Back to Journals » Patient Preference and Adherence » Volume 16
Impact of Whole-Layer Barbed Suture Closure on the Postoperative Effect and Aesthetic Satisfaction with Incision After Knee Arthroplasty
Authors Zhou Y ![]() , Chen J, Dong X
, Chen J, Dong X
Received 5 March 2022
Accepted for publication 27 July 2022
Published 10 August 2022 Volume 2022:16 Pages 2041—2049
DOI https://doi.org/10.2147/PPA.S365143
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Naifeng Liu
Yongchun Zhou, Jing Chen, XiangHui Dong
Department of Orthopedic, Shaanxi Provincial People’s Hospital, Xi’an, People’s Republic of China
Correspondence: XiangHui Dong, Department of Orthopedic, Shaanxi Provincial People’s Hospital, 256 # You-yi West Road, Xi’an, Shaanxi, 710068, People’s Republic of China, Email [email protected]
Objective: To evaluate the effect of whole-layer barbed suture for incision closure on the clinical outcome and aesthetic satisfaction of patients with the incision following total knee arthroplasty (TKA).
Materials and Methods: A retrospective analysis was conducted on 94 patients (37 men and 57 women, 50– 84 years old) who underwent a first TKA between May 2018 and April 2021. The enrolled patients were divided into two groups according to the suture mode, with 45 cases (group A) receiving closure of the deep tissue with a barbed suture and intradermal suture of the incision with another barbed suture and 49 cases (group B) receiving closure of the deep tissue with absorbable suture and interrupted suture of the incision with nonabsorbable suture. Further comparisons were performed regarding incision length, suture time, postoperative incision complications, Hollander Wound Evaluation Score (HWES), Hospital for Special Surgery (HSS) knee score, American Knee Society (AKS) score, and Patient and Observer Scar Assessment Scale (POSAS). The clinical effects of the two suture modes in TKA and the patients’ aesthetic satisfaction with the incision were also evaluated at 2 weeks, 3 months and 6 months after the operation.
Results: Compared with group B, group A had higher HWES at 2 weeks after the operation (P < 0.05), shorter suture times (P < 0.05) and lower POSAS scores at 3 and 6 months after the operation (P < 0.05). However, no significant difference was observed between the two groups in incision length, complication rate, HSS or AKS scores (P > 0.05).
Conclusion: Compared with the interrupted suture, the use of whole-layer barbed suture for incision closure after TKA has the advantages of a safe and effective outcome, short operation time, high cosmesis degree of the wound scar and high patient satisfaction.
Keywords: barbed suture, knee arthroplasty, interrupted suture, aesthetic satisfaction of incision
Background
With the improvements in living standards and the development of medical technology, there has been a gradual increase in individuals’ requirements for beauty. To improve the joint function and satisfaction of patients who have undergone joint replacement, an increasing amount of attention is being paid to incision sutures.1 During joint replacement, incision closure is generally achieved by closing the deep tissue (including the articular capsule and subcutaneous tissue) using an absorbable or nonabsorbable suture and performing an interrupted suture of the skin using anastomotic nails or nonabsorbable suture2,3 or by using surgical appliance adhesive and absorbable suture for cosmetic suture.4–6 The use of a nonabsorbable suture is the most common and simple strategy for interrupted suture of the deep tissue, whereas the use of anastomotic nail or nonabsorbable suture is the most common strategy for suturing skin. However, these methods have many disadvantages, such as increased suture knots resulting in an increased risk of infection; prolonged operation time; the need to remove the sutures 10 to 14 days after the operation; and the potential formation of centipede leg–like scars in later stages.7,8 The research findings of Vincent et al9 provide support for these disadvantages. Currently, suturing of deep tissue is usually achieved by using interrupted or over-and-over whip sutures with an absorbable suture. However, this type of suture has several problems, such as the need for assistance during the suturing process, possible foreign-body reaction induced by suture knots, the provision of a parasitic place for bacteria, an increased risk of postoperative infection, postoperative intractable pain and prolonged operation time.10 Meanwhile, absorbable sutures can also be used to achieve cosmetic sutures of the skin.8 Nevertheless, a long incision is required following knee arthroplasty, which is located at the apex of flexion and extension during functional exercise with a large local bearing force. Complete closure and tight suture at all layers with sufficient pulling force are required during suture, which means higher requirements for both suture materials and methods.11,12 Absorbable antibacterial Vicryl and surgical appliance adhesive cannot provide sufficient tension and are prone to exudation or splitting.13 Meanwhile, a nonabsorbable suture may increase the risk of infection by increasing the number of subcutaneous suture knots, incision dehiscence, nonunion and even infection, which can be disastrous. Thus, nonabsorbable sutures are rarely used in the field of joint replacement in the early stage.13
Both patients and doctors unceasingly pursue satisfactory joint function and a beautiful incision postoperatively. At the patient level, a cosmetic suture does not require dressing change or suture removal, thereby fully meeting the beauty and satisfaction requirements of patients. Owing to material limitations, cosmetic suture is still in the stage of continuous exploration and optimisation. In recent decades, with the advancements in materials science, an absorbable barbed suture has been accepted and applied in the fields of plastic surgery14 and gynaecology,15 among others. However, this type of suture is still in the early period of application in the field of orthopaedics and, as reported by most studies, has been applied only in the suturing of deep tissue during joint replacement.16 Because of the previous shortcomings of available materials, this suture type is used less often for suturing skin, mainly because of the fear of incision splitting. Few studies have specifically evaluated the effect of skin closure using a barbed suture on the postoperative outcome of total knee arthroplasty (TKA).17 According to a literature review by Faour et al,16 most studies have used a barbed suture only in deep tissue closure, and only a few studies have compared the complications of barbed sutures and conventional suture in skin closure. Reports evaluating the use of whole-layer barbed sutures for closing the deep tissue and skin and its effect on the patients’ aesthetic satisfaction with the incision are extremely rare. In particular, its safety in TKA remains in doubt.18,19 Therefore, in this study, we used whole-layer barbed sutures to close the deep tissue and skin after TKA to observe the postoperative clinical effect of this operation and patients’ aesthetic satisfaction with the incision.
Materials and Methods
General Data
We conducted a retrospective analysis of 94 patients (37 men and 57 women, aged 50–84 years) who underwent TKA for the first time between May 2018 and April 2021. A total of 45 cases (18 men and 27 women) received a barbed suture to close the deep tissue and intradermal suture of the skin incision with another barbed suture (group A), and 49 cases (19 men and 30 women) received an absorbable suture to close the deep tissue and an interrupted suture of the incision with a nonabsorbable suture (group B).
Inclusion and Exclusion Criteria
The inclusion criteria included the following: (1) patients with primary knee osteoarthritis who met the indications for TKA for the first time, (2) patients with varus and valgus deformity <20°, (3) patients without other limb dysfunction diseases, (4) patients with a body mass index (BMI) < 35 kg/m2 and (5) patients with stable control of common medical diseases. The exclusion criteria were (1) patients with previous knee surgery and trauma, an old local scar, sinus and so forth; (2) patients with a medical history of knee joint tumour or tuberculosis and (3) patients with infection, coagulation dysfunction, and mental illness.
Surgical and Incision Closure Methods
All operations of the studied patients were completed by doctors in the same medical group under the leadership of the same chief physician. All patients received a pneumatic tourniquet at the root of the thigh, spinal anaesthesia and an anterior median incision of the knee joint with a length of about 15–18 cm. The articular capsule was cut open 0.5 to 1.0 cm from the inside of the patella, and the patella was turned outward. The surgeons took care to protect the patellar tendon. The next steps were conventional osteotomy and moulding trial, with the placement of a suitable prosthesis (PS type, LINK, Germany) and a thorough rinse with a disposable pulse (3000-mL normal saline). One drainage tube was placed, and the knee was bent to 60° for suture. The incision length and suture time were recorded for each operation.
In group A, an absorbable suture V-LOC 0# (Covidien) was used to continuously suture the articular capsule from the proximal end to the distal end, with a stitch length of 1–1.5 cm. To prevent reverse folding of the suture, the suture was tightened while suturing. The stitch length was appropriately reduced on the surface of the patella, about 0.8–1 cm. After two stitches were sutured in situ at the distal end, the suture was turned back, and the subcutaneous tissue was sutured continuously, with a stitch length of 1.5–2 cm, followed by cutting off the suture at the same suture level. Finally, for the intradermal suture, an absorbable suture V-LOC 3-0 (Covidien) was used. After skin suture, the maximum flexion angle was tested again. In the case of large incision tension, a local interrupted suture was provided for additional strength. In group B, an absorbable suture Vicryl® 0# (Ethicon®, Johnson & Johnson) was used for interrupted suture of the articular capsule, and an absorbable suture Vicryl® 2-0 (Ethicon®, Johnson & Johnson) was used for interrupted suture of the subcutaneous tissue layer with a stitch length of 1.0 cm. The surgeon aimed to eliminate the slip knot and dead cavity as much as possible during the suture. After suture, an interrupted suture of the skin was performed using the braided nonabsorbable suture MERSILK 3-0 (Ethicon®, Johnson & Johnson), with a stitch length of 1.0 cm. In group A, the suture was removed 14 days after operation for those with local intermittent sutures, and in group B, the suture was removed 14 days after operation.
Postoperative Processing
All patients received the same postoperative treatment, including postoperative antibiotic treatment, analgesia, anticoagulation, principles and methods of wound care and discharge.
Follow-Up Time and Evaluation Indices
The patients were followed up 2 weeks, 3 months and 6 months after the operation. The observational indices were (1) the incision length and suture time (ie time from the beginning of the suture of the articular capsule to the end of the suture); (2) the incidence of incision complications (exudation, swelling, dehiscence, infection, etc.) and Hollander Wound Evaluation Score (HWES), for which the appearance of the wound was evaluated at 2 weeks after the operation;8 (3) the Hospital for Special Surgery (HSS) knee score and the American Knee Society (AKS) score,20,21 for which joint function was evaluated before the operation and at 2 weeks, 3 months and 6 months after the operation; and (4) the Patient and Observer Scar Assessment Scale (POSAS),22 for which the degree of cosmesis of the wound scar was evaluated by both physicians and patients at 3 and 6 months after the operation.
Statistical Analysis
We used SPSS 19.0 for the statistical analysis in this study. Measurement data (age, BMI, incision length, suture time, HSS and AKS scores, POSAS score, etc.) in normal distribution were described using mean ± standard deviation and analysed by the t-test. Counting data (gender, lesion location, concomitant medical diseases, incidence of complications, etc.) were analysed using the χ2 test. P < 0.05 was considered to indicate a statistically significant difference.
Results
General Data
No significant difference was observed between group A and group B in age, gender, BMI, lesion location or concomitant medical diseases (P > 0.05; Table 1).
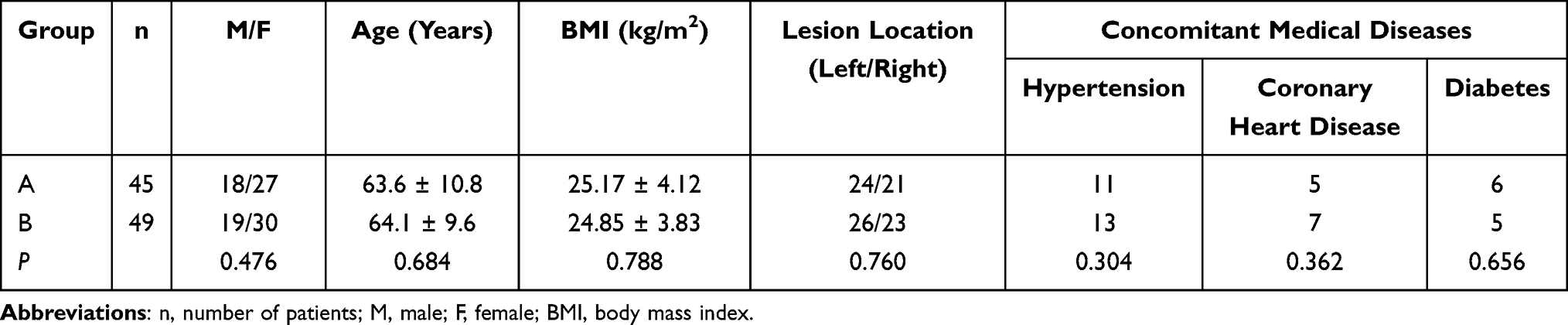 |
Table 1 Comparison of General Data Between Groups |
Incision Length and Closing Time
No significant difference was observed in the length of surgical incision between the two groups (P > 0.05). The closing time was 16.9 ± 3.1 min in group A and 22.7 ± 3.5 min in group B, and the difference between the two groups was statistically significant (P < 0.05; Table 2).
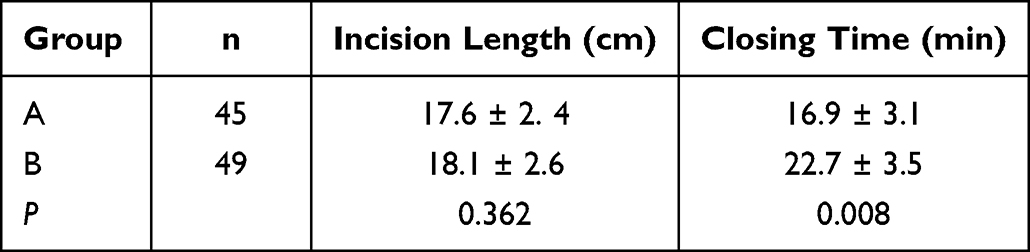 |
Table 2 Comparison of Incision Length and Closing Time Between Groups |
Comparison of the Joint Function Between the Two Groups at Different Times
No significant difference was observed in the preoperative HSS or AKS score between the two groups (P > 0.05; Table 3). Furthermore, the HSS and AKS scores of the two groups showed a significant increasing trend before operation and at 2 weeks, 3 months and 6 months after the operation, but there was no significant difference between groups A and B (P > 0.05; Table 3).
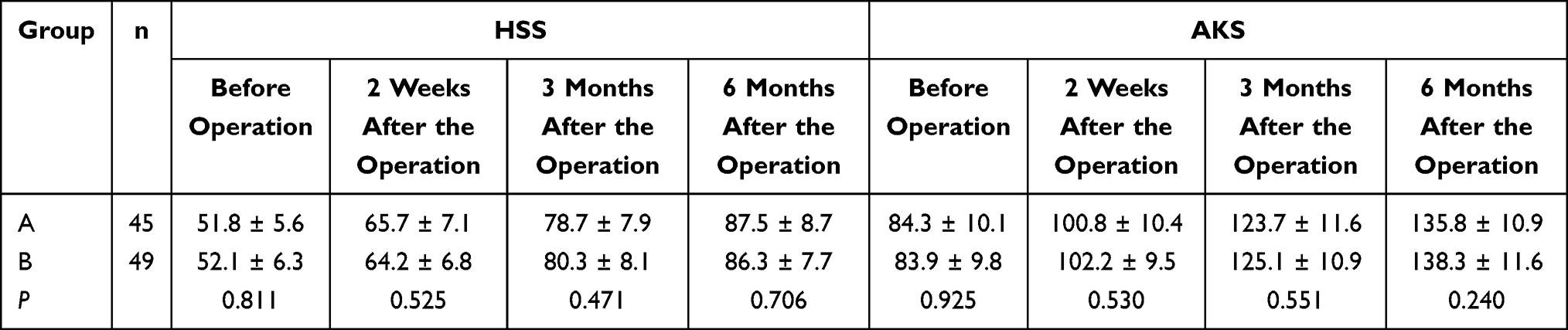 |
Table 3 Joint Function Between the Groups According to the HSS and AKS Scores |
Wound Appearance 2 Weeks After the Operation
Two weeks after the operation, the HWES in group A was 4.77 ± 0.41 points, whereas that in group B was 3.95 ± 0.36 points. The incision healing score in group A was significantly higher than that in group B (P < 0.05).
Aesthetic Satisfaction with Wound Scar 3 and 6 Months After the Operation
In the evaluation of the patients’ aesthetic satisfaction with the postoperative wound scar, the POSAS score of group A was 17.8 ± 4.2 points, whereas that of group B was 21.3 ± 5.7 points at 3 months after the operation, showing a statistically significant difference (P < 0.05; Table 4). Meanwhile, 6 months after the operation, the POSAS score of group A was 13.6 ± 3.1 points, and that of group B was 17.2 ± 4.0 points, with a significant difference between the two groups (P < 0.05; Table 4).
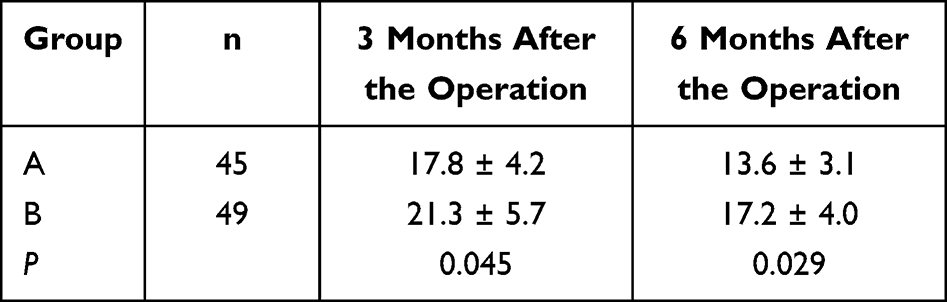 |
Table 4 Cosmesis Score Between Groups According to the POSAS Score |
Postoperative Incision Complications
There were eight cases of incision complications in group A, all of which were mild complications, including four cases of incision exudation, one case of mild incision redness and swelling, two cases of slight dehiscence (length < 15% of incision length) and one case of superficial infection, with no cases of serious complications, such as full layer dehiscence and deep infection. Meanwhile, there were nine cases of incision complications in group B, all of which were mild complications, including six cases of incision exudation, two cases of mild incision redness and swelling and one case of slight dehiscence (2 cm in length); no serious complications (full layer dehiscence and deep infection) were noted. The number of incision exudation cases in groups A and B accounted for 50% and 66.7% of the total number of complications, respectively, with a statistically significant difference (P < 0.05). In addition, the total complication and serious complication rates of group A were 17.8% and 0%, respectively, whereas those of group B were 18.3% and 0%, respectively. No significant difference was observed in the total complication and serious complication rates between the two groups (P > 0.05; Table 5).
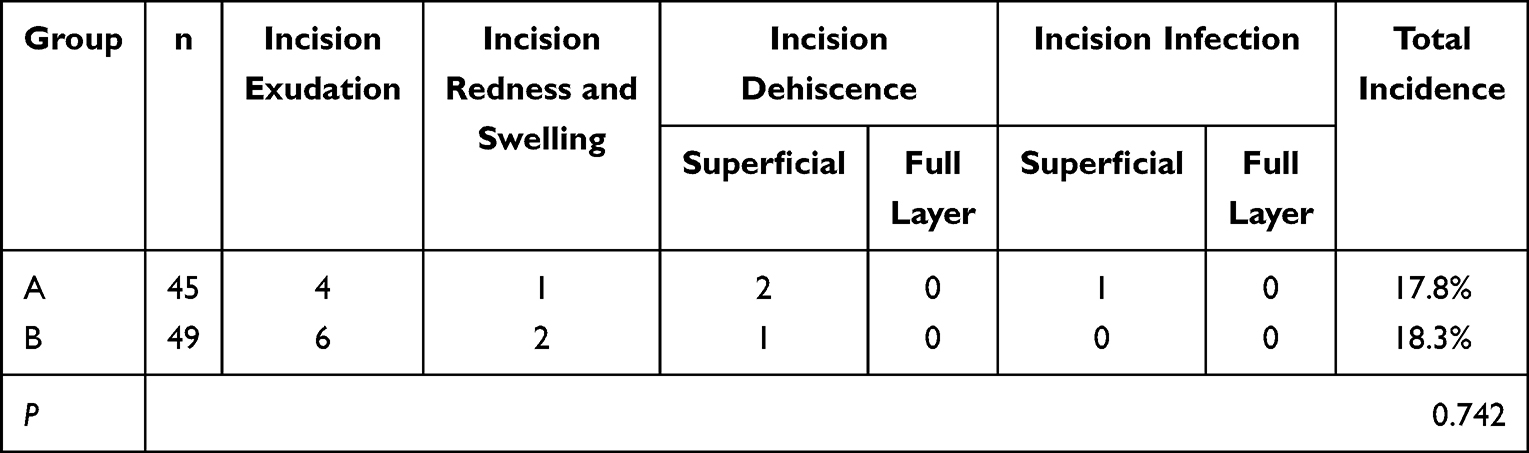 |
Table 5 Incidence of Incision Complications in the Two Groups |
Discussion
Various suture materials and different techniques are used for incision closure in TKA. The common purposes are to shorten the operation time, reduce postoperative complications such as dehiscence and infection, quickly improve joint function, reduce scar formation and improve patient satisfaction. Interrupted suture with a nonabsorbable suture is the most common method with the most simple operation and lowest cost. However, as verified by Vincent et al,9 this technique has numerous disadvantages, such as increased suture knots, increased risk of infection, prolonged operation time, increased hospital stay and cost and formation of centipede leg–like scars in the later stage.7,8 The use of anastomotic nails for suturing results in a poor appearance, requires repeated removal with professional tools and causes obvious pain. In addition, despite the advantage of reducing the formation of scars, the absorbable suture or surgical appliance adhesive is not strong enough and carries a risk of wound dehiscence that requires constant special attention during postoperative functional exercise.13 The TKA incision is located at the apex of knee flexion and extension, and the tension is much higher than that of a general surgical incision, which results in higher requirements for suture materials and methods.11,12 With the development of nonabsorbable sutures and synthetic absorbable sutures, and with the subsequent maturity and promotion of barbed suture materials, these materials have been widely applied in joint replacement surgery by an increasing number of physicians. The barbed suture has been reported to be safe and efficient in operation, and its strength and surrounding tissue reaction were equivalent to those of traditional absorbable sutures.23 In addition, there is no need for knotting, which reduces the difficulty of the operation and significantly improves the speed and quality of the suture.18 In terms of its use in TKA, most studies have applied the barbed suture only for suturing deep tissue.16 As reported in the literature review conducted by Faour et al,16 most studies used a barbed suture only in deep tissue closure, and only a few studies have compared the complications of barbed sutures and conventional suture in skin closure. The main reasons for the low application rate of this suture type are the shortcomings of previous materials and the fear of incision splitting. Moreover, few studies have specifically evaluated the effect of skin closure with a barbed suture on the postoperative outcome of TKA,17 and even fewer studies have explored the effect of deep tissue and skin suture simultaneously using a barbed suture on the postoperative effect and wound scar satisfaction.
The results of our study indicated that the use of whole-layer barbed suture to close the deep tissue and skin not only reduces the operation time without increasing the rate of complications, such as incision dehiscence, but also significantly improves joint function, reduces postoperative scarring and improves patient satisfaction. Traditional suture knotting has potential risks, such as prominent suture knot, subcutaneous palpable keloid, local micro-infarction, suture breakage and slip knot. Meyer et al24 reported that an interrupted suture can produce more knots, increase foreign-body reaction, provide parasitic sites for bacteria and increase the risk of postoperative infection. In their research, Gililland et al25,26 found that the use of an absorbable barbed suture can shorten the suture time by 4–6 min, or 30%, as compared with an interrupted suture that requires knotting. Smith et al27 also reported that the use of a barbed suture can reduce the average suture time by about 9.72 min and save about $550; however, this type of suture is accompanied by an increased incidence and severity of incision-related complications. In addition, Namba et al28 demonstrated that the risk of incision infection increases by 9% with every 15 min of operation time prolongation, suggesting that, theoretically, shortening the operation time can reduce the incidence of incision complications. Currently, whether the use of a barbed suture can increase the risk of potential complications of joint replacement remains controversial. Barbed sutures can provide more uniform tissue tension, thereby reducing the risk of ischaemia; they also have no subcutaneous knots, thus decreasing the possibility of local inflammatory response and sterile abscess, both of which result in a reduced risk of wound complications.29 A prior meta-analysis30 revealed that barbed sutures did not significantly increase the risk of mild or serious complications. In our study, the whole-layer suture time in group A was 16.9 ± 3.1 min, and that in group B was 22.7 ± 3.5 min. When using a barbed suture, the suture time was accelerated by about 6 min. Moreover, the incidence rates of complications were 17.8% and 18.3% in groups A and B, respectively. There was no significant difference between the two groups, which was consistent with the results of previous research.31,32 Furthermore, of the total number of cases with complications, the proportion with incision exudation was 50% in group A and 66.7% in group B. The reason for this result is that the barbs are evenly distributed on the whole suture, and loosening or breaking a single suturing ring has no significant effect on the failure of the whole suture. Previous research also demonstrated that as compared with traditional sutures, the use of barbed sutures can reduce the rate of postoperative wound leakage by 74%.33 In our opinion, the occurrence of incision-related complications may be related to vascular angulation caused by continuous sutures, surgeon learning curves and patients’ own diseases, among others. The application of a barbed suture is in its early stage in orthopaedics, and a learning curve is required as surgeons have little knowledge of its performance, indications and suture skills. Simultaneously, the inappropriate selection of patients might also increase the incidence of complications, such as the long-term use of immunosuppressive drugs in rheumatoid diseases, poor glucose control in diabetes, long-term use of hormones and low body weight. Barbed sutures should be avoided in patients with the aforementioned conditions. For example, Campbell et al25 reported higher rates of infection and overall complications when using barbed sutures in patients with obesity, diabetes or rheumatoid arthritis.
The complete absorption of the absorbable suture Vicryl® takes 2 to 3 months. The barbed suture can be absorbed in a minimum of 3 months after the operation and completely absorbed within 6 months. A previous study reported that the joint range of motion and Knee Society Score (KSS) of the conventional suture group were slightly higher than those of the barbed suture group at 6 weeks and 3 months after the operation, without a statistically significant difference.9 Han et al29 also reported no significant difference in the joint range of motion between the barbed suture group and the traditional suture group in the early (<6 weeks) and middle (<3 months) stages after the operation. This finding is consistent with previous reports,26,31 namely, that there was no obvious difference between the traditional suture and barbed suture in the average extension and flexion as well as the KSS score. In addition, Wang et al found that patients who received a barbed suture within 2 weeks after the operation had a higher visual analogue scale score and poor joint mobility and joint function; however, no significant difference was observed between 6 and 12 weeks after the operation, and the effect of the suture on functional recovery gradually weakened with the reduction of suture absorption and tension. In our study, the HSS and AKS scores of the two groups showed a significant increasing trend according to the observation before operation and at 2 weeks, 3 months and 6 months after the operation but without a statistically significant difference. This suggests that the barbed suture had no significant effect on the recovery of joint function in the early and middle stages. We speculated that the long-term efficacy of the barbed suture would be similar to that of the traditional suture after 6 months of complete absorption. However, this hypothesis requires verification by randomised controlled trials based on long-term follow-up.
According to statistics, the rate of dissatisfaction with TKA is as high as 20% and can be affected by pain, infection, scar appearance, incision and other related complications.34 Clearly, the appearance of a surgical scar is an extremely important part of a patient’s postoperative satisfaction. Patients frequently take the initiative to require an absorbable suture for incision suture. Significantly, a cosmetic suture has distinct advantages in the alignment of the incision and improvement in overall beauty. In the present study, the HWES were 4.77 ± 0.41 points in group A and 3.95 ± 0.36 points in group B, indicating a significantly higher wound-healing score in group A than in group B. This result supports the significant superiority of the barbed suture to the traditional suture in the overall beauty of the incision at 2 weeks after the operation. Similarly, Campbell et al25 reported that an absorbable barbed suture can speed up the time of an intermittent suture that requires knotting by 4–6 min, and the patient satisfaction and cosmetic effect were similar at 6 weeks after the operation. Meanwhile, it has been reported that in patients who received a barbed suture, the width of the incision scar was significantly smaller than in those with an interrupted suture, with a beautiful incision scar and no significant difference in the KSS scores.35 Moreover, some researchers also considered that the barbed suture had a better cosmetic effect and could improve patient satisfaction.17 In this study, we used the POSAS to evaluate patients’ aesthetic satisfaction with the incision at 3 and 6 months after the operation, because the POSAS is the most comprehensive and commonly used scar evaluation scale and is the first scale to comprehensively evaluate the views of both observers and patients. The findings of our study indicated that the POSAS score of group A was significantly higher than that of group B at 3 and 6 months after the operation, suggesting that the barbed suture has obvious advantages in improving the aesthetic satisfaction with the postoperative incision scar. After interrupted suture and suture removal 2 weeks after the operation, the scar will gradually thicken and widen due to the continuous stimulation of knee flexion and extension. The support time of the barbed suture is 2 months. The scar is strong enough at this time, and complete absorption of this suture takes no longer than 6 months. It can produce lasting tension on the skin margin and effectively inhibit scar hyperplasia. After 6 months of follow-up, we found that the patients’ satisfaction with the incision was significantly higher than that of the interrupted suture.
This study also has some limitations, including the small sample size, short follow-up time and lack of analysis of diabetes and other related factors. Further exploration is needed via multicentre research with larger sample size and longer research period.
Conclusion
In the present study, as compared with interrupted sutures, the use of whole-layer barbed sutures for deep tissue and skin incision closure has obvious advantages in shortening the TKA operation time, improving the beauty of the incision scar and increasing the degree of patient satisfaction. In addition, it has no significant impact on the increase in the risk of complications, such as wound dehiscence. The findings in our study may benefit from further discussions and measures that may contribute to the improvement of the appearance of postoperative scars and enhancement of the patients’ degree of satisfaction in the short or medium term.
Abbreviations
TKA, Total knee arthroplasty; HWES, Hollander Wound Evaluation Score; HSS, Hospital for Special Surgery; AKS, American Knee Society; POSAS, Patient and Observer Scar Assessment Scale.
Data Sharing Statement
The datasets supporting the conclusions of this article are included within the article. The raw data can be requested from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Ethical approval from the Ethics Committee of the Shaanxi Provincial People’s Hospital (No. 2021-0127) was obtained for this study. Each author certifies that all investigations were conducted in conformity with ethical principles and the declaration of Helsinki. Written informed consent was obtained from all patients included in the study.
Consent for Publication
Written informed consent was obtained from the patient for the publication of this study.
Acknowledgments
We would like to extend our gratitude to Shaanxi Provincial People’s Hospital, for allowing and facilitating us to conduct the project.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Shaanxi Provincial People’s Hospital Science and Technology Talent Program Project (No.2021YJY-46 and 2021YJY-34). The Shaanxi Provincial People’s Hospital Science and Technology Talent Program Project had no role in the study design, collection, analysis and interpretation of data nor in the writing of the manuscript and in the decision to submit the manuscript for publication.
Disclosure
The authors declare that they have no competing interests.
References
1. Lefevre S, Valois A, Truchetet F. Allergic contact dermatitis caused by Dermabond ®. Contact Dermatitis. 2016;75(4):240–241. doi:10.1111/cod.12597
2. Smith TO, Sexton D, Mann C, et al. Sutures versus staples for skin closure in orthopaedic surgery: meta-analysis. BMJ. 2010;340:c1199. doi:10.1136/bmj.c1199
3. Khan RJ, Fick D, Yao F, et al. A comparison of three methods of wound closure following arthroplasty: a prospective, randomised, controlled trial. J Bone Joint Surg Br. 2006;88(2):238–242. doi:10.1302/0301-620X.88B2.16923
4. Eggers MD, Fang L, Lionberger DR. A comparison of wound closure techniques for total knee arthroplasty. J Arthroplasty. 2011;26(8):1251–1258. doi:10.1016/j.arth.2011.02.029
5. Wang YF, Liu HM, Liao YJ, et al. Effects of new type barbed suture on early function and pain after primary total knee replacement. Chin J Joint Surg. 2018;12(06):762–767.
6. Kang Y, Zhou ZK, Yang HL, et al. A guideline on the management of incisions for the enhanced recovery after orthopedic surgery in. China Chin J Bone Joint Surg. 2018;11(01):3–10. doi:10.3969/j.issn.2095-9958.2018.01.003
7. Wyles CC, Jacobson SR, Houdek MT, et al. The chitranjan ranawat award: running subcuticular closure enables the most robust perfusion after TKA: a randomized clinical trial. Clin Orthop Relat Res. 2016;1(474):47–56. doi:10.1007/s11999-015-4209-x
8. Wang Y, Wu D, Li J, et al. Comparison of skin cosmetic suture and traditional method for wound closure in total knee arthroplasty. Chin J Bone Joint Surg. 2019;12(02):117–121. doi:10.3969/j.issn.2095-9958.2019.02.08
9. Chan VWK, Chan PK, Chiu KY, et al. Does barbed suture lower cost and improve outcome in total knee arthroplasty? A randomized controlled trial. J Arthroplasty. 2017;32(5):1474–1477. doi:10.1016/j.arth.2016.12.015
10. Yang SS, Zhang C, Yao Y, et al. Application of knot - free barb suture in deep tissue suture of knee replacement. J Med Res. 2021;50(02):117–121.
11. Yang LQ, Ma C, Du S. Pain management in perioperative period of total knee arthroplasty. Orthoped J China. 2017;25(03):247–250. doi:10.3977/j.issn.1005-8478.2017.03.12
12. Lostak J, Gallo J, Slavik L, et al. Monitoring of fibrinolytic system activity with plasminogen, D-dimers and FDP in primary total knee arthroplasty (TKA) after topical, intravenous or combined administration of tranexamic acid. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2020;164(2):168–176. doi:10.5507/bp.2019.034
13. Li ZY, Shi B. Tang ST, et al. Clinical application of reinforced continuous intradermal suture in Hip and knee joint replacement incisions.Chinese. J Bone Joint Surg. 2019;12(10):782–785, 795. doi:10.3969/j.issn.2095-9958.2019.10.08
14. Duscher D, Pollhammer MS, Wenny R, et al. Barbed sutures in body-contouring: outcome analysis of 695 procedures in 623 patients and technical advances. Aesthetic Plast Surg. 2016;40(6):815–821. doi:10.1007/s00266-016-0701-2
15. Abraham C. A randomized clinical trial of knotless barbed suture vs conventional suture for closure of the uterine incision at cesarean delivery. Am J Obstet Gynecol. 2018;219(2):220–221. doi:10.1016/j.ajog.2018.04.028
16. Faour M, Khlopas A, Elmallah RK, et al. The role of barbed sutures in wound closure following knee and hip arthroplasty: a review. J Knee Surg. 2018;31(9):858–865. doi:10.1055/s-0037-1615812
17. Vieira RB, Waldolato G, Fernandes JS, et al. Evaluation of three methods of suture for skin closure in total knee arthroplasty: a randomized trial. BMC Musculoskelet Disord. 2021;22(1):747. doi:10.1186/s12891-021-04627-5
18. Meena S, Gangary S, Sharma P, et al. Barbed versus standard sutures in total knee arthroplasty: a meta-analysis. Eur J Orthop Surg Traumatol. 2015;25(6):1105–1110. doi:10.1007/s00590-015-1644-z
19. Austin DC, Keeney BJ, Dempsey BE, et al. Are barbed sutures associated with 90-day reoperation rates after primary TKA? Clin Orthop Relat Res. 2017;475(11):2655–2665. doi:10.1007/s11999-017-5474-7
20. Rames RD, Haynes J, Hellman M, et al. Impact of tourniquet strategy on perioperative results of modern TKA. J Knee Surg. 2020;33(10):987–991. doi:10.1055/s-0039-1688919
21. Millar JS, Lawes CM, Farrington B, et al. Incidence of venous thromboembolism after total Hip, total knee and Hip fracture surgery at Waitemata District Health Board following a peer-reviewed audit. N Z Med J. 2020;133(1511):52–60.
22. Nicholas RS, Falvey H, Lemonas P, et al. Patient-related keloid scar assessment and outcome measures. Plast Reconstr Surg. 2012;129(3):648–656. doi:10.1097/PRS.0b013e3182402c51
23. Song Y, Tang QH, Zhou YX. Comparison of standard suture vs barbed suture for closing the porcine knee joint: evaluation of biomechanical integrity and permeability. J Arthroplasty. 2018;33(3):903–907. doi:10.1016/j.arth.2017.10.008
24. Meyer Z, Ricci WM. Knee extensor mechanism repairs: standard suture repair and novel augmentation technique. J Orthop Trauma. 2016;30(Suppl 2):S30–S31. doi:10.1097/BOT.0000000000000604
25. Campbell A, Patrick J, Liabaud B, et al. Superlìcial wound closure complications wilh barbed sutures following knee arthroplasty. J Arthroplasty. 2014;5(29):966–969. doi:10.1016/j.arth.2013.09.045
26. Gililland JM, Anderson LA, Barney JK, et al. Barbed versus standard sutures for closure in total knee arthroplasty: a multicenter prospective randomized trial. J Arthroplasty. 2014;29(9 Suppl):135–138. doi:10.1016/j.arth.2014.01.041
27. Smith EL, DiSegna ST, Shukla PY, et al. Barbed versus traditional sutures: closure time, cost, and wound related outcomes in total joint arthroplasty. J Arthroplasty. 2014;29(2):283–287. doi:10.1016/j.arth.2013.05.031
28. Namba RS, Inacio MC, Paxton EW. Risk factors associated with deep surgical site infections after primary total knee arthroplasty: an analysis of 56,216 knees. J Bone Joint Surg Am. 2013;95(9):775–782. doi:10.2106/JBJS.L.00211
29. Han Y, Yang W, Pan J, et al. The efficacy and safety of knotless barbed sutures in total joint arthroplasty: a meta-analysis of randomized-controlled trials. Arch Orthop Trauma Surg. 2018;138(10):1335–1345. doi:10.1007/s00402-018-2979-9
30. Borzio RW, Pivec R, Kapadia BH, et al. Barbed sutures in total Hip and knee arthroplasty: what is the evidence? A meta-analysis. Int Orthop. 2016;40(2):225–231. doi:10.1007/s00264-015-3049-3
31. Gililland JM, Anderson LA, Sun G, et al. Perioperative closure-related complication rates and cost analysis of barbed suture for closure in TKA. Clin Orthop Relat Res. 2012;470(1):125–129. doi:10.1007/s11999-011-2104-7
32. Shermak MA. The application of barbed sutures in body contouring surgery. Aesthet Surg J. 2013;33(3 Suppl):72S–75S. doi:10.1177/1090820X13499915
33. Nett M, Avelar R, Sheehan M, et al. Water-tight knee arthrotomy closure: comparison of a novel single bidirectional barbed self-retaining running suture versus conventional interrupted sutures. J Knee Surg. 2011;24(1):55–59. doi:10.1055/s-0031-1275400
34. Liang CB. Research Progress on Influencing Factors of patient satisfaction after total knee arthroplasty. J Clin Med Pract. 2017;21(08):231–234. doi:10.7619/jcmp.201708078
35. Dai Y, Bolch C, Jung A, et al. Accuracy and precision in resection alignment: insights from 10,144 clinical cases using a contemporary computer-assisted total knee arthroplasty system. Knee. 2020;27(3):1010–1017. doi:10.1016/j.knee.2020.02.024
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.