Back to Journals » International Journal of Women's Health » Volume 17
Impact of Different Delivery Modalities on Maternal and Neonatal Outcomes During Prolonged Deceleration in the Second Stage of Labor: A Retrospective Study
Authors Jian WQ, Yang F, Jian J, He MP, Yuan CL, Huang JC, Wei QF, Zhao KS ![]()
Received 28 September 2025
Accepted for publication 9 December 2025
Published 31 December 2025 Volume 2025:17 Pages 5839—5850
DOI https://doi.org/10.2147/IJWH.S570950
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Wen Qian Jian,1,* Feng Yang,2,* Jun Jian,3 Mei Ping He,1 Chun Lan Yuan,1 Jian Chun Huang,1 Qing Fang Wei,1 Kai Sun Zhao1
1Department of Obstetrics, The Third Affiliated Hospital of Guangxi Medical University, The Second Nanning People’s Hospital, Nanning, Guangxi, 530031, People’s Republic of China; 2Department of Gynaecology, The Third Affiliated Hospital of Guangxi Medical University, The second Nanning People’s Hospital, Nanning, Guangxi, 530031, People’s Republic of China; 3Department of Anesthesiology, The Third Affiliated Hospital of Guangxi Medical University, The Second Nanning People’s Hospital, Nanning, Guangxi, 530031, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Kai Sun Zhao, Department of Obstetrics, The Third Affiliated Hospital of Guangxi Medical University, The Second Nanning People’s Hospital, No. 13, Dancun Road, Jiangnan District, Nanning City, Guangxi Zhuang Autonomous Region, People’s Republic of China, Tel +86 0771 4808241, Email [email protected] Qing Fang Wei, Department of Obstetrics, The Third Affiliated Hospital of Guangxi Medical University, The Second Nanning People’s Hospital, No. 13, Dancun Road, Jiangnan District, Nanning City, Guangxi Zhuang Autonomous Region, People’s Republic of China, Tel +86 0771 4808241, Email [email protected]
Objective: To investigate the effects of three delivery methods—vacuum extraction, forceps-assisted delivery, and cesarean section—on maternal and neonatal outcomes during prolonged deceleration (PD) in the second stage of labor, providing evidence-based support for clinical decision-making.
Methods: This retrospective cohort study analyzed 114 singleton, term pregnancies with vertex presentation experiencing PD in the second stage of labor between January 2022 and December 2024. Participants were categorized by delivery method: vacuum extraction (n=62), forceps delivery (n=30), and cesarean section (n=22). Primary outcomes included maternal morbidity indicators (eg, blood loss, hospital stay) and neonatal outcomes (eg, umbilical artery pH, NICU admission).
Results: The cesarean section group had a higher fetal station, a longer deceleration-to-delivery interval, and significantly increased maternal morbidity, including longer postpartum hospital stay, higher costs, extended antibiotic use and catheterization, and greater blood loss compared to instrumental delivery groups (all P < 0.05). The forceps group had a higher incidence of wound erythema than the cesarean group (P < 0.05). Critically, neonatal outcomes were comparable across all three groups (P > 0.05).
Conclusion: During PD in the second stage of labor, both operative vaginal delivery and cesarean section present a trade-off between maternal morbidity and procedural expediency. The choice of delivery method should be individualized, based on a rapid assessment of fetal station, labor progress, and operator expertise, as neonatal short-term outcomes were similar regardless of the mode of delivery.
Keywords: second stage of labor, prolonged deceleration, cesarean section, vacuum extraction, forceps delivery
Introduction
Against the backdrop of declining global fertility rates,1 improving the childbirth experience holds significant strategic importance for enhancing fertility intentions and addressing negative population growth. With the widespread adoption of electronic fetal monitoring (EFM), clinicians’ ability to identify fetal heart rate deceleration patterns has markedly improved. Prolonged deceleration (PD) is defined as a decrease in fetal heart rate of 15 beats per minute (bpm) or more below the baseline, lasting for at least 2 minutes but less than 10 minutes; if it persists for 10 minutes or longer, it is classified as a baseline change.2–4 The primary mechanisms involve fetal myocardial hypoxia and vagal reflexes. The clinical management of PD remains contentious. Some experts regard it as a sign of acute fetal distress, advocating for active intervention and expedited delivery.4 Conversely, others suggest that not all PD episodes require immediate cesarean section, especially when caused by reversible factors such as uterine tachysystole or maternal supine hypotension.2,5 Moreover, increasing duration or depth of deceleration significantly raises the risk of neonatal acidosis and adverse outcomes.6 In the first stage of labor, there is a general clinical consensus to consider cesarean delivery when persistent decelerations indicate acute fetal hypoxia, aiming to optimize perinatal outcomes.7 In contrast, decision-making in the second stage is more complex, involving a choice between proceeding with an operative vaginal delivery (vacuum or forceps) or performing a full-dilatation cesarean section, each with distinct maternal and neonatal risks. The American College of Obstetricians and Gynecologists (ACOG) advises against the combined use of vacuum extractor and forceps in an operative vaginal delivery.8 Selecting the appropriate delivery mode is crucial for optimizing both maternal and neonatal outcomes.9 Despite its clinical significance, comparative evidence on the outcomes of these different approaches specifically during PD in the second stage is scarce.
This study aimed to compare the impact of vacuum extraction, forceps delivery, and cesarean section on maternal and neonatal outcomes following PD in the second stage of labor. Our goal is to provide evidence-based guidance to assist obstetric teams in making timely and rational decisions, ultimately enhancing maternal and neonatal safety.
Materials and Methods
Study Population and Design
This single-center retrospective observational study was conducted at Nanning Second People’s Hospital. We included singleton, vertex-presenting pregnancies at ≥34 weeks gestation who experienced PD in the second stage of labor between January 2022 and December 2024. PD was defined per standard criteria:2–4 a fetal heart rate deceleration of ≥15 bpm below baseline, lasting ≥2 minutes but <10 minutes, occurring after full cervical dilation.
Inclusion and Exclusion Criteria
Inclusion criteria were:
(1) PD in the second stage;
(2) singleton, vertex presentation;
(3) gestational age ≥34 weeks;
(4) complete clinical data.
Exclusion criteria were categorized as:
(1) Fetal factors: non-vertex presentation, known congenital anomalies, multiple gestation.
(2) Maternal factors: significant comorbidities (eg, severe preeclampsia, cardiac disease), pelvic deformities.
(3) Delivery outcome: spontaneous vaginal delivery after PD.
After screening, 114 patients were enrolled and stratified by delivery method: vacuum extraction (n=62, KIWI system), forceps delivery (n=30, Simpson forceps), and cesarean section (n=22). All operative vaginal deliveries were conducted at fetal station ≥+2, whereas the cesarean group predominantly had station ≤+2.
Clinical Management and Data Collection
The decision to intervene and the choice of delivery method were at the discretion of the attending obstetrician, based on a comprehensive assessment including fetal station, position, estimated fetal weight, maternal pelvis, and clinical urgency. Standard intrauterine resuscitation (maternal repositioning, oxygen, intravenous fluids) was routinely attempted prior to intervention.
The case selection process involved retrieving all cases containing the keyword “prolonged deceleration” from the electronic medical record system. Cases where PD did not occur in the second stage, as well as five cases where PD occurred in the second stage but culminated in spontaneous vaginal delivery, were excluded. Ultimately, enrolled patients were divided into three groups based on delivery method: a vacuum extraction group (n=62, using KIWI vacuum system), a forceps delivery group (n=30, using Simpson forceps), and a cesarean section group (n=22). All women undergoing operative vaginal delivery had fetal station ≥+2; in contrast, the cesarean group had fetal station ≤+2. (Fetal station was defined as follows: the leading point of the fetal skull at the level of the ischial spines is “0”; one centimeter below the spines is “+1”, and so forth).
This study was approved by the Ethics Committee of Nanning Second People’s Hospital. Given its retrospective nature and anonymized data, the committee waived the requirement for informed consent in accordance with the Declaration of Helsinki and relevant regulations.
Data Were Extracted from Electronic Medical Records and Included
Baseline characteristics: maternal age, BMI, parity, hemoglobin.
Fetal monitoring parameters: deceleration-to-delivery interval, number/duration/depth of decelerations.
Neonatal outcomes: birth weight, umbilical artery blood gas (pH, lactate), NICU admission. (Umbilical cord blood was routinely sampled immediately after delivery for gas analysis). (pH < 7.20 is a critical threshold for neonatal asphyxia diagnosis,10 indicating neonatal acidosis.11)
Maternal outcomes: estimated blood loss (measured via gravimetric + volumetric suction), postpartum hospital stay, hospitalization costs, antibiotic/catheter duration, and complications (eg, wound erythema, fever).
Related Work Disclosure: This study utilizes a cohort that overlaps with that of a related study by our group focusing on risk factors for umbilical acidosis during prolonged deceleration. The two manuscripts address distinct, sequential research questions (risk factors vs. management outcomes) and are reported separately to maintain analytical clarity.12
Statistical Analysis
Statistical analyses were performed using SPSS version 29.0. Categorical data are expressed as numbers (percentages) and compared with the chi-square (χ2) test; Fisher’s exact test was used when expected cell counts were less than 5. Continuous data were assessed for normality. For normally distributed variables, results are presented as mean ± standard deviation (SD), and group comparisons were conducted using one-way analysis of variance (ANOVA). For non-normally distributed variables, results are expressed as median (interquartile range, IQR), and comparisons among groups used the Kruskal–Wallis H-test. Post-hoc pairwise comparisons used the Bonferroni correction. A P-value < 0.05 was considered statistically significant for all analyses. Given the sample size limitations, findings were interpreted with emphasis on clinical significance. Given the sample size limitations, findings were interpreted with emphasis on clinical significance. In the results presentation, exact P-values are reported where appropriate, and P < 0.001 is used to denote high statistical significance beyond the preset threshold.
Results
Comparison of Baseline Characteristics
No statistically significant differences were observed among the three groups regarding maternal age, pre-pregnancy BMI, pre-delivery BMI, gestational weight gain, gravidity, or parity (all P > 0.05), (Table 1).
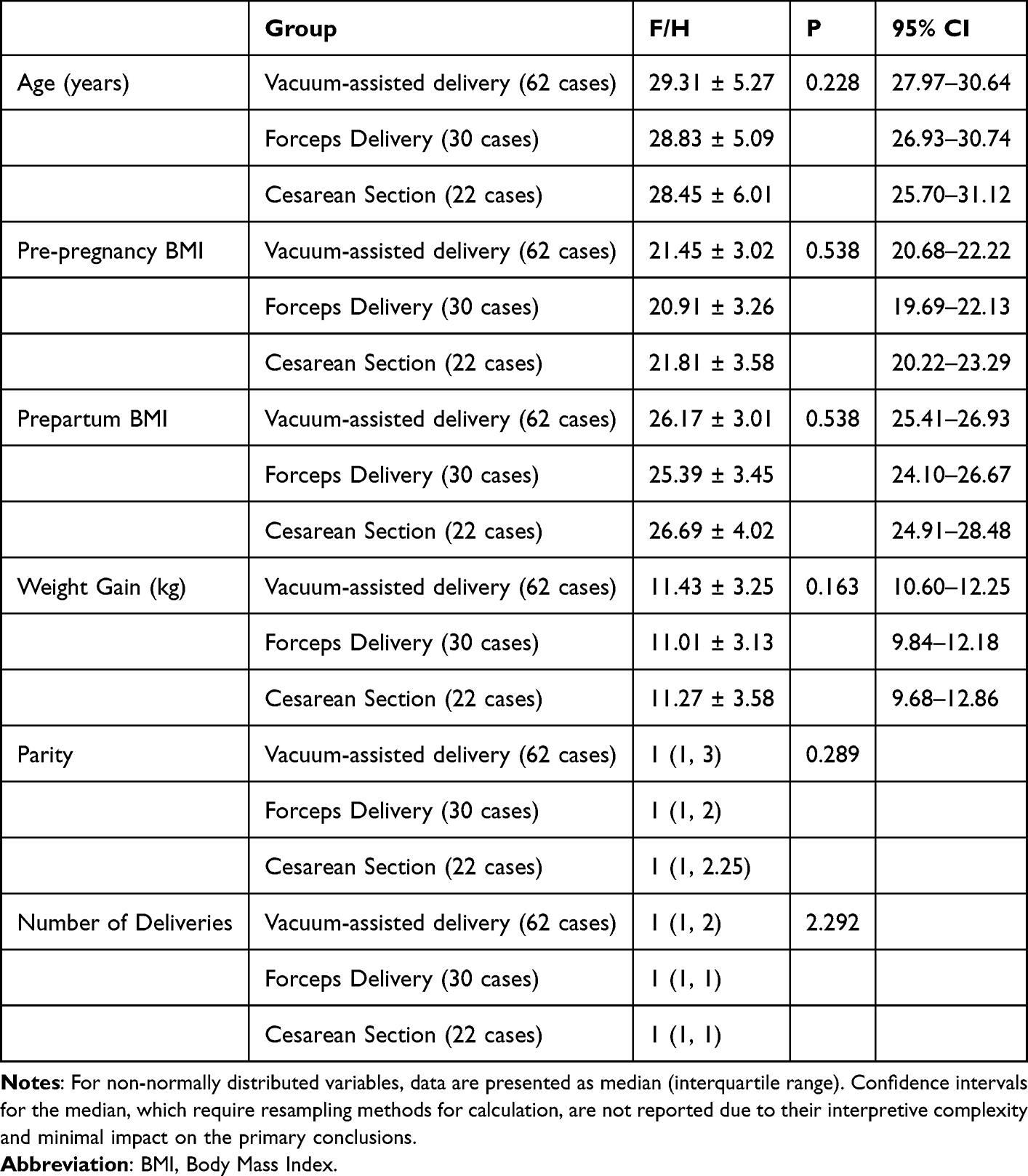 |
Table 1 Comparison of General Data of the Three Groups |
Comparison of Fetal Monitoring Indicators and Pregnancy Charact
Key differences were observed in parameters influencing delivery method selection and timing (Table 2). The deceleration-to-delivery interval was significantly longer in the cesarean section group compared to both the vacuum and forceps groups (P < 0.05). Conversely, the number of deceleration episodes was lower in the cesarean group than in the vacuum group (P < 0.05). Fetal station was significantly higher (less descent) in the cesarean group than in both operative vaginal delivery groups (P < 0.001). Pre-delivery hemoglobin was lower in the vacuum group than in the forceps group (P < 0.05). No significant differences were found in other fetal monitoring parameters or pregnancy complication rates.
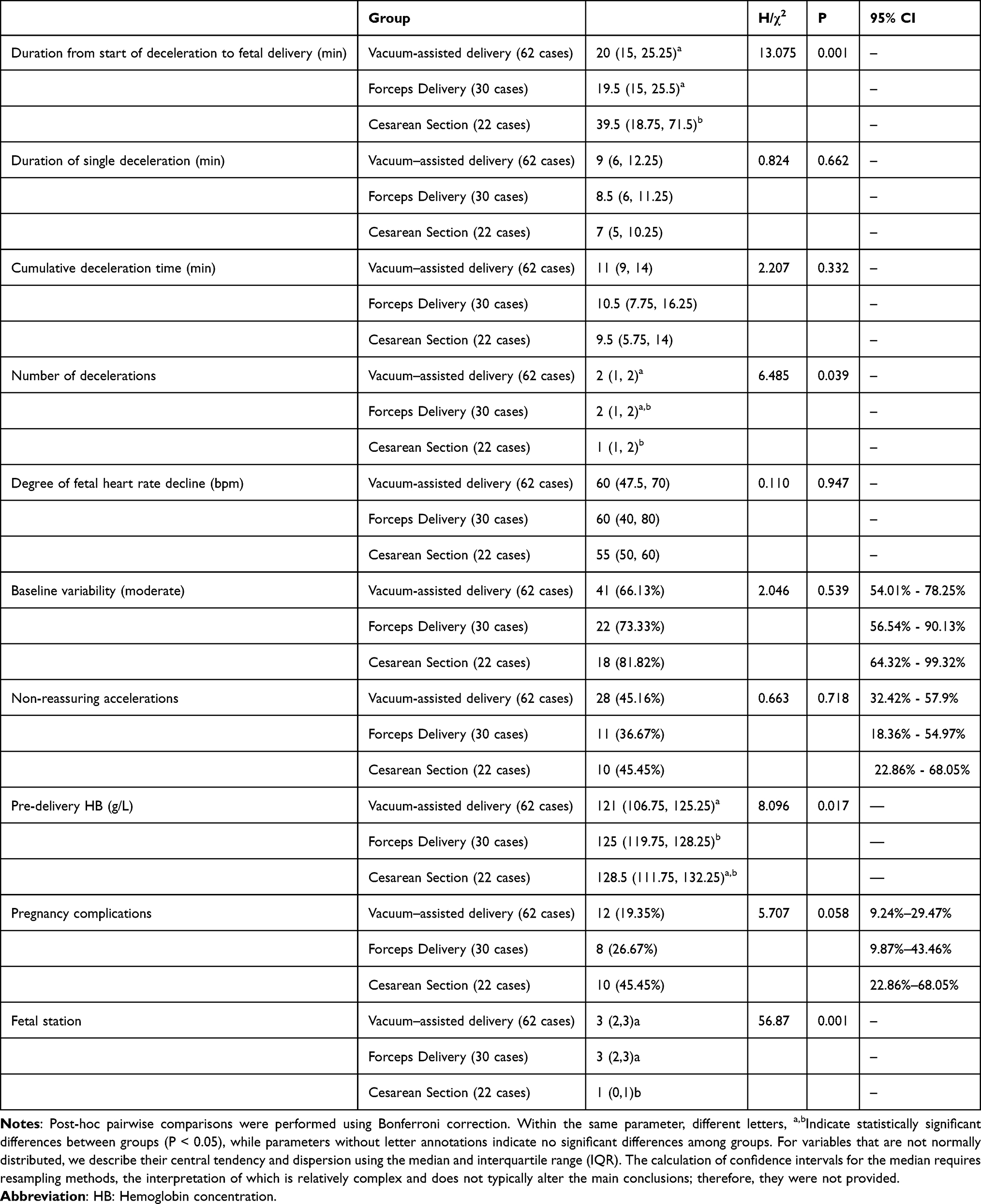 |
Table 2 Comparison of Fetal Monitoring Indicators and Pregnancy Conditions |
Neonatal Outcomes
Most importantly, no statistically significant differences were observed among the three groups for any neonatal outcome measure, including birth weight, gestational age, umbilical artery pH <7.20, lactate levels, rates of neonatal asphyxia, or NICU admission (all P > 0.05, Table 3).
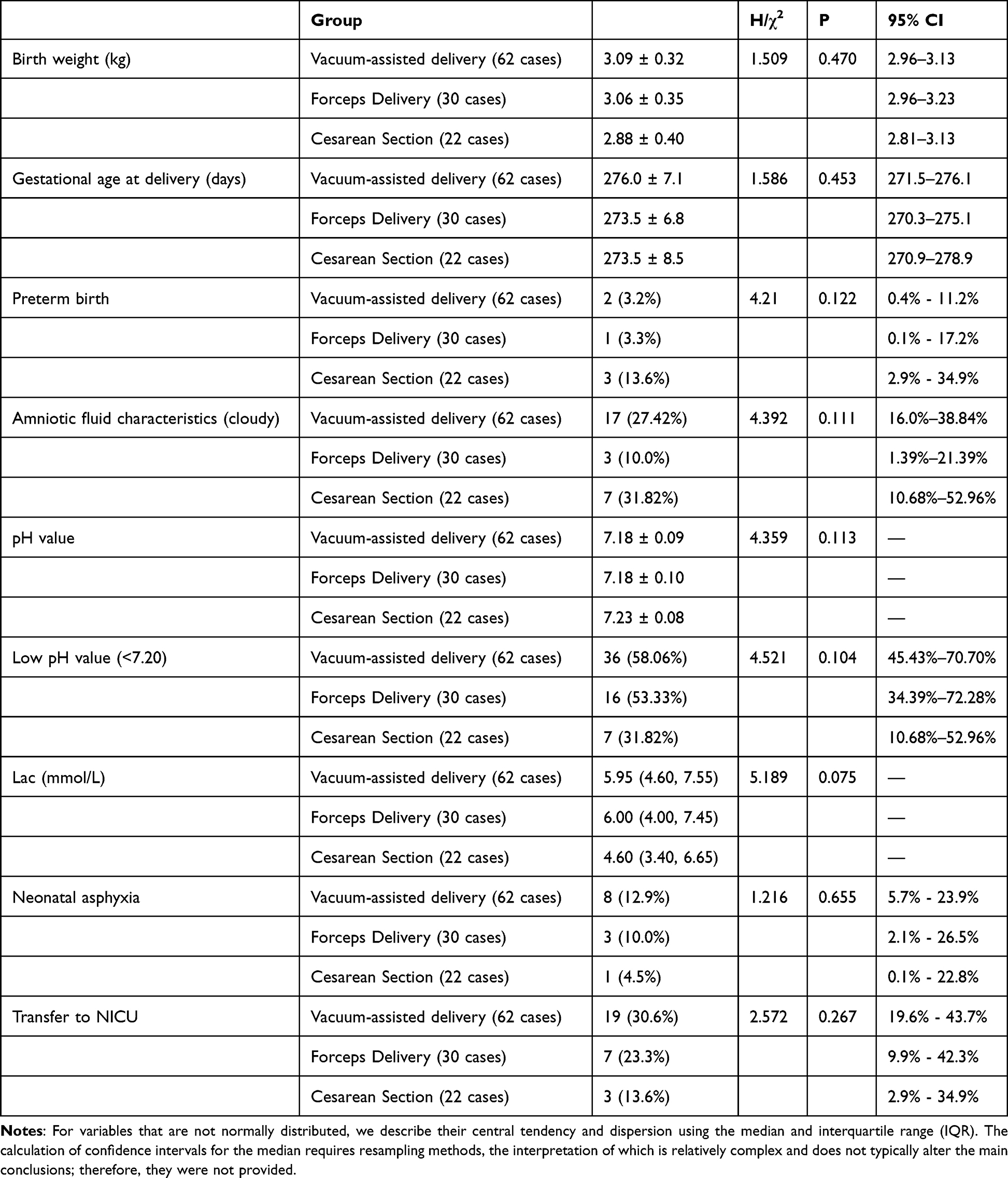 |
Table 3 Comparison of Neonatal Outcomes |
Maternal Outcomes
Cesarean section was associated with significantly increased maternal morbidity across multiple domains (Table 4). The cesarean group had a longer postpartum hospital stay, higher hospitalization costs, longer durations of antibiotic use and urinary catheterization, and greater estimated blood loss compared to both operative vaginal delivery groups (all P < 0.001). The incidence of wound erythema was higher in the forceps group than in the cesarean group (P < 0.05). No significant differences were found in rates of urinary retention, postpartum fever, or postpartum hemorrhage (as defined by blood loss ≥1000mL) among the groups.
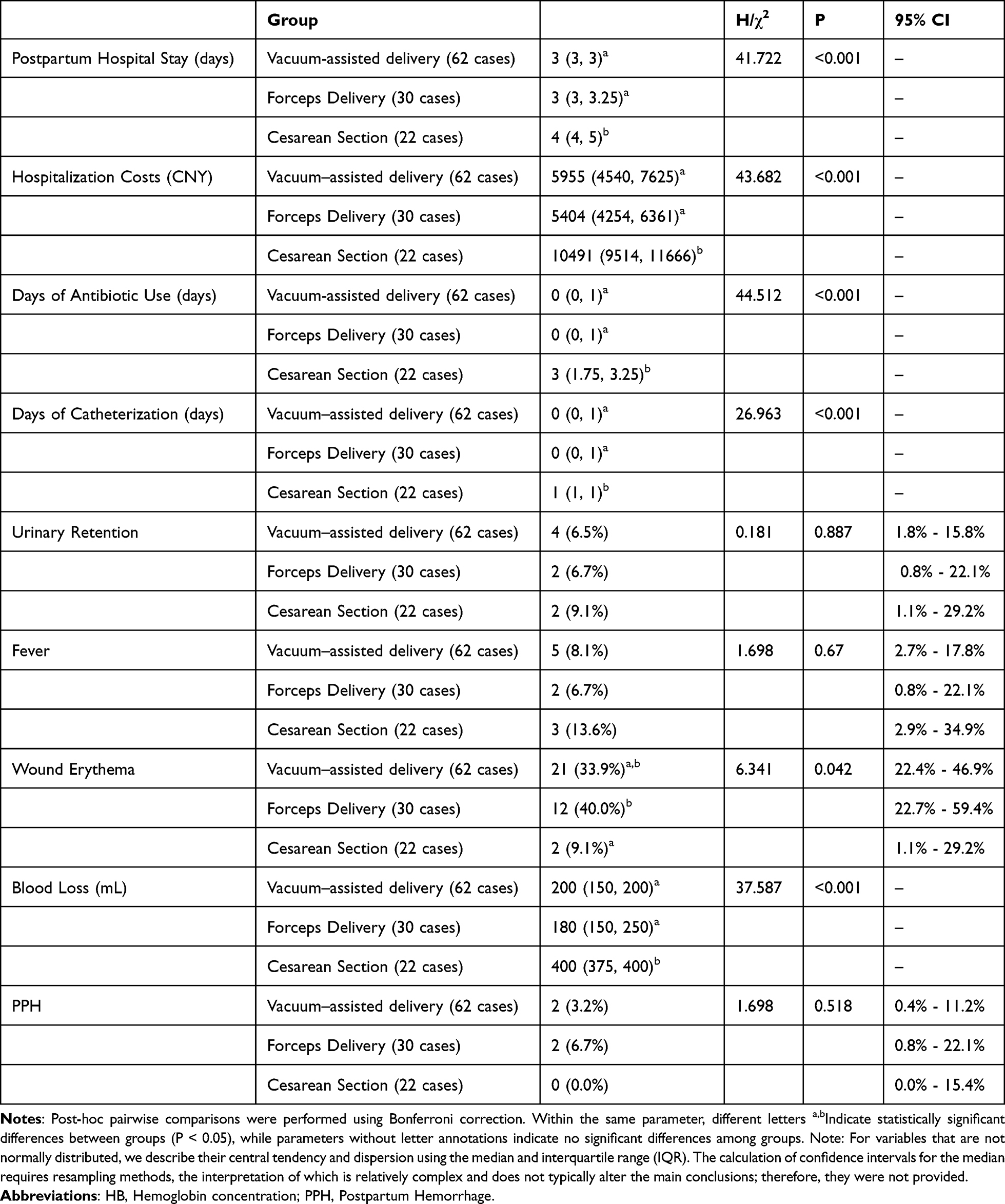 |
Table 4 Comparison of Maternal Outcomes |
Discussion
This retrospective study analyzed 114 cases of PD occurring in the second stage of labor to compare maternal and neonatal outcomes associated with three delivery methods: vacuum extraction, forceps delivery, and cesarean section. The principal findings indicate a distinct trade-off between these approaches. Cesarean section was associated with a longer interval from deceleration to delivery, significantly increased postpartum blood loss, prolonged hospitalization, and higher medical costs. However, the fewer deceleration episodes recorded in this group suggest that the decision for surgical intervention may have been made at an earlier stage of the fetal heart rate abnormality.
In contrast, operative vaginal delivery (vacuum extraction and forceps) demonstrated a significant advantage in shortening the duration of potential fetal compromise and offered benefits in terms of reduced maternal trauma and faster recovery. Nonetheless, forceps delivery was linked to a higher incidence of perineal wound erythema. The lower pre-delivery hemoglobin level observed in the vacuum extraction group may indicate underlying baseline differences in this patient cohort.
Collectively, these results underscore that there is no single universally optimal delivery method for managing PD in the second stage of labor. The cornerstone of clinical decision-making lies in a rapid, structured assessment: when fetal station is favorable (≥ +2) and an experienced operator is available, operative vaginal delivery should be prioritized to expedite delivery and minimize maternal morbidity; whereas cesarean section is reserved for high fetal stations (≤ +1) or when vaginal delivery is unsafe, with the understanding that it carries greater maternal morbidity.8,13,14 The choice between vacuum and forceps involves a balance of risks, with forceps posing a higher risk of maternal perineal trauma and vacuum extraction carrying a greater risk of neonatal scalp injury.15–18
Analysis of Fetal Monitoring Indicators and Baseline Characteristics
Our results indicate that the interval from the onset of fetal heart rate deceleration to delivery was significantly longer in the cesarean section group compared to both the vacuum extraction and forceps groups (P<0.05). Conversely, the number of deceleration episodes recorded was significantly lower in the cesarean section group than in the two operative vaginal delivery groups (P<0.05). No significant differences were observed among the three groups in other fetal monitoring parameters, including the duration of single deceleration episodes, total deceleration time, depth of deceleration, baseline variability, or the presence of non-periodic accelerations (P>0.05). These findings suggest that different management strategies for PD in the second stage of labor have distinct time-related implications. Upon identifying PD, clinicians must promptly investigate possible causes, such as maternal circulatory compromise (eg, supine hypotension), umbilical cord prolapse, vagal reflex triggered by rapid fetal descent, uterine tachysystole, or prolonged uterine contractions.2,19 If fetal heart rate abnormalities persist despite corrective measures, especially if evolving into a prolonged deceleration lasting more than 10 minutes (which indicates terminal bradycardia),4,13 expedited delivery becomes critical.
The longer interval from deceleration to delivery in the cesarean group primarily reflects the necessary time for transferring the patient to the operating room, administering anesthesia, and completing preoperative preparations. Additionally, interruptions in fetal monitoring during these processes likely contributed to the fewer recorded deceleration episodes in this group. This underscores the importance of efficient multidisciplinary collaboration and standardized protocols to minimize fetal hypoxia exposure during obstetric emergencies.20 Fetal station was a key factor influencing delivery mode selection. The significantly higher fetal station (indicating less descent) in the cesarean section group compared to the operative vaginal delivery groups (P<0.05) aligns with clinical practice, as a fetal station of ≤ +2 is generally considered unfavorable for successful instrumental delivery.14 Therefore, immediate assessment of fetal station at the occurrence of PD is crucial. Subsequent decision-making should incorporate this information along with fetal descent degree, maternal condition, labor progress, and operator experience to rapidly select the safest and most effective delivery method.
Regarding baseline characteristics, the pre-delivery hemoglobin level was significantly lower in the vacuum extraction group than in the forceps and cesarean groups (P<0.05). Considering the retrospective design and the unequal group sizes (vacuum extraction, n=62; forceps, n=30; cesarean, n=22), this finding might be influenced by confounding factors. Whether pre-delivery hemoglobin levels affect the choice of delivery method during second-stage emergencies, and how they impact maternal and neonatal outcomes, warrants further investigation in larger, prospective studies.
Analysis of Neonatal Outcomes
The pathophysiology of PD during the second stage of labor primarily involves fetal myocardial hypoxia and the vagal reflex.21 When fetal monitoring indicates Category II or III patterns, it suggests a potential hypoxic state, which triggers a compensatory shift to anaerobic metabolism. This results in increased lactate production and accumulation. Given lactate’s neurotoxicity and the high susceptibility of brain tissue to hypoxia, the buildup of lactate significantly increases the risk of cerebral cell injury, forming a core pathological basis for severe complications such as hypoxic-ischemic encephalopathy.22 Failure to promptly correct hypoxia elevates the risks of neonatal acidosis, need for NICU admission, and birth asphyxia, which in severe cases can progress to multi-organ dysfunction or perinatal death.23
This study demonstrated no statistically significant differences among the three groups in various neonatal outcomes, including birth weight, gestational age at delivery, preterm birth rate, amniotic fluid characteristics, umbilical artery pH, incidence of acidosis (pH<7.20), lactate levels, rates of birth asphyxia, or NICU admissions (all P > 0.05). We posit that the timely recognition of PD and the subsequent expedited intervention itself—irrespective of the final route—is the most critical factor in preserving neonatal well-being. The comparable neonatal results across the three delivery modalities likely reflect a balance of their respective advantages and disadvantages, mitigated by prompt action. However, it is crucial to note that our study assessed only short-term neonatal outcomes; long-term neurodevelopmental follow-up studies are warranted to rule out more subtle differences.24,25
Instrumental vaginal delivery can enable rapid fetal expulsion, potentially reducing intrauterine hypoxia duration. Forceps-assisted delivery is particularly effective for swift completion of labor and may be associated with a lower risk of fetal scalp hematoma compared to vacuum extraction. However, its application is limited in certain fetal positions, such as occiput transverse or posterior, and improper use increases the risk of maternal soft tissue injury and neonatal facial trauma.15 Vacuum extraction is simpler to perform, can aid in fetal head rotation, and generally causes less maternal soft tissue damage but carries a higher risk of neonatal scalp injuries.16,17 Overall, vaginal instrumental delivery may be associated with neonatal complications such as skin lacerations, intracranial hemorrhage, and facial nerve palsy,18 although some long-term follow-up studies have not established a definitive link with adverse neurodevelopmental outcomes.24,25 In contrast, emergency cesarean section, while avoiding the mechanical trauma associated with passage through the birth canal, involves longer preoperative preparation, anesthesia administration, and surgical duration, which can prolong fetal hypoxia exposure. A deeply engaged fetal head poses a significant technical challenge during second-stage cesarean sections, with an incidence reaching up to 11% in emergency cases.26–28 This can lead to difficulties in fetal extraction, extension of the uterine incision, increased intraoperative hemorrhage, and neonatal injury. Although various techniques—such as reverse breech extraction or push-up maneuvers—are employed to manage impacted fetal heads, high-quality evidence supporting the superiority of any single method remains lacking.29–31
The results of this study indicate no significant differences in short-term neonatal outcomes among the three modes of delivery during PD in the second stage. This emphasizes the importance of individualized clinical decision-making. Obstetric teams should comprehensively evaluate fetal station, labor progress, fetal tolerance, maternal condition, and operator experience to select the most appropriate approach for rapid and safe delivery. The key is the accurate and timely identification of fetal heart rate abnormalities to enable swift, effective intervention, thereby maximizing maternal and neonatal safety.32
Analysis of Maternal Outcomes
The results of this study demonstrate that the cesarean section group experienced significantly longer postpartum hospital stays, higher hospitalization costs, prolonged durations of antibiotic administration and indwelling catheterization, and greater postpartum blood loss compared to both the vacuum extraction and forceps groups (all P < 0.05). These findings align with existing literature, which indicates that cesarean delivery during the second stage of labor is typically associated with a longer recovery period and increased utilization of medical resources.13,33 These differences are intrinsically linked to the specific characteristics of each delivery method. Cesarean section is an abdominal surgical procedure classified as a Class II incision, generally requiring a longer operative time, urinary catheterization, and carrying a higher risk of postoperative infection—hence the routine use of prophylactic antibiotics.34 Conversely, operative vaginal deliveries usually do not necessitate routine prophylactic antibiotics,35 which explains the longer course of antibiotic use observed in the cesarean group. Additionally, prolonged fetal head pressure during the second stage can cause edema and impair contractility of the lower uterine segment. When coupled with a low fetal station, these factors can increase the difficulty of fetal extraction and the likelihood of extension of the uterine incision during cesarean section, thus elevating the risk of hemorrhage.36,37 This correlates with the higher blood loss observed in the cesarean group. Regarding soft tissue injury, the incidence of wound redness was significantly higher in the forceps group compared to the cesarean group (P < 0.05). However, this result should be interpreted cautiously due to the relatively small sample size of the forceps group (n=30) and the absence of a significant difference between the vacuum extraction and cesarean groups. Nonetheless, forceps application can potentially exacerbate trauma to edematous and pressure-affected perineal tissues, increasing local inflammatory responses. Therefore, forceps-assisted delivery should be performed with gentle techniques to prevent excessive traction, and close postoperative monitoring of the perineal wound is essential, with appropriate anti-inflammatory or antibiotic treatment if needed.
From the maternal outcome perspective, this study confirms that each delivery method used during the second stage of labor carries a distinct risk profile. Cesarean section is associated with higher risks of hemorrhage, longer recovery times, and increased medical costs. While operative vaginal delivery can shorten the duration of labor, forceps assistance may elevate the risk of soft tissue trauma. These findings underscore the importance of comprehensive preoperative assessment during urgent decision-making, including evaluation of maternal baseline status, labor progression, fetal station, and potential complications, in order to select the most suitable individualized delivery strategy. Seamless teamwork, accurate risk assessment, and adherence to standardized operative techniques are key to optimizing maternal outcomes and enhancing the childbirth experience.
Limitations
This study has several limitations inherent to its retrospective design. The potential for selection bias and unmeasured confounding must be acknowledged, particularly regarding operator experience and preference, which significantly influenced the choice of delivery method but could not be analyzed. The small sample size, especially in the forceps and cesarean groups, limits the statistical power and generalizability of our findings. Future prospective studies are needed to validate these results.
Conclusion
In summary, during prolonged deceleration in the second stage of labor, the choice of delivery method presents a trade-off between maternal morbidity and procedural expediency. Our findings support a management strategy centered on rapid assessment: prioritizing operative vaginal delivery when fetal station is low and operator expertise is sufficient, and opting for cesarean section when conditions are unfavorable for vaginal birth. The consistent neonatal outcomes across all modes of delivery should reassure clinicians that, within this framework, the primary focus can be on selecting the safest and most efficient route to achieve delivery for the individual mother-baby dyad.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, KaiSun Zhao, upon reasonable request.
Ethics Approval and Consent to Participate
This study received approval from the Ethics Committee of the Second Nanning People’s Hospital [Y2025062]. Waiver of informed consent was granted.
Acknowledgments
We acknowledge the clinical support provided by the obstetric team at The Second Nanning People’s Hospital during data collection. The study received no external funding. All researchers maintained independence in study design, data analysis, and interpretation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There are no funding sources to be declared.
Disclosure
The authors report no conflicts of interest in this work.
References
1. GBD 2021 Fertility and Forecasting Collaborators. Global fertility in 204 countries and territories, 1950-2021, with forecasts to 2100: a comprehensive demographic analysis for the Global Burden of Disease Study 2021, Lancet. 2024;403(10440):2057–2099. PMID: 38521087 PMCID: PMC11122687. doi:10.1016/S0140-6736(24)00550-6
2. Chinese Maternal and Child Health Association. Perinatal Medicine Education Professional Committee of the Chinese Medical Education Association. Expert consensus on clinical practice of electronic fetal heart monitoring during prenatal and perinatal periods. Chin J Pract Gynecol Obstetrics. 2022;38(7):714–725. doi:10.19538/j.fk2022070111
3. Obstetrics Group of the Obstetrics and Gynecology Branch of the Chinese Medical Association, Perinatal Medicine Branch of the Chinese Medical Association. Guidelines for normal delivery. Chin J Perinatal Med. 2020;23(6):361–370. doi:10.3760/cma.j.cn113903-20200526-00493
4. Chandraharan E, Ghi T, Fieni S, Jia YJ. Optimizing the management of acute, prolonged decelerations and fetal bradycardia based on the understanding of fetal pathophysiology. Am J Obstet Gynecol. 2023;228(6):645–656. PMID: 37270260. doi:10.1016/j.ajog.2022.05.014
5. Morgan JA, Hankins ME, Wang Y, et al. Prolonged fetal heart rate decelerations in labor: can we reduce unplanned primary cesarean sections in this group? Adv Ther. 2020;37(10):4325–4335. PMID: 32839938. doi:10.1007/s12325-020-01468-x
6. Triebwasser JE, Colvin R, Macones GA, Cahill AG. Nonreassuring fetal status in the second stage of labor: fetal monitoring features and association with neonatal outcomes. Am J Perinatol. 2016;33(7):665–670. PMID: 26862724. doi:10.1055/s-0036-1571316
7. Leoni RS, Tomich MF, Meireles PT, Galvão Petrini C, Júnior EA, Peixoto AB. Accuracy of intrapartum cardiotocography in identifying acidemia at birth by umbilical cord blood gasometry in high-risk pregnancies. Rev Assoc Med Bras. 2023;69(11):e20230511. eCollection 2023. PMID: 37820165 PMCID: PMC10561908. doi:10.1590/1806-9282.20230511
8. CoP BO. ACOG practice bulletin No. 154: Operative vaginal delivery. Obstet Gynecol. 2015;126(5):e56–e65.
9. Dahan O, Zibenberg A, Goldberg A. Birthing consciousness and the flow experience during physiological childbirth. Midwifery. 2024;138:104151. PMID: 39173536. doi:10.1016/j.midw.2024.104151
10. Chinese Medical Association Perinatal Medicine Branch Neonatal Resuscitation Group. Expert consensus on the clinical application of umbilical artery blood gas analysis in neonates (2021). Chin J Perinatal Med. 2021;24(6):401–405. doi:10.3760/cma.j.cn113903-20210413-00346
11. Low JA, Lindsay BG, Derrick EJ. Threshold of metabolic acidosis associated with newborn complications. Am J Obstet Gynecol. 1997;177(6):1391–1394. PMID: 9423740. doi:10.1016/s0002-9378(97)70080-2
12. He M, Yan J, et al. The impact of prolonged deceleration during the second stage of labor on umbilical artery blood gas analysis. Int J Womens Health. In press 2026.
13. Watkins VY, O’Donnell CM, Perez M, et al. The impact of physical activity during pregnancy on labor and delivery. Am J Obstet Gynecol. 2021;225(4):437.e1–437.e8. PMID: 34081895; PMCID: PMC10564562. doi:10.1016/j.ajog.2021.05.036
14. Blanc J, Castel P, Mauviel F, et al. Prophylactic manual rotation of occiput posterior and transverse positions to decrease operative delivery: the PROPOP randomized clinical trial. Am J Obstet Gynecol. 2021;225(4):444.e1–444.e8. PMID: 34033811. doi:10.1016/j.ajog.2021.05.020
15. Feng J, Zhang X. Analysis of perinatal outcome of forceps delivery and risk factors of postpartum hemorrhage. Altern Ther Health Med. 2024;30(4):102–107. PMID: 38064601.
16. Murphy DJ, Strachan BK, Bahl R. Royal college of obstetricians and gynaecologists. assisted vaginal birth: Green-top guideline No. 26. BJOG. 2020;127(9):e70–e112. PMID: 32346983. doi:10.1111/1471-0528.16092
17. Thierens S, van Binsbergen A, Nolens B, van den Akker T, Bloemenkamp K, Rijken MJ. Vacuum extraction or caesarean section in the second stage of labour: a systematic review. BJOG. 2023;130(6):586–598. PMID:36660890. doi:10.1111/1471-0528.17394
18. Chinese Medical Association Obstetrics and Gynecology Branch Obstetrics Group. Guidelines for vaginal operative delivery (2016). Chin J Obstetrics Gynecol. 2016;51(8):565–567. doi:10.3760/cma.j.issn.0529-567x.2016.08.002
19. Froeliger A, Deneux-Tharaux C, Madar H, Bouchghoul H, Le Ray C, Sentilhes L; TRAAP study group. Closed- or open-glottis pushing for vaginal delivery: a planned secondary analysis of the TRAnexamic Acid for Preventing postpartum hemorrhage after vaginal delivery study. Am J Obstet Gynecol. 2024;230(3S):S879–S889.e4. PMID: 37633725. doi:10.1016/j.ajog.2023.07.017
20. Cahill AG, Macones GA. Optimizing the length of the second stage and management of pushing. Am J Obstet Gynecol. 2024;230(3S):S876–S878. PMID: 38462261. doi:10.1016/j.ajog.2022.07.017
21. Jia Y-J, Ghi T, Pereira S, Perez-Bonfils AG, Chandraharan E. Pathophysiological interpretation of fetal heart rate tracings in clinical practice. Am J Obstet Gynecol. 2023;228(6):622–644. PMID:37270259. doi:10.1016/j.ajog.2022.05.023
22. Paladugu V, Sreedhar S, Chitra R, Mannava ST, Sreekumar S, Mangalakanthi J. Association of CTG diagnosis of intrapartum fetal distress and immediate postpartum acidemia in foetal umbilical artery. J Obstet Gynaecol India. 2023;73(1):28–35. PMID: 36879941. doi:10.1007/s13224-022-01702-2
23. Uzianbaeva L, Yan Y, Joshi T, et al. Methods for monitoring risk of hypoxic damage in fetal and neonatal brains: a review. Fetal Diagn Ther. 2022;49(1–2):1–24. PMID: 34872080 PMCID: PMC8983560. doi:10.1159/000520987
24. Bahl R, Patel RR, Swingler R, Ellis M, Murphy DJ. Neurodevelopmental outcome at 5 years after operative delivery in the second stage of labor: a cohort study. Am J Obstet Gynecol. 2007;197(2):147.e1–6. PMID: 17689628. doi:10.1016/j.ajog.2007.03.034
25. Wesley BD, van den Berg BJ, Reece EA. The effect of forceps delivery on cognitive development. Am J Obstet Gynecol. 1993;169(5):1091–1095. PMID: 8238165. doi:10.1016/0002-9378(93)90261-g
26. Levy R, Chernomoretz T, Appelman Z, Levin D, Or Y, Hagay ZJ. Head pushing versus reverse breech extraction in cases of impacted fetal head during Cesarean section. Eur J Obstet Gynecol Reprod Biol. 2005;121(1):24–26. PMID: 15961214. doi:10.1016/j.ejogrb.2004.09.014
27. Wyn Jones N, Mitchell EJ, Wakefield N, et al. Impacted fetal head during second stage Caesarean birth: a prospective observational study. Eur J Obstet Gynecol Reprod Biol. 2022;272:77–81. PMID: 35290876. doi:10.1016/j.ejogrb.2022.03.004
28. Cornthwaite K, Draycott T, Bahl R, Hotton E, Winter C, Lenguerrand E. Impacted fetal head: a retrospective cohort study of emergency caesarean section. Eur J Obstet Gynecol Reprod Biol. 2021;261:85–91. PMID: 33901776. doi:10.1016/j.ejogrb.2021.04.021
29. Cornthwaite K, van der Scheer JW, Kelly S, et al. Management of impacted fetal head at cesarean birth: a systematic review and meta-analysis. Acta Obstet Gynecol Scand. 2024;103(9):1702–1713. PMID: 38787368; PMCID: PMC11324922. doi:10.1111/aogs.14873
30. Fong YF, Arulkumaran S. Breech extraction--an alternative method of delivering a deeply engaged head at cesarean section. Int J Gynaecol Obstet. 1997;56(2):183–184. PMID: 9061396. doi:10.1016/s0020-7292(96)02817-2
31. Bloch C, Dore S, Hobson S. Committee Opinion No. 415: impacted fetal head, second-stage cesarean delivery. J Obstet Gynaecol Can. 2021;43(3):406–413. PMID: 33640101. doi:10.1016/j.jogc.2021.01.005
32. Thayer SM, Faramarzi P, Krauss MJ, et al. Heterogeneity in management of category II fetal tracings: data from a multihospital healthcare system. Am J Obstet Gynecol MFM. 2023;5(7):101001. PMID: 37146688. doi:10.1016/j.ajogmf.2023.101001
33. McCoy JA, Kim YY, Nyman A, Levine LD. Prolonged labor and adverse cardiac outcomes in pregnant patients with congenital heart disease. Am J Obstet Gynecol. 2023;228(6):728.e1–728.e8. PMID: 36427597; PMCID: PMC10205915. doi:10.1016/j.ajog.2022.11.1292
34. Hamel MS, Tuuli M. Prevention of postoperative surgical site infection following cesarean delivery. Obstet Gynecol Clin North Am. 2023;50(2):327–338. PMID: 37149313. doi:10.1016/j.ogc.2023.02.012
35. Peaceman AM. Operative vaginal birth: ACOG practice bulletin, Number 219. Obstet Gynecol. 2020;135(4):e149–e159. PMID: 32217976. doi:10.1097/AOG.0000000000003764
36. Ashwal E, Bson RB, Aviram A, Hadar E, Yogev Y, Hiersch L. Risk factors for postpartum hemorrhage following cesarean delivery. J Matern Fetal Neonatal Med. 2022;35(18):3626–3630. PMID: 33508987. doi:10.1080/14767058.2020.1834533
37. Lauterbach R, David CB, Bachar G, et al. Higher risk of hemorrhage and maternal morbidity in vaginal birth after second stage of labor C-section. Arch Gynecol Obstet. 2022;305(6):1431–1438. PMID: 34546434. doi:10.1007/s00404-021-06254-w
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prolonged Second Stage of Labor in Thai Women: A Retrospective Cohort Study
Panichayatham P, Pongsatha S, Kamlungkuea T, Luewan S, Tongsong T
International Journal of Women's Health 2026, 18:561682
Published Date: 6 January 2026
The Impact of Prolonged Deceleration During the Second Stage of Labor on Umbilical Artery Blood Gas Analysis
He MR, He MP, Yan J, Yuan CL, Jian WQ, Huang JC, Huang HF, Zhao KS
International Journal of Women's Health 2026, 18:542850
Published Date: 13 April 2026