Back to Journals » Clinical Interventions in Aging » Volume 17
Implementation and Evaluation of Clinical Pharmacy Services on Improving Quality of Prescribing in Geriatric Inpatients in Vietnam: An Example in a Low–Resources Setting
Authors Dong PTX ![]() , Pham VTT, Dinh CT, Le AV, Tran HTH, Nguyen HTL
, Pham VTT, Dinh CT, Le AV, Tran HTH, Nguyen HTL ![]() , Hua S
, Hua S ![]() , Li SC
, Li SC
Received 5 April 2022
Accepted for publication 2 July 2022
Published 21 July 2022 Volume 2022:17 Pages 1127—1138
DOI https://doi.org/10.2147/CIA.S368871
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Nandu Goswami
Phuong Thi Xuan Dong,1,2 Van Thi Thuy Pham,1,3 Chi Thi Dinh,3 Anh Van Le,3 Ha Thi Hai Tran,4 Huong Thi Lien Nguyen,1 Susan Hua,2 Shu Chuen Li2
1Department of Clinical Pharmacy, Hanoi University of Pharmacy, Hanoi, Vietnam; 2School of Biomedical Sciences and Pharmacy, College of Health, Medicine and Wellbeing, University of Newcastle, Callaghan, NSW, Australia; 3Department of Pharmacy, Friendship Hospital, Hanoi, Vietnam; 4Department of Internal Cardiology, Friendship Hospital, Hanoi, Vietnam
Correspondence: Shu Chuen Li, School of Biomedical Sciences and Pharmacy, College of Health, Medicine and Wellbeing, University of Newcastle, NSW, Australia, Tel +061 0249215921, Fax +061 0249217903, Email [email protected]
Purpose: Geriatric inpatients generally have a high risk of drug-related problems (DRP) in prescribing following hospital admission, which are likely to cause negative clinical consequences. This is particularly evident in developing countries such as Vietnam. Therefore, clinical pharmacy service (CPS) aims to identify and resolve these DRPs to improve the quality use of medicines in the older population following hospital admission.
Patients and Methods: The study was conducted as a prospective, single-center study implemented at a general public hospital in Hanoi. Patients aged ≥ 60 years with at least three chronic diseases admitted to the Internal Medicine Department between August 2020 and December 2020 were eligible to be enrolled. A well-trained clinical pharmacist provided a structured CPS to identify any DRP in prescribing for each patient in the study. Clinical pharmacist interventions were then proposed to the attending physicians and documented in the DRP reporting system.
Results: A total of 255 DRP were identified in 185 patients during the study period. The most frequent types of DRP were underuse (21.2%), dose too high (12.2%), and contraindication (11.8%). There was a very high rate of approval and uptake by the physicians regarding the interventions proposed by the clinical pharmacist (82.4% fully accepted and 12.5% partially accepted). Of the interventions, 73.4% were clinically relevant (pADE score ≥ 0.1). In general, 9 out of 10 physicians agreed that CPS has significant benefits for both patients and physicians.
Conclusion: Improving clinical pharmacy services can potentially have a positive impact on the quality of prescribing in elderly inpatients. These services should officially be implemented to optimize the quality use of medicines in this population group in Vietnam.
Keywords: pharmacy practice, quality use of medicine, geriatrics
Introduction
Optimizing prescribing for the geriatric population is a challenge, especially in the hospital setting, due to a number of factors, such as multi-morbidity associated polypharmacy, age-related physiological changes, and pharmacokinetic and pharmacodynamic alterations.1,2 Studies on elderly inpatients worldwide have highlighted that Drug-Related Problems (DRP) in prescribing following hospital admission are frequent in this vulnerable population, including unintentional medication discrepancies3–7 and potentially inappropriate prescribing (PIP).8–10 These DRPs have been associated with adverse consequences, such as prolonged hospital stays, worsening clinical conditions, and increasing healthcare costs.11 Therefore, prescribing in elderly inpatients requires special consideration and attention to optimize quality use of medicines and minimize or avoid drug-related issues.
Implementation of clinical pharmacy services (CPS) is aimed at improving patient outcomes and minimizing medication harm through the provision of patient-centered pharmaceutical care.12 In the hospital setting, clinical pharmacists work with physicians in a multidisciplinary team to optimize medication prescribing by identifying, correcting, and preventing DRPs. Clinical pharmacist interventions (CPI) are defined as “any actions initiated by a pharmacist that directly result in a change to patient management or drug therapy”.13 Clinical pharmacists have played essential roles in improving the quality use of medicines in many settings. The positive clinical and economic outcomes of their interventions have been well established for many decades in North America, Australia, and European countries.12,14–18
In Vietnam, the proportion of the population aged 60 and over is increasing dramatically and will constitute 10% of the total population by 2025.19 There will be a resultant increase in demand for health services as the older population is known to consume more healthcare resources.20 However, Vietnamese physicians currently face a heavy workload in their routine practice – with a reported ratio of 7.8 doctors per 10,000 population in 2016. The situation is unlikely to improve in the short to medium term. Our recent findings suggest that prescribing issues, particularly in geriatric inpatients in Vietnam, will continue to be a serious concern stemming from heavy clinical workloads.7 Similar to other health care services, optimal prescribing in geriatric inpatients requires inter-professional teamwork, with the involvement of clinical pharmacists. However, the contribution of clinical pharmacists as an integrated part of a multi-disciplinary team in improving the quality use of medicines has not been widely evaluated in Vietnam up to now. Currently, the extent of implementation of CPS in Vietnamese hospitals varies widely due to differences in pharmacy human resources and the level of acceptance of CPS by medical staff at the hospital.21–23 Identified barriers to the implementation of CPS include limited research on the effectiveness of the activity and the lack of institutional implementation strategies.
In order to provide support for the implementation of CPS in Vietnamese hospitals, the impact of these services needs to be assessed. Therefore, this study aimed to evaluate bedside CPS for geriatric inpatients as an example of a model of pharmacist-led pharmaceutical care engaged in clinical practice in a low-resources setting. The outcome measures of the study were the number of DRPs in prescribing identified by the clinical pharmacist, the number of clinical pharmacy interventions (CPI), and the physicians’ acceptance of the clinical pharmacy interventions. The perceptions and opinions of physicians regarding CPS were also evaluated.
Methods
Study Setting and Study Population
This study was conducted at Friendship Hospital, an 800-bed public general hospital that provides healthcare services for retired geriatric patients in Hanoi. CPS was implemented in a pilot program at the 80-bed Internal Medicine Department over five months from August 2020 to December 2020. This was the first model of ward-based pharmacy services implemented in the study hospital. Patients at high risk of DRPs were included in the study. In particular, the patients targeted for CPS were those aged over 60 years, currently taking at least three drugs regularly to manage chronic diseases, and with at least three chronic conditions. Patients were expected to stay in the ward for a minimum of 48 hours.
Usual Care Before Implementing CPS
Before the implementation of CPS, the attending physician was solely responsible for prescribing medications to patients throughout the duration of their hospital admission. In some special clinical situations, the attending physician may request a consultation for additional prescribing advice from senior physicians or other specialties. Clinical pharmacists were not involved in the physician’s prescribing process for the patients.
Clinical Pharmacy Services (CPS)
A clinical pharmacist was assigned to work for 4 hours per day (0.5 Full-time Equivalent) at the study department from Monday to Friday every week during the study period. The assigned pharmacist was trained with a clinical pharmacy-orientated curriculum at the undergraduate level, was eligible to practice clinical pharmacy according to the standards of Decree No. 131 about Clinical Pharmacy Practice in Vietnam, and had a 6-month internship at the study department before officially implementing CPS. The clinical pharmacist provided bedside activities for each enrolled patient according to a structured process, focusing on improving the quality of prescribing with the primary goal of detecting, evaluating, and resolving DRPs in their prescribed medications. The CPS process followed by the pharmacist is summarized in Figure 1.
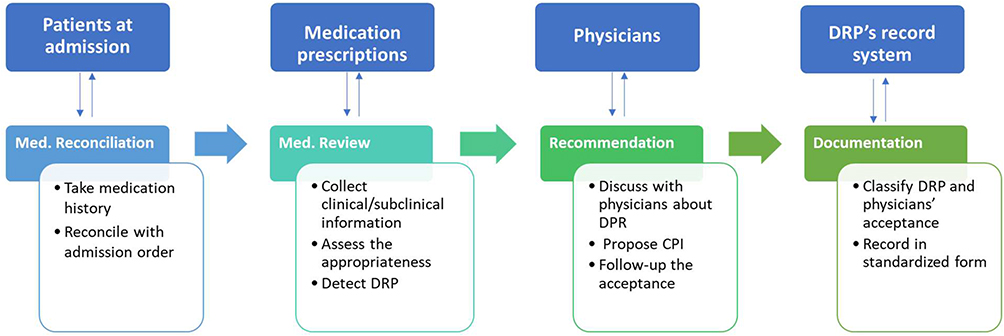 |
Figure 1 Process of clinical pharmacy services in the study. Abbreviations: DRP, drug-related problem; CPI, clinical pharmacist interventions. |
Briefly, the pharmacist conducted medication reconciliation for each eligible patient and recorded the patient’s medication history on the pharmacist’s medication reconciliation form. After that, the pharmacist collected information related to diagnosis, clinical and laboratory test results, and patient’s symptoms – these were recorded in the pharmacist’s Patient Monitoring Form. The pharmacist then reviewed each medication in the admission order for all aspects of appropriate prescribing, including indication, dose, dosage form, dosing regimen, timing of administration, lack of treatment, and lack of clinical/laboratory test monitoring to identify any potential DRPs. The clinical judgment was made using evidence-based materials, including current/official Vietnamese or hospital therapeutic guidelines, Summary of Product Characteristic (SmPC) and potentially inappropriate prescribing screening tools for the elderly, such as STOPP/START version 2.24
In addition, patients were also reviewed to determine whether follow-up was needed based on defined criteria (e.g., patients prescribed antibiotics, patients with a severe acute condition, and patients prescribed narrow therapeutic index medications). The DRPs detected during this process were recorded on the DRP summary sheet as a basis for discussion with the attending physicians. The clinical pharmacist actively communicated with the physicians the identified DRPs and the proposed CPI through face-to-face communication during ward-rounds, text messages, or phone calls. As part of the CPS, the clinical pharmacist also provided medication information on the selection, dosage, and adverse drug reactions (ADR) of drugs if requested by the physicians at the study ward.
The physicians’ acceptance rate for CPIs and their responses at three levels were recorded. The following shows the definition of the three levels. “Completely accepted” – the physician agreed with the DRP and the clinical pharmacist’s intervention, and the prescribing order was changed according to the recommendation of the clinical pharmacist. “Partially accepted” – the physician agreed with the DRP but the change of prescribing order may not be the same as the clinical pharmacist’s intervention (eg, change to a drug that was not the same as suggested or the changed dose was not the same as recommended). “Not accepted” – the physician disagreed with the DRP and the clinical pharmacist’s intervention, and no changes to the medical order were made. For medication information related to prescribing (ie, the physicians asked the clinical pharmacist to calculate the drug dose or select a drug for an indication), the intervention was counted as being “completely accepted” if the physician agreed with the drug/active ingredient corresponding to the pharmacist’s advice.
Data Collection
Information about the patients, characteristics of DRPs, and approval status of CPIs by physicians were collected through (i) Pharmacist’s Medication reconciliation form, (ii) Pharmacist’s Patient Monitoring sheet, (iii) DRP summary sheet for each patient, and (iv) Weekly Pharmacist’s Summary Report. The Weekly Pharmacist’s Summary Report was sent to the Head of Pharmacy Department and the head of the study department. The demographic information collected for each patient included age, gender, weight, primary diagnosis, comorbidities, list of medication history, medications prescribed for 48 hours, duration of hospital admission, and Charlson Comorbidity Index.25 The Pharmaceutical Care Network Europe (PCNE) DRP classification system was used to classify and document DRPs.26
Outcome Measure
The impact of CPS was assessed through the number of DRPs identified, the number of clinical pharmacist interventions, and the physician’s acceptance rate of clinical pharmacist interventions. In addition, the clinical significance of accepted DRPs and the physicians’ assessment of CPS were also evaluated.
Assessment of Clinical Significance of DRPs
Determination of the potential and severity of harm that a patient would experience due to a DRP was based on the methodology described by Nesbit et al27–29 to produce a potential Adverse Drug Event (pADE) score. The pADE score is a potential and severity score for discomfort, harm, and/or clinical deterioration caused by a DRP. The assessment uses the following categories for probability and severity of harm: 0 (no harm expected by the DRP), 0.01 (very low: some harm is expected, but not clinically relevant), 0.1 (low: some harm is expected but poorly clinically relevant), 0.4 (medium; harm is expected, clinically relevant), or 0.6 (high; damage is expected, life-threatening). After being randomly presented and blinded, DRPs identified were sent to two external clinical experts (one pharmacist with advanced training in pharmacotherapy and one internist – both had 10-year experience in practice) to assess the potential clinical significance. Each expert independently assigned a pADE score to each DRP and resolved any difference in assessment through consensus in a meeting of the two aforementioned experts.
Evaluation of Physicians’ Opinions on Clinical Pharmacy Services
All physicians who worked in the study department were sent an anonymous questionnaire about their views on CPS during the implementation period. The research team designed the questionnaire to determine the level of agreement of the physicians across four themes: (i) the pharmacist’s competence, (ii) the contribution of each CPS, (iii) the overall benefit of the CPS, and (iv) the expectation in the future. The questionnaire used a 5-point Likert scale to determine the physicians’ perspectives, whereby level 1 corresponded to “strongly disagree” and level 5 corresponded to “strongly agree”. The questionnaire was delivered to and collected from the physicians by a research member that was independent of the CPS implemented in the study department. The survey took place in January 2021.
Data Analysis
Data related to participants, medication prescriptions, and clinical pharmacist interventions were recorded into an Excel database (version 2020 Microsoft Corporation, Redmond, WA, USA). Statistical analysis was performed using SPSS version 27 (SPSS, Inc, Chicago, IL, USA). Descriptive statistics included median and interquartile range (IQR) for nonparametric data; mean and standard deviation were calculated for normally distributed data. Characteristics of DRPs were described by percentage and frequency.
Results
Participant Characteristics
A total of 185 geriatric inpatients were included in the study during the implementation period. The demographics and baseline characteristics of these patients are shown in Table 1. The average age of the study participants was relatively high at 78.9 (± 8.0) years, and 68.6% were males. The most common chronic diseases in the study participants were hypertension (83.2%), chronic coronary syndrome (73.0%), heart failure (37.8%), type 2 diabetes (35.1%), and hyperlipidemia (23.2%). The average number of co-morbidities was 4.4 ± 1.9. Each patient was prescribed an average of 7.7 (± 2.3) medications on their admission prescription order and stayed 14.0 (± 7.6) days at the study department.
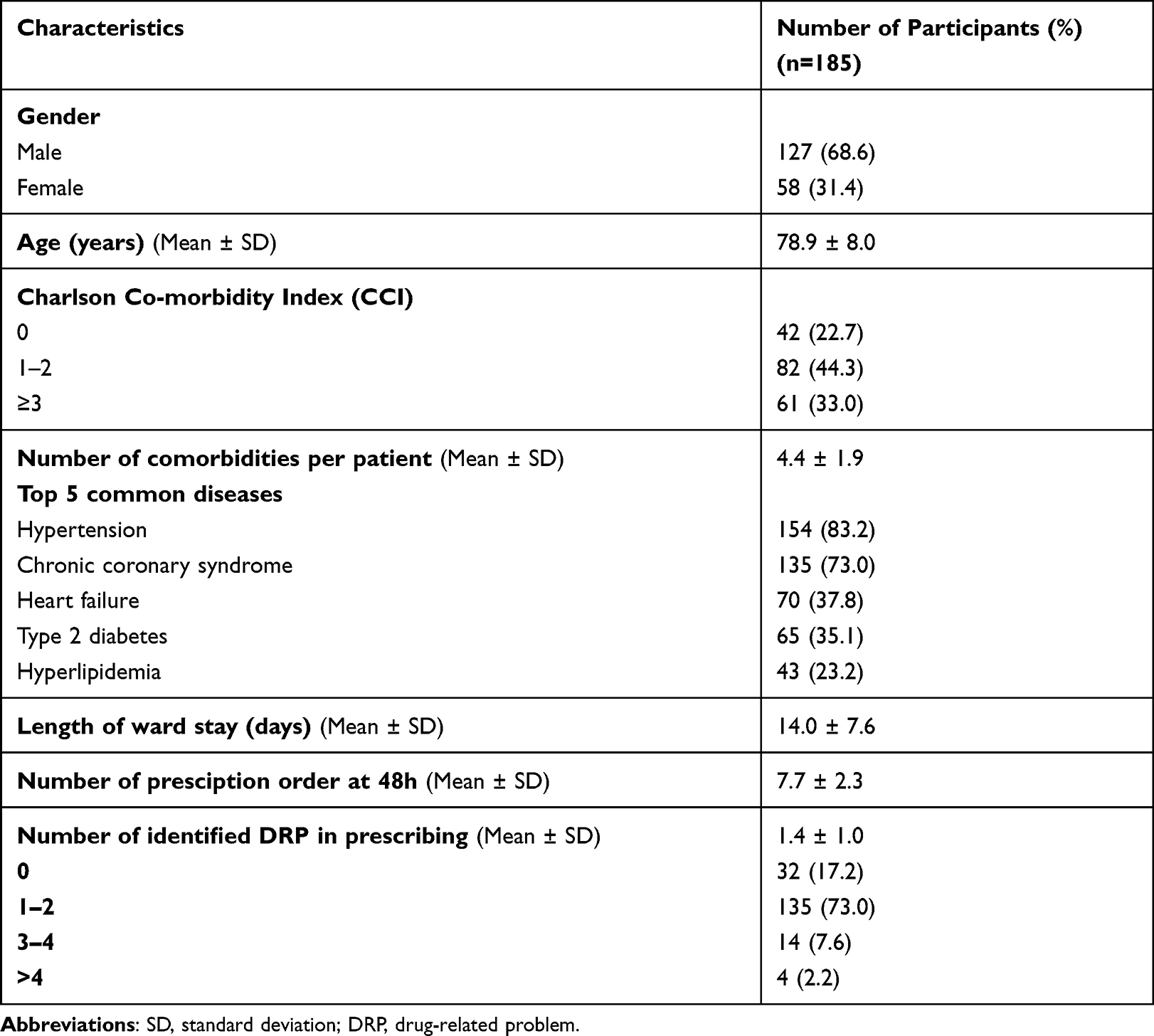 |
Table 1 Demographics and Characteristics of the Study Participant |
Characteristics of Drug-Related Problems Identified by a Clinical Pharmacist
The clinical pharmacist detected a total of 255 DRPs, involving 285 drugs (Table 2). The number of DRPs related to inappropriate prescribing accounted for a very high rate, with the most frequent types of DRP being underuse (21.2%), dose too high (12.2%), and contraindication (11.8%). Drug-related problems were found in many different classes of drugs. The most commonly involved drug groups were cardiovascular drugs (anti-ischemic agents, antihypertension agents, antithrombotic agents, anti-hyperlipidemic agents), proton pump inhibitors, and antidiabetic drugs (Table 3).
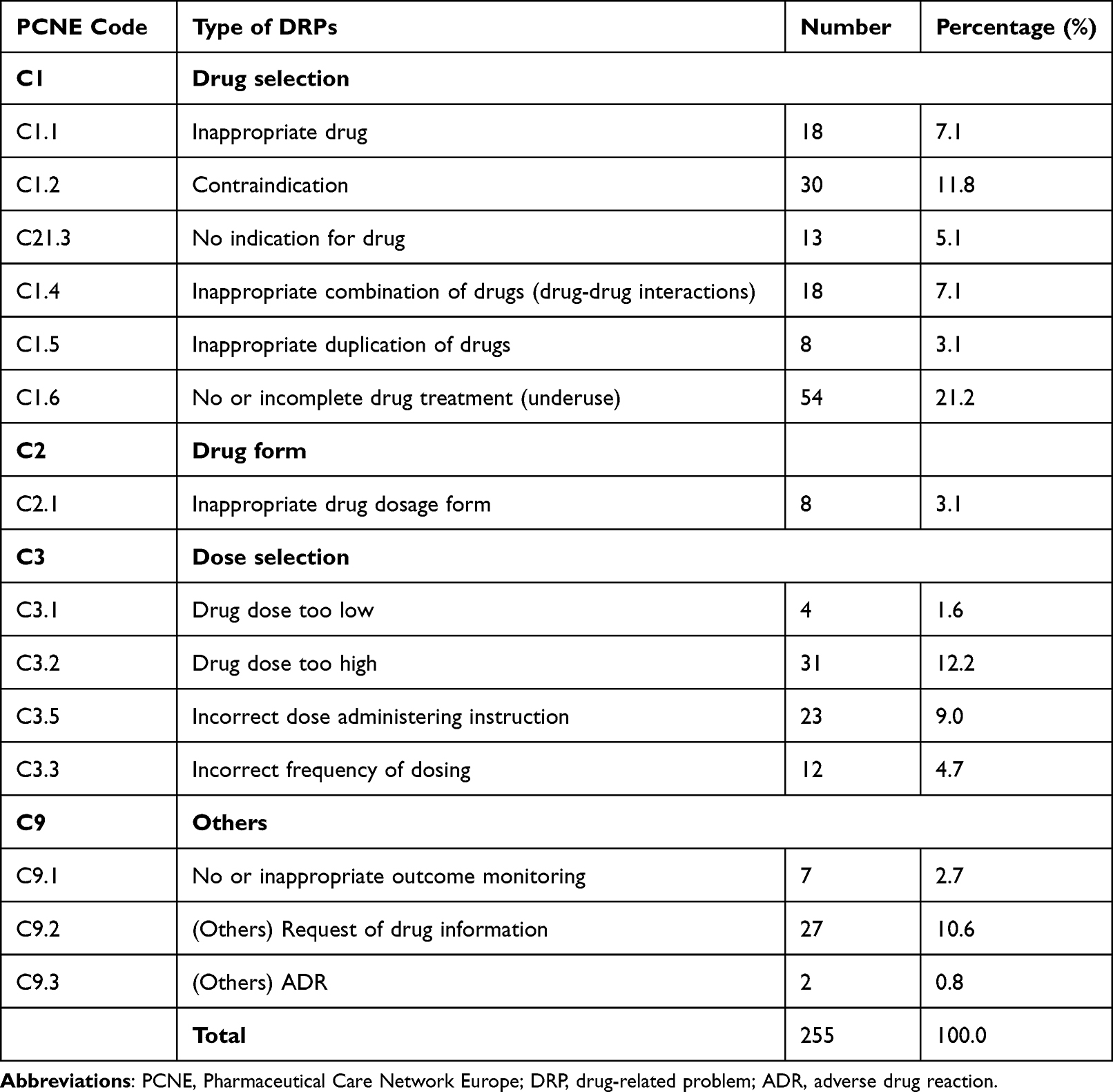 |
Table 2 Types of Identified Drug-Related Problems (n = 255) |
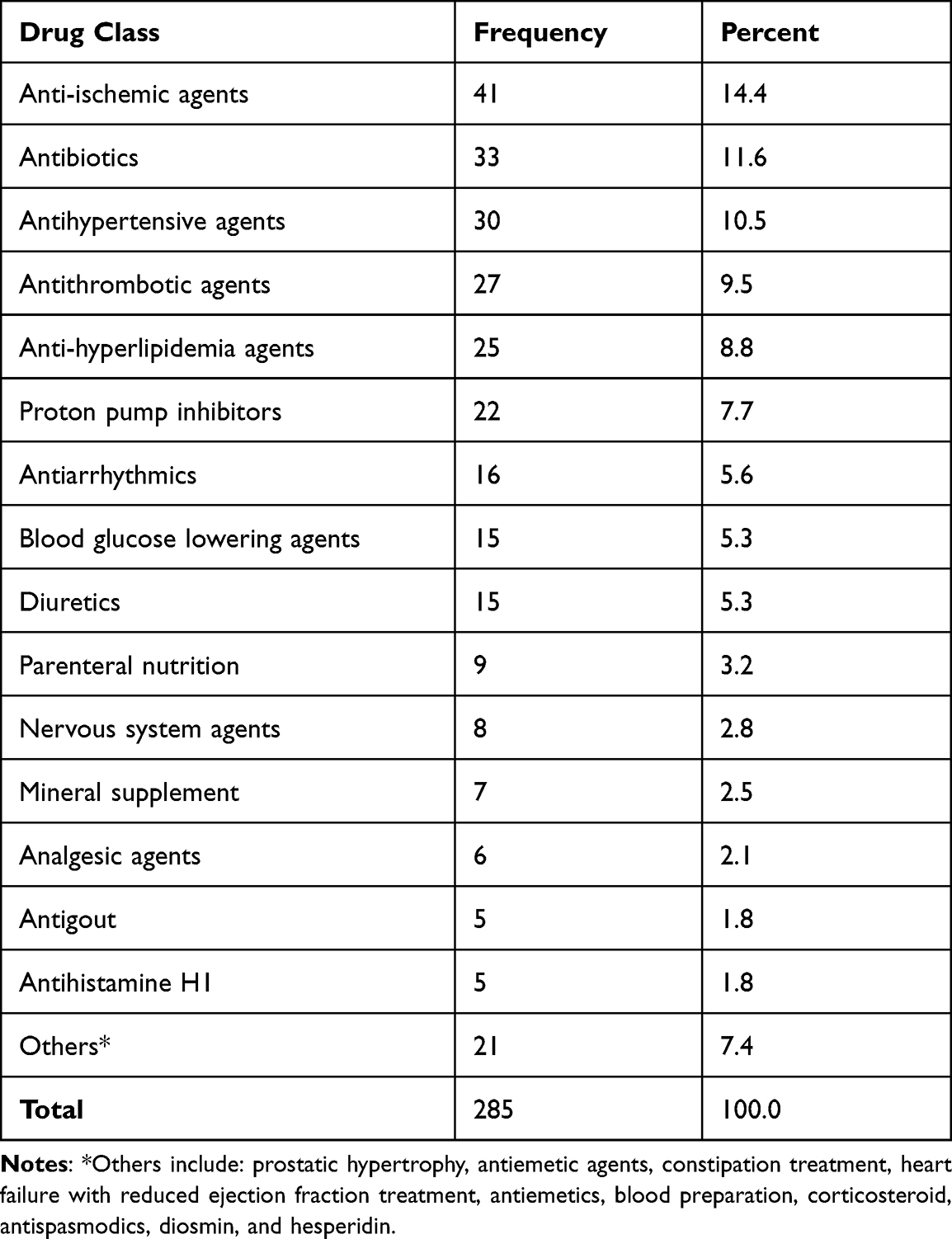 |
Table 3 Categories of Medications Related to DRPs (n = 285) |
Type, Acceptance Rate and Clinical Significance of Clinical Pharmacist Interventions
The type, acceptance rate and clinical significance of CPIs are summarized in Table 4. Corresponding to the types of DRP detected, the most common clinical pharmacist interventions were initiation of a new drug (21.2%), discontinuation of a drug (17.6%), and change of drug (17.3%). The overall rate of physicians’ approval with the interventions proposed by the clinical pharmacist was very high (82.4% fully accepted and 12.5% partially accepted). Although there was variation in acceptability for different types of interventions, a high acceptance rate was observed in all types of interventions. Among these, 100% of cases of counseling of drug or dose selection were accepted, followed by discontinuation (91.1%), dose reduction (84.4%), and clinical/subclinical monitoring (85.8%). In terms of clinical significance of clinical pharmacist interventions, 73.4% of interventions were considered as clinically relevant (pADE score ≥0.1). One-fifth of them had at least moderate clinical significance, according to the experts’ assessment.
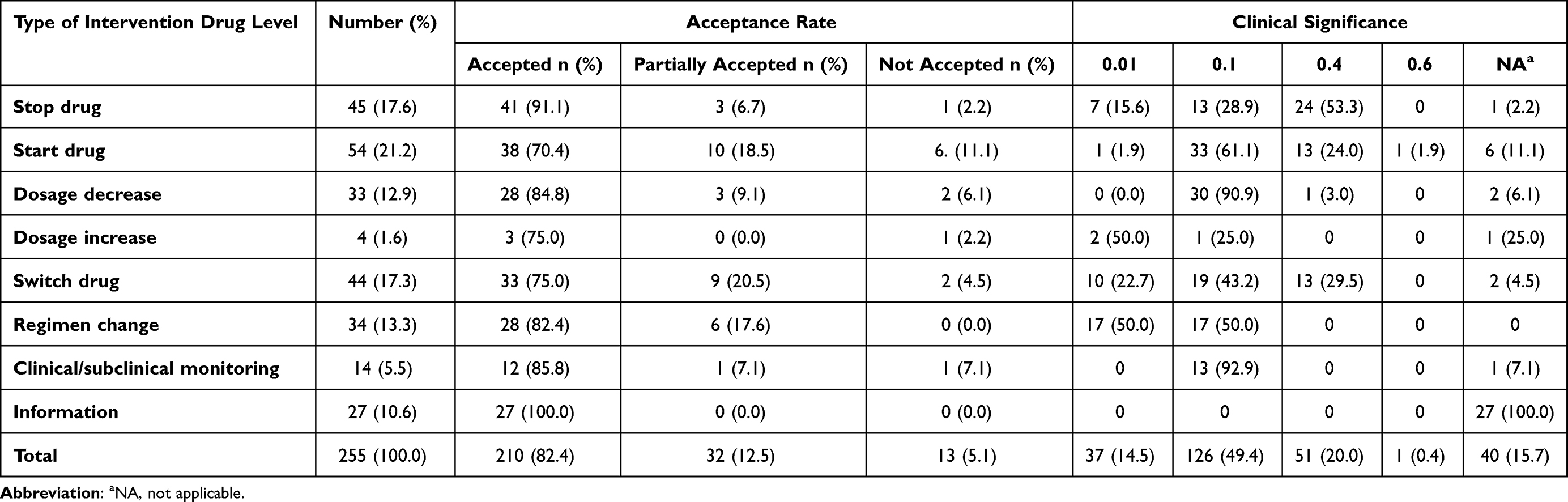 |
Table 4 Type, Acceptance Rate and Clinical Significance of Clinical Pharmacist Interventions |
Physicians’ Perspectives About Clinical Pharmacy Services
All physicians (n = 10) that worked in the study department of Friendship Hospital during the CPS implementation period answered the questionnaire with generally positive opinions (Table 5). The level of satisfaction of the physicians with the clinical pharmacist’s knowledge and skills was very high. For example, 6/10 physicians strongly agreed and 3/10 physicians agreed that the clinical pharmacist had sufficient knowledge regarding medications and therapeutics, and 9/10 physicians strongly agreed that the clinical pharmacist demonstrated effective communication skills. Related to each CPS activity, all physicians agreed that the clinical pharmacist provided an accurate medication history and in a timely manner (9/10 strongly agreed and 1 agreed) as well as provided appropriate medication information when requested (9/10 strongly agreed and 1 agreed). In general, 9/10 physicians agreed that CPS have significant benefit for both patients and physicians.
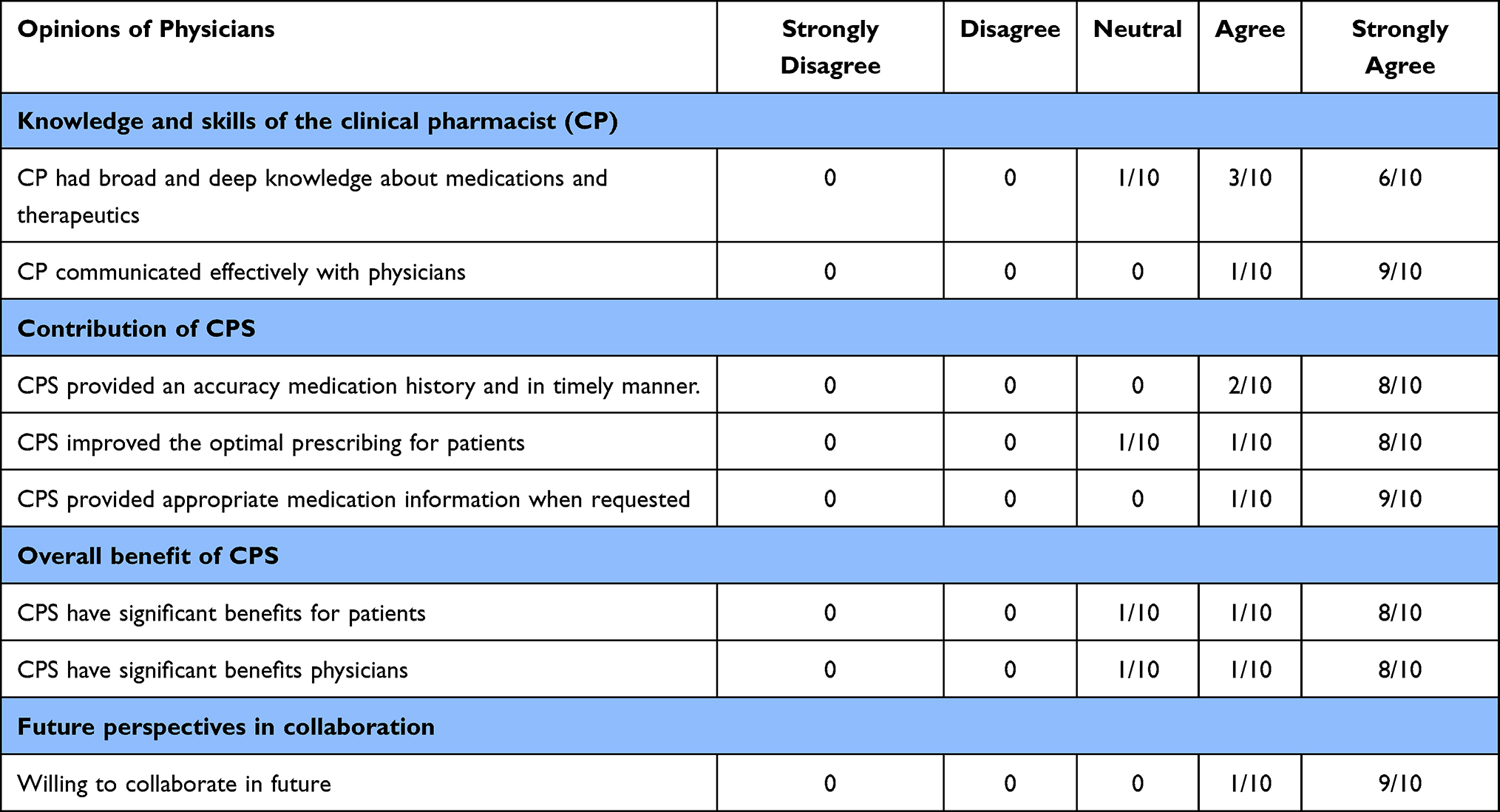 |
Table 5 Physicians’ Perspectives About Clinical Pharmacy Services (CPS) (n = 10) |
Discussion
To the best of our knowledge, this is the first study in Vietnam to investigate the role of CPS in improving the quality of prescribing in the geriatric population in a hospital setting. As confirmed in several studies, pharmaceutical care activities on individualized patients have not been standardized in Vietnamese hospitals.21–23 The participation of pharmacists in optimizing prescribing for inpatients has been limited and varied depending on the available human resources, the hospital policies, as well as the approach of each pharmacist. This study is expected to provide meaningful evidence of how to implement novel CPS in Vietnamese hospital settings as well as demonstrate their impact.
The shortage of human resources is one of the most significant barriers to implementing CPS in hospitals.21–23 With this lack of human resources, it is essential to identify priority patients and prioritize clinical pharmacy activities. In this study, with 0.5 FTE clinical pharmacist per 80 beds, we developed a structured process of CPS for geriatric inpatients to make this process sustainable, time-efficient, and effective. Geriatric patients were selected as the target population for CPS because they are highly vulnerable to DRPs and suboptimal prescribing due to multiple risk factors. Our study results provide supporting evidence for the positive contribution of clinical pharmacists in the multidisciplinary team to improving the quality of prescribing in geriatric patients in a developing country. This was demonstrated through several important outcomes: (i) a large number of DRPs in prescribing were identified, (ii) the high rates of physicians acceptance of CPI, (iii) the high proportion of clinically significant CPIs, and (iv) the physicians’ positive assessment of the overall effectiveness of CPS. Therefore, there is significant opportunity for clinical pharmacists in Vietnamese hospitals to contribute to enhancing the quality use of medicines, especially in geriatric inpatients.
Numbers and Types of DRPs
The amount of DRPs and the characteristics of the DRP detected by CPS vary widely in the literature. This is likely attributed to the different study settings, the capacity of clinical pharmacists, number of the pharmacist/number of bed ratio, and the type of DRP that was the focus of each study.30–32 For this current study, only the CPIs that improved the quality of prescriptions was described and only the DRPs that were communicated to the physicians were calculated. Some other groups of DRPs, such as those related to patients’ medication adherence and medication administration, were not included in the study. Therefore, the average number of DRPs for each patient in this study may be lower compared to those reported by other studies. Despite this, our study has unequivocally shown that DRPs in geriatric inpatients are relatively common in Vietnam, thereby confirming the necessity of CPS in improving the quality of prescribing in this population group. Furthermore, DRPs were detected across many different drug groups, with the most common (eg, cardiovascular drugs and diabetes drugs) related to long-term medications for managing chronic diseases in geriatric patients. Therefore, the detection and resolution of these DRPs during the hospital stay could be expected to provide long-term benefits to the patient post-discharge into the community.
Clinical Pharmacist Interventions and Physicians’ Acceptance Rate
In this study, the physicians’ approval rate for the clinical pharmacist’s interventions was relatively high (82.4% of CPI). This rate is congruent with a number of other published studies30–37 that were in the range of 76% to 93%. However, this is in contrast to some other studies in the geriatric population, such as the study by Somer et al, which reported a 54% acceptance rate.38 There are several reasons for the difference in acceptance rates. Factors that are associated with higher acceptance include the class of medications, types of CPI, types of diseases, physicians’ specialties, and experiential background of clinical pharmacists.39,40 The latter could partly explain the high acceptance rate in this current study through a high degree of physicians’ appreciation of the pharmacist’s knowledge and expertise. This shows that pharmacist competence is the core to providing effective CPS. The high acceptance rates also indicate that the physicians in the study department of the hospital are open to collaboration with pharmacists, although CPS is still a new concept in Vietnam. This study included an assessment of the clinical significance of the approved interventions. Of the DRPs and corresponding CPIs, 69.8% were assessed as clinically significant with a pADE score ≥0.1 and one-fifth of the interventions were classified as having moderate-to-high clinical significance. The results also emphasize the contribution of CPI to the prescribing practice of physicians in this study.
Physicians’ Opinion About CPS
All physicians working in the department during the study period participated in answering the questions. Physicians generally agreed that the benefits of CPS to physicians and patients are substantial, thereby indicating that the introduction of CPS activities to support prescribing was successful. In this study, the positive reviews could be explained by a number of factors: (i) the pharmacist had 6 months of familiarity with the study department before implementing CPS; (ii) Standard Operating Procedures were developed and introduced to the physicians; and (iii) CPIs were made based on evidence and communicated appropriately. Studies across the world on the implementation of new clinical pharmacy activities have shown similar results in terms of physicians’ perspectives on cooperation with CPS. This reinforces the attitude of physicians to working in collaboration with pharmacists and shows an open view of physicians when there is one more support person to improve the quality of prescriptions for patients41–45
Limitations
There are several limitations to our study. The study was conducted in only one internal medicine department at a large hospital in Hanoi, with one clinical pharmacist involved in the provision of services. Therefore, the amount of DRPs detected as well as the physicians’ approval were significantly dependent on the pharmacist’s expertise and communication skills as well as the perception of the physicians with regard to CPS. The study did not evaluate the impact of CPS using solid clinical endpoints (ie, mortality, morbidity) nor calculate the costs related to the service (healthcare utilization) or quality of life of patients. The process parameters, including the number of identified DRPs, the acceptance rate of physicians, and the clinical significance of DRPs were employed to demonstrate the benefits of CPS in this initial study. Despite these limitations, the results represent a very important finding that CPS is likely to deliver benefits for patients in Vietnam. Lastly, during the study period, all physicians were aware of the purpose of the study. Hence, the occurrence of the Hawthorne effect46 could not be ruled out, meaning the physician may have taken the prescription/action differently from usual because they perceived that they were a part of the study and, therefore, caused a reduction in DRPs observed during the study period.
Conclusion
This study clearly demonstrates that the prevalence of DRPs in prescribing was high among geriatric inpatients in Vietnam. A well-developed CPS can contribute to the detection and resolution of these DRPs with good acceptance by physicians. The results suggest a positive benefit for ward-based pharmacy services in improving the quality of use of medicines in geriatric inpatients. These results can also form a basis for developing a standard operating model of clinical pharmacy activities aimed at utilizing the limited human resources in the Vietnamese healthcare system in a more effective way.
Abbreviations
CCI, Charlson co-morbidity index (CCI); CI, confidence intervals; CPS, clinical pharmacy services; CPI, clinical pharmacist intervention; DRPs, drug-related problems; pADE, potential adverse drug event; QUM, quality use of medicine; SD, standard deviation; SOP, standard operating procedure; WHO, World Health Organization.
Data Sharing Statement
All data generated and analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
This study was granted ethics approvals by The Hospital Science and Technology Committee at Friendship Hospital, Vietnam and the Human Research Ethics Committee (HREC) at the University of Newcastle, Australia (Approval Number H-2020-0187). The study was performed in accordance with the Declaration of Helsinki.
Consent to Participate
All participants have provided written consents to participate
Consent to Publication
All listed authors have approved the manuscript before submission, including the names and order of authors
Acknowledgments
The authors wish to thank Dr Le Ngoc Tien, Msc. Thuy Thi Thu Nguyen, Msc. Thao Thi Nguyen and the staff at the Department of Pharmacy as well as the physicians, nurses and patients at the Friendship Hospital for their collaboration in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests.
References
1. Jacobs JM, Maaravi Y, Cohen A, Bursztyn M, Ein-Mor E, Stessman J. Changing profile of health and function from age 70 to 85 years. Gerontology. 2012;58(4):313–321. doi:10.1159/000335238
2. Steinman MA, Landefeld CS, Rosenthal GE, Berthenthal D, Sen S, Kaboli PJ. Polypharmacy and prescribing quality in older people. J Am Geriatr Soc. 2006;54(10):1516–1523.
3. Belda-Rustarazo S, Cantero-Hinojosa J, Salmeron-Garcia A, Gonzalez-Garcia L, Cabeza-Barrera J, Galvez J. Medication reconciliation at admission and discharge: an analysis of prevalence and associated risk factors. Int J Clin Pract. 2015;69(11):1268–1274.
4. Rodriguez Vargas B, Delgado Silveira E, Iglesias Peinado I, Bermejo Vicedo T. Prevalence and risk factors for medication reconciliation errors during hospital admission in elderly patients. Int J Clin Pharm. 2016;38(5):1164–1171.
5. Magalhães GF, de Carvalho Santos GBN, Rosa MB, Noblat L. Medication reconciliation in patients hospitalized in a cardiology unit. PLoS One. 2014;9(12):e115491.
6. Cornu P, Steurbaut S, Leysen T, et al. Effect of medication reconciliation at hospital admission on medication discrepancies during hospitalization and at discharge for geriatric patients. Ann Pharmacother. 2012;46(4):484–494.
7. Dong PTX, Pham VTT, Nguyen TT, Nguyen HTL, Hua S, Li SC. Unintentional Medication Discrepancies at Admission Among Elderly Inpatients with Chronic Medical Conditions in Vietnam: a Single-Centre Observational Study. Drugs Real World Outcomes. 2022;9(1):141–151.
8. Hill-Taylor B, Sketris I, Hayden J, Byrne S, O’Sullivan D, Christie R. Application of the STOPP/START criteria: a systematic review of the prevalence of potentially inappropriate prescribing in older adults, and evidence of clinical, humanistic and economic impact. J Clin Pharm Ther. 2013;38(5):360–372.
9. Abegaz TM, Birru EM, Mekonnen GB. Potentially inappropriate prescribing in Ethiopian geriatric patients hospitalized with cardiovascular disorders using START/STOPP criteria. PLoS One. 2018;13(5):e0195949.
10. Argoullon L, Manciaux MA, Valance A, Bonneville A. Potentially inappropriate prescribing in elderly patient: analyze before/after hospitalization. Geriatr Psychol Neuropsychiatr Vieil. 2018;16(2):155–163.
11. van den Bemt PM, Egberts TC. Drug-related problems in hospitalised patients. Drug Saf. 2000;22(4):321–333.
12. American College of Clinical Pharmacy. The definition of clinical pharmacy. Pharmacotherapy. 2008;28(6):816–817.
13. Pharmaceutical Society of Australia. Guidelines for Pharmacists Performing Clinical Interventions. Deakin West: Pharmaceutical Society of Australia; 2018.
14. Rose O, Derendorf H, Erzkamp S, et al. Development of clinical pharmacy services in Australia, Austria, Belgium, Bosnia-Herzegovina, Canada, Germany, Japan, Kosovo, Switzerland, the Netherlands, Thailand, USA and correlation with educational standards, level of research, and implemen. Int J Clin Pharmacol Ther. 2018;56(11):518–530.
15. Kaboli PJ, Hoth AB, McClimon BJ, Schnipper JL. Clinical pharmacists and inpatient medical care: a systematic review. Arch Intern Med. 2006;166(9):955–964.
16. Gallagher J, McCarthy S, Byrne S. Economic evaluations of clinical pharmacist interventions on hospital inpatients: a systematic review of recent literature. Int J Clin Pharm. 2014;2:36.
17. Pedersen CA, Schneider PJ, Scheckelhoff DJ. ASHP national survey of pharmacy practice in hospital settings: prescribing and transcribing-2016. Am J Health Syst Pharm. 2017;74(17):1336–1352.
18. Pedersen CA, Schneider PJ, Ganio MC, Scheckelhoff DJ. ASHP national survey of pharmacy practice in hospital settings: prescribing and transcribing-2019. Am J Health Syst Pharm. 2020;77(13):1026–1050.
19. websites C. Vietnam Population clock 2017. Available from: http://countrymeters.info/en/Vietnam.
20. Lehnert T, Heider D, Leicht H, et al. Review: health care utilization and costs of elderly persons with multiple chronic conditions. Med Care Res Rev. 2011;68(4):387–420.
21. Trinh HT, Nguyen HTL, Pham VTT, et al. Hospital clinical pharmacy services in Vietnam. Int J Clin Pharm. 2018;40(5):1144–1153.
22. Nguyen-Thi HY, Nguyen-Ngoc TT, Le NH, Le NQ, Le NDT. Current status of clinical pharmacy workforce, services and clinical pharmacist recruitment in Ho Chi Minh City, Vietnam. Int J Health Plann Manage. 2020;35(5):1205–1218.
23. Nguyen-Thi HY, Nguyen-Ngoc TT, Do-Tran MT, Do DV, Pham LD, Le NDT. Job satisfaction of clinical pharmacists and clinical pharmacy activities implemented at Ho Chi Minh city, Vietnam. PLoS One. 2021;16(1):e0245537.
24. O’Mahony D, O’Sullivan D, Byrne S, O’Connor MN, Ryan C, Gallagher P. STOPP/START criteria for potentially inappropriate prescribing in older people: version 2. Age Ageing. 2015;44(2):213–218.
25. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383.
26. Pharmaceutical Care Network Europe Association. PCNE Classification for Drug-Related Problems V9.1 2020. Pharmaceutical Care Network Europe Association; 2020.
27. Bosma LBE, Hunfeld NGM, Quax RAM, et al. The effect of a medication reconciliation program in two intensive care units in the Netherlands: a prospective intervention study with a before and after design. Ann Intensive Care. 2018;8(1):19.
28. Gallagher J, Byrne S, Woods N, Lynch D, McCarthy S. Cost-outcome description of clinical pharmacist interventions in a university teaching hospital. BMC Health Serv Res. 2014;14:177.
29. Nesbit TW, Shermock KM, Bobek MB, et al. Implementation and pharmacoeconomic analysis of a clinical staff pharmacist practice model. Am J Health Syst Pharm. 2001;58(9):784–790.
30. Hailu BY, Berhe DF, Gudina EK, Gidey K, Getachew M. Drug related problems in admitted geriatric patients: the impact of clinical pharmacist interventions. BMC Geriatr. 2020;20(1):13.
31. O’Sullivan D, O’Mahony D, O’Connor MN, et al. The impact of a structured pharmacist intervention on the appropriateness of prescribing in older hospitalized patients. Drugs Aging. 2014;31(6):471–481.
32. Ertuna E, Arun MZ, Ay S, Koçak FÖK, Gökdemir B, Ispirli G. Evaluation of pharmacist interventions and commonly used medications in the geriatric ward of a teaching hospital in Turkey: a retrospective study. Clin Interv Aging. 2019;14:587–600.
33. Spinewine A, Dhillon S, Mallet L, Tulkens PM, Wilmotte L, Swine C. Implementation of ward-based clinical pharmacy services in Belgium–description of the impact on a geriatric unit. Ann Pharmacother. 2006;1:40.
34. Miller G, Franklin BD, Jacklin A. Including pharmacists on consultant-led ward rounds: a prospective non-randomised controlled trial. Clin Med. 2011;11:312.
35. Nielsen TR, Andersen SE, Rasmussen M, Honoré PH. Clinical pharmacist service in the acute ward. Int J Clin Pharm. 2013;35:1137.
36. Lombardi N, Wei L, Ghaleb M, et al. Evaluation of the implementation of a clinical pharmacy service on an acute internal medicine ward in Italy. BMC Health Serv Res. 2018;1:18.
37. Zaal RJ, den Haak EW, Andrinopoulou ER, van Gelder T, Vulto AG, van den Bemt P. Physicians’ acceptance of pharmacists’ interventions in daily hospital practice. Int J Clin Pharm. 2020;42(1):141–149.
38. Somers A, Robays H, Paepe P, Maele G, Perehudoff K, Petrovic M. Evaluation of clinical pharmacist recommendations in the geriatric ward of a Belgian university hospital. Clin Interv Aging. 2013;1:8.
39. Saadah LM, Nazzal YM, Abdelmaksoud SI, Nazzal MK, El AS, Qasemi AA. Predictors of physicians acceptance of clinical pharmacy recommendations at a military hospital in the United Arab Emirates. Int J Pharm. 2014;4:5418.
40. Mann A, Esse T, Abughosh SM, Serna O. Evaluating pharmacist-written recommendations to providers in a medicare advantage plan: factors associated with provider acceptance. J Manag Care Spec Pharm. 2016;22:49–55.
41. Gillespie U, Mörlin C, Hammarlund-Udenaes M, Hedström M. Perceived value of ward-based pharmacists from the perspective of physicians and nurses. Int J Clin Pharm. 2012;34:127.
42. Farrell B, Pottie K, Woodend K, Yao V, Dolovich L, Kennie N. Shifts in expectations: evaluating physicians’ perceptions as pharmacists become integrated into family practice. J Interprof Care. 2010;24:80.
43. Vinterflod C, Gustafsson M, Mattsson S, Gallego G. Physicians’ perspectives on clinical pharmacy services in Northern Sweden: a qualitative study. BMC Health Serv Res. 2018;18(1):35.
44. Shanika LGT, Wijekoon CN, Jayamanne S, et al. Acceptance and attitudes of healthcare staff towards the introduction of clinical pharmacy service: a descriptive cross-sectional study from a tertiary care hospital in Sri Lanka. BMC Health Serv Res. 2017;17(1):46.
45. Li X, Huo H, Kong W, Li F, Wang J. Physicians’ perceptions and attitudes toward clinical pharmacy services in urban general hospitals in China. Int J Clin Pharm. 2014;36:547.
46. McCarney R, Warner J, Iliffe S, van Haselen R, Griffin M, Fisher P. The Hawthorne Effect: a randomised, controlled trial. BMC Med Res Methodol. 2007;7(1):30.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.