Back to Journals » Clinical Ophthalmology » Volume 19
Impact of Intraocular Lens Design on Refractive Endpoint Selection: A Call for a New Paradigm
Authors Skrzypecki J, Przybek-Skrzypecka J ![]()
Received 9 July 2025
Accepted for publication 14 October 2025
Published 27 November 2025 Volume 2025:19 Pages 4325—4334
DOI https://doi.org/10.2147/OPTH.S552549
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Janusz Skrzypecki,1 Joanna Przybek-Skrzypecka2
1Department of Experimental Physiology and Pathophysiology, Medical University of Warsaw, Warsaw, Poland; 2Department of Ophthalmology, Medical University of Warsaw, Warsaw, Poland
Correspondence: Janusz Skrzypecki, Department of Experimental Physiology and Pathophysiology, Medical University of Warsaw, Banacha 1B, Warsaw, 02-097, Poland, Tel +22 116 6195, Fax +22 57 20 734, Email [email protected]
Abstract: As intraocular lens (IOL) technology continues to evolve, the selection of an optimal refractive target has become increasingly complex and critical to achieving patient satisfaction following cataract surgery or refractive lens exchange. A recently proposed classification system divides IOLs into partial- and full-range-of-field categories based on defocus curve characteristics. However, this framework does not fully capture the diversity of modern IOL designs or account for key optical factors such as spherical aberration and lens-specific tolerance to residual refractive error. This review highlights the importance of understanding the interaction between IOL optical properties—particularly spherical aberration profiles—and refractive target strategies. It examines how different IOL designs, including enhanced monofocal, extended depth-of-field (EDOF), and full-range-of-vision lenses (eg, multifocal or spiral optics), respond to various refractive targets. The evidence suggests that a universal refractive target (eg, plano) may be suboptimal for many advanced IOLs and that customized refractive planning—often incorporating mini-monovision or asymmetrical targets—can improve visual outcomes. Future research should aim to standardize defocus measurement techniques and refine classification systems to better guide clinical decision-making.
Keywords: intraocular lens, monovosion, depth of field, depth of focus
Introduction
Cataract is the opacification of the crystalline lens, a transparent structure essential for focusing light onto the retina. The standard treatment is lens extraction followed by implantation of an intraocular lens (IOL). Increasingly, cataract surgery is considered a refractive procedure, aiming not only to restore lens transparency but also to minimize defocus and provide functional vision at distance, intermediate, and near. To this end, various IOL designs have been introduced: monofocal IOLs provide a single focal point, typically for distance vision; when combined with a monovision strategy, one eye is targeted for distance and the fellow eye for near, thereby extending the range of vision; and multifocal or extended-depth-of-field (EDOF) designs, redistribute or elongate the focus of light to improve visual performance across multiple distances.1,2
A new classification system for IOLs has recently been proposed to accommodate the growing diversity of lens designs aimed at enhancing pseudoaccommodation and reducing dependence on spectacles. This framework goes beyond the traditional distinction between monofocal and multifocal IOLs by introducing broader categories—namely, partial -range-of-vision and full- range-of-vision IOLs—based on optical characteristics, particularly the defocus curve.3
This classification allows for the inclusion of emerging technologies, such as lenses with spiral optics or truly accommodating IOLs. Nevertheless, most currently available IOLs achieve extended visual performance by either splitting or elongating the focal point on the retina.4 Many optical designs have been introduced to achieve this goal. Monofocal plus IOLs are designed to increase positive spherical aberration or are shaped to enhance central optical power, thereby improving near or intermediate vision.4,5 EDOF IOLs feature a variety of designs, including diffractive, refractive, and pinhole optics.5 Full- range-of-vision IOLs encompass multifocal lenses with diffractive or refractive optics, as well as newer designs incorporating spiral optics6,7 (Table 1). Even among monofocal lenses, distinctions exist: some utilize positive spherical aberration (spherical designs), while others are aspherical with negative spherical aberration, or are neutral with respect to spherical aberration.8,9
 |
Table 1 Classification of IOL Types with Key Optical Features and Spherical Aberration Profiles |
Given that the ultimate goal of cataract surgery and refractive lens exchange with IOL implantation is to achieve a predetermined functional refractive outcome, it is essential to determine the optimal refractive target for each IOL design. This includes potential differences in target refraction between the dominant and non-dominant eyes (Table 2).
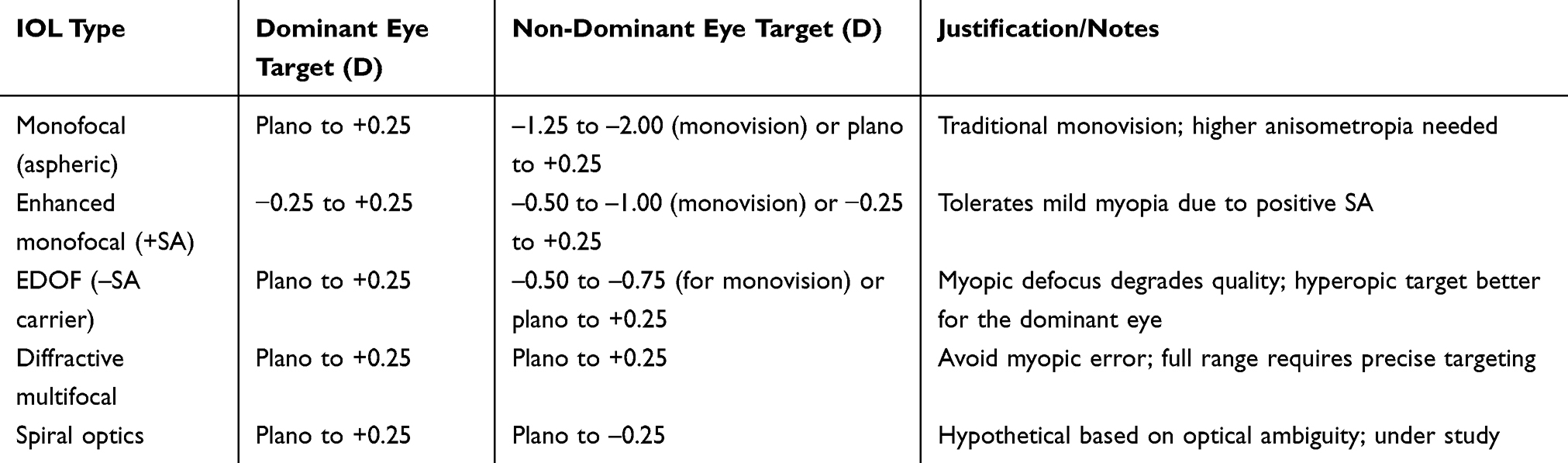 |
Table 2 Tentative Refractive Target Recommendations for Different IOL Types Based on Current Evidence (Subject to Validation in Clinical Trials) |
This is especially important because any remaining refractive error that impairs the expected visual outcome is one of the strongest predictors of patient dissatisfaction after cataract surgery.10
Moreover, some surgeons advocate for a mix-and-match strategy, in which different types of IOLs are implanted in each eye.11 While this approach may enhance visual performance across distances, it introduces additional complexity in selecting appropriate refractive targets and necessitates a thorough, evidence-based evaluation.12
Finally, it is important to emphasize that while pseudoaccommodative lenses increase depth of field, they significantly reduce depth of focus compared to monofocal IOLs. As a result, the traditional refractive target of plano (0.00 D), derived from experience with monofocal lenses, may not be ideal for these advanced designs. However, only a limited number of studies have specifically addressed this issue.13
First, we will review key optical and functional concepts that require improved standardization in future research on optimal refractive targets for various IOLs. These include defocus curve measurement, monovision, and the distinction between depth of focus and depth of field.
Next, we will examine the current evidence on refractive targets that provide the best functional outcomes for different IOL types, with reference to the recently proposed classification of IOLs.
Search Methodology
We performed a targeted search of PubMed, Embase, Cochrane Library, Web of Science, and Scopus on IOL designs affecting refractive targets and tolerance to residual refractive error. The following keywords were utilized: full-range-of-field, multifocal, extended depth-of-field, monofocal, enhanced monofocal, pseudoaccommodation, refractive target, residual refractive error, defocus curve, and spherical aberration. Two reviewers independently screened records. As a narrative (not systematic) review, we omit a PRISMA diagram.
Key Optical and Functional Concepts
Defocus Curve Measurement Techniques in the Context of the New IOL Classification
In 2024, a new classification of IOLs was proposed based on monocular defocus curves.14 The authors categorized IOLs into two groups: partial -range-of-field lenses, which tolerate less than 2.3 diopters of defocus while maintaining a visual acuity of 0.2 logMAR or better, and full -range-of-field lenses, which tolerate at least 2.3 diopters under the same visual acuity threshold.14 Partial- range-of-field IOLs are further divided into monofocal IOLs, enhanced monofocal IOLs and EDOF IOLs. Full- range-of-field IOLs are further divided based on the shape of their defocus curve.14
However, this classification has several limitations. It overlooks the low reproducibility of defocus curve measurements and fails to account for critical factors such as IOL design and performance under hyperopic defocus.15 This is especially important because certain IOLs — such as enhanced monofocals with positive spherical aberration — can tolerate a slightly myopic refractive target without compromising distance vision.16 This effectively broadens their functional pseudoaccommodation, a property not captured by current classification systems. In contrast, IOLs with negative spherical aberration may perform better under mild hyperopic defocus, further underscoring the need for a more nuanced and design-aware classification framework.
It should also be emphasized that the interaction between the specific design of a pseudoaccommodative IOL and factors influencing the variability of defocus curve measurements may lead to inconsistent outcomes. In his 2022 review, Prof. Kohnen pointed out that defocus curve testing is not standardized and is prone to bias related to the testing conditions.15 Several variables may significantly affect the measured level of pseudoaccommodation, including pupil size, dioptric step intervals, and distance from the visual acuity chart.15
Furthermore, some authors suggest that biometric parameters, such as axial length, may influence the shape and interpretation of the defocus curve for a given IOL.17 This underscores the importance of controlling for biometric variability when comparing defocus curves across different lenses, particularly in studies involving diverse patient populations.
Authors also critically evaluate the methods used to compare defocus curves and note that direct curve-to-curve comparisons may not be the most reliable approach.18 Instead, they recommend alternative metrics such as the range of vision—defined as the total dioptric range over which visual acuity remains above a predetermined level—or the area under the defocus curve, both of which may offer a more comprehensive assessment of functional performance.15
Monovision
Monovision is one of the most commonly used techniques for correcting presbyopia. Traditionally employed with monofocal IOLs, it is now increasingly applied with newer pseudoaccommodative lenses, which allow for milder degrees of monovision while still achieving a high level of spectacle independence.19 Moreover, advancements in IOL technology—particularly those that expand the depth of field—now provide functional intermediate vision, which is typically not attainable with traditional full-monovision strategies.19
However, the optimal degree of monovision remains a subject of debate, particularly in the context of different IOL types.20
Although ocular dominance tests are commonly performed—based on the assumption that the non-dominant eye better tolerates distance blur resulting from near correction—the clinical relevance of these tests is controversial. While various methods have been developed to assess ocular dominance, growing evidence suggests that ocular dominance is a fluid phenomenon, potentially shifting with changes in gaze direction or visual task.21
Moreover, several authors argue that sighting dominance—as assessed by standard tests such as the hole-in-the-card or shooting test—is a poor predictor of monovision tolerance. In contrast, contact lens trials that alternate monovision between eyes, though time-consuming, may offer the most accurate assessment of individual patient preference.22
Interestingly, some clinical studies report that assigning the near correction to the preoperatively determined dominant eye does not negatively affect patient satisfaction.23
Moreover, sensory eye dominance may contribute to the determination of ocular dominance. It describes the phenomenon in which the visual cortex assigns greater weight to input from one eye than from the other. Although long considered stable in adulthood, growing evidence indicates that sensory eye dominance retains a degree of neuroplasticity. This is further supported by studies suggesting that preoperative identification of the dominant eye may not always be essential.24
Finally, monovision appears to be a reasonable alternative to diffractive IOLs. In a study comparing diffractive IOL implantation with monovision using monofocal lenses set to −1.25 D in the non-dominant eye, patients in the monovision group were significantly less likely to request an IOL exchange.25
Depth of Focus vs Depth of Field
While discussing pseudoaccommodative lenses, it is important to differentiate between two seemingly similar terms: depth of focus and depth of field. Depth of field refers to the situation in which the object is repositioned, yet the patient is still able to perceive a clear image. In contrast, depth of focus describes the degree of deviation of light from the retinal plane that is still tolerable for the patient. By definition, monofocal lenses have the greatest depth of focus but the smallest depth of field. In contrast, multifocal IOLs provide the greatest depth of field but the lowest depth of focus—that is, they are less tolerant of residual refractive error.3,25,26
Longitudinal Spherical Aberration and Zernike Representation of Spherical Aberration
For a clearer understanding of refractive target selection in IOLs with varying amounts of spherical aberration, it is essential to distinguish between longitudinal spherical aberration and the Zernike representation of spherical aberration. Clinically, we often conceptualize spherical aberration longitudinally—where positive spherical aberration causes peripheral light rays to focus in front of the retina (suggesting a myopic effect), and negative spherical aberration causes them to focus behind the retina (suggesting a hyperopic effect). However, measurement devices quantify spherical aberration using Zernike polynomials, specifically Z (4, 0), where the interpretation differs: positive Zernike spherical aberration is associated with hyperopic defocus, while negative Zernike spherical aberration leads to myopic defocus. Recognizing this distinction is crucial for accurate refractive targeting, as misunderstanding the direction of induced defocus may result in suboptimal postoperative outcomes.27
Refractive Target Selection
Partial-Range-of-Field IOLs
Monofocal Intraocular Lenses
Schallhorn et al demonstrated that residual myopia in the range of –0.25 to –0.50 D has a stronger negative impact on patient satisfaction following monofocal IOL implantation than an equivalent amount of residual hyperopia.28 This finding challenges the common assumption that a mildly myopic outcome of –0.17 D, which corresponds to 20/20 vision on a reading chart positioned at 6 meters (ie, plano for infinity), represents the optimal refractive target.29
However, when interpreting these results, it is important to consider that the study primarily analyzed aspheric monofocal IOLs with a negative spherical aberration profile.28 Because spherical aberration is typically expressed in Zernike terms, it is relevant that negative spherical aberration induces a slight myopic shift in best focus. Thus, aiming mildly hyperopic (eg, +0.25 D) may yield a functional plano and optimize distance performance. Moreover, when an aberration-neutralizing IOL is used and a slight hyperopic target is selected, residual sources of “pseudophakic accommodation” (eg, pupil dynamics, subtle IOL position changes with ciliary contraction) can pull the focal point onto the retina. By contrast, implanting the same aberration-neutralizing IOL with a mild myopic target offers no comparable compensatory mechanism and may therefore degrade distance vision.30
Historically, spherical monofocal IOLs were the first to be introduced to the market. These lenses induce positive spherical aberration, which may lead to a positive defocus, further complicating the relationship between refractive outcome and functional vision. In that context, slight residual myopia might have appeared advantageous for improving near vision, but these effects are influenced by the IOL’s optical design—particularly its spherical aberration profile.
Numerous studies have compared pseudoaccommodation between spherical monofocal IOLs (with positive spherical aberration) and aspheric monofocal IOLs (with negative spherical aberration), but their results have been inconsistent.31–33 To our knowledge, none of these studies consider that pseudoaccommodation with spherical IOLs could be enhanced by setting a slightly myopic refractive target. This approach could improve near vision without compromising distance visual acuity, due to the positive defocus effect associated with positive Zernike spherical aberration. In contrast, leaving slight myopic defocus in a lens with negative spherical aberration would impair distance vision – which is in line with observations by Schallhorn et al.28 Moreover, majority of studies assess the defocus curve using best distance correction, which effectively shifts the positive defocus induced by spherical aberration behind the retina—thus negating the potential pseudo accommodation benefits of a properly set myopic target.
This reasoning aligns with a recent study by Kozaya et al, which demonstrated that adding positive Zernike spherical aberration to a distance-corrected monofocal IOL does not improve pseudoaccommodation.34
Therefore, we believe that achieving the best functional outcomes depends on setting a personalized and precisely targeted postoperative refraction.
In the context of monovision, monofocal IOLs require a higher degree of anisometropia to achieve functional near vision.25 However, inducing greater myopia in the non-dominant eye may compromise intermediate vision and reduce stereoacuity. Studies have shown that even with a refractive target of –1.25 D, stereoacuity remains inferior compared to patients implanted with bilateral multifocal IOLs.25,35 Nevertheless, other studies have demonstrated that monovision up to –2.0 D, as well as crossed monovision—where the dominant eye is targeted for –2.0 D—are generally well tolerated.36 Interestingly, some authors report patient satisfaction rates as high as 90% with monovision targeted at –2.75 D,37 while groups targeted at –1.25 D showed the lowest satisfaction, primarily due to inadequate unaided near vision.25,38
That said, eyes implanted with monofocal IOLs are less likely to require an IOL exchange as compared with multifocal IOL, although this comes at the cost of a higher percentage of patients needing spectacles for certain visual tasks.25
Nevertheless, additional studies directly comparing full monovision and multifocal IOLs are needed to determine which option offers better outcomes for patients.
Enhanced Monofocal IOLs
Enhanced monofocal IOLs have only recently been introduced with the aim improve intermediate vision without compromising distance vision.39 Compared to other partial-range-of-focus lenses, they exert significantly less negative impact on distance visual quality. Consequently, there is growing support for the idea that enhanced monofocal lenses could become the standard of care in cataract surgery.40
These lenses are classified as partial-range-of-focus IOLs, providing a functional depth of field corresponding to a visual acuity of 0.2 logMAR within a defocus range of approximately 1.2 to 1.58 diopters.14 Despite being grouped together, they differ significantly in optical design. For instance, the Tecnis Eyhance (Johnson & Johnson, USA) increases refractive power centrally through a gradual elevation of curvature.41 In contrast, the Rayner EMV (Rayner, Germany) is specifically engineered to induce a controlled increase in positive spherical aberration.16,42 The Isopure (BVI Medical, USA) and VIVINEX Impress (Hoya, Japan) lenses utilize optics that extend the focal range both anterior and posterior to the primary focal point for distance vision.43,44
Given these IOL-specific differences, the strategy to maximize visual function and minimize spectacle dependence should be tailored to lens design. In our experience, Tecnis Eyhance achieves these benchmarks most reliably when targeted at plano or slight hyperopia, whereas Rayner EMV, Isopure, and Impress tend to perform best with a mild myopic target.
Interestingly, a recent study by Zeilinger et al reported that manifest refraction in non-dominant eye of patients implanted with Rayner EMV was less myopic than in those with the Vivity (Alcon, USA),45 despite both being targeted for mini-monovision in the non-dominant eye. The authors attribute the difference to a non-optimized lens constant; however, they do not report the A-constant, and the early A-constant was in fact higher—so more myopic, not hyperopic, early outcomes would be expected. An alternative explanation is earlier attainment of distance acuity during subjective refraction in 0.25-D steps, consistent with a hyperopic shift from positive spherical aberration (as noted above).
Moreover, the latest classification of IOLs based on depth of field relies on defocus curves obtained in eyes corrected for distance. This approach may underestimate the functional performance of certain lenses, particularly those designed to enhance pseudoaccommodation with a myopic target without compromising distance vision.
It is also plausible that tolerance to mini-monovision or full monovision varies depending on the lens design. Lenses that induce positive spherical aberration or extend the depth of focus by creating inflection points in the central or full optic zone—such as Isopure and Hoya VIVINEX Impress—may facilitate smoother blending of defocus. This contrasts with lenses like the Eyhance, which rely primarily on a central refractive profile change.46,47
Regarding monovision strategies, clinical studies have shown that enhanced monofocal lenses targeted at –0.5 D in the non-dominant eye can provide functional binocular near vision.45 Targets of –1.0 D may offer even greater comfort for near tasks without compromising overall visual quality or patient satisfaction.4 A recent meta-analysis found no significant differences in spectacle independence when comparing monovision (non-dominant eye targeted up to –2.0 D) among monofocal, enhanced monofocal, and EDOF lenses.48 However, the myopic targets in the EDOF and enhanced monofocal groups were significantly lower (–0.75 D) compared to the monofocal group (up to –2.0 D). Other studies have shown that when the same myopic target (–0.75 D to –1.25 D) is applied across lens types, enhanced monofocal IOLs provide superior near and intermediate vision performance.4
Extended Depth-of-Field Lenses
The American Academy of Ophthalmology has established consensus guidelines for the definition and clinical evaluation of EDOFi IOLs. According to these guidelines, studies should include a minimum of 100 patients in the EDFOF IOL group, with a control group of comparable composition for valid comparisons. The EDFOF IOL must demonstrate monocular best-corrected distance visual acuity (BCDVA) that is statistically noninferior to that of monofocal IOLs, using a noninferiority margin of 0.1 logMAR and a one-sided significance level of 0.05. Additionally, the monocular depth of focus in the EDFOF group must exceed that of the monofocal control by at least 0.5 diopters at the 0.2 logMAR (20/32) acuity level. Intermediate visual performance is also a critical measure: the mean monocular distance-corrected intermediate visual acuity (DCIVA) should be assessed under photopic conditions at a testing distance of 66 cm at six months postoperatively. This metric must demonstrate statistical superiority over the control group using a one-sided significance level of 0.025. Furthermore, at least 50% of eyes in the EDF group must achieve a monocular DCIVA of logMAR 0.2 (20/32) or better at 66 cm, assessed with a chart using 0.1 log unit steps, such as the ETDRS chart. These criteria ensure that EDF IOLs provide not only acceptable distance acuity but also a demonstrably enhanced range of functional vision.49
These lenses provide good intermediate vision and can also offer functional near vision when used with monovision. However, spectacle independence for near tasks in micro-monovision (up to −0.75 D) is typically lower compared to multifocal IOLs. The advantage, though, is significantly reduced photic phenomena such as glare and halos, which is particularly low in IOLs which do not use diffractive optics.11,50
Optical bench studies suggest that residual myopic refractive error may cause a greater decline in visual quality with EDOF lenses—especially those with diffractive optics—compared to hyperopic error. This aligns with the fact that most EDOF lenses incorporate negative spherical aberration in the carrier optic, which induces mild myopic defocus. Additionally, these lenses are designed to provide pseudoaccommodation, ideally in a continuous manner, which tends to compensate more effectively for hyperopic defocus than for myopic error.3
Most studies take a conservative approach to monovision with EDOF lenses.51 Therefore the outcomes suggest that these lenses should not be implanted in patients who desire complete independence from glasses. Yet, since these lenses extend the depth of field by approximately 1.5 D, higher levels of monovision should not compromise patient satisfaction. For example, in the Presbyond (Zeiss, Germany) approach—where the dominant eye’s depth of field is smaller than that achieved with an EDOF IOL—a monovision target of −1.5 D is commonly used without adverse outcomes.52 Moreover, some reports indicate that even more pronounced levels of monovision, up to −3.25 D, may still be well tolerated by certain patients.53
Nevertheless, there are reports that patients are intolerant of mini-monovision at the level of −0.75D spherical equivalent.11 Therefore, an effort should be undertaken to precisely identify group of patients who would benefit from this approach. Particularly, population of patients with clear lens which undergo refractive lens exchange and population of cataract patients should be differentiated. Finally, patients with preexisting anisometropia should be offered a monovision approach.
Studies also show that patients implanted with EDOF lenses maintain excellent stereopsis at both distance and near.54
Available evidence confirms that EDOF lenses offer a broader depth of field than standard monofocal lenses, and an extended depth of focus that provides resilience to residual refractive errors within ±0.50 D of the intended target.3
Full-Range-of Field IOLs
Full-range-of field are classified as IOLs which provide defocus of 2.3D at the level of visual acuity of 0.2logMAR. It is known that intraocular lenses that provide wide range of field have a narrow focus therefore are very sensitive to any residual refractive error, tilt or decentration.55 Therefore, it is very important to assess precise refractive target for each optical construction which will provide full-range-of field.
There are reports showing that full-range-of field IOLs are very sensitive to any residual refractive error.3 Schallhorn et al has shown that patient’s implanted with multifocal IOLs are more satisfied with residual hyperopia than residua myopia.28 This might be related to the fact that the carrier optic of many multifocal IOLs has negative spherical aberration that produces myopic defocus.11,28
Nevertheless, there are various types of full-range-of field IOls available, including diffractive, refractive or spiral optics available. To the best of our knowledge no studies analyzed the refractive targets for these types of IOLs.
The recently introduced spiral optic design in Rayner Galaxy IOLs (Rayner, Germany) is particularly intriguing. However, detailed optical data from the manufacturer is currently unavailable, and there is ongoing discussion about the lens’s functional zones—specifically, whether the carrier optic is optimized for distance or intermediate vision, while the spiral optic contributes to near and intermediate, or possibly near and far vision.56,57 Given this uncertainty, it would be valuable to investigate whether a mini-monovision approach—setting the dominant eye slightly hyperopic and the non-dominant eye slightly myopic relative to plano—could enhance pseudoaccommodation with this lens design.
Regarding the diffractive optics we know that these lenses have low tolerance of residual refractive error and the data presented by Schallhorn et al shows that the refractive target should be set at the lowest plus possible.28 One study comparing Panoptix (Alcon, USA) with Rayone Trifocal (Rayner, Germany) showed that the halo effect is larger with myopic defocus in Rayone Trifocal but not in Panoptix.58 This is however another study which showes that slight hyperopic error, particularly in IOLs with negative spherical aberration would be better for patients than slight myopic error. Optical bench studies also show that dispersion of light is higher with myopic defocus than with hyperoic defocus.3
Conclusion
Based on the comprehensive review, it is evident that refractive target selection must be individualized and tailored to the optical design of the IOL. The traditional “plano” target, derived from experience with monofocal lenses, may not be ideal for modern pseudoaccommodative IOLs—especially those with altered spherical aberration or complex optical structures such as diffractive, refractive, or spiral optics. The new classification of IOLs into partial and full range-of-field categories reflects the diversity in lens behavior, but limitations in defocus curve standardization, measurement bias, and neglect of IOL-specific design factors suggest the need for a more nuanced, evidence-based approach to refractive planning.
Furthermore, clinical and optical data consistently indicate that the same refractive error may yield different outcomes depending on the IOL’s spherical aberration profile. Lenses with negative spherical aberration often benefit from a slight hyperopic target, while those with positive aberration may tolerate or even benefit from mild myopia. Additionally, strategies such as mini-monovision or crossed monovision can enhance spectacle independence when properly matched to lens design, though tolerance varies by patient and IOL type. Ultimately, refractive target optimization—especially in newer lens designs like enhanced monofocal, EDOF, and spiral-optic IOLs—remains critical for achieving patient satisfaction and maximizing the functional range of vision after cataract or refractive lens surgery.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. O’Brart D. The future of cataract surgery. Eye. 2025;39(8):1451–1456. doi:10.1038/s41433-025-03745-x
2. Chen SP, Woreta F, Chang DF. Cataracts: a review. JAMA. 2025;333(23):2093–2103. doi:10.1001/jama.2025.1597
3. Black DA, Bala C, Alarcon A, Vilupuru S. Tolerance to refractive error with a new extended depth of focus intraocular lens. Eye. 2024;38(Suppl 1):15–20. doi:10.1038/s41433-024-03040-1
4. Beltraminelli T, Rizzato A, Toniolo K, Galli A, Menghini M. Comparison of visual performances of enhanced monofocal versus standard monofocal IOLs in a mini-monovision approach. BMC Ophthalmol. 2023;23(1):170. doi:10.1186/s12886-023-02920-6
5. Kanclerz P, Toto F, Grzybowski A, Alio JL. Extended depth-of-field intraocular lenses: an update. Asia Pac J Ophthalmol. 2020;9(3):194–202. doi:10.1097/APO.0000000000000296
6. Kaymak H, Potvin R, Neller K, Klabe K, Anello RD, Group NS. Customizing clinical outcomes with implantation of two diffractive trifocal IOLs of identical design but differing light distributions to the far, intermediate and near foci. Clin Ophthalmol. 2024;18:1009–1022. doi:10.2147/OPTH.S456007
7. Salerno LC, Tiveron MC, Alio JL. Multifocal intraocular lenses: types, outcomes, complications and how to solve them. Taiwan J Ophthalmol. 2017;7(4):179–184. doi:10.4103/tjo.tjo_19_17
8. Stern B, Saad A, Gatinel D. In vitro comparison of an aspherical monofocal lens inducing positive spherical aberrations with a spherical lens. J Refract Surg. 2025;41(5):e481–e491. doi:10.3928/1081597X-20250403-02
9. McCabe CM, Peterson R, Hull J, Bala C. Impact of aspheric monofocal intraocular lens implantation on uncorrected intermediate visual acuity: a combined analysis. Clin Ophthalmol. 2024;18:1491–1501. doi:10.2147/OPTH.S458125
10. Nakagawa S, Kato Y, Totsuka K, Kanda S, Okinaga K, Ishii K. Surgically induced astigmatism and refractive outcomes after minimally invasive glaucoma surgery combined with cataract surgery. Sci Rep. 2025;15(1):13966. doi:10.1038/s41598-025-96619-x
11. Alvarez-Garcia MT, Fuente-Garcia C, Munoz-Puyol C, Pinero DP. Clinical outcomes with extended depth of focus intraocular lenses in cases in which multifocal lenses are not primarily recommended. J Ophthalmol. 2023;2023:8814627. doi:10.1155/2023/8814627
12. Naujokaitis T, Labuz G, Khoramnia R, Auffarth GU. Review of mix-and-match approach and binocular intraocular lens systems. J Clin Med. 2025;14(12):4263. doi:10.3390/jcm14124263
13. Jackson MA, Edmiston AM, Bedi R. Optimum refractive target in patients with bilateral implantation of extended depth of focus intraocular lenses. Clin Ophthalmol. 2020;14:455–462. doi:10.2147/OPTH.S237457
14. Ribeiro F, Dick HB, Kohnen T, et al. Evidence-based functional classification of simultaneous vision intraocular lenses: seeking a global consensus by the ESCRS Functional Vision Working Group. J Cataract Refract Surg. 2024;50(8):794–798. doi:10.1097/j.jcrs.0000000000001502
15. Kohnen T, Lemp-Hull J, Suryakumar R. Defocus curves: focusing on factors influencing assessment. J Cataract Refract Surg. 2022;48(8):961–968. doi:10.1097/j.jcrs.0000000000000906
16. Madhivanan N, Nivean PD, Madanagopalan VG, Priya S, Madhivanan N, Arthi M. Clinical results after binocular implantation of a unique nondiffractive enhanced monofocal intraocular lens designed for enhanced monovision to increase the depth of focus. Indian J Ophthalmol. 2024;72(1):63–65. doi:10.4103/IJO.IJO_447_23
17. Gimenez-Calvo G, Bartol-Puyal FA, Altemir I, et al. Influence of ocular biometric factors on the defocus curve in an enlarged depth-of-focus intraocular lens. Int Ophthalmol. 2023;43(3):945–955. doi:10.1007/s10792-022-02496-y
18. Law EM, Buckhurst HD, Aggarwal RK, et al. Optimising curve fitting techniques to look for standardisation of the analysis of defocus curves derived from multifocal intraocular lenses. Ophthalmic Physiol Opt. 2022;42(4):887–896. doi:10.1111/opo.12986
19. Evans BJ. Monovision: a review. Ophthalmic Physiol Opt. 2007;27(5):417–439. doi:10.1111/j.1475-1313.2007.00488.x
20. Levy I, Shah RP, Mukhija R, Nanavaty MA. Outcomes of mini-monovision with monofocal, enhanced monofocal and extended depth-of-focus intraocular lenses. Front Med. 2025;12:1522383. doi:10.3389/fmed.2025.1522383
21. Min SH. Ocular dominance plasticity: a mini-review. Eye Brain. 2025;17:37–48. doi:10.2147/EB.S532627
22. Rodriguez-Lopez V, Barcala X, Zaytouny A, Dorronsoro C, Peli E, Marcos S. Monovision correction preference and eye dominance measurements. Transl Vis Sci Technol. 2023;12(3):18. doi:10.1167/tvst.12.3.18
23. Fujita Y, Nomura Y, Itami E, Oshika T. A comparative study of mini-monovision, crossed mini-monovision, and emmetropia with enhanced monofocal intraocular lenses. Sci Rep. 2025;15(1):916. doi:10.1038/s41598-024-80663-0
24. Ooi TL, He ZJ. Sensory eye dominance: relationship between eye and brain. Eye Brain. 2020;12:25–31. doi:10.2147/EB.S176931
25. Wilkins MR, Allan BD, Rubin GS, et al. Randomized trial of multifocal intraocular lenses versus monovision after bilateral cataract surgery. Ophthalmology. 2013;120(12):2449–2455e1. doi:10.1016/j.ophtha.2013.07.048
26. Marcos S, Moreno E, Navarro R. The depth-of-field of the human eye from objective and subjective measurements. Vision Res. 1999;39(12):2039–2049. doi:10.1016/s0042-6989(98)00317-4
27. Skrzypecki J, Izdebska J, Ordon AJ, Przybek-Skrzypecka J, Szaflik JP. Spherical aberrations and their role in modern ophthalmology. Clin Exp Optom. 2023;106(7):703–710. doi:10.1080/08164622.2022.2160235
28. Schallhorn SC, Hettinger KA, Hannan SJ, Venter JA, Teenan D, Schallhorn JM. Effect of residual sphere on uncorrected visual acuity and satisfaction in patients with monofocal and multifocal intraocular lenses. J Cataract Refract Surg. 2024;50(6):591–598. doi:10.1097/j.jcrs.0000000000001418
29. Kniestedt C, Stamper RL. Visual acuity and its measurement. Ophthalmol Clin North Am. 2003;16(2):155–70, v. doi:10.1016/s0896-1549(03)00013-0
30. Stern B, Gatinel D. Comment on: impact of spherical aberration on visual quality and depth of focus. J Cataract Refract Surg. 2024;50(12):1297–1298. doi:10.1097/j.jcrs.0000000000001551
31. Nishi T, Taketani F, Ueda T, Ogata N. Comparisons of amplitude of pseudoaccommodation with aspheric yellow, spheric yellow, and spheric clear monofocal intraocular lenses. Clin Ophthalmol. 2013;7:2159–2164. doi:10.2147/OPTH.S52771
32. Shentu X, Tang X, Yao K. Spherical aberration, visual performance and pseudoaccommodation of eyes implanted with different aspheric intraocular lens. Clin Exp Ophthalmol. 2008;36(7):620–624. doi:10.1111/j.1442-9071.2008.01856.x
33. Thiagarajan M, McClenaghan R, Anderson DF. Comparison of visual performance with an aspheric intraocular lens and a spherical intraocular lens. J Cataract Refract Surg. 2011;37(11):1993–2000. doi:10.1016/j.jcrs.2011.05.046
34. Kozhaya K, Kenny PI, Esfandiari S, Wang L, Weikert MP, Koch DD. Effect of spherical aberration on visual acuity and depth of focus in pseudophakic eyes. J Cataract Refract Surg. 2024;50(1):24–29. doi:10.1097/j.jcrs.0000000000001314
35. Labiris G, Toli A, Perente A, Ntonti P, Kozobolis VP. A systematic review of pseudophakic monovision for presbyopia correction. Int J Ophthalmol. 2017;10(6):992–1000. doi:10.18240/ijo.2017.06.24
36. Xun Y, Wan W, Jiang L, Hu K. Crossed versus conventional pseudophakic monovision for high myopic eyes: a prospective, randomized pilot study. BMC Ophthalmol. 2020;20(1):447. doi:10.1186/s12886-020-01694-5
37. Greenbaum S. Monovision pseudophakia. J Cataract Refract Surg. 2002;28(8):1439–1443. doi:10.1016/s0886-3350(02)01218-x
38. Xiao J, Jiang C, Zhang M. Pseudophakic monovision is an important surgical approach to being spectacle-free. Indian J Ophthalmol. 2011;59(6):481–485. doi:10.4103/0301-4738.86318
39. Dell SJ, Hannan SJ, Venter JA, et al. Comparative analysis of clinical and patient-reported outcomes of a new enhanced monofocal IOL and a conventional monofocal IOL. Clin Ophthalmol. 2024;18:1157–1169. doi:10.2147/OPTH.S456332
40. Campos N. Clinical outcomes and patient satisfaction of an enhanced depth of focus intraocular lens targeted for mini-monovision. Clin Ophthalmol. 2024;18:1607–1613. doi:10.2147/OPTH.S459868
41. Gigon E, Bouthour W, Panos GD, Pajic B, Massa H. Real world outcomes of the new Tecnis Eyhance IOL. Eur J Ophthalmol. 2023;33(3):1390–1397. doi:10.1177/11206721221146675
42. Garcia-Bella J, Burgos-Blasco B, Vidal-Villegas B, Garzon N, Villanueva C, Garcia-Feijoo J. Visual and refractive outcomes after bilateral implantation of an enhanced monofocal intraocular lens: prospective study. J Cataract Refract Surg. 2024;50(6):585–590. doi:10.1097/j.jcrs.0000000000001422
43. Ansari E. The BVI ISOPURE((R)) 123 intraocular lens: a new hydrophobic preloaded extended monofocal IOL with intermediate vision correction. Front Ophthalmol. 2023;3:1330335. doi:10.3389/fopht.2023.1330335
44. Kabura R, Takeshita T, Furushima K, et al. Comparative evaluation of clinical results and patient-reported outcomes of enhanced monofocal and conventional monofocal intraocular lenses. J Cataract Refract Surg. 2025;51(6):520–524. doi:10.1097/j.jcrs.0000000000001641
45. Zeilinger J, Kronschlager M, Schlatter A, et al. Comparing an advanced monofocal with a non-diffractive extended depth of focus intraocular lens using a mini-monovision approach. Am J Ophthalmol. 2025;271:86–95. doi:10.1016/j.ajo.2024.10.014
46. Tandogan T, Urbonavicius A, Langenegger M, Goldblum D, Tappeiner C. Erfahrungen aus dem klinischen Alltag mit der Hoya Vivinex Impress Intraokularlinse mit einer erweiterten Tiefenscharfe [Real-world clinical results with the Hoya Vivinex impress intraocular lens with enhanced depth of focus]. Klin Monbl Augenheilkd. 2024;241(4):374–377. doi:10.1055/a-2220-0620
47. Fernandez J, Rocha-de-Lossada C, Zamorano-Martin F, Rodriguez-Calvo-de-Mora M, Rodriguez-Vallejo M. Positioning of enhanced monofocal intraocular lenses between conventional monofocal and extended depth of focus lenses: a scoping review. BMC Ophthalmol. 2023;23(1):101. doi:10.1186/s12886-023-02844-1
48. Li J, Sun B, Zhang Y, et al. Comparative efficacy and safety of all kinds of intraocular lenses in presbyopia-correcting cataract surgery: a systematic review and meta-analysis. BMC Ophthalmol. 2024;24(1):172. doi:10.1186/s12886-024-03446-1
49. MacRae S, Holladay JT, Glasser A, et al. Special report: American Academy of Ophthalmology Task Force consensus statement for extended depth of focus intraocular lenses. Ophthalmology. 2017;124(1):139–141. doi:10.1016/j.ophtha.2016.09.039
50. Pusnik A, Petrovski G, Lumi X. Dysphotopsias or unwanted visual phenomena after cataract surgery. Life. 2022;13(1):53. doi:10.3390/life13010053
51. Wanten JC, Bauer NJC, Berendschot T, van den Biggelaar F, Nuijts R. Two novel extended depth-of-focus intraocular lenses targeted for mini-monovision: a prospective randomized controlled trial. Am J Ophthalmol. 2025;276:286–296. doi:10.1016/j.ajo.2025.04.024
52. Russo A, Reinstein DZ, Filini O, et al. Visual and refractive outcomes following laser blended vision with non-linear aspheric micro-anisometropia (PRESBYOND) in myopic and hyperopic patients. J Refract Surg. 2022;38(5):288–297. doi:10.3928/1081597X-20220323-01
53. Lentz PC, Stockard A, Wagner IV, Ten Hulzen RD. Extreme monovision with EDOF intraocular lenses. JCRS Online Case Rep. 2024;12(4):e00127.
54. He Y, Zhu B, Li B, Zou H, Ma Y. Stereopsis following implantation of presbyopia-correcting intraocular lenses: a narrative review. Ophthalmol Ther. 2024;13(9):2331–2341. doi:10.1007/s40123-024-01004-y
55. Guo D, Meng J, Zhang K, et al. Tolerance to lens tilt and decentration of two multifocal intraocular lenses: using the quick contrast sensitivity function method. Eye Vis. 2022;9(1):45. doi:10.1186/s40662-022-00317-y
56. Spiral optics presentation and explanations [Hompage on the Internet]. Available from: https://www.gatinel.com/spiral-optics-presentation-and-explanations/.
57. Galinier L, Renaud-Goud P, Brusau J, Kergadallan L, Augereau J, Simon B. Spiral diopter: freeform lenses with enhanced multifocal behavior. Optica. 2024;11(2):238–244.
58. Rementeria-Capelo LA, Contreras I, Garcia-Perez JL, Blazquez V, Ruiz-Alcocer J. Visual performance and impact of residual refractive errors with trifocal intraocular lenses of different aspheric design. Eur J Ophthalmol. 2022:11206721221144928. doi:10.1177/11206721221144928
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.