Back to Journals » Research and Reports in Urology » Volume 16
Impact of Testosterone Therapy on Major Cardiovascular Risk in Erectile Dysfunction Patients with Testosterone Deficiency
Authors Poopuangpairoj T ![]() , Sirisopana K, Ketsuwan C
, Sirisopana K, Ketsuwan C ![]() , Kongchareonsombat W, Phengsalae Y, Matang W
, Kongchareonsombat W, Phengsalae Y, Matang W ![]() , Sangkum P
, Sangkum P
Received 2 July 2024
Accepted for publication 6 September 2024
Published 17 September 2024 Volume 2024:16 Pages 195—203
DOI https://doi.org/10.2147/RRU.S476804
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Guglielmo Mantica
Tanawin Poopuangpairoj, Kun Sirisopana, Chinnakhet Ketsuwan, Wisoot Kongchareonsombat, Yada Phengsalae, Wijittra Matang, Premsant Sangkum
Division of Urology, Department of Surgery, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Premsant Sangkum, Division of Urology, Department of Surgery, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand, Email [email protected]
Objective: The objective of this study was to evaluate major adverse cardiovascular events in erectile dysfunction (ED) patients who received testosterone replacement therapy (TRT) compared with those who did not.
Materials and Methods: From January 2012 to October 2021, we collected the retrospective data of patients with ED at Ramathibodi Hospital. We divided the patients into two groups: those who received TRT (TRT group) and those with normal testosterone levels and therefore not requiring TRT (non-TRT group). The patients’ baseline clinicodemographic data were collected. Major adverse cardiovascular events, including cardiovascular death, ST- and non-ST-elevation myocardial infarction, hospitalization from congestive heart failure, transient ischemic attack, and ischemic stroke, were collected and analyzed within 2 years after treatment in all groups.
Results: Of the 221 patients, 111 were in the TRT group and 110 were in the non-TRT group. In the non-TRT group, one event each of the following occurred: myocardial infarction, transient ischemic attack, and stroke. In the TRT group, no major cardiovascular event occurred during the 2-year follow-up period. However, no significant difference in major cardiovascular events was noted between the two groups (p = 0.314).
Conclusion: TRT in ED patients with testosterone deficiency does not increase adverse cardiovascular events when compared with ED patients with normal testosterone level.
Keywords: erectile dysfunction, testosterone deficiency, testosterone replacement therapy, major adverse cardiovascular events
Introduction
Erectile dysfunction (ED) is a condition in which the penis does not become sufficiently rigid for sexual intercourse. In 2002, approximately 37.5% of Thai men aged 40–70 years had this condition, amounting to 3 million people across the country.1 One study in 2006 found that 38.5% of Asian people had this condition and that the prevalence of ED was rising with increasing aging.2
There are many contributing factors to ED. One of the most common concomitant endocrine conditions is hypogonadism or testosterone deficiency, which is found in 33% of patients with ED.3 The causes of ED and testosterone deficiency are usually multifactorial and share the same risk factors as cardiovascular disease.4 Signs and symptoms of testosterone deficiency are decreased libido, ED, fatigue, anemia, decreased bone density, and depression.5
Testosterone replacement therapy (TRT) has many forms, including intramuscular, subcutaneous, transdermal, buccal, and oral formulations.6 Currently, TRT is becoming more common in aging hypogonadal men. It is increasingly being used in the US, and in 2011, its use was three times higher than in 2001.7 In the UK, TRT usage increased by 90% between 2001 and 2011.8 Overall, TRT is safe and significantly improves patient symptoms. However, there are some possible adverse effects, including erythrocytosis, obstructive sleep apnea, gynecomastia, acne, aggravation of urinary symptoms in large prostate patients, and infertility.9,10 Because erythrocytosis is one of the side effects of TRT, there are some concerns about adverse cardiovascular events during TRT.
Many studies have been conducted to evaluate this potential risk, but they have had conflicting results. Basaria et al reported in 2010 that TRT in old-age men had a higher rate of cardiac events compared with the placebo group.11 However, recent meta-analyses on this related topic have not found a significant association between TRT and cardiovascular risk.12,13 Even the American Urological Association’s (AUA) 2018 guidelines were unable to conclude this relationship.14 Therefore, many researchers have realized the importance of this matter, and more clinical studies are still required to confirm the cardiovascular safety of TRT in hypogonadal men. In this study, we evaluated the major adverse cardiovascular events in patients with ED who received TRT for the treatment of concomitant hypogonadism and compare them with those in patients with ED who had a normal testosterone level.
Methods and Materials
Patient Population
We conducted a retrospective cohort study between January 2012 and October 2021 at Ramathibodi Hospital, Bangkok, Thailand, including patients with ED with a history of at least 2 years of follow-up who have available data on baseline and follow-up testosterone levels. Erectile dysfunction (ED) can be defined as a persistent or recurrent inability to achieve and/or maintain an adequate penile erection for sexual satisfaction and satisfactory sexual performance.15 Patients who did not have a testosterone level prior to ED treatment and who had used TRT before January 2012 were excluded. We divided the patients with ED into two groups: those with low testosterone levels who received TRT (the TRT group) and those with normal testosterone levels not requiring TRT (the non-TRT group). The principles of the Helsinki Declaration were followed during the study, and the confidentiality of the patients’ data was guaranteed. All protocols were approved by the Human Research Ethics Committee, Faculty of Medicine Ramathibodi Hospital, Mahidol University.
Baseline Characteristics and Pretreatment Parameters
The following data were collected from all patients at the beginning of ED treatment: age, body weight (kg), height (cm), body mass index (BMI), underlying disease, current medications, history of smoking and alcohol drinking, vital signs at the second visit, IIEF 5 score, EHS score, prostate-specific antigen (PSA) level, testosterone level, fasting blood sugar (FBS), lipid profile, blood urea nitrogen (BUN), creatinine, and hematocrit level.
Testosterone Replacement Therapy
Testosterone deficiency was diagnosed as morning serum total testosterone level of <300 ng/dL. Testosterone deficiency is characterized not only by low testosterone production but also by the presence of symptoms or signs associated with low serum total testosterone levels.14 In this study, three formulations of TRT were used: transdermal testosterone gel, intramuscular testosterone undecanoate, and oral testosterone undecanoate (although this has not been available in Thailand since 2017). The choice of medication depended on the patient’s preferences. The testosterone level was monitored, and the dosage was adjusted according to the patient’s testosterone level. Each group was administered a PDE5 inhibitor as the treatment of ED.
Posttreatment Outcome
Major adverse cardiovascular events, including cardiovascular death, ST- and non-ST-elevation myocardial infarction, unstable angina, hospitalization with congestive heart failure, transient ischemic attack, and ischemic stroke, within 2 years of treatment were collected from the medical records for both groups. BMI and laboratory parameters, including testosterone level, PSA, hematocrit, FBS, lipid profile, BUN, and creatinine, during 2 years after treatment were collected to compare other covariate factors.
In our practice, the goal of testosterone treatment is to maintain levels within the mid-normal range (350–750 ng/mL). We did not collect data comparing different testosterone formulations. Instead, we monitor testosterone levels, adjust dosages, and occasionally change formulations to ensure levels remain within the appropriate range.
Statistical Analysis
Quantitative data are presented as median (IQR) as appropriate, and categorical data are presented as counts and percentages. Quantitative variables were compared between groups using the independent t test, and categorical variables were compared between groups using the chi-square test. Comparison between the first clinical lab and follow-up over 2 years for the TRT group was done using the Wilcoxon signed-rank test. Interpretation of the odds ratio was done using logistic regression analysis on accepting factors affecting the participation rate of clinical events. P < 0.05 was considered statistically significant. STATA version 14.1 (STATA Corp., Texas, USA) was used for all statistical analyses.
Results
Two hundred and sixty patients with ED were found to have been treated between January 2012 and October 2021, of whom 137 were in the testosterone deficiency with TRT group. Following the exclusion of 26 patients due to prior treatment before 2012, 111 patients remained in this group. There were 123 patients with ED in the non-TRT group; after 13 patients were excluded due to prior treatment before 2012, there were 110 patients in this group.
The demographic data are presented in Table 1. The baseline demographic data of patients in the testosterone deficiency with TRT group and the non-TRT group were not significantly different in terms of median age, height, ED duration, IIEF 5 score, EHS, heart rate, FBS, and cholesterol level. However, significant differences were noted in body weight, BMI, systolic and diastolic blood pressure, obstructive sleep apnea, and antiulcerative drug usage (Table 1).
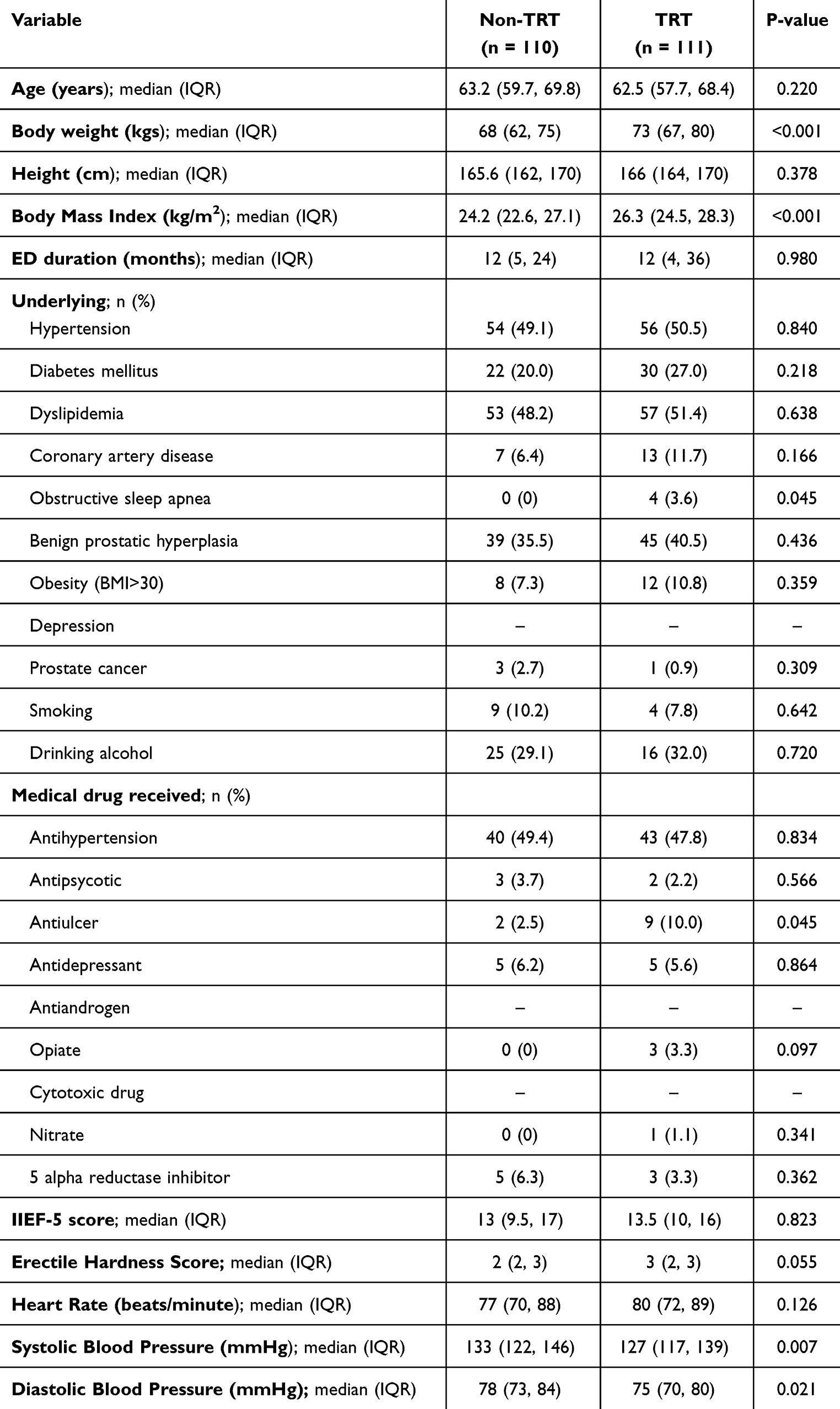 |
Table 1 Baseline Characteristics of the Study Population (n = 221) Stratified by Categories of Baseline Testosterone Level |
The baseline testosterone levels were 475 and 250 ng/dL in the non-TRT and TRT groups, respectively. Table 2 presents the laboratory test results after 2 years of treatment. There was a slight increase in FBS (100 vs 107, p = 0.039) in the non-TRT group. In the TRT group, testosterone level (250 vs 355, p < 0.001), PSA (1.1 vs 1.2 ng/mL, p = 0.005), and Hct (43% vs 44%, p < 0.001) increased significantly after treatment. No significant between-group differences were observed in other laboratory parameters. There was no evidence of erythrocytosis or polycythemia during the treatment period.
 |
Table 2 Changes in Testosterone Level and Other Parameters from Baseline (n = 221) |
The major adverse cardiovascular events are presented in Table 3. In the non-TRT group, there was one event each of myocardial infarction, transient ischemic attack, and stroke. No major cardiovascular events occurred in the TRT group. However, the between-group difference in the occurrence of major cardiovascular events was not significant (p = 0.314). The patient with myocardial infarction had triple-vessel disease, and the event occurred 16 months after ED treatment. This patient had a testosterone level of 780 ng/mL and well-controlled hypertension, and the initial lab results revealed only untreated hypercholesterolemia (cholesterol 218 mg/dL, triglyceride (TG) 80 mg/dL, low-density lipoprotein cholesterol (LDL) 147 mg/dL, high-density lipoprotein cholesterol (HDL) 47 mg/dL); otherwise, he was unremarkable. In the patient with transient ischemic attack, the event occurred after 8 months of ED treatment. He had a testosterone level of 1348 ng/mL and a history of smoking, and the initial lab results revealed untreated hypercholesterolemia (cholesterol 237 mg/dL, TG 117 mg/dL, LDL 132 mg/dL, HDL 88 mg/dL). In the patient with ischemic stroke, the event occurred 15 months after ED treatment. He had a testosterone level of 833 ng/mL and a history of prior hemorrhagic stroke 10 years before treatment; otherwise, he was unremarkable.
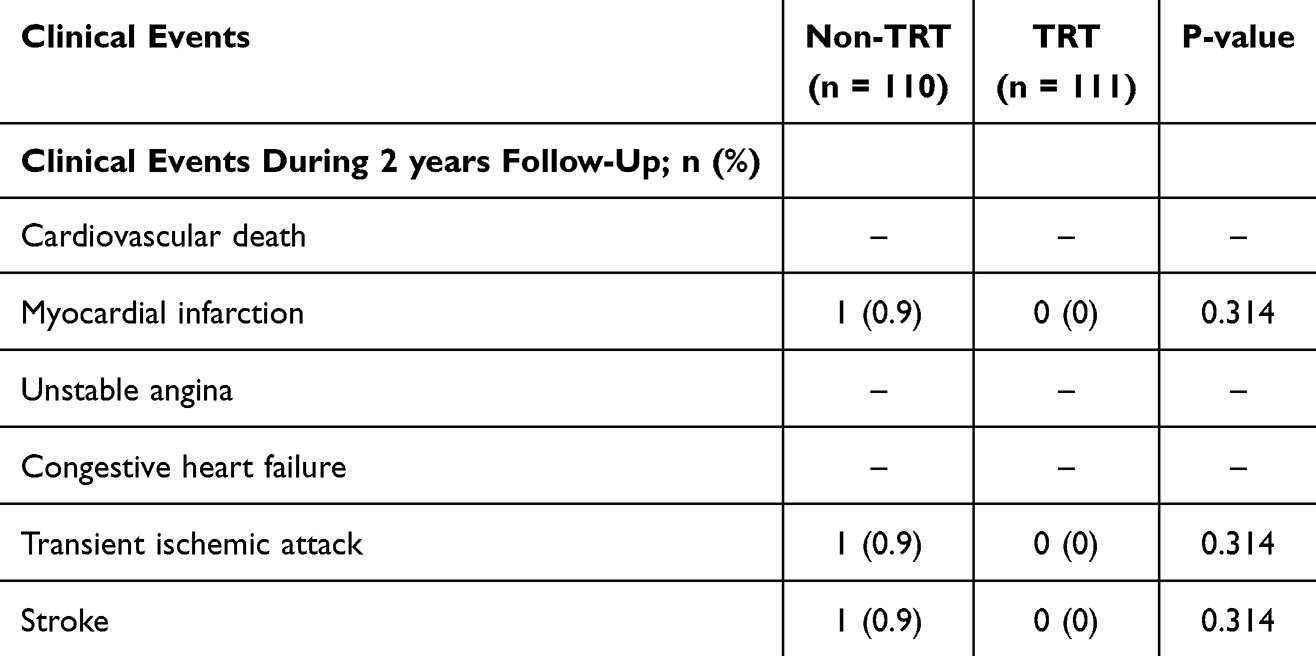 |
Table 3 Adverse Cardiovascular Events During 2 Years Follow-Up (n = 221) |
The between-group differences in baseline demographics did not affect adverse cardiovascular events in this study. Poisson regression analysis indicated a nonsignificant association. We observed that BMI, blood pressure, FBS, and baseline Hct were not significantly associated with adverse cardiovascular events (Table 4).
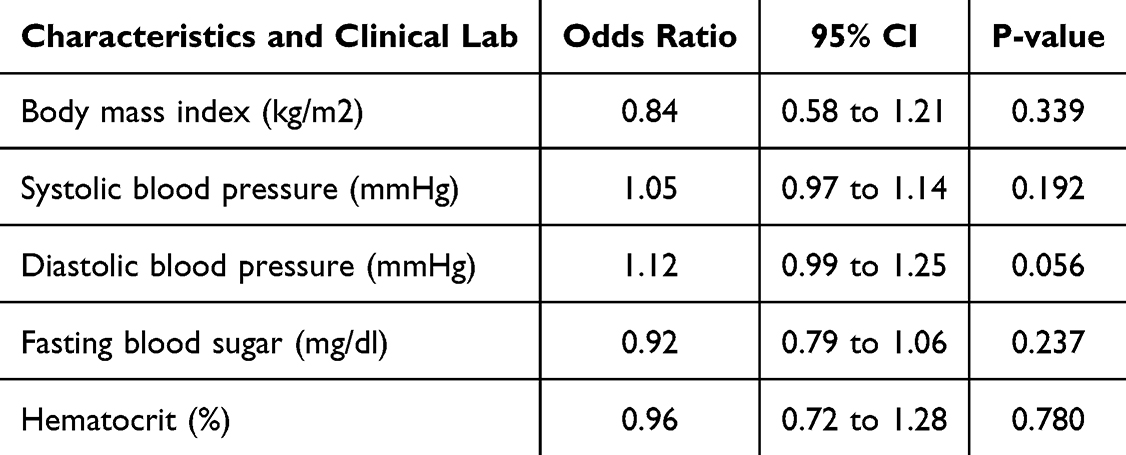 |
Table 4 Odds Ratio for Total Clinical Events (n = 221) |
Discussion
TRT has become more popular among aging men during the past decade.7 TRT offers many benefits for men with hypogonadism, such as improvement of erectile function, sexual desire, anemia, and bone mineral density.14 However, TRT and cardiovascular risk remain controversial issues. In 2015, the US Food and Drug Administration warned that TRT may increase the risk of heart attack and stroke.16 Nevertheless, many clinical studies have confirmed the benefits of TRT on cardiovascular risk.12,13 The 2018 AUA and Endocrine Society guidelines could not draw a conclusion in this regard.14,17 Furthermore, the data are limited, especially in Asian populations.
Testosterone is a male sex hormone that also plays a role in the cardiovascular system, including systemic and coronary vasodilation,18 increasing Hct levels,19 the expression of platelet thromboxane A2 receptors, and the promotion of platelet aggregation;20 positively inotropic effects on cardiomyocytes;21 and shortened QT interval on an electrocardiogram.22 Basaria et al reported in 2010 that TRT in old-age men had a higher rate of cardiac events compared with the placebo group,11 although the primary objective of this study was not to evaluate adverse cardiovascular events. Furthermore, the study tended to terminate early, and the investigators stated that the cardiovascular events that occurred might have occurred by chance.11 Several clinical studies have indicated that TRT may increase cardiovascular risk.23,24 However, most of these studies had limitations, especially due to their retrospective design, short follow-up period, and lack of a true control group.25
By contrast, the results from the Testosterone Trials, which used a prospective randomized placebo control study design in old-age men, indicated no significant difference in major cardiovascular events between the two groups.26 Various studies have shown a possible beneficial effect or no significant association between TRT and cardiovascular risk.27,28 Furthermore, data from recent meta-analyses similarly demonstrated that TRT does not increase cardiovascular risk.12,13,29,30
Patients with ED may have concomitant testosterone deficiency. TRT offers several benefits in ED patients. TRT improves erectile function, sexual activity, hypogonadal symptoms, and sexual desire. Additionally, other sexual function parameters, including intercourse, orgasm, and overall satisfaction, are also enhanced. Furthermore, combination therapy of TRT with a PDE5 inhibitor is superior to PDE5 inhibitors alone in improving erectile function. In other domains, TRT improves body composition, insulin resistance, depressive symptoms, and bone mineral density, which may benefit in elderly patients.31,32
We evaluated cardiovascular risk in patients with ED who had hypogonadism and received TRT. In our study, no major adverse cardiovascular event occurred in the patients with ED who had low testosterone and received TRT. The major cardiovascular events that occurred in this study were not different than that in the non-TRT group. Our results support the cardiovascular safety identified in recent meta-analyses. From this result, we can imply that normalized testosterone levels in ED patients who have low testosterone levels will not increase cardiovascular risk compared with ED patients who have normal testosterone level.
We observed that the baseline characteristics of patients in the TRT group had a higher cardiovascular risk (higher body weight, BMI, cholesterol, and LDL level). However, there was no incidence of a major adverse cardiovascular event during 2 years of follow-up in the TRT group. We identified only three major cardiovascular events, and all of these events were in the non-TRT group. Our study found that hematocrit increased slightly from 43% to 44% during TRT, but this level does not meet the criteria of erythrocytosis. This might explain why we do not have cardiovascular events in the TRT group. We believe that the proper diagnosis of testosterone deficiency before starting treatment and hematocrit monitoring are necessary to prevent cardiovascular events during TRT.
The data from recent meta-analyses indicated no significant association between TRT and major cardiovascular events.29,30,33 However, most clinical studies included in these meta-analyses had some limitations, such as heterogeneity of the cutoff value of low testosterone, short follow-up duration, bias of the selected population, and impact of funding. Furthermore, most clinical studies included mostly non-Asian populations, which may have had different demographics. We believe that more clinical studies in various populations with long-term follow-up are still necessary to further confirm cardiovascular safety during TRT.
The strength of this study is that the diagnoses of testosterone deficiency were valid, based on the patients’ symptoms and signs of testosterone deficiency. All patients had baseline and follow-up testosterone level. Although this was a retrospective study, all the data were collected from real outpatient visits and not based on prescriptions or insurance claim forms. Moreover, all of the patients in this study were patients with ED. Our results reflect the real-life situation in which most testosterone deficiency patients are patients with ED who are seeking treatment. Furthermore, Corona et al reported that most adverse cardiovascular events occurred within 2 years of TRT.29 Therefore, we collected 2 years of results after TRT, which is long enough to see the effect of TRT on cardiovascular risk.
This study has several limitations. First, it is a retrospective study. The patients’ baseline demographics between the two groups were different in body weight, BMI, obstructive sleep apnea, and blood pressure. Second, we do not routinely evaluate free testosterone or sex hormone binding globulin level in our clinical practice, precluding the evaluation of these parameters. Third, we had a small number of testosterone deficiency patients without TRT (only six patients). We could not directly compare adverse cardiovascular events between treated and untreated hypogonadism patients due to the small number of patients in the untreated hypogonadism group. Therefore, we used ED patients with normal testosterone level as a control group. In addition, we had only three major cardiovascular events in this study, and there were only 9% of patients who had a history of coronary artery disease. In fact, the patients with ED in our cohort usually took phosphodiesterase 5 inhibitors, which usually require stable cardiovascular status before starting medication, for their ED treatment. Therefore, the outcomes may have been different if we had a greater sample size or more cardiovascular disease patients in the study. Further prospective randomized placebo control studies with a higher case volume are still required to confirm our findings.
Conclusion
TRT does not increase adverse cardiovascular events in patients with ED with testosterone deficiency compared with patients with ED with normal testosterone level. The results of this study confirm the cardiovascular safety of TRT, especially when there has been proper diagnosis of testosterone deficiency and treatment monitoring during TRT. Further randomized, prospective studies are required to elucidate this finding.
Data Sharing Statement
All relevant (unidentifiable) data are within the manuscript. Additional patient data (unidentifiable) can be requested from the first or corresponding authors upon reasonable reason.
Ethics Approval
Study protocols were approved by Human Research Ethics Committee, Faculty of Medicine Ramathibodi Hospital, Mahidol University (Approval certificate ID MURA2021/941). The need for informed consent was waived by the Human Research Ethics Committee, Faculty of Medicine Ramathibodi Hospital, Mahidol University, because of the retrospective nature of the study.
Acknowledgments
The authors thank Dr. Napaphat Poprom for their statistical analysis consultation of this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors declare no research funding.
Disclosure
The authors declare no conflicts of interest.
References
1. Kongkanand A. Prevalence of erectile dysfunction in Thailand. Thai Erectile Dysfunction Epidemiological Study Group. Int J Androl. 2000;23:77–80. doi:10.1046/j.1365-2605.2000.00022.x
2. Cheng JY, Ng EM, Chen RY, Ko JS. Prevalence of erectile dysfunction in Asian populations: a meta-analysis. Int J Impot Res. 2007;19(3):229–244. doi:10.1038/sj.ijir.3901517
3. Köhler TS, Kim J, Feia K, et al. Prevalence of androgen deficiency in men with erectile dysfunction. Urology. 2008;71(4):693–697. doi:10.1016/j.urology.2007.11.073
4. wein AJ. Campbell-Walsh Urology. Vol. 1502. Elsevier; 2020:27p.
5. Schubert M, Jockenhövel F. Late-onset hypogonadism in the aging male (LOH): definition, diagnostic and clinical aspects. J Endocrinol Invest. 2005;28(3 Suppl):23–27.
6. w AJ. Campbell-Walsh Urology. Elsevier; 2020:1530p.
7. Layton JB, Li D, Meier CR, et al. Testosterone lab testing and initiation in the United Kingdom and the United States, 2000 to 2011. J Clin Endocrinol Metab. 2014;99(3):835–842. doi:10.1210/jc.2013-3570
8. Gan EH, Pattman S, S HSP, Quinton R. A UK epidemic of testosterone prescribing, 2001-2010. Clin Endocrinol. 2013;79(4):564–570. doi:10.1111/cen.12178
9. Wein AJ. Campbell-Walsh Urology. Elsevier; 2020:1529p.
10. Fink J, Ide H, Horie S. Management of male fertility in hypogonadal patients on testosterone replacement therapy. Medicina. 2024;60(2):275. doi:10.3390/medicina60020275
11. Basaria S, Coviello AD, Travison TG, et al. Adverse events associated with testosterone administration. N Engl J Med. 2010;363(2):109–122. doi:10.1056/NEJMoa1000485
12. Ayele HT, Brunetti VC, Renoux C, Tagalakis V, Filion KB. Testosterone replacement therapy and the risk of venous thromboembolism: a systematic review and meta-analysis of randomized controlled trials. Thromb Res. 2021;199:123–131. doi:10.1016/j.thromres.2020.12.029
13. Lee JH, Shah PH, Uma D, Salvi DJ, Rabbani R, Hamid P. Testosterone Replacement Therapy in Hypogonadal Men and Myocardial Infarction Risk: systematic Review & Meta-Analysis. Cureus. 2021;13(8):e17475. doi:10.7759/cureus.17475
14. Mulhall JP, Trost LW, Brannigan RE, et al. Evaluation and Management of Testosterone Deficiency: AUA Guideline. J Urol. 2018;200(2):423–432. doi:10.1016/j.juro.2018.03.115
15. NA BAL, Breau RH, Breau RH, et al. Erectile dysfunction: AUA guideline. J Urol. 2018;200(3):633. doi:10.1016/j.juro.2018.05.004
16. FDA drug safety communication. FDA cautions about using testosterone products for low testosterone due to aging; requires labeling change to inform of possible increased risk of heart attack and stroke with use2015. Available from: https://www.fda.gov/drugs/drugsafety/ucm436259.htm.
17. Bhasin S, Brito JP, Cunningham GR, et al. Testosterone Therapy in Men With Hypogonadism: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2018;103(5):1715–1744. doi:10.1210/jc.2018-00229
18. Kelly DM, Jones TH. Testosterone: a vascular hormone in health and disease. J Endocrinol. 2013;217(3):R47–71. doi:10.1530/JOE-12-0582
19. Coviello AD, Kaplan B, Lakshman KM, Chen T, Singh AB, Bhasin S. Effects of graded doses of testosterone on erythropoiesis in healthy young and older men. J Clin Endocrinol Metab. 2008;93(3):914–919. doi:10.1210/jc.2007-1692
20. Ajayi AA, Mathur R, Halushka PV. Testosterone increases human platelet thromboxane A2 receptor density and aggregation responses. Circulation. 1995;91(11):2742–2747. doi:10.1161/01.CIR.91.11.2742
21. Tsang S, Wong SS, Wu S, Kravtsov GM, Wong TM. Testosterone-augmented contractile responses to alpha1- and beta1-adrenoceptor stimulation are associated with increased activities of RyR, SERCA, and NCX in the heart. Am J Physiol Cell Physiol. 2009;296(4):C766–82. doi:10.1152/ajpcell.00193.2008
22. Schwartz JB, Volterrani M, Caminiti G, et al. Effects of testosterone on the Q-T interval in older men and older women with chronic heart failure. Int J Androl. 2011;34(5 Pt 2):e415–21. doi:10.1111/j.1365-2605.2011.01163.x
23. Vigen R, O’Donnell CI, Barón AE, et al. Association of testosterone therapy with mortality, myocardial infarction, and stroke in men with low testosterone levels. JAMA. 2013;310(17):1829–1836. doi:10.1001/jama.2013.280386
24. Finkle WD, Greenland S, Ridgeway GK, et al. Increased risk of non-fatal myocardial infarction following testosterone therapy prescription in men. PLoS One. 2014;9(1):e85805. doi:10.1371/journal.pone.0085805
25. Traish AM, Guay AT, Morgentaler A. Death by testosterone? We think not! J Sex Med. 2014;11(3):624–629. doi:10.1111/jsm.12464
26. Snyder PJ, Bhasin S, Cunningham GR, et al. Effects of Testosterone Treatment in Older Men. N Engl J Med. 2016;374(7):611–624. doi:10.1056/NEJMoa1506119
27. Anderson JL, May HT, Lappé DL, et al. Impact of Testosterone Replacement Therapy on Myocardial Infarction, Stroke, and Death in Men With Low Testosterone Concentrations in an. Integr Health Care Syst Am J Cardiol. 2016;117(5):794–799.
28. Li H, Mitchell L, Zhang X, Heiselman D, Motsko S. Testosterone Therapy and Risk of Acute Myocardial Infarction in Hypogonadal Men: an Administrative Health Care Claims Study. J Sex Med. 2017;14(11):1307–1317. doi:10.1016/j.jsxm.2017.09.010
29. Corona G, Maseroli E, Rastrelli G, et al. Cardiovascular risk associated with testosterone-boosting medications: a systematic review and meta-analysis. Expert Opin Drug Saf. 2014;13(10):1327–1351. doi:10.1517/14740338.2014.950653
30. Fallara G, Pozzi E, Belladelli F, et al. Cardiovascular Morbidity and Mortality in Men - Findings From a Meta-analysis on the Time-related Measure of Risk of Exogenous Testosterone. J Sex Med. 2022;19(8):1243–1254. doi:10.1016/j.jsxm.2022.05.145
31. AS DG, Bettocchi C, Jones TH, Kliesch S. European Association of Urology (EAU) guidelines on male hypogonadism. In European Association of Urology (EAU) guidelines. Arnhem. 2018;15:
32. Barone B, Napolitano L, Abate M, et al. The Role of Testosterone in the Elderly: what Do We Know? Int J Mol Sci. 2022;23(7):3535. doi:10.3390/ijms23073535
33. Elliott J, Kelly SE, Millar AC, et al. Testosterone therapy in hypogonadal men: a systematic review and network meta-analysis. BMJ Open. 2017;7(11):e015284. doi:10.1136/bmjopen-2016-015284
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.