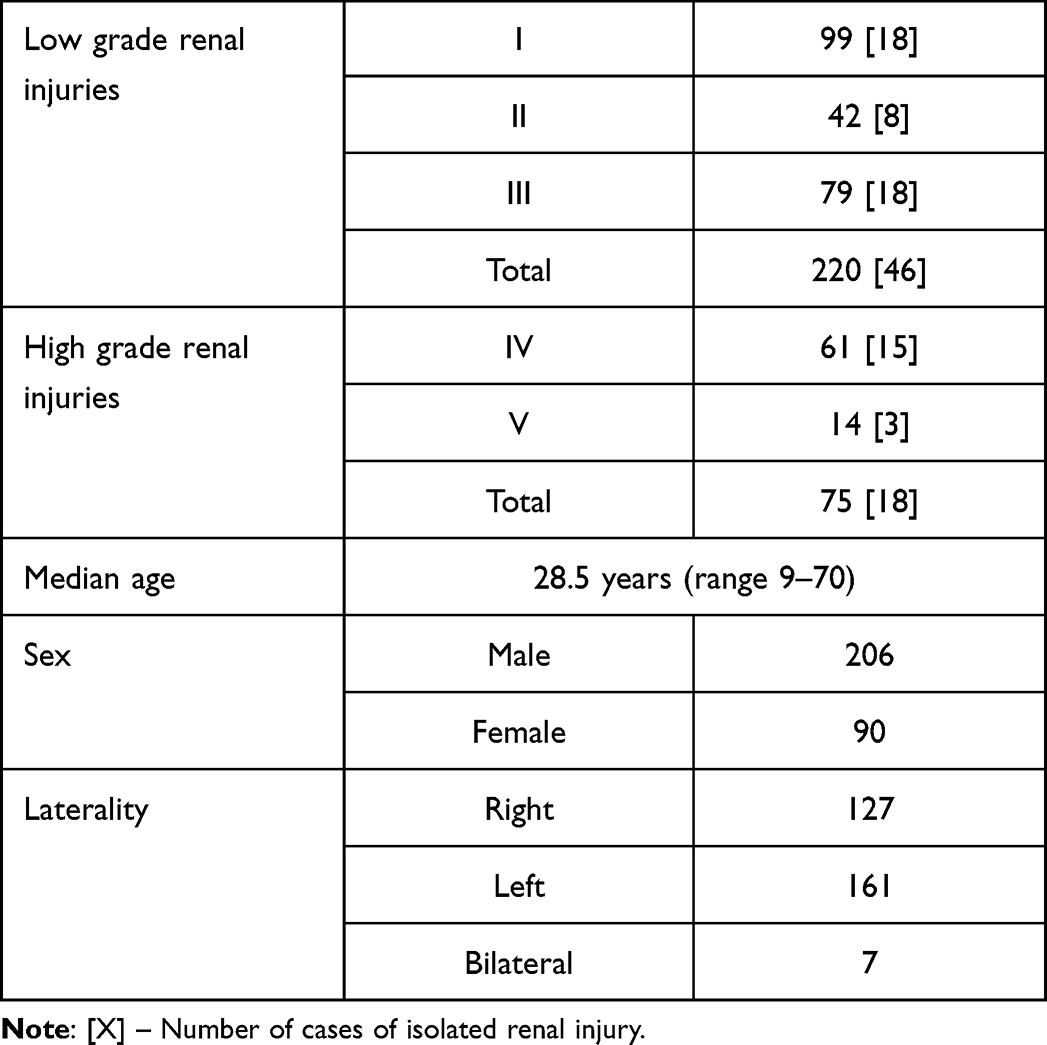 |
Table 2 Patient Demographics |
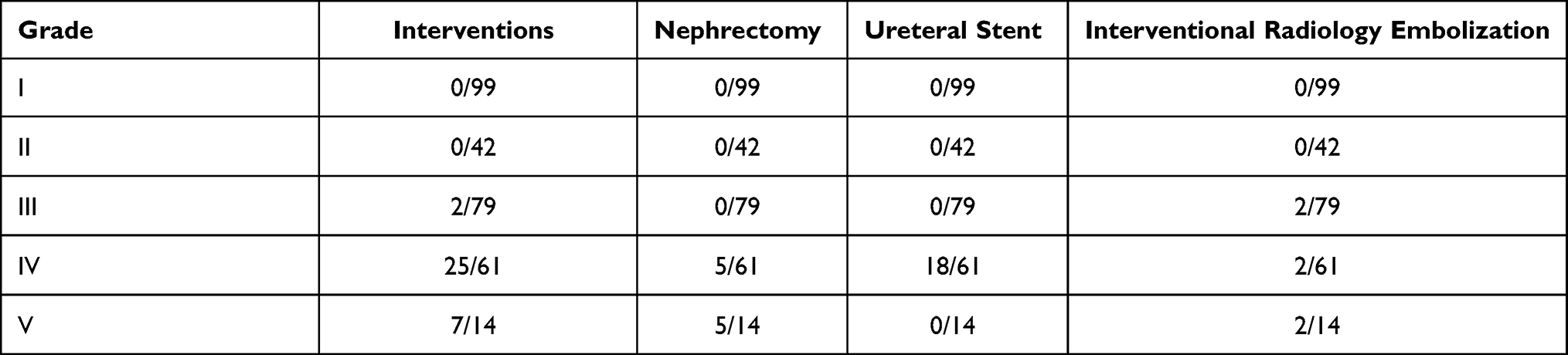 |
Table 3 Interventions Performed |
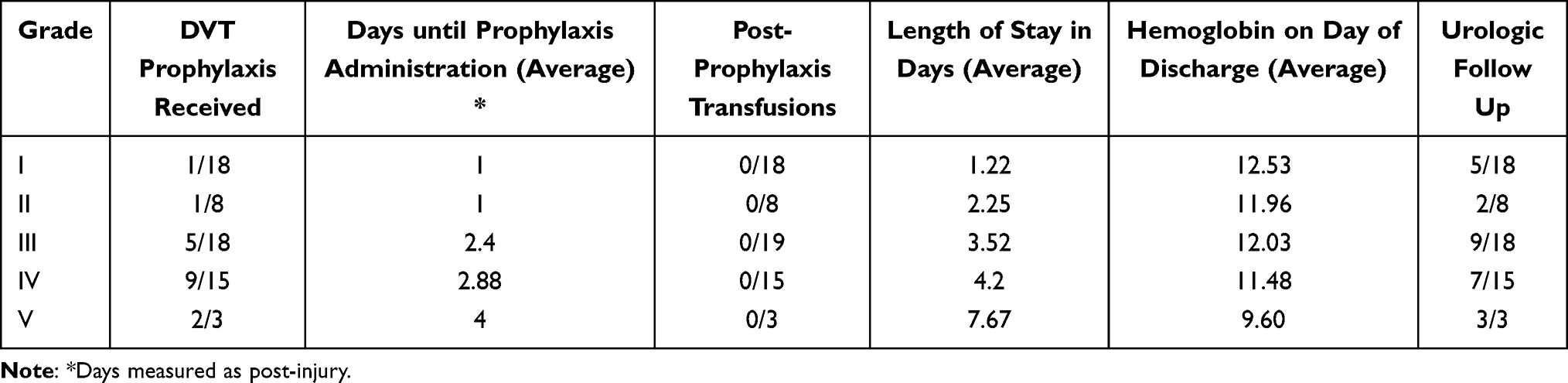 |
Table 4 Isolated Renal Injury |
Discussion
In summary, the vast majority of low-grade renal injuries at our institution have been managed non-operatively for the past ten years, in keeping with current practice. Implementation of our protocol, which at the time was characterized by early ambulation and DVT prophylaxis, did not reveal evidence of harmful effects, such as hemorrhage or requirement of surgical intervention. Of note, ambulation and prophylaxis were initiated regardless of the presence or absence of gross hematuria. Our results bolster the idea of conservative management of renal trauma and indicate DVT prophylaxis and early ambulation should be included in standardized renal trauma protocols. However, clinicians must be careful when encouraging early ambulation, as it can be easily mistaken by overenthusiastic patients. Clinicians should exercise caution when incorporating these findings into their renal trauma protocols, as further study is needed. One of the most striking findings was the overutilization of medical resources for low-grade injuries, including urologic consultation and transfer of care.
In 2014, specific recommendations were published by the Urological Society of Australia and New Zealand (USANZ), which detailed conservative managements such as bedrest, serial examinations, antibiotics, frequency of hemoglobin draws, and imaging studies.3 They recommended, along with others, against routine follow-up imaging or antibiotic prophylaxis in low-grade injuries.3,4,8 Hemodynamic stability of the patient is the highest priority, and unstable patients with renal injury should be considered for embolization or laparotomy if embolization is not feasible.3,8
Our protocol created in 2012 shares many similarities with the USANZ protocol, especially regarding low grade renal trauma. The protocol has undergone alterations, such as reduced bed rest and sooner thromboprophylaxis, but has otherwise largely remained unchanged as noted in Table 5. Notably, our protocol administers thromboprophylaxis to all renal trauma patients, whereas the USANZ guidelines recommend decisions based on a case by case basis and against routine use.3 This is additionally in contrast to those who may have instituted risk assessment profiles such as the Greenfield Risk Assessment Profile.9,10 In our sample, we had no cases requiring transfusion following initiation of DVT prophylaxis in isolated renal injury. Of the ten high-grade isolated renal injuries who received chemical DVT prophylaxis, there was no requirement for any subsequent surgical intervention or transfusion. Two of these high-grade injuries were initially managed with transfusion of packed red blood cells and received enoxaparin at post-trauma day 3 without any further transfusion requirement. It is important to note that a large proportion of our patients did not receive thromboprophylaxis. Typically, this was due to the patient being discharged home on the day of or prior to initiation of DVT prophylaxis. Although specific follow-up data regarding any incidence of venous thromboembolic events is lacking, this begs the question of whether many patients should receive any chemical DVT prophylaxis if they have quickly been deemed appropriate for discharge. Discharge was advocated for patients who were afebrile, tolerating regular diet with adequate pain control, and maintaining a stable hemoglobin.3,11 Coincidentally, the Western Trauma Association recently updated their guidelines regarding initiation of DVT prophylaxis and, accordingly, many of our isolated trauma patients who did not receive chemoprophylaxis would likely have fallen into a low-risk category.12
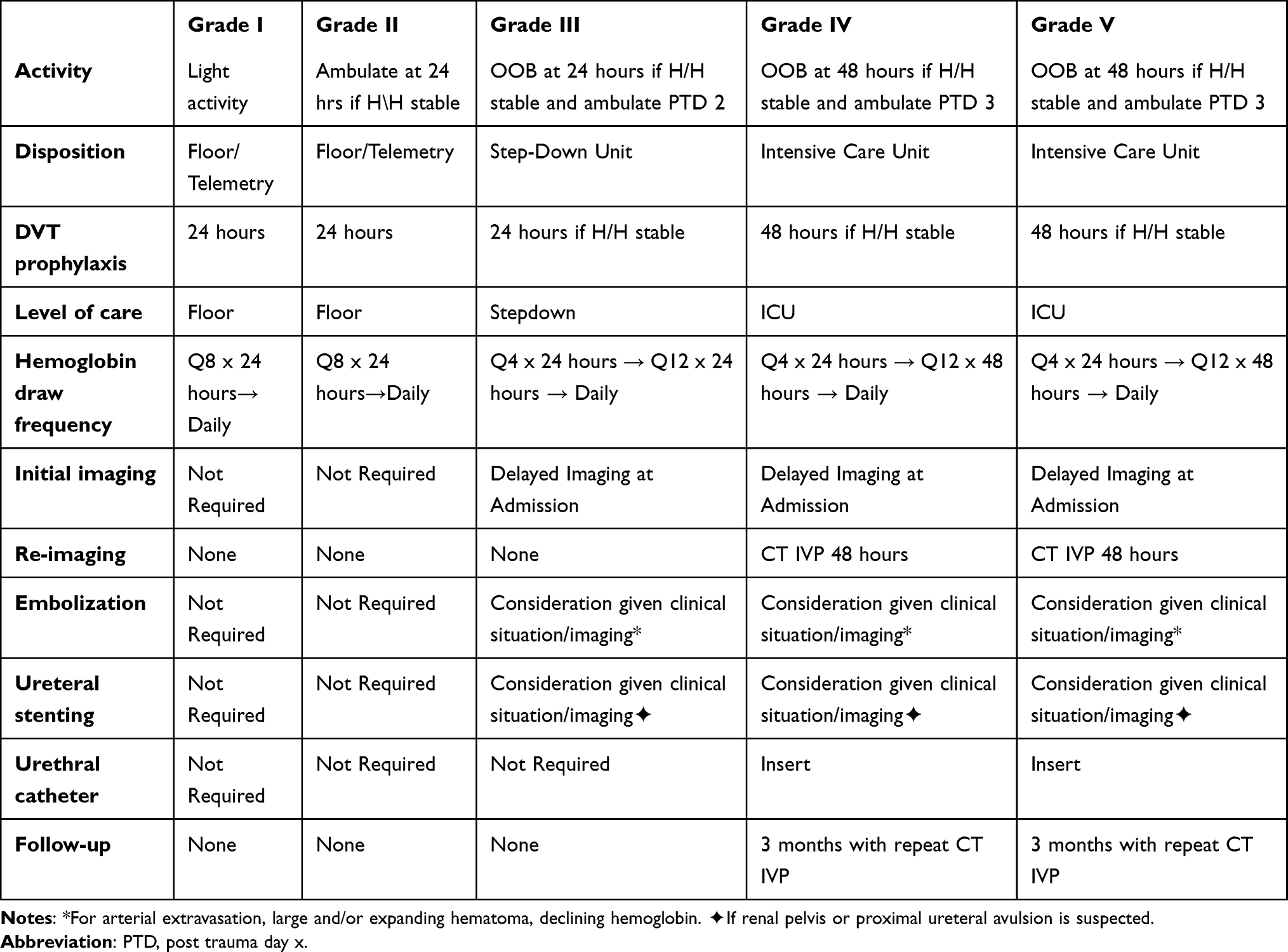 |
Table 5 West Virginia University Adult Renal Trauma Protocol (2020) |
Interestingly, of the 45 isolated low-grade injuries, 32 were transferred from outside facilities for management. Of these patients, only one underwent any procedure, which was conducted by interventional radiology. This could indicate a lack of knowledge or comfort among rural providers regarding the current best practice conservative management, especially in the setting of low-grade renal injury. However, our data make clear that the vast majority of isolated renal injuries, especially low-grade injuries, may be safely managed without transfer to a tertiary care center. Given West Virginia’s status as the state with the lowest median family income in the country and the high cost of patient transfer, we recommend against transfer for management of low-grade isolated renal injuries.13 This represents an area where community outreach and education may have a meaningful impact on patient care and overall medical cost.
Our database included all renal trauma regardless of age. The AUA guidelines apply to both adults and children, although within the field there appears to be discrepancy regarding certain protocols. Children are at increased risk of renal injury with blunt abdominal trauma given their relative increased renal size and mobility.14 Recently, a large literature review with management guidelines was published in The Journal of Trauma and Acute Care Surgery.15 The article concluded with broad recommendations that pediatric renal trauma be managed nonoperatively in hemodynamically stable patients, with angioembolization rather than surgery in hemodynamically stable patients with high-grade injuries and undergo routine blood pressure checks to monitor for post-trauma hypertension.15 In our study, all pediatric patients underwent initial CT imaging for diagnosis, however patients variably underwent renal ultrasound and CT IVP for follow-up imaging. This indicates that an area of improvement and initiation of a pediatric renal trauma protocol is underway. Furthermore, a pediatric-specific protocol with subsequent review of outcomes may provide additional data to the field for more concrete guidelines.
In 2020, after a review of the available literature and our own internal data, we updated our renal trauma protocol to be more reflective of current, conservative practice as shown in Table 5. Specific changes were made to the day of ambulation and initiation of DVT prophylaxis. Given the low rate of intervention, we will likely make further changes to reduce the frequency of laboratory testing and alter the disposition to be based on clinical status rather than imaging findings. Further consideration is especially warranted for further reduction in DVT prophylaxis in the isolated low-grade renal trauma population given their typically low-risk profile.
Our study is inherently limited by its design as a prospectively collected but retrospectively reviewed database. It provides a modest sample size for renal trauma in general and is notable for having adhered to a conservative protocol since its inception with minimal changes, unlike similar, longer running studies.16 The vast majority of injuries in our database were secondary to blunt injuries, and thus any conclusions may not apply as strongly to penetrating injuries. As with most studies on trauma, our study suffers from a general lack of follow-up. Given our rural patient population and large proportion of transfers from bordering states, this lack of follow-up is to be expected. There was a disappointing lack of adherence to the protocol regarding thromboprophylaxis in isolated renal injuries, typically due to early discharge. Overall, our study confirms the principle of conservative management in renal trauma and provides a measure of support regarding the safety of thromboprophylaxis in renal trauma, although further study is required in this area.
Conclusion
In conclusion, a review of all renal trauma managed at our level-one trauma center from 2009 to 2019 revealed consistently conservative management, especially regarding low-grade renal injury. Given the lack of urologic intervention in any low-grade renal trauma, there remains an overutilization of medical resources both in the form of urologic consultation and in the context of institutional transfers. Early initiation of ambulation and DVT prophylaxis in isolated renal trauma, while small in sample size, revealed no evidence of increased risk of hemorrhage or surgical intervention. Given these findings, we have altered our renal trauma protocol and would recommend that other institutions treating blunt renal trauma consider the inclusion of early DVT prophylaxis and ambulation in their renal trauma protocol, as further study is required in this field.
Statement of Ethics Approval
Approval of our study was granted by the West Virginia University's Institutional Review Board (Protocol # 1307059849R007). Additional specific ethical approval was not required. The study is a retrospective chart review dating back approximately 10 years, including transient patients admitted for trauma. Information was de-identified upon entry into the database. Therefore, obtaining informed consent for each individual was deemed neither feasible nor necessary.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Morey A, Brandes S, Dugi D, et al. Urotrauma: AUA guideline. J Urol. 2014;192(2):327–335. doi:10.1016/j.juro.2014.05.004
2. Summerton DJ, Djakovic N, Kitrey ND, et al. Guidelines on urological trauma, limited update 2018. Available from: http://uroweb.org/guideline/urologicaltrauma/.
3. Mccombie S, Thyer I, Corcoran N, et al. The conservative management of renal trauma: a literature review and practical clinical guideline from Australia and New Zealand. BJU Int. 2014;114(Suppl 1):13–21. doi:10.1111/bju.12902
4. Malcolm J, Derweesh I, Mehrazin R, et al. Nonoperative management of blunt renal trauma: is routine early follow-up imaging necessary? BMC Urol. 2008;8:11. doi:10.1186/1471-2490-8-11
5. Geerts W, Code K, Jay R, et al. A prospective study of venous thromboembolism after major trauma. N Engl J Med. 1994;331:1601–1606. doi:10.1056/NEJM199412153312401
6. Geerts W. Prevention of venous thromboembolism in high-risk patients. Hematology Am Soc Hematol Educ Program. 2006;2006(1):462–466. doi:10.1182/asheducation-2006.1.462
7. Knudson MM, Ikossi DG, Khaw L, et al. Thromboembolism after trauma: an analysis of 1602 episodes from the American College of Surgeons National Trauma Data Bank. Ann Surg. 2004;240(3):490–498. doi:10.1097/01.sla.0000137138.40116.6c
8. Shoobridge JJ, Corcoran NM, Martin KA, et al. Contemporary management of renal trauma. Rev Urol. 2011;13(2):65–72.
9. Hegsted D, Gritsiouk Y, Schlesinger P, et al. Utility of the risk assessment profile for risk stratification of venous thrombotic events for trauma patients. Am J Surg. 2013;205(5):517–520. doi:10.1016/j.amjsurg.2013.01.022
10. Greenfield LJ, Proctor MC, Rodriguez JL, et al. Posttrauma thromboembolism prophylaxis. J Trauma. 1997;42(1):100–103. doi:10.1097/00005373-199701000-00017
11. Fraser JD, Aguayo P, Ostlie DJ, et al. Review of the evidence on the management of blunt renal trauma in pediatric patients. Pediatr Surg Int. 2009;25(2):125–132. doi:10.1007/s00383-008-2316-4
12. Ley E, Brown C, Moore E, et al. Updated guidelines to reduce venous thromboembolism in trauma patients: a Western Trauma Association critical decisions algorithm. J Trauma Acute Care Surg. 2020;89(5):971–981. doi:10.1097/TA.0000000000002830
13. United States Census Bureau. 2018 Median Household Income in the United States; Updated September 26, 2019. Available from: https://www.census.gov/library/visualizations/interactive/2018-median-household-income.html.
14. Casale AJ. Urinary Tract Trauma: Pediatric Urology. Philadelphia, PA: Elsevier Inc; 2010:720–736.
15. Hagedorn JC, Fox N, Ellison JS, et al. Pediatric blunt renal trauma practice management guidelines: collaboration between the Eastern Association for the surgery of trauma and the pediatric trauma society. J Trauma Acute Care Surg. 2019;86(5):916–925. doi:10.1097/TA.0000000000002209
16. Hampson LA, Radadia KD, Odisho AY, et al. Conservative management of high-grade renal trauma does not lead to prolonged hospital stay. Urology. 2018;115:92–95. doi:10.1016/j.urology.2017.11.018
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.