Back to Journals » Drug Design, Development and Therapy » Volume 20
Impact of Sugammadex versus Neostigmine on Diaphragmatic Function and Respiratory Recovery in Morbidly Obese Patients with Moderate Neuromuscular Block: A Randomised Double-Blind Controlled Trial
Authors Chai YX, Wang YH, Wu L, Wang LX, Li SR, Qiu Z, Yin JW, Zhang BS, Wang GL ![]()
Received 30 October 2025
Accepted for publication 23 March 2026
Published 7 April 2026 Volume 2026:20 577208
DOI https://doi.org/10.2147/DDDT.S577208
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Yu-Xin Chai,1,2 Yu-Hui Wang,1,2 Lei Wu,1,2 Lin-Xin Wang,3 Shu-Ran Li,1,2 Zhuang Qiu,1,2 Jing-Wen Yin,1,2 Bao-Shuang Zhang,1,2 Guang-Lei Wang1,2
1Department of Anesthesiology, The Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 2Jiangsu Province Key Laboratory of Anesthesiology, Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 3Department of Anesthesiology, Zhongshan Hospital, Fudan University, Shanghai, People’s Republic of China
Correspondence: Guang-Lei Wang, Department of Anesthesiology, The Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China, Tel +86 13852087156, Email [email protected]
Purpose: Compared with neostigmine, sugammadex promotes faster neuromuscular recovery, but its impact on diaphragmatic function and respiratory recovery in the morbidly obese cohort, and the mechanism underlying its reduction of postoperative pulmonary complications remain unclear. This study aims to compare the effects of sugammadex and neostigmine on diaphragmatic function and respiratory recovery in morbidly obese patients after surgery, and to investigate the role of diaphragmatic function in the reduction of sugammadex-associated postoperative pulmonary complications.
Patients and Methods: For neuromuscular blockade reversal, 104 morbidly obese patients with moderate neuromuscular block (train-of-four count = 2, ratio < 0.9) were randomly assigned to receive either neostigmine (50 μg kg-1+atropine 20 μg kg-1, n=51) or sugammadex (2 mg kg-1, n=53). Measurements of diaphragmatic excursion (DE) and thickening fraction (TF) were taken during deep and quiet breathing at T0 (baseline), T1 (10 min), and T2 (30 min) after extubation. The primary outcome measure was the change in deep breathing diaphragmatic excursion (ΔDEDB) from baseline at T2. The secondary outcome measures included ΔDEQB, ΔDEDB, and ΔTF at T1; ΔDEQB and ΔTF at T2; postoperative oxygenation index; number of respiratory reminders; and the frequency of postoperative pulmonary complications.
Results: At T2, the ΔDEDB was smaller in the sugammadex group compared with the neostigmine group (0.05 cm vs. 0.28 cm; P < 0.001). At T1, the ΔDEQB, ΔDEDB, and ΔTF all differed significantly between groups, as did the ΔTF at T2 (all P ≤ 0.001). The sugammadex group also demonstrated a higher oxygenation index (P=0.004) and a lower incidence of postoperative pulmonary complications (P=0.007).
Conclusion: In morbid obesity, sugammadex promotes faster diaphragmatic recovery and improves respiratory outcomes compared with neostigmine and is associated with a lower incidence of postoperative pulmonary complications.
Keywords: diaphragm, obesity, morbid, sugammadex, postoperative pulmonary complications
Introduction
As the principal muscle responsible for inspiration, the diaphragm is uniquely the core respiratory muscle that can efficiently generate negative intrathoracic pressure to drive inspiration.1 This muscle accounts for over 60% of the volume of air displaced in a typical breath,2 generates effective cough pressure to clear airway secretions, facilitates alveolar expansion and improves oxygenation.3 In patients with morbid obesity, significant alterations in diaphragmatic function occur due to factors such as intra-abdominal fat accumulation, elevated intra-abdominal pressure, chronic mechanical overload, metabolic abnormalities, and systemic inflammation.4–6 As an integral part of the respiratory muscle ensemble, impaired diaphragmatic function due to residual neuromuscular blockade also constitutes a key risk factor hindering the complex physiological process of postoperative respiratory recovery.7 Previous studies have reported that the incidence of postoperative pulmonary complications (PPCs) ranges from 2.6% to 7.6% in the general surgical population,8 but it approximates 22% in patients with obesity,9 profoundly impairing recovery and increasing healthcare costs, and the mortality rate.
The presence of residual neuromuscular blockade following surgery elevates the risk for PPCs.10,11 Sugammadex reverses deeper levels of neuromuscular blockade more effectively than neostigmine—a pharmacological advantage consistently observed across diverse patient populations. This advantage is particularly clinically relevant in patients with morbid obesity, who face an increased risk of postoperative pulmonary complications.12 Sugammadex promotes a faster recovery of the train-of-four (TOF) ratio to ≥0.9. However, this expedited recovery has not been directly linked to a significant decrease in PPCs.13 Instead, the recovery of respiratory muscle function to preoperative levels may be the underlying reason for the decreased incidence of PPCs in patients with obesity. Ultrasonographic assessment of diaphragmatic excursion has been validated as a reliable and valid method for evaluating diaphragmatic function.14 It remains unclear whether sugammadex accelerates postoperative diaphragmatic recovery, improves respiratory outcomes, and reduces PPCs in morbidly obese patients. This study therefore aimed to compare its effects with neostigmine on these measures, explore the underlying mechanisms, and provide evidence for optimizing enhanced recovery after surgery protocols after bariatric surgery.
Materials and Methods
Ethical Approval and Study Design
This prospective, randomized, single-center study was conducted in accordance with the Declaration of Helsinki at the Affiliated Hospital of Xuzhou Medical University between January and May 2025. The Institutional Review Board of the Affiliated Hospital of Xuzhou Medical University gave its approval to the study protocol (Approval No.: XYFY2024-KL575-01; Approval Date: November 19, 2024; Chairperson: Tie Xu). Prior to patient enrollment, the study was registered on https://clinicaltrials.gov (Registration No.: ChiCTR2400094886; Registration Date: December 30, 2024). Furthermore, informed consent in writing was secured from all subjects involved in the research.
Participants
The inclusion criteria comprised adult patients with a diagnosis of morbid obesity who were scheduled for elective laparoscopic bariatric surgery. To qualify for enrollment, participants were required to meet the following criteria: aged between 18 and 64 years, and possess a BMI of ≥40 kg m−2, or a BMI of ≥35 kg m−2 accompanied by one or more obesity-related co-morbidities, such as hypertension or type 2 diabetes mellitus.15 Exclusion criteria were: (1) known allergy to or contraindication to sugammadex, neostigmine, atropine, or ultrasound coupling gel; (2) known diaphragmatic paralysis or severe diaphragmatic dysfunction, significant pleural effusion, history of pneumonectomy, severe pulmonary dysfunction, or other significant respiratory or neurological disorders; (3) severe cardiac dysfunction (NYHA class III–IV), significant renal or hepatic impairment; (4) acute or chronic alcohol intoxication; (5) active infectious disease requiring systemic antibiotic therapy; (6) pre-existing chronic pain, chronic opioid use, psychotropic drug use, or history of drug abuse; (7) psychiatric illness or communication barriers. Withdrawal criteria for the primary analysis were: (1) conversion from laparoscopic to open surgery; (2) inability to obtain technically adequate diaphragmatic ultrasonographic images; (3) intraoperative blood loss ≥600 mL or haemoglobin level <80 g L−1; (4) unplanned reintubation in the post-anaesthesia care unit (PACU); (5) postoperative admission to the ICU; (6) withdrawal of consent.
Randomisation and Blinding
Participants were equally allocated to either the neostigmine group or the sugammadex group using computer-generated random numbers. Sequentially numbered, opaque, sealed envelopes were used to assure allocation concealment. Study drugs were prepared by staff not involved in clinical care or assessment in identical syringes labelled only with randomisation codes. Patients, anaesthesiologists, and assessing staff remained blinded.
Anaesthesia Methods
A standardized anaesthetic protocol was used. Monitoring included ECG, SpO2, end-tidal carbon dioxide, temperature, and invasive arterial pressure via radial catheter. Anaesthetic depth was assessed with bispectral index (BIS). Neuromuscular function was monitored using a piezoelectric neuromuscular monitor (GE Datex-Ohmeda E-NMT-00) with TOF stimulation (2 Hz, 0.2 ms, 60 mA) every 20s. Electrodes were positioned over the ulnar nerve with the sensor on the thumb. After calibration to a stable baseline TOF, the monitor continuously recorded TOF ratio and TOF count throughout surgery.
Drug doses were calculated using ideal body weight (IBW) or corrected body weight (CBW), defined as: IBW = Height (cm) – 100 (male) or 105 (female); CBW = IBW + 0.4 × (actual body weight – IBW). No premedication was given. After 3–5 min preoxygenation, anaesthesia was induced with etomidate 0.3 mg kg−1 IBW, sufentanil 0.5 μg kg−1 IBW, remifentanil 1 μg kg−1 IBW, and rocuronium 0.9 mg kg−1 IBW.
Propofol (2–5 mg kg−1 h−1 IBW) and remifentanil (0.1–0.3 μg kg−1 min−1 IBW) were continuously infused to maintain anaesthesia, and sevoflurane (1–2%) was breathed. Infusions were titrated to maintain BIS 40–60. Haemodynamics were kept within 20% of baseline using vasopressors/fluids as needed. Neuromuscular blockade was maintained at TOF count 0 and post-tetanic count 1–3; rocuronium 0.2 mg kg−1 IBW was given if TOF count ≥2. Intraperitoneal pressure was maintained at 14 mmHg. Thirty minutes before the procedure ended, sevoflurane was terminated, and no further rocuronium was administered. Propofol ended after abdominal manipulation, remifentanil at skin closure. Postoperative nausea and vomiting prophylaxis included dexamethasone 5 mg and tropisetron 2 mg; preventive analgesia was provided with intravenous flurbiprofen axetil 50 mg.
Intervention
Following surgery, patients received neuromuscular blockade reversal based on CBW when the TOF count reached 2: the neostigmine group was given 0.05 mg kg−1 along with 20 μg kg−1 of atropine, while the sugammadex group was given 2 mg kg−1 of sugammadex.16 Extubation occurred after TOF ratio ≥0.9 and meeting standard clinical criteria for extubation. Patients were transferred to the PACU, and TOF monitoring was discontinued post-extubation. Transfer to the ward followed haemodynamic stability. Analgesia (oxycodone/flurbiprofen axetil) targeted a visual analogue scale (VAS) score ≤4; patients with severe PONV received intravenous metoclopramide 10 mg.
Ultrasonographic Measurements
Diaphragmatic function was assessed by a single trained anaesthesiologist blinded to group allocation using a Wilson Navis ultrasound system at three timepoints: before the administration of neuromuscular blocking agents (T0), 10 min (T1), and 30 min (T2) after extubation. Patients were positioned semi-recumbent (head elevated 45°). Diaphragmatic excursion (DE) was measured using a low-frequency convex probe (1–5 MHz) placed in the right subcostal midclavicular line. After identifying the diaphragm via the liver window, excursion was recorded during quiet (DEQB) and deep breathing (DEDB) using M-mode (scan speed 25 mm s−1). Diaphragmatic thickening fraction (TF) was assessed with a high-frequency linear probe (4–15 MHz) placed over the right apposition zone (8th–9th intercostal space, midaxillary line), visualizing the three-layer structure (pleura-diaphragm-peritoneum). Thickness was measured at end-inspiration (TI) and end-expiration (TE) during deep breathing; TF was calculated as: [(TI – TE)/TE] × 100%. The average of three respiratory cycles was recorded for both DE and TF (Figure 1). Pain intensity assessed by visual analogue scores (VAS) and presence of PONV (yes/no) were also recorded at each timepoint.
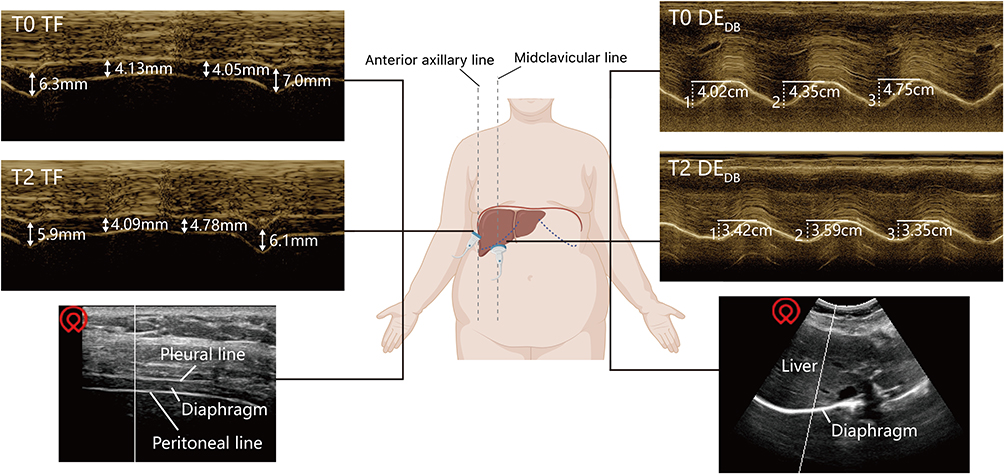 |
Figure 1 Schematic diagram illustrating the measurement of diaphragmatic thickening fraction (TF) and diaphragmatic excursion during deep breathing (DEDB), performed before induction of anaesthesia (T0) and 30 minutes after extubation (T2). |
Data Collection
The arterial oxygenation index (PaO2/FiO2) was calculated from blood gas analysis performed at T0 and T2 while patients were breathing room air. The time to TOF ratio of 0.9 after reversal agent administration was recorded. PACU data included: number of SpO2<90% episodes; breathing prompts (triggered by SpO2 drop>10 s or reduced chest movement); and PACU stay duration. We also collected the incidence of PPCs within 24 hours. PPCs were defined as the occurrence of any of the following: (1) respiratory failure (defined as PaO2 < 60 mmHg on room air, PaO2/FiO2 ratio < 300 mmHg, or SpO2 < 90% requiring supplemental oxygen); (2) pleural effusion; (3) atelectasis; (4) pneumothorax; (5) bronchospasm; (6) aspiration pneumonia; (7) pneumonia, assessed according to the diagnostic criteria established in previous literature17–19 and the EPCO classification.20
Outcomes
Demographic and intraoperative data were recorded. We analyzed the changes in all diaphragmatic function parameters from preoperative baseline to each postoperative time point. The primary outcome was ΔDEDB at T2. Secondary outcomes comprised: (1) ΔDEQB and ΔTF at T2; (2) ΔDEDB, ΔDEQB, and ΔTF at T1; (3) time to TOF ratio of 0.9; (4) PaO2/FiO2 at T2; (5) number of SpO2<90% episodes in PACU; (6) number of breathing prompts in PACU; (7) PACU stay duration; (8) 24-hour PPCs incidence.
Statistical Analysis
Data were analyzed using SPSS (version 29.0) and GraphPad Prism (version 9.0.0 for Mac OS). A two-sided P < 0.05 was considered significant. Normally distributed data are compared with the independent samples t-test; non-normal data are compared with the Mann–Whitney U-test (Hodges-Lehmann median difference [MD] and 95% CI reported). A Generalized Estimating Equations (GEE) model (continuous outcome, exchangeable working correlation) was used, in which we first tested the group-time interaction, followed by Bonferroni-adjusted comparisons if significant. Categorical data are presented as n (%) and analysed with the χ2-test (Relative Risk (RR) and 95% CI reported). Bonferroni correction was applied to two secondary outcome families: diaphragmatic recovery (5 tests) and respiratory recovery (6 tests). Mediation analysis (PROCESS Macro, Model 4) assessed whether ΔDEDB at T2 mediated the effect of sugammadex on PPCs, with adjustment for potential clinical confounders, using bootstrapping (5000 samples) with effects reported as log-odds and 95% Boot CI. ROC (Receiver Operating Characteristic) analysis evaluated ΔDEDB’s predictive value for hypoxaemia (defined as PaO2/FiO2 ≤300 mmHg on room air), reporting AUC (95% CI) and the optimal cut-off via Youden’s index.
Sample Size Calculations
As no prior data existed for ΔDEDB comparing sugammadex and neostigmine in morbid obesity, the sample size was determined using data obtained from our preliminary investigations conducted prior to this trial. The mean±SD ΔDEDB for sugammadex vs neostigmine were 0.018±0.47 cm vs 0.34±0.42 cm. Using PASS 15.0 (90% power, α=0.05), 42 patients per group were required. With a 20% dropout rate, 106 patients were needed.
Results
Of 140 patients assessed for eligibility, 34 were excluded, leaving 106 for analysis (Figure 2). Two patients (neostigmine group) were excluded due to inadequate ultrasonographic images. Between groups, patient characteristics were similar (Tables 1 and 2).
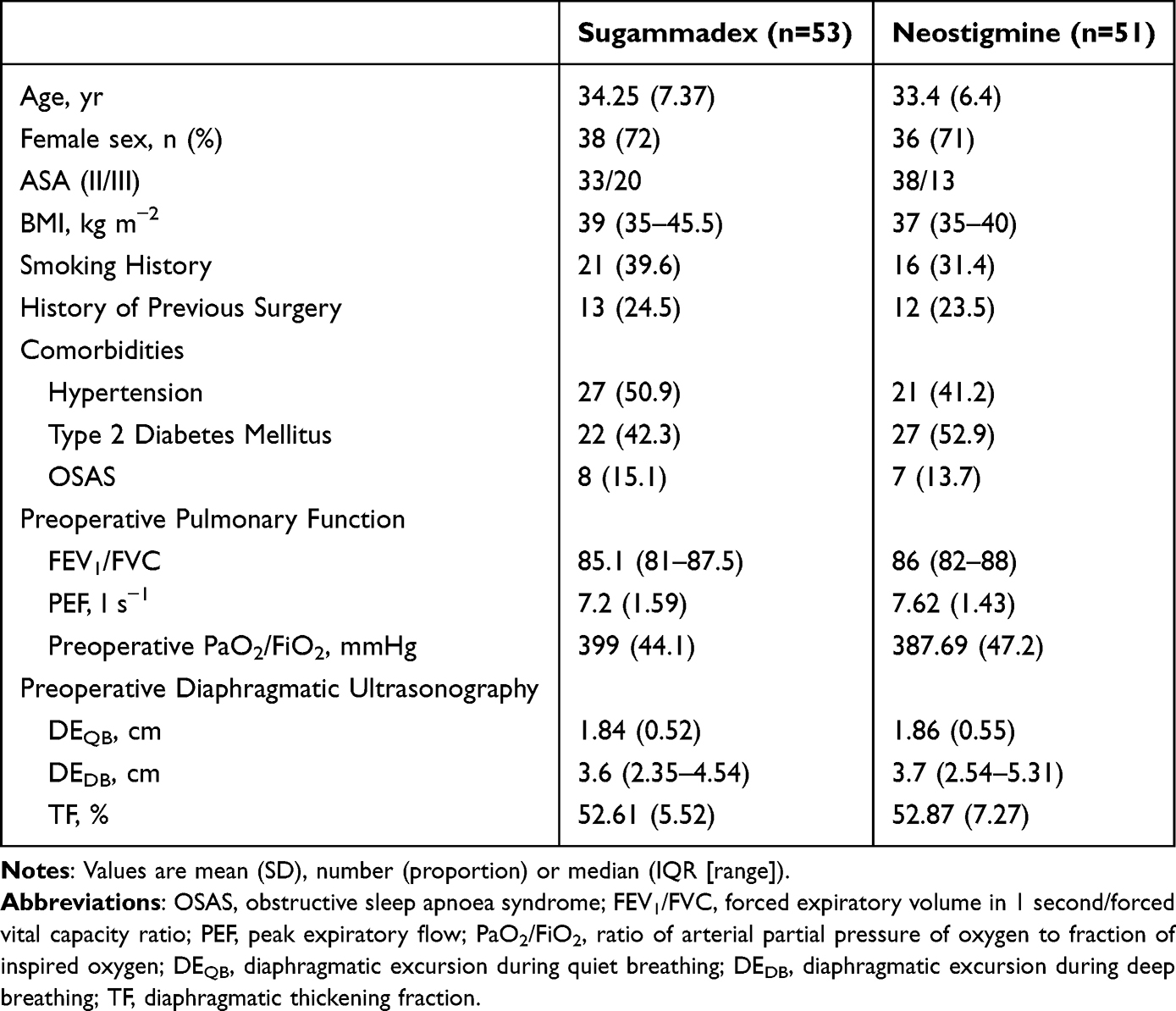 |
Table 1 Baseline Characteristics of Patients Receiving Sugammadex or Neostigmine for Bariatric Surgery |
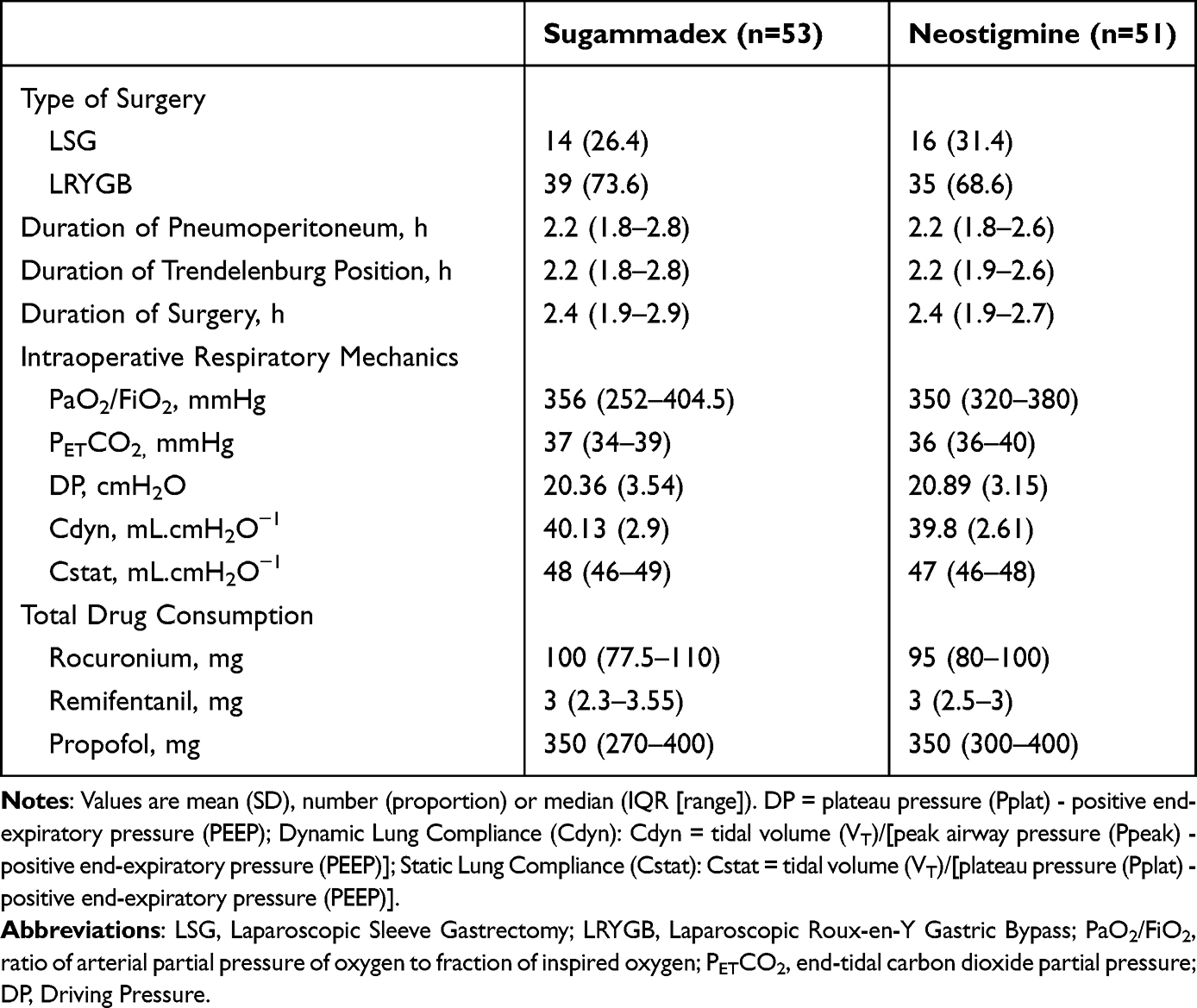 |
Table 2 Perioperative Characteristics of Patients Receiving Sugammadex or Neostigmine for Bariatric Surgery |
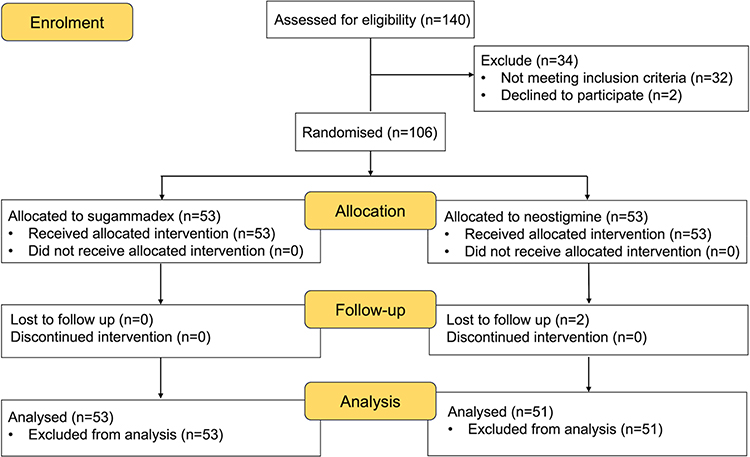 |
Figure 2 Study flow diagram. |
Primary Outcome
The sugammadex group showed a significantly smaller ΔDEDB at T2 than the neostigmine group (median [IQR]: 0.05 [0 to 0.11]cm vs. 0.28 [0.05 to 0.9]cm; MD, 0.19; 95% CI, 0.08 to 0.29; P<0.001) (Table 3).
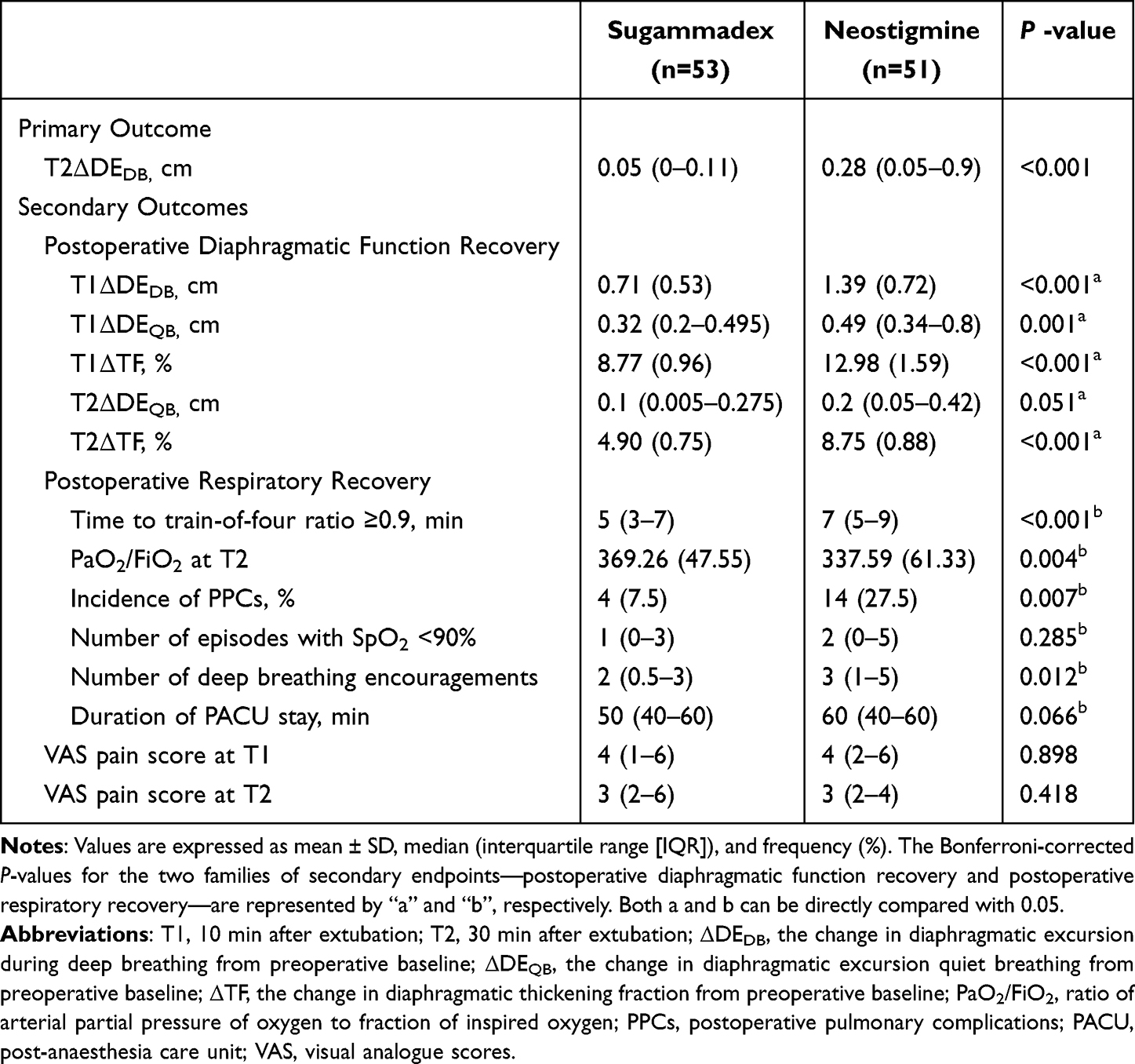 |
Table 3 Primary and Secondary Outcomes in Patients Receiving Sugammadex or Neostigmine for Bariatric Surgery |
Compared with the neostigmine group, the sugammadex group experienced a considerably decreased incidence of PPCs (7.5% vs 27.5%; RR = 0.216, 95% CI: 0.066 to 0.709; P=0.007). The distribution of PPC subtypes was as follows: in the neostigmine group, a total of 14 events occurred, including respiratory failure in 7 cases (13.7%), atelectasis in 6 cases (11.7%), and pleural effusion in 1 case (1.9%); in the sugammadex group, a total of 4 events occurred, including atelectasis in 3 cases (5.6%) and respiratory failure in 1 case (1.9%). Due to the limited number of events in each subtype, between-group statistical comparisons were not performed. An exploratory path analysis, adjusted for BMI, surgery duration, total rocuronium dose, OSAS, and Diabetes, was conducted to assess the potential role of diaphragmatic function (ΔDEDB at T2). ΔDEDB at T2 remained significantly lower in the sugammadex group (β = −0.350, P<0.001). However, its association with PPCs risk was not significant (β = 0.875, P=0.177). Consequently, the indirect effect of sugammadex on PPCs through ΔDEDB at T2 was not statistically significant (β = −0.306, 95% Bootstrap CI: −1.098 to 0.159). The direct protective effect of sugammadex on PPCs remained significant after adjustment (β = −2.128, P=0.0079).
Secondary Outcomes
Postoperative Diaphragmatic Function Recovery
At T1, the sugammadex group showed significantly smaller changes from baseline in ΔDEDB (MD, 0.63; 95% CI, 0.4 to 0.92), ΔDEQB (MD, 0.18; 95% CI, 0.08 to 0.3), and ΔTF (MD, 0.042; 95% CI, 0.036 to 0.048) compared with the neostigmine group (all Bonferroni-corrected P≤0.001). At T2, the ΔTF remained significantly smaller in the sugammadex group (MD, 0.039; 95% CI, 0.035 to 0.042; Bonferroni-corrected P<0.001), while the difference in ΔDEQB between groups was not statistically significant (MD, 0.08; 95% CI, 0 to 0.2; Bonferroni-corrected P=0.051) (Table 3).
GEE analysis, adjusted for BMI and baseline (T0) diaphragmatic function, showed different temporal trends in diaphragmatic recovery between groups (Figure 3). Significant group-by-time interactions occurred for DEDB (P<0.001), DEQB (P=0.004), and TF (P=0.004). In both groups, values at T1 and T2 differed significantly from those at T0 (all P<0.001). The sugammadex group had higher DEDB and TF at T1 and T2 (all P<0.001), and higher DEQB at T1 (P<0.001) and T2 (P=0.006) than the neostigmine group. Each 1 kg m−2 increase in BMI was associated with a 0.02 cm reduction in DEDB (β =−0.02; 95% CI: −0.027 to −0.013; P<0.001), but no associations were seen between BMI and DEQB (P=0.073) or TF (P=0.696).
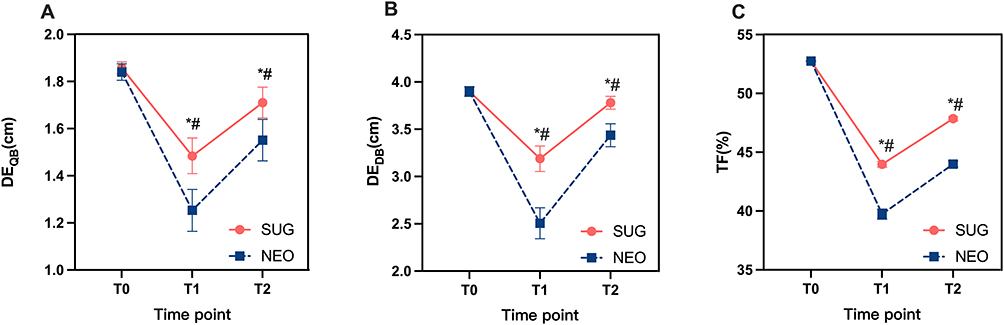 |
Figure 3 Diaphragmatic function parameters between the two patient groups at each time point. (A) Comparison of diaphragmatic excursion during quiet breathing (DEQB) between patient groups at each time point; (B) Comparison of diaphragmatic excursion during deep breathing (DEDB) between patient groups at each time point; (C) Comparison of diaphragmatic thickening fraction (TF) between patient groups at each time point. T0: before induction; T1: 10 min after extubation; T2: 30 min after extubation; *P < 0.05 (sugammadex group vs Neostigmine group at the respective time point). #: P < 0.001 (each time point within a group vs baseline (T0)). |
Postoperative Respiratory Recovery
The sugammadex group had a shorter time to TOF ratio≥0.9 (median[IQR]: 5[3 to 7]min vs 7[5 to 9]min; MD, 2 min; 95% CI, 1 to 3 min; Bonferroni-corrected P<0.001), higher PaO2/FiO2 at T2 (Bonferroni-corrected P=0.004), and fewer deep breathing prompts (Bonferroni-corrected P=0.012) than the neostigmine group. There were no discernible variations in the quantity of SpO2<90% occurrences, (Bonferroni-corrected P=0.285), PACU stay duration (Bonferroni-corrected P=0.066). VAS pain ratings showed no discernible variations at T1 or T2 in either group, additionally, no episodes of PONV were recorded in either group at these time points (Table 3).
ROC analysis showed that ΔDEDB at T2 had moderate predictive value for postoperative hypoxemia (defined as PaO2/FiO2 ≤300 mmHg; AUC=0.7854; 95% CI: 0.6515 to 0.9193; P<0.001) (Supplementary Figure 1). At the optimal cutoff of 0.215 cm, sensitivity was 86.7%, specificity 75.3% (Youden’s index = 0.62), Positive Predictive Value 40%, and Negative Predictive Value 97.1%, indicating high sensitivity and Negative Predictive Value but limited Positive Predictive Value. The predictive performance of ΔDEDB at T2 (AUC = 0.7854) was superior to that of ΔDEDB at T1 (AUC = 0.6981), ΔDEQB at T1 (AUC = 0.7509), and ΔDEQB at T2 (AUC = 0.7577).
Discussion
Significantly less time was required to attain a TOF ratio of 0.9 in the sugammadex group compared to the neostigmine group. This finding is unsurprising and consistent with previous studies.16 Our results further demonstrate that the sugammadex cohort maintained a statistically significant advantage in diaphragmatic contractile function throughout the 30-minute post-extubation period relative to the neostigmine group. The changes from baseline in DEDB, DEQB, and TF at T1, and in DEDB and TF at T2, were all significantly smaller in the sugammadex group, indicating more rapid and complete functional recovery. Although the effect size estimated from the pilot data was overestimated, the prespecified sample size successfully detected a statistically significant between-group difference in the primary outcome, confirming the adequacy of the sample size calculation for the present study. Although the between-group difference in ΔDEDB at T2 was modest (0.19 cm), its occurrence during the immediate post-extubation period reflects a meaningful acceleration in early neuromuscular recovery, which may carry potential clinical implications for morbidly obese patients with limited respiratory reserve. GEE analysis revealed differing temporal trends in ΔDEDB between the two groups. These differences stem from the distinct mechanisms of each reversal agent: neostigmine, an acetylcholinesterase inhibitor, increases acetylcholine to competitively antagonize neuromuscular blocking agents (NMBAs), but in morbid obesity, adipose tissue may sequester and later release NMBAs, potentially leading to recurarization21 and inadequate neostigmine concentrations. In contrast, sugammadex forms specific complexes with aminosteroid NMBAs (eg, rocuronium), inactivating and promoting their renal excretion,22 thereby lowering plasma concentrations and restoring neuromuscular function more rapidly and completely. These results confirm that sugammadex facilitates quicker diaphragmatic recovery in morbid obesity, promoting early spontaneous breathing and aiding in the prevention of postoperative residual neuromuscular blockade.
A notable finding was the significant between-group difference in ΔDEDB at T2, but not in ΔDEQB. This is physiologically explained by the fact that quiet breathing requires only about 8% of the maximal transdiaphragmatic pressure generated during a deep inspiration.23,24 By 30 minutes post-extubation, neuromuscular recovery in both groups was sufficient for quiet breathing, potentially masked in morbidly obese patients by compensatory chest breathing and accessory muscle use. Deep breathing, requiring maximal diaphragmatic contraction, is a more robust strength test. The superior DEDB recovery, higher oxygenation index, and lower 24-hour PPCs incidence (7.5% vs 27.5%) with sugammadex all indicate enhanced respiratory recovery.
The exploratory path analysis, conducted with adjustment for key perioperative confounders, did not yield a statistically significant indirect effect of sugammadex on PPCs through diaphragmatic function. This suggests that the clinical advantage of sugammadex in reducing PPCs is likely mediated through mechanisms beyond a singular improvement in early diaphragmatic recovery. This finding aligns with the established view that postoperative pulmonary complications are more strongly linked to impaired coordination of upper airway and pharyngeal muscles rather than isolated diaphragmatic dysfunction.7 Therefore, the superior efficacy of sugammadex may stem from its ability to ensure more complete and rapid recovery of global neuromuscular function, thereby enhancing the integrity of the entire respiratory system and airway protective reflexes.
Although extubation was carried out after TOF ratio ≥0.9 in both groups, diaphragmatic function had not fully returned to baseline by the end of observation. This aligns with reports that respiratory muscle strength may remain impaired even at TOF ratio=1, possibly due to persistent neuromuscular transmission deficits.25 In morbid obesity, intra-abdominal fat accumulation and laparoscopic surgery-related pneumoperitoneum induced increased intra-abdominal pressure may mechanically compromise diaphragmatic function. Additionally, adipose-derived pro-inflammatory cytokines (eg, TNF-α26) might impair diaphragmatic mitochondrial function and oxidative phosphorylation,27 limiting its capacity for deep breathing and contributing to prolonged diaphragmatic function recovery.
Although prior studies indicate sugammadex enhances immediate post-extubation diaphragmatic recovery compared with neostigmine,13,14 the immediate post-extubation period is often complicated by cardiovascular instability (eg, hypertension, tachycardia), patient movement, and retained secretions, which can impair patient cooperation and the reliability of ultrasound measurements for diaphragmatic indices. Allowing 10 minutes post-extubation improves patient adaptation to spontaneous breathing and compliance with deep inspiration commands, increasing the accuracy of measurements at 10 min post-extubation (T1).
Morbidly obese patients have reduced oxygen reserves. Diaphragmatic dysfunction often precedes oxygen desaturation. Ultrasonographic diaphragmatic excursion is a non-invasive, safe,28 and easily operable bedside tool offering real-time assessment, avoiding delays from difficult blood gas sampling (eg, challenging vascular access in obese patients). Monitoring ΔDEDB is clinically valuable post-bariatric surgery. ROC analysis showed that ΔDEDB at T2 has high sensitivity (86.7%) for predicting postoperative hypoxaemia. A ΔDEDB<0.215 cm at 30 min post-extubation may prompt early intervention (eg, non-invasive ventilation) to prevent hypoxaemia-related complications. However, this finding is derived from a single-center exploratory study with a limited sample size and may be subject to overfitting. External validation in larger, multicenter cohorts is warranted before this threshold can be considered for clinical application.
This study employed acceleromyography combined with kinemyographic signal processing for neuromuscular monitoring. While this method is commonly used clinically, its underlying principle differs from electromyography, which measures the compound muscle action potential more directly. It is noteworthy that kinemyography may overestimate the TOF ratio.29 This might explain why the recovery time in the neostigmine group in our study (median 7 minutes, IQR 5–9) was shorter than that reported in some previous studies.25,30
This study has several limitations. First, although ultrasonographic measurements were standardized, this technique remains partially dependent on patient effort; variability in inspiratory depth due to inconsistent patient cooperation may therefore introduce measurement bias. Furthermore, despite the use of a single trained and blinded operator to ensure consistency, intra-observer variability and potential subconscious bias cannot be entirely excluded. Second, PPCs were assessed only within the first 24 hours postoperatively, a window that may fail to capture delayed-onset complications (eg, pneumonia or respiratory failure occurring 48–72 hours after surgery). This limitation could lead to an underestimation of the overall incidence of PPCs. Third, the findings are based on a specific cohort of patients aged 18–55 years undergoing laparoscopic bariatric surgery, which limits the generalizability of our results to other surgical procedures (eg, open bariatric surgery, thoracic surgery) or age groups (eg, elderly patients, adolescents). Regarding future directions, the use of electromyography, which offers higher precision, may be considered to monitor the depth of neuromuscular blockade. Additionally, this study did not include a cost-effectiveness analysis. Although sugammadex has a higher acquisition cost than neostigmine, determining whether its clinical benefits translate into overall healthcare cost savings warrants further investigation.
Conclusion
In conclusion, in morbidly obese patients with moderate neuromuscular block (TOF count of 2), sugammadex facilitates more rapid recovery of diaphragmatic and respiratory function than neostigmine, with benefits for at least 30 minutes after extubation. Future studies should examine the long-term effects of sugammadex on diaphragmatic function and compare both agents under guideline-recommended minimal block (TOF ratio ≥ 0.4) using electromyography (EMG)-based monitoring for more precise and valid assessment.
Data Sharing Statement
All data will be shared from the corresponding author (Guanglei Wang).
Acknowledgments
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
No funding was received.
Disclosure
All authors declare no competing interests.
References
1. Sieck GC, Fogarty MJ. Diaphragm muscle: a pump that can not fail. Physiol Rev. 2025;105(4):2589–11. doi:10.1152/physrev.00043.2024
2. Nguyen-Huu T, Molgó J, Servent D, Duvaldestin P. Resistance to D-tubocurarine of the rat diaphragm as compared to a limb muscle: influence of quantal transmitter release and nicotinic acetylcholine receptors. Anesthesiology. 2009;110(5):1011–1015. doi:10.1097/ALN.0b013e31819faeaa
3. Fu X, Wang Z, Wang L, et al. Increased diaphragm echodensity correlates with postoperative pulmonary complications in patients after major abdominal surgery: a prospective observational study. BMC Pulm Med. 2022;22(1):400. doi:10.1186/s12890-022-02194-6
4. Sood A. Altered resting and exercise respiratory physiology in obesity. Clin Chest Med. 2009;30(3):445–vii. doi:10.1016/j.ccm.2009.05.003
5. Buras ED, Converso-Baran K, Davis CS, et al. Fibro-adipogenic remodeling of the diaphragm in obesity-associated respiratory dysfunction. Diabetes. 2019;68(1):45–56. doi:10.2337/db18-0209
6. Rodrigues GC, Rocha NN, Maia LA, et al. Impact of experimental obesity on diaphragm structure, function, and bioenergetics. J Appl Physiol. 2020;129(5):1062–1074. doi:10.1152/japplphysiol.00262.2020
7. Fuchs-Buder T, Schmartz D. Neuromuskuläre Restblockade [Residual neuromuscular blockade]. Anaesthesist. 2017;66(6):465–476. doi:10.1007/s00101-017-0325-1
8. Carron M, Tamburini E, Ieppariello G, Linassi F. Reversal of neuromuscular block with sugammadex compared with neostigmine and postoperative pulmonary complications in obese patients: meta-analysis and trial sequential analysis. Br J Anaesth. 2023;130(6):e461–e463. doi:10.1016/j.bja.2023.03.003
9. Bluth T, Serpa Neto A, Schultz MJ, et al; Writing Committee for the PROBESE Collaborative Group of the PROtective VEntilation Network (PROVEnet) for the Clinical Trial Network of the European Society of Anaesthesiology. Effect of intraoperative high positive end-expiratory pressure (PEEP) with recruitment maneuvers vs low PEEP on postoperative pulmonary complications in obese patients: a randomized clinical trial. JAMA. 2019;321(23):2292–2305. doi:10.1001/jama.2019.7505
10. Mazzinari G, Díaz-Cambronero O, Garutti I, Errando CL, Ferrando C; iPROVE-OLV investigators. Impact of neuromuscular block monitoring and reversal on postoperative pulmonary complications in thoracic surgery: a Bayesian analysis of the iPROVE-OLV trial. Br J Anaesth. 2025;135(5):1428–1440. doi:10.1016/j.bja.2024.11.041
11. Cammu G. Residual neuromuscular blockade and postoperative pulmonary complications: what does the recent evidence demonstrate? Curr Anesthesiol Rep. 2020;10(2):131–136. doi:10.1007/s40140-020-00388-4
12. Kheterpal S, Vaughn MT, Dubovoy TZ, et al. Sugammadex versus neostigmine for reversal of neuromuscular blockade and postoperative pulmonary complications (STRONGER): a multicenter matched cohort analysis. Anesthesiology. 2020;132(6):1371–1381. doi:10.1097/ALN.0000000000003256
13. Kirmeier E, Eriksson LI, Lewald H, et al; POPULAR Contributors. Post-anaesthesia pulmonary complications after use of muscle relaxants (POPULAR): a multicentre, prospective observational study. Lancet Respir Med. 2019;7(2):129–140. doi:10.1016/S2213-2600(18)30294-7
14. Cappellini I, Ostento D, Loriga B, Tofani L, De Gaudio AR, Adembri C. Comparison of neostigmine vs. sugammadex for recovery of muscle function after neuromuscular block by means of diaphragm ultrasonography in microlaryngeal surgery: a randomised controlled trial. Eur J Anaesthesiol. 2020;37(1):44–51. doi:10.1097/EJA.0000000000001055
15. Koskinas KC, Van Craenenbroeck EM, Antoniades C, et al. Obesity and cardiovascular disease: an ESC clinical consensus statement. Eur J Prev Cardiol. 2025;32(3):184–220. doi:10.1093/eurjpc/zwae279
16. Gaszynski T, Szewczyk T, Gaszynski W. Randomized comparison of sugammadex and neostigmine for reversal of rocuronium-induced muscle relaxation in morbidly obese undergoing general anaesthesia. Br J Anaesth. 2012;108(2):236–239. doi:10.1093/bja/aer330
17. Miskovic A, Lumb AB. Postoperative pulmonary complications. Br J Anaesth. 2017;118(3):317–334. doi:10.1093/bja/aex002
18. Qaseem A, Snow V, Fitterman N, et al. Clinical efficacy assessment subcommittee of the American college of physicians: risk assessment for and strategies to reduce perioperative pulmonary complications for patients undergoing noncardiothoracic surgery: a guideline from the American college of physicians. Ann Intern Med. 2006;144(8):575–580. doi:10.7326/0003-4819-144-8-200604180-00008
19. Smetana GW. Postoperative pulmonary complications: an update on risk assessment and reduction. Cleve Clin J Med. 2009;76(10 suppl 4):S60–S65. doi:10.3949/ccjm.76.s4.10
20. Jammer I, Wickboldt N, Sander M, et al. Standards for definitions and use of outcome measures for clinical effectiveness research in perioperative medicine: European perioperative clinical outcome (EPCO) definitions: a statement from the ESA-ESICM joint taskforce on perioperative outcome measures. Eur J Anaesthesiol. 2015;32(2):88–105. doi:10.1097/EJA.0000000000000118
21. Ekinci O, Gulmez D, Subasi F, Ozgultekin A, Demiroluk O. Neostigmine versus sugammadex on post-operative recovery following bariatric surgery. North Clin Istanb. 2022;9(4):311–316. doi:10.14744/nci.2021.94715
22. Chandrasekhar K, Togioka BM, Jeffers JL. Sugammadex. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023.
23. Fogarty MJ, Mantilla CB, Sieck GC. Breathing: motor control of diaphragm muscle. Physiology. 2018;33(2):113–126. doi:10.1152/physiol.00002.2018
24. Sieck GC. Physiological effects of diaphragm muscle denervation and disuse. Clin Chest Med. 1994;15(4):641–659. doi:10.1016/S0272-5231(21)00958-8
25. Huang C, Wang X, Gao S, et al. Sugammadex versus neostigmine for recovery of respiratory muscle strength measured by ultrasonography in the postextubation period: a randomized controlled trial. Anesth Analg. 2023;136(3):559–568. doi:10.1213/ANE.0000000000006219
26. Tzanavari T, Giannogonas P, Karalis KP. TNF-alpha and obesity. Curr Dir Autoimmun. 2010;11:145–156.
27. Davizon-Castillo P, McMahon B, Aguila S, et al. TNF-α-driven inflammation and mitochondrial dysfunction define the platelet hyperreactivity of aging. Blood. 2019;134(9):727–740. doi:10.1182/blood.2019000200
28. Lang J, Liu Y, Zhang Y, Huang Y, Yi J. Peri-operative diaphragm ultrasound as a new method of recognizing post-operative residual curarization. BMC Anesthesiol. 2022;22(1):25. doi:10.1186/s12871-022-01565-0
29. Hemmerling TM, Donati F. The M-NMT mechanosensor cannot be considered as a reliable clinical neuromuscular monitor in daily anesthesia practice. Anesth Analg. 2002;95(6):1826–1827. doi:10.1097/00000539-200212000-00086
30. Sun Y, Sun S, Chen R, et al. Diaphragm ultrasonography as a monitor in assessing antagonistic effect of sugammadex on rocuronium in patients with Child-Pugh grades A and B. Front Med Lausanne. 2024;11:1370021. doi:10.3389/fmed.2024.1370021
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Sugammadex vs Neostigmine for Reversal of Neuromuscular Blockade and Association with Postoperative Atelectasis After Video-Assisted Thoracoscopic Surgery: A Propensity Score-Matched Cohort Study
Hung KC, Weng HL, Wu JY, Hsu CW, Yang CP, Lai YC, Chen IW
Drug Design, Development and Therapy 2026, 20:593657
Published Date: 6 March 2026