Back to Journals » Clinical Ophthalmology » Volume 19
Impact of Pre-Suction Corneal Contact Area on Postoperative Refractive Outcomes in SMILE Surgery: A Retrospective Study
Authors Tan X, Shao Q, Cai J, Li X
Received 20 July 2025
Accepted for publication 24 September 2025
Published 30 October 2025 Volume 2025:19 Pages 4017—4025
DOI https://doi.org/10.2147/OPTH.S546189
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Xiying Tan,* Qing Shao,* Jinfeng Cai, Xia Li
Department of Refractive Surgery, Shanghai Aier Eye Hospital, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xia Li, Department of Refractive Surgery, Shanghai Aier Eye Hospital, Wuzhonglu 83, Shanghai, 200235, People’s Republic of China, Tel +86 13816957393, Email [email protected] Jinfeng Cai, Department of Refractive Surgery, Shanghai Aier Eye Hospital, Wuzhonglu 83, Shanghai, 200235, People’s Republic of China, Tel +86 13816957393, Email [email protected]
Objective: To investigate the relationship between corneal contact area before suction initiation and postoperative refractive outcomes in SMILE surgery.
Methods: A retrospective study was conducted in the refractive department of Shanghai Aier Eye Hospital. Eligible patients who underwent SMILE surgery between January and May 2023 were included. Preoperative and postoperative visual acuity and refractive outcomes were assessed at 1 and 3 months. The pre-suction corneal contact area was quantified using Adobe Photoshop.
Results: A total of 53 patients (28 males, 25 females; mean age, 25 years) were enrolled. A significant positive correlation was found between the pre-suction corneal contact area and postoperative refraction (Spearman’s r = 0.65, p < 0.05). Receiver operating characteristic (ROC) curve analysis indicated an area under the curve (AUC) of 0.803 (Std. Error = 0.066, p = 0.001), indicating good predictive ability for overcorrection, with the optimal threshold identified at 70%.
Conclusion: Pre-suction corneal contact area plays a critical role in the refractive outcomes of SMILE surgery. Optimizing this parameter may reduce the risk of overcorrection and enhance surgical precision and patient satisfaction.
Keywords: SMILE, refractive surgery, corneal biomechanics, corneal contact area
Introduction
Small-Incision Lenticule Extraction (SMILE) has emerged as a promising refractive surgery technique in which a femtosecond laser is used to create and extract an intrastromal lenticule.1,2 This procedure offers biomechanical advantages3 and reduces corneal denervation4,5 compared to traditional methods.
Several perioperative factors have been reported to affect surgical outcomes, including suction loss and decentration, which are among the leading causes of suboptimal postoperative vision.6 During SMILE, suction is employed to stabilize the eye, ensuring accurate lenticule creation. The corneal contact area before suction initiation could affect corneal biomechanics and, consequently, the refractive outcome.
Previous studies have explored various factors affecting SMILE outcomes, but the specific impact of pre-suction corneal contact area has received little attention.
However, the optimal pre-suction corneal contact area remains an area of interest and investigation. While the manufacturer generally recommends maintaining a contact area of 80%-90%, there is a lack of empirical evidence defining an optimal range.
Understanding how variations7 in corneal contact area influence the stability of lenticule creation and separation is crucial for refining surgical techniques and improving postoperative refractive results. This study aims to determine the relationship between pre-suction corneal contact area and postoperative refractive outcomes in SMILE surgery.
Methods
Study Design and Patients
A retrospective study was conducted involving 53 patients (106 eyes) with myopia and/or astigmatism, who underwent small-incision lenticule extraction (SMILE) surgery at Shanghai Aier Eye Hospital between January and May 2023. All procedures were performed by the same experienced surgeon.
The study aimed to evaluate whether the proportion of pre-suction corneal contact area is associated with postoperative refractive predictability. We hypothesized that a smaller contact area would be associated with less favorable refractive outcomes.
Inclusion and Exclusion Criteria
Inclusion criteria were as follows: age between 18 and 32 years, stable refractive error (manifest refractive spherical equivalent [MRSE] change ≤0.50 D) for over 1 year within the past 2 years, and discontinuation of contact lens wear for at least 2 weeks before corneal tomography. Exclusion criteria included inadequate preoperative corneal pachymetry (less than 500 μm), residual stromal bed thickness after SMILE less than 280 μm, corneal tomographic abnormalities such as keratoconus or pellucid marginal degeneration, corneal scars, pregnancy or lactation, and ocular comorbidities like cataract, glaucoma, or ocular inflammation.
Ethical Considerations
This study adhered to the tenets of the Declaration of Helsinki and received approval from the Institutional Review Board of Shanghai Aier Eye Hospital (Approval No. SHAIER2025YN010). Written informed consent was obtained from all patients for the use of their anonymized data.
Surgical Procedure
All SMILE procedures were performed under topical anesthesia using the VisuMax femtosecond system (Carl Zeiss Meditec, Jena, Germany) with standardized parameters of 130 μm cap thickness, 140 nJ power, and 3 mm corneal side-cut length. The planned optical zone diameter was 6.5 mm, and the cap diameter was 7.5 mm. The small-cone package (500 kHz laser, standard mode) was applied in all cases to ensure consistency across patients.
Measurement of Pre-Suction Corneal Contact Area
The corneal contact area before suction initiation was automatically captured by the VisuMax system and exported as TIFF images (Figure 1). Image analysis was performed using Adobe Photoshop CC (Adobe Systems, San Jose, CA, USA) with standardized pixel-based segmentation. Two independent observers repeated the measurements on a random subset of 20 eyes to evaluate reproducibility. Both intra- and inter-observer intra-class correlation coefficients (ICCs) exceeded 0.90, indicating excellent reliability. Patients were divided into two groups according to the proportion of corneal contact area relative to the total corneal surface: Low contact group: ≤70% and High contact group: >70%. The cutoff value of 70% was determined using receiver operating characteristic (ROC) curve analysis.
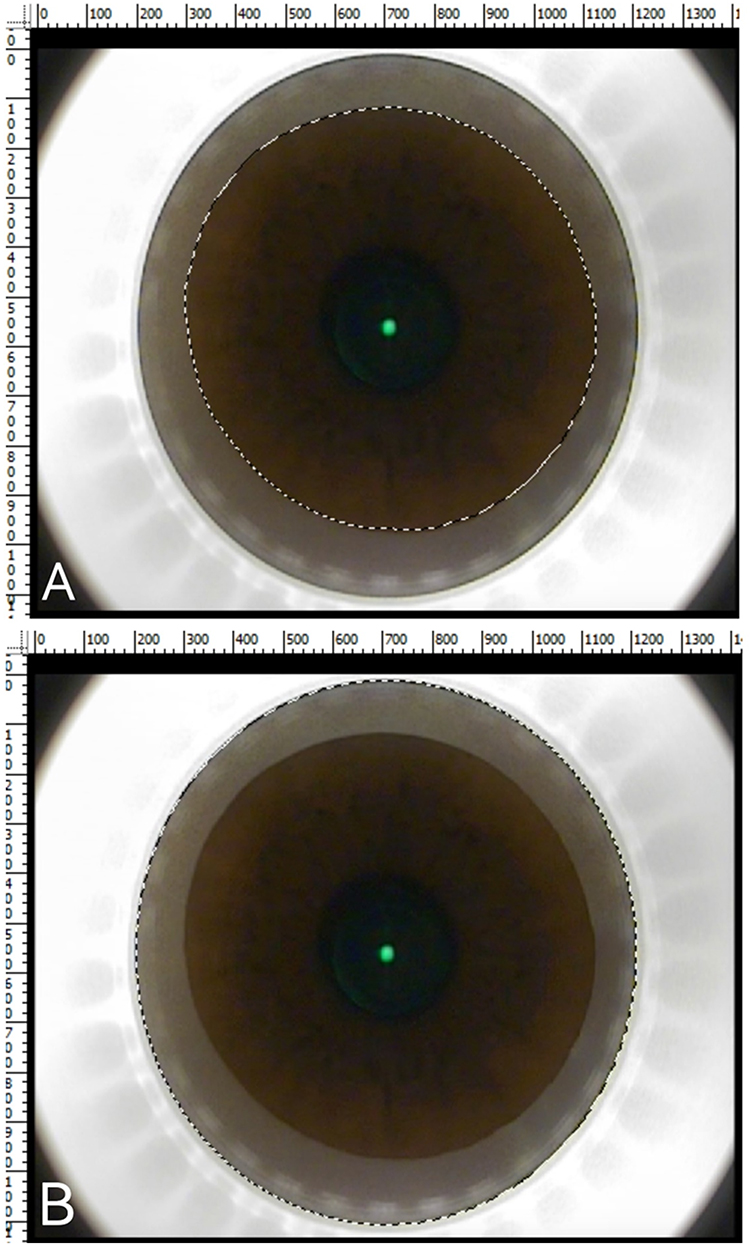 |
Figure 1 Calculation of pre-suction corneal contact area as the proportion of the dotted region to the total corneal area. (A) Calculation of the corneal contact area (delineated by the dashed line). (B) Calculation of the total corneal area (delineated by the dashed line). The corneal contact area ratio was calculated as A / B, where A represents the contact area and B represents the total corneal area. |
Clinical Examinations
Comprehensive ophthalmic examinations were performed preoperatively and at 1-month, and 3-month postoperative visits, including: uncorrected and corrected distance visual acuity (UCVA, CDVA), manifest and cycloplegic refraction, intraocular pressure (Goldmann applanation tonometry), slit-lamp biomicroscopy and dilated fundus examination, corneal tomography (Pentacam, OCULUS Optikgeräte GmbH), and contrast sensitivity assessment. A single experienced optometrist with over 20 years of clinical practice conducted all refraction measurements.
Postoperative Medication
The postoperative medication regimen included topical corticosteroids (0.1% Fluorometholone Eye Drops, Santen) for 1 month (four times a day for the first week, tapered weekly), topical antibiotics (0.5% Levofloxacin Eye Drops) four times daily for 1 week, and lubricants (Systane Ultra Eye Drops) four times daily for 3 months.
Outcomes
The primary outcome was postoperative refractive predictability, defined as the difference between attempted and achieved MRSE at 1 month. Secondary outcomes included CDVA, safety index, and contrast sensitivity changes. Spearman correlation analysis was performed to evaluate the relationship between pre-suction corneal contact area and postoperative refractive outcomes (Table 1). Linear regression was used to quantify the effect size, and Receiver Operating Characteristic (ROC) curve analysis was conducted to determine the optimal threshold for corneal contact area in predicting overcorrection.
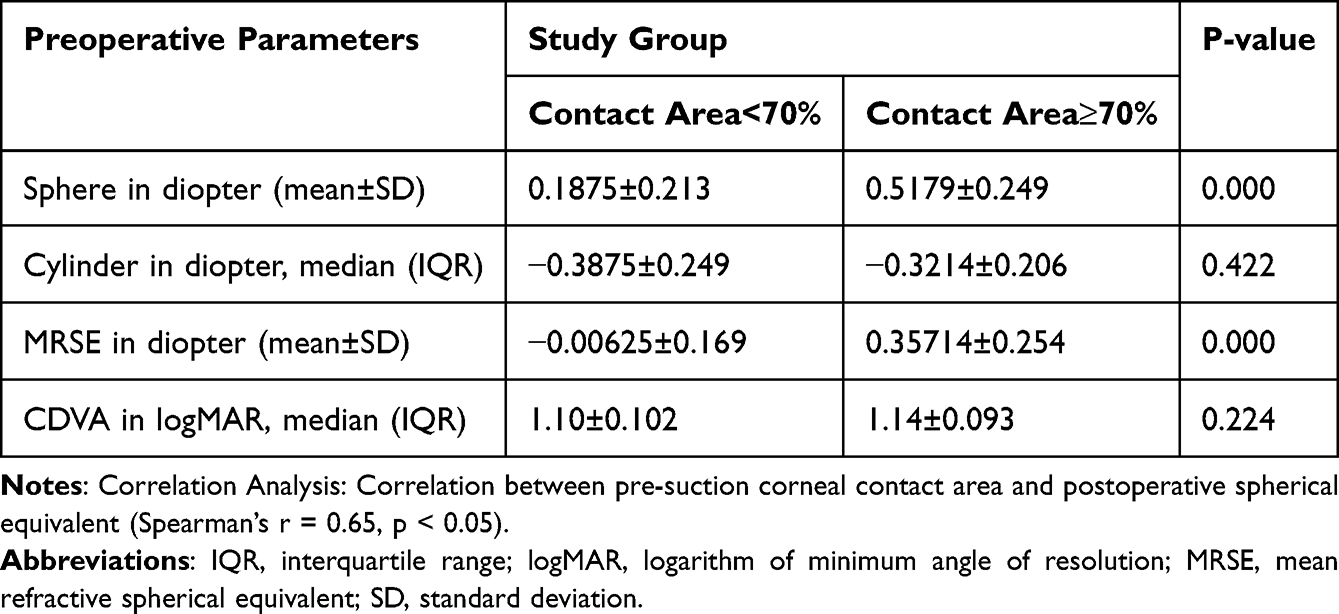 |
Table 1 Comparison of 1 month Postoperative Parameters Between the Study Groups |
Statistical Analysis
Statistical analysis was performed using SPSS version 10.0 (SPSS Inc., Chicago, IL, USA). Data normality was assessed using the Shapiro–Wilk test. CDVA values were converted from Snellen acuity to logMAR for analysis. Continuous variables were presented as mean ± standard deviation (SD), and categorical variables as counts and percentages. Student’s t-test or Mann–Whitney U-test for continuous variables, χ²-test or Fisher’s exact test for categorical variables. Spearman correlation coefficient was performed to evaluate the association between pre-suction corneal contact area and postoperative refractive outcomes. Multivariable linear regression was used to quantify the effect of contact area while adjusting for potential confounders (age, preoperative MRSE, central corneal thickness). Additionally, Receiver Operating Characteristic (ROC) curve analysis was conducted to determine the optimal cutoff value of contact area, with sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) calculated using the Youden index. A p-value <0.05 was considered statistically significant.
Results
Demographics
A total of 53 patients (106 eyes) were included, comprising 28 males and 25 females, with a mean age of 25.0 ± 3.2 years (range: 18–32 years). Baseline demographic and preoperative clinical characteristics are summarized in Table 2. No significant differences were observed between the low (≤70%) and high (>70%) corneal contact groups regarding age, sex distribution, preoperative MRSE, or central corneal thickness (p > 0.05).
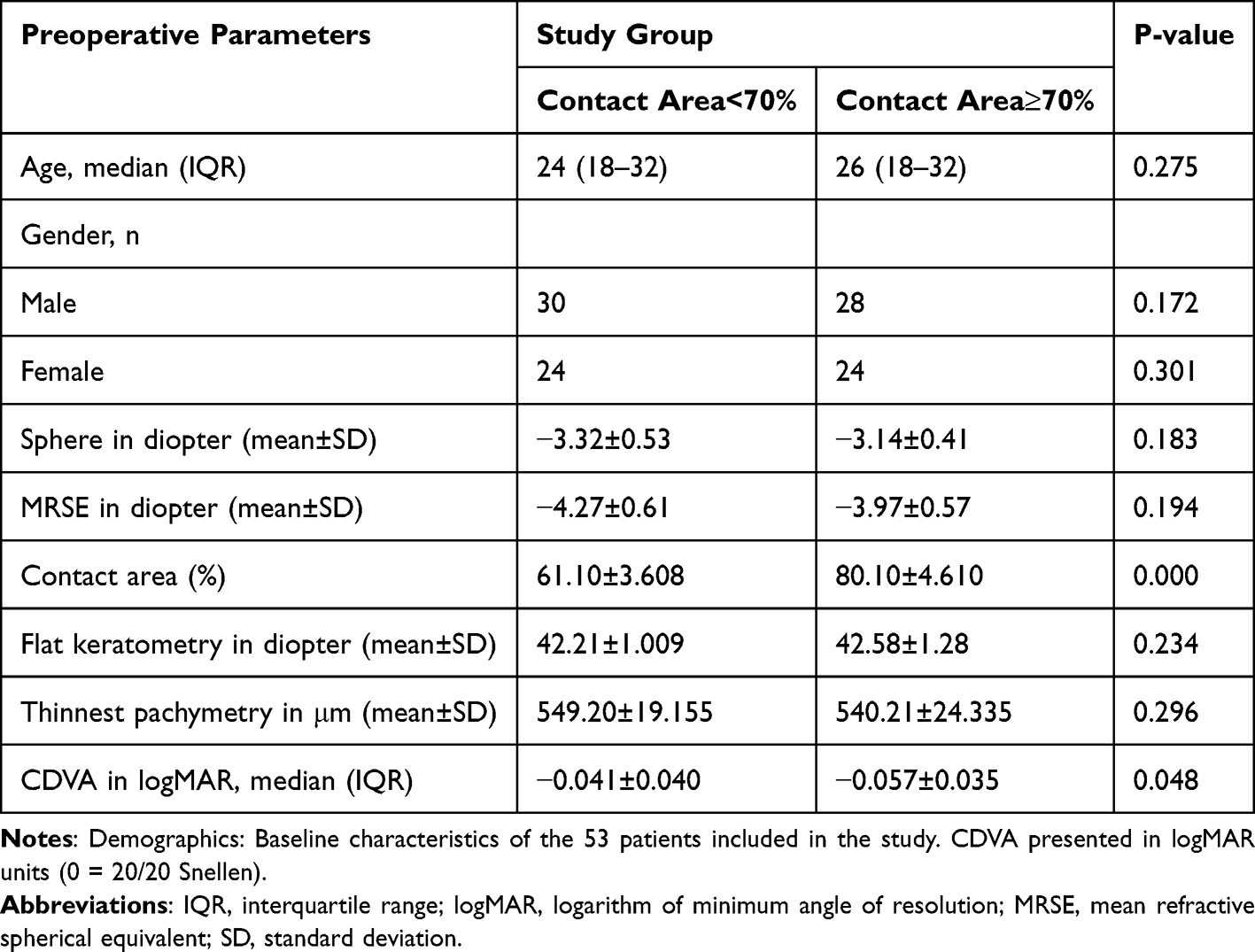 |
Table 2 Comparison of Preoperative Parameters Between the Study Groups |
Visual and Refractive Outcomes
At both 1 and 3 months postoperatively, the majority of eyes achieved uncorrected distance visual acuity (UDVA) of 20/20 or better. Postoperative MRSE was closer to the intended correction in the high-contact group compared with the low-contact group (data shown in Table 1). No significant complications were observed during surgery or follow-up.
Correlation Analysis
Spearman correlation analysis demonstrated a significant positive correlation was found between the proportion of pre-suction corneal contact area and postoperative MRSE at 1 month (r = 0.65, p < 0.05). Larger contact area was correlated with smaller residual refractive error (Table 1).
Regression Analysis
In the multivariable linear regression model including age, central corneal thickness, and preoperative MRSE, pre-suction corneal contact area showed a positive association with postoperative spherical equivalent but did not reach statistical significance (β = 0.447, p = 0.346). Although the variance inflation factor (VIF) values indicated no multicollinearity among the included variables, the limited sample size may have reduced the statistical power to detect an independent effect (Table 3).
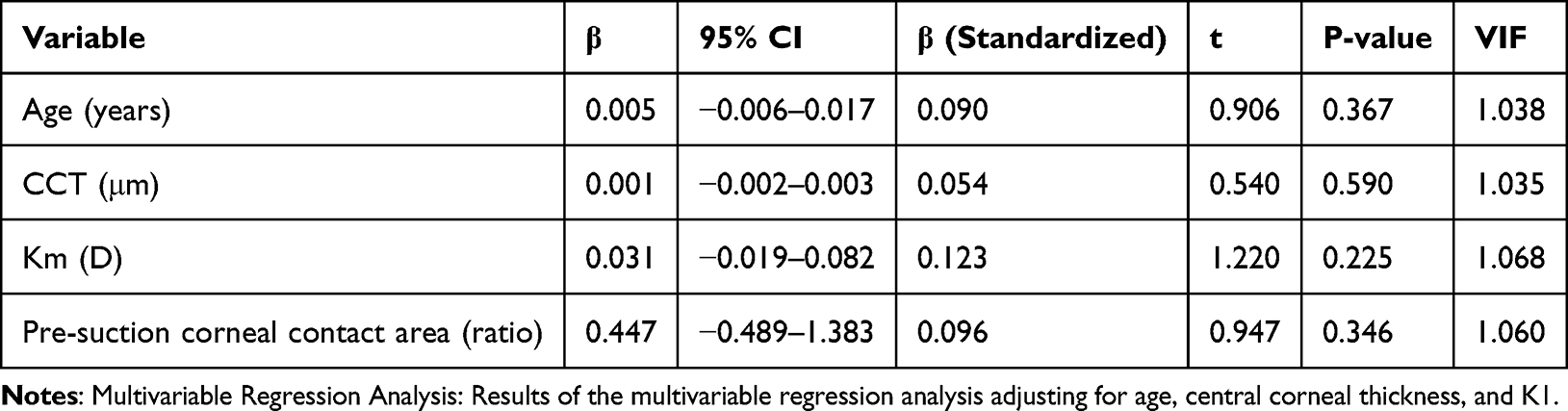 |
Table 3 Multivariable Linear Regression Analysis of Factors Associated with Postoperative Spherical Equivalent (SE) |
ROC Analysis
The ROC curve analysis indicated an area under the curve (AUC) of 0.803 (Std. Error = 0.066, p = 0.001), with an asymptotic 95% confidence interval ranging from 0.674 to 0.931 (Figure 2). The optimal threshold was identified at 70% contact area, determined using the Youden index. At this cutoff, the sensitivity was 78.2%, specificity was 72.5%, positive predictive value (PPV) was 69.2%, and negative predictive value (NPV) was 82.2%, suggesting good discriminatory ability of corneal contact area in predicting postoperative overcorrection (Figure 2).
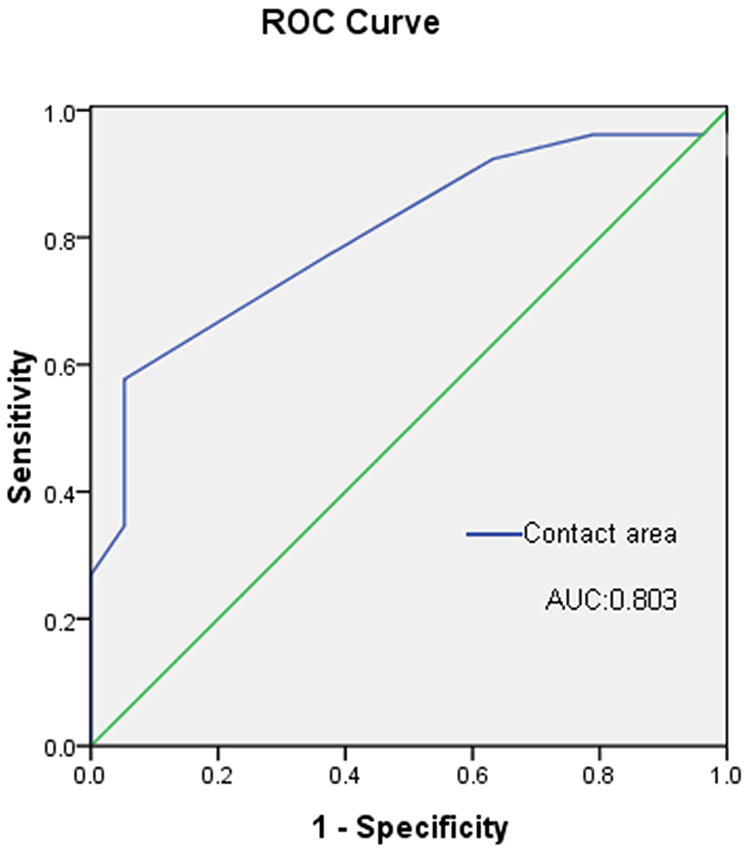 |
Figure 2 ROC curve of corneal contact area predicting postoperative overcorrection (AUC = 0.803). |
Discussion
The study demonstrates that larger corneal contact areas prior to suction initiation is associated with overcorrection following SMILE surgery. These results suggest that suction-induced corneal deformation may alter lenticule extraction accuracy (Table 1) and thereby affect refractive predictability. Although SMILE is considered less invasive compared to LASIK due to the absence of a flap, our results indicate that the biomechanics of corneal–suction interface remain critical for surgical outcomes.
The underlying mechanism is likely biomechanical. Previous studies have shown that central corneal thickness and intraocular pressure (IOP) are strongly correlated, with thicker corneas exhibiting greater IOP elevations during suction.8,9 Similar effects are observed in LASIK, where suction ring pressure can alter corneal curvature and biomechanics.10 In SMILE, a larger contact area amplifies this effect by compressing a greater portion of the cornea, resulting in transient thinning and increased IOP. This deformation reduces corneal hysteresis, diminishing the tissue’s ability to absorb and dissipate energy during femtosecond laser application.11–13 Consequently, laser–tissue interaction may become inconsistent, producing subtle variations in lenticule thickness and shape, and ultimately leading to overcorrection or residual refractive error.14
Comparisons with other corneal refractive procedures further highlight this mechanism. In LASIK, flap creation itself induces biomechanical weakening, whereas in SMILE the femtosecond laser is applied within an intact corneal cap. This theoretically preserves corneal strength, but also makes outcomes more dependent on the uniformity of suction and lenticule cutting. Studies on corneal biomechanics after LASIK versus SMILE have reported higher corneal hysteresis preservation in SMILE.15 However, our findings suggest that this advantage may be partly offset when suction contact is excessive, as increased compression alters corneal rigidity before cutting. Thus, optimizing suction parameters may be particularly relevant for SMILE.
From a clinical perspective, these findings highlight the importance of optimizing suction parameters to minimize excessive contact. Although manufacturer guidelines recommend a corneal contact area of 80–90%, our data suggest that a threshold of approximately 60–70% may achieve better refractive predictability by reducing biomechanical stress during the procedure. Real-time feedback on contact area could allow surgeons to individualize suction levels for each patient, taking into account baseline corneal thickness, biomechanics, and refractive error. The integration of automated image analysis or intraoperative monitoring into femtosecond systems may therefore enhance procedural consistency and safety in the future.
Another consideration is suction loss, which can occur at various stages of SMILE and necessitates redocking. Previous studies have shown that immediate reapplication without parameter adjustment does not significantly affect outcomes.16,17 However, our findings suggest that changes in corneal contact area during redocking may influence refractive predictability. Contact area could therefore serve as an additional parameter in deciding whether adjustments are needed after suction loss.
In the multivariable regression analysis, pre-suction corneal contact area lost its statistical significance as an independent predictor of postoperative spherical equivalent after adjusting for age, central corneal thickness, and preoperative MRSE. This result may be attributed to the relatively small sample size, which could reduce the statistical power of the model. Moreover, some degree of intercorrelation among ocular biometric parameters might dilute the independent effect of corneal contact area, even though variance inflation factors (VIFs) indicated no obvious collinearity. Importantly, the consistent trend of positive association between larger contact areas and postoperative overcorrection across both univariable and multivariable models suggests a potential predictive role. These findings highlight the need for larger prospective studies with more balanced covariate distributions to validate the independent contribution of pre-suction corneal contact area to SMILE refractive outcomes.
Implications
These findings highlight the critical importance of optimizing corneal contact area in SMILE surgery to enhance refractive outcomes. Proper management of corneal contact areas can improve surgical precision and patient satisfaction. Future research is needed to establish comprehensive guidelines for ideal contact area parameters to further refine surgical techniques and outcomes.
Limitations
This study is limited by its retrospective design and relative small sample size, which may affect the generalizability of the results. In addition, corneal contact area was measured by a single observer, and inter-observer reproducibility was not assessed. Finally, we did not account for inter-individual differences in corneal biomechanics, such as baseline corneal hysteresis or elasticity, which could also influence outcomes. Future prospective studies with larger cohorts and standardized measurement protocols are needed to confirm the optimal contact area threshold and validate its role in improving surgical predictability. Such studies will help confirm the optimal contact area for minimizing complications and achieving the best possible refractive outcomes.
Conclusion
The pre-suction corneal contact area is a crucial factor influencing refractive outcomes in SMILE surgery. Adjusting this parameter can enhance surgical precision, leading to improved patient satisfaction and reduced risk of complications. Understanding and optimizing the contact area are essential for achieving the best possible results in SMILE surgery.
Ethics Statement
This study was reviewed and approved by the Ethics Committee of Shanghai Aier Eye Hospital. Written informed consent was obtained from all participants prior to their inclusion in the study. All procedures involving human participants were conducted in accordance with the ethical standards outlined in the Declaration of Helsinki and its later amendments.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Xia F, Chen Z, Miao H, et al. Ten-year outcomes following small incision lenticule extraction for up to −10 Dioptres myopia. Clin Exp Optom. 2024;107(3):285–290. doi:10.1080/08164622.2023.2203313
2. Huang G, Melki S. Small Incision Lenticule Extraction (SMILE): myths and realities. Semin Ophthalmol. 2021;36(4):140–148. doi:10.1080/08820538.2021.1887897
3. Spiru B, Kling S, Hafezi F, et al. Biomechanical differences between Femtosecond Lenticule Extraction (FLEx) and Small Incision Lenticule Extraction (SmILE) tested by 2D-extensometry in ex vivo porcine eyes. Invest Ophthalmol Vis Sci. 2017;58(5):2591–2595. doi:10.1167/iovs.16-20211
4. Zhang Y, Shen Q, Jia Y, et al. Clinical outcomes of SMILE and FS-LASIK used to treat myopia: a meta-analysis. J Refract Surg. 2016;32(4):256–265. doi:10.3928/1081597X-20151111-06
5. Mohamed-Noriega K, Riau AK, Lwin NC, et al. Early corneal nerve damage and recovery following small incision lenticule extraction (SMILE) and laser in situ keratomileusis (LASIK). Invest Ophthalmol Vis Sci. 2014;55(3):1823–1834. doi:10.1167/iovs.13-13324
6. Wang Y, Xie L, Yao K, et al; Writing Committee for the Guideline Working Group. Evidence-based guidelines for keratorefractive lenticule extraction surgery. Ophthalmology. 2025;132(4):397–419. doi:10.1016/j.ophtha.2024.11.016
7. Cao H, Zhang L, Liang S, et al. Predictive factors of posterior corneal shift after small incision lenticule extraction: a 5-year follow-up study. Acta Ophthalmol. 2022;100(7):e1431–e1438. doi:10.1111/aos.15166
8. Iyamu E, Ituah I. The relationship between central corneal thickness and intraocular pressure: a comparative study of normals and glaucoma subjects. Afr J Med Med Sci. 2008;37(4):345–353.
9. Qu ZX, Li XM, Yuan YY, et al. In vivo corneal biomechanical response to three different laser corneal refractive surgeries. J Refract Surg. 2024;40(5):e344–e352. doi:10.3928/1081597X-20240322-01
10. Mirshahi A, Kohnen T. Effect of microkeratome suction during LASIK on ocular structures. Ophthalmology. 2005;112(4):645–649. doi:10.1016/j.ophtha.2004.11.046
11. Lee H, Kang DSY, Ha BJ, et al. Biomechanical properties of the cornea using a dynamic scheimpflug analyzer in healthy eyes. Yonsei Med J. 2018;59(9):1115–1122. doi:10.3349/ymj.2018.59.9.1115
12. Kotecha A, Crabb DP, Spratt A, et al. The relationship between diurnal variations in intraocular pressure measurements and central corneal thickness and corneal hysteresis. Invest Ophthalmol Vis Sci. 2009;50(9):4229–4236. doi:10.1167/iovs.08-2955
13. Chan JS, Han E, Lim CHL, et al. Incisional surface quality of electron-beam irradiated cornea-extracted lenticule for stromal keratophakia: high nJ-energy vs. low nJ-energy femtosecond laser. Front Med. 2023;10:1289528. eCollection 2023. doi:10.3389/fmed.2023.1289528
14. Yang S, Huang T, Wang Y, et al. Short-term impact of different corneal incision positions on postoperative astigmatism and visual quality after SMILE surgery. Ophthalmol Ther. 2023;12(5):2453–2464. doi:10.1007/s40123-023-00748-3
15. Wu D, Wang Y, Zhang L, et al. Corneal biomechanical effects: small-incision lenticule extraction versus femtosecond laser-assisted laser in situ keratomileusis. J Cataract Refract Surg. 2014;40(6):954–962. doi:10.1016/j.jcrs.2013.07.056
16. Ganesh S, Brar S, Pawar A. Outcomes of small incision lenticule extraction (SMILE) in eyes with intraoperative suction loss. J Refract Surg. 2017;33(1):59–64.
17. Chung B, Ryu IH, Lee IS, et al. Clinical outcomes of the immediate reapplication of small-incision lenticule extraction without adjusting the surgical parameters after suction loss. Sci Rep. 2022;12(1):15973. doi:10.1038/s41598-022-20403-4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Three-Month Outcomes of SMILE Pro with the VISUMAX 800 for Myopic Astigmatism in a Large Population
Cung HS, Tran LHT, Tran TN
Clinical Ophthalmology 2025, 19:417-425
Published Date: 7 February 2025