Back to Journals » Clinical Optometry » Volume 17
Impact of Wearing Defocus Incorporated Multiple Segments Spectacle Lenses for 12 Months on Accommodation and Binocular Functions in Myopic Children
Authors Norazman FNN, Mohd-Ali B ![]() , Syed Mohd Dardin SF
, Syed Mohd Dardin SF ![]() , Mohamad Shahimin M
, Mohamad Shahimin M ![]() , Mohamad Fadzil N, Mohd Saman MN
, Mohamad Fadzil N, Mohd Saman MN
Received 6 March 2025
Accepted for publication 2 October 2025
Published 15 October 2025 Volume 2025:17 Pages 327—338
DOI https://doi.org/10.2147/OPTO.S526690
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Mr Simon Berry
Fatin Nur Najwa Norazman,1,2 Bariah Mohd-Ali,1 Syarifah Faiza Syed Mohd Dardin,1,3 Mizhanim Mohamad Shahimin,1 Norliza Mohamad Fadzil,4 Mohd Norhafizun Mohd Saman1
1Optometry and Vision Science Program, Research Centre for Community Health (Reach), Faculty of Health Sciences, Universiti Kebangsaan Malaysia, Kuala Lumpur, Malaysia; 2Centre for Optometry Studies, Faculty of Health Sciences, Universiti Teknologi MARA Cawangan Selangor, Kampus Puncak Alam, Selangor, 42300, Malaysia; 3Optometry Service, Allied Health Science Division, Medical Programme, Ministry of Health, Putrajaya, Malaysia; 4Optometry and Vision Science Program, Centre for Rehabilitation and Special Needs Study (Icarehab), Faculty of Health Sciences, Universiti Kebangsaan Malaysia, Kuala Lumpur, Malaysia
Correspondence: Bariah Mohd-Ali, Optometry and Vision Science Program and Centre for Community Health, Faculty of Health Science, Universiti Kebangsaan Malaysia, Jalan Raja Muda Abdul Aziz, Kuala Lumpur, 50300, Malaysia, Tel +60 39 289 7602, Email [email protected]
Introduction: Spectacle lens design for myopia control incorporates either lenslet or diffusion technology to slow down the eye growth, which may impact the binocular vision functions of a myopic child. This study aimed to investigate the changes in accommodation and binocular functions in myopic children over 12 months wear of myopia control spectacle lenses.
Methods: 21 myopic children aged 7– 12 years were prescribed with Defocus Incorporated Multiple Segments (DIMS) lenses and assessed at baseline, 1, 3, 6, 9, and 12 months. The parameters measured were refractive error, axial length (AL), visual acuity (VA), accommodative lag (LA), amplitude of accommodation (AA), negative/positive relative accommodation (NRA/PRA), stereoacuity, near point of convergence (NPC), phoria, negative/positive fusional vergence (NFV/PFV), and accommodation convergence per accommodation ratio (AC/A).
Results: Mean spherical equivalent (SE) and AL increase from − 2.90 ± 1.15 D and 24.51 ± 0.99 mm to − 3.19 ± 1.25 D and 24.60 ± 0.97 mm at 12 months respectively. Visual acuity (VA) significantly improved (p < 0.001) in both high-contrast and low-contrast conditions at distance and near. Regarding accommodation and binocular functions, significant improvements were observed in lag of accommodation (LA), stereoacuity and gradient AC/A ratio (p < 0.001). The NPC reduced slightly but was still within normal limits. Distance and near phoria shifted toward esophoria with changes less than 1 PD. Additionally, distance NFV and near PFV recovery points increased significantly.
Conclusion: This study demonstrated insignificant changes in accommodation and binocular functions in myopic children after 12 months of wearing DIMS lenses. However, the absence of a control group limits causal interpretation, as observed changes may be influenced by natural development, repeated testing, or regression to the mean. Further research with controlled designs is warranted to clarify these effects.
Keywords: myopic schoolchildren, myopia control spectacle, accommodation, binocular function
Introduction
Myopia has emerged as a significant global public health concern, with projections suggesting that nearly 50% of the world’s population could be affected by 2050.1 The increasing prevalence of myopia is particularly alarming among children, especially in East Asian countries. The myopia prevalence has been reported to reach 85.6% among children aged 6–12 years in China, 77% in Taiwan, 62.2% in Singapore, and 36.2% in Hong Kong.2–5 A recent meta-analysis of 276 studies involving over 5.4 million participants from 50 countries further demonstrated a steady global increase in myopia prevalence, rising from 24.3% in 1990 to 35.8% in 2023.6 This rapid increase of myopia prevalence is concerning because progressive myopia, if left uncontrolled, can lead to high myopia, which significantly increases the risk of sight-threatening complications such as retinal detachment, glaucoma, and myopic maculopathy.7–9
One of the significant risk factors for myopia progression is hyperopic defocus, a condition where light focuses behind the retina, causing a blurred retinal image and often resulting from high accommodative demands and prolonged near-work activities. These visual tasks, such as reading, writing, and excessive screen time, could cause strain on the accommodative system and disrupt the synergistic relationship between the accommodation and vergence systems.10–12 When the eye struggles to maintain clear focus while doing near work, it often results in blurred retinal images due to unstable accommodative response. This persistent retinal blur due to hyperopic defocus, signals the eye to grow longer to improve focus, leading to myopia progression.13 Over time, excessive axial elongation increases the risk of developing high myopia and associated ocular complications. These potential risks of visual impairment emphasize the need for effective myopia control strategies to slow down myopia progression and protect long-term eye health.
Various approaches have been introduced to control myopia progression, including optical interventions, pharmacological agents, and behavioral modifications. Among them, atropine, orthokeratology, and multifocal contact lenses have all shown strong efficacy in controlling myopia progression, with reductions of up to 50–60% reported in clinical studies.14–17 However, both pharmacological and contact lens interventions may carry side effects such as conjunctivitis, keratitis, photophobia, allergies, or systemic toxicity.18,19 Spectacles, being non-invasive and safe, remain the most practical treatment option for children.
Myopia control spectacle lenses incorporates either lenslet or diffusion technology to control the growth of axial length.20 Defocus Incorporated Multiple Segments (DIMS) lenses were designed with a 9 mm diameter central optical zone to correct the distance refractive error, and are surrounded by 33 mm concentric multiple small segments (lenslets) with +3.50 diopters (D) addition power in the mid-peripheral zone, which aim to slow axial elongation while simultaneously providing clear vision. Previous studies have demonstrated the efficacy of DIMS lenses in reducing 52% of myopia progression and 62% of axial elongation in children over two years of study period compared to single vision lenses.21 This myopia control effect was sustained in the third- and six-years following lens wear, with no significant adverse effects reported.22,23
While the effectiveness of DIMS lenses in slowing myopia progression is well-documented, their impact on accommodation and binocular functions remains uncertain. Myopia control interventions, including orthokeratology (OK) and multifocal (MF) lenses, have been shown to cause various responses in the accommodation and vergence systems, with some interventions inducing significant changes in these functions. This raises concerns about potential disruptions to visual comfort and performance following DIMS lens wear. The dual-power design of DIMS lenses, incorporating +3.50 D lenslets, has the potential to disrupt accommodation and vergence, particularly due to under-accommodation when viewing through these lenslets.10 However, findings from a study on Chinese children in Hong Kong suggest that DIMS lenses successfully control myopia progression without causing significant disruptions to binocular functions.21,24 Despite the overall stability in binocular vision with DIMS lens wear, some accommodative changes have been reported. Specifically, two years of DIMS lens wear was associated with a reduction in amplitude of accommodation (AA),24 whereas OK lenses have been shown to increase AA.25 Additionally, studies on MF, OK, and DIMS lenses have consistently reported a reduction in accommodative lag (LA), suggesting an improvement in accommodative response.24,26,27 However, no significant changes in phoria have been observed with OK, DIMS, or MF lens wear.24,28,29 These variations effects of myopia control strategies on accommodation and vergence parameters, highlight the need for further research to comprehensively evaluate overall binocular functions.
Thus, this study aimed to evaluate the 12 months effect of DIMS lens wear on myopia progression, binocular vision, and accommodative functions among Malay myopic primary schoolchildren. All parameters were measured while participants were wearing their DIMS spectacle lenses, representing the visual experience of actual lens wear. This approach offers a more accurate reflection of patient outcomes in daily life and provides clinicians with stronger evidence to support informed, evidence-based decisions when prescribing DIMS lenses.
Material and Methods
Study Design and Participants
The Myopia Control Study in Kuala Lumpur (MyCOSKL) is an ongoing longitudinal study that evaluates myopia progression following DIMS lens wear among Malay primary schoolchildren. In this study, the effects of myopia-control spectacle lens wear on accommodation and binocular functions were evaluated at baseline and after the spectacle lenses intervention.30 The data collection and follow-up assessments were conducted over a 12-month period to evaluate longitudinal changes in accommodative and binocular functions with DIMS lens wear.
This paper specifically reports on changes in accommodation and binocular vision parameters at baseline, as well as at 1, 3, 6, 9, and 12 months of DIMS spectacle lens wear. Based on sample size calculations, 24 myopic children were enrolled in this study. The sample size was determined using G*Power software (version 3.1.9.4) for an ANOVA repeated measures statistical test with an alpha level of 0.05. A minimum of 19 subjects was required to achieve 80% power in detecting a 0.25 D difference in visual function and accommodation measurements. To account for an estimated 20% dropout rate, the study aimed to recruit at least 24 participants.
The eligible criteria for the MyCOSKL study were Malay primary school students, aged 7 to 12 years, with spherical equivalent (SE) between −0.50 D and −5.00 D, astigmatism and anisometropia of less than 1.50 D, and a monocular best-corrected visual acuity (VA) of 6/6 or better. Prior to enrolment, none had undergone any myopia control treatment, and all participants were free from ocular or systemic abnormalities as well as binocular vision disorders. Participants were prescribed with DIMS spectacle lenses and were instructed to wear them at all times, with a minimum requirement of 10 hours per day. All assessments were conducted while the participants were wearing their DIMS lenses.
This study was carried out at the Optometry Clinic, Faculty of Health Sciences, Universiti Kebangsaan Malaysia, Kuala Lumpur Campus, following ethical approval from the Human Subjects Ethics Subcommittee of Universiti Kebangsaan Malaysia (UKM PPI/111/8/JEP-2020-667). The study complied with the principles outlined in the Declaration of Helsinki, and informed consent was obtained from both the participants and their parents before the study commenced.
Study Procedures
Refraction and Axial Length
This study assessed the changes in refraction and axial length (AL) to monitor myopia progression. The refraction was measured following cycloplegia to ensure accuracy. Two drops of 1% cyclopentolate were instilled in each eye at a five-minute interval, and measurements were taken 30 minutes later. Cycloplegic autorefraction was performed using the Shin-Nippon NVision-WAM 5500 open-field autorefractor (Ajinomoto Trading Inc., Tokyo, Japan), followed by subjective refraction. The spherical equivalent refraction (SER) was determined by combining the spherical component with half of the cylindrical value. Axial length (AL) was measured using the Lenstar LS900 (Haag-Streit AG, Switzerland), with the final value derived from the average of five consecutive measurements for each eye.
Visual Acuity
Visual acuity (VA) assessment was conducted for both distance and near vision using standardized LogMAR charts. Distance high-contrast (100% contrast) VA (HCVA) and low contrast (10%) VA (LCVA) were measured with the LogMAR ETDRS chart (Precision Vision Inc., Woodstock, IL, USA) placed on an illuminated cabinet at 4 m, while near VA was assessed at 40 cm using the Mixed Contrast European-Wide Near Vision Card (Precision Vision Inc., Woodstock, IL, USA). Each letter on the chart corresponded to a logMAR value of 0.02. Participants were instructed to read the letters starting from the largest line until they misread three or more letters in a row. VA measurements were performed under standardized room illumination (500 cd/m²) and recorded both monocularly and binocularly.
Accommodation and Binocular Functions
The accommodation and binocular functions tests were administered in a structured sequence to maintain data accuracy and minimize visual fatigue. The evaluated parameters included lag of accommodation (LA), stereoacuity, near point of convergence (NPC), monocular and binocular amplitude of accommodation (AA), horizontal phoria at distance and near, negative and positive relative accommodation (NRA/PRA), as well as fusional vergence at both distances. All measurements were performed while the participants wore their best-corrected prescription to ensure reliable results.
Accommodative response was assessed using an open-field autorefractor (Shin-Nippon NVision-WAM 5500; Ajinomoto Trading Inc., Tokyo, Japan) while participants viewed a 6/9 letter target binocularly at 40 cm. The lag of accommodation was then calculated as the difference between the measured accommodative response and the accommodative stimulus (2.50 D).24,30
Stereoacuity was evaluated using the Frisby stereotest (Clement Clarke International Ltd., Haag Streit UK Ltd., Harlow, Essex), which allows for stereopsis evaluation without the need for additional filter glasses. The test consisted of three transparent plates with varying thicknesses of 6 mm, 3 mm, and 1.5 mm, each containing four squares. Only one of these squares featured a circular target printed on the opposite side, creating a real-depth effect. Participants were instructed to identify the square in which the circle appeared to stand out stereoscopically. Their responses were recorded in seconds of arc (arcsec) to quantify their level of stereoacuity.
The NPC, monocular, and binocular AA were assessed using the Royal Air Force (RAF) ruler. For NPC measurement, participants fixated on a small circle target as the examiner gradually moved it toward their nose. The NPC distance (in cm) was determined when the participant either reported double vision or when the examiner observed an eye deviation. The push-up method was used to measure both monocular and binocular AA. Participants were instructed to keep an N5 word target clear while the examiner slowly moved the chart towards them. The measurement was recorded in diopters when the participant first experienced a sustained blur, even after blinking. Each test was performed three times, and the average value was used for analysis.
Horizontal distance and near phoria were assessed using Howell phoria cards positioned at 3 m and 33 cm, respectively. To determine the magnitude and direction of the phoria, a 6-prism diopter (PD) base-down was placed over the right eye, and participants were asked to report the arrow’s pointing position on the chart. Esophoria values, represented by odd numbers in the yellow box, were recorded as positive, while exophoria values, shown as even numbers in the blue box, were recorded as negative. Phoria measurements were repeated at near with a +2.00 D lens added to both eyes. The AC/A ratio was determined using the gradient method by calculating the difference between the near phoria and the near phoria with the +2.00 D lens.
Fusional vergence was assessed in free space using a prism bar, with base-out prisms used for positive fusional vergence (PFV) and base-in prisms for negative fusional vergence (NFV). The prism strength was increased gradually until participants reported the “break point” where they could no longer maintain single vision, followed by the “recovery point” where single vision was regained. Measurements were taken at both distance and near with 0.2 logMAR target, with NFV tested before PFV to minimize prism adaptation. Due to the young age of the participants, “blur point” measurements were excluded to ensure result reliability. Each test was conducted three times, and the average value was recorded in PD.
Negative relative accommodation (NRA) was measured by introducing plus lenses in 0.25 D increments while participants focused on a 0.2 logMAR target at a distance of 40 cm. The process continued until the participant reported sustained blur, at which the total amount of plus lenses added was recorded. Similarly, positive relative accommodation (PRA) was evaluated using the same method but with minus lenses, and the total amount of minus lenses added was recorded. To minimize any potential influence on accommodation, NRA was assessed before PRA.
Statistical Analysis
Statistical analyses were performed using SPSS software version 21.0 (SPSS Inc., Chicago, IL). The normality of data distribution was assessed using Shapiro–Wilk test. For normally distributed data, repeated measures analysis of variance (RM-ANOVA) was applied to evaluate differences over time, while the Friedman test was used for non-normally distributed data. A p-value of less than 0.05 was considered statistically significant. In cases where RM-ANOVA or the Friedman test indicated a significant difference, post-hoc pairwise comparisons or the Wilcoxon signed-rank test with Bonferroni correction were performed, with a significance threshold of p < 0.008 for comparisons between visits.
Results
Baseline Demographic Data
A total of 24 myopic children aged 7 to 12 years were initially enrolled in the study and prescribed DIMS spectacle lenses. However, 3 participants were excluded from the analysis as they did not meet the requirement of wearing the lenses for a minimum of 10 hours per day. As a result, data from 21 participants (mean age: 9.90 ± 1.45 years) were included in the final analysis. Among them, 5 (24%) were male, and 16 (76%) were female. A post-hoc power analysis based on the final sample confirmed that the study retained 86% power, indicating sufficient statistical strength to detect meaningful differences in the targeted visual function parameters.
A comparison of monocular data between the right and left eyes showed no statistically significant differences (p > 0.05) and demonstrated a strong and significant relationship for cycloplegic SE refractive power (r = 0.94, p < 0.001) and AL (r = 0.98, p < 0.001). As a result, only data from the right eye were included in the statistical analysis. The mean SE before wearing DIMS lenses was −2.90 ± 1.15 D, and AL was 24.51 ± 0.99 mm.
Myopia Progression
After 12 months of wearing DIMS spectacle lenses, there was a significant progression in myopia, as indicated by changes in SE and AL. The cycloplegic refractive error increased by −0.29 ± 0.41 D over the study period (F2.4,48.9 = 3.48, p = 0.03), with a statistically significant difference (p < 0.05) observed at 12-month lens wear compared to baseline. Additionally, AL showed a significant elongation of 0.08 ± 0.15 mm over 12 months (t20 = 2.47, p = 0.023). Detailed changes in SE and AL across the study period are presented in Figure 1.
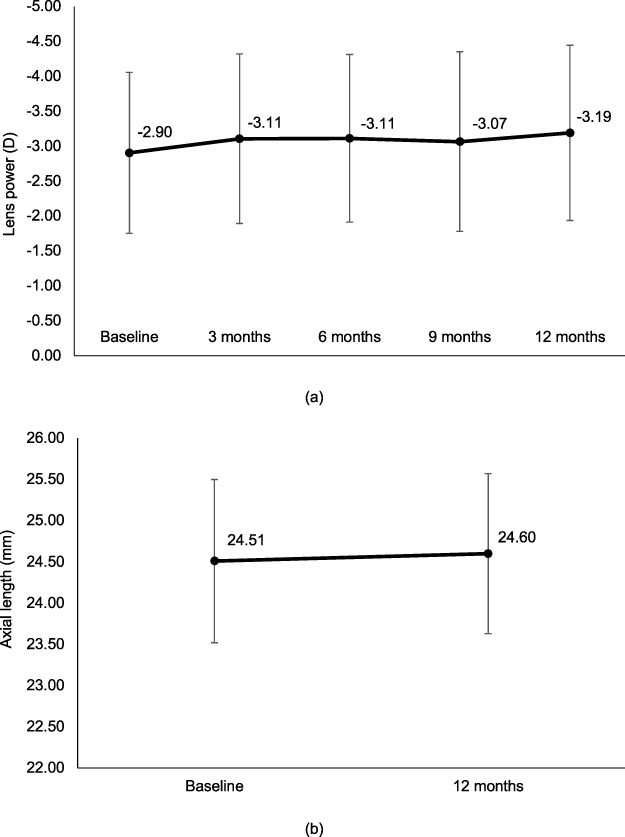 |
Figure 1 Cycloplegic refraction (a) and axial length (b) changes over 12 months wearing DIMS spectacle lenses. |
Visual Acuity Changes
Significant improvements in both distance and near VA were observed over the study period (Table 1). At 4 m, HCVA improved by approximately one line after 12 months compared to baseline for both monocular (F5,100 = 17.59, p < 0.001) and binocular (F3.4,68.4 = 25.76, p < 0.001). Similarly, monocular LCVA (F3,59.9 = 8.06, p < 0.001) and binocular LCVA (F5,100 = 9.18, p < 0.001) also improved significantly over time. The improvements in monocular and binocular HCVA at 4 m became statistically significant (p < 0.05) from the third month onward, whereas LCVA improvements were evident from the sixth month. Near VA at 40 cm also improved significantly for monocular HCVA (F3.4,67.2 = 5.45, p = 0.001) and binocular HCVA (F5,100 = 11.13, p < 0.001), as well as monocular LCVA (F3.4,67 = 8.96, p < 0.001) and binocular LCVA (F3.4,68.1 = 9.59, p < 0.001). All near VA improved significantly (p < 0.05) from the sixth month of lens wear onward compared to baseline.
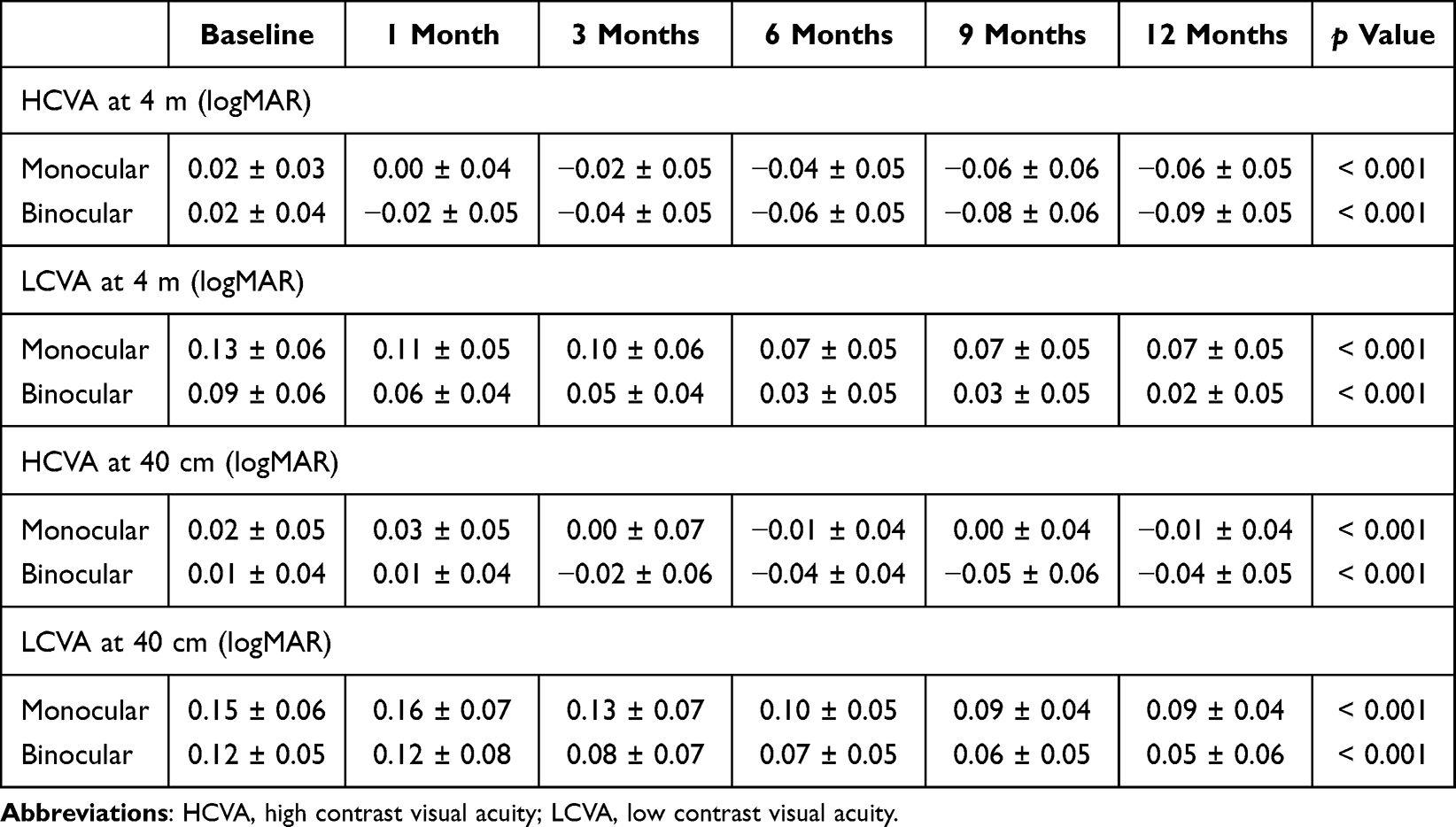 |
Table 1 Visual Acuity Changes Over 12 months Wearing DIMS Spectacle Lenses (n=21) |
Accommodation and Binocular Functions Changes
Table 2 shows the changes in accommodation and binocular functions parameters over 12 months. For accommodation function, only LA demonstrated a statistically significant change (F2.5,50.3 = 3.13, p = 0.04), with an overall decrease of 0.20 ± 0.31 D after 12 months of DIMS lens wear. However, no significance difference was observed between visits. Meanwhile, monocular AA (F3.1,61.2 = 0.65, p = 0.59), binocular AA (F3.2,63.7 = 1.66, p = 0.18), NRA (F2.5,50 = 1.37, p = 0.26), and PRA (F2.7,53.2 = 1.97, p = 0.14) did not show significant changes throughout the study period. Although binocular AA showed an initial decline in the first month of lens wear, it increased in the third month and remained stable until the end of the study.
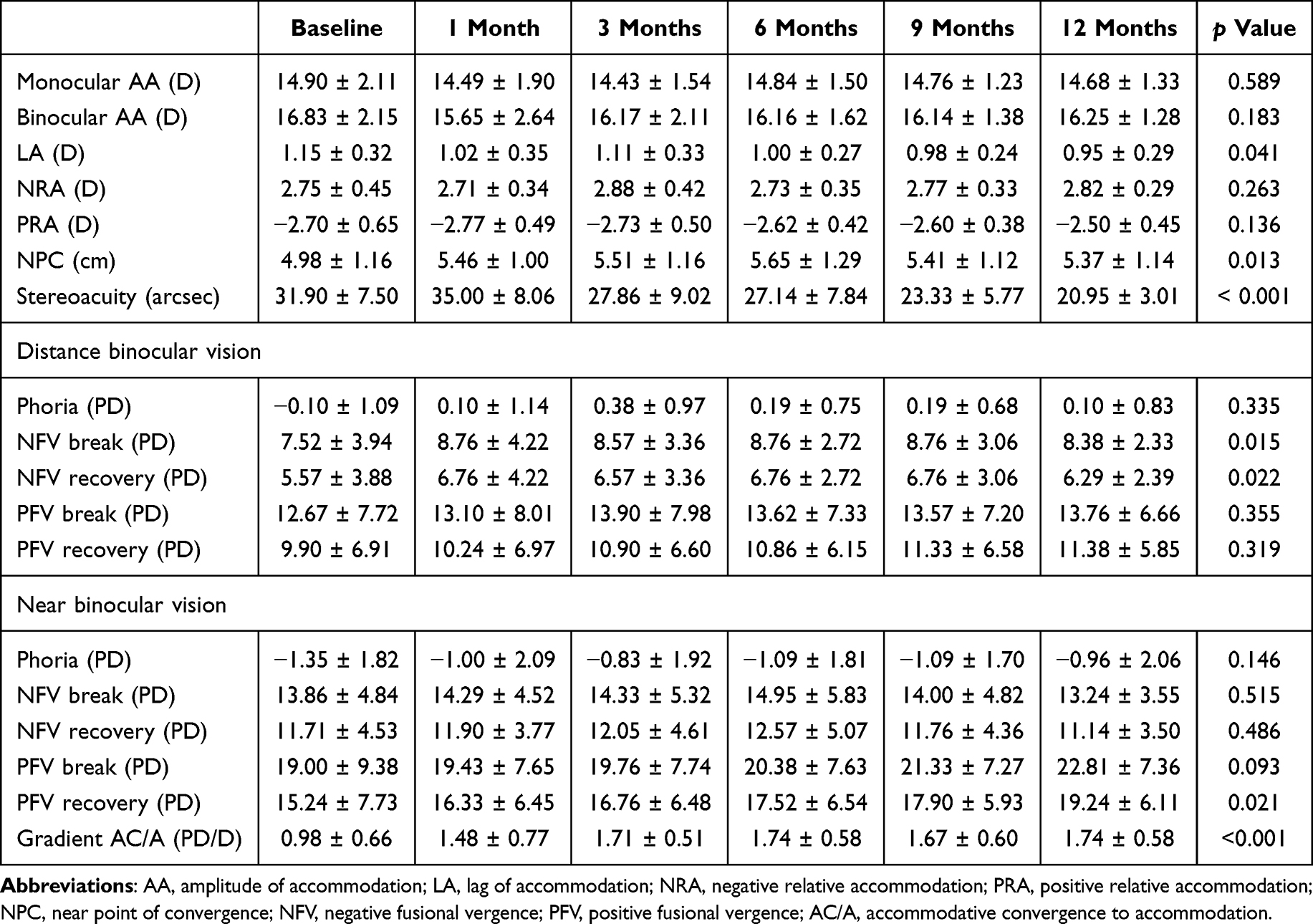 |
Table 2 Binocular Vision and Accommodation Changes Over 12 months Wearing DIMS Spectacle Lenses (n = 21) |
For binocular functions, stereoacuity significantly improved after 12 months of wearing DIMS lenses (χ25 = 52.84, p < 0.001). A transient decreased in stereoacuity was noted after one month, but subsequent improvements were observed. Post-hoc analysis using the Wilcoxon test with Bonferroni correction revealed a significant improvement in stereoacuity by the third month compared to the first month (p = 0.008), with a mean difference of 7.14 ± 10.44 arcseconds. The NPC also showed a significant increase over 12 months of DIMS lens wear (F3.2,63 = 3.79, p = 0.01), with an overall increase of 0.38 ± 0.92 cm compared to baseline. However, no significant differences were detected between visits (p > 0.05). Phoria values at both distance (F2.7,53.6 = 1.15, p = 0.34) and near (F3.1,62.2 = 1.68, p = 0.15) remained unchanged over the 12-month study period. A significant increase in the gradient AC/A ratio was observed with +2.00 DS lenses over 12 months of DIMS lens wear (F3.5,69.6 = 7.15, p < 0.001), with the first notable change occurring at three months (p = 0.002). Additionally, significant increase were found in some fusional vergence parameters, including distance NFV break point (χ25 = 14.08, p = 0.02), distance NFV recovery point (χ25 = 13.19, p = 0.02), and near PFV recovery point (χ25 = 13.24, p = 0.02). However, no significance difference was observed between visits (p > 0.008). Other fusional vergence measures, such as distance PFV break and recovery points, near NFV break and recovery points, and near PFV break point, showed no significant changes over the study period (p > 0.05).
Discussion
This study examined the impact of wearing DIMS spectacle lenses on accommodation and binocular functions among myopic Malay schoolchildren. The findings indicate that wearing DIMS lenses for 12 months effectively controlled myopia progression without disrupting binocular vision balance, with recorded SE progression after 12 months was −0.29 ± 0.41 D and AL elongation was 0.08 ± 0.15 mm. Although significant changes were observed in several accommodation and binocular functions, such as receded NPC and improvement in LA, stereoacuity, AC/A ratio, distance NFV and near PFV, these changes remained within normal clinical limits.31
These results are aligned with previous research by Lam et al21,23,24 which reported no adverse effects on visual functions such as VA, phoria, AA, LA and stereopsis following long-term DIMS lens wear. However, these prior studies had limitations in the range of accommodation and binocular functions assessed, and only reported findings after 6 months of lens wear.24 Furthermore, single-vision correction was used during testing to eliminate any potential influence of the DIMS lenses. In contrast, the present study evaluated the effects of DIMS lenses on accommodation and binocular functions by having participants wear them as they would in their daily activities. This approach allowed for a more comprehensive understanding of how DIMS lenses impact accommodation and binocular functions, with changes observed as early as one month after lens wear, and assessments conducted at three-month intervals up to 12 months.
A significant improvements in VA using both high-contrast and low-contrast charts were found following DIMS lens wear in myopic Malay schoolchildren, aligning with previous study that reported improvement in distance HCVA following DIMS lens wear.24 The improvement in VA was observed over time, with distance HCVA significantly change by the third month and distance LCVA, near HCVA, and near LCVA by the sixth month. This pattern may be influenced by measurement protocols, learning effects from repeated testing, and high blur adaptation among myopes.24,32 The micro-lenslet design of DIMS lenses may initially reduce VA in the mid-peripheral region,33,34 contributing to a longer adaptation period for near vision improvements.
Wearing DIMS spectacle lenses for 12 months significantly changes accommodation and binocular functions of myopic Malay children. The LA decreased by 0.20 D (p < 0.05), indicating an improvement in accommodative response over time. This improvement suggests better focusing ability, which can enhance visual comfort during near work tasks. Similar findings were reported by Lam et al24 where a reduction in LA was noted among Chinese children after 24 months of DIMS lens wear. However, the decrease in LA was not significantly different to that seen in single-vision lens wearers, suggesting that factors such as accommodative adaptation and lens compliance may also play a role.24,35 The AA remained stable, with a binocular AA reduction of 0.57 D after 12 months, aligning with expected age-related changes, as previous studies have reported that AA decreases with increasing age.24,36 Similarly, NRA and PRA showed no significant changes (p > 0.05), reinforcing the idea that DIMS lenses do not negatively impact accommodative function.
An improvement in stereoacuity was recorded between the third and twelfth months of lens wear, correlating with near VA improvements. However, the temporary reduction observed at one month indicates an adaptation period, aligning with previous research on visual function changes associated with myopia control lenses.37 This initial decline in stereoacuity may reflect the adjustment process to lens-induced visual modifications, while the subsequent improvement is likely attributed to enhanced binocular vision control and alignment, leading to better coordination and depth perception over time. A slight receded in NPC of 0.38 cm was detected over 12 months, indicating a minor reduction in convergence amplitude. This change, along with the reduction in AA, suggests possible adaptations in accommodative-vergence interactions. Despite this, NPC remained below the clinical cut-off value of 7.5 cm, which is considered the threshold for symptomatic convergence insufficiency.38 Although the observed NPC changes in this study were not clinically significant, annual assessments are recommended when using DIMS lenses to ensure that prolonged wear does not negatively affect vergence function.
In this study, both distance and near phoria showed a slight shift from exophoria toward esophoria after 12 months of DIMS lens wear. However, these changes were less than 1 PD, making them clinically insignificant. Statistical analysis also revealed no significant differences in phoria values, suggesting that binocular alignment remained stable throughout the study period. These findings align with previous research on myopic children wearing myopia control.24,37
Significant changes in fusional vergence were observed after 12 months of DIMS lens wear, with notable increases in distance NFV break points, distance NFV recovery points, and near PFV recovery points. Other vergence parameters remained stable, likely due to sample size limitations. Although the increase in distance NFV were statistically significant, it was less than 1 PD, making it clinically insignificant. The increase in PFV aligns with the slight shift toward esophoria, indicating improved vergence stability and the ability to maintain single binocular vision even when convergence demands increase.31 This finding is consistent with previous research showing that individuals with esophoria tend to have greater PFV amplitudes.39 Notably, the PFV improvements observed in this study reflects patterns reported in hyperopic individuals, suggesting that DIMS lenses may enhance vergence function to levels closer to emmetropic norms.40
Additionally, the gradient AC/A ratio showed a significant increase, suggesting an adaptive response to DIMS lenses in maintaining binocular vision stability. After 12 months of lens wear, the AC/A ratio shifted toward normative values,31 reflecting improved accuracy in the accommodation-convergence interaction in children. The use of +2.00 DS lenses in measuring the AC/A ratio using gradient method enhances the convergence-accommodation response. The +2.00 D lens functions to relax the accommodation system by reducing the accommodative demand, but the contraction of the extraocular muscles needs to be increased to adjust to this change and maintain binocular alignment. The contraction of the vergence system muscles to support an increase in accommodative response is reflected by the increase in the AC/A ratio value.41 According to Singh, Mani, and Hussaindeen,42 adaptation to the use of positive lenses leads to an increase in the AC/A ratio using the gradient method. The increase in AC/A with +2.00 D lens indicates that the vergence system has adapted to the use of DIMS lenses. This adaptation helps sustain single binocular vision by enhancing the convergence-accommodation response.
This study also confirms that myopic Malay children wearing DIMS lenses for 12 months experienced significantly slower myopia progression compared to those without myopia control. The recorded SE progression of −0.29 ± 0.41 D and AL elongation of 0.08 ± 0.15 mm align with previous findings,21,22 showing greater control than the typical −0.50 D to −1.00 D SE progression and 0.33 mm AL increase per year in children without myopia control.43–46 The study by Lam et al21 reported a 12-month SE progression of −0.23 D and AL elongation of 0.11 mm in children wearing DIMS lenses, demonstrating a 52% reduction in myopia progression and a 62% decrease in AL elongation compared to single-vision lenses. Their effectiveness surpasses other spectacle-based interventions, such as bifocal lenses (39%) and multifocal lenses (20%),47–51 and is also comparable to orthokeratology (60%) and multifocal contact lenses (50–60%).17,52 The success of DIMS lenses is attributed to their myopic defocus design (+3.50 D), which helps slow myopia progression while maintaining clear vision.21 Compared to other myopia control interventions such as orthokeratology and multifocal contact lenses, DIMS lenses offer a non-invasive and easily accessible option. While orthokeratology and multifocal contact lenses have shown significant myopia control effects, they require more complex fitting procedures and may not be suitable for all children. DIMS lenses provide a practical alternative with demonstrated effectiveness in controlling myopia progression.
Overall, while significant changes were noted in some of binocular vision and accommodation functions, they remained within normal clinical limits. This study concludes that DIMS lenses do not disrupt binocular vision balance in myopic Malay primary schoolchildren. Instead, they enhance the adaptability of the accommodation and vergence systems to the optical changes induced by the lens design. Improved accommodative response was evident through the reduction in LA, while receded NPC, and increase in NFV and PFV indicate adjustments within the vergence system. Additionally, the increase in AC/A ratio suggests better coordination between accommodation and vergence functions. These adaptations help maintain single, clear, and comfortable vision during lens wear. The myopic defocus design of DIMS lenses (+3.50 D) creates a peripheral hyperopic blur that signals the eye to slow axial elongation. This mechanism not only controls myopia progression but also appears to enhance the accommodative response and binocular coordination, as evidenced by the improvements in LA and the AC/A ratio. These findings highlight the importance of regular binocular vision assessments, particularly NPC, NFV, and PFV, into myopia management protocols with DIMS lenses. Furthermore, ensuring proper frame selection based on the wearer’s pupillary distance (PD) is crucial for optimizing the effectiveness of myopia control. Both factors should be carefully considered by optometrists and ophthalmologists when prescribing DIMS lenses to ensure long-term success in myopia management.
This study has several limitations. Firstly, the absence of a control group prevents direct comparison of the intervention’s effectiveness and its impact on binocular functions. Without a comparison group, it is unclear whether the observed changes resulted from myopia control treatment or other factors. Secondly, the 12-month study duration may be insufficient to assess long-term effects, as some binocular vision parameters fluctuated but did not show significant changes. Longer follow-ups are recommended to determine if these trends persist over time. Another notable limitation is the relatively small final sample size, which may increases the risk of Type II errors, where meaningful differences may go undetected. However, based on our post-hoc power analysis, the study achieved approximately 86% power, indicating sufficient statistical strength to detect meaningful effects for the primary outcomes. Nonetheless, the results should be interpreted with caution and validated in larger cohorts. Lastly, the study focused only on myopic children with normal binocular vision, limiting its applicability to those with binocular vision disorders. Future research should explore the effects of DIMS lenses on children with binocular vision anomalies to broaden their clinical relevance.
Conclusion
Wearing DIMS lenses for 12 months successfully controlled myopia progression and resulted in insignificant changes in accommodation and binocular functions in myopic Malay schoolchildren. These findings suggest that DIMS lenses help maintain stable binocular vision functions, particularly the accommodation and vergence interactions, reinforcing their safety and effectiveness for myopia management. However, comprehensive assessments before prescribing DIMS lenses, proper lens fitting and regular binocular vision evaluations, particularly NPC, PFV, and NFV during follow-up visits are recommended. It is important to note that the absence of a control group in this study limits causal interpretation, as observed changes may reflect natural developmental trends, repeated testing effects, or regression to the mean. While the study demonstrated insignificant changes in accommodation and binocular functions over 12 months, it is unclear whether these effects would remain stable over several years. Longitudinal studies are needed to assess the sustained impact of DIMS lenses on visual functions, as prolonged use may lead to adaptive changes not observed in the short term. Therefore, further research using controlled and larger-scale longitudinal designs is warranted to explore the sustained impact of DIMS lenses on accommodation and binocular functions stability, as prolonged use may lead to adaptive changes not observed in the short term wear.
Ethics Statement
This research adhered to the tenets of the Declaration of Helsinki. This research also received an ethical approval from the Human Subjects Ethics Subcommittee of Universiti Kebangsaan Malaysia (UKM PPI/111/8/JEP-2020-667).
Consent to Participate
The subjects and their parents received a detailed explanation of the study, and informed consent was obtained from them before the research began.
Acknowledgments
The authors sincerely appreciate the cooperation of all subjects and their parents. We also acknowledge the Optometry & Vision Science Program, UKM, for instruments and facility support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received a University Research Grant (GUP-2020-054) from the Universiti Kebangsaan Malaysia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–1042. doi:10.1016/j.ophtha.2016.01.006
2. Tsai TH, Liu YL, Ma IH, et al. Evolution of the prevalence of myopia among Taiwanese schoolchildren: a review of survey data from 1983 through 2017. Ophthalmology. 2021;128(2):290–301. doi:10.1016/j.ophtha.2020.07.017
3. Saw SM, Cheng A, Fong A, Gazzard G, Tan DTH, Morgan I. School grades and myopia. Ophthalmic Physiol Opt. 2007;27(2):126–129. doi:10.1111/j.1475-1313.2006.00455.x
4. Zhang XJ, Zhang Y, Kam KW, et al. Prevalence of myopia in children before, during, and after Covid-19 restrictions in Hong Kong. JAMA Netw Open. 2023;6(3):e234080. doi:10.1001/jamanetworkopen.2023.4080
5. Ma D, Wei S, Li SM, et al. Progression of myopia in a natural cohort of Chinese children during Covid-19 pandemic. Graefes Arch Clin Exp Ophthalmol. 2021;259(9):2813. doi:10.1007/s00417-021-05305-x
6. Liang J, Pu Y, Chen J, et al. Global prevalence, trend and projection of myopia in children and adolescents from 1990 to 2050: a comprehensive systematic review and meta-analysis. Br J Ophthalmol. 2025;109(3):362–371. doi:10.1136/bjo-2024-325427
7. Chen SJ, Lu P, Zhang WF, Lu JH. High myopia as a risk factor in primary open angle glaucoma. Int J Ophthalmol. 2012;5(6):750–753. doi:10.3980/j.issn.2222-3959.2012.06.18
8. Haarman AEG, Enthoven CA, Willem J, et al. The complications of myopia: a review and meta-analysis. Invest Ophthalmol Vis Sci. 2020;61(4):49. doi:10.1167/iovs.61.4.49
9. Ikuno Y. Overview of the complications of high myopia. Retina. 2017;37(12):2347–2351. doi:10.1097/IAE.0000000000001489
10. Logan NS, Radhakrishnan H, Cruickshank FE, et al. IMI Accommodation and binocular vision in myopia development and progression. Invest Opthalmol Vis Sci. 2021;62(5):4.
11. Saw SM, Chua WH, Hong CY, et al. Nearwork in early-onset myopia. Invest Ophthalmol Vis Sci. 2002;43(2):332–339.
12. Kaur K, Gurnani B, Nayak S, et al. Digital Eye Strain- A Comprehensive Review. Ophthalmol Ther. 2022;11(5):1655. doi:10.1007/s40123-022-00540-9
13. Troilo D, Smith EL, Nickla DL, et al. IMI Report on experimental models of emmetropization and myopia. Invest Ophthalmol Vis Sci. 2019;60(3):M31–M88. doi:10.1167/iovs.18-25967
14. Lawrenson JG, Shah R, Huntjens B, et al. Interventions for myopia control in children: a living systematic review and network meta-analysis. Cochrane Database Syst Rev. 2023;2023(2):CD014758.
15. Zaabaar E, Zhang Y, Kam KW, et al. Low-concentration atropine for controlling myopia onset and progression in East Asia. Asia-Pac J Ophthalmol. 2024;13(6):100122. doi:10.1016/j.apjo.2024.100122
16. Sun Y, Xu F, Zhang T, et al. Orthokeratology to control myopia progression: a meta-analysis. PLoS One. 2015;10(4):e0124535. doi:10.1371/journal.pone.0124535
17. Raffa L, Allinjawi K, Sharanjeet-Kaur SK, Akhir S, Mutalib H. Myopia control with soft multifocal contact lenses: 18-month follow-up. Saudi J Ophthalmol. 2021;35(4):325–331. doi:10.4103/1319-4534.347305
18. Bullimore MA, Sinnott LT, Jones-Jordan LA. The risk of microbial keratitis with overnight corneal reshaping lenses. Optometry Vision Sci. 2013;90(9):937–944. doi:10.1097/OPX.0b013e31829cac92
19. Gong Q, Janowski M, Luo M, et al. Efficacy and adverse effects of atropine in childhood myopia: a meta-analysis. JAMA Ophthalmol. 2017;135(6):624–630. doi:10.1001/jamaophthalmol.2017.1091
20. Atchison DA, Charman WN. Optics of spectacle lenses intended to treat myopia progression. Optometry Vision Sci. 2024;101(5):238–249. doi:10.1097/OPX.0000000000002140
21. Lam CSY, Tang WC, Tse DYY, et al. Defocus Incorporated Multiple Segments (DIMS) spectacle lenses slow myopia progression: a 2-year randomised clinical trial. Br J Ophthalmol. 2020;104(3):363–368. doi:10.1136/bjophthalmol-2018-313739
22. Lam CSY, Tang WC, Lee PH, et al. Myopia control effect of Defocus Incorporated Multiple Segments (DIMS) spectacle lens in Chinese children: results of a 3-year follow-up study. Br J Ophthalmol. 2022;106(8):1110–1114. doi:10.1136/bjophthalmol-2020-317664
23. Lam CSY, Tang WC, Zhang HY, et al. Long-term myopia control effect and safety in children wearing DIMS spectacle lenses for 6 years. Sci Rep. 2023;13(1):5475. doi:10.1038/s41598-023-32700-7
24. Lam CSY, Tang WC, Qi H, et al. Effect of Defocus Incorporated Multiple Segments spectacle lens wear on visual function in myopic Chinese children. Transl Vis Sci Technol. 2020;9(9):1–10. doi:10.1167/tvst.9.9.11
25. Yang Y, Wang L, Li P, Li J. Accommodation function comparison following use of contact lens for orthokeratology and spectacle use in myopic children: a prospective controlled trial. Int J Ophthalmol. 2018;11(7):1234–1238. doi:10.18240/ijo.2018.07.26
26. Gwiazda JE, Hyman L, Norton TT, et al. Accommodation and related risk factors associated with myopia progression and their interaction with treatment in COMET children. Invest Ophthalmol Vis Sci. 2004;45(7):2143–2151. doi:10.1167/iovs.03-1306
27. Fang J, Huang Z, Long Y, et al. Retardation of myopia by multifocal soft contact lens and orthokeratology: a 1-year randomized clinical trial. Eye Contact Lens. 2022;48(8):328–334. doi:10.1097/ICL.0000000000000911
28. Zhu X, Wang D, Li N, Zhao F. Effects of customized progressive addition lenses vs. single vision lenses on myopia progression in children with esophoria: a randomized clinical trial. J Ophthalmol. 2022;2022:9972761. doi:10.1155/2022/9972761
29. Kang P, watt K, Chau T, Zhu J, Evans BJW, Swarbrick H. The impact of orthokeratology lens wear on binocular vision and accommodation: a short-term prospective study. Contact Lens Anterior Eye. 2018;41(6):501–506. doi:10.1016/j.clae.2018.08.002
30. Norazman FNN, Mohd-Ali B, Syed Mohd Dardin SF, et al. Baseline accommodation and binocular vision measures in Malay schoolchildren enrolled in the Myopia Control Study Using Spectacle Lenses in Kuala Lumpur. Clin Optom. 2024;16:45–52. doi:10.2147/OPTO.S432496
31. Scheiman M, Wick B. Clinical Management of Binocular Vision: Heterophoric, Accommodative, and Eye Movement Disorders. Lippincott Williams & Wilkins; 2008. https://books.google.com.my/books?id=jGGROHBFYt8C.
32. Cufflin MP, Mankowska A, Mallen EAH. Effect of blur adaptation on blur sensitivity and discrimination in emmetropes and myopes. Invest Ophthalmol Vis Sci. 2007;48(6):2932–2939. doi:10.1167/iovs.06-0836
33. Li X, Ding C, Li Y, et al. Influence of lenslet configuration on short-term visual performance in myopia control spectacle lenses. Front Neurosci. 2021;15:667329. doi:10.3389/fnins.2021.667329
34. Lu Y, Lin Z, Wen L, et al. The adaptation and acceptance of Defocus Incorporated Multiple Segment lens for Chinese children. Am J Ophthalmol. 2020;211:207–216. doi:10.1016/j.ajo.2019.12.002
35. Chen Y, Drobe B, Zhang C, et al. Accommodation is unrelated to myopia progression in Chinese myopic children. Sci Rep. 2020;10(1):1–8. doi:10.1038/s41598-019-56847-4
36. Castagno VD, Vilela MAP, Meucci RD, et al. Amplitude of accommodation in schoolchildren. Curr Eye Res. 2017;42(4):604–610. doi:10.1080/02713683.2016.1220586
37. Huang Y, Li X, Wang C, et al. Visual acuity, near phoria and accommodation in myopic children using spectacle lenses with aspherical lenslets: results from a randomized clinical trial. Eye and Vision. 2022;9(1):1–8. doi:10.1186/s40662-022-00304-3
38. Menjivar AM, Kulp MT, Mitchell GL, Toole AJ, Reuter K. Screening for convergence insufficiency in school‐age children. Clin Exp Optom. 2018;101(4):578–584. doi:10.1111/cxo.12661
39. Anderson H, Stuebing KK, Fern KD, Manny RE. Ten-year changes in fusional vergence, phoria, and nearpoint of convergence in myopic children. Optometry Vision Sci. 2011;88(9):1060–1065. doi:10.1097/OPX.0b013e31822171c0
40. Masihuzzaman M, Dhakal P, Gautam K. Relationship of negative, positive relative accommodation and negative, positive fusional vergence in ammetropes and emmetropes in a young population of Nepal. Acta Sci Ophthalmol. 2021;4(1):3–8.
41. Mutti DO, Mitchell GL, Jones-Jordan LA, et al. The response AC/A ratio before and after the onset of myopia. Invest Ophthalmol Vis Sci. 2017;58(3):1594–1602. doi:10.1167/iovs.16-19093
42. Singh NK, Mani R, Hussaindeen JR. Changes in stimulus and response AC/A ratio with vision therapy in convergence insufficiency. J Optom. 2017;10(3):169–175. doi:10.1016/j.optom.2016.10.001
43. Hou W, Norton TT, Hyman L, Gwiazda J. Axial elongation in myopic children and its association with myopia progression in the Correction of Myopia Evaluation Trial. Eye Contact Lens Sci Clin Pract. 2018;44(4):248–259. doi:10.1097/ICL.0000000000000505
44. Rozema J, Dankert S, Iribarren R, Lanca C, Saw SM. Axial growth and lens power loss at myopia onset in Singaporean children. Invest Ophthalmol Vis Sci. 2019;60(8):3091–3099. doi:10.1167/iovs.18-26247
45. Tideman JWL, Polling JR, Vingerling JR, et al. Axial length growth and the risk of developing myopia in European children. Acta Ophthalmol. 2018;96(3):301–309. doi:10.1111/aos.13603
46. Yang Y, Cheung SW, Cho P, Vincent SJ. Comparison between estimated and measured myopia progression in Hong Kong children without myopia control intervention. Ophthalmic Physiol Opt. 2021;41(6):1363–1370. doi:10.1111/opo.12895
47. Cheng D, Woo GC, Drobe B, Schmid KL. Effect of bifocal and prismatic bifocal spectacles on myopia progression in children: three-year results of a randomized clinical trial. JAMA Ophthalmol. 2014;132(3):258–264. doi:10.1001/jamaophthalmol.2013.7623
48. Hasebe S, Jun J, Varnas SR. Myopia control with positively aspherized progressive addition lenses: a 2-year, multicenter, randomized, controlled trial. Invest Ophthalmol Vis Sci. 2014;55(11):7177–7188. doi:10.1167/iovs.12-11462
49. Walline JJ. Myopia control: a review. Eye Contact Lens. 2016;42(1):3–8. doi:10.1097/ICL.0000000000000207
50. Walline JJ, Lindsley KB, Vedula SS, et al. Interventions to slow progression of myopia in children. Cochrane Database Syst Rev. 2020;2020(1):CD004916.
51. Huang J, Wen D, Wang Q, et al. Efficacy comparison of 16 interventions for myopia control in children: a Network Meta-analysis. Ophthalmology. 2016;123(4):697–708. doi:10.1016/j.ophtha.2015.11.010
52. Eppenberger LS, Grzybowski A, Schmetterer L, Ang M. Myopia control: are we ready for an evidence based approach? Ophthalmol Ther. 2024;13(6):1453–1477. doi:10.1007/s40123-024-00951-w
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Baseline Accommodation and Binocular Vision Measures in Malay Schoolchildren Enrolled in the Myopia Control Study Using Spectacle Lenses in Kuala Lumpur
Norazman FNN, Mohd-Ali B, Syed Mohd Dardin SF, Mohamad Shahimin M, Mohamad Fadzil N, Mohd Saman MN, Mohidin N
Clinical Optometry 2024, 16:45-52
Published Date: 20 February 2024