Back to Journals » Vascular Health and Risk Management » Volume 17
Impact of Pre-, Intra-and Post-Operative Parameters on In-Hospital Mortality in Patients Undergoing Emergency Coronary Artery Bypass Grafting: A Scarce Single-Center Experience in Resource-Scare Setting
Authors Hung DQ, Minh NT, Vo HL ![]() , Hien NS, Tuan NQ
, Hien NS, Tuan NQ
Received 25 January 2021
Accepted for publication 21 April 2021
Published 17 May 2021 Volume 2021:17 Pages 211—226
DOI https://doi.org/10.2147/VHRM.S303726
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Takashi Kajiya
Doan Quoc Hung,1,2 Nguyen Thai Minh,3 Hoang-Long Vo,1 Nguyen Sinh Hien,3 Nguyen Quang Tuan1,4
1Hanoi Medical University, Hanoi, 100000, Vietnam; 2Department of Cardiovascular and Thoracic Surgery, Viet Duc University Hospital, Hanoi, 100000, Vietnam; 3Hanoi Heart Hospital, Hanoi, 100000, Vietnam; 4Bach Mai Hospital, Hanoi, 100000, Vietnam
Correspondence: Doan Quoc Hung; Hoang-Long Vo Email [email protected]; [email protected]
Background: In-hospital mortality after emergency coronary artery bypass grafting (CABG) remains an important issue that has needed considerable attention in recent years as the mortality rate is still high and prevention factors are not yet optimal. Our study presents the first largest cohort of emergency CABG from one large institution in Vietnam with the primary aim of comparing a large variety of pre-, intra-and post-operative parameters between in-hospital mortality patients and in-hospital survival patients and investigate risk factors of in-hospital mortality in patients undergoing emergency CABG.
Methods: We conducted a retrospective evaluation of prospectively collected data in patients undergoing emergency CABG at the Hanoi Heart Hospital (Hanoi, Vietnam) from January 1, 2017, to December 31, 2019. Primary outcome variable was in-hospital mortality.
Results: A total of 71 patients were included in final analysis. The mean age of the cohort was 68.68 years (± 9.28, range 38– 86). The mean weight, height and body mass index were 54.35 kg (± 9.17, range 37– 77), 158.96 (± 7.64, range 145– 179) and 21.48 kg/m2 (± 3.08, range 13.59– 30.08), respectively. In-hospital mortality rate was 9.86%. Preoperative risk factors for in-hospital mortality included diabetes, decreased ejection fraction (EF), EF below 30%, cardiogenic shock, elevated systolic pulmonary artery pressure (PAP), elevated NT-ProBNP, and Euroscore II. Without grafting with left internal thoracic artery, and prolonged cardiopulmonary bypass (CPB) time were increased intraoperative factors for in-hospital mortality risk. In-hospital mortality’s postoperative risk factors were found to be postextubation respiratory failure requiring mechanical ventilation, ventricular fibrillation, dialysis-requiring acute renal failure, pneumonia, bacterial sepsis, gastrointestinal bleeding, and prolonged mechanical ventilation time. Significant predictors determining in-hospital mortality were known as prolonged CPB time in surgery and postoperative ventricular fibrillation.
Conclusion: Our hospital mortality rate after emergency CABG was relatively high. An optimal preventive strategy in emergency CABG management should target significant factors combined with other previously identified risk factors to reduce in-hospital mortality.
Keywords: emergency coronary artery bypass grafting, early mortality, in-hospital mortality, risk factor, Vietnam
Background
Acute coronary syndrome (ACS), known as the most serious consequence of coronary artery disease, can result in long-term disability and mortality. Treatment for ACS patients is, to date, posed to be coronary revascularization. Though the outcomes of emergency coronary artery bypass grafting (CABG) were improved in previous reports, the early mortality still remains highly great (21–52%),1–4 especially within first 48 hours from onset.5
There are no formal research investigation and analysis on the number of performed CABG procedures in Vietnam, this figure still, to the best of our knowledge, increase annually in Vietnam in the past decade. A small proportion of these procedures are performed in emergency situations, most often because of ongoing ischemia, angiographic accidents, multivessel disease but anatomic unsuitability for percutaneous coronary intervention (PCI) and mechanical complications of acute myocardial infarction. Several previous authors form developed countries have reported the risk factors for in-hospital mortality after emergency CABG, but there are still the inconsistencies and inadequacy in input data between the surgical centers.6–8 Importantly, in-hospital mortality after emergency CABG remains an important issue that needs considerable attention in recent years as mortality rate is still high and prevention factors are not yet optimal. A comprehensive understanding of the country-specific risk and prognosis of in-hospital mortality after CABG is crucial to reduce overall emergency-related in-hospital mortality in Vietnam. This study sought to compare a large variety of pre-, intra- and post-operative parameters between in-hospital mortality patients and in-hospital survival patients and investigate risk factors of in-hospital mortality in patients under going emergency CABG.
Methods
Study Design and Patients
Retrospective evaluation of prospectively collected data at the Hanoi Heart Hospital (Hanoi, Vietnam), was conducted. The clinical profile, preoperative characteristics, and medications, intraoperative data, and postoperative outcomes were retrieved from prospective patients' medical records and computerized database. From January 1, 2017, to December 31, 2019, a total of 71 patients underwent an emergency CABG in Hanoi Heart Hospital and were included in this study.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was approved by the Ethics Committee of Hanoi Medical University.
Because this was a retrospective study, individual patient informed consent was waived. Personal information of the subjects was kept confidential and encrypted.
Surgical Procedure
Decision for emergency CABG surgery, was made by a standard heart team of experienced physicians (including 1 cardiologist, 1 interventionist, 1 anesthetist and 1 surgeon), was based on clinical examination (chest pain severity, hemodynamic status), changes in cardiac enzymes (creatine kinase–myocardial band [CK-MB], High-sensitivity cardiac troponin T), changes in an electrocardiogram (ECG), lesion complexity on the coronary angiogram, echocardiography findings (ejection fraction [EF], severity of mitral regurgitation, regurgitation mechanism, left ventricular [LV] diameter, pulmonary artery pressure [PAP], and mechanical complications). Patients undergoing emergency surgery were those who after being indicated until they arrived in the operating room before the next working day (classified on the European System for Cardiac Operative Risk Evaluation [EuroSCORE II] scale9).
Towards surgical preparation for special cases, in case of the hemodynamic instability and or acute pulmonary edema, we conducted endotracheal intubation, central venous line and invasive blood pressure monitoring line during the duration of operating room preparation. Intra-aortic balloon counterpulsation (IABP) and/or extracorporeal membrane oxygenation (ECMO) were performed when the vasopressors increasing cardiac contractility did not stabilize hemodynamics. When patients were preoperatively on antiplatelet agents (clopidogrel and/or ticagrelor), we prepared 4-unit of red blood cell, 1–2- unit of platelet apheresis or 2–4- unit of platelet pool, and 1–2- unit of factor VIII.
Variable Definitions
Outcome Variable
In-hospital mortality or early mortality was defined as “death due to any cause within 30 days of surgery or during hospitalization.”
Preoperative Parameters
- General characteristics
Age (years), sex (male/female), height (cm), weight (kg), and body mass index (BMI) (kg/m2).
- Medical history and comorbidities
Hypertension, diabetes, lipid disorder, chronic obstructive pulmonary disease (COPD), history of myocardial infarction, history of coronary intervention, history of cerebrovascular accident, and peripheral vascular disease (PVD).
- Clinical features
Unstable angina: angina at rest, new angina, increased angina. Non-ST segment elevation myocardial infarction (STEMI): having chest pain, similar to the unstable angina but elevated cardiac enzymes (CK-MB and/or Troponin). STEMI, was according to Universal Definition of Myocardial Infarction Guidelines.10
- Coronary lesions in coronary angiography
Significant stenosis in a coronary artery: was detected as >50% stenosis of the left main stem or >70% stenosis in a major coronary vessel.11
- Echocardiographic parameters
EF (%), LV dimensions in diastole (mm), systolic PAP (mmHg), the degree of mitral valve regurgitation, aortic valve regurgitation and tricuspid valve regurgitation, mechanism of mitral valve regurgitation (anemia damage or mechanical complications of myocardial infarction), and pericardial fluid.
- Platelet agglutination inhibitor
Platelet agglutination inhibitors were used to the time of surgery, including Aspirin, Clopidogrel, and Ticagrelor.
- Indications for emergency surgery
Ongoing myocardial infarction but coronary anatomy not suitable for intervention: were cases of that, chest pain increased in intensity and frequency, cardiac enzymes may increase gradually, and diabetes may change in pain although optimal medical treatment (vasodilators, morphine) and coronary angiography were performed.
Accidents of PCI: were that cases undergoing PCI might not be due to acute myocardial infarction. During or after the procedure documented hemodynamic instability, or signs of cardiac tamponade due to pericardial hemorrhage. Coronary angiogram shows the signs of contrast agent drainage out of the coronary artery or the images of large coronary artery stems dissection or acute thrombosis in stent.
Acute myocardial infarction with cardiogenic shock: were that cases with acute myocardial infarction had complex coronary lesions on percutaneous coronary angiography, could not intervene or open the culprit branch but hemodynamics did not improve with optimal medical treatment. Cardiogenic shock was defined as systolic blood pressure of less than 90 mmHg for more than 30 minutes or the need for a catecholamine infusion to maintain systolic blood pressure above 90 mmHg.
Mechanical complications of acute myocardial infarction: were cases of LV free-wall rupture, acute mitral regurgitation due to papillary muscle or chordae rupture, and interventricular septal rupture.
- Preoperative severe hemodynamic status
IABP, ECMO, and cardiopulmonary resuscitation (CRP).
- The European System for Cardiac Operative Risk Evaluation (EuroSCORE II)
The EuroSCORE II was used to estimate risk of in-hospital death after cardiac surgery.12
Intraoperative Parameters
On pump or off pump. Number of distal anastomosis were calculated by the number of anastomosis performed on coronary arteries. Types of grafts included internal thoracic arteries, radial artery, and saphenous veins. Management of combined lesions during surgery included LV patch, ventricular septal repair, mitral valve repair/replacement, and repair/replacement of other valves. Aortic cross-clamp time (mins). Cardiopulmonary bypass (CPB) time (mins).
Postoperative Parameters
Mechanical ventilation time (hours), mediastinal drainage values in the first 24 hours (mL), postextubation respiratory failure requiring mechanical ventilation, bleeding required re-operated, ECMO for acute heart failure, ventricular fibrillation, new-onset atrial fibrillation, dialysis-requiring acute renal failure, pneumonia, bacterial sepsis, cerebrovascular accident, ischemic stroke, gastrointestinal bleeding, peritonitis, and surgical wound infection.
Data Analysis
All statistical analyses were performed with Stata® 15 (StataCorp LLC, USA). All data was first performed a visual inspection for coding errors, outliers, or funky distributions. We divided outcome study variable into two groups of in-hospital mortality patient group and in-hospital survival patient group. Categorical variables are expressed as frequencies and percentages and were compared by use of the χ2 or Fisher exact test. Continuous variables are expressed as mean±SD and interquartile range (IQR) and compared by Mann–Whitney U-test (not normally distributed) or t-test (normally distributed). We used univariate logistic regression analysis to identify risk factors of early death. Then, in each pre-, intra- and post-operative parameter groups, we selected significant variables of univariate logistic regression models to run as impossible independent risk into multivariate logistic regression models in particular. Hence, a total of 3 models with multivariate logistic regression were reported. Odds ratios with 95% confidence intervals were constructed. Statistically significant independent variables in both univariate and multivariate analysis were more clearly illustrated with the Stata’ function of bar chart and box plot.
Results
Overall, the total number of patients undergoing emergency CABG in our institution increased from 13 patients in 2017 to 39 patients in 2019. Of the total, the proportion of postoperative in-hospital mortality cases significantly decreased from 30.77% in 2017 to 5.13% in 2019 (Figure 1).
 |
Figure 1 Trends in in-mortality survival and in-hospital mortality after emergency CABP. |
Preoperative Data Among In-Hospital Mortality Patients and In-Hospital Survival Patients
A total of 71 patients undergoing emergency CABG were included in the analysis. The mean age of the cohort was 68.68 years (± 9.28, range 38–86). The mean weight, height and BMI was 54.35 kg (± 9.17, range 37–77), 158.96 (±7.64, range 145–179) and 21.48 kg/m2 (±3.08, range 13.59–30.08), respectively. The majority were male (n = 47, 66.20%). The most common medical history/comorbidity was hypertension (n = 65, 91.55%) (Table 1).
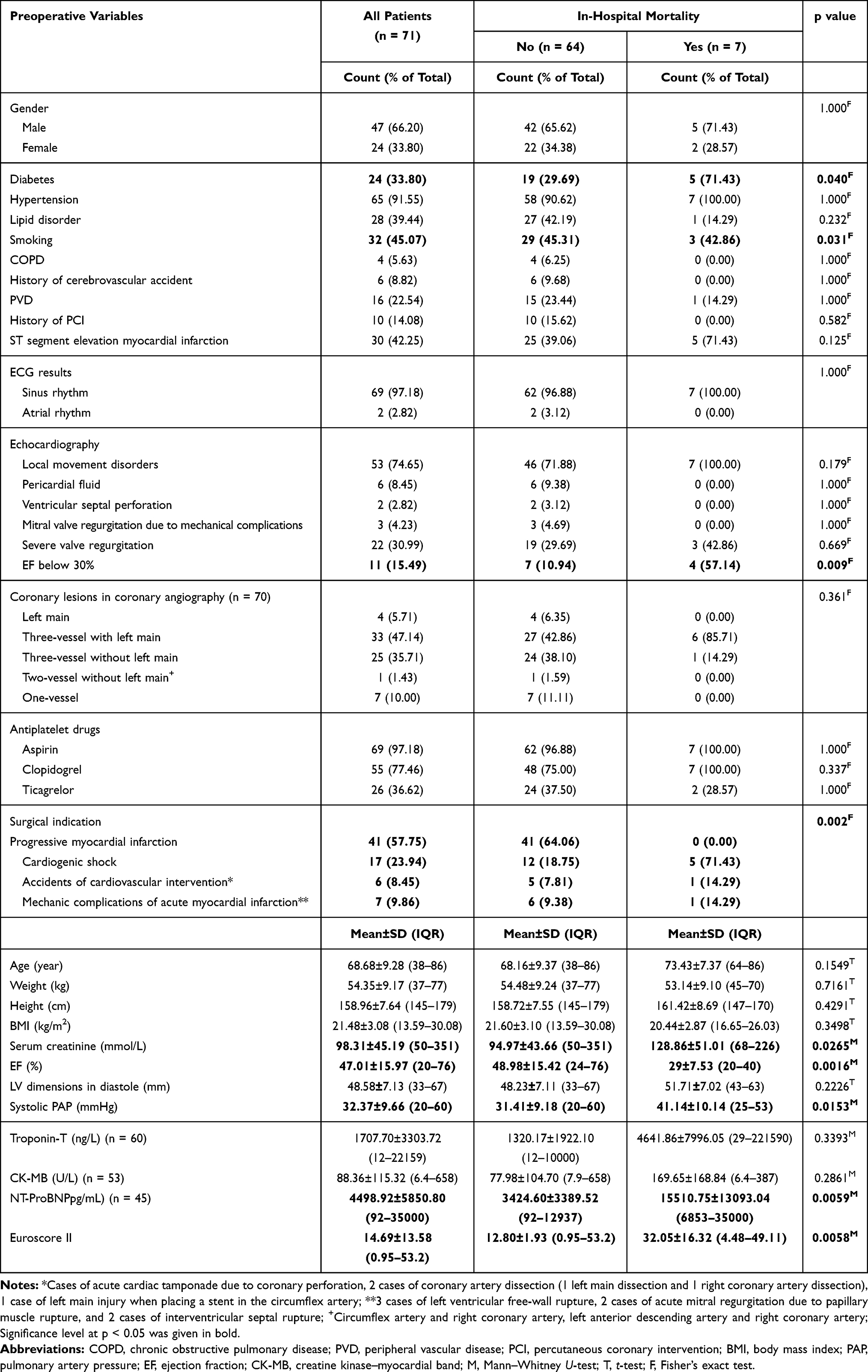 |
Table 1 Difference of Preoperative Data Among In-Hospital Mortality Patient Group and In-Hospital Survival Patient Group |
Seventy out of 71 study patients underwent preoperative coronary angiography because 1 patient with LV free wall rupture did not have timely coronary angiography. Echocardiography revealed local movement disorders in 53 patients (74.65), pericardial fluid in 6 patients (8.45%), and ventricular septal perforation in 2 patients (2.82%) (Table 1).
STEMI was seen in 30 patients (42.25%). Sixty-nine patients (97.18%) with sinus rhythm were on the ECG, while 2 patients (2.82%) had atrial rhythm. The mean EF was 47.01% (±15.97, range 33–67) and 11 patients (15.49%) had EF below 30%. The mean LV dimensions in diastole was 48.58 mm (±7.13, range 33–67). The mean systolic PAP was 32.37 mmHg (±9.66, range 20–60) (Table 1).
Cardiac enzymes recorded the mean troponin T of 1707.70 ng/L (±3303.72, range 12–22159), the mean CK-MB of 88.36 U/L (±115.32, range 6.4–658) and the mean NT-ProBNP of 4498.92 pg/mL (±5850.80, range 92–35000). The mean serum creatinine before surgery was 98.31 mmol/L (±45.19, range 50–351). The mean Euroscore II was 14.69 (±13.58, range 0.95–53.2) and in-hospital mortality patient group had significantly higher mean Euroscore II compared to in-hospital survival patient group (32.05±16.32 vs. 12.80±1.93). In study cohort, the most indications for emergency surgery were ongoing myocardial infarction (n = 41, 57.75%) and cardiogenic shock (n = 17, 23.94%) (Table 1).
Significant differences were observed in preoperative variables of diabetes (p = 0.04), smoking (p = 0.031), EF below 30% (p = 0.009), mean EF value (p=0.016), surgical indication (p = 0.002), serum creatinine (mmol/L) (p = 0.026), systolic PAP (p = 0.015), mean NT-proBNP (ng/L) (p = 0.0059), and Euroscore II (p = 0.0058) (Table 1).
Intraoperative Data Among In-Hospital Mortality Patients and In-Hospital Survival Patients
Intraoperative data amongst two groups was shown in Table 2. Seventy our of 71 patients underwent surgery with CPB, and of these, only 2 patients did not suffer cardiac arrest. No patients must be placed on CMO in surgery. Thirty patients (42.25%) underwent 4 distal anastomosis on coronary arteries, following by 3 distal anastomosis (n = 19, 26.76%), 2 distal anastomosis (n = 12, 16.90%) and 1 distal anastomosis (n = 8, 11.27%). Management of combined lesions during surgery was performed in 17 patients (23.94%). The mean aortic cross-clamping time in 68 patients and the mean CPB time in 70 patients were 72.24 minutes (±26.41, range 30–167) and 101.31 minutes (±37.30, range 40–264), respectively.
 |
Table 2 Difference of Intraoperative Data Among In-Hospital Mortality Patient Group and In-Hospital Survival Patient Group |
In the intraoperative characteristics, significant differences between in-hospital mortality patients and in-hospital survival patients were indicated among internal thoracic artery (p = 0.041), the number of saphenous veins (p = 0.010), and CPB time (p = 0.010) (Table 2).
Postoperative Data Among In-Hospital Mortality Patients and In-Hospital Survival Patients
As was revealed in Table 3, pneumonia (n = 17, 23.94%) was the most common in-hospital complications after surgery, while another complications were documented as dialysis-requiring acute renal failure in 9 patients (12.68%), ventricular fibrillation in 8 patients (11.27%), postextubation respiratory failure requiring mechanical ventilation in 7 patients (9.86%), re-operation for bleeding in 7 patients (9.86%), cerebrovascular accidents in 7 patients (9.86%), surgical wound infection in 7 patients (9.86%), bacterial sepsis in 4 patients (5.63%), ischemic stroke in 4 patients (5.63%), gastrointestinal bleeding in 3 patients (4.23%), new-onset atrial fibrillation in 2 patients (2.82%), ECMO for acute heart failure in 1 patient (1.41%), and peritonitis in 1 patient (1.41%).
 |
Table 3 Difference of Postoperative Data Among In-Hospital Mortality Group and In-Hospital Survival Group |
Significant differences between two patient groups were observed in postextubation respiratory failure requiring mechanical ventilation (p = 0.018), IABP (p = 0.000), ventricular fibrillation (p = 0.002), dialysis-requiring acute renal failure (p=0.000), pneumonia (p = 0.007), bacterial sepsis (p = 0.002), gastrointestinal bleeding (p = 0.024), mechanical ventilation time (p = 0.0003).
Preoperative Risk Factors of In-Hospital Mortality in Patients Undergoing Emergency CABG
In univariate logistic regression analysis, preoperative risk factors that were significantly associated with in-hospital mortality included diabetes in treatment (OR: 5.92, 95% CI: 1.05–33.24), decreased EF (OR: 0.87, 95% CI: 0.77–0.97), EF below 30% (OR: 10.86, 95% CI: 2.00–58.86), cardiogenic shock (OR: 10.83, 95% CI: 1.87–62.71), elevated systolic PAP (OR: 1.10, 95% CI: 1.01–1.19), elevated NT-ProBNP (OR: 1.0004, 95% CI: 1.00002–1.0008), and Euroscore II (OR: 1.08, 95% CI: 1.03–1.14). However, 5 selected risk factors in multivariate logistic regression model were not significantly independently associated with in-hospital mortality (p >0.05) (Table 4).
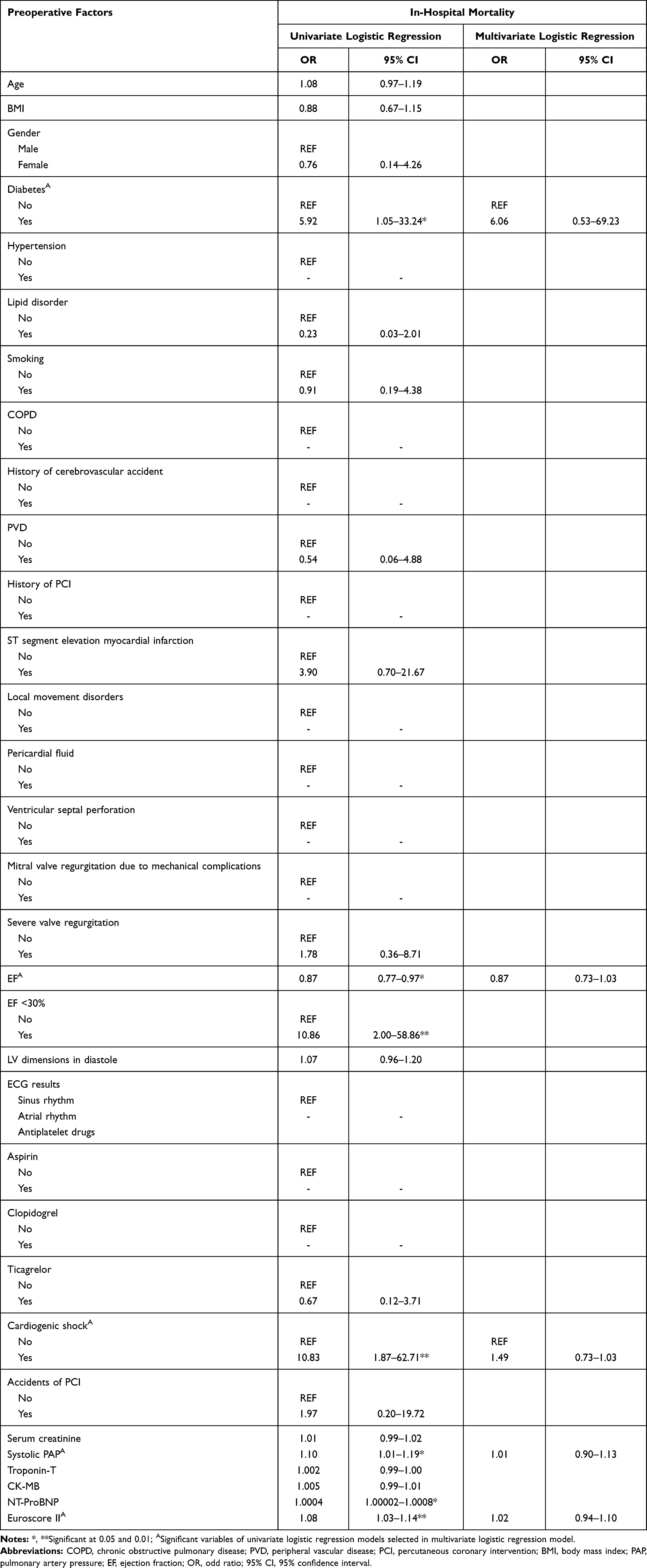 |
Table 4 Preoperative Risk Factors of In-Hospital Mortality in Patients Undergoing Emergency CABG: Univariate and Multivariable Regression Analysis |
Intraoperative Risk Factors of In-Hospital Mortality in Patients Undergoing Emergency CABG
Intraoperative risk factors for in-hospital mortality was shown in Table 5. Univariate logistic regression analysis indicated without grafting with left internal thoracic artery (OR: 0.17, 95% CI: 0.03–0.88), prolonged CPB time (OR: 1.03, 95% CI: 1.01–1.05). In the model of multivariate logistic regression analysis including 3 selected intraoperative risk factors, prolonged CPB time was found to be a significantly independent predictor for in-hospital mortality (OR: 38.87, 95% CI:4.63–325.96). Figure 2 clearly illustrates significant differences of CPB time among in-hospital mortality patient group and in-hospital survival patient group.
 |
Table 5 Intraoperative Risk Factors of In-Hospital Mortality in Patients Undergoing Emergency CABG: Univariate and Multivariable Regression Analysis |
 |
Figure 2 The measurement of cardiopulmonary bypass time among in-hospital mortality patient group and in-hospital survival patient group. |
Postoperative Risk Factors of In-Hospital Mortality in Patients Undergoing Emergency CABG
As was shown in Table 6, postextubation respiratory failure requiring mechanical ventilation (OR: 11.25, 95% CI: 1.85–68.54), ventricular fibrillation (OR: 20.00, 95% CI: 3.28–121.84), dialysis-requiring acute renal failure (OR: 37.5, 95% CI: 5.46–257.59), pneumonia (OR: 10.83, 95% CI: 1.87–62.71), bacterial sepsis (OR: 47.25, 95% CI: 3.96–563.42), gastrointestinal bleeding (OR: 25.20, 95% CI: 1.93–328.39), and prolonged mechanical ventilation time (OR: 1.20, 95% CI: 1.05–1.37) were significantly increased risk factors for in-hospital mortality in univariate logistic regression analysis. In the model 1 of multivariate logistic regression analysis including 7 selected postoperative risk factors (excluding the variable IABP), ventricular fibrillation was significant predictor for in-hospital mortality (OR: 51.95, 95% CI: 1.75–1546.01) (Model 1: Pseudo R2 = 0.6299). The association of postoperative ventricular fibrillation with in-hospital mortality was clearly illustrated in Figure 3. However, no significant association was found in model 2 of multivariate logistic regression analysis that was included the variable IABP (Model 2: Pseudo R2 = 0.6880).
 |
Table 6 Postoperative Risk Factors of In-Hospital Mortality in Patients Undergoing Emergency CABG: Univariate and Multivariable Regression Analysis |
 |
Figure 3 The incidence of in-hospital mortality in postoperative ventricular fibrillation group and without postoperative ventricular fibrillation. |
Discussion
Our study presents the first largest cohort of emergency CABG patients from one large institution in Vietnam. Our hospital mortality rate was 9.86%, with 3 deaths due to severe heart failure, and 4 further patients dying from non-cardiovascular causes (3 those in gastrointestinal bleeding and 1 those in septic shock due to bacterial sepsis). The in-hospital mortality rate in our study belongs to the group below 10%. Comparing with the EuroSCORE II of 14.7%, the mortality rate in our study was lower than forecast. In a retrospective, single-center study of outcomes in 57 patients who underwent emergency CABG, in-hospital mortality rate of 12.2% was reported by Christiansen and Autschbach,13 compared with our rate of 9.86%. In a similar study, Sezai et al14 reported an 11.4% mortality rate for patients after emergency CABG for acute myocardial infarction. However, our in-hospital mortality rate was consistent with a 10-year retrospective cohort of Schumer et al15 (8.7%) and a 10-year multicenter, retrospective study of Biancari et al16 (8.7%). In the studies examining immediate surgical coronary revascularization for acute myocardial infarction, Khaladj et al17 showed a 30-day mortality rate of 6%, slightly lower than ours, while, in another study, Sezai et al14 reported an 11.4% mortality rate for patients after emergency CABG for acute myocardial infarction. Khaladj and Sezai’s cohorts included the patients presenting with acute myocardial infarction, while we analyzed the whole patients undergoing emergency CABG including the group with mechanical complications of acute myocardial infarction that was known with higher death risk. This may be main difference amongst our cohort and Khaladj’ and Sezai’. Despite early mortality rate variations, these studies indicate that mortality rates remain high after emergency CABG and may be greatly dependent on comorbidities and indications for revascularization.
Interestingly, we found the comorbidity of diabetes was known to a risk factor for in-hospital mortality after emergency CABG in univariate analysis, but not being significant in multivariate model. Based on Cox proportional hazards model, Axelsson et al showed that diabetes was a risk factor for poor overall survival with a HR of 1.74.18 However, the risk of diabetes was non-significant for in-hospital mortality in Axelsson’s report.18 Previous studies have shown that patients with diabetes have an increased risk for long-term mortality after emergency CABG, with an even higher risk if other comorbidities such as extracardiac arteriopathy or renal disease are also present. There is a debate in the literature whether diabetes is an independent risk factor for operative mortality after CABG.19,20
One of the main findings of this study was that preoperative EF is a statistically significant risk factor for higher rates of early mortality after CABG, which was consistent with previous evidence.21,22 Patients with a low EF had a worse survival than did patients whose EF was within normal limits. Revascularization in patients with a low EF has been reported by several authors to be superior to medical therapy. Although CABG enables longer survival and a better quality of life than medical therapy, the postsurgical outcomes of patients with a low EF have been shown to be considerably worse than those in patients with a higher EF.23,24
In our study, most patients underwent surgery with CPB (70 out of 71). One patient who did not undergo CPB had right coronary artery dissection after intervention, so we performed one bypass to the right coronary artery by the saphenous vein. There were 2 cases of running CPB but no cardiac arrest. These are 2 patients with acute myocardial infarction with cardiogenic shock due to left anterior descending artery. We initially expected not to use CPB, however, stable hemodynamics was not maintained with the drug. We therefore decided to perform CPB but not cardiac arrest. Importantly, according our current analysis, prolonged CPB time was found to be significantly intraoperative predictor for increasing in-hospital mortality after emergency CABG. This finding was reasonable for our cohort when more prolonged CPB time indicated more complicated surgery, or required more techniques, or very severe heart failure requiring longer-term support.
Postoperative ventricular fibrillation was significantly predictor for in-hospital mortality. Those suffered from ventricular fibrillation after emergency CABG had 51.95 times higher risk of in-hospital mortality compared to those without. Postoperative ventricular fibrillation in our patients indicates severe postoperative heart failure. Other main explanations need to be clearly acknowledged, which may influence the early mortality in patients with postoperative ventricular fibrillation, were the inadequate of equipment after surgery such as ECMO and IABP, along with the payment difficulties of patients and their families. According to our understanding, this may be the first analysis to indicate this association.
A number of limitations should be acknowledged. First, like most similar reports, our study was based on the retrospective evaluation of patient charts and being single-center results. Second, the study had relatively small sample size of patients and some parameters still could not be adequately measured. Third, importantly, with the recent few years’ progress in cardiothoracic surgery, the 3-year time period from which the patients in this study were recruited may also introduce a time factor error. Certainly, more large number of patients in many-year cohort from should be required in further studies from developing countries like Vietnam. Our group recommend caution in interpreting the results of the comparison with the general population because the annual number of patients undergoing CABG in Vietnam is unclear. Because of the scope of the study objective, the medium- and long-term outcomes will be reported by the authors in a follow-up study.
Conclusions
The in-hospital mortality rate was 9.86%. Preoperative risk factors for in-hospital mortality included diabetes, decreased EF, EF below 30%, cardiogenic shock, elevated systolic PAP, elevated NT-ProBNP, and Euroscore II. Without using internal thoracic artery, and prolonged CPB time were increased intraoperative factors for in-hospital mortality risk. In-hospital mortality’ postoperative risk factors were found to be postextubation respiratory failure requiring mechanical ventilation, ventricular fibrillation, dialysis-requiring acute renal failure, pneumonia, bacterial sepsis, gastrointestinal bleeding, and prolonged mechanical ventilation time. Significant predictors determining in-hospital mortality were known as prolonged CPB time in surgery and postoperative ventricular fibrillation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Babaev A, Frederick PD, Pasta DJ, et al. Trends in management and outcomes of patients with acute myocardial infarction complicated by cardiogenic shock. JAMA. 2005;294(4):448–454. doi:10.1001/jama.294.4.448
2. Mehta R, Grab J, O’Brien S, et al. Society of thoracic surgeons national cardiac database investigators: clinical characteristics and in-hospital outcomes of patients with cardiogenic shock undergoing coronary artery bypass surgery: insights from the society of thoracic surgeons national cardiac database. Circulation. 2008;117:876–885. doi:10.1161/CIRCULATIONAHA.107.728147
3. Nieminen MS, Brutsaert D, Dickstein K, et al. EuroHeart Failure Survey II (EHFS II): a survey on hospitalized acute heart failure patients: description of population. Eur Heart J. 2006;27(22):2725–2736. doi:10.1093/eurheartj/ehl193
4. Santarpino G, Ruggieri VG, Mariscalco G, et al. Outcome in patients having salvage coronary artery bypass grafting. Am J Cardiol. 2015;116(8):1193–1198. doi:10.1016/j.amjcard.2015.07.034
5. Hochman JS, Buller CE, Sleeper LA, et al. Cardiogenic shock complicating acute myocardial infarction—etiologies, management and outcome: a report from the SHOCK trial registry. J Am Coll Cardiol. 2000;36(3 Supplement 1):1063–1070. doi:10.1016/S0735-1097(00)00879-2
6. Davierwala PM, Leontyev S, Verevkin A, et al. Temporal trends in predictors of early and late mortality after emergency coronary artery bypass grafting for cardiogenic shock complicating acute myocardial infarction. Circulation. 2016;134(17):1224–1237. doi:10.1161/CIRCULATIONAHA.115.021092
7. Wang W-H, Hsiao S-H, Lin K-L, Wu C-J, Kang P-L, Chiou K-R. Left atrial expansion index for predicting atrial fibrillation and in-hospital mortality after coronary artery bypass graft surgery. Ann Thorac Surg. 2012;93(3):796–803. doi:10.1016/j.athoracsur.2011.11.007
8. Glance LG, Osler TM, Mukamel DB, Dick AW. Effect of complications on mortality after coronary artery bypass grafting surgery: evidence from New York state. J Thorac Cardiovasc Surg. 2007;134(1):53–58. doi:10.1016/j.jtcvs.2007.02.037
9. Nashef SA, Roques F, Sharples LD, et al. EuroSCORE II. Eur J Cardiothorac Surg. 2012;41(4):734–744. doi:10.1093/ejcts/ezs043
10. Thygesen K, Alpert JS, Jaffe AS, et al. Third universal definition of myocardial infarction. J Am Coll Cardiol. 2012;60(16):1581–1598. doi:10.1016/j.jacc.2012.08.001
11. Neglia D, Rovai D, Caselli C, et al. Detection of significant coronary artery disease by noninvasive anatomical and functional imaging. Circ Cardiovasc Imaging. 2015;8(3):e002179. doi:10.1161/CIRCIMAGING.114.002179
12. QxMD Software. Euroscore II. Available from: https://qxmd.com/calculate/calculator_285/EuroSCORE-ii.
13. Christiansen S, Autschbach R. Results and treatment strategy for patients undergoing emergent coronary artery bypass grafting. Ann Thorac Cardiovasc Surg. 2010;16(3):168–173.
14. Sezai A, Hata M, Yoshitake I, et al. Results of emergency coronary artery bypass grafting for acute myocardial infarction: importance of intraoperative and postoperative cardiac medical therapy. Ann Thorac Cardiovasc Surg. 2012;18(4):338–346. doi:10.5761/atcs.oa.11.01821
15. Schumer EM, Chaney JH, Trivedi JR, et al. Emergency coronary artery bypass grafting: indications and outcomes from 2003 through 2013. Tex Heart Inst J. 2016;43(3):214–219. doi:10.14503/THIJ-14-4978
16. Biancari F, Onorati F, Rubino AS, et al. Outcome of emergency coronary artery bypass grafting. J Cardiothorac Vasc Anesth. 2015;29(2):275–282. doi:10.1053/j.jvca.2014.10.019
17. Khaladj N, Bobylev D, Peterss S, et al. Immediate surgical coronary revascularisation in patients presenting with acute myocardial infarction. J Cardiothorac Surg. 2013;8:167. doi:10.1186/1749-8090-8-167
18. Axelsson TA, Mennander A, Malmberg M, Gunn J, Jeppsson A, Gudbjartsson T. Is emergency and salvage coronary artery bypass grafting justified? The Nordic Emergency/Salvage coronary artery bypass grafting study. Eur J Cardiothorac Surg. 2016;49(5):1451–1456.
19. Antunes PE, de Oliveira JF, Antunes MJ. Coronary surgery in patients with diabetes mellitus: a risk-adjusted study on early outcome. Eur J Cardiothorac Surg. 2008;34(2):370–375. doi:10.1016/j.ejcts.2008.05.008
20. Leavitt BJ, Sheppard L, Maloney C, et al. Effect of diabetes and associated conditions on long-term survival after coronary artery bypass graft surgery. Circulation. 2004;110(11 Suppl 1):Ii41–44. doi:10.1161/01.CIR.0000138197.07051.e7
21. Trachiotis GD, Weintraub WS, Johnston TS, Jones EL, Guyton RA, Craver JM. Coronary artery bypass grafting in patients with advanced left ventricular dysfunction. Ann Thorac Surg. 1998;66(5):1632–1639. doi:10.1016/S0003-4975(98)00773-5
22. Bouchart F, Tabley A, Litzler P, Haas-Hubscher C, Bessou J, Soyer R. Myocardial revascularization in patients with severe ischemic left ventricular dysfunction. Long term follow-up in 141 patients. Eur J Cardiothorac Surg. 2001;20(6):1157–1162. doi:10.1016/S1010-7940(01)00982-4
23. Scott SM, Deupree RH, Sharma GV, Luchi RJVA. Study of unstable angina. 10-year results show duration of surgical advantage for patients with impaired ejection fraction. Circulation. 1994;90(5 Pt 2):Ii120–123.
24. Christakis GT, Weisel RD, Fremes SE, et al. Coronary artery bypass grafting in patients with poor ventricular function. Cardiovascular surgeons of the university of Toronto. J Thorac Cardiovasc Surg. 1992;103(6):1083–1091. doi:10.1016/S0022-5223(19)34872-X
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.