Back to Journals » International Journal of Women's Health » Volume 18
Impact of Short-Term Estrogen Therapy on Endometrial Polyps Recurrence in Women with Intrauterine Adhesion and Endometrial Polyps: A Retrospective Cohort Study
Authors Jiang S, Yi X, Zheng M, Ouyang Y, Chen Y, Xie M, Chen S, Chen D, Zhong X
Received 30 December 2025
Accepted for publication 6 March 2026
Published 10 March 2026 Volume 2026:18 577906
DOI https://doi.org/10.2147/IJWH.S577906
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vinay Kumar
Sushi Jiang,1– 3,* Xinyu Yi,3,* Miaoxian Zheng,1,2 Yanlan Ouyang,4 Yaxiao Chen,1,2 Meiqing Xie,1,2 Shengfu Chen,1,2 Dongmei Chen,1,2 Xiaozhu Zhong1,2
1Department of Obstetrics and Gynecology, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, People’s Republic of China; 2Guangdong Provincial Clinical Research Center for Obstetrical and Gynecological Diseases, Guangzhou, People’s Republic of China; 3Department of Reproductive Medicine, Guangzhou First People’s Hospital, School of Medicine, Guangzhou Medical University, Guangzhou, People’s Republic of China; 4Department of Obstetrics and Gynecology, Huizhou First Maternal and Child Health Care Hospital, Huizhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaozhu Zhong; Dongmei Chen, Email [email protected]; [email protected]
Objective: To investigate whether short-term postoperative estrogen-related therapy is associated with recurrence of intrauterine adhesions (IUA), endometrial polyps (EPs), and pregnancy outcomes in women with concomitant IUA and EPs.
Methods: This single-center retrospective cohort study included women (18– 45 years) diagnosed with both IUA and EPs who underwent concurrent hysteroscopic transcervical resection of adhesions (TCRA) and polypectomy from January 2019 to June 2024. Patients were grouped by postoperative regimen: (1) estradiol–dydrogesterone sequential therapy (Femoston; estradiol 2 mg/dydrogesterone 10 mg; 2– 3 months), (2) combined oral contraceptive (Yaz; ethinylestradiol 0.02 mg/drospirenone 3 mg; 3 months), or (3) no hormonal therapy. Recurrence was confirmed by transvaginal ultrasound and/or hysteroscopy.
Results: A total of 166 women were included (sequential therapy, n=47; COC, n=32; no hormone, n=87). Baseline polyp multiplicity differed among groups (P=0.003), with a higher proportion of multiple EPs in the COC group. Postoperative IUD/balloon placement also differed among groups (P=0.012). Overall recurrence rates were 6.6% for IUA and 4.8% for EPs. No statistically significant differences were observed among groups in postoperative menstrual changes, recurrence rates, time to recurrence, or pregnancy outcomes (all P> 0.05). Follow-up duration did not differ significantly among groups.
Conclusion: In this retrospective cohort, no statistically significant differences were observed among short-term sequential estrogen–progestin therapy, COC use, and no hormonal therapy with respect to IUA recurrence, EP recurrence, or pregnancy outcomes. Short-term estradiol–dydrogesterone therapy was not associated with increased EP recurrence in women with IUA and a single EP. These findings are observational and should be confirmed in prospective studies.
Keywords: intrauterine adhesions, endometrial polyps, estrogen, recurrence, pregnancy outcomes
Introduction
Intrauterine adhesions (IUA) and endometrial polyps (EPs) are common intrauterine disorders that can adversely affect reproductive outcomes, including reduced pregnancy rates and increased miscarriage rates.1,2 IUA (Asherman’s syndrome) often results from injury to the basal endometrium following intrauterine procedures, leading to fibrous tissue formation and partial or complete obliteration of the uterine cavity.3,4 Hysteroscopy is considered the gold standard for diagnosis and for evaluating postoperative uterine cavity restoration.
EPs are a common cause of abnormal uterine bleeding and are frequently detected on transvaginal ultrasound, whereas hysteroscopic resection is the definitive treatment.5,6 Recurrence rates after polypectomy vary widely,7 and recurrence is associated with factors such as polyp multiplicity and polyp size.8
Postoperative management after hysteroscopic adhesiolysis aims to prevent re-adhesion and to promote endometrial regeneration. The American Association of Gynecologic Laparoscopists (AAGL) and the European Society of Gynecological Endoscopy (ESGE) recommend cyclic estrogen–progestin therapy after transcervical resection of adhesions (TCRA) to facilitate endometrial repair.9 However, estrogen exposure is also implicated in the pathogenesis of EPs, creating a clinical dilemma for women with concomitant IUA and EPs: estrogen may support endometrial healing after adhesiolysis, yet it may theoretically increase the risk of polyp recurrence.
Evidence guiding postoperative hormonal strategies specifically for women with coexisting IUA and EPs remains limited, and postoperative regimens are often individualized in real-world practice. Therefore, we conducted a retrospective cohort study to evaluate whether short-term postoperative estrogen-related therapy is associated with recurrence of IUA and EPs and with pregnancy outcomes in women undergoing concurrent hysteroscopic adhesiolysis and polypectomy.
Materials and Methods
Study Design and Population
This was a single-center retrospective cohort study approved by the Institutional Review Board of Sun Yat-sen Memorial Hospital, Sun Yat-sen University (SYSKY-2025-070-01). Women aged 18–45 years diagnosed with both IUA and EPs who underwent concurrent hysteroscopic TCRA and polypectomy between January 2019 and June 2024 were eligible. Patients with incomplete clinical data or loss to follow-up were excluded. Informed consent was obtained from patients. All procedures involving human participants were performed in accordance with the Declaration of Helsinki.
Treatment Groups and Postoperative Hormonal Regimens
Participants were categorized according to the postoperative hormonal regimen received (non-randomized, real-world practice):
- Group 1 (Sequential therapy): cyclic estradiol–dydrogesterone sequential therapy (Femoston; estradiol 2 mg/dydrogesterone 10 mg) for 2–3 months postoperatively.
- Group 2 (COC group): combined oral contraceptive (Yaz; ethinylestradiol 0.02 mg/drospirenone 3 mg) for 3 months postoperatively.
- Group 3 (No-hormone group): no postoperative hormonal medication.
Regimen selection was based on clinical judgement considering adhesion severity and polyp characteristics; therefore, selection bias and confounding by indication are possible.
Surgical Procedure and Postoperative Management
All surgeries were performed by experienced hysteroscopic surgeons under general anesthesia using a STORZ hysteroscopic system. IUA severity was assessed intraoperatively according to the American Fertility Society (AFS) classification (1988).10 Adhesiolysis was performed using hysteroscopic scissors or a needle electrode. Polypectomy was performed using a loop electrode until the uterine cavity anatomy was restored.
Immediately after surgery, depending on intraoperative findings, an intrauterine device (IUD) or balloon was placed, sodium hyaluronate gel was applied, or no adjuvant barrier was used. If placed, the IUD/balloon was typically removed at second-look hysteroscopy approximately 2–3 months postoperatively.
Outcome Measures and Follow-Up
Primary outcomes were recurrence of IUA and EPs, confirmed by transvaginal ultrasound and/or hysteroscopy, and time to recurrence. Time to recurrence was defined as the interval from the index surgery date to the first confirmatory examination date at which recurrence was identified. If recurrence was detected during routine second-look hysteroscopy (typically ~2–3 months postoperatively), that date was used.
Secondary outcomes included patient-reported postoperative menstrual volume change (less/same/more than before) and pregnancy outcomes among women attempting conception during follow-up. Follow-up was conducted through outpatient visits, telephone contact, and ultrasound review. Chronic endometritis was diagnosed histopathologically by the presence of plasma cells in the endometrial stroma.11
Follow-up duration did not differ significantly among groups; detailed follow-up time will be summarized in the final dataset table.
Statistical Analysis
Normality was assessed using the Kolmogorov–Smirnov test. Normally distributed continuous variables are presented as mean ± standard deviation and compared using one-way ANOVA. Non-normally distributed variables are presented as median (interquartile range) and compared using the Kruskal–Wallis H-test. Categorical variables are presented as n (%) and compared using the chi-square test or Fisher’s exact test, as appropriate. Statistical analysis was performed using SPSS 25.0 (IBM), with two-sided P<0.05 considered statistically significant.
Results
Participant Selection and Baseline Characteristics
After eligibility assessment, 166 women were included: 47 in the sequential therapy group, 32 in the COC group, and 87 in the no-hormone group (Figure 1). Baseline characteristics and outcomes are presented in Table 1.
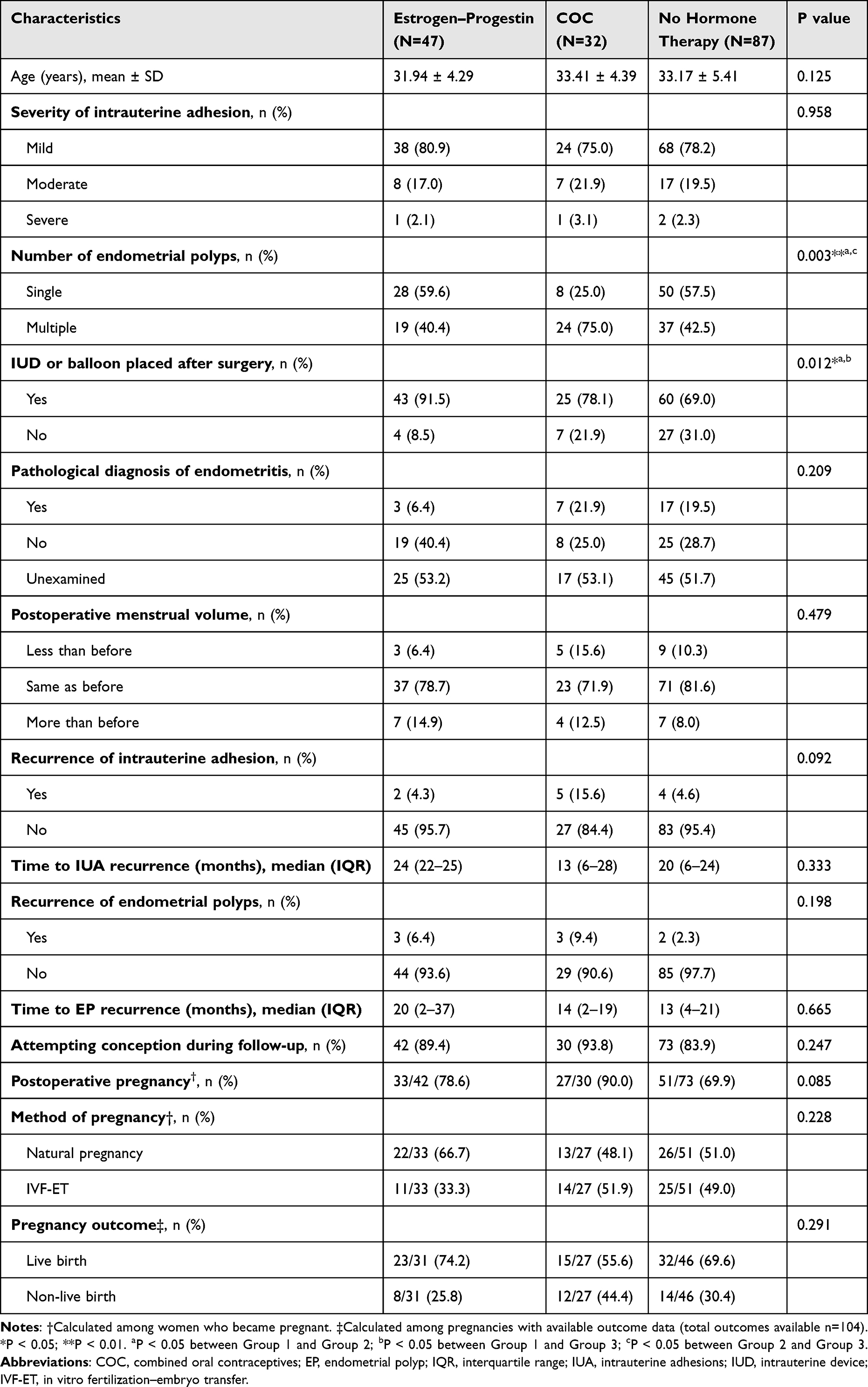 |
Table 1 Comparison of Clinical Characteristics and Pregnancy Outcomes Among the Three Groups |
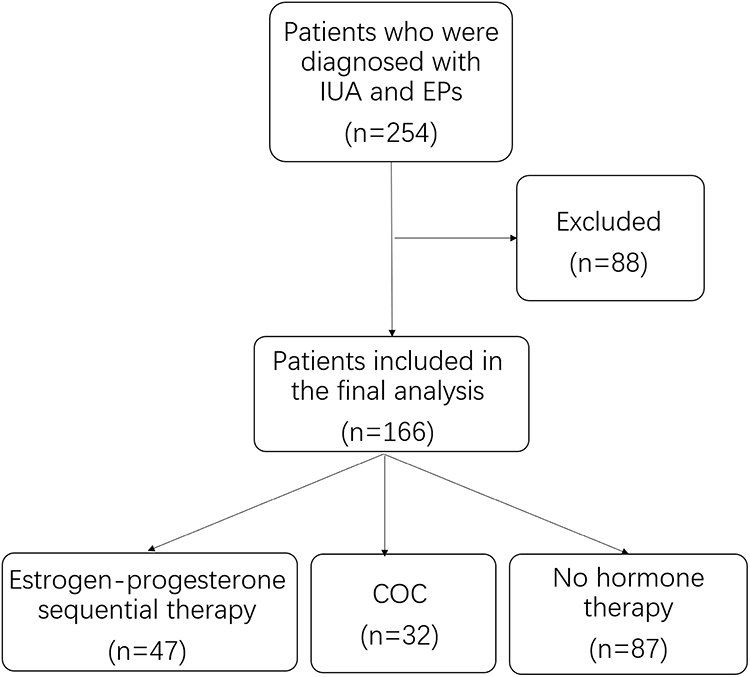 |
Figure 1 Flow chart of participant selection and group allocation. |
The proportion of multiple EPs differed significantly among groups (P=0.003), with a higher proportion in the COC group. Postoperative IUD/balloon placement also differed among groups (P=0.012). Age distribution and IUA severity were comparable among groups (Table 1).
Recurrence and Pregnancy Outcomes
Overall recurrence rates were 6.6% (11/166) for IUA and 4.8% (8/166) for EPs. No statistically significant differences were observed among the three groups in postoperative menstrual volume change, IUA recurrence, EP recurrence, time to recurrence, or pregnancy outcomes (all P>0.05; Table 1).
Among women attempting conception during follow-up (n=145; Group 1 n=42, Group 2 n=30, Group 3 n=73), postoperative pregnancy occurred in 111 women (76.6%). Pregnancy outcomes did not differ significantly among groups (Table 1). Comparisons between women with and without IUA recurrence (Table 2) and between women with and without EP recurrence (Table 3) showed no statistically significant differences in baseline characteristics or pregnancy outcomes; however, recurrence subgroup sizes were small.
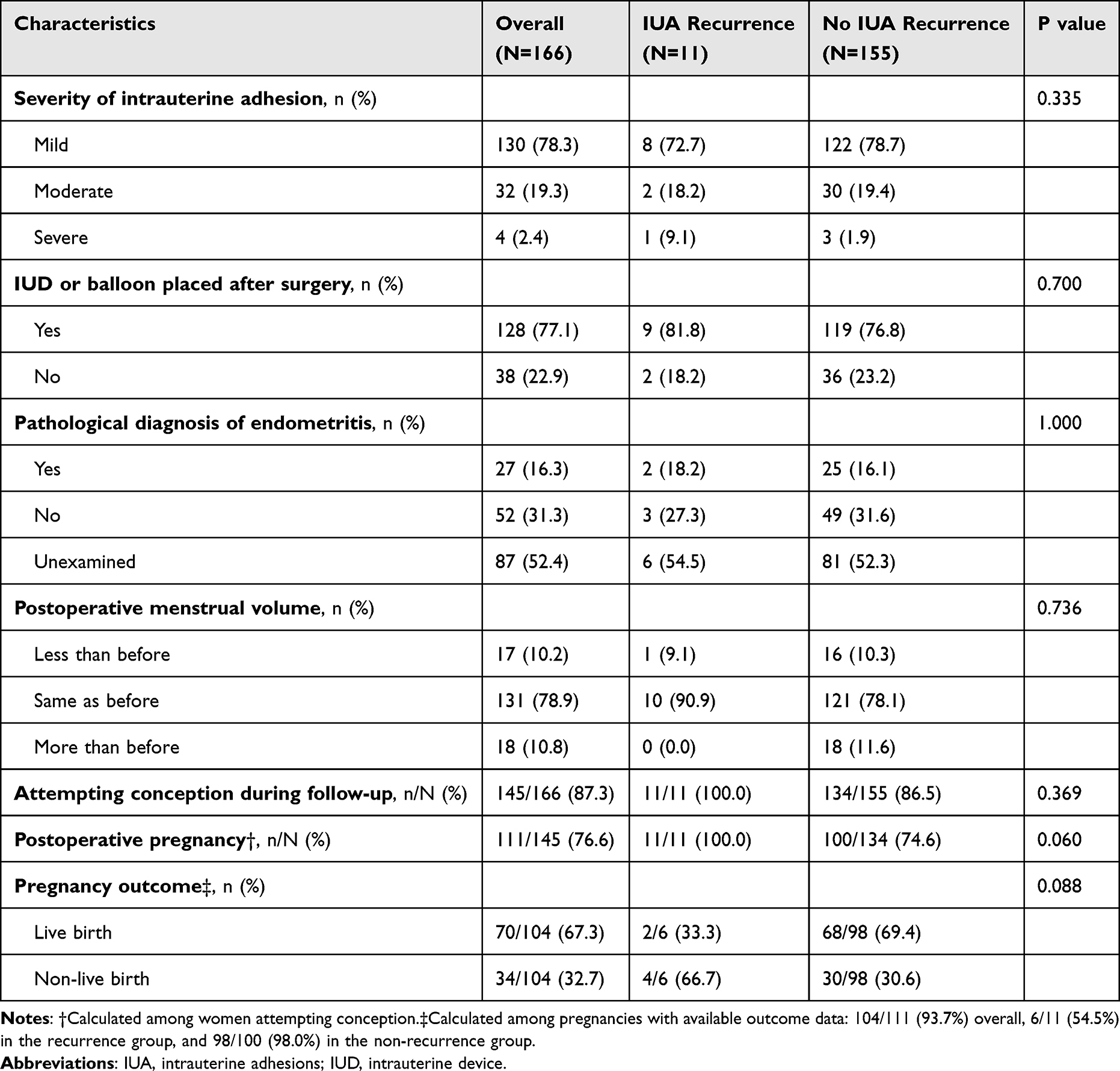 |
Table 2 Comparison of Clinical Characteristics and Pregnancy Outcomes Between Recurrent and Non-Recurrent IUA |
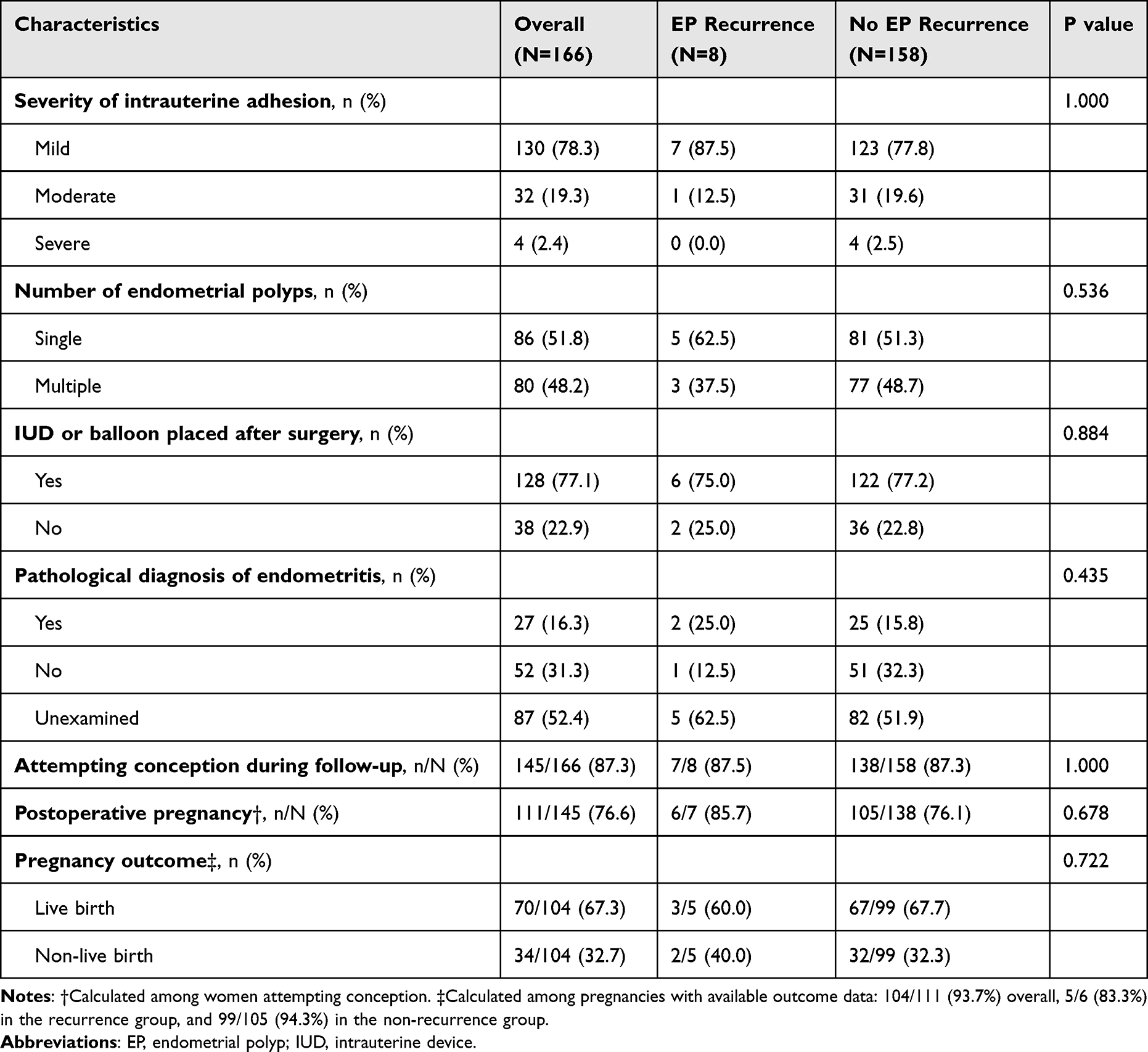 |
Table 3 Comparison of Clinical Characteristics and Pregnancy Outcomes Between Recurrent and Non-Recurrent EPs |
Discussion
In this retrospective cohort of women with concomitant IUA and EPs undergoing concurrent hysteroscopic adhesiolysis and polypectomy, we observed no statistically significant differences among short-term postoperative sequential estrogen–progestin therapy (Femoston), COC use (Yaz), and no hormonal therapy with respect to IUA recurrence, EP recurrence, time to recurrence, menstrual changes, or pregnancy outcomes. Notably, short-term estradiol–dydrogesterone therapy was not associated with an increased EP recurrence rate in women with IUA and a single EP.
The pathogenesis of endometrial polyps is often attributed to a local imbalance between estrogen and progesterone, characterized by relative estrogen excess and progesterone deficiency.12 Given the critical role of steroid hormones and their receptors in polyp development and growth,12,13 a theoretical concern exists that postoperative estrogen therapy for IUA could increase the risk of EPs recurrence in patients with both conditions. To date, no prior studies have confirmed that short-term estrogen use elevates this risk. Literature indicates that polyp multiplicity14 and chronic endometritis15,16 are significant risk factors for recurrence. Established strategies to reduce postoperative recurrence in premenopausal patients include levonorgestrel-releasing intrauterine systems (LNG-IUS), COCs, and dydrogesterone.17,18
Clinically, estrogen therapy is widely used to promote endometrial regeneration after adhesiolysis and is supported by AAGL/ESGE guidance.9,19 At the same time, EP development has been linked to estrogen exposure and endometrial proliferation, raising concern regarding potential recurrence in women with EPs.20,21 When IUA and EPs coexist, clinicians face a real-world dilemma in balancing endometrial healing needs against a theoretical risk of promoting polyp recurrence.19 Our findings provide observational data suggesting that short-term postoperative estrogen–progestin sequential therapy, as administered in our cohort, was not associated with higher EP recurrence in the subgroup of women with single EPs.
We also acknowledge that adjuvant barrier measures (IUD/balloon placement and hyaluronate gel) were used in a clinically individualized manner and differed between groups. Because these measures may affect endometrial healing and adhesion reformation, they may confound recurrence comparisons in observational data.
Strengths
This study focuses on an understudied but clinically relevant population—women with concomitant IUA and EPs treated in the same operative setting—and compares commonly used real-world postoperative hormonal strategies. Surgeries were performed by experienced hysteroscopists, and clinically meaningful outcomes included both recurrence and pregnancy-related endpoints.
Limitations
Several limitations should be considered. First, the retrospective single-center design limits generalizability. Second, treatment allocation was non-random and based on clinical judgement, introducing selection bias and confounding by indication (eg, baseline polyp multiplicity and IUD/balloon use differed between groups) Third, the number of recurrence events was small, which may limit statistical power and increase the risk of type II error; therefore, a lack of statistical significance should not be interpreted as evidence of equivalence. Fourth, recurrence assessment was based on real-world practice (ultrasound and/or hysteroscopy), which may introduce heterogeneity in detection. Finally, some follow-up information relied on patient report, which may be subject to recall bias. Prospective studies with larger samples and adjusted analyses are needed to confirm these findings.
Conclusion
In this retrospective cohort, no statistically significant differences were observed among short-term sequential estrogen–progestin therapy (Femoston), COC use (Yaz), and no hormonal therapy in terms of IUA recurrence, EP recurrence, time to recurrence, or pregnancy outcomes. Short-term estradiol–dydrogesterone sequential therapy was not associated with increased EP recurrence in women with IUA and a single EP. These findings are observational and hypothesis-generating and require confirmation in prospective studies.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding authors Xiaozhu Zhong and Dongmei Chen upon reasonable request, subject to institutional and ethics approval.
Ethics Approval and Consent to Participate
The study was approved by the Institutional Review Board of Sun Yat-sen Memorial Hospital, Sun Yat-sen University (SYSKY-2025-070-01). Informed consent was obtained from all patients. All procedures performed in this study involving human participants were in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Guangdong Basic and Applied Basic Research Foundation (2023A1515140167 and 2024A1515013191) and the National Natural Science Foundation of China (grant 82171670).
Disclosure
The authors declare no competing interests in this work.
References
1. Carbonnel M, Pirtea P, de Ziegler D, Ayoubi JM. Uterine factors in recurrent pregnancy losses. Fertil Steril. 2021;115(3):538–9. doi:10.1016/j.fertnstert.2020.12.003
2. Taylor E, Gomel V. The uterus and fertility. Fertil Steril. 2008;89(1):1–16. doi:10.1016/j.fertnstert.2007.09.069
3. Mo X, Qin G, Zhou Z, Jiang X. Assessment of risk factors of intrauterine adhesions in patients with induced abortion and the curative effect of hysteroscopic surgery. J Invest Surg. 2019;32(1):85–89. doi:10.1080/08941939.2017.1376130
4. Rein DT, Schmidt T, Hess AP, Volkmer A, Schöndorf T, Breidenbach M. Hysteroscopic management of residual trophoblastic tissue is superior to ultrasound-guided curettage. J Minim Invasive Gynecol. 2011;18(6):774–778. doi:10.1016/j.jmig.2011.08.003
5. Worldwide AA. AAGL practice report: practice guidelines for the diagnosis and management of endometrial polyps. J Minim Invasive Gynecol. 2012;19(1):3–10. doi:10.1016/j.jmig.2011.09.003
6. Berceanu C, Cernea N, Căpitănescu RG, et al. Endometrial polyps. Rom J Morphol Embryol. 2022;63(2):323–334. doi:10.47162/RJME.63.2.04
7. Pavone ME. Predicting the recurrence of endometrial polyps: a commentary. Fertil Steril. 2018;109(3):445. doi:10.1016/j.fertnstert.2018.01.033
8. Liu J, Liang Y, Ouyang J, Yang S. Analysis of risk factors and model establishment of recurrence after endometrial polypectomy. Ann Palliat Med. 2021;10(11):11628–11634. doi:10.21037/apm-21-2747
9. AAGL Elevating Gynecologic Surgery J. AAGL practice report: practice guidelines on intrauterine adhesions developed in collaboration with the European Society of Gynaecological Endoscopy (ESGE). Gynecol Surg. 2017;14(1):6. doi:10.1186/s10397-017-1007-3
10. Society TA. The American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, müllerian anomalies and intrauterine adhesions. Fertil Steril. 1988;49(6):944–955. doi:10.1016/S0015-0282(16)59942-7
11. Singh N, Sethi A. Endometritis - diagnosis, treatment and its impact on fertility - a scoping review. JBRA Assist Reprod. 2022;26(3):538–546. doi:10.5935/1518-0557.20220015
12. Kossai M, Penault-Llorca F. Role of hormones in common benign uterine lesions: endometrial polyps, leiomyomas, and adenomyosis. Adv Exp Med Biol. 2020;1242:37–58.
13. Yan C, Xing C, Wei T, et al. Impact of estrogen and progesterone receptor expression on the incidence of endometrial polyps. Biomark Med. 2023;17(21):881–887. doi:10.2217/bmm-2023-0411
14. Gu F, Zhang H, Ruan S, et al. High number of endometrial polyps is a strong predictor of recurrence: findings of a prospective cohort study in reproductive-age women. Fertil Steril. 2018;109(3):493–500. doi:10.1016/j.fertnstert.2017.11.029
15. Qu D, Liu Y, Zhou H, Wang Z. Chronic endometritis increases the recurrence of endometrial polyps in premenopausal women after hysteroscopic polypectomy. BMC Women’s Health. 2023;23(1):88. doi:10.1186/s12905-023-02232-3
16. Huang J, You X, Zhao Z, Jiang X, Qu D. Chronic endometritis multiplies the recurrence risk of endometrial polyps after transcervical resection of endometrial polyps: a prospective study. BMC Women’s Health. 2024;24(1):372. doi:10.1186/s12905-024-03221-w
17. Wang Y, Yang M, Huang X, Li X, Lin E, Feng Y. Prevention of benign endometrial polyp recurrence using a levonorgestrel-releasing intrauterine system in premenopausal patients: a retrospective cohort study. J Minim Invasive Gynecol. 2020;27(6):1281–1286. doi:10.1016/j.jmig.2019.11.023
18. Jiang Y, Li X, Wu J, Jiang C, Yang Y, Wei H. The efficacy of levonorgestrelintrauterine system, drospirenone & ethinylestradiol tablets (II) and dydrogesterone in preventing the recurrence of endometrial polyps. Arch Gynecol Obstet. 2024;310(3):1645–1649. doi:10.1007/s00404-024-07605-z
19. Robinson JK, Colimon LM, Isaacson KB. Postoperative adhesiolysis therapy for intrauterine adhesions (Asherman’s syndrome). Fertil Steril. 2008;90(2):409–414. doi:10.1016/j.fertnstert.2007.06.034
20. Kou L, Jiang X, Xiao S, Zhao YZ, Yao Q, Chen R. Therapeutic options and drug delivery strategies for the prevention of intrauterine adhesions. J Control Release. 2020;318:25–37. doi:10.1016/j.jconrel.2019.12.007
21. Johary J, Xue M, Zhu X, Xu D, Velu PP. Efficacy of estrogen therapy in patients with intrauterine adhesions: systematic review. J Minim Invasive Gynecol. 2014;21(1):44–54. doi:10.1016/j.jmig.2013.07.018
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.