Back to Journals » Clinical Ophthalmology » Volume 19
Implementation of a Modified Risk Stratification Score in Cataract Surgery at a Swiss Public Hospital
Authors Kaiser KP ![]() , Turgut F, Ernst SCK, Somfai GM, Zoellin JRT
, Turgut F, Ernst SCK, Somfai GM, Zoellin JRT ![]() , Saad A, Davolio N, Hornberger U, Nilius H, Heussen JS, Becker MD, Heussen FM
, Saad A, Davolio N, Hornberger U, Nilius H, Heussen JS, Becker MD, Heussen FM ![]()
Received 3 June 2025
Accepted for publication 26 August 2025
Published 9 September 2025 Volume 2025:19 Pages 3307—3316
DOI https://doi.org/10.2147/OPTH.S544354
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Bharat Gurnani
Klemens Paul Kaiser,1,2,* Ferhat Turgut,1,3– 5,* Sophie-Christin Kornelia Ernst,1,3,6 Gabor Mark Somfai,1,3,5 Jay Rodney Toby Zoellin,1 Amr Saad,1,3 Noah Davolio,1 Ute Hornberger,1,3 Henning Nilius,7 Julie Susan Heussen,1,3 Matthias Dieter Becker,1,3,8 Florian M Heussen1,3,9
1Department of Ophthalmology, Stadtspital Zürich, Zurich, Switzerland; 2Department of Ophthalmology, Goethe-University, Frankfurt am Main, Germany; 3Werner H. Spross Foundation for the Advancement of Research and Teaching in Ophthalmology, Zurich, Switzerland; 4Gutblick Research, Pfäffikon, Switzerland; 5Department of Ophthalmology, Semmelweis University, Budapest, Hungary; 6Department of Ophthalmology, University Hospital Basel, Basel, Switzerland; 7Department of Clinical Chemistry, Inselspital University Hospital Bern, Bern, Switzerland; 8Department of Ophthalmology, University of Heidelberg, Heidelberg, Germany; 9Department of Ophthalmology, Inselspital, University Hospital Bern, Bern, Switzerland
*These authors contributed equally to this work
Correspondence: Florian M Heussen, Department of Ophthalmology, Inselspital, University Hospital Bern, Freiburgstrasse 10, Bern, 3010, Switzerland, Email [email protected]
Introduction: This study evaluates the impact of a modified risk stratification system on intraoperative complication rates in cataract surgeries conducted at a Swiss Public Hospital.
Methods: In this retrospective study cataract surgeries were analyzed before and after implementation of the Triemli Cataract Score (TCS) at a public referral hospital. The TCS was utilized to classify patients preoperatively based on their risk profile, categorizing cases into three levels of complexity: “routine”, “complex”, and “highly complex”. The primary endpoint is the frequency of intraoperative complications pre-/post-TCS implementation, as well as alignment with the designated risk groups.
Results: A total of 1776 eyes were included in the study, with 704 eyes (39.6%) assessed prior to and 1072 (60.4%) post-TCS implementation. Overall, intraoperative complications were observed in 146 surgeries (8.2%), with a higher incidence observed before (9.5%) compared to post-TCS (7.4%; p=0.054). Post-TCS, 625 (63.2%) were classified as “routine”, 250 eyes (25.3%) as “complex”, and 113 eyes (11.4%) as “highly complex”, based on their risk factors. The intraoperative complication rate varied significantly among these groups (p=0.014): the lowest rate was seen in the routine group (5.6%), followed by the highly complex group (8.8%), and the highest in the complex group (11.2%).
Discussion: Implementing a risk stratification system for cataract surgery enables efficient and consistent preoperative categorization of patients into defined risk groups. This approach has the potential to reduce intraoperative complications, improve the comparability of study outcomes, streamline the classification process for surgeons, and establish structured checkpoints for training ophthalmic surgeons.
Keywords: cataract surgery, risk stratification, cataract score, intraoperative complications
Introduction
Since its inception, cataract surgery has evolved rapidly, becoming the most frequently performed surgery worldwide.1,2 Advances in technology and the refinement of phacoemulsification techniques have transformed it into a primarily outpatient procedure, yielding better visual and refractive outcome alongside a substantial reduction in intraoperative complications.3–6 Although phacoemulsification with intraocular lens implantation is generally considered routine, with intraoperative complication rates between 3–10% have been reported depending on institutional, geographic, and surgeon-related factors, it remains technically demanding, with minimal margin for error.7–10 While most adverse events are transient or pose little threat to vision, some may result in significant, long-term visual impairment.11 Several risk stratification systems for cataract surgery have been developed and effectively implemented.12,13 A widely adopted stratification model was introduced by Muhtaseb et al, based on an analysis of intraoperative complications in 1441 cataract surgeries.14–16 This model identifies anatomical and demographic risk factors - including age, ametropia, previous surgeries (eg, vitrectomy), corneal scarring, pupil size, anterior chamber depth, pseudoexfoliation, cataract stage and phakodonesis – each linked to a higher likelihood of complications, such as posterior capsule rupture. Each factor assigned a point value based on its potential to increase surgical risk, resulting in a cumulative score that categorizes patients into one of four risk groups. This system supports (1) improved preoperative counseling for individual patients; (2) allocation of patients to surgeons based on patient risk profile, and (3) risk-adjusted comparisons of outcomes across surgeons and institutions.
In 2019, a preoperative risk stratification system was incorporated into the routine preoperative assessment of patients referred for cataract surgery at Stadtspital Zürich. Multiple existing risk stratification models were evaluated using two key criteria: (1) practicality for use in an outpatient setting, and (2) ability to reliably differentiate between low-risk cases and those with complex or highly complex profiles. The scoring system proposed by Muhtaseb et al was selected as the most suitable foundation and was subsequently modified to better align with the hospital’s specific needs.15
This study aims to evaluate the impact of implementing the modified risk stratification system in daily practice within a public hospital setting. Additionally, it seeks to investigate the correlation between cataract risk scores and the rates of intra- and postoperative complication.
Methods
This single-center, retrospective, comparative clinical study was conducted at the public eye hospital Stadtspital Zürich, Zurich, Switzerland, including surgeries performed between January 2019 and December 2022. For this study a positive vote of the institutional ethics committee (Ethics Committee of the Canton of Zurich [KEK-ZH], number 2023–01867) was obtained. The study was conducted in adherence to the Declaration of Helsinki and all applicable Swiss laws. All patients included in this study provided general consent for the use of non-personal data for scientific purposes.
Inclusion and Exclusion Criteria
This study included only patients who underwent phacoemulsification cataract surgery with planned in-the-bag implantation of an injectable, foldable IOL, performed by two high-volume cataract surgeons with consultant status (M.B., F.H.) at Stadtspital Zürich, Switzerland between January 2019 and December 2022. Only cases with complete datasets were considered for the analysis. Different anesthesia types were considered, including topical, sub-Tenon’s, peribulbar anesthesia, and general anesthesia based on surgeon preference.
Cases were excluded if they involved refractive lens exchange, IOL exchange, secondary IOL explantation, and combined surgeries, such as phacovitrectomy, phacoemulsification with glaucoma surgery, or explantation of a phakic intraocular lens alongside cataract surgery. Teaching surgeries were excluded in the study. To reduce biases from less experienced surgeons, surgeries performed by any surgeon other than the two designated surgeons were also excluded.
Intraocular Lens Types
The majority IOL types were the Zeiss Asphina 509MP (Carl Zeiss Meditec AG, Jena, Germany), accounting for 86.64% of all IOLs. Other IOLs included the MA50BM (Alcon, Fort Worth, TX, USA; 2.97%), PhysIOL Micropure (1.35%), PhysIOL ANKORIS toric (0.94%) (PhysIOL S.A., Liège, Belgium), Zeiss Asphina 509M (0.67%), CLAREON CNA0T0 (Alcon; 0.40%), Ophtec Artiflex (Ophtec BV, Groningen, Netherlands; 0.80%), and other models including Kowa 3PC, Kowa One-piece (Kowa Company, Ltd., Nagoya, Japan), MA60MA (Alcon), Isopure (PhysIOL), SA60WF (Alcon), and AT Torbi 709MP/M (Zeiss), each comprising ≤0.27% of the total.
Endpoints
The primary endpoint was the incidence of intraoperative complications before and after implementing the TCS. Post-implementation, intraoperative complications were further analyzed according to the designated risk groups based on the TCS.
Data Collection and Database
In this study, data from cataract surgeries were initially collected manually from electronic health records and surgical reports for cases between January 2019 and December 2020. In December 2019, an electronic database for ophthalmic operations was introduced, utilizing the Intellect database (Dendrite Clinical Systems, Reading, United Kingdom) to provide a fully auditable platform for clinical data management. From January 2021 to December 2022, data were directly exported from the Dendrite database, allowing for more streamlined and accurate data handling. During this period, a comprehensive database was built, including all patients who provided written consent and underwent ophthalmic surgery at our hospital. This database captured demographic details, preoperative and perioperative parameters, follow-up clinical notes, and health questionnaire responses completed by the patients. All data entries were carefully managed by a data manager from our study center and quality assurance team, ensuring accuracy and consistency.
Intraoperative complications were classified into specific categories, including iris trauma, zonular lysis, posterior capsular rupture, vitreous loss, nuclear loss, anterior capsular tear, hemorrhage and other specified issues, which were extracted from the surgery report by the data manager.
Postoperative complications were documented with similar detail, including raised intraocular pressure (IOP), ptosis, external eye infection, intraocular hypotony, wound dehiscence, endophthalmitis, corneal edema, and other complications to be specified. However, as postoperative follow-ups for some patients were conducted by their private ophthalmologists, not all postoperative complications may have been fully captured in this documentation.
Triemli Cataract Score
To develop the Triemli Cataract Score (TCS), we conducted an extensive literature review on existing risk stratification systems and common intra-/postoperative complications in phacoemulsification cataract surgery. This review, combined with clinical experience, led to modifications of the Muhtaseb et al score and the New Zealand Cataract Risk Stratification (NZCRS) scoring system.15,16 In the TCS (Table 1), each ocular or systemic comorbidity and patient factor is assigned 2 to 5 points, with higher scores indicating an increased risk for intra- or postoperative complications. In contrast to the two aforementioned risk stratification system (RSS), the TCS accounts for specific risk factors such as hypotony and advanced glaucoma, each assigned 2 points. Advanced glaucoma was included due to its known association with zonular weakness, while hypotony (<6 mmHg) increases the risk of intraoperative instability. Additionally, cases with a history of capsular rupture in the fellow eye or those involving a single functioning eye receive 5 points. However, posterior capsule plaque is not included in this score. For surgeries performed under local anesthesia, factors such as patient positioning difficulties, tremors, claustrophobia, and language or hearing impairments were considered, as these could impact the procedure. These considerations do not apply for surgeries using peribulbar or general anesthesia.
 |
Table 1 Triemli Cataract Risk Stratification Score |
The patient’s clinical records were reviewed prior to surgery, and a “cataract score”, representing an aggregated preoperative risk score, was calculated individually by either the surgeon or resident. The risk classification was organized into three categories: 0–3 points indicated a routine procedure, 3–5 points signified a complex procedure, and >5 points indicated a highly complex procedure. The purpose of the TCS modification was to be as specific as possible with regards to allocating cases into the “routine” and “highly complex” groups, as these patients were felt to be most at risk in case of an incorrect risk group allocation. Surgeons were instructed to enter the operative report directly into the electronic medical record, with intraoperative complications documented in a dedicated field.
Statistical Analysis
The surgeries were divided into two groups: pre-TCS surgery and post-TCS surgery. Supplementary Figure 1 presents the distributions of continuous predictors, namely age (A) and cataract score (B). Differences between these groups were evaluated using the Wilcoxon signed rank test for numerical values, and the chi-squared test or Fisher’s exact test for categorical variables. Both univariable and multivariable logistic regression models were created to assess the association between TCS implementation and intra- and postoperative complications. The multivariable models were adjusted for age, sex, eye side, lead surgeon, and type of anesthesia, with coefficients converted to odds ratios (OR) to facilitate interpretation. A p-value below 0.05 was considered statistically significant.
Only patients with a TCS were included in the analysis to compare outcome across routine, complex, and highly complex surgery groups. Differences between these complexity groups were evaluated using the statistical methods described above. All statistical analyses were performed using R version 4.3.1 (R Core Team, Vienna, Austria), employing the “stats”, “gtsummary” and “ggplot2” packages.17 We illustrated the theoretically achievable power of the study across a range of odds ratios to show which effect sizes could be reliably detected given the sample size and event rate (Supplementary Figure 2).
Results
A total of 1776 eyes were included in the analysis, with 741 eyes assessed pre- and 1035 eyes post-TCS. The median age of the cohort was 74.57 years (interquartile range [IQR]: 66.55, 80.90 years). Among the patients, 937 male (52.8%) and 839 female (47.2%) underwent surgery. Of the total eyes operated, 881 were right eyes (49.6%) and 895 were left eyes (50.4%). The surgeries were distributed unevenly between the two surgeons, with one surgeon performing a larger share of the surgeries (1283 surgeries, 72.2%) compared to the other (493, 27.8%). Overall, intraoperative complications occurred in 146 cases (8.2%) and postoperative complications were noted in 476 cases (28.6%). Table 2 provides an overview of the baseline demographics, along with a comparison of demographics pre- and post-TCS.
 |
Table 2 Demographics and Clinical Characteristics Before and After Implementation of the Triemli Cataract Score |
The overall intraoperative complication rate for all 1776 analyzed surgeries was 8.2%, with a rate of 9.5% observed pre-TCS and 7.4% after. However, the difference between the two groups was not statistically significant (p=0.123). Table 3 presents a summary of the various intraoperative complication types across both groups. In the multivariate logistic regression analysis, the TCS implementation resulted in an odds ratio (OR) of 0.71 for intraoperative complications (95% confidence interval [CI]: 0.50, 1.01, p=0.054). Additionally, no significant correlation was found between age and intraoperative complications (OR = 1.00, 95% CI: 0.87, 1.72, p>0.90), nor between male sex and intraoperative complications (OR = 1.22, 95% CI: 0.87, 1.72, p=0.30). The intraoperative complication rate was not statistically significantly associated with the type of anesthesia used (local vs general), with an OR of 0.77 (0.39, 1.49, p=0.40).
 |
Table 3 Intraoperative Complications Before and After Implementation of the Triemli Cataract Score |
The distribution of operated eyes across the risk groups included 625 eyes in the “routine” group (63.2%), 250 in the “complex” group (25.3%), and 113 in the “highly complex” group (11.4%). The intraoperative complication rate differed significantly among these groups (p=0.014), with the lowest incidence in the routine group (5.6%), followed by the highly complex group (8.8%), and the highest in the complex group (11.2%) (Table 4).
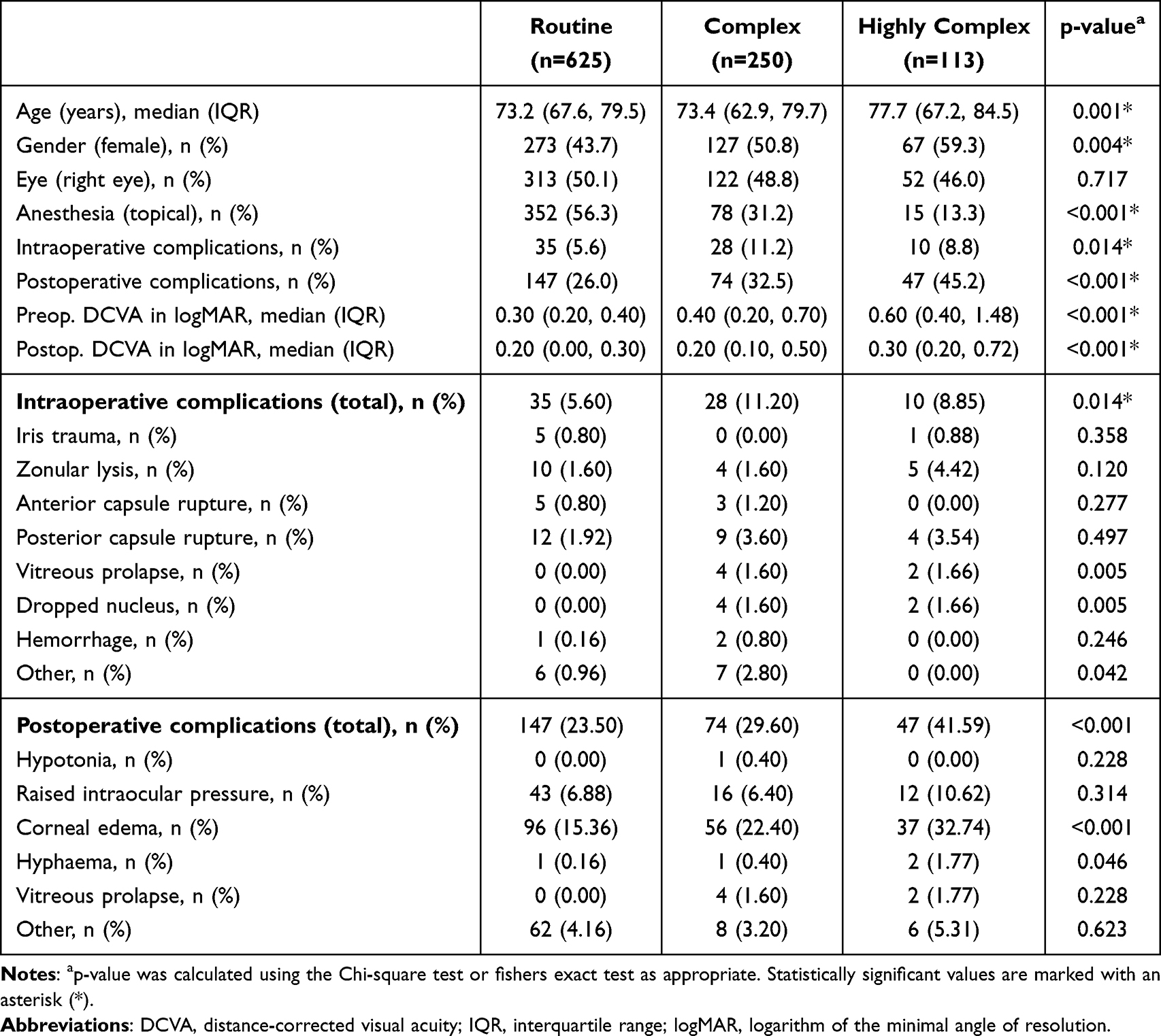 |
Table 4 Demographics, Clinical Characteristics, Intraoperative and Postoperative Complications Across the Risk Groups |
Group-specific intraoperative complication rates are detailed in Table 4. With regard to postoperative complications, there was a notable increase in complication rates across the risk groups (p<0.001), as shown in Table 4.
Similarly, the duration of surgeries correspondingly increased with the complexity of the risk groups, as illustrated in Figure 1.
 |
Figure 1 Violin plots of operating times for single phacoemulsification procedures classified according to preoperative risk group (routine, complex and highly complex) showed that the latter two groups were statistically significantly longer than routine procedures, with no statistically significant difference between the complex and highly complex groups. |
Discussion
Risk stratification systems (RSS) in medicine enable individualized clinical care, preventive strategies, and efficient resource allocation.18 The implementation is anticipated to enhance the quality of care while potentially reducing healthcare costs.18
In cataract surgery, several preoperative RSS have been developed to identify high-risk patients and reduce the likelihood of intraoperative complications.15,16,19–21 Muhtaseb et al’s RSS has gained international recognition and has been validated in multiple studies.15,22,23 Subsequent modifications have aimed further reducing complication rates. For example, the NZCRS system was specifically adapted for public training hospitals.16 Muhtaseb’s RSS assigns points to key risk factors to categorize patients by cumulative score, while the NZCRS system incorporates three additional factors, enabling a refined classification between “low risk” and “high-risk” patients.15,16
The TCS further refined this system by incorporating additional factors specific to complex cases. For instance, advanced glaucoma is included as a risk factor, recognizing the elevated risk for zonulopathy.24,25 In the TCS, “high ametropia” is replaced by criteria such as an axial length greater than 28 mm, a shallow anterior chamber (< 2.5 mm), or an axial length under 20 mm as significant risk factors.26,27 Furthermore, the TCS assigns five points if a capsular rupture has previously occurred in the fellow eye, acknowledging the markedly increased risk in such cases.28 Ocular hypotension (< 6 mmHg) is also considered a risk factor in the TCS.29
For cases performed under local anesthesia, the TCS includes specific patient factors—such as positioning difficulties, tremors, claustrophobia, deafness, or language barriers—that may complicate the procedure. These factors are not applicable to surgeries conducted under general anesthesia. Routine procedures are recommended for less experienced surgeons, while complex and highly complex cases should be allocated to more experienced surgeons. In addition to streamlining the assignment of appropriate surgeons, the three distinct risk groups can serve as valuable checkpoints in training. This approach could facilitate safer training environments and help emerging surgeons gain experience with appropriate cases. Further research on the impact of TCS on surgical training outcomes and skill development would be valuable.
The TCS also holds value in reporting outcomes and benchmarking, as it enables standardized differentiation between routine and complex cases, making it easier to compare results across clinics and studies.
PCR is a widely recognized metric for RSS performance. While PCR did not differ significantly between groups, its observed trend supports proper case allocation by the TCS. The lack of statistical significance may reflect low event rates or effective surgeon allocation strategies.
By differentiating cases based on complexity, the TCS may provide a framework for more precise resource allocation. Highly complex cases, associated with higher complication rates and potentially longer operative times, could justify adjustments in procedural costs and reimbursement rates. A future cost-benefit analysis could evaluate whether this risk-adjusted approach leads to more efficient use of resources and potentially reduces overall healthcare costs by preemptively addressing high-risk factors. With clear categorization into risk groups, the TCS enables more informed preoperative counseling. Surgeons can better communicate potential risks to patients based on their specific profiles, helping to manage patient expectations and improve satisfaction. Additionally, discussing risk stratification may enhance patient confidence in the surgical plan, particularly in high-risk cases. Future studies could explore patient satisfaction metrics in relation to preoperative risk discussions using TCS.
In this retrospective study, 1776 cataract surgeries were analyzed, comprising 704 cases before and 1072 after the implementation of TCS. The intraoperative complication rate was 9.5% before TCS and 7.4% after its introduction. This difference resulted in a p-value of 0.054. Although not statistically significant by conventional thresholds, the calculated odds ratio of 0.71 (95% CI: 0.50–1.01; p=0.054) may indicate a potential trend toward reduced risk. Nevertheless, given the high number of cataract surgeries performed globally, a 2.1% reduction is considered to be clinically relevant. Specific reductions were observed in the occurrence of zonular lysis (by just over 1%) and posterior capsule rupture (by 0.5%), though these decreases were not statistically significant (p>0.05, for each). It is notable that the pre-TCS group exhibited a statistically significant higher median age than the post-TCS group (76.7 vs 73.2 years, p<0.001), which may have influenced outcomes. A study by Han et al supports the value of RSS: the intraoperative complication rate was 8.1% without an RSS, which dropped to 6.11% with the Muhtaseb RSS and further to 5.2% with the modified NZCRS.15,16,30 Unfortunately, our data set lacks pre-implementation risk group categorization, limiting a direct comparison of surgical complexity before and after TCS introduction. We hypothesize that the observed reduction in intraoperative complications may partly be attributed to the Hawthorne effect, where individuals—in this case, surgeons—modify their behavior when they know they are being observed. However, the retrospective design of this study likely minimized the influence of the Hawthorne effect. Our findings are partially in line with Moussa et al, who demonstrated improved outcomes with resident case allocation using preoperative RSS.22 Unlike their focus on resident surgeries, our system was applied in a real-world public hospital setting with experienced surgeons.
The statistically significantly lower postoperative DCVA (p<0.001) observed post-TCS likely reflects changes in follow-up care, as recent follow-ups were primarily handled by the referring ophthalmologists. Residual keratopathy identified during these intervals may have contributed to the DCVA reduction. While TCS implementation did not have statistically significant impact postoperative complication rates, it is important to note that inconsistent follow-up across patients limits our ability to make direct comparisons.
Post-TCS, the intraoperative complication rates exhibited a notable disparity across the three groups (p = 0.014), The lowest complication rate was in the routine group (5.6%), followed by the highly complex group (8.8%), and the highest rate was observed in the complex group (11.2%). The difference in intraoperative complication rates among the risk groups underlines the importance of risk stratification. This finding reinforces the value of the TCS in identifying higher-risk patients who may benefit from additional preoperative planning and experienced surgical teams. Additionally, the unexpected higher rate in the complex group compared to the highly complex group may suggest nuances in case complexity that the TCS could refine further. Further validation is required to optimize the discriminatory power of the individual criteria and groups. This is necessary to verify the correct application of the score in clinical practice. The TCS presented was further adapted to simplify it. This could eliminate weak points of the score, such as the fact that some criteria overlap (eg long/short axis length and high ametropia). Nevertheless, the outcome of the recently updated TCS is not yet forthcoming.
A key strength of this study is the large sample size of cataract surgeries analyzed, which enhances the reliability of the findings. Additionally, only surgeries performed by two experienced surgeons were included, eliminating potential variability from less experienced surgeons or teaching cases. As a result, the intraoperative complications can be attributed with greater accuracy to the identified risk groups. Moreover, this study reflects real-world outcomes in a public teaching hospital setting.
However, the study has certain limitations, notably the inability to directly compare the pre- and post-TCS patient cohorts due to missing data on risk factor profiles pre-TCS. A further limitation is the absence of postoperative auditing of the score by an experienced surgeon. As surgeries were performed by only two experienced surgeons, this may limit generalizability. While we aimed to reduce bias by including only experienced surgeons, stratification by surgeon experience would provide additional insights, particularly regarding score impact on less experienced surgeons. Additionally, the cases were not distributed equitably between the two surgeons, and the postoperative data were not recorded in a systematic and uniform manner. To address these limitations and verify the practicality of the TCS, we recommend conducting prospective studies that will enable further adaptation and validation of this risk stratification system.
To conclude, the TCS implementation has demonstrated potential in enhancing preoperative risk stratification and reducing intraoperative complication rates in cataract surgery within a public hospital setting. By categorizing patients into distinct risk groups, the TCS allows for tailored surgical planning and patient counseling, optimized surgeon allocation, and a structured approach to training. Although this retrospective study provides valuable insights, further prospective research is needed to fully validate the TCS and assess its long-term impact on surgical outcomes. Overall, the TCS represents a promising tool to improve patient safety and resource allocation in cataract surgery.
Abbreviations
DCVA, distance-corrected visual acuity; IOL, intraocular lens; RSS, risk stratification system; TCS, Triemli cataract score.
Data Sharing Statement
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Statement of Ethics
For this study a positive vote of the institutional ethics committee (IRB number 2023-01867) was obtained. The study was conducted in adherence to the Declaration of Helsinki and all federal state laws of Switzerland. All patients included in this study provided general consent for the use of non-personal data for scientific purposes.
Acknowledgments
This work was presented at the 2024 Congress of the German Society of Ophthalmology (DOG), the 2024 Annual Meeting of the European Society of Cataract and Refractive Surgeons (ESCRS), and as a poster presentation at the 2025 Annual Meeting of the Association for Research in Vision and Ophthalmology (ARVO). The abstract of the poster presentation was published in the 2025 Abstract Issue of Investigative Ophthalmology & Visual Science and is available at: [https://iovs.arvojournals.org/article.aspx?articleid=2807808]. We thank the Werner H. Spross Foundation for its unrestricted support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research work is sponsored by the Werner H. Spross Foundation for the advancement of research and teaching in ophthalmology.
Disclosure
Dr Klemens Kaiser reports lecture fees from Oculus Optikgeräte GmbH, outside the submitted work. Dr Sophie-Christin Ernst reports salary as a part time research fellow from Werner H. Spross Stiftung zur Förderung der Augenheilkunde; consultant and member of sounding board for Roche AG Switzerland; training supports from Bayer Schweiz AG, outside the submitted work. Dr Gabor Mark Somfai reports personal fees from Abbvie, Bayer, Novartis, Roche, and Carl Zeiss Meditec, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Liu Y-C, Wilkins M, Kim T, Malyugin B, Mehta JS. Cataracts. Lancet. 2017;390(10094):600–612. doi:10.1016/S0140-6736(17)30544-5
2. Chen X, Xu J, Chen X, Yao K. Cataract: advances in surgery and whether surgery remains the only treatment in future. Adv Ophthalmol Pract Res. 2021;1(1):100008. doi:10.1016/j.aopr.2021.100008
3. Chia WL, Goldberg I. Comparison of extracapsular and phaco-emulsification cataract extraction techniques when combined with intra-ocular lens placement and trabeculectomy: short-term results. Aust N Z J Ophthalmol. 1998;26(1):19–27. doi:10.1046/j.1440-1606.1998.00074.x
4. Gogate PM, Kulkarni SR, Krishnaiah S, et al. Safety and efficacy of phacoemulsification compared with manual small-incision cataract surgery by a randomized controlled clinical trial: six-week results. Ophthalmology. 2005;112(5):869–874. doi:10.1016/j.ophtha.2004.11.055
5. Wu S, Yao D, Hua S, Li X, Shi Y. Comparison of effect and safety of phacoemulsification surgery performed by resident and attending physicians. Front Med Lausanne. 2024;11:1401482. doi:10.3389/fmed.2024.1401482
6. Carifi G, Miller MH, Pitsas C, et al. Complications and outcomes of phacoemulsification cataract surgery complicated by anterior capsule tear. Am J Ophthalmol. 2015;159(3):463–469. doi:10.1016/j.ajo.2014.11.027
7. Rutar T, Porco TC, Naseri A. Risk factors for intraoperative complications in resident-performed phacoemulsification surgery. Ophthalmology. 2009;116(3):431–436. doi:10.1016/j.ophtha.2008.10.028
8. Grzybowski A, Krzyżanowska-Berkowska P. Intraoperative floppy iris syndrome (IFIS): what complication rates can we expect? Graefes Arch Clin Exp Ophthalmol. 2014;252(5):845–846. doi:10.1007/s00417-013-2536-8
9. Af Segerstad P H. Risk model for intraoperative complication during cataract surgery based on data from 900 000 eyes: previous intravitreal injection is a risk factor. Br J Ophthalmol. 2022;106(10):1373–1379. doi:10.1136/bjophthalmol-2020-318645
10. Zetterberg M, Kugelberg M, Nilsson I, Lundström M, Behndig A, Montan P. A composite risk score for capsule complications based on data FRom the Swedish National Cataract Register: relation to surgery volumes. Ophthalmology. 2021;128(3):364–371. doi:10.1016/j.ophtha.2020.07.033
11. Astbury N, Nyamai LA. Detecting and managing complications in cataract patients. Community Eye Health. 2016;29(94):27–29.
12. Vedantham V. Endophthalmitis following phacoemulsification. Eye. 2005;19(1):113–114. doi:10.1038/sj.eye.6701402
13. Cao X, Liu A, Zhang J, et al. Clinical analysis of endophthalmitis after phacoemulsification. Can J Ophthalmol. 2007;42(6):844–848. doi:10.3129/i07-173
14. Pooprasert P, Hansell J, Young-Zvandasara T, Muhtaseb M. Can applying a risk stratification system, preoperatively, reduce intraoperative complications during phacoemulsification? Curr Eye Res. 2021;46(3):318–323. doi:10.1080/02713683.2020.1801759
15. Muhtaseb M. A system for preoperative stratification of cataract patients according to risk of intraoperative complications: a prospective analysis of 1441 cases. Br J Ophthalmol. 2004;88(10):1242–1246. doi:10.1136/bjo.2004.046003
16. Kim BZ, Patel DV, Sherwin T, McGhee CNJ. The Auckland Cataract Study: assessing preoperative risk stratification systems for phacoemulsification surgery in a teaching hospital. Am J Ophthalmol. 2016;171:145–150.
17. Sjoberg DD, Whiting K, Curry M, Lavery JA, Larmarange J. Reproducible summary tables with the gtsummary package. R J. 2021;13(1):570. doi:10.32614/RJ-2021-053
18. Powers BW, Chaguturu SK, Ferris TG. Optimizing high-risk care management. JAMA. 2015;313(8):795–796. doi:10.1001/jama.2014.18171
19. Tsinopoulos IT, Lamprogiannis LP, Tsaousis KT, et al. Surgical outcomes in phacoemulsification after application of a risk stratification system. Clin Ophthalmol. 2013;7:895–899. doi:10.2147/OPTH.S42726
20. Shekhar M, Choudhury P, Ramya G, Sankarananthan R, Balagiri S, Wijesinghe HK. Cataract surgery risk stratification in phacoemulsification and manual small incision cataract surgery in a teaching hospital. Int Ophthalmol. 2022;42(1):201–209. doi:10.1007/s10792-021-02014-6
21. Reeves SW, Tielsch JM, Katz J, Bass EB, Schein OD. A self-administered health questionnaire for the preoperative risk stratification of patients undergoing cataract surgery. Am J Ophthalmol. 2003;135(5):599–606. doi:10.1016/S0002-9394(02)02236-5
22. Moussa O, Frank T, Valenzuela IA, et al. Efficacy of preoperative risk stratification on resident phacoemulsification surgeries. Clin Ophthalmol. 2022;16:2137–2144. doi:10.2147/OPTH.S368633
23. Osborne SA, Adams WE, Bunce CV, Fraser SG. Validation of two scoring systems for the prediction of posterior capsule rupture during phacoemulsification surgery. Br J Ophthalmol. 2006;90(3):333–336. doi:10.1136/bjo.2005.080754
24. Dureau P. Pathophysiology of zonular diseases. Curr Opin Ophthalmol. 2008;19(1):27–30. doi:10.1097/ICU.0b013e3282f29f01
25. Salimi A, Fanous A, watt H, Abu-Nada M, Wang A, Harasymowycz P. Prevalence of zonulopathy in primary angle closure disease. Clin Exp Ophthalmol. 2021;49(9):1018–1026. doi:10.1111/ceo.13983
26. Yosar JC, Zagora SL, Grigg JR. Cataract surgery in short eyes, including nanophthalmos: visual outcomes, complications and refractive results. Clin Ophthalmol. 2021;15:4543–4551. doi:10.2147/OPTH.S344465
27. Fesharaki H, Peyman A, Rowshandel M, et al. A comparative study of complications of cataract surgery with phacoemulsification in eyes with high and normal axial length. Adv Biomed Res. 2012;1:67. doi:10.4103/2277-9175.102971
28. Elhusseiny AM, Toma J, Ibrahim SN, et al. Risk of posterior capsule ruptures in fellow-eye cataract surgeries: a multicenter comparative study. Semin Ophthalmol. 2024;1–6.
29. Rebolleda G, Muñoz-Negrete FJ. Phacoemulsification in eyes with functioning filtering blebs: a prospective study. Ophthalmology. 2002;109(12):2248–2255. doi:10.1016/S0161-6420(02)01246-0
30. Han JV, Patel DV, Wallace HB, Kim BZ, Sherwin T, McGhee CNJ. Auckland Cataract Study III: refining preoperative assessment with cataract risk stratification to reduce intraoperative complications. Am J Ophthalmol. 2019;197:114–120. doi:10.1016/j.ajo.2018.09.026
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.