Back to Journals » Patient Preference and Adherence » Volume 17
Impact of the First SARS-CoV-2 Lockdown on Adherence to Biological Treatment in Patients with Immune-Mediated Inflammatory Diseases in the Netherlands
Authors van der Groef R, de Jong PHP, Hijnen DJ, van der Woude CJ ![]() , van Laar JAM, van der Kuy PHM
, van Laar JAM, van der Kuy PHM ![]() , Brugma JD, Pasma A
, Brugma JD, Pasma A
Received 9 October 2022
Accepted for publication 7 December 2022
Published 19 January 2023 Volume 2023:17 Pages 167—174
DOI https://doi.org/10.2147/PPA.S392290
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Romy van der Groef,1 Pascal HP de Jong,1 Dirk Jan Hijnen,2 Christien J van der Woude,3 Jan AM van Laar,4 P Hugo M van der Kuy,5 Jan-Dietert Brugma,6 Annelieke Pasma1
1Department of Rheumatology, Erasmus University Medical Center, Rotterdam, the Netherlands; 2Department of Dermatology, Erasmus University Medical Center, Rotterdam, the Netherlands; 3Department of Gastroenterology and Hepatology, Erasmus University Medical Center, Rotterdam, the Netherlands; 4Department of Internal Medicine and Immunology, Erasmus University Medical Center, Rotterdam, the Netherlands; 5Department of Clinical Pharmacy, Erasmus University Medical Center, Rotterdam, the Netherlands; 6Department of Outpatient Pharmacy, Erasmus University Medical Center, Rotterdam, the Netherlands
Correspondence: Romy van der Groef, Erasmus University Medical Center, Department of Rheumatology, Room Na-523, PO Box 2040, 3000 CA, Rotterdam, the Netherlands, Tel +31 648284141, Email [email protected]
Purpose: During the SARS-CoV-2 pandemic, national and international societies have recommended continuing biological agents in patients with immune-mediated inflammatory diseases (IMID) in the absence of SARS-CoV-2 symptoms. However, adherence to biological treatment might decrease, because these recommendations contradict patients’ beliefs. Especially an increased concern about side effects could have influenced the adherence to biological treatment during the first lockdown. The primary objective was to investigate the impact of the first SARS-CoV-2 lockdown on adherence to biological treatment in IMID patients.
Patients and Methods: In this prospective cohort study, IMID patients who received a biological agent before and during the first SARS-CoV-2 lockdown (March 2020- June 2020) were included. Patients were excluded if they did not complete the medication adherence report scale-5 (MARS-5) questionnaire at ≥ 1 visit before the lockdown and ≥ 1 visit during the lockdown. Adherence to biological treatment was measured with the MARS-5 and Medication Possession Ratio (MPR).
Results: We included 157 IMID patients. The percentage of adherent patients, defined as MARS-5 score > 21, was significantly lower during the lockdown compared to the period before the lockdown (88.5% vs 84.1%, p< 0.001). Additionally, the overall percentage of adherent patients during the lockdown based on the MPR ≥ 90% was significantly lower compared to adherence based upon the MARS-5 (65.1% vs 84.1%, p< 0.001).
Conclusion: This study showed that the first SARS-CoV-2 lockdown negatively impacts adherence to biological treatment in IMID patients. Therefore, treating physicians should be aware of this problem to minimize the potential harmful effects of non-adherence.
Keywords: adherence, biological, SARS-CoV-2, immune-mediated inflammatory diseases
Introduction
During the SARS-CoV-2 pandemic patients with Immune-mediated inflammatory diseases (IMID) and especially those treated with biologicals, have been closely observed. Multiple studies have shown that biological treatment does not seem to be a risk factor for acquiring SARS-CoV-2 infection or developing (life-threatening) complications compared to the general population.1–3 Moreover, national and international societies recommend continuing the biological agent in IMID patients in the absence of SARS-CoV-2 symptoms. Still, the fear of SARS-CoV-2 infection might be higher among IMID patients, because of their belief that using immunosuppressants will make them more vulnerable to infections. Adherence to their biological treatment might decrease because these recommendations contradict patients ‘beliefs.3
Adherence can be defined as “the extent to which a patient participates in a treatment regimen after he or she agrees to that regimen”.4 Adherence is a process that includes three behavioral components: initiation, implementation, and discontinuation of treatment.5 Increasing fear of infection in IMID patients, who already are treated with biologicals, could interfere with the discontinuation and implementation components of adherence behavior. Patients could stop taking their prescribed medication or their received medication dose can deviate from the prescribed dosage. This can result in poor execution non-adherence or even discontinuation non-adherence. These types of non-adherence to biological treatment can result in disease flares and loss of biological agent efficacy due to anti-drug antibodies, which emphasizes the importance of continuing biological treatment.1,6
Previous studies in Germany and the Czech Republic have shown that adherence behavior to biological treatment minimally changed in specific IMID patients during their national SARS-CoV-2 lockdown.7,8 This could be due to the way information about SARS-CoV-2 infections in those specific countries was delivered to IMID patients. We cannot adopt these results for the Dutch IMID patient population, because different information may have been exchanged. Furthermore, adherence was not measured with a validated questionnaire, which may influence the reliability of the results. Therefore, we investigated the impact of the first SARS-CoV-2 lockdown on execution adherence to biological treatment as measured with the medication adherence report scale-5 (MARS-5) questionnaire in IMID patients.
Material and Methods
Patients
We used data from the Biological Registry, a prospective cohort including IMID patients from the Erasmus Medical Center, an academic center in the Netherlands. The Biological Registry is a value-based healthcare initiative monitoring patient-reported outcomes (PROs) of IMID patients treated with biologicals at the Erasmus Medical Center. This registry started in 2018 and includes the following IMIDs: Inflammatory bowel diseases (IBD; Crohn’s disease and Colitis Ulcerosa), inflammatory arthritis (IA; Rheumatoid arthritis, psoriatic arthritis, and spondyloarthritis), inflammatory skin diseases (psoriasis and atopic dermatitis) and other IMIDs (eg Morbus Behcet, Sarcoidosis, Systemic Vasculitis, and Uveitis). Patients were consecutively enrolled in the Biological Registry.
For the present study, we included IMID patients who received a biological agent before and during the first SARS-CoV-2 lockdown. We excluded patients who did not complete the MARS-5 questionnaire for ≥1 visit before and during the lockdown. In the Netherlands, the first lockdown started on the 23rd of March 2020 and ended in June 2020. The Biological Registry and the present study conformed to the 1975 Declaration of Helsinki and were approved by the Erasmus MC medical research ethics committee (MEC 2018–1075). All participants gave informed consent before participation.
Data Collection and Adherence Measurement
Patient characteristics including age, gender, diagnosis, and duration of disease were collected from digital patient files. Data on the type of biological and medication fill dates were collected from the pharmacy database. Data from the patient files and pharmacy records were part of usual care and were extracted by the researchers. Adherence specific to the biological treatment was measured with the MARS-5 questionnaire. The MARS-5 was one of the online PROs questionnaires which were sent out automatically by an online data collection tool (Gemstracker). In the first year of follow-up, the MARS-5 questionnaire was sent each three months and in the second year, every six months. The MARS-5 was translated into Dutch and validated for use in the Dutch population by the Netherlands Institute for Health Services Research.9 The MARS-5 rates the frequency of adherent-related behaviors using a five-point Likert scale. A higher score indicates higher adherence to the prescribed treatment. We also calculated the Medication Possession Ratios (MPRs) using data from our local pharmacy. The MPRs were calculated by dividing the estimated days’ supply of the biological treatment by the number of days in the period between the last prescription before the lockdown and the first prescription in the lockdown. The MPR measures the percentage of time a patient has access to medication, which can be used to estimate medication adherence based on fill rates.10,11 Patients were defined as treatment adherent if they reported a MARS-5 score >21 and if the MPR was ≥90%.12
Statistical Analyses
The acquired sample size for this study was calculated with the sample size formula for paired proportions.13 Assuming that 20% of the patients switch from adherent to nonadherent and 5% from non-adherent to adherent, and after applying continuity correction, the study would require a sample size of 92 participants. To achieve a power of 80% and a two-sided significance of 5% for detecting a difference of −0.15 between the discordant proportions. Expected discordant proportions were based on the results of a previous study and expert opinion.14 Characteristics of the study population and adherence measurements were described with means, standard deviations, medians, interquartile ranges, and percentages as appropriate. The internal reliability of the MARS-5 was calculated using Cronbach’s α. For all participants, mean MARS-5 scores were calculated from multiple measurements before and during the lockdown. Medians of the overall and individual mean MARS-5 scores were analyzed with the Wilcoxon Rank Sum Test. Differences in frequencies of adherent patients before and during the lockdown were analyzed with McNemar’s Chi-squared test. This statistical test was also used to analyze differences in frequencies of adherent patients based on the MARS-5 and MPR during the lockdown. A sensitivity analysis was performed using a lower and higher cut-off score for the MARS-5. Analyses were also stratified for IMID diagnosis and type of biological agent. If a patient had more than one IMID, the first diagnosed IMID was used for the stratified analysis. All statistical analyses were done in SPSS (version 27.0) and R (version 4.0.0). A p<0.05 was considered statistically significant.
Results
At the time of data extraction, 933 patients were enrolled in the Biological Registry. For the present study, 157 patients were included and most of them had >1 year of follow-up in the Biological Registry. We excluded 765 patients for not completing the MARS-5 questionnaire for ≥1 visit before and during the first lockdown. An additional 11 patients were excluded for not receiving a biological agent during the first lockdown according to pharmacological data. Patient characteristics are presented in Table 1. Patients had a mean age of 46 years (SD 15.08) and 58.6% were female. In addition, 53 patients (33.8%) were diagnosed with an inflammatory skin disease, 50 patients (31.8%) with IA, 37 patients (23.6%) with IBD, and 17 patients (10.8%) had another IMID. TNF-inhibitors were the most prescribed biologicals (46.4%).
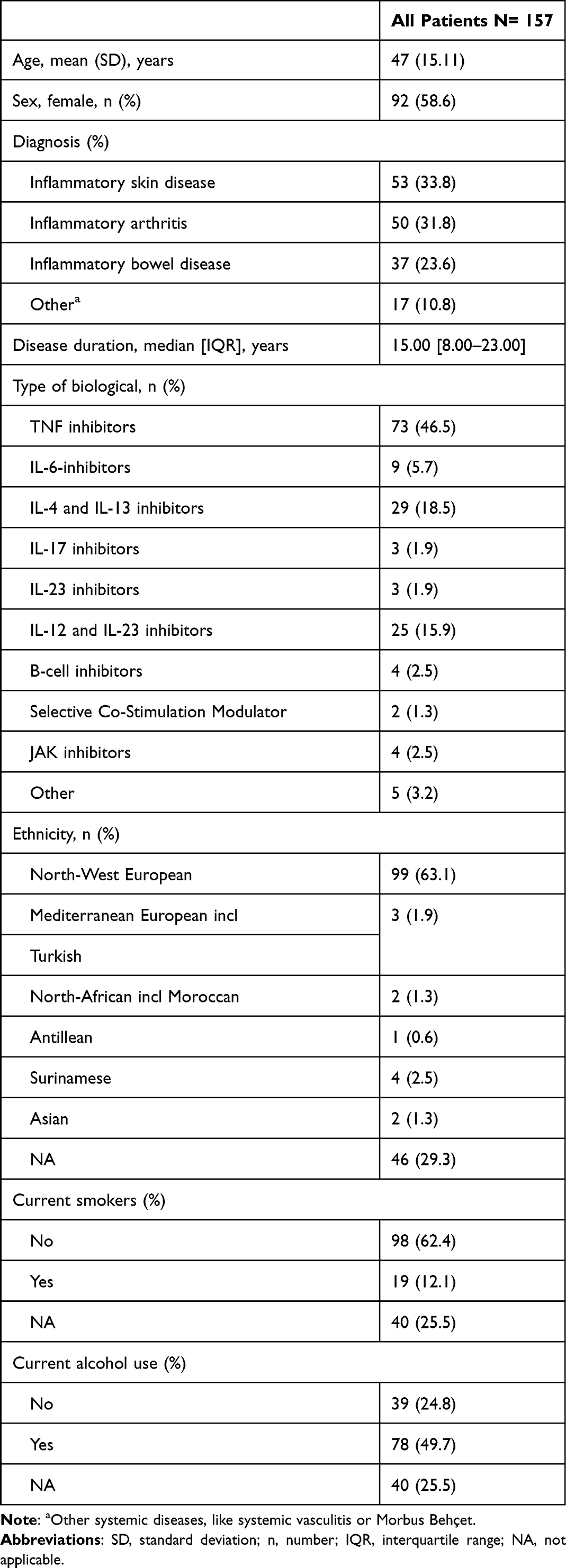 |
Table 1 Patient Characteristics During the First Lockdown |
The percentage of adherent patients based on MARS-5 scores (score >21) was significantly lower during the lockdown compared to the period before the lockdown (84.1% vs 88.5%, p<0.01, Table 2). After stratification for diagnosis, the percentages of adherent patients in almost all groups were lower during the lockdown compared to the period before the lockdown, except for patients diagnosed with IA. In this group, adherence increased during the lockdown (Table 2). Stratification for each type of biological was due to the small sample size per group not possible. Our sensitivity analysis showed that lowering the MARS-5 cut-off to 20 and increasing it to 22 did not change our findings. The internal consistency of MARS-5 was high (Cronbach’s α = 0.834). Cronbach’s α ranged from 0.770 to 0.871 if an item of the MARS-5 was deleted.
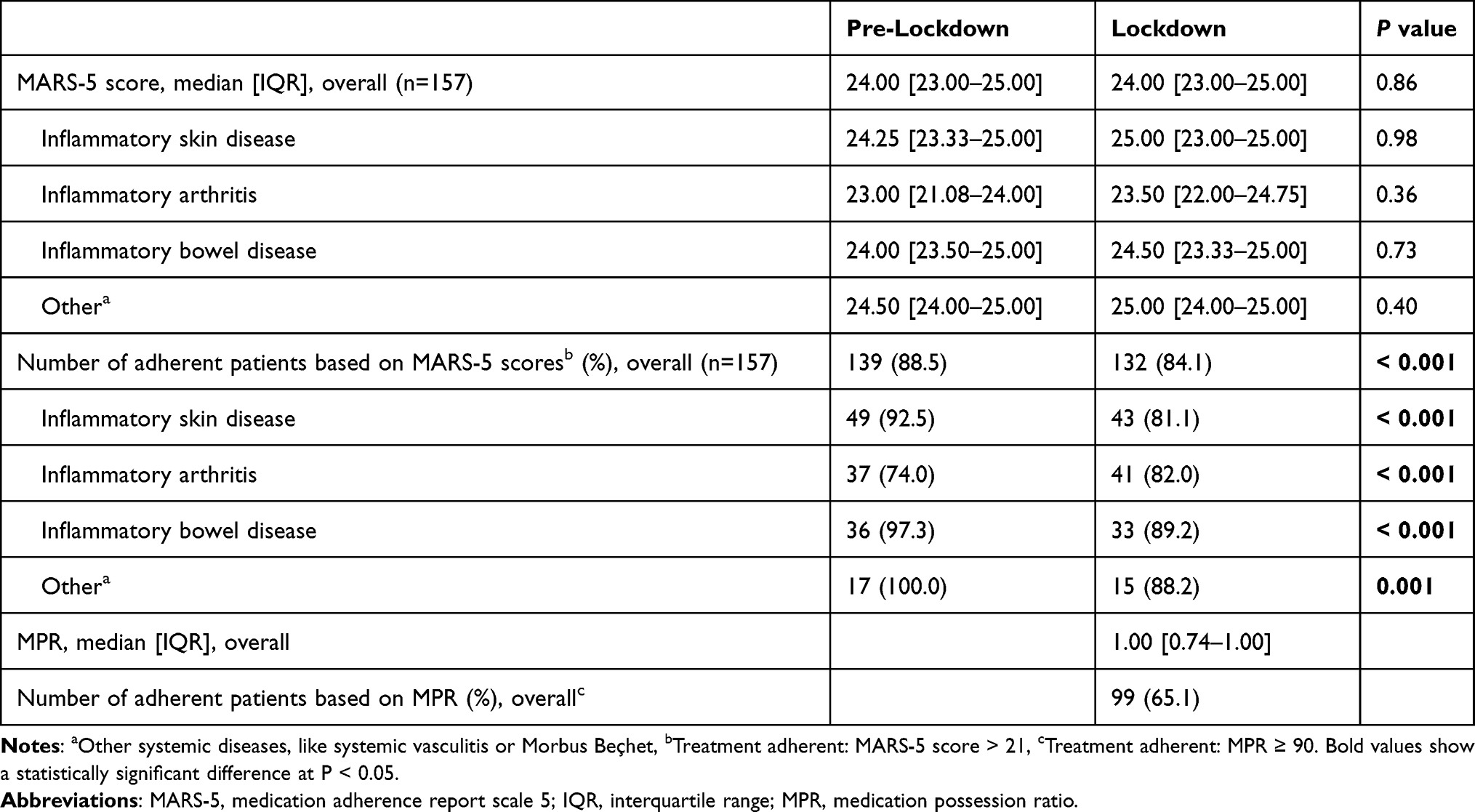 |
Table 2 Treatment Adherence Measurements |
From the 139 adherent patients pre-lockdown, 17 patients changed to non-adherent during the lockdown. The MARS-5 questions that changed the most in these non-adherent patients can be found in Table 3. Additionally, the percentage of adherent patients based on the MPR score was significantly lower compared to adherence based upon the MARS-5 during lockdown (65.1% vs 84.1%, p<0.001).
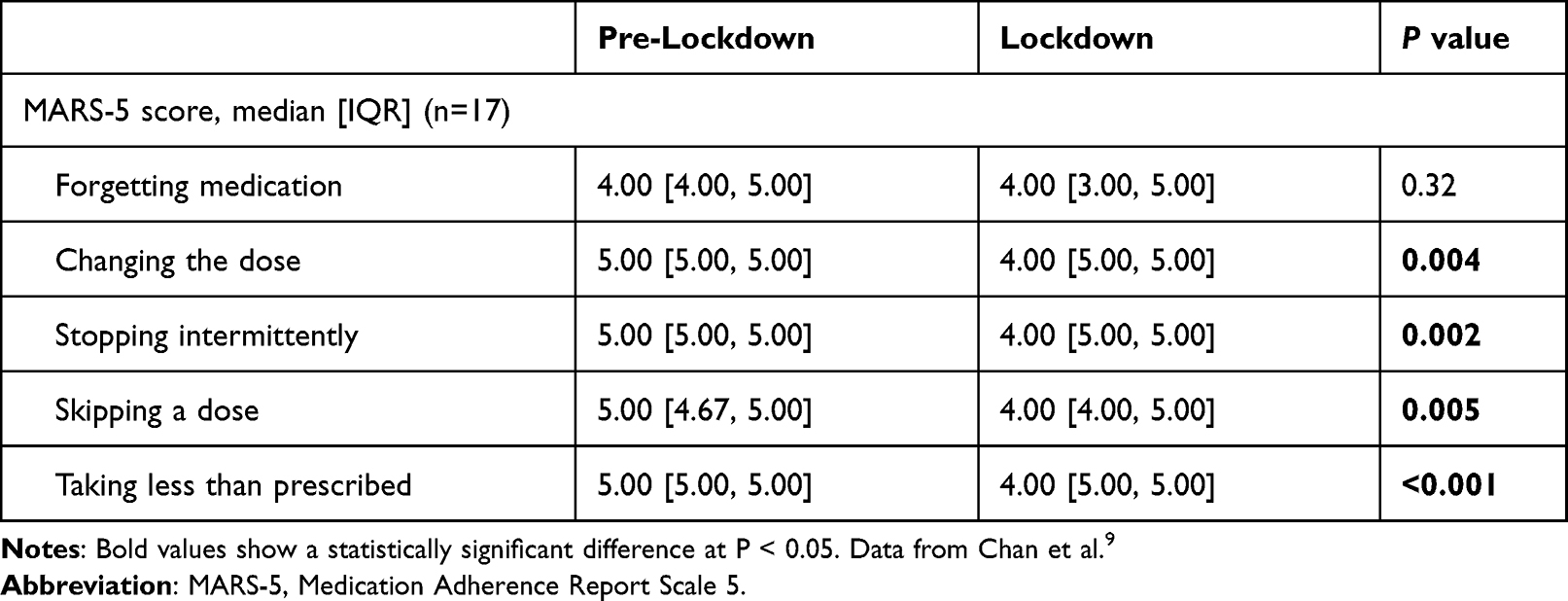 |
Table 3 Median MARS-5 Question Scores for Patients Changing to non-adherent during Lockdown (n= 17) |
Discussion
This study showed that the first SARS-CoV-2 lockdown negatively impacts IMID patients’ execution adherence to biological treatment, as measured with the MARS-5. Moreover, the percentage of adherent patients measured with the MPR was even lower than measured with the MARS-5 score.
The lower percentage of adherent patients during the lockdown can be explained by a change in psychosocial contributors to adherence behavior. All MARS-5 questions, except the first question, were scored worse in non-adherent patients during the lockdown. The first question asks whether the patient has forgotten to take his or her medication during a certain period.15 These results imply that the non-adherence behavior of these patients can be explained by intentional decisions and not by unintentional ones, such as forgetfulness. Increased concern about side effects of biological treatment, such as an increased vulnerability to infections, might be the reason why adherence was lower during the first SARS-CoV-2 lockdown. This is underscored by the study of Horne et al that showed that higher adherence was significantly associated with fewer concerns about treatment (OR = 0.504, 95% CI: [0.450, 0.564]).16 In addition, the study by Kalyoncu et al showed that 18.1% of patients with inflammatory arthritis discontinued their biological treatment. The main reason for discontinuation was fear of the side effects of biological treatment.14 This reason is in line with our (abovementioned) hypothesis of non-adherent behavior during the first SARS-CoV-2 lockdown.
Another reason for non-adherence can be due to reduced and alternate forms of consultation (eg telemedicine) during the first lockdown. Moreover, a recent study showed that treatment intensification, especially to biologicals, occurred less often in IMID patients during the first lockdown.17 Although, the aforementioned study focused on the initiation component of non-adherence, the postponement of face-to-face consultation could negatively impact the implementation of adherence during the first lockdown.
Other studies on the other hand showed that the first lockdown had a minimal impact on adherence to immune-modulatory medication.7,8 This difference might be due to the fact that we used a validated questionnaire over a longer time period in comparison to the aforementioned studies. Furthermore, it is important to keep in mind that adherence is a dynamic process that is influenced by multiple factors.18 These factors could vary between the different healthcare institutions during the first lockdown and, therefore, explain the different adherence measures in the abovementioned studies.
The Capability, Opportunity, and Motivation Model of Behavior (COM-B) can be used to identify barriers to adherent behavior during the first lockdown.19 As mentioned above, we assumed that motivational behavior aspects such as increasing fears and concerns about side effects have affected adherence in IMID patients. However, opportunity factors, such as local delivery problems of biologicals, and knowledge or capability-related factors, such as patients’ knowledge of their vulnerability getting infected while using biological agents, could also have contributed to non-adherence during the first lockdown. In particular, the reduced face-to-face consultations and alternative forms of consultations (eg telemedicine) could have influenced both the capability domain of the COM-B model, as well as the motivation domain.
Strong aspects of our study are that we used a validated questionnaire to measure treatment adherence and that we calculated mean MARS-5 scores from multiple measurements before and during the lockdown. This approach can provide more stable and reliable adherence results, especially for the pre-lockdown period. Moreover, this study provides the first results of adherence to biological therapy in a diverse group of IMID patients. This provides insight into the general effect of the first SARS-CoV-2 lockdown on adherence to biological treatment.
The limitations of our study are that we used a patient-reported adherence questionnaire to measure adherence to biological treatment. Although we used the MARS-5, which is designed to minimize socially desirable answers, these questionnaires can still be prone to overreporting due to recall bias and cannot prevent socially desirable responses.20,21 This is also seen in our study, where the percentage of adherent patients based on the MPR score was significantly lower than the adherence based on the MARS-5 during lockdown (65.1% vs 84.1%). Noteworthy is the fact that a low MPR can also be caused by delivery problems of medication during the lockdown, which is in our case unlikely.
Another limitation is that we had to exclude many patients due to missing data in the first lockdown period. In the Biological Registry, the MARS-5 was sent each three months in the first year of follow-up and every six months during the following years. Due to the large periods between the questionnaires, there was a high chance that many patients had not received the MARS-5 questionnaire during the first lockdown. For the same reason, data on disease activity, beliefs about medication, and quality of life were mainly missing during the first lockdown period. Due to these missing data multivariable statistical analyses could not be performed.
For future research, we would advise monitoring treatment adherence based on methods that are less prone to reporting bias, such as indirect measurement with prescription data or direct measurement of drug concentration in blood.22 Besides, when new lockdowns occur, we would advise decreasing the interval in which PRO questionnaires are sent to patients. This will provide more accurate data on the consequences of a lockdown on treatment adherence and other PROs. Additionally, qualitative data on reasons for (non-) adherence, gathered by interviews, may provide additional insight, since adherence may be influenced by many factors that might not all be captured by PROs.
Clinicians should be aware of the complexity of adherence behavior to medical treatment, in which both unintentional non-adherence, such as forgetfulness and intentional non-adherence, eg due to specific fears, should be considered. Having an open conversation about fears of side effects or other reasons for intentional non-adherence can be a worthwhile intervention for healthcare providers to prevent non-adherence.
Conclusion
This study showed that the first SARS-CoV-2 lockdown negatively impacts adherence to biological treatment in IMID patients. This emphasizes the importance of awareness of adherence influencing factors, such as the SARS-CoV-2 pandemic, to maintain high adherence and minimize the potential harmful effects of non-adherence.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Felsenstein S, Herbert JA, McNamara PS, Hedrich CM. COVID-19 Immunology and treatment options. Clin Immunol. 2020;215:108448. doi:10.1016/j.clim.2020.108448
2. Gianfrancesco M, Hyrich KL, Al-Adely S, et al. Characteristics associated with hospitalisation for COVID-19 in people with rheumatic disease: data from the COVID-19 global rheumatology alliance physician-reported registry. Ann Rheum Dis. 2020;79(7):859–866. doi:10.1136/annrheumdis-2020-217871
3. Calabrese C, Lehman B. COVID-19 a primer for the rheumatologist: management of patients and care settings. Curr Opin Rheumatol. 2020;32(5):429–433. doi:10.1097/BOR.0000000000000732
4. Balkrishnan R. The importance of medication adherence in improving chronic-disease related outcomes: what we know and what we need to further know. Med Care. 2005;43(6):517–520. doi:10.1097/01.mlr.0000166617.68751.5f
5. Vrijens B, De Geest S, Hughes DA, et al. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. 2012;73(5):691–705. doi:10.1111/j.1365-2125.2012.04167.x
6. Bashyam AM, Feldman SR. Should patients stop their biologic treatment during the COVID-19 pandemic. J Dermatolog Treat. 2020;31(4):317–318.
7. Hasseli R, Muller-Ladner U, Keil F, et al. The influence of the SARS-CoV-2 lockdown on patients with inflammatory rheumatic diseases on their adherence to immunomodulatory medication - a cross sectional study over 3 months in Germany. Rheumatology. 2021;60:SI51–SI58. doi:10.1093/rheumatology/keab230
8. Rob F, Hugo J, Tivadar S, et al. Compliance, safety concerns and anxiety in patients treated with biologics for psoriasis during the COVID-19 pandemic national lockdown: a multicenter study in the Czech Republic. J Eur Acad Dermatol Venereol. 2020;34(11):e682–e684. doi:10.1111/jdv.16771
9. Chan AHY, Horne R, Hankins M, Chisari C. The medication adherence report scale: a measurement tool for eliciting patients’ reports of nonadherence. Br J Clin Pharmacol. 2020;86(7):1281–1288. doi:10.1111/bcp.14193
10. Steiner JF, Koepsell TD, Fihn SD, Inui TS. A general method of compliance assessment using centralized pharmacy records. Description and validation. Med Care. 1988;26(8):814–823. doi:10.1097/00005650-198808000-00007
11. Steiner JF, Prochazka AV. The assessment of refill compliance using pharmacy records: methods, validity, and applications. J Clin Epidemiol. 1997;50(1):105–116. doi:10.1016/S0895-4356(96)00268-5
12. Watanabe JH, Bounthavong M, Chen T. Revisiting the medication possession ratio threshold for adherence in lipid management. Curr Med Res Opin. 2013;29(3):175–180. doi:10.1185/03007995.2013.766164
13. Dhand NK, Khatkar MS Statulator: an online statistical calculator. sample size calculator for comparing two paired proportions; 2014. Available from: http://statulator.com/SampleSize/ss2PP.html.
14. Kalyoncu U, Pehlivan Y, Akar S, et al. Preferences of inflammatory arthritis patients for biological disease-modifying antirheumatic drugs in the first 100 days of the COVID-19 pandemic. Turk J Med Sci. 2021;51(4):1615–1623. doi:10.3906/sag-2012-5
15. de Ridder D, Theunissen N. De rol van ziektepercepties in therapietrouw bij hypertensie. [The role of illness perceptions in adherence to hypertension regimens.]. Gedrag Gezondheid. 2003;31(4):237–249.
16. Horne R, Chapman SC, Parham R, Freemantle N, Forbes A, Cooper V. Understanding patients’ adherence-related beliefs about medicines prescribed for long-term conditions: a meta-analytic review of the necessity-concerns framework. PLoS One. 2013;8(12):e80633. doi:10.1371/journal.pone.0080633
17. Kutschera M, Ritschl V, Reichardt B, et al. Impact of COVID-19 pandemic on initiation of immunosuppressive treatment in immune-mediated inflammatory diseases in Austria: a nationwide retrospective study. J Clin Med. 2022;11(18):5308. doi:10.3390/jcm11185308
18. Ritschl V, Stamm TA, Aletaha D, et al. 2020 EULAR points to consider for the prevention, screening, assessment and management of non-adherence to treatment in people with rheumatic and musculoskeletal diseases for use in clinical practice. Ann Rheum Dis. 2021;80(6):707–713. doi:10.1136/annrheumdis-2020-218986
19. Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42. doi:10.1186/1748-5908-6-42
20. Tedla YG, Bautista LE. Factors associated with false-positive self-reported adherence to antihypertensive drugs. J Hum Hypertens. 2017;31(5):320–326. doi:10.1038/jhh.2016.80
21. Mahler C, Hermann K, Horne R, et al. Assessing reported adherence to pharmacological treatment recommendations. Translation and evaluation of the Medication Adherence Report Scale (Mars) in Germany. J Eval Clin Pract. 2010;16(3):574–579. doi:10.1111/j.1365-2753.2009.01169.x
22. Anghel LA, Farcas AM, Oprean RN. An overview of the common methods used to measure treatment adherence. Med Pharm Rep. 2019;92(2):117–122. doi:10.15386/mpr-1201
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Attitude and Willingness to Get COVID-19 Vaccines by a Community Pharmacist in Saudi Arabia: A Cross-Sectional Study
Alshahrani SM, Orayj K, Alqahtani AM, Alfatease A, Alshahrani A, Ibrahim ARN
Patient Preference and Adherence 2022, 16:2821-2834
Published Date: 19 October 2022