Back to Journals » Journal of Healthcare Leadership » Volume 18
Impact of Diagnosis-Intervention Packet (DIP) Payment Reform on County Hospitals: Evidence from Z City, China
Received 27 July 2025
Accepted for publication 30 January 2026
Published 13 February 2026 Volume 2026:18 556559
DOI https://doi.org/10.2147/JHL.S556559
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Russell Taichman
Xinyi Peng,1 Huawei Tan,1,* Yingchun Chen1,2,*
1Department of Health Management, School of Medicine and Health Management, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 2Research Centre for Rural Health Service, Key Research Institute of Humanities and Social Sciences of Hubei Provincial Department of Education, Wuhan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yingchun Chen, Email [email protected] Huawei Tan, Email [email protected]
Background: In 2020, China introduced an innovative case-based payment method called “Diagnosis-Intervention Packet (DIP).” However, the implementation of DIP may present significant challenges to county hospitals. Therefore, this study aims to assess the impact of DIP on inpatient Volume and inpatient medical revenue at county hospitals, as well as its effect on patient flow.
Methods: We collected detailed data on inpatient expenses and reimbursements from the Z City Medical Insurance Bureau for the years 2020– 2022, encompassing a total of 5,339,996 records. A single-group interrupted time series analysis was conducted to examine changes in inpatient volumes and their regional distribution across municipal hospitals, county hospitals, and primary healthcare institutions before and after the DIP reform. Additionally, the impact of the reform on medical revenue at county hospitals and its regional share was analyzed. Heterogeneity by insurance type was also explored.
Results: Following the implementation of the DIP reform, county hospitals experienced significant declines in both inpatient volume and inpatient medical revenue growth. Monthly inpatient visits decreased by 610.4 (p=0.063), with their market share dropping 0.28% (p=0.003). The impact was particularly pronounced for patients with Urban-Rural Residents Basic Medical Insurance (URRBMI), where monthly volume fell by 1,228.13 (p=0.012) and share decreased by 0.39% (p< 0.001). Inpatient medical revenue growth reversed significantly, with the slope decreasing 3.58% (p=0.014) and regional share falling 0.38% (p=0.008).
Conclusion: DIP implementation creates significant challenges for county hospitals through patient diversion to primary facilities and increased competition with municipal hospitals. This threatens to create a cycle of declining volume, revenue, and capabilities. To prevent rural patients from being forced to seek care at distant urban facilities, policy interventions should focus on providing targeted support to maintain county hospitals’ vital role in rural healthcare delivery.
Keywords: DIP, case-based payment system, county hospitals, inpatient volume, medical revenue
Introduction
The rapid escalation of healthcare costs is a shared challenge faced by countries worldwide.1,2 Reforming healthcare payment systems has become a critical strategy to mitigate escalating expenses and improve service efficiency. Many countries have explored and implemented various healthcare payment reforms.3 For example, the United States has adopted performance-based payment, bundled payments, and Diagnosis-Related Group (DRG) payments.4 Germany has introduced several payment schemes under a global budget, such as payments based on average length of stay, DRGs, and certain project-specific reimbursements.5 Japan has combined project-based payments with the Diagnosis Procedure Combination (DPC) system.6
However, existing research highlights that while these innovative payment systems aim to regulate the supply of healthcare services through economic incentives to achieve policy goals, their effects on healthcare systems are multifaceted.7,8 For instance, Taiwan’s global budget system, while controlling medical costs to some degree, has exacerbated the concentration of patients in larger medical institutions, disrupting market balance.9 Similarly, in Germany, the implementation of regional budgets for outpatient care—where health insurance funds are allocated based on service volume shares—has intensified competition and incentivized providers to increase service quantity.10 This phenomenon underscores the potential trade-offs between cost control and the equitable distribution of healthcare resources under such payment reforms.
Healthcare expenditures in China have surged rapidly from 2010 to 2023. According to the Statistical Bulletin on the Development of Health and Wellness in China, total healthcare spending increased from 1.98 trillion RMB to 9.06 trillion RMB, while per capita healthcare expenses grew from 1,490 RMB to 6,425 RMB. This increase in healthcare costs has outpaced the global average.11 This has been accompanied by the overuse and inefficient allocation of medical resources.12 To control escalating costs, prevent over-medicalization, and enhance the quality and efficiency of healthcare services, China launched the DIP (Diagnosis-Initiated Payment) payment reform in 2020. The reform was rolled out as a national pilot in 71 cities. Similar to the payment systems in Taiwan and Germany, the DIP payment employs a global budget approach. The DIP is an innovative hybrid that combines a regional global budget with a case-based payment mechanism. The system’s foundation is the global budget, which functions as a strict price control measure by setting a mandatory annual expenditure cap for the entire regional inpatient healthcare system. To distribute this budget, DIP utilizes historical case data to categorize diseases and interventions into standardized packets, known as DIP groups. Payment for these services is structured around Points and Point Value (PV). Points are assigned based on a case’s historical cost relative to the regional average. Crucially, the PV is dynamically generated based on the ratio of the region’s current budget to the total accumulated points across all cases. This mechanism ensures that total expenditure is strictly constrained by the annual budget ceiling. However, this structure introduces a risk of competition among healthcare providers to increase inpatient service volume, thereby attempting to capture a larger portion of the available healthcare budget.
The healthcare delivery system in rural China consists of village clinics, township health centers (THCs), and county hospitals. Positioned between urban tertiary hospitals and rural primary healthcare facilities, county hospitals serve over 900 million residents, accounting for more than 70% of the total population of China.13 These hospitals are critical for rural residents to access basic medical services, ensuring healthcare equity by facilitating geographic and service accessibility. They primarily offer diagnosis and treatment for common and frequently occurring diseases, emergency services, as well as disease prevention and health promotion. By offering accessible medical services close to home, county hospitals help reduce the costs and time associated with traveling to other regions for care, easing the financial burden on patients and promoting healthcare equity.
For rural residents, particularly those in remote areas, county hospitals are indispensable in promoting equitable access to healthcare resources. Moreover, compared to urban tertiary hospitals, county hospitals are characterized by lower medical costs and higher reimbursement rates under health insurance systems,14 which alleviates the economic burden of disease. In terms of the overall healthcare system, county hospitals are a critical component in optimizing the tiered healthcare delivery system. They manage minor and less severe cases, while referring complex and severe cases to higher-level hospitals. This dual function helps alleviate the pressure on urban tertiary hospitals, thereby preventing the overcrowding of these facilities with both serious and routine cases.15
Due to China’s urban-rural dual structure, there is a significant disparity in both the quantity and quality of healthcare resources between urban and rural areas, with high-quality medical resources concentrated in major cities.16,17 Patients possess substantial autonomy in healthcare decision-making, patients often bypass them in favor of urban tertiary hospitals. The healthcare supply in China exhibits a distinct “inverted pyramid” structure, with a total of 245 million hospital admissions in 2023, of which 148.34 million (60.55%) occurred in tertiary hospitals.18,19 In this context, where large municipal medical institutions already experience a significant siphoning effect, the implementation of the DIP payment reform may exacerbate competition among healthcare providers, further intensifying the survival pressures on county hospitals. This could lead to patient and financial resource losses at the county level, limiting or even reversing the development of healthcare services in rural areas and hindering the advancement of rural healthcare systems. As a result, the geographical and economic accessibility of healthcare for rural residents would be diminished, forcing them to seek care at higher-level hospitals, thereby increasing both direct and indirect medical costs. Furthermore, the relatively low reimbursement rates for municipal hospitals would further aggravate the economic burden on patients, undermining healthcare equity for rural populations.
The DIP payment reform, which applies separate global budgets for inpatient care under different types of medical insurance, may result in differentiated impacts. China’s current basic health insurance system is divided into two types: the Urban Employee Basic Medical Insurance (UEBMI) and the Urban-Rural Resident Basic Medical Insurance (URRBMI). The UEBMI primarily covers employed individuals, including both formally employed workers and those in flexible employment, while the URRBMI mainly serves unemployed individuals, farmers, and even those living in poverty. Due to lower funding levels, the URRBMI has a more limited pool of available health insurance funds.20 Under the DIP payment reform, the two types of insurance are budgeted separately according to their respective funding levels, rather than being pooled together. As a result, patients with the same condition under different insurance schemes face varying payment standards. One study has indicated that the DIP reform leads to different changes in per capita inpatient costs and average length of hospital stay for the two insurance groups, with the payment standards under the URRBMI generally lower than those under the UEBMI.21 Given these differential reimbursement standards, healthcare providers may have incentives and opportunities to adopt strategic responses to payment changes. Hospitals may seek to minimize financial losses by reducing the admission of patients covered under the lower-reimbursement URRBMI scheme. Since approximately 90% of patients treated at county hospitals are URRBMI beneficiaries, the lower reimbursement rates may adversely affect equitable access to care for these patients, raising concerns about healthcare fairness.
Existing studies on the DIP payment reform primarily focus on changes in medical expenses,22–24 healthcare efficiency,25,26 and service quality.27 The findings generally suggest that the DIP reform effectively curbs healthcare costs and reduces patients’ out-of-pocket expenses. Some research also indicates that DIP can improve the quality of healthcare services. Additionally, a few studies have explored the reform’s role in fostering an orderly healthcare delivery system.25,28 However, limited attention has been paid to the institutional impacts—particularly the implications for county hospitals, which are essential to rural health systems.
This study aims to analysis institutional impacts by focusing on Z City1 (“Z City”is used as a pseudonym in accordance with the data-sharing agreement signed with the Z city’ health insurance bureau), a national DIP pilot site. Using an interrupted time series analysis (ITSA), we examine trends in inpatient discharges across municipal hospitals, county hospitals, and primary care institutions, as well as the inpatient revenue of county hospitals. The aim is to assess the impact of DIP reform on service volume, inpatient revenue, and patient flow in county hospitals. We seek to address three key questions: First, did the reform affect inpatient volume and revenue at county hospitals? Does the reform bring challenges to county hospitals? Second, did municipal hospitals absorb patients who would have otherwise sought care at county hospitals, thereby exacerbating the marginalization of county hospitals and intensifying urban-rural healthcare resource disparities? Third, did healthcare institutions adopt different strategic behaviors based on the type of medical insurance coverage? By answering these questions, this study aims to provide new insights into the institutional impacts of the DIP reform, particularly its implications for county hospitals—the cornerstone of rural health systems. Unlike previous studies that have primarily focused on aggregate outcomes such as healthcare costs and efficiency, this research offers a detailed examination of patient redistribution and revenue trajectories, which are essential to understanding the reform’s heterogeneous effects across healthcare tiers.
Materials and Methods
Study Setting
Z City is situated in southwestern China. According to the 2024 Z City Bulletin on National Economic and Social Development, its GDP reached 502.72 billion RMB, making it the second-largest economy in the province in 2024. According to the 2023 Z City Statistical Bulletin on the Development of Medical Security, the total revenue of the city’s UEBMI fund was 475.69 million RMB, with expenditures totaling 412.93 million RMB; the revenue for the URRBMI fund was 659.72 million RMB, with expenditures amounting to 714.63 million RMB. Z City administratively encompasses three districts, seven counties, two autonomous counties, and two directly governed cities. The city is served by 716 healthcare facilities, which include 181 municipal hospitals, 149 county hospitals, and 386 township hospitals and community health service centers.
In November 2020, Z City was designated as one of the first pilot cities for the DIP reform. The reform was officially launched on January 1, 2022. DIP is an innovative payment approach that integrates global budgeting with case-based payments. The global budget is allocated to the regional inpatient healthcare system, setting an annual budget ceiling. Z City has established two distinct regional budgets: one for UEBMI and another for URRBMI. Based on data from the past three years of inpatient case records, treatment methods such as conservative treatment, diagnostic procedures, therapeutic operations, and relevant surgeries were clustered to form distinct DIP groups. Z City has developed a total of 4,281 DIP groups. Similar with the DRG payment, the DIP payment scheme develops a point schedule to reflect the relative resource utilization. Each DIP group is assigned a certain amount of points.22 The payment for each case is calculated by multiplying the point volume with the corresponding point value (PV). Unlike the fixed point value in the DRG model, the PV in the DIP reform fluctuates, and the final payment amount is only determined at the end of the year. As indicated in Formula (1), the PV is the ratio of the pre-determined regional budget to the total points for all inpatient cases within the region. Therefore, the reimbursement amount received by each medical institution is influenced not only by the total point volume of the DIP groups it handles but also by the total point volume processed by other institutions within the same region.

Additionally, adjustment coefficients are established to account for variables such as the healthcare institution’s service management capacity, the level of medical care provided, the complexity of cases involving insured patients, and the resources consumed. These adjustment coefficients are divided into two main categories: institutional grade coefficients and additive coefficients. The final score is adjusted based on both the institutional grade coefficient and the additive coefficient. The institutional grade coefficient is determined by the classification of the medical institution into one of four levels—provincial, municipal, county, or township—with the coefficient decreasing as the institution’s level decreases. Hence, for the same condition, higher-level institutions receive higher reimbursement amounts. To encourage medical institutions to reasonably treat special populations, additional weight is given to cases involving individuals aged 70 and above, children aged six and under, low-birth-weight infants, and infectious disease cases, through the application of an additive coefficient. Therefore, the actual reimbursement amount for each medical institution is determined, as shown in Formula (2).

To promote the establishment of an orderly healthcare system and facilitate the redirection of common and frequently occurring diseases to primary healthcare institutions, the Medical Security Bureau of City Z has designated a subset of core disease categories as the primary DIP group. The selection criteria for these categories include relatively low technical complexity, historically high patient visit rates at primary healthcare institutions, and suitability for diagnosis and treatment at designated primary healthcare facilities. After expert demonstration, a total of 37 disease groups has been incorporated into the primary DIP group. The adjustment coefficient for primary disease groups is set at 1, ensuring that the reimbursement price for the same disease remains consistent across all medical institutions.
Study Design and Data Sources
This study adopts a retrospective comparative research design. The dataset was obtained from the Z City Healthcare Security Bureau, encompassing inpatient expenditure details and reimbursement records from January 1, 2020, to December 31, 2022, with an initial sample of 5,339,996 records. The dataset includes key variables such as patient demographics, diagnostic information, healthcare institution details, hospital classification, insurance type, total medical expenses, and reimbursement amounts covered by the healthcare fund. To enhance the accuracy and reliability of the findings, rigorous inclusion and exclusion criteria were applied. First, 300,082 records of out-of-city hospitalizations were excluded. Second, 104 records with incomplete data were removed. Lastly, to precisely evaluate the impact of the disease-based payment (DIP) policy, cases not settled under the DIP system—including COVID-19 cases, psychiatric cases, and rehabilitation cases—were further excluded. Following data cleansing, the final analytical sample comprised 4,686,571 inpatient reimbursement records, including 649,664 records under the UEBMI and 4,036,907 records under the URRBMI.
To assess the impact of the DIP reform on county hospitals, medical institutions were classified into three categories based on facility type and regional location: municipal hospitals, county hospitals, and primary healthcare institutions. The study analyzed inpatient service volumes and hospitalization revenues for each category and conducted a comparative assessment of changes in service volume and its proportion within the region before and after the DIP reform. Additionally, the study examined variations in county hospital revenues and their regional share. To explore potential differential effects of the reform, we performed a subgroup analysis based on insurance type (UEBMI and URRBMI). Specifically, we ran the standard ITSA model independently for each insurance type’s dataset. The analysis was designed to evaluate the differential impacts of the reform on inpatient volumes and medical revenue based on the varying reimbursement levels associated with each insurance type.
Statistical Analysis
This study first performed descriptive analyses using Excel 2019, employing frequency counts and percentages to summarize inpatient discharge volumes and hospitalization revenues across different types of medical institutions.
To evaluate the impact of the DIP reform on county-level hospitals, a single-group Interrupted Time Series Analysis (ITSA)—a robust quasi-experimental method—was utilized.29 The ITSA was conducted to examine changes in inpatient discharge volumes and their regional proportions across different medical institutions, as well as hospitalization revenues and their regional shares for county-level hospitals. To ensure a normal distribution, hospitalization revenue data were log-transformed prior to analysis. The DIP reform was officially implemented on January 1, 2022. Therefore, the policy intervention point was set at January 2022. The study analyzes its effects by comparing pre-reform data (January 2020 to December 2021) with post-reform data (January 2022 to December 2022). Given the potential impact of the COVID-19 pandemic from 2020 to 2022, data anomalies were anticipated. To address this, pandemic control reports from City Z during this period were analyzed to assess the occurrence of sporadic and large-scale outbreaks. The findings indicated that overall pandemic control in City Z was relatively effective, with predominantly sporadic cases (see Appendix 1 for details). However, a large-scale outbreak occurred around November 26, 2022, suggesting potential data distortions in December 2022. To enhance data accuracy, a multiple imputation method was applied to adjust and replace the December 2022 data.
Additionally, to account for periodic fluctuations in the data, such as seasonal variations, this study applied Fourier transformation by converting the time variable into angular values. This method facilitated the identification and modeling of cyclical patterns within the time series, thereby enhancing the accuracy of trend analysis for the outcome variables. First, the time variable (measured in months) was transformed into an angular value by dividing by 12 to obtain the year fraction and then multiplying by 360 to derive the corresponding angle. This transformation aimed to capture seasonal and other periodic variations within the time series.30 Subsequently, Fourier transformation was applied to the converted angular data, generating first- and second-order cosine and sine terms. These Fourier components represented underlying cyclical patterns in the data and enabled the identification of potential periodic fluctuations within the time series. To enhance the precision of trend analysis before and after the implementation of the DIP payment reform, these Fourier terms were incorporated as control variables in the ITSA model to control for seasonality. The regression model was specified as follows:

In this model, Y represents the observed outcome variable, while β0 denotes the baseline level of the outcome measure. β1 captures the pre-intervention trend, β2 reflects the immediate level change at the time of intervention, and β3 represents the change in trend following the intervention, with  indicating the post-intervention trend.31 The variable Time is a continuous variable ranging from 1 to 36. Intervention is a binary variable, coded as 0 before policy implementation and 1 after implementation. Time after intervention is also a continuous variable, assigned a value of 0 before the intervention and ranging from 25 to 36 after the intervention. The error term is represented by ε. The analysis was conducted using Stata 17.0 statistical software.
indicating the post-intervention trend.31 The variable Time is a continuous variable ranging from 1 to 36. Intervention is a binary variable, coded as 0 before policy implementation and 1 after implementation. Time after intervention is also a continuous variable, assigned a value of 0 before the intervention and ranging from 25 to 36 after the intervention. The error term is represented by ε. The analysis was conducted using Stata 17.0 statistical software.
Robustness Checks
To ensure the reliability and robustness of the study findings while minimizing potential biases caused by confounding factors such as regional development disparities and variations in healthcare infrastructure, this study selected three counties in City Z representing high, middle, and low levels of economic development. The proportion of county-level hospital discharges in each of the three counties relative to the overall total in City Z was analyzed, followed by separate ITSA for each county. This approach aimed to assess whether the impact of the DIP reform on county-level hospitals remained consistent across regions with different levels of economic development.
Results
Descriptive Statistics
Table 1 provides a detailed comparison of inpatient volume and inpatient medical revenue across municipal hospitals, county hospitals, and primary medical institutions from 2020 to 2022. The data include both the absolute number of inpatient volume and their respective proportion within the total figures.
 |
Table 1 Basic Description |
In terms of inpatient volume, inpatient visits have shown a steady increase from 2020 to 2022. Municipal hospitals accounted for the largest proportion of inpatient visits across all three years, with a slight decline in share from 40.13% in 2021 to 39.20% in 2022, despite an overall increase in the absolute number of visits (from 642,323 in 2021 to 658,768 in 2022). County hospitals followed, with a consistent share of approximately 35%, though their absolute inpatient visits also showed an increase (from 572,120 in 2021 to 585,614 in 2022). Primary medical institutions demonstrated the smallest share of inpatient visits, but their contribution increased proportionally from 24.12% in 2021 to 25.96% in 2022, with a notable rise in absolute numbers (from 386,097 in 2021 to 436,251 in 2022).
In terms of inpatient medical revenue, municipal hospitals generated the highest revenue, rising from 4,199,85.97 ten thousand CNY in 2020 to 4,559,40.51 ten thousand CNY in 2022. However, their share of citywide inpatient revenue decreased from 65.52% to 62.49%. County hospitals saw a steady increase in revenue, from 1,773,63.60 ten thousand CNY in 2020 to 2,210,40.57 ten thousand CNY in 2022, with their proportion rising from 27.67% to 30.30%. Primary medical institutions recorded the lowest revenue, growing from 436,60.68 ten thousand CNY in 2020 to 526,12.29 ten thousand CNY in 2022, with their share increasing from 6.81% to 7.21%.
ITSA Results for Inpatient Volumes Across Healthcare Institution Levels
Figure 1 and Table 2 present the ITSA results for inpatient discharge volumes across different types of healthcare institutions and patient categories before and after the DIP reform. Prior to the reform, both municipal (β1 = 460.53, P = 0.034) and county hospitals (β1 = 435.15, P = 0.032) showed a significant increasing trend in inpatient volumes. After the implementation of the DIP reform, the instantaneous changes in inpatient discharge volumes at all levels of healthcare institutions were not statistically significant (P>0.05). However, county hospitals suggested a notable downward trend post-reform, with inpatient volumes declining by approximately 1,045.66 discharges per month after the reform (β3=−1045.55, P=0.063). It represents a substantial monthly reduction and indicating that the reform likely altered patient distribution patterns within the local health system.
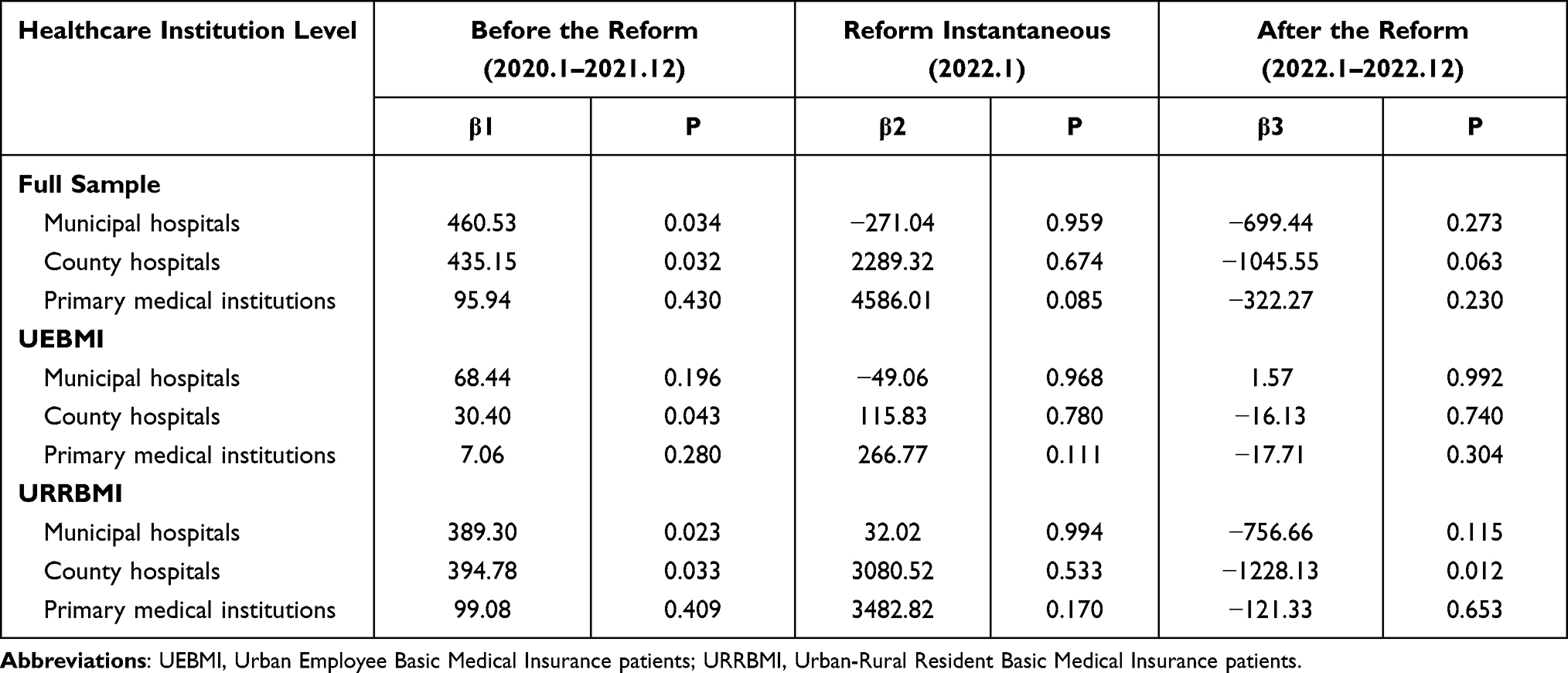 |
Table 2 ITSA Results for Inpatient Volumes Across Healthcare Institution Levels |
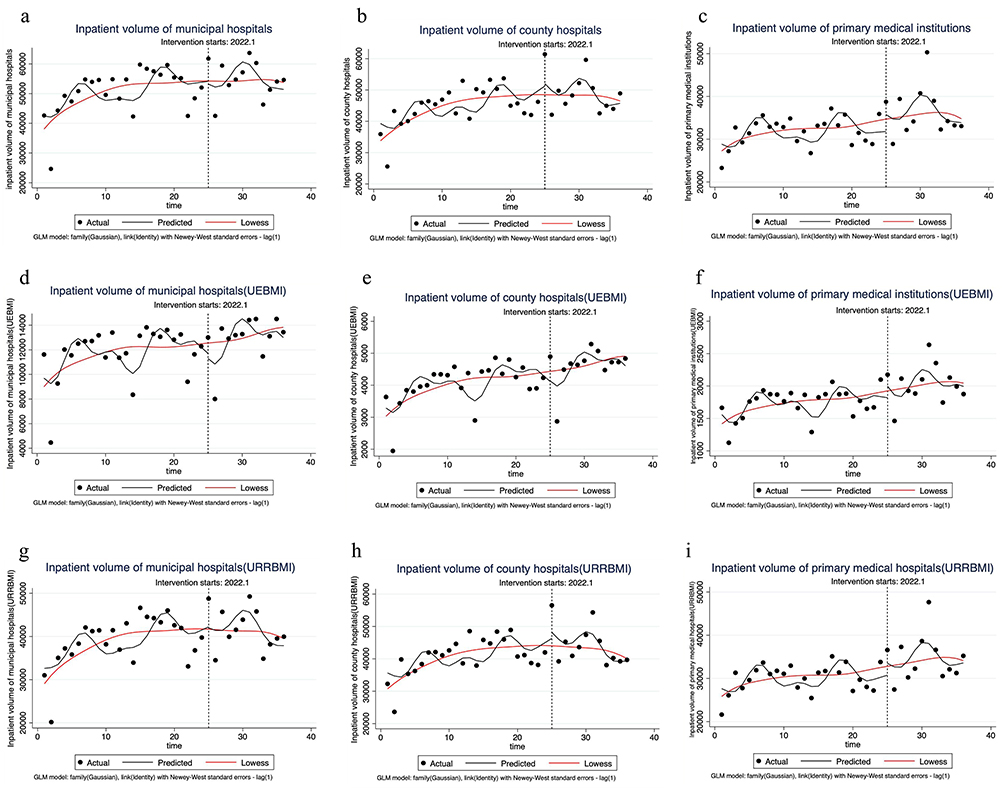 |
Figure 1 ITSA Results for Inpatient Volumes across Healthcare Institution Levels. (a) Trends in inpatient volumes at municipal hospitals. (b) Trends in inpatient volumes at county hospitals. (c) Trends in inpatient volumes at primary healthcare institutions. (d) Trends in inpatient volumes of Urban Employee Basic Medical Insurance (UEBMI) patients at municipal hospitals. (e) Trends in inpatient volumes of UEBMI patients at county hospitals. (f) Trends in inpatient volumes of UEBMI patients at primary healthcare institutions. (g) Trends in inpatient volumes of Urban and Rural Resident Basic Medical Insurance (URRBMI) patients at municipal hospitals. (h) Trends in inpatient volumes of URRBMI patients at county hospitals. (i) Trends in inpatient volumes of URRBMI patients at primary healthcare institutions. |
Regarding the UEBMI, before the reform, county hospitals exhibited a modest pre-reform increase (β1 = 30.40, P = 0.043), while municipal hospitals and primary institutions remained stable After the reform, the instantaneous changes and trend shift across all healthcare institutions were not significant (P>0.05). This pattern suggests that the DIP reform did not meaningfully redirect UEBMI patients in the short term, and their care-seeking behavior remained largely unchanged.
For inpatient volumes under the URRBMI, municipal (β1 = 389.30, P = 0.023) and county hospitals (β1 = 394.78, P = 0.033) both experienced steadily rising inpatient volumes before the reform. Post-reform, county hospitals showed a clear and sizable downward trend, with an average monthly reduction of 1,228 inpatient visits (β3=−1028.12, P=0.012).The pattern of change was consistent with the overall trend.
ITSA Results for the Proportion of Inpatient Volumes Across Healthcare Institution Levels
Figure 2 and Table 3 present the ITSA results for the proportion of inpatient volumes at different healthcare institutions and among various patient types before and after the DIP reform. Prior to the reform, county hospitals and primary healthcare institutions showed an increasing trend in their share of inpatient volume within the city (P<0.05). After the reform, no significant instantaneous changes were observed in the trends for any healthcare institution level (P>0.1). For county hospitals, the post-reform slope decreased by 0.28 percentage points per month compared with the pre-reform trend (β3 = −0.0027651, P=0.003). Although numerically small, this consistent downward shift indicates a gradual erosion of county hospitals’ market share and suggests that the reform may have influenced patient redistribution over time. No significant changes were found in municipal hospitals or primary healthcare institutions. Regarding the UEBMI, no significant changes were observed before or after the reform (P>0.01). Regarding the URRBMI, prior to the reform, the proportion of inpatient discharges from primary healthcare institutions suggested a slight decreasing trend in the city’s total share (β1 = −0.0014881, P=0.067), while no significant trends were observed in municipal or county hospitals. After the reform, the slope for county hospitals decreased by 0.39 percentage points per month compared to before the reform (β3 = −0.0039171, P=0.000). In contrast, primary healthcare institutions experienced a 0.45 percentage-point increase in monthly slope (β3 = −0.0044984, P=0.014). These opposite movements suggest a meaningful shift of URRBMI patients toward primary care settings following the reform.
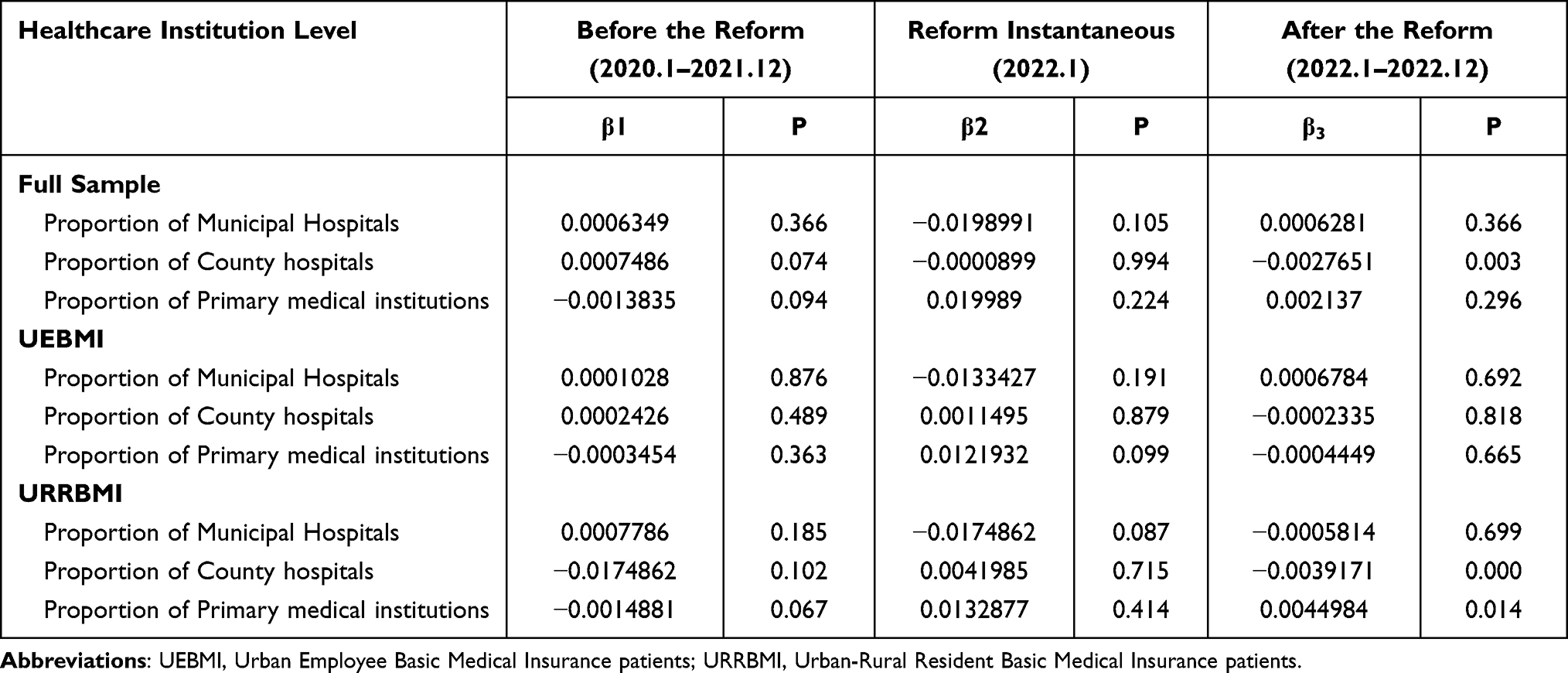 |
Table 3 ITSA Results for the Proportion of Inpatient Volumes Across Healthcare Institution Levels |
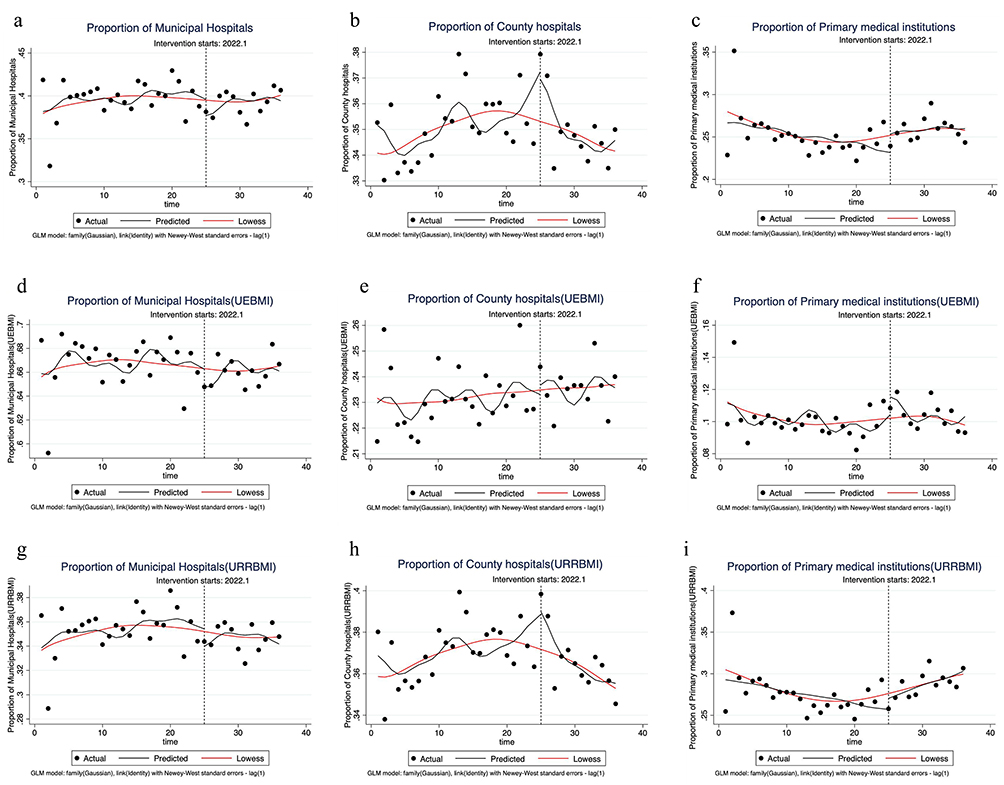 |
Figure 2 ITSA Results for the Proportion of Inpatient Volumes across Healthcare Institution Levels. (a) Trends in the proportion of inpatient discharges at municipal hospitals relative to total inpatient discharges citywide. (b) Trends in the proportion of inpatient discharges at county hospitals relative to total inpatient discharges citywide. (c) Trends in the proportion of inpatient discharges at primary healthcare institutions relative to total inpatient discharges citywide. (d) Trends in the proportion of inpatient discharges of Urban Employee Basic Medical Insurance (UEBMI) patients at municipal hospitals relative to all UEBMI inpatient discharges citywide. (e) Trends in the proportion of inpatient discharges of UEBMI patients at county hospitals relative to all UEBMI inpatient discharges citywide. (f) Trends in the proportion of inpatient discharges of UEBMI patients at primary healthcare institutions relative to all UEBMI inpatient discharges citywide. (g) Trends in the proportion of inpatient discharges of Urban and Rural Resident Basic Medical Insurance (URRBMI) patients at municipal hospitals relative to all URRBMI inpatient discharges citywide. (h) Trends in the proportion of inpatient discharges of URRBMI patients at county hospitals relative to all URRBMI inpatient discharges citywide. (i) Trends in the proportion of inpatient discharges of URRBMI patients at primary healthcare institutions relative to all URRBMI inpatient discharges citywide. |
ITSA Results for Inpatient Medical Revenue and Its Proportion at County Hospitals
Figure 3 and Table 4 present the ITSA results on inpatient medical revenue at county hospitals before and after the implementation of DIP, as well as its proportion in the total municipal inpatient medical revenue. Prior to the reform, the total inpatient medical revenue at county hospitals exhibited an upward trend, with a monthly growth rate of 1.62% (β1 = −0.0162225, P=0.007). Following the implementation of the reform, the slope decreased by 3.58% compared to the pre-reform period (β3 = −0.035775, P=0.014) The reversal from steady revenue growth to a sustained monthly decline suggests a substantial shift in county hospitals’ financial trajectory. Similarly, the proportion of county hospitals’ inpatient medical revenue in the total municipal inpatient revenue showed an increasing trend before the reform, with a monthly growth rate of 0.13% (β1 = −0.0012696, P=0.001). However, after the reform, this growth rate declined by 0.38% (β3 = −0.003844, P=0.008). Although the percentage point change appears modest, the consistent downward slope indicates a gradual loss of revenue share for county hospitals.
 |
Table 4 ITSA Results for Inpatient Medical Revenue and Its Proportion at County Hospitals |
 |
Figure 3 ITSA Results for Inpatient Medical Revenue and Its Proportion at County Hospitals. (a) Trends in inpatient medical revenue at county hospitals. (b) Trends in the proportion of inpatient medical revenue at county hospitals relative to total inpatient medical revenue citywide. |
Robustness Checks
Appendix 2 presents the changes in the proportion of inpatient discharges from county hospitals across three counties with varying levels of economic development in Z City, ensuring the reliability of the study findings. The results indicate that in Counties A and B, which exhibit higher and moderate levels of economic development, respectively, the proportion of inpatient discharges from county hospitals declined significantly following the implementation of the DIP reform. In contrast, County C, characterized by a relatively lower level of economic development, had already exhibited a marked downward trend in the proportion of inpatient volumes prior to the reform, with no significant changes observed post-reform. These results suggest that the DIP reform exerted a certain degree of influence on county hospitals, with varying impacts depending on the economic development level of the region.
Discussion
This study examines the impact of the DIP reform on inpatient volumes across different tiers of healthcare institutions within the city and on inpatient medical revenue at county hospitals. The findings indicate that prior to the reform, both the absolute number and proportion of inpatient volumes at county hospitals exhibited an increasing trend, which reversed to a declining trend post-reform. In contrast, municipal hospitals maintained a consistent upward trend in inpatient volumes both before and after the reform. Primary healthcare institutions showed no significant change in absolute inpatient numbers, but their share of total volumes, which was declining pre-reform, stabilized afterward.
Heterogeneity analysis based on health insurance type revealed significant differences. Specifically, among UEBMI beneficiaries, the number and proportion of inpatient volumes across different healthcare tiers did not exhibit significant changes post-reform. Among URRBMI beneficiaries, the trend aligned with the overall pattern: municipal hospitals’ upward trend persisted, county hospitals shifted from growth to decline in both volume and share, and primary institutions saw their declining share reverse to an increase post-reform. Given the substantial impact of inpatient service volume on hospital revenue, we further analyzed changes in inpatient medical revenue at county hospitals. The results indicate that both inpatient medical revenue and its proportion of total citywide inpatient revenue showed an increasing trend before the reform but declined after DIP implementation.
The post-reform decline in county hospital volumes alongside sustained growth at municipal hospitals suggests a continued centralization of inpatient care toward higher-tier institutions. This patterns, observed in other pilot regions,24,32 highlights a pronounced “siphoning effect” under DIP—whereby major hospitals leverage their superior resources, brand recognition, and service capacity to attract patients, including those with conditions that could be managed at lower-level facilities. Under the DIP payment mechanism, a hospital’s reimbursement from the medical insurance fund is determined by its total case-mix points and the point value. Since the point value remains consistent across all medical institutions, differences in reimbursement primarily depend on the total case-mix points. Hospitals can increase their total points through two main strategies: (1) expanding the provision of high-value medical conditions and (2) increasing the overall volume of services. The competition for case-mix points under the DIP payment rules intensifies service volume competition among healthcare institutions. Municipal hospitals, with their stronger medical service capabilities, hold a competitive advantage over county and primary healthcare institutions. This advantage is further reinforced by the large-scale expansion of tertiary hospitals and the construction of new hospital campuses.33 Given that many tertiary hospitals still have unused inpatient capacity, they remain incentivized to admit more patients. Similar centralization effects have been documented under analogous floating point value payment system in Taiwan and Germany. Evidence from Taiwan indicates that large medical institutions have a greater capacity to attract patients and expand service volumes.9 Markus Worz’s study on Germany also found that physicians shortened consultation times to increase service volume. Additionally, hospitals strategically arranged patient transfers or required patients to be discharged and readmitted in order to maximize their share of the medical insurance fund distribution.34 These systems are all founded on case-mix classification, operate under global budget caps, and utilize a floating-point value.
As the leading healthcare providers within county-level healthcare systems, county hospitals play a critical role in meeting the medical needs of local residents. However, the intensified siphoning effect of municipal hospitals under the DIP payment may exacerbate the survival challenges faced by county hospitals, further constraining the development of county-level healthcare systems. As the inpatient volume at county hospitals declines, their total medical revenue also inevitably decreases. The total inpatient medical revenue at county hospitals showed an upward trend before the reform, but after the reform, the slope of this trend decreased. Similarly, the share of county hospitals’ inpatient medical revenue in the city’s total medical revenue was increasing before the reform, but after the reform, the slope of this trend decreased. Since the DIP payment system is based on the point volume and PV, with PV being relatively consistent across institutions, competition for the point volume is inevitable. Inpatient volume is directly related to the point volume and is the most immediate influencing factor. Given that medical service income constitutes the largest share of hospital revenue,35,36 a sustained reduction can strain financial sustainability, potentially leading to long-term operational difficulties and undermining the development of robust county-level systems. This shift in patient flow also carries significant equity implications. It weakens geographic accessibility, forcing county residents to seek care at distant, higher-level hospitals. Consequently, both direct and indirect medical expenditures for patients increase. Lower reimbursement ratios at these hospitals further exacerbate the financial burden on patients, particularly URRBMI enrollees, threatening healthcare equity and exacerbating the urban-rural divide.
Heterogeneity analysis reveals significant differences in the distribution of inpatient visits between UEBMI and URRBMI beneficiaries across different hospital tiers. Notably, for UEBMI patients, the number and proportion of inpatient volumes across different levels of healthcare institutions did not exhibit significant changes following the reform. However, the distribution of URRBMI patients demonstrated a significant shift post-reform. Specifically, inpatient volumes at municipal hospitals exhibited an increasing trend prior to the reform, with no significant change afterward. The proportion of inpatient visits at municipal hospitals also remained stable before and after the reform. In contrast, county hospitals experienced an increasing trend in discharges before the reform, followed by a decline post-reform, with their proportion also decreasing. Primary healthcare institutions saw no significant changes in absolute numbers, but their proportion of discharges declined before the reform and increased afterward. These observed differences primarily stem from variations in reimbursement rates for the same disease across different insurance types. Under the DIP payment, payment per case is determined by the product of case-mix points and the point value, with the latter varying according to the financing capacity of different insurance schemes. The point value is calculated by dividing the total regional budget by the sum of all case-mix points assigned to healthcare institutions within the region. Since the total budget is allocated separately based on the financing capacities of different insurance types, the global budget for UEBMI and URRBMI differs. Consequently, the same DIP group cases are subject to different reimbursement standards under these two insurance schemes.
Specifically, the financing capacity of URRBMI is relatively low, as it covers a broad population, including farmers, unemployed individuals, and other high-risk groups with a greater likelihood of illness.20,37 As a result, the reimbursement rates under URRBMI are generally lower than those of UEBMI. Conversely, UEBMI benefits from a higher financing capacity and a more substantial budget, allowing for significantly higher inpatient reimbursement rates (ie, post-hoc settlement prices) compared to URRBMI21 Given these disparities, healthcare institutions at all levels exhibit a clear strategic preference in patient selection. Due to the higher settlement prices associated with UEBMI, insured employees are prioritized for admission across different tiers of hospitals, ensuring stable revenue streams for healthcare providers. Consequently, the number and proportion of inpatient volumes among UEBMI patients remained largely unchanged before and after the reform. By contrast, URRBMI patients, subject to lower settlement prices, pose a higher financial risk for hospitals, necessitating more cautious admission policies. Municipal hospitals tend to admit patients with more severe conditions and higher case-mix index values to mitigate potential financial losses. Meanwhile, primary healthcare institutions benefit from the Primary DIP group “same city, same disease, same price” policy, which ensures that reimbursement rates for the Primary DIP group exceed actual treatment costs.38 This policy allows primary healthcare institutions to admit a substantial number of eligible lower-complexity cases while minimizing financial losses. In contrast, county hospitals lack similar policy protections and face substantial financial risks when admitting low-reimbursement URRBMI patients. To avoid revenue losses, county hospitals tend to minimize the admission of low-standard or non-medically justified inpatients under URRBMI. This strategic response directly contributes to a post-reform decline in both the absolute number and proportion of URRBMI discharges at county hospitals. Compared to primary healthcare institutions, county hospitals receive less policy support; and relative to municipal hospitals, they are less capable of attracting high-complexity, high-reimbursement cases. This dual disadvantage places county hospitals in a structurally weaker position under the DIP payment reform, potentially exacerbating their financial strain and limiting their capacity to provide equitable healthcare services.
While this study highlights the challenges and distributional effects of the DIP reform, it is important to acknowledge its potential positive goals, such as containing cost growth and incentivizing operational efficiency within hospitals. The key policy challenge lies in achieving these efficiency gains without undermining the viability of county-level providers or exacerbating inequities. To mitigate the adverse effects identified, it may be worth exploring policy options to support county hospitals—such as moderately expanding the number of primary DIP groups to guide less complex cases back to lower-tier institutions, or adjusting institutional coefficients to better reflect the constraints faced by county-level providers. However, such policy adjustments should be carefully evaluated against evidence and piloted to ensure alignment with the broader goals of cost containment and service equity.
This study offers several strengths. First, it utilizes a comprehensive dataset, encompassing 4,686,571 patient settlement records from all medical institutions in Z City between 2019 and 2022, which ensures the thoroughness of the evaluation. Moreover, the data is sourced from the Z City Medical Insurance Bureau, providing high-quality and reliable data. Second, a robust Interrupted Time Series Analysis (ITSA) approach is employed, allowing for a clear understanding of the reform’s impact on the outcome indicators. Third, the inclusion of heterogeneity analysis across different health insurance types offers a deeper, more granular perspective.
However, the study also has certain limitations. First, the relatively short study period limits the ability to assess the long-term effects of the reform. Second, the absence of a control group from non-reformed regions restricts the ability to make direct comparisons. Third, the focus on a single regional sample introduces concerns about the generalizability of the findings.
Conclusion
This study analyzes the impact of the DIP reform on level hospitals and their patient flow characteristics. The findings reveal that following the implementation of DIP, there has been a reduction in inpatient volume at county hospitals, with inpatient patients shifting toward municipal hospitals. From a systemic perspective, the DIP reform contributes to medical insurance budget control, but county hospitals have experienced a decline in total inpatient medical revenue, facing pressures from both patient attrition and revenue loss. Under the current DIP payment, county hospitals may face a dual “squeeze” dilemma: they are subjected to the diversion of patients by primary healthcare institutions while struggling to compete with the competitive advantages of municipal hospitals, leading to a cycle of “reduced service volume – decreased revenue – weakened capacity.” Due to the weakening of county-level hospitals, rural patients are confronted with increased financial burdens and reduced access to healthcare services. Critically, sustaining county hospitals is not only an economic issue but also a structural pillar for maintaining the stability of China’s tiered healthcare system. These findings suggest the need for policy refinements within the DIP framework, such as incorporating protective adjustment factors for county hospitals or expand the number of DIP primary groups that encourage them to serve local populations, thereby safeguarding healthcare equity and access in underserved areas.
Data Sharing Statement
The data supporting the findings of this study are available from the Medical Security Bureau information system in City Z. However, restrictions apply to the availability of these data, which were used under license for the current study and are therefore not publicly available. Data are however available from the corresponding author (Prof. Yingchun Chen) upon reasonable request and with permission of the Medical Security Bureau.
Ethics Approval and Consent to Participate
The study design was approved by the ethics institutional review board of Huazhong University of Science and Technology, Wuhan, China (approval number: 2022LSZ-S145). All the methods were carried out in accordance with relevant guidelines and regulations. The need for informed consent was waived by the ethics institutional review board of Huazhong University of Science and Technology because of the retrospective nature of the study. All authors confirm that this research caused no harm (physical or mental) to any participants. The research process complies with the Declaration of Helsinki. The health data was anonymously provided by the Medical Security Bureau in City Z.
Funding
YC were supported by National Natural Science Foundation of China (grant 72374076 to YC).
Disclosure
Huawei Tan is now affiliated with the Department of Labor and Social Security, School of Public Administration, Chongqing Technology and Business University, Chongqing, People’s Republic of China. The authors declare that there were no competing interests in this work.
References
1. Dieleman JL, Templin T, Sadat N, et al. National spending on health by source for 184 countries between 2013 and 2040. Lancet. 2016;387(10037):2521–15. doi:10.1016/S0140-6736(16)30167-2
2. Chang AY, Cowling K, Micah AE. Past, present, and future of global health financing: a review of development assistance, government, out-of-pocket, and other private spending on health for 195 countries, 1995-2050. Lancet. 2019;393(10187):2233–2260. doi:10.1016/S0140-6736(19)30841-4
3. McClellan M. Reforming payments to healthcare providers: the key to slowing healthcare cost growth while improving quality? J Econ Perspect. 2011;25(2):69–92. doi:10.1257/jep.25.2.69
4. Feldhaus I, Mathauer I. Effects of mixed provider payment systems and aligned cost sharing practices on expenditure growth management, efficiency, and equity: a structured review of the literature. BMC Health Serv Res. 2018;18(1):996. doi:10.1186/s12913-018-3779-1
5. Klein-Hitpaß U, Scheller-Kreinsen D. Policy trends and reforms in the German DRG-based hospital payment system. Health Policy. 2015;119(3):252–257. doi:10.1016/j.healthpol.2015.01.006
6. Hayashida K, Murakami G, Matsuda S, Fushimi K. History and profile of Diagnosis Procedure Combination (DPC): development of a real data collection system for acute inpatient care in Japan. J Epidemiol. 2021;31(1):1–11. doi:10.2188/jea.JE20200288
7. Cashin C, Langenbrunner J, O’Dougherty S. Designing and implementing health care provider payment systems: how-to manual. World Bank Publications; 2009.
8. Ginsburg PB. Achieving health care cost containment through provider payment reform that engages patients and providers. Health Aff. 2013;32(5):929–934. doi:10.1377/hlthaff.2012.1007
9. Chen B, Fan VY. Strategic provider behavior under global budget payment with price adjustment in Taiwan. Health Econ. 2015;24(11):1422–1436. doi:10.1002/hec.3095
10. Schmitz H. Practice budgets and the patient mix of physicians - the effect of a remuneration system reform on health care utilisation. J Health Econ. 2013;32(6):1240–1249. doi:10.1016/j.jhealeco.2013.09.013
11. Yip WC, Hsiao WC, Chen W, Hu S, Ma J, Maynard A. Early appraisal of China’s huge and complex health-care reforms. Lancet. 2012;379(9818):833–842. doi:10.1016/S0140-6736(11)61880-1
12. Zhang Y, Zhou Z, Si Y. When more is less: what explains the overuse of health care services in China? Soc sci med. 2019;232:17–24. doi:10.1016/j.socscimed.2019.04.018
13. Zhu Y, Zhao Y, Dou L, et al. The hospital management practices in Chinese county hospitals and its association with quality of care, efficiency and finance. BMC Health Serv Res. 2021;21(1):449. doi:10.1186/s12913-021-06472-7
14. Zhu M, Ou J. Thinking about the fairness of the convergence mechanism between medical insurance financing and treatment of Chinese residents. Chin Med Insurance. 2024; (02):47–59.
15. Wei Z, Bai J, Feng R. Optimization referral rate design for hierarchical diagnosis and treatment system based on accessibility-utilization efficiency bi-objective collaboration: a case study of China. Soc Sci Med. 2023;322:115827. doi:10.1016/j.socscimed.2023.115827
16. Ma Y, Zhang K. Medical insurance policy to promote graded diagnosis and treatment: mechanism and future path: based on the practice of medical reform in Dongguan City. Zhejiang J. 2024; (03):171–180.
17. Hou J, Ke Y. Addressing the shortage of health professionals in rural China: issues and progress comment on “Have health human resources become more equal between rural and urban areas after the new reform?”. Int J Health Policy Manag. 2015;4(5):327–328. doi:10.15171/ijhpm.2015.57
18. Liao Z. Institutional reasons for the difficult formation of graded diagnosis and treatment order in China. President Chin Hospital. 2020; (09):80–82.
19. Statistical bulletin of China’s health development in 2023: website of NHC; Available from: https://www.gov.cn/lianbo/bumen/202408/content_6971241.htm.
20. Zhu K, Zhang L, Yuan S, Zhang X, Zhang Z. Health financing and integration of urban and rural residents’ basic medical insurance systems in China. Int J Equity Health. 2017;16(1):194. doi:10.1186/s12939-017-0690-z
21. Lin K, Li Y, Yao Y, Xiong Y, Xiang L. The impact of an innovative payment method on medical expenditure, efficiency, and quality for inpatients with different types of medical insurance: evidence from a pilot city, China. Int J Equity Health. 2024;23(1):115. doi:10.1186/s12939-024-02196-2
22. Lai Y, Fu HQ, Li L, Yip W. Hospital response to a case-based payment scheme under regional global budget: the case of Guangzhou in China. Soc Sci Med. 2022;292:114601.
23. Qian M, Zhang X, Chen Y, Xu S, Ying X. The pilot of a new patient classification-based payment system in China: the impact on costs, length of stay and quality. Soc Sci Med. 2021;289:114415. doi:10.1016/j.socscimed.2021.114415
24. Lin K, Yao Y, Xiong Y, Xiang L. The effect of an innovative payment method on inpatient volume and bed resources and their regional distribution: the case of a central province in China. Int J Equity Health. 2024;23(1):159. doi:10.1186/s12939-024-02243-y
25. Shi H, Cheng Z, Liu Z, Zhang Y, Zhang P. Does a new case-based payment system promote the construction of the ordered health delivery system? Evidence from a pilot city in China. Int J Equity Health. 2024;23(1):55. doi:10.1186/s12939-024-02146-y
26. Zhang T, Lu B, Yan Z, Huang X, Lu W. Impacts of a new episode-based payment scheme on volume, expenditures, and efficiency in public hospitals: a quasi-experimental interrupted time-series study in Jinhua, China. Risk Manage Healthcare Policy. 2022;15:1659–1669. doi:10.2147/RMHP.S376516
27. Chen Y-J, Zhang X-Y, Tang X, Yan J-Q, Qian M-C, Ying X-H. How do inpatients’ costs, length of stay, and quality of care vary across age groups after a new case-based payment reform in China? An interrupted time series analysis. BMC Health Serv Res. 2023;23(1):160. doi:10.1186/s12913-023-09109-z
28. Shi H, Cheng Z, Cao Z. Does an innovative case-based payment scheme promote the hierarchical medical system? A tripartite evolutionary game analysis. Int J Equity Health. 2024;23(1):251. doi:10.1186/s12939-024-02336-8
29. P P. An interrupted time-series analysis to assess impact of introduction of. D - 101150314. (- 1179-1896 (Electronic)):- 515-23.
30. Iwok IA. Seasonal modeling of Fourier series with linear trend. Int J Statist Probabilit. 2016;5(6):65–72. doi:10.5539/ijsp.v5n6p65
31. G D, M D, S E. Analysis of interrupted time series mortality trends: an example to evaluate. D - 1254074. (- 0090-0036 38-46.
32. Wang R, Yan J, Zhang X, Qian M, Ying X. Impact of the diagnosis-intervention packet payment reform on provider behavior in china: a controlled interrupted time series study. Int J Health Policy Manag. 2024. doi:10.34172/ijhpm.8463
33. Zheng Y, Yuqing Z, Mengping Z, Jun L. Do hospitals need to establish multiple hospital districts? A hospital-based perspective on the benefits of scale. Front Public Health. 2023;11:1019331. doi:10.3389/fpubh.2023.1019331
34. Wörz M, Busse R. Analysing the impact of health-care system change in the EU member states--Germany. Health Econ. 2005;14(Suppl 1):S133–49. doi:10.1002/hec.1032
35. Li F, Sun R, Chen J, et al. Compensation policy and economic operation of public hospitals from 2015 to 2023: a case study of A City. Health Economic Res. 2024;41(12):7–11.
36. Luo C, Kuang P, Guo R, Xu L, HU Y. Analysis of economic operation of public hospitals in Wuhan. Soft Sci Health. 2025;39(1):67–72. doi:10.3969/j.issn.1003-2800.2025.01.013
37. Ren Y, Zhou Z, Cao D, et al. Did the integrated urban and rural resident basic medical insurance improve benefit equity in China? Value Health. 2022;25(9):1548–1558. doi:10.1016/j.jval.2022.03.007
38. Peng X, H TAN, Yang Q, ZHANG X, Bi S, Chen Y.Analysis of the influence of paying according to the value of disease on the number of inpatients and expenses in primary medical and health institutions. Health Develop Policy Res. 2024;27(02):142–147.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.