Back to Journals » Medical Devices: Evidence and Research » Volume 18
Implementation of a Cost and Variation Reduction Program for Hemostasis Products at a Large Academic Medical Center: A Multi-Stakeholder Perspective
Authors Shah T, Brethauer S, Danker III WA ![]() , Doshi I, O'Hara M
, Doshi I, O'Hara M ![]() , Silber A, Vasileff WK
, Silber A, Vasileff WK
Received 23 July 2024
Accepted for publication 16 December 2024
Published 24 January 2025 Volume 2025:18 Pages 63—73
DOI https://doi.org/10.2147/MDER.S488279
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Tejen Shah,1 Stacy Brethauer,1 Walter A Danker III,2 Ishita Doshi,2 Matthew O’Hara,3 Abigail Silber,3 William K Vasileff4
1Department of Surgery, The Ohio State University Wexner Medical Center, Columbus, OH, USA; 2Ethicon, Inc., Raritan, NJ, USA; 3Trinity Life Sciences, Waltham, MA, USA; 4Department of Orthopaedics, Sports Medicine Research Institute, The Ohio State University Wexner Medical Center, Columbus, OH, USA
Correspondence: Stacy Brethauer, Email [email protected]
Goal: Cost-saving initiatives targeting surgical supplies management have become increasingly common to address rising healthcare costs. However, few studies provide details on hospital stakeholder experiences or learnings from implementing such initiatives. Thus, we sought to evaluate hospital stakeholder satisfaction with conversion to a sole supplier for hemostasis products, in addition to economic and clinical impacts, to help develop best practices for implementation.
Methods: This cross-sectional study assessed satisfaction with converting to a sole supplier for hemostasis products at a large US academic medical center using qualitative interviews and quantitative surveys with clinical and non-clinical stakeholders, on the decision-making process, conversion, and vendor-supported hemostasis optimization program (HOP) post-implementation (February 2022–May 2022). Perioperative hemorrhage events, adjunctive hemostat utilization, and total annual hospital expenditure on hemostatic products were also evaluated pre- and post-conversion (2020– 2022) to identify impacts on clinical and economic outcomes.
Findings: Ten hospital stakeholders completed qualitative interviews (n = 7 surgeons, n = 2 surgical technicians, n = 1 administrator) and 22 completed quantitative surveys (n = 6 surgeons, n = 5 surgical technicians, n = 11 nurses). Survey respondents noted overall satisfaction with conversion, including the level of input they provided in the decision-making process (75% were somewhat to extremely satisfied), availability of hemostatic agents during the conversion process (87%), and the vendor-supported HOP (100%). The outcomes analyses revealed a nearly 25% decrease in supply expenditure without changes to the number of postoperative hemorrhage events following implementation.
Practical Applications: Converting to a sole vendor for hemostasis products was achieved with high satisfaction among hospital stakeholders and cost savings to the institution without impacting the quality of patient care. This study provides a roadmap of best practices for other institutions interested in implementing similar initiatives and presents an example of a successful transition to a sole vendor for hemostasis products driven by effective supplier, institution, and hospital stakeholder coordination.
Keywords: hemostatic agent, cost savings, variation reduction, surgical care, hospital inventory
Background
Over the past several decades, rising healthcare costs have led to an increasing number of initiatives focused on cost and variation reduction in surgical care.1 Surgical care is estimated to account for nearly one-third of healthcare expenditures in the United States (US).2 Moreover, the burden of cost containment has shifted in recent years from insurers to hospitals (eg, healthcare providers [HCPs], supply chains, and administrators) as payment structures have transitioned from traditional fee-for-service to bundled payment models, in which hospitals are reimbursed a predetermined value for each surgical episode.3
Cost-saving initiatives in surgical care frequently target management of supplies and medical devices for the operating room (OR). Strategies such as pricing capitation or contract negotiations with suppliers can help to consolidate purchasing and reduce variation in addition to decreasing overall costs.4,5 For example, studies have shown that transitioning to single/preferred vendor procurement for certain surgical supplies and devices can lead to considerable cost savings with either no change or improvements in outcomes (eg, the need for revision surgery, readmission, complications, patient-reported outcomes, length of stay, and operative time).6–8 Such initiatives often target high-cost, high-value products, such as surgical implants. Comparatively, less evidence is available concerning the potential benefits of similar vendor consolidation initiatives for procuring low-cost, high-use surgical supplies, such as products used for hemostasis. However, given the extensive resources required for surgical care, even small cost savings may help to improve overall profitability, particularly when supplies are frequently utilized.
Hemostatic agents are an attractive potential target for variation reduction efforts in surgical care. They play a role in controlling disruptive bleeding in an estimated 30% of all surgical procedures.9 Uncontrolled or disruptive bleeding can lead to increased costs, length of stay, readmission, and procedure complexity, including a higher risk of mortality.10–12 Primary methods to achieve hemostasis typically include suturing, electrocautery, or vascular clips, but if residual bleeding persists, adjunctive hemostats can be used to achieve control across a variety of bleeding sites and situations.13–15 Compared to conventional methods of hemostasis alone, adjunctive hemostats and sealants have been shown to reduce hospital resource utilization, including blood transfusions, length of stay, and time in the OR.16–19 Despite the importance of adjunctive hemostats, inconsistent terminology and clinical guidance on optimal utilization of available products13,14,20–22 may complicate use or create unnecessary variability in bleeding management. Moreover, hospitals may need to keep a large inventory of different adjunctive hemostatic agents to ensure a comprehensive approach to bleeding management, which may contribute to preventable cost and/or inefficiency of inventory management.
This study evaluated a large US academic medical center’s conversion to single-vendor procurement for hemostatic products, a process driven by the desire for consistency in product use and cost savings without impacting quality of care or patient safety. Perspectives on, and experiences with, the conversion were captured across multiple stakeholder types, including HCPs and administrators. We present our findings as a roadmap of learnings and best practices for multi- to single-vendor conversions for surgical supplies, including benefits, hurdles, and satisfaction with the initiative.
Methods
Study Overview
This was a cross-sectional study, including qualitative interviews, quantitative surveys, clinical case and hemostat utilization review to assess clinical and economic impact, satisfaction with and perspectives on converting to a single supplier for hemostasis products for surgical care (Ethicon, Inc.) at a large US academic medical center (The Ohio State University Wexner Medical Center). The full conversion took place over approximately 2 years from Q2 2020 to Q2 2022 and was comprised of three key phases:
- Decision-making process.
- Conversion process.
- Vendor-supported hemostasis optimization program (HOP).
The Ohio State University Wexner Medical Center utilizes a clinically integrated supply chain model that includes three physician leaders with protected time to serve in these roles (Medical Director and two Associate Medical Directors). Prior to implementation of this project with institution-wide impact, the medical director for supply chain was chosen as the clinical program lead to communicate with a broad group of specialists.
Decision-Making Process
As a first step, a decision-making committee was formed at the institution to evaluate current spend in the product category and to determine existing unmet needs associated with hemostasis product use in the surgical suite. The top hemostat users in the institution were identified by the clinical program lead, and other physicians within the institution’s surgical department were selected and invited to participate in the committee. A value scorecard was used to evaluate the merits of the sourcing project across specific components, such as improvements in patient outcomes, level of clinical evidence, cost savings, and inventory impact (Supplementary File 1). All variables were included in the initial discussion, with a finer point placed on specific items following receipt of vendor proposals. The committee reviewed proposals from multiple potential vendors before selecting a single-source hemostasis product supplier for the conversion process. It should be emphasized that, in keeping with a clinically integrated supply chain model, the physicians voted on the final decision for the single-source supplier contract.
Conversion Process
Prior to introducing the new product line, the clinical program lead and other project advisors (eg, commodity managers and supplier representatives) discussed all product replacements with nurse managers. A “trial period” was subsequently initiated where HCPs were provided access to the full suite of previous hemostasis products as well as the new supplier’s products to ensure familiarity and comfort prior to use in patients. During this trial period, supplier representatives were on-site to train HCPs on proper use of the new products.
Vendor-Supported Hemostasis Optimization Program (HOP)
The vendor-supported HOP was provided for 18 months post-conversion to foster collaboration between the institution and supplier representatives and included formal product in-services, hands-on tabletop training for surgeons and nurses, surgical resident’s skills lab, as well as product conversion posters and preference card updates. The same methods were used to train all staff on the vendor-supported HOP, which was developed to address some of the challenges with surgical bleeding, such as inconsistent terminology and variability in management, by providing support tools (eg, decision trees) on the recommended use of different adjunctive hemostats based on bleeding site and situation. To ensure ongoing success of the conversion, these training materials are now part of the surgical staff on-boarding process at the institution.
HCP and Hospital Administrator Interviews and Surveys
The quantitative surveys and qualitative interviews were conducted post-conversion from February 2022 to May 2022 and assessed hospital stakeholder perspectives on the different aspects of the initiative. Stakeholders were referred for participation in the qualitative interviews and quantitative surveys using clinical program lead based on their role at the hospital and their participation in the conversion process. To ensure the assessment was comprehensive and reflected diverse perspectives, both clinical and non-clinical stakeholders with roles at different points in the care pathway were gathered, including surgeons, nurses, surgical technicians, and hospital administrators.
Qualitative Interviews
A series of qualitative interviews were used to capture perspectives on the decision-making process, the conversion process, and the vendor-supported HOP at the institution. Interviews were conducted with respondents who had been directly involved in the conversion and who volunteered to participate in the study. Qualitative interview data were systematically categorized into themes using an inductive approach to characterize similarities and dissimilarities in experiences across respondents.
Quantitative Surveys
The assessment also included 2 quantitative surveys: Survey 1 focused on the decision-making and conversion processes, and Survey 2 focused on the vendor-supported HOP. Questions were designed to evaluate respondents’ satisfaction with specific aspects of the initiative on a 7-point Likert scale, with 1 indicating “not at all satisfied” and 7 indicating “extremely satisfied”. The results were analyzed to report both an average score for each question and the proportion of responses across three scoring categories: low (1–2 points), medium (3–5 points), and high (6–7 points). Completion of the surveys was done on a voluntary basis. The surveys were sent to all surgical and administrative stakeholders at the institution.
Clinical Case Series Review and Cost Analyses
A clinical case series review was conducted by an OSU clinician team on perioperative hemorrhage events (Agency for Healthcare Research and Quality Patient Safety Indicator 9 [PSI-09]) occurring from 2020 to 2022, inclusive of cases both pre- and post-conversion, to understand the clinical context of these events and qualitatively assess any notable events or trends during program implementation. In addition, adjunctive hemostat utilization by vendor was assessed from 2020 to 2022 to quantify the impact on inventory management within the hospital and OR. Total annual hospital expenditure on hemostatic products over the study period was also evaluated.
Results
Qualitative and Quantitative Respondent Characteristics
Ten hospital stakeholders completed the qualitative interviews (Table 1). Interviews focused on decision-making (n = 5) were conducted with 4 surgeons and 1 administrator, and interviews focused on the conversion process (n = 2) were conducted with 2 surgery technologists. Three surgeons were interviewed regarding the vendor-supported HOP. Of note, 3 respondents that were interviewed regarding the decision-making process (2 surgeons and 1 administrator) also discussed the conversion process, unprompted. These responses were also included in the findings.
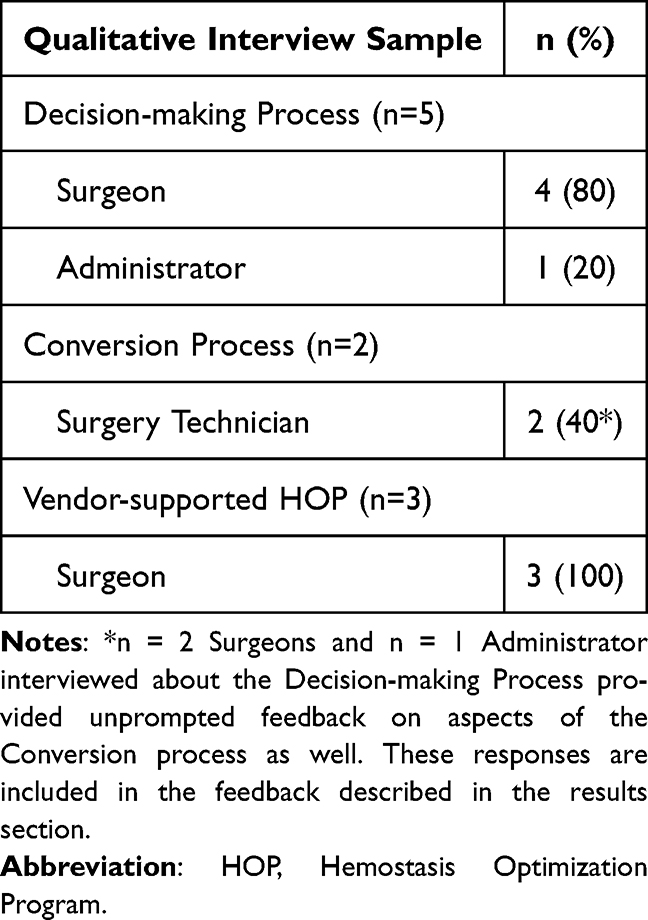 |
Table 1 Qualitative Interview Sample Overview |
Two different quantitative surveys were used to collect stakeholder satisfaction with aspects of the decision-making and conversion processes, as well as the vendor-supported HOP. The clinical roles of the respondents in Survey 1 (n = 12) and Survey 2 (n = 10) are shown in Table 2. Since respondents were not required to answer all questions in the survey, sample sizes vary across specific questions. Half of the respondents to the quantitative surveys were nurses, while the other 50% were a mix of surgeons and surgical technicians. The average length of time in practice across the respondents was approximately 17 years.
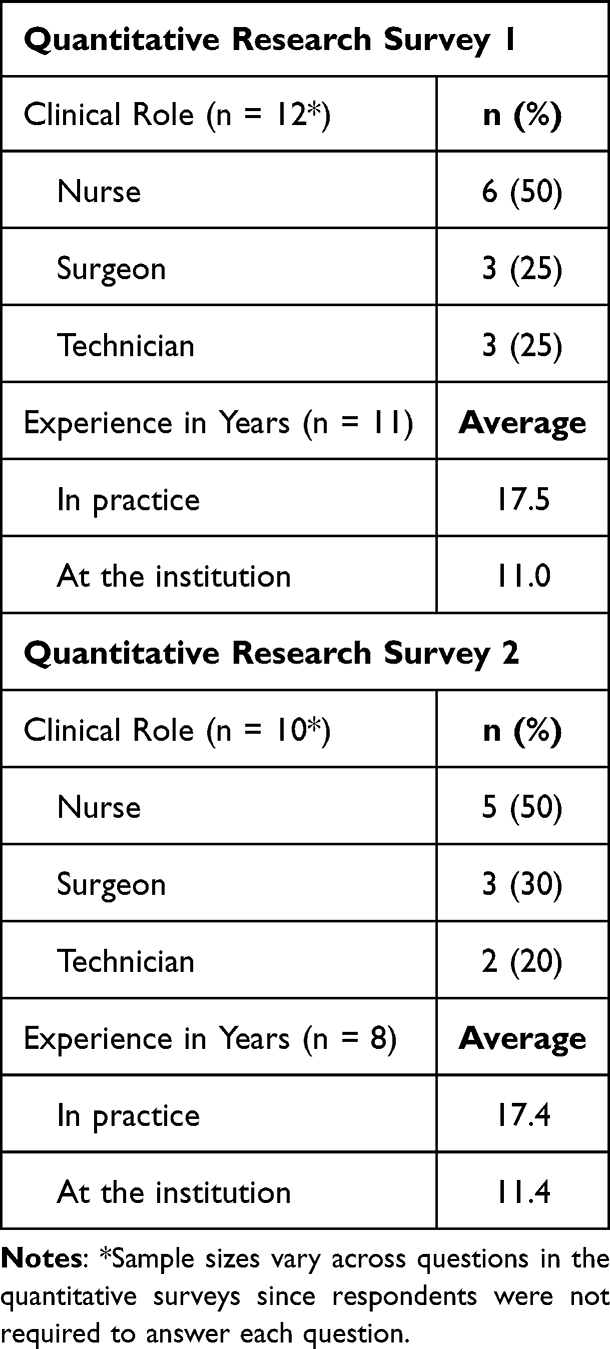 |
Table 2 Quantitative Survey Respondent Clinical Roles and Experience |
Decision-Making Process
Qualitative Insights
Most respondents (n = 4/5), particularly surgeons, found the decision-making process to be transparent, but the hospital administrator indicated a preference for earlier involvement. Most respondents (n = 4) cited cost as the primary driver for conversion; clinical outcomes were not expected to have significant change given that hemostatic agents are primarily used as adjuncts to stop minor bleeding. All respondents stressed the importance of transparency in the conversion process, as well as an overlap period where both previously used and newly introduced products are available to facilitate comfort with the transition. Areas identified for improvement included wider outreach, particularly to non-surgeon stakeholders. Respondents also noted a desire for greater data validation of products prior to conversion, including more information about the potential impact on clinical endpoints, cost-savings, and waste reduction.
Quantitative Results
Quantitative findings on the decision-making process show that 75% of respondents (n=6/8) were either at least somewhat satisfied (≥3 on 7-point scale) or extremely satisfied (≥6 on 7-point scale), with both the level of input that their department was able to provide in the decision-making process and the availability of hemostatic agents during the trial/evaluation period (Figure 1). Moreover, nearly two-thirds of respondents (62%) indicated they were at least somewhat satisfied with the level of planning in their department for the conversion. Most respondents (n = 7) were aware that hemostatic agents were being reviewed.
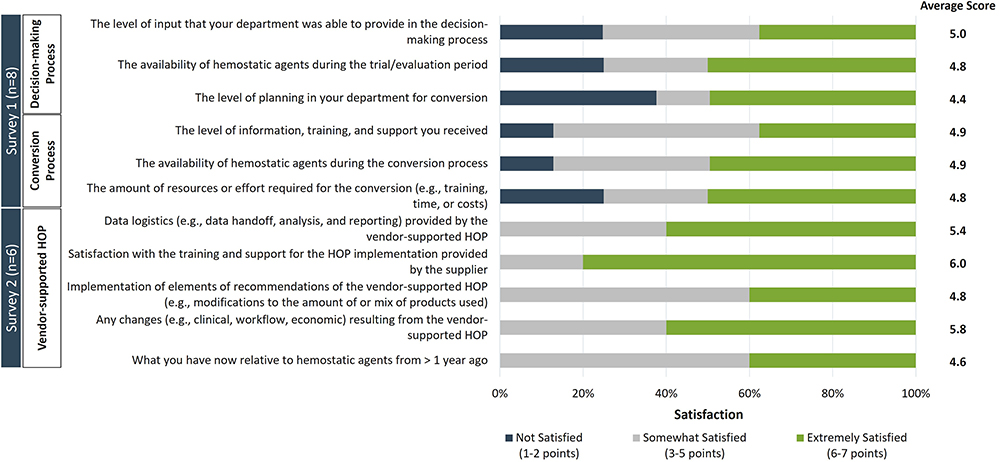 |
Figure 1 Satisfaction with the Decision-making Process, Conversion Process, and Vendor-supported HOP. Hospital stakeholders were asked to rate their satisfaction across two different surveys describing 1) the decision-making and conversion processes (n = 8 respondents), and 2) the vendor-supported HOP (n=6 respondents). Respondents provided their rating on a 7-point Likert scale, with a 1 indicating “not at all satisfied” and a 7 indicating “extremely satisfied”. For each question, responses were grouped into one of three scoring categories: Not Satisfied (1–2 points, dark blue bars), Somewhat Satisfied (3–5 points, gray bars), and Extremely Satisfied (6–7 points, green bars). Average scores for each question are shown in the right column. |
Conversion Process
Qualitative Insights
Qualitative interview respondents that evaluated the conversion process (n = 2 surgical technicians) reported it to be smooth and satisfactory. One of the surgical technicians noted that there was a significant learning curve for HCPs, particularly among junior surgeons that did not have prior experience using the new supplier’s products. They suggested earlier notification prior to conversion to help mitigate this issue. Notably, both surgical technicians cited comprehensive training and support from the new supplier’s representatives as increasing comfort with the new products. Cost savings were highlighted as an additional benefit by one of the technicians. There were no major changes cited in clinical outcomes. One of the surgical technicians noted that although they found the products equivalent, the increased availability of the new supplier’s products prevented surgery delays. One product was reverted to previously used products for one surgery type.
Quantitative Results
Consistent with the qualitative interview responses, quantitative findings on the conversion process show that 87% of respondents (n=7/8) were either somewhat satisfied or extremely satisfied with the level of information, training, and support they received, and with the availability of hemostatic agents during the conversion process (Figure 1). Three-quarters of respondents (n = 6) also indicated they were at least somewhat satisfied with the amount of resources or effort required for the conversion in terms of training, time, or costs. All respondents also indicated they were either somewhat satisfied or extremely satisfied with the hemostatic agents they have post-conversion compared to pre-conversion.
Vendor-Supported HOP
Qualitative Insights
During interviews, respondents (n = 3 surgeons) indicated they were generally satisfied with the vendor-supported HOP but noted a desire for additional information on costs related to the new products, including long-term benefits and savings. The respondents highlighted a particular interest in pricing (n = 1), waste reduction (n = 2), and outcomes (n = 1) of the program. In addition, one respondent suggested a greater emphasis be placed on younger surgeons, particularly those unfamiliar with the new supplier’s products, and a different respondent requested that the supplier’s representatives spend a longer period of time at the institution.
Quantitative Results
Respondents (n = 6) indicated they were at least somewhat satisfied with every aspect of the vendor-supported HOP evaluated in the survey, including data logistics (eg, data handoff, analysis, and reporting), training and support, and changes and recommendations resulting from the program (Figure 1). The highest satisfaction was with the training and support for the program provided by the supplier, and changes resulting from the program (eg, clinical, workflow, economic).
Clinical Case Series Review and Cost Analyses
A clinical case series review of charts of patients who experienced perioperative hemorrhage events between 2020 and 2022 did not reveal notable events nor trends over the program implementation period. An analysis of costs and hemostat utilization revealed that overall procedural supply expenditure decreased by nearly 25% following initiation of program implementation. The percent total expenditure on hemostat products by vendor also changed post-conversion; in 2020, the largest vendor accounted for 64% of the institution’s total spend, whereas in 2022, 98% of hemostat expenditures were going through a single source (Figure 2).
 |
Figure 2 Hemostat Product Expenditure by Vendor, 2020–2022. Percent expenditure on hemostat products was measured before (2020), during (2021), and after (2022) the cost and variation reduction initiative across the partnering vendor (blue circles, blue line), and the two non-partnering vendors (vendor 2: Orange circles, orange line; vendor 3: grey circles, grey line). |
Discussion
To our knowledge, this is the first study describing an experience of converting to a single supplier for surgical bleeding management at a large US academic medical center, including clinical and economic impacts, and overall satisfaction with the process. Rather than approach this as solely a cost-driven initiative, we also sought to capture and collate our learnings throughout the conversion. One of our goals at the outset of this study was to develop a roadmap for success, based on the diverse perspectives and experiences of different hospital stakeholders, for other institutions interested in implementing similar initiatives. After analyzing the qualitative and quantitative feedback received, our recommendations for best practices are as follows: 1) encourage engagement and participation from both clinical and non-clinical stakeholders via widespread outreach and clear communication, 2) ensure ample opportunity for HCPs to test and gain comfort using newly-introduced products, particularly for less experienced HCPs, and 3) report long-term findings that demonstrate the overall effects of the conversion back to all internal stakeholders, including clinical impact, cost-savings, and waste reduction, as applicable. Although our study focused specifically on the process of transitioning to single-vendor procurement for hemostasis products, many of our findings, particularly around the importance of communication with stakeholders and sharing long-term data on key implications, will be broadly applicable to other sourcing and variation reduction initiatives.
A value scorecard, developed at this medical center for physician-led sourcing projects, was used during the decision-making stages to ensure that the needs of different hospital stakeholders were adequately balanced, including provider preference and autonomy, patient care, inventory management and variation reduction, and cost. This data-driven approach helped to ensure that concerns and priorities across both clinical and non-clinical stakeholders were factored into the value determination for each opportunity. In our experience, this step is key to a clinically integrated supply chain. This value scorecard (Supplementary File 1) can potentially serve as an impactful tool for other hospitals interested in implementing similar initiatives moving forward.
Reducing costs without adversely impacting patient outcomes is a key focus of quality improvement in surgical care. Indeed, in our study, cost was cited by multiple stakeholders as the primary driver for conversion, and following program implementation, we showed a decrease in supply expenditure without notable events or trends in the quality of patient care, albeit evaluated in the context of a clinical case series review. To our knowledge, this is the first study describing conversion to a sole supplier for hemostatic products; however, studies exist describing vendor rationalization initiatives targeting other surgical supplies.4,7,8 One recent study evaluated changes in patient outcomes and costs following conversion from multi- to dual-, and finally single-vendor procurement for non-specialized, commodity spinal implants (eg, pedicle screws, rods, anterior cervical plates).6 Cost savings were realized following both conversion steps – even moving from a dual- to a single-vendor model (+21% additional reduction in the cost of commodity products) – without any adverse impact on surgical outcomes (eg, 12-month revision surgery, complications, 30-days readmissions, and postoperative patient-reported outcomes). Notably, to maximize cost savings, the authors employed a 2-pronged strategy, including converting to a single vendor for non-specialized implants (described above) as well as a capitated pricing strategy to lower the cost of specialized devices, demonstrating the incremental value of cost initiatives focused on both low- and high-cost supplies. The increasing use of adjunctive hemostats may make them a more important focus in cost saving initiatives moving forward. From 2000 to 2010, utilization of hemostatic agents increased from 28.5% to 35.2% in the United States in patients who underwent major general, gynecologic, urologic, cardiothoracic, or orthopedic surgery.9
Surgeons play an important role in cost containment in the OR through operative decision-making and surgical supply utilization – the latter of which is often dictated by preference. In fact, physician preference cards, which instruct hospital staff on the equipment and supplies a surgeon needs to successfully perform a specific procedure, have been shown to contribute to considerable differences in expenses across surgeons.23 As a result, they are often the focus of standardization programs aimed at reducing cost.24,25 Despite these preferences, however, studies indicate that physicians are amenable to improvement initiatives targeting surgical supplies. A prior study found that implementation of a surgeon-specific scorecard for lower-extremity joint arthroplasties to promote shared accountability in value-based care led to significant reductions in total cost (including implant cost) and healthcare resource utilization.26 Additionally, a prior survey of orthopedic surgeons (n = 492) found that respondents generally supported the practice of hospital’s limiting the number of implant vendors to reduce costs.27 Surgeon education programs have also been shown to successfully reduce disposable equipment costs.28 Given the importance of preference in surgical care, early involvement of physicians in initiatives targeting surgical devices and supplies is critical. In our study, the surgeons that were interviewed cited clear communication, and a sense of inclusion as key positive aspects of the conversion process. Preference card updates were also used in our initiative to help facilitate the conversion process and ensure ongoing success with variability reduction. Physician participation has similarly been noted as an important component of cost-saving programs in other vendor rationalization studies.7
Across the three components of the initiative (ie, the decision-making process, conversion, and vendor-supported HOP), respondents reported the highest satisfaction scores for the vendor-supported HOP. The HOP was designed to help address some of the current challenges with bleeding management during surgery. Surgeons can encounter a variety of different surgical bleeding situations, such as bleeds that are continuously oozing, difficult to access, or originate from high-pressure vessels. This is compounded by the multitude of different adjunctive hemostatic products available,20 each with unique properties and approaches to bleeding management. Several studies have attempted to provide guidance on bleeding control, but terminology is often inconsistent, and multiple products are recommended for each type of bleed, making the recommendations potentially difficult to apply to specific bleeding situations.13,14,20–22 In this study, the vendor-supported HOP was implemented to help mitigate these issues by harmonizing terminology and providing guidance and recommendations for the supplier’s hemostasis products, based on factors such as the bleeding site and situation, via a systematic, stepwise approach (eg, decision trees). Respondents rated the highest satisfaction with the support program in our study as vendor support has been previously shown to be an important factor in physician preference for surgical implants.29 In fact, in the qualitative interviews on the conversion process in our study, both surgical technicians noted comprehensive training and support from the supplier representatives as allowing them to feel comfortable with the new products.
In a qualitative case series review, there were no notable perioperative hemorrhage events or trends pre- versus post-implementation. This was also consistent with prior studies describing transitions to a single/preferred-vendor model for other surgical devices, even specialized implants, which did not demonstrate impacts on patient outcomes, such as the need for revision surgery, readmission, or complications.6,7
Limitations
Since participation in both the qualitative interviews and quantitative surveys was optional, self-selection could potentially attract a disproportionate number of respondents that had highly positive or highly negative experiences with the intervention. This is an inherent limitation of this type of voluntary qualitative research. However, given that we received similar feedback and satisfaction ratings across different stakeholder types (eg, hospital administrators, surgeons, nurses, and surgical technicians) and on different aspects of the process (eg, the decision-making process, conversion process, and vendor-supported HOP), we do not anticipate that responses were biased meaningfully either positively or negatively. These results could be validated in future study with a larger sample.
Another potential limitation is the limited sample size of respondents across the two quantitative surveys. There were several challenges with recruiting participation in this research. First, although the clinical program lead referred approximately n = 20 and n = 100 stakeholders for the qualitative interviews and quantitative surveys, respectively, participation was optional and self-selected by respondents. Second, the inclusion criteria limited the number of respondents invited to participate in the study to those that had direct interaction with either the hemostasis products, conversion process, planning process, or the vendor-supported HOP. As a result, our sample may not accurately represent the views of all potential stakeholders, limiting the generalizability of our findings. Importantly, however, findings describing cost savings and clinical events post-conversion used institution-wide data. Additionally, as this study was conducted at a single center, results of this study may have limited generalizability to other centers based on institutional characteristics.
Additionally, the only clinical and economic outcome measures assessed in this study were the occurrence of perioperative hemorrhage events, percent change in hemostat expenditure by vendor, and changes in procedural supply expenditure. Prior literature has identified additional complications associated with hemostat use in various surgical settings;30,31 in this study, based on the data available, no complications other than perioperative hemorrhage events were analyzed, but future study could evaluate additional outcomes. An interesting consideration is whether the vendor-supported HOP led to a more systematic and streamlined bleeding management program, possibly increasing efficiency in the OR. Even small savings in OR time can have meaningful impacts on costs.32,33 For example, one study found that optimizing surgical trays to reduce the number of instruments decreased the tray preparation time by approximately 5 minutes, leading to a projected hospital-wide annual savings of $28,000 for instrument processing alone.32 However, our study did not evaluate this directly, and future research is needed to determine whether additional OR efficiency could be achieved with improved bleeding management.
Conclusions
This study presents our data-driven, clinically led approach to transitioning to a sole supplier for surgical bleeding management at a large US academic medical center, resulting in a nearly 25% decrease in supply expenditure without discernable changes to the quality of patient care and demonstrating high overall satisfaction among both clinical and non-clinical hospital stakeholders. Based on perspectives shared during this study, we present a roadmap for success in implementing similar initiatives moving forward, including effectively engaging with a diverse group of hospital stakeholders, ensuring all providers have adequate time to get comfortable with the new products, and providing data on long-term impacts of program implementation. In future studies, it will be important for other groups to share their experiences, with similar sourcing and variation reduction initiatives to help validate and expand on the findings we present here.
Abbreviations
HCP, Healthcare Provider; HOP, Hemostasis Optimization Program; OR, Operating Room; PSI-09, Agency for Healthcare Research and Quality Patient Safety Indicator 9; US, United States.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was reviewed and approved by the Ohio State Biomedical Sciences Institutional Review Board (Study Number: 2021H0348). All participants provided informed consent prior to study participation.
Acknowledgments
The authors thank Atish De, MS (Trinity Life Sciences), and Emily Sharpe, PhD (Trinity Life Sciences), for providing medical writing assistance.
Author Contributions
TS, AS and MOH collected the data and conducted data synthesis and analysis. AS and MOH were major contributors in writing the manuscript. SB, WD, ID, and WV supervised the study and were involved in the interpretation of the data. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
MOH and AS are employed by Trinity Life Sciences and received consulting fees from Ethicon, Inc. WD and ID are employed by Ethicon, Inc. WV Vasileff reports educational consultant for Stryker Sports Med and Zimmer Sports Med. TS and SB declare that they have no competing interests.
References
1. Childers CP, Showen A, Nuckols T, Maggard-Gibbons M. Interventions to reduce intraoperative costs: a systematic review. Ann Surg. 2018;268(1):48–57. doi:10.1097/SLA.0000000000002712
2. Munoz E, Munoz W, Wise L. National and surgical health care expenditures, 2005–2025. Ann Surg. 2010;251(2):195–200. doi:10.1097/SLA.0b013e3181cbcc9a
3. Nathan H, Dimick JB. Medicare’s shift to mandatory alternative payment models: why surgeons should care. JAMA Surg. 2017;152(2):125–126. doi:10.1001/jamasurg.2016.4005
4. Althausen PL, Lapham J, Mead L. Financial impact of dual vendor, matrix pricing, and sole-source contracting on implant costs. J Orthop Trauma. 2016;30(Suppl 5):S37–S39. doi:10.1097/BOT.0000000000000719
5. Gupta A, Lee J, Chawla A, et al. A stepwise replicable approach to negotiating value-driven supply chain contracts for orthobiologics. J Am Acad Orthop Surg. 2023;31(9):470–476. doi:10.5435/JAAOS-D-21-01008
6. Blackburn CW, Thompson NR, Tanenbaum JE, Passerallo AJ, Mroz TE, Steinmetz MP. Association of cost savings and surgical quality with single-vendor procurement for spinal implants. JAMA Netw Open. 2019;2(11):e1915567. doi:10.1001/jamanetworkopen.2019.15567
7. Boylan MR, Chadda A, Slover JD, Zuckerman JD, Iorio R, Bosco JA. Preferred single-vendor program for total joint arthroplasty implants: surgeon adoption, outcomes, and cost savings. J Bone Joint Surg Am. 2019;101(15):1381–1387. doi:10.2106/JBJS.19.00008
8. Boylan MR, Chadda A, Bosco JA, Jazrawi LM. A preferred vendor model reduces the costs of sports medicine surgery. Arthroscopy. 2021;37(4):1271–1276. doi:10.1016/j.arthro.2020.10.051
9. Wright JD, Ananth CV, Lewin SN, et al. Patterns of use of hemostatic agents in patients undergoing major surgery. J Surg Res. 2014;186(1):458–466. doi:10.1016/j.jss.2013.07.042
10. Stokes ME, Ye X, Shah M, et al. Impact of bleeding-related complications and/or blood product transfusions on hospital costs in inpatient surgical patients. BMC Health Serv Res. 2011;11:135. doi:10.1186/1472-6963-11-135
11. Corral M, Ferko N, Hollmann S, Broder MS, Chang E. Health and economic outcomes associated with uncontrolled surgical bleeding: a retrospective analysis of the premier perspectives database. Clinicoecon Outcomes Res. 2015;7:409–421. doi:10.2147/CEOR.S86369
12. Johnston SS, Afolabi M, Tewari P, Danker W. Clinical and economic burden associated with disruptive surgical bleeding: a retrospective database analysis. Clinicoecon Outcomes Res. 2023;15:535–547. doi:10.2147/CEOR.S411778
13. Chiara O, Cimbanassi S, Bellanova G, et al. A systematic review on the use of topical hemostats in trauma and emergency surgery. BMC Surg. 2018;18(1):68. doi:10.1186/s12893-018-0398-z
14. Spotnitz WD. Hemostats, sealants, and adhesives: a practical guide for the surgeon. Am Surg. 2012;78(12):1305–1321. doi:10.1177/000313481207801221
15. Docimo G, Filograna Pignatelli M, Ferrandes S, et al. Role of absorbable polysaccharide hemostatic powder in the prevention of bleeding and wound events after thyroid surgery. J Clin Med. 2023;12(17):5684. doi:10.3390/jcm12175684
16. Natour E, Suedkamp M, Dapunt OE. Assessment of the effect on blood loss and transfusion requirements when adding a polyethylene glycol sealant to the anastomotic closure of aortic procedures: a case-control analysis of 102 patients undergoing Bentall procedures. J Cardiothorac Surg. 2012;7:105. doi:10.1186/1749-8090-7-105
17. Testini M, Marzaioli R, Lissidini G, et al. The effectiveness of FloSeal matrix hemostatic agent in thyroid surgery: a prospective, randomized, control study. Langenbecks Arch Surg. 2009;394(5):837–842. doi:10.1007/s00423-009-0497-5
18. Notarnicola A, Moretti L, Martucci A, et al. Comparative efficacy of different doses of fibrin sealant to reduce bleeding after total knee arthroplasty. Blood Coagul Fibrinolysis. 2012;23(4):278–284. doi:10.1097/MBC.0b013e3283518846
19. Briceno J, Naranjo A, Ciria R, et al. A prospective study of the efficacy of clinical application of a new carrier-bound fibrin sealant after liver resection. Arch Surg. 2010;145(5):482–488. doi:10.1001/archsurg.2010.62
20. Gabay M, Boucher BA. An essential primer for understanding the role of topical hemostats, surgical sealants, and adhesives for maintaining hemostasis. Pharmacotherapy. 2013;33(9):935–955. doi:10.1002/phar.1291
21. Shander A, Kaplan LJ, Harris MT, et al. Topical hemostatic therapy in surgery: bridging the knowledge and practice gap. J Am Coll Surg. 2014;219(3):570–9e4. doi:10.1016/j.jamcollsurg.2014.03.061
22. Sileshi B, Achneck H, Ma L, Lawson JH. Application of energy-based technologies and topical hemostatic agents in the management of surgical hemostasis. Vascular. 2010;18(4):197–204. doi:10.2310/6670.2010.00015
23. Allen JW, Polk HC. A study of added costs of laparoscopic cholecystectomy based on surgery preference cards. Am Surg. 2002;68(5):474–476. doi:10.1177/000313480206800516
24. Geppert P, Daily B, Casanova S. Achieving surgical supply savings through preference card standardization. J Med Syst. 2020;44(6):115. doi:10.1007/s10916-020-01576-9
25. Skarda DE, Rollins M, Andrews S, et al. One hospital, one appendectomy: the cost effectiveness of a standardized doctor’s preference card. J Pediatr Surg. 2015;50(6):919–922. doi:10.1016/j.jpedsurg.2015.03.009
26. Winegar AL, Jackson LW, Sambare TD, et al. A surgeon scorecard is associated with improved value in elective primary hip and knee arthroplasty. J Bone Joint Surg Am. 2019;101(2):152–159. doi:10.2106/JBJS.17.01553
27. Burns LR, Housman MG, Booth RE Jr, Koenig A. Implant vendors and hospitals: competing influences over product choice by orthopedic surgeons. Health Care Manage Rev. 2009;34(1):2–18. doi:10.1097/01.HMR.0000342984.22426.ac
28. Gitelis M, Vigneswaran Y, Ujiki MB, et al. Educating surgeons on intraoperative disposable supply costs during laparoscopic cholecystectomy: a regional health system’s experience. Am J Surg. 2015;209(3):488–492. doi:10.1016/j.amjsurg.2014.09.023
29. Burns LR, Housman MG, Booth RE, Koenig AM. Physician preference items: what factors matter to surgeons? Does the vendor matter? Med Devices. 2018;11:39–49. doi:10.2147/MDER.S151647
30. Gambardella CA-O, Clarizia G, Patrone R, et al. Advanced hemostasis in axillary lymph node dissection for locally advanced breast cancer: new technology devices compared in the prevention of seroma formation. BMC Surg. 2019;18:1–9. doi:10.1186/s12893-018-0454-8
31. Patrone RA-O, Gambardella C, Romano RM, et al. The impact of the ultrasonic, bipolar and integrated energy devices in the adrenal gland surgery: literature review and our experience. BMC Surg. 2019;18:1–7. doi:10.1186/s12893-018-0457-5
32. Dyas AR, Lovell KM, Balentine CJ, et al. Reducing cost and improving operating room efficiency: examination of surgical instrument processing. J Surg Res. 2018;229:15–19. doi:10.1016/j.jss.2018.03.038
33. Lonner JH, Goh GS, Sommer K, et al. Minimizing surgical instrument burden increases operating room efficiency and reduces perioperative costs in total joint arthroplasty. J Arthroplasty. 2021;36(6):1857–1863. doi:10.1016/j.arth.2021.01.041
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.